Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Latent Profile Analysis and Influencing Factors Associated with the Coping Styles of Dyspnea-Related Fear Among Patients with Chronic Obstructive Pulmonary Disease: A Multicenter Cross-Sectional Study
Authors Miao X ![]() , Jing S, Han Y
, Jing S, Han Y ![]() , Jin X, Gao T, Qian J, Zhao Q, Shen Y, Zhang B, Niu M
, Jin X, Gao T, Qian J, Zhao Q, Shen Y, Zhang B, Niu M
Received 1 May 2025
Accepted for publication 7 November 2025
Published 15 November 2025 Volume 2025:20 Pages 3737—3752
DOI https://doi.org/10.2147/COPD.S537900
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Xiaolang Miao,* Suxian Jing,* Yanxia Han,* Xiaoliang Jin, Tingting Gao, Jiale Qian, Qian Zhao, Ying Shen, Beilei Zhang, Meie Niu
Department of Pulmonary and Critical Care Medicine, the First Affiliated Hospital of Soochow University, Jiangsu, Suzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ying Shen, Department of Pulmonary and Critical Care Medicine, the First Affiliated Hospital of Soochow University, 899th, Pinghai Road, Suzhou, 215006, People’s Republic of China, Tel +86 13814889733, Email [email protected] Beilei Zhang, Department of Pulmonary and Critical Care Medicine, the First Affiliated Hospital of Soochow University, 899th, Pinghai Road, Suzhou, 215006, People’s Republic of China, Tel +86 15312178367, Email [email protected]
Purpose: To describe and analyze the potential profile characteristics associated with coping styles of dyspnea-related fear among patients with chronic obstructive pulmonary disease (COPD) and to explore the influencing factors of potential categories.
Patients and Methods: From March 2023 to August 2024, a cross-sectional study survey, involving 539 COPD patients from four tertiary hospitals, was conducted in Suzhou, China, by convenience sampling. The general information questionnaire, medical coping modes questionnaire, breathlessness beliefs questionnaire, 13-Beck depression inventory, revised COPD anxiety questionnaire, breathlessness catastrophizing scale, COPD self-efficacy scale and the modified medical research council dyspnea scale were employed for data collection. Latent profile analysis was performed to analyze the characteristics on coping styles of dyspnea-related fear among COPD patients, and logistic regression analysis was performed to explore the influencing factors of potential categories.
Results: Four profiles of coping styles of dyspnea-related fear were identified, designated as “low fear–confrontation (n = 151, 28.01%)”, “moderate-high fear–acceptance-resignation (n = 126, 23.38%)”, “moderate fear–confrontation (n = 160, 29.69%)”, and “high fear–avoidance (n = 102, 18.92%)”. Logistic regression analysis showed that disease duration, lung function, frequency of acute exacerbation during the previous year, depression, degree of dyspnea, anxiety, comorbidities and disease knowledge were factors influencing the coping styles of dyspnea-related fear in the different subgroups (P < 0.05).
Conclusion: There are obvious characteristic profiles on coping styles of dyspnea-related fear among patients with COPD, with differences in disease duration, frequencies of acute exacerbation, lung function, knowledge of COPD, comorbidity, degree of dyspnea, anxiety and depression across subgroups, which provide insight to identify and adopt early intervention strategies.
Keywords: COPD, coping style, dyspnea-related fear, depression, latent profile analysis
Introduction
Chronic obstructive pulmonary disease (COPD) is a heterogeneous lung condition characterized by persistent respiratory symptoms and airflow limitation and is a public health challenge worldwide, leading to the third highest mortality rate.1 Nearly 100 million people in China live with COPD.2 Dyspnea is the most common symptom in COPD. Almost 98% of the patients experienced dyspnea.3,4 The experience of dyspnea involves two components of breathlessness, dyspnea sensation (air hunger, work, tightness) and emotional reaction (dyspnea-related worry and fear). A previous study suggested that dyspnea-related fear could predict outcomes more than dyspnea sensation.5 Dyspnea-related fear is a dimension of dyspnea, which is an adaptive emotional response generated when an individual perceives the threat of dyspnea.6 It is the third factor hindering COPD patients’ participation in daily activities, which often occurs after breathlessness and fatigue.7 A previous cross-sectional study, conducted in China, revealed that catastrophizing breathlessness, anxiety, depression, self-efficacy, and body mass index (BMI) were important factors for dyspnea-related fear in COPD patients.8 Several qualitative studies demonstrated that fear of dyspnea in patients with COPD affected their coping strategies.9,10
Coping, a coping strategy, is the cognitive or behavioral regulation strategy adopted by individuals to manage different stressors. It has an important predictive role in disease cognition, physical and mental regulation, illness rehabilitation or progression, and even mortality.11 Some studies have argued that coping styles have both positive and negative response.12 A positive coping style, such as confrontation, responding to fear can improve the ability of patients living with chronic disease to solve difficulties, while a passive style (eg coping strategy as acceptance-resignation and avoidance) may increase their perceive of uncertainty about disease, reduce compliance with treatment and rehabilitation, further long-term avoidance will lead to “disease waste” state.12 Previous studies have focused on negative-avoidant coping styles for fear. Some avoiders avoid physical and social activities completely, which may lead to impaired function, increased loss of skeletal muscle, heavier dyspnea, and a vicious cycle of dyspnea, further decreasing the quality of life and resulting in a poor prognosis.13–15 In fact, patients with COPD adopted coping modes such as acceptance-resignation or confrontation although they were all at a higher level of dyspnea-related fear according to our interview results.9 Moreover, based on the Fear-Avoidance model, we found that virtual reality (VR) combined with cognitive behavioral therapy (CBT) may alleviate dyspnea-related fear, further decreasing avoidance behavior.16 However, the tool used to assess the level of dyspnea-related fear was unable to discriminate between grades of fear; therefore, we failed to implement individual interventions.
Latent profile analysis (LPA) is an “individual-centred” analysis method that divides individuals into different categories to determine their potential characteristics based on explicit reactions assessed by scales.17,18 Researchers can characterize potentially different subgroups of coping strategies for dyspnea-related fear among COPD patients using LPA, which could accurately identify target patients who require intervention.
The current study aimed to (1) describe the latent profile of coping styles of dyspnea-related fear among COPD patients and (2) explore the characteristics and influencing factors of different categories among different subgroups, to develop scientific and effective individualized coping strategies for dyspnea-related fear in patients with COPD.
Materials and Methods
Design
This is an exploratory cross-sectional study.
Participants
This study included the patients (Outpatients and inpatients) diagnosed with COPD who visited the medical institutions in Suzhou, Jiangsu province, China (The First Affiliated Hospital of Soochow University, the Second Affiliated Hospital of Soochow University, Suzhou Municipal Hospital, and Suzhou Xiangcheng People’s Hospital) by the convenience sampling, from March 2023 to August 2024. All the subjects met the following criteria:
The inclusion criteria were patients diagnosed with COPD based on the 2025 Global Initiative for Chronic Obstructive Lung Disease (GOLD);1 females and males aged ≥18 years who were well aware of their own conditions, and could complete the questionnaires independently or with the assistance of the researchers. The exclusion criteria were cognitive disorders, such as dementia and mental disorders, and those who were too severe to complete the questionnaires.
Sample Size
According to Kendall’s principle, the sample size was 10–20 times the number of independent variables in a cross-sectional survey.19 Moreover, Nylund-Gibson et al suggested that the sample size used to conduct LPA should be 300 cases at least.20
Data Collection
The survey was conducted face-to-face, using a paper-based questionnaire. The data collectors received special training on survey administration and implementation methods. If the subjects were unable to finish the questionnaire by themselves for some reasons, trained investigators provided assistance. After completing the questionnaires, the data collectors would check the papers on the spot. Missing over 10% or obvious logical errors were regarded as invalid. A total of 575 questionnaires were administered, of which 539 were deemed valid. The efficacy rate was 93.7%.
