Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Knowledge, Attitudes, and Practices Toward Microvascular Decompression for Hemifacial Spasm Among Neurosurgeons: A Multicenter Cross-Sectional Study
Authors Xu Y, Dong S, Zhao R, Liu J, Han P, Guo Y, Jiang R
Received 25 June 2025
Accepted for publication 18 December 2025
Published 27 December 2025 Volume 2025:18 Pages 8277—8291
DOI https://doi.org/10.2147/JMDH.S549601
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Veronica Swallow
Yinfu Xu,1,2,* Shiying Dong,1,* Ruichen Zhao,1 Jie Liu,2 Peijun Han,2 Yuchen Guo,2 Rongcai Jiang1,3
1Department of Neurosurgery, Tianjin Neurological Institute, State Key Laboratory of Experimental Hematology, Laboratory of Post‐Neuroinjury Neurorepair and Regeneration in Central Nervous System, Tianjin & Ministry of Education, Tianjin Medical University General Hospital, Tianjin, People’s Republic of China; 2Department of Neurosurgery, The Second People’s Hospital of Liaocheng, Linqing, Shandong, People’s Republic of China; 3Department of Neurosurgery, Xuanwu Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Rongcai Jiang, Email [email protected]
Objective: Hemifacial spasm (HFS) is a rare but significantly impactful neuromuscular disorder that affects patients’ quality of life, yet research on healthcare providers’ readiness to manage this condition remains limited. This study aims to investigate the knowledge, attitudes, and practices (KAP) toward microvascular decompression (MVD) for HFS among neurosurgeons.
Methods: This multicenter cross-sectional study was conducted between May and June 2024, involving multiple institutions across Eastern China. Data were collected through a structured questionnaire, which included sociodemographic information and KAP scores of participants.
Results: A total of 223 valid questionnaires were collected, 218 (97.76%) were males. Multivariable logistic regression analysis found that both higher knowledge scores (P = 0.013) and attitude scores (P = 0.001) were independently associated with positive practice. Path analysis showed that the presence of neurosurgical microsurgery equipment and instruments (P = 0.025), title (P < 0.001), past experience in diagnosis and treatment of HFS (P < 0.001), and past experience in MVD surgery for HFS (P < 0.001) had direct effects on knowledge. Knowledge (P < 0.001) had a direct effect on attitude. Further, knowledge (P < 0.001) and attitude (P < 0.001) had direct effects on practice.
Conclusion: Based on these findings, we recommend prioritizing the establishment of well-equipped surgical facilities, developing structured training programs that particularly benefit less experienced surgeons, and implementing regular assessment and education initiatives to enhance both knowledge and attitudes among neurosurgeons performing MVD procedures.
Keywords: hemifacial spasm, microvascular decompression, knowledge, attitudes, practices, neurosurgeons, cross-sectional study
Introduction
Hemifacial spasm (HFS) is a rare motor disorder characterized by intermittent, involuntary tonic and clonic contractions of unilateral facial muscles. The most common etiology for HFS is compression of the facial nerve at its root exit zone by an arterial or venous loop.1 Although HFS is not life-threatening, the chronic facial twitching can cause significant social embarrassment and impair social interactions, potentially leading to psychiatric comorbidities.2,3 The primary medical treatment for HFS is the injection of botulinum neurotoxin, which offers effective but temporary symptom relief.4 The use of anticonvulsant drugs is limited by their side effects and low efficacy.5
Microvascular decompression (MVD) surgery is a well-established treatment for HFS. MVD aims to alleviate the vascular compression of the centrally myelinated portion of the facial nerve, addressing one of the possible etiologies and pathological mechanisms of the disorder.6 Advances in microsurgical techniques and neuromonitoring have enabled neurosurgeons to increase the cure rate of MVD to over 90% while significantly reducing the rate of complications that could result in permanent neurological sequelae.7 However, performing MVD presents numerous challenges, including the technical intricacy of the procedure, the steep learning curve associated with mastering the required microsurgical techniques, and the need for precise intraoperative neuromonitoring to minimize risks. Complications such as cerebrospinal fluid leakage, cranial nerve deficits, and hearing loss remain concerns, despite improvements in surgical methods.8,9 Nevertheless, a proper understanding of the pros and cons of MVD is necessary for the surgeons to be able to have an informed discussion with the patients and help them to make the best decision for themselves. Identifying the gaps, misconceptions, and misunderstandings is necessary before designing targeted educational activities.
The knowledge, attitude, and practice (KAP) model is a systematic framework widely utilized in healthcare research to assess the cognitive, affective, and behavioral dimensions related to a specific health issue or intervention.10,11 The primary purpose of the KAP model is to identify gaps in knowledge, clarify prevailing attitudes, and understand actual practices among target populations-often healthcare professionals or patients. By elucidating these dimensions, researchers can design more effective interventions and educational strategies tailored to the identified needs, ultimately aiming to promote positive behavior change and improve health outcomes.10,12 The KAP model asserts that individual behaviors are influenced by one’s knowledge and attitudes.10 In public health, the examination of behavioral practices often involves assessing knowledge and risk perception through KAP surveys, underscoring the model’s critical role in understanding