Measurement
General Information Questionnaire
A general information questionnaire was utilized to assess the patients’ demographic characteristics and clinical data, including age, gender, education (primary and below, junior, senior and above), marital status (married or else), BMI, income, payment method (medical insurance or else), smoking status (never, ever, or current), occupational status, self-evaluated economic burden, comorbidity (This study aimed to explore the coping styles for COPD patients of dyspnea-related fear, which mainly involved psychological disorders, and thus, the count of comorbidities excluded mental issues such as anxiety, depression that were listed separately later); stage of disease (stable or acute exacerbation), lung function (GOLD 1~4),1 disease duration, the frequency of acute exacerbation during last year and knowledge of COPD.
Medical Coping Modes Questionnaire
Medical Coping Modes Questionnaire (MCMQ) was used to measure coping strategies for dyspnea-related fear in patients with COPD, a 20-item instrument covering three domains: confrontation (8-item), avoidance (7-item), acceptance-resignation (5-item of Chinese version VS 4-item of original scale).21 Items are rated on a 4-grade from 1 to 4, and total scores of three subscales ranged 8–32, 7–28, 5–20 respectively, with a higher score on which subscale indicating that the patients were more likely to adopt this cope style. In this study, three subscales’ Cronbach’s α coefficients were 0.69, 0.60, and 0.76, and test–retest reliability were 0.66, 0.85, 0.69, respectively.22
Breathlessness Beliefs Questionnaire
Breathlessness Beliefs Questionnaire (BBQ) was an 11-item measurement tool encompassing two domains: activity avoidance (BBQ-AA) and somatic focus (BBQ-SF).23 The subscale of BBQ-SF consists 5 items was employed to assess the level of dyspnea-related fear. Items are rated on a 5-point Likert score from “strongly disagree” to “strongly agree”. Total scores rang from 5 to 25, with a higher score indicating more dyspnea-related fear. A Cronbach’s α coefficient of BBQ-SF was 0.62 when BBQ was validated in China,24 and achieved 0.83 in present study.8
Beck Depression Inventory-13
Beck Depression Inventory-13 (BDI-13),25 a short form of 13-item with focusing on emotion, cognition and physical symptoms, was utilized to assess the depression levels over past week. Items are rated on a 4-grade by 0 to 3, and the total scores rang from 0 to 39 (score >4 indicates depression), with a higher score indicating greater depression in patients with COPD. In this study, the scale’s Cronbach’s α coefficient was 0.91.26
Revised COPD Anxiety Questionnaire
The revised COPD Anxiety Questionnaire (CAF-R) was used to evaluate the COPD patients’ anxiety, a 25-item instrument covering six domains: fear of dyspnea, fear of physical activity, fear of progression, fear of social exclusion, sleep-related worries, and economic-related worries (this domain was added when introduced to China). Items are rated on a 5-grade from 0 (never) to 4 (always), and the total scores rang from 0 to 100, with a higher score indicating greater worry.27,28 The original scale’s Cronbach’s α coefficients ranged from 0.78 to 0.87. In current study, the CAF-R achieved Cronbach’s α coefficients ranging from 0.70 to 0.91, and test–retest reliability were from 0.84 to 0.90. Additionally, the CAF-R has a cutoff value of 50.5, with score >50.5 indicating anxiety.29
Breathlessness Catastrophizing Scale
Breathlessness Catastrophizing Scale (BCS),30 a single-dimensional scale with 13-item, was used to evaluate the degree of the breathlessness catastrophizing which was developed and revised by the pain catastrophizing scale (PCS). Items are rated on a 5-grade from 0 (never) to 4 (always). And the total scores rang from 0 to 52, with a higher score indicating greater catastrophizing. In present study, the scale’s Cronbach’s α coefficient was 0.96, and its test–retest reliability was 0.90.31
COPD Self-Efficacy Scale
COPD Self-efficacy Scale (CSES) was applied to assess the patients’ level of self-efficacy.32 The 31-item measure includes five domains: negative affect, intense emotional arousal, physical exertion, weather/environment and behavioral risk factors. Items are presented on a 5-piont Likert scale from “not at all confident” to “very confident”. Total scores rang from 31 to 155, with higher scores indicating higher self-efficacy. The CSES exhibited Cronbach’s α coefficients ranging from 0.66 to 0.85, respectively, and content validity ranging from 0.64 to 0.84 in this study.33
Modified Medical Research Council Dyspnea Scale
The modified Medical Research Council Dyspnea Scale (mMRC), widely used in worldwide, was employed to assess the severity of breathlessness in daily activities rated on a 5-piont scale, with a higher score suggesting heavier dyspnea.34
Statistical Analysis
Using Mplus 8.3 software to conduct LPA, starting from a single category model and gradually increasing the number of categories in the model until the best model fitting index reaches the model. The model fit index included Akaike information criteria (AIC), Bayesian information criteria (BIC), and sample size-adjusted BIC (aBIC). All three indices gradually decreasing indicated a better model fit. The entropy value ranged from 0 to 1, and the precision of the model classification was over 90% if the entropy was ≥0.8. If the P-value of Lo-Mendell-Rubin (LMR) and Bootstrap likelihood ratio test (BLRT) <0.05 indicated that the k-category model fits better than the k-1-category.35 Discriminant analysis was used to verify the accuracy of the optimal model in LPA.
Data were input by two researchers using Excel to ensure the accuracy, and processing and analysis was performed using the SPSS 25.0. The Kolmogorov–Smirnov (K-S) test was employed to assess the normality of continuous variables. Measurement data meeting the normal distribution was expressed as mean and standard deviation (SD), and one-way analysis of variance (ANOVA) was used for comparisons between multiple subgroups; otherwise, data were presented as median and interquartile range. Counting data was expressed as percentages, and compared between subgroups using Kruskal–Wallis tests, X2-test or Fisher’s exact probability. An unordered multivariate logistic regression analysis was applied to explore the factors influencing coping styles of dyspnea-related fear among the subgroups. Statistical significance was set at P ≤0.05 (two-sided tests).
Ethical Considerations
This study followed the ethical standards of the Declaration of Helsinki and was approved by the Ethics Committee of the First Affiliated Hospital of Soochow University (Ethical approval Nos. 2022251 and 2025169). All participants volunteered to participate in this study and signed informed consents form before the survey beginning.
Results
Participant Characteristics
A total of 539 COPD patients (male, n = 453 VS female, n = 86) were enrolled in this cross-sectional study, with ages ranging from 32 to 92 (71.15 ± 9.45) years. Of the patients, 80.9% (n = 436) were married, and 15.0% (n = 81) lived alone. Other details are provided in Table 1.
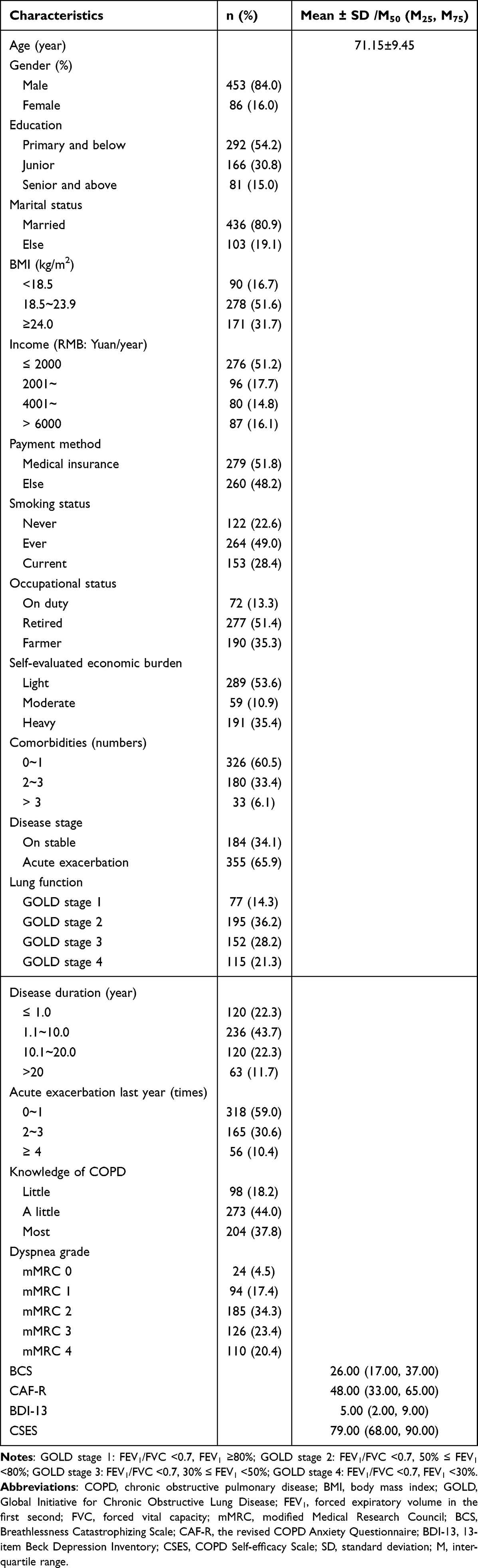 |
Table 1 Demographic and Clinical Characteristics of Patients with COPD (n = 539) |
As the variables measured by the questionnaires in this study were mainly self-reported by the patients themselves, Harman-univariate analysis was used to test for common method bias. The results showed that there were five factors with eigenvalues >1, and the variance contribution of the first factor was 41.87% (<50% recommended criteria), suggesting that there was no serious common method bias.36
The Kolmogorov–Smirnov test showed that the measurement data in present study was non-normally distributed. The MCMQ-confrontation score was [20.00 (15.00, 25.00)], MCMQ–avoidance [15.00 (11.00, 19.00)], MCMQ–acceptance-resignation [11.00 (7.00, 16.00)]. BBQ–SF score was [19.00 (17.00, 22.00)]. CAF-R was [48.00 (33.00, 65.00)], with a cutoff value of 50.5,29 and 46.0% (n = 248) of the subjects in this study lived with anxiety.
Latent Profiles of Coping Styles
The potential profile models of Categories 1–5 were fitted and analyzed, as shown in Table 2. As the number of categories increased, AIC, BIC, and aBIC values gradually decreased. The entropy values of models 2 to 5 were all greater than 0.8, but the P-values of LMR and BLRT were less than 0.05 in model 2 and 4. Given its practical significance, a model comprising four latent profiles was selected. The posterior probability of patients in each category belonging to each latent category in Model 4 was 0.958, 0.908, 0.901, and 0.951, indicating that the model was reliable with high discriminative power.37 Four subgroups were identified and accounted 28.0% (n = 151), 23.4% (n = 126), 29.7% (n = 160), and 18.9% (n = 102), respectively. The line plot was drawn to analyze the characteristics of the four potential categories of coping styles of dyspnea-related fear in COPD patients (Figure 1), which also conducted the names as “low fear–confrontation” (class-1), “moderate-high fear–acceptance-resignation” (class-2), “moderate fear–confrontation” (class-3), and “high fear–avoidance” (class-4).
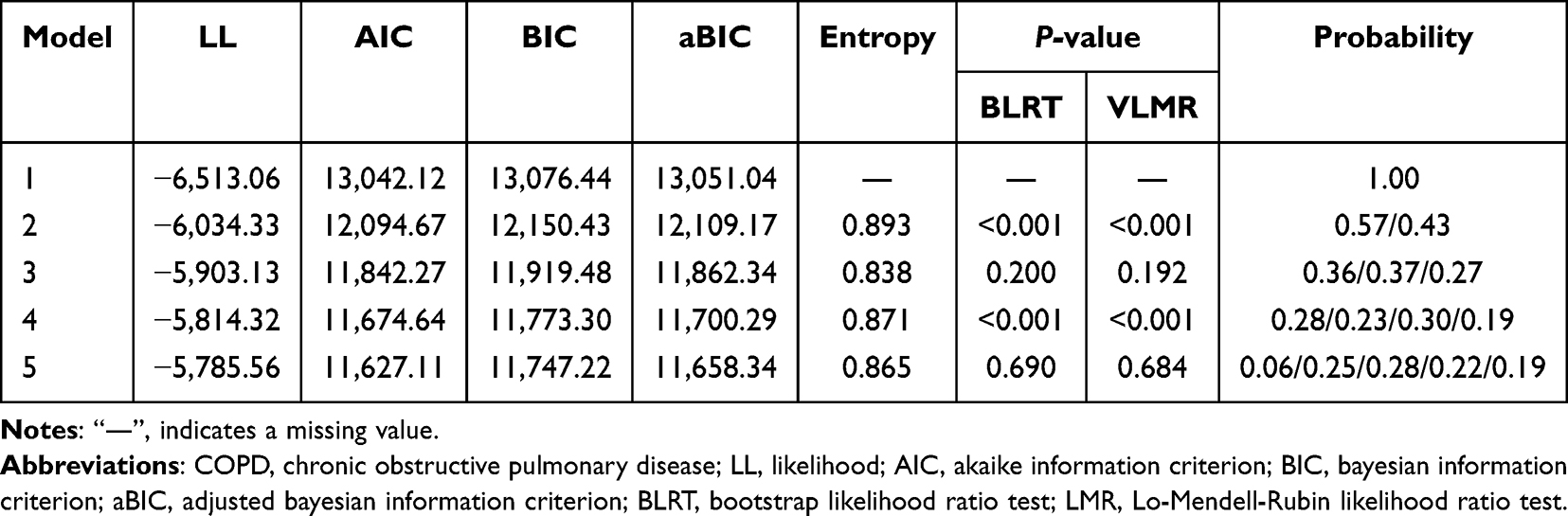 |
Table 2 Fit Indices of Latent Profile Analysis on Coping Styles of Dyspnea-Related Fear Among COPD (n = 539) |
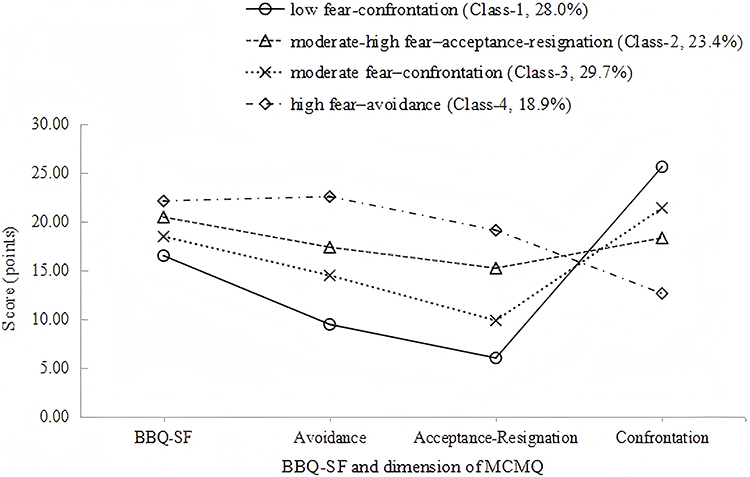 |
Figure 1 Characteristics of the four subgroups coping styles of dyspnea-related fear in COPD patients based on latent profile analysis results. Abbreviations: BBQ-SF, subscale of somatic focus of Breathlessness Beliefs Questionnaire; MCMQ, Medical Coping Modes Questionnaire. |
Sociodemographic and Characteristics of Each Latent Profile
Univariate analysis showed that the four potential coping styles of dyspnea-related fear had significant differences in age, education, BMI, income, smoking status, occupation, self-evaluated economic burden, comorbidities (except anxiety and depression), disease stage (stable/acute exacerbation), lung function, disease duration, frequencies of acute exacerbation during last year, knowledge of COPD (P <0.05). The details are listed in Tables 3 and 4.
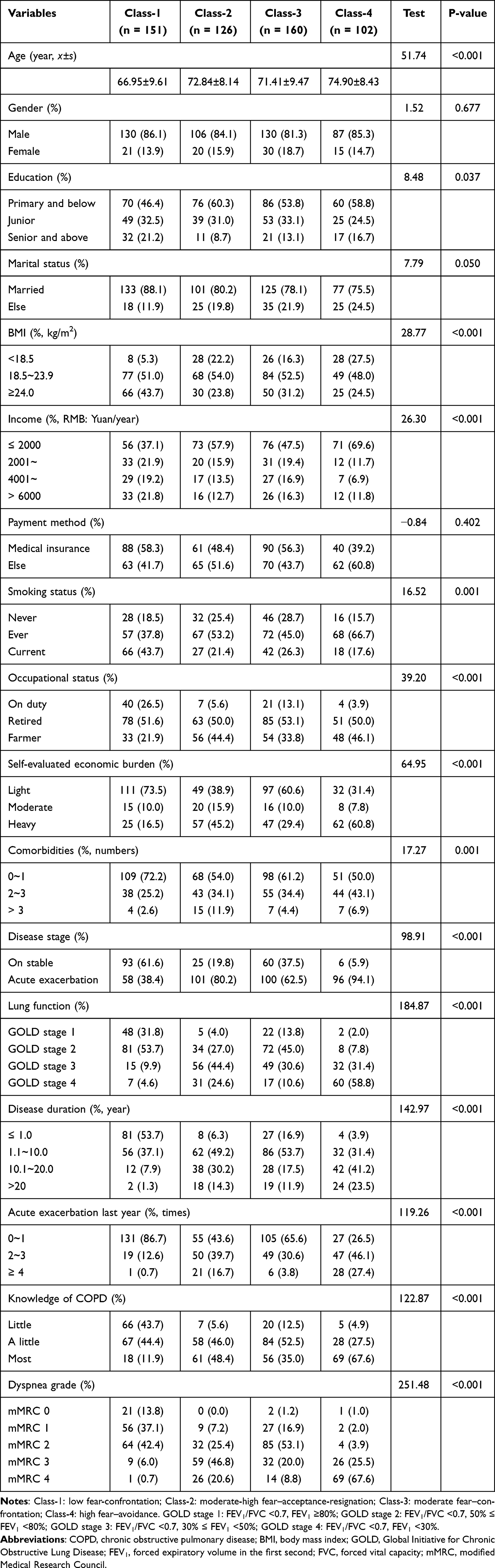 |
Table 3 Univariate Analysis of Latent Class Coping Styles of Dyspnea-Related Fear Among Patients with COPD |
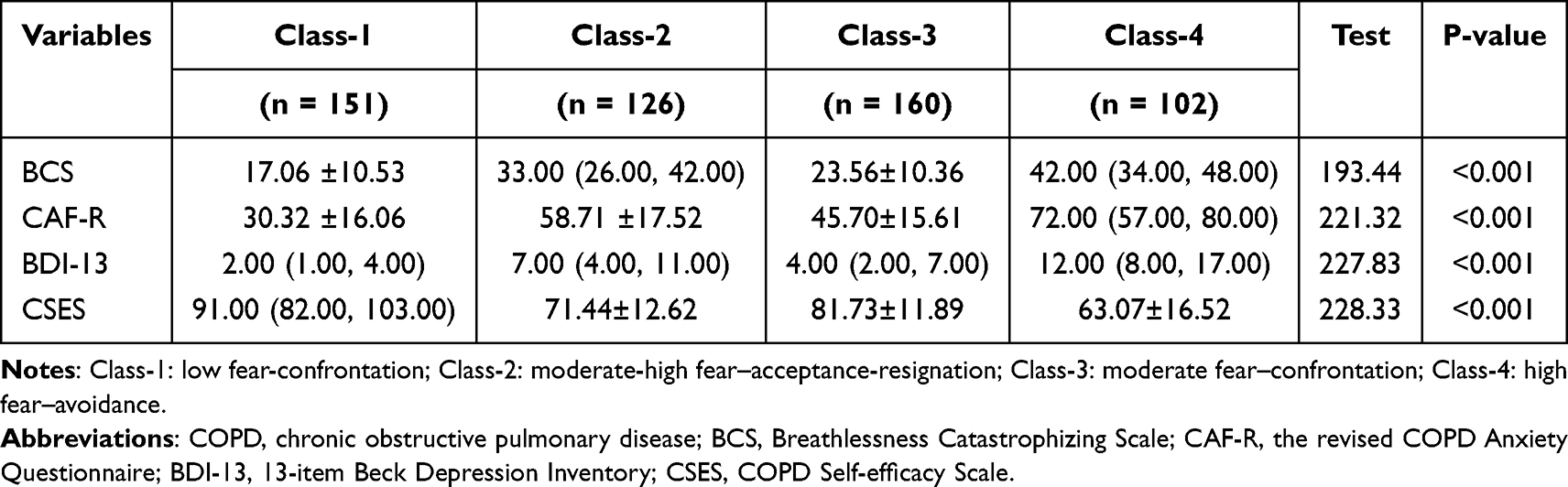 |
Table 4 Comparison of Main Independent Variables between the 4 Latent Class Coping Styles of Dyspnea-Related Fear Among Patients with COPD |
The category of low fear–confrontation (class-1) was used as the reference, the variables with statistical significance in the univariate analysis were taken as independent variables, and multiple logistic regression was constructed for further analysis. Moreover, because patients with dyspnea grades 0 and 1 of Class-2 and Class-4 presented rarely (n <3), the mMRC scored of 2 was chosen as the reference. Results indicated that, anxiety (OR=1.05, 95% CI=1.00~1.10), depression (OR=1.51, 95% CI=1.27~1.80), disease duration over one year but no more than ten years (OR=3.44, 95% CI=1.08~10.98), duration during 10.1~20 years (OR=8.82, 95% CI=2.18~35.73), duration over 20 years (OR=67.23, 95% CI=8.00~565.30), GOLD stage 3 (OR=8.74, 95% CI=1.71~44.53), knowing most knowledge (OR=15.73, 95% CI=3.28~75.37), knowing a little knowledge (OR=6.39, 95% CI=1.58~25.75), comorbidities ≥4 (OR=7.32, 95% CI=1.10~48.85), and grade-2 of dyspnea (OR=3.91, 95% CI=1.24~12.27) were more possible to be assigned into Class-2. Anxiety (OR=1.04, 95% CI=1.00~1.08), depression (OR=1.22, 95% CI=1.05~1.42), disease duration during 1.1~10 years, during 10.1~20 years, over 20 years [(OR=3.18, 95% CI=1.45~6.96), (OR=3.42, 95% CI=1.12~10.40), (OR=30.09, 95% CI=4.87~186.00)], knowing most knowledge (OR=4.45, 95% CI=1.49~13.35), and grade-0 of dyspnea (OR=0.09, 95% CI=0.01~0.65) were more likely to be assigned into Class-3. Depression (OR=1.67, 95% CI=1.39~2.02), disease duration from 10.1~20 years (OR=9.11, 95% CI=1.42~58.39), duration of >20 years (OR=81.62, 95% CI=6.61~1007.34), acute exacerbation during the last year ≥4 (OR=16.64, 95% CI=1.30~212.46), knowing most knowledge (OR=9.01, 95% CI=1.30~62.36), grade-3 of dyspnea (OR=13.30, 95% CI=2.75~64.27) and grade-4 (OR=106.75, 95% CI=7.96~1432.50) were positively associated with the allocation into Class-4. Details are presented in Table 5.
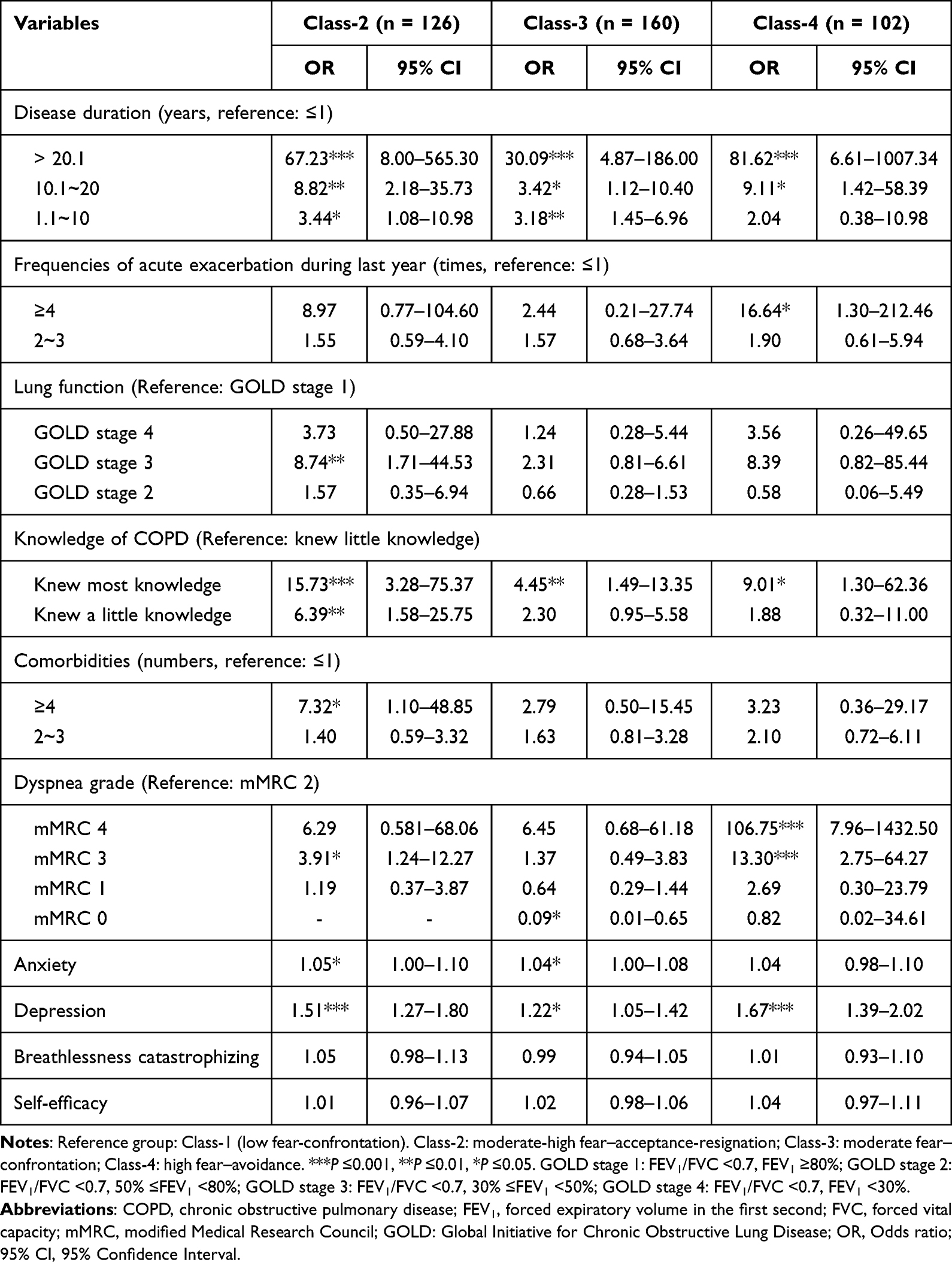 |
Table 5 Multiple Logistic Regression on Coping Styles of Dyspnea-Related Fear Among COPD Subgroups (n = 539) |
Discussion
Many previous studies have reported the coping styles of patients with COPD, but less known about coping with dyspnea-related fear.38–40 Existing studies have mainly focus on styles or damage of avoidance-coping facing fear of breathlessness during pulmonary rehabilitation,5 the current study focus on analyzing the coping strategies of dyspnea-related fear among COPD patients in daily life, using a person-centered approach of LPA. Four distinct categories were identified and named as “low fear–confrontation” (Class-1, 28.0%), “moderate-high fear–acceptance-resignation” (Class-2, 23.4%), “moderate fear–confrontation” (Class-3, 29.7%), and “high fear–avoidance” (Class-4, 18.9%), respectively, suggesting there was obvious heterogeneity in the coping styles of dyspnea-related fear. Patients in Class-1 and Class-3 showed the lower level in dyspnea-related fear, with BBQ-SF scores of [17.00 (15.00, 19.00)] and [18.00 17.00, 21.00)]. This may be attributed to their better educational level, normal BMI, higher socioeconomic status, fewer comorbidities, employed most and less farmer, shorter disease duration with less acute exacerbations, mild pulmonary function impairment and dyspnea, lower breathlessness catastrophic, less negative emotions, and higher self-efficacy, which enable them to better manage fear of dyspnea through proactive coping strategies. In contrast, patients in Class-4 showed the highest fear of dyspnea with a BBQ-SF score of [23.00 (20.00, 24.00)]. This group was characterized by the older, lower BMI, poorer socioeconomic status, more comorbidities, longer disease duration with more frequent acute exacerbations and most was under the stage of acute exacerbation, poorer pulmonary function, heavier dyspnea and severe breathlessness catastrophic, more negative emotions and lower self-efficacy, what led to a stronger inclination toward avoidance as a passive coping style. The level of dyspnea-related fear on Class-2 was positioned in the middle of Class-3 and Class-4, with a BBQ-SF score of [21.00 (18.00, 23.00)]. And the distributions of basic and disease characteristics were similar with this. Consistent with the previous study,41 this study found that socioeconomic status and psychological disorders influenced the patients’ coping strategies on dyspnea-related fear. Notably, the present study focused on the fact that dyspnea-related fear did not only lead to avoidance, but also could promote active-coping to some extent what was seen the trend of Class-3 in line chart. And this was the reason why “moderate fear–confrontation” was named. In fact, the previous qualitative studies had mentioned the finding.8,9 As such, in clinical nursing practice, the medical staff should evaluate the patients’ level of dyspnea-related fear early, analyze the impacts on the coping styles, further understand the patients’ socioeconomic status and psychological problems, so as to take personalized measures to promote patients’ good coping.
This study indicated that disease duration was a risk predictor for coping strategies for dyspnea-related fear, which was in line with a cross-sectional study conducted in China.8 One possible reason is that patients living with chronic airway disease are so common with dyspnea and experience times of exacerbation that have an excessive burden of symptoms and emotion, even giving up the coping strategy of confrontation.42 In addition, patients generally prefer confrontation as a coping tactic at the beginning of disease diagnosis, but acceptance-resignation in the process and avoidance in advanced stages, based on a qualitative study.9 This reminds us that healthcare should focus on patients with COPD at an early stage. Health institutions should pay special attention to the development and promotion of COPD prevention and treatment. Clinical medical staff should screen high-risk groups with the aim of early diagnosis, treatment, and rehabilitation to avoid irreversible impairments and passive coping strategies resulting from a prolonged course.
Acute exacerbation of COPD (AECOPD) over 4 times in last year was more likely to cope with “avoidance” in present study, consistent with a study conducted in Poland.43 The key symptom of AECOPD is increased dyspnea. A positive association between exacerbation and dyspnea-related fear was reported in a previous study.8 Avoidance is an adaptive coping strategy for acute injury. However, long-term avoidance will lead to the loss of skeletal muscles, increased risk of heavier dyspnea and fear, more acute exacerbations, and trapping patients into a vicious circle of dyspnea, dyspnea-related fear and avoidance,30,44,45 and even increase the mortality of advanced COPD.11 Hurst et al argued that acute exacerbations are more likely to occur in patients with heavier dyspnea,45 and further increasing the risk of more frequent severe exacerbations.46 Therefore, medical staff should pay attention to patients who more frequently experience acute exacerbations to detect and diagnose AECOPD early, and reduce the events of exacerbation.
Depression was correlated with coping styles of dyspnea-related fear in current study. Previous studies have shown that coping styles are significantly related to depression.47–49 A possible reason is that depressed patients feature a lack of confidence, lower physical energy levels and motivation, manifested as a slower response, rumination, which leads to passive coping styles.50 However, Yasinski et al argued that avoidance might increase depression.51 As we all know, depression is common on chronic illness, as an estimated prevalence of 8~80% in COPD patients.52 This findings highlight medical staff should screen for depression disorders in COPD patients early, look for influencing factors, and take measures to reduce the level of depression, such as cognitive interventions, virtual reality (VR), and artificial intelligence (AI)53 to improve their coping with the fear of dyspnea.
Compared with Class-1, anxiety was a protective factor in Class-2 and Class-3. A meta-analysis argued that psychological disorders such as anxiety may increase avoidance; in turn, coping styles of avoidance exacerbated anxiety in individuals with chronic illnesses of rheumatoid arthritis. Their relationship was bidirectional.49 Surprisingly, anxiety showed no statistically significant effect on the comparison between Clss-4 and Class-1, which may be related to the different findings about anxiety influencing coping styles in previous studies, or it may be that the mediating role of some variable diluted the effect of anxiety on them. Given the few studies conducted on coping strategies of dyspnea-related fear among patients with COPD, further research is required.
Regarding disease-related knowledge, the study found the more patients knew, the more likely to response negatively. It seems incredibly. However, patients with more knowledge may cope well with acceptance-resignation because of lower expectations of recovery.21 They may avoid coping with life-threatening situations caused by breathlessness, further learning and reinforcement. Based on these experiences, avoidance coping is often employed as a strategy for non-life-threatening patients with chronic illnesses. This confirms the double-sided effects of avoidance of dyspnea-related fear on health promotion of patients with COPD. Thereby, patients should be instructed to dynamically evaluate avoidance and to choose adaptive coping styles in different situations. Nevertheless, the level of disease knowledge was evaluated by patients’ self-reports rather than an objective questionnaire, which may have caused bias in the results. And a specific questionnaire about disease knowledge is looked for in the future.
Multiple logistic regression analysis showed that compared with Class-1, dyspnea grades 3–4 were a protective factor for Class-4. The fear-avoidance model explains the relationship between pain-related fear and avoidance in patients with chronic back pain,12 and Zhu et al verified its application in patients with COPD.54 Another study also showed that individuals with higher dyspnea among COPD focused more on perceived dyspnea, which increased dyspnea-related fear and adopted avoidant strategies.6 PR is recommended for patients with COPD to improve dyspnea and related mood.1 As such, individualized PR maybe an effective measure to help patients cope with dyspnea-related fear.
Patients with grade of Gold 3, comorbidities over 4 were more likely to belong to the moderate-high fear–acceptance-resignation subgroup. Similar findings from a qualitative study from the UK showed that comorbidity and lung function are factors influencing coping strategies.55 A possible reason is that patients with COPD are older, with a mean age are (71.15±9.45) years in this study, and they have many comorbidities that are incurable. Moreover, the limited pulmonary function in patients with COPD is irreversible. These factors resulted in they were used to their symptoms and cope with acceptance-resignation. This highlights the importance of early prevention and recovery from chronic diseases.
Limitations
This study has several limitations. First of all, it must be mentioned that only 16% female was included in present study, although gender was not statistically significant. It should be noted that, there is indeed a situation in the southern region of the Chinese mainland, where the reported prevalence of COPD among women is lower than that among men. However, this portion is lower than the study conducted by Yang et al (female account for 24%) from China.56 The difference might be attributed to the study requires subjects who can write or communicate with data collectors orally. As patients, especially the elderly women live in Suzhou, are low educated that used to speak dialects and cannot write mostly, which are barriers for communication leading to the exclusion. This might be contributed to selection bias. Regional characteristics should be taken into account when recruiting data collectors to enlarge the portion of female sample for a more balance representation in the future. Second, the questionnaires were all self-reported by the patients themselves, which increased the risk of common method bias, and even if many measures such as statistical method were taken to control the quality, further objective methods might be expected. Third, the presence of extreme values when logistic regression analysis was conducted among inter-group comparisons (i.g. GOLD stage, dyspnea grade), reduced the stability and representation, potentially leading to result bias such as false positives. Thereby, the findings of the study should be reviewed with caution and be interpreted with the sample’s clinical characteristics. More researches with large sample sizes, robust statistical methods, and repeated sampling are expected to reduce the influence of extreme values and improve the reliability of conclusions in the future. Finally, a cross-sectional design limits causal inferences, future prospective, longitudinal studies should be conducted to explore the dynamically trajectories on coping styles of dyspnea-related fear among patients with COPD, so as to clarify the causal relationships.
Conclusion
This study revealed heterogeneity on coping styles of dyspnea-related fear among patients with COPD, which was classified into four latent profiles, named as “low fear–confrontation”, “moderate-high fear–acceptance-resignation”, “moderate fear–confrontation” and “high fear–avoidance”, respectively. Disease duration, lung function, frequency of acute exacerbation during the last year, knowledge of COPD, comorbidities, dyspnea, anxiety, and depression were the factors influencing coping styles of dyspnea-related fear in the subgroups. Additionally, the study focuses on the fact that some level fear of dyspnea promote positive coping besides avoidance, which provides a novel perspective for future management of dyspnea-related fear. Medical staff should assess the level of fear in patients with COPD, identify the individual characteristics on coping styles of dyspnea-related fear early, explore influencing factors, and develop tailored interventions to improve coping strategies.
Abbreviations
COPD, chronic obstructive pulmonary disease; BMI, body mass index; VR, virtual reality; CBT, cognitive behavioral therapy; LPA, Latent profile analysis; GOLD, Global Initiative for Chronic Obstructive Lung Disease; MCMQ, Medical Coping Modes Questionnaire; BBQ, Breathlessness Beliefs Questionnaire; BBQ-AA, subscale of activity avoidance of BBQ; BBQ-SF, subscale of somatic focus of BBQ; BDI, Beck Depression Inventory; CAF-R, the Revised COPD Anxiety Questionnaire; BCS, Breathlessness Catastrophizing Scale; PCS, Pain Catastrophizing Scale; CSES, COPD Self-efficacy Scale; mMRC, the modified Medical Research Council Dyspnea Scale; AIC, Akaike information criteria; BIC, Bayesian information criteria; aBIC, adjust BIC; LMR, Lo-Mendell-Rubin; BLRT, Bootstrap likelihood ratio test; SD, standard deviation; OR, Odds ratio; CI, Confidence Interval; AECOPD, Acute exacerbation of COPD; AI, artificial intelligence. FEV1, forced expiratory volume in the first second; FVC, forced vital capacity.
Data Sharing Statement
Researchers may request the corresponding author (Ying Shen) and the co-author (Yanxia Han, [email protected]) for the datasets used in this study.
Ethics Approval and Consent to Participate
The study protocol was approved by the Ethics Committee of the First Affiliated Hospital of Soochow University, Suzhou, China (Ethical approval Nos. 2022251 and 2025169). This study strictly followed the principles of informed consent of research subjects. The purpose, significance, benefits, and risks of the study were explained in detail to the subjects, who were informed of the principle of voluntariness and confidentiality. The study was conducted after obtaining consent from the subjects.
Acknowledgments
We thank all the participants involved in this research project. We thank the staff at the First Affiliated Hospital of Soochow University, Second Affiliated Hospital of Soochow University, Suzhou Municipal Hospital, and Suzhou Xiangcheng People’s Hospital for their assistance in collecting the questionnaires.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work followed the ethical standards of the Declaration of Helsinki and was supported by the National Natural Science Foundation of China (Grant No: 72204182), Suzhou Science and Technology Development Plan Project (Grant No: SKY2022122), and “Zhou Shi” project of the First Affiliated Hospital of Soochow University (Grant No: HLYJ-Z-202512).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Global Initiative For Chronic Obstructive Lung Disease. Global strategy for prevention, diagnosis and management of COPD: 2025 report. 2025. Available from: https://goldcopd.org/2025-gold-report/.
2. Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. doi:10.1016/S0140-6736(18)30841-9
3. Miravitlles M, Murio C, Tirado-Conde G, et al. Geographic differences in clinical characteristics and management of COPD: the EPOCA study. Int J Chronic Obstr. 2008;3(4):803–814. doi: 10.2147/copd.s4257
4. Schloesser K, Bergmann A, Eisenmann Y, et al. Only I know now, of course, how to deal with it, or better to deal with it: a mixed methods phase II study of a cognitive and behavioral intervention for the management of episodic breathlessness. J Pain Symptom Manag. 2022;63(5):758–768. doi:10.1016/j.jpainsymman.2021.11.003
5. Janssens T, De Peuter S, Stans L, et al. Dyspnea Perception in COPD: association between anxiety, dyspnea-related fear, and dyspnea in a pulmonary rehabilitation program. Chest. 2011;140(3):618–625. doi:10.1378/chest.10-3257
6. Benke C, Krause E, Hamm AO, et al. Predictors of behavioral avoidance during respiratory symptom provocation. Behav Res Ther. 2019;112:63–67. doi:10.1016/j.brat.2018.11.012
7. Michalovic E, Jensen D, Dandurand RJ, et al. Description of participation in daily and social activities for individuals with COPD. COPD. 2020;17(5):543–556. doi:10.1080/15412555.2020.1798373
8. Miao X, Niu M, Han Y, et al. Influencing factors and the pathway analysis of dyspnea-related fear in patients with chronic obstructive pulmonary disease. J Nurs Sci. 2024;39(18):37–41+47. doi:10.3870/j.issn.1001-4152.2024.18.037
9. Miao X, Niu M, Han Y, et al. Experiences and coping styles of dyspnea-related fear among patients with chronic obstructive pulmonary disease: A qualitative research. Chin J Nurs. 2023;58(15):1815–1820. doi:10.3761/j.issn.0254-1769.2023.15.004
10. Sigurgeirsdottir J, Halldorsdottir S, Arnardottir RH, et al. COPD patients’ experiences, self-reported needs, and needs-driven strategies to cope with self-management. Int J Chron Obstruct Pulmon Dis. 2019;14:1033–1043. doi:10.2147/COPD.S201068
11. Moskowitz JT, Folkman S. Coping: pitfalls and Promise. Annu Rev Psychol. 2004;55(1):745–774. doi:10.1146/annurev.psych.55.090902.141456
12. Lethem J, Slade PD, Troup JD, et al. Outline of a fear-avoidance model of exaggerated pain perception—I. Behav Res Ther. 1983;21(4):401–408. doi:10.1016/0005-7967(83)90009-8
13. Carrieri-Kohlman V, Donesky-Cuenco D, Park SK, et al. Additional evidence for the affective dimension of dyspnea in patients with COPD. Res Nurs Health. 2010;33(1):4–19. doi:10.1002/nur.20359
14. Livermore N, Sharpe L, McKenzie D. Catastrophic interpretations and anxiety sensitivity as predictors of panic-spectrum psychopathology in chronic obstructive pulmonary disease. J Psychosom Res. 2012;72(5):388–392. doi:10.1016/j.jpsychores.2012.02.001
15. Donesky D, Nguyen HQ, Paul SM, et al. The affective dimension of dyspnea improves in a dyspnea self-management program with exercise training. J Pain Symptom Manag. 2014;47(4):757–771. doi:10.1016/j.jpainsymman.2013.05.019
16. Lu X, Niu M, Han Y, et al. Development of a virtual reality-based fear of dyspnea adaptation program for patients with chronic obstructive pulmonary. Mil Nurs. 2023;40(09):52–55,91. doi:10.3969/j.issn.2097-1826.2023.09.013
17. Wang M, Li D, Li J, et al. Professional competencies in geriatric nursing for geriatric nurses: a latent profile analysis. Bmc Nurs. 2024;23(1):512. doi:10.1186/s12912-024-02157-8
18. Lanza ST, Rhoades BL. Latent class analysis: an alternative perspective on subgroup analysis in prevention and treatment. Prev Sci. 2013;14(2):157–168. doi:10.1007/s11121-011-0201-1
19. Jin M, Qian R, Wang J, et al. Influencing factors associated with mental workload among nurses: a latent profile analysis. Int J Nurs Sci. 2024;11(3):330–337. doi:10.1016/j.ijnss.2024.04.002
20. Nylund-Gibson K, Garber AC, Carter DB, et al. Ten frequently asked questions about latent transition analysis. Psychol Methods. 2023;28(2):284–300. doi:10.1037/met0000486
21. Feifel H, Strack S, Tong NV. Coping strategies and associated features of medically III patients. Psychosom Med. 1987;49(6):616–625. doi:10.1097/00006842-198711000-00007
22. Shen X, Jiang Q. Report on application of Chinese version of MCMQ in701patients. Chin J Behav Med Sci. 2000;9(01):22–24.
23. De Peuter S, Janssens T, Van Diest I, et al. Dyspnea-related anxiety: the Dutch version of the breathlessness beliefs questionnaire. Chron Resp Dis. 2011;8(1):11–19. doi:10.1177/1479972310383592
24. Wu Q, Guo A, Zhao Y, et al. Reliability and validity of the Chinese version of the breathlessness beliefs questionnaire. Chron Resp Dis. 2018;15(2):114–122. doi:10.1177/1479972317715551
25. Beck AT, Rial WY, Rickels K, et al. Short form of depression inventory: cross-validation. Psychol Rep. 1974;34(3):1184–1186. doi:10.1177/003329417403403s01
26. Guo Y, Gao Y, Tian Y, et al. Negative emotion, level of hope of patients treated with VA-ECMO and their correlation. J Guizhou Med Univ. 2021;46(12):1414–1420. doi:10.19367/.j.cnki.2096-8388.2021.12.009
27. Kühl K, Kuhn C, Kenn K, et al. Der COPD-Angst-Fragebogen (CAF): ein neues Instrument zur Erfassung krankheitsspezifischer Ängste bei COPD-Patienten [The COPD-Anxiety-Questionnaire (CAF): a new instrument to assess illness specific anxiety in COPD patients]. Psychother Psych Med. 2011;61(1):e1–9. doi:10.1055/s-0030-1248281
28. Keil DC, Stenzel NM, Kühl K, et al. The impact of chronic obstructive pulmonary disease-related fears on disease-specific disability. Chron Resp Dis. 2014;11(1):31–40. doi:10.1177/1479972313516881
29. Miao X, Han Y, Wu Z, et al. Reliability, validity, modification and expansion of the Chinese version of the disease-specific anxiety questionnaire for chronic obstructive pulmonary disease. Int J Chronic Obstr. 2024;19:1047–1060. doi:10.2147/COPD.S455171
30. Solomon BK, Wilson KG, Henderson PR, et al. A breathlessness catastrophizing scale for chronic obstructive pulmonary disease. J Psychosom Res. 2015;79(1):62–68. doi:10.1016/j.jpsychores.2014.11.020
31. Lu X, Niu M, Jin X, et al. Translation and validation of the Chinese version of the Breathlessness Catastrophizing scale inpatients with COPD. J Nurs Sci. 2024;39(09):52–55. doi:10.3870/j.issn.1001-4152.2024.09.052
32. Wigal JK, Creer TL, Kotses H. The COPD self-efficacy scale. Chest. 1991;99(5):1193–1196. doi:10.1378/chest.99.5.1193
33. Wong K, Wong F, Chan M. Effects of nurse-initiated telephone follow-up on self-efficacy among patients with chronic obstructive pulmonary disease. J Adv Nurs. 2005;49(2):210–222. doi:10.1111/j.1365-2648.2004.03280.x
34. Mahler DA, Wells CK. Evaluation of clinical methods for rating dyspnea. Chest. 1988;93(3):580–586. doi:10.1378/chest.93.3.580
35. Huang GH, Wang SM, Hsu CC. Optimization-based model fitting for latent class and latent profile analyses. Psychometrika. 2011;76(4):584–611. doi:10.1007/s11336-011-9227-3
36. Podsakoff PM, MacKenzie SB, Lee J, et al. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol. 2003;88(5):879–903. doi:10.1037/0021-9010.88.5.879
37. Wen Z, Xie J, Wang H. Principles, steps and procedures of the latent profile model. J East Normal Univ. 2023;41(01):1–15. doi:10.16382/j.cnki.1000-5560.2023.01.001
38. Stoilkova-Hartmann A, Franssen FME, Augustin IML, et al. COPD patient education and support - achieving patient-centredness. Patient Educ Couns. 2018;101(11):2031–2036. doi:10.1016/j.pec.2018.05.024
39. Mesquita R, Da Silva GPF, Do Nascimento FAB, et al. Religiosity and religious coping in patients with COPD: a cross-sectional comparison between Brazil and the Netherlands and associations with physical and psychological health. J Relig Health. 2022;61(5):4039–4050. doi:10.1007/s10943-021-01341-3
40. Stoilkova A, Janssen DJ, Franssen FM, et al. Coping styles in patients with COPD before and after pulmonary rehabilitation. Resp Med. 2013;106(6):825–833. doi:10.1016/j.rmed.2013.03.001
41. Yuet LM, Alexander M, Chun CJ. Coping and adjustment in Chinese patients with chronic obstructive pulmonary disease. Int J Nurs Stud. 2002;39(4):383–395. doi:10.1016/S0020-7489(01)00036-0
42. Tabała K, Wrzesińska M, Stecz P, et al. Personality traits, level of anxiety and styles of coping with stress in people with asthma and chronic obstructive pulmonary disease - a comparative analysis. Psychiatr Pol. 2016;50(6):1167–1180. doi:10.12740/PP/62726
43. Müllerová H, Shukla A, Hawkins A, et al. Risk factors for acute exacerbations of COPD in a primary care population: a retrospective observational cohort study. BMJ Open. 2014;4(12):e006171. doi:10.1136/bmjopen-2014-006171
44. Han Y, Wu Z, Zhao Q, et al. Association between anthropometric indices and skeletal-muscle atrophy in Chinese patients with stable chronic obstructive pulmonary disease: a cross-sectional study. Int J Chronic Obstr. 2022;17:2529–2539. doi:10.2147/COPD.S373880
45. Hurst JR, Skolnik N, Hansen GJ, et al. Understanding the impact of chronic obstructive pulmonary disease exacerbations on patient health and quality of life. Eur J Intern Med. 2020;73:1–6. doi:10.1016/j.ejim.2019.12.014
46. Zhang J, Chen F, Wang Y, et al. Early detection and prediction of acute exacerbation of chronic obstructive pulmonary disease. Chin Med J. 2023;1(2):102–107. doi:10.1016/j.pccm.2023.04.004
47. Ozsaker E, Atila N. Depression, anxiety, stress levels, and coping styles of caregivers of patients with left ventricular assist device. Perspect Psychiatr C. 2022;58(4):2414–2422. doi:10.1111/ppc.13076
48. Chen C, Zhou Y, Wang D, et al. Anxiety, depression, and coping styles among patients with chronic pancreatitis in East China. Bmc Psychiatry. 2023;23(1):212. doi:10.1186/s12888-023-04691-2
49. Sirois FM, Hinch R. A meta‐analysis of coping strategies and psychological distress in rheumatoid arthritis. Brit J Health Psych. 2024;29(3):771–787. doi:10.1111/bjhp.12726
50. Yohannes AM, Murri MB, Hanania NA, et al. Depressive and anxiety symptoms in patients with COPD: a network analysis. Resp Med. 2022;198:106865. doi:10.1016/j.rmed.2022.106865
51. Yasinski C, Hayes AM, Ready CB, et al. Processes of change in cognitive behavioral therapy for treatment-resistant depression: psychological flexibility, rumination, avoidance, and emotional processing. Psychother Res. 2020;30(8):983–997. doi:10.1080/10503307.2019.1699972
52. Martínez-Gestoso S, García-Sanz M, Carreira J, et al. Impact of anxiety and depression on the prognosis of COPD exacerbations. BMC Pulm Med. 2022;22(1):169. doi:10.1186/s12890-022-01934-y
53. Spiegel BMR, Liran O, Clark A, et al. Feasibility of combining spatial computing and AI for mental health support in anxiety and depression. Npj Digit Med. 2024;7(1):22. doi:10.1038/s41746-024-01011-0
54. Zhu XM. Status and Influence Factors of Breathlessness Beliefs of Patients with Chronic Obstructive Pulmonary Disease. Yangtze University; 2019.
55. Brien SB, Lewith GT, Thomas M. Patient coping strategies in COPD across disease severity and quality of life: a qualitative study. Npj Prim Care Resp M. 2016;26:16051. doi:10.1038/npjpcrm.2016.51
56. Yang M, Wang Z, Zhao Y, et al. Association of patient-reported outcome patterns and major clinical factors with frailty in stable COPD. Int J Chronic Obstr. 2025;20:1927–1937. doi:10.2147/COPD.S517270
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The COPD Assessment Test (CAT) and Depression: A Longitudinal Analysis During the COVID-19 Pandemic
Beech A, Singh D
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1187-1195
Published Date: 13 June 2023
Anxiety and Depression Among US Nursing Home Residents with Chronic Obstructive Pulmonary Disease
Osundolire S, Goldberg RJ, Lapane KL
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1867-1882
Published Date: 28 August 2023
Path Analysis of Self-Efficacy, Coping Style and Resilience on Depression in Patients with Recurrent Schizophrenia
Wang L, Li M, Guan B, Zeng L, Li X, Jiang X
Neuropsychiatric Disease and Treatment 2023, 19:1901-1910
Published Date: 1 September 2023
Exploring Patterns of COPD Exacerbations and Comorbid Flare-Ups
van Dijk SHB, Brusse-Keizer MGJ, Effing T, van der Valk PDLPM, Ploumen EH, van der Palen J, Doggen CJM, Lenferink A
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2633-2644
Published Date: 16 November 2023
Efficacy and Safety of Escitalopram in Alleviating Depression and Anxiety Symptoms in COPD Patients: A Randomized Double-Blind Placebo-Controlled Trial
Gao Z, Tang S, Zhang W, Zhang M, Wei Z, Long Z, Wang B, Qin H, Qian H, Yin Y, Wang G, He B
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:572465
Published Date: 7 February 2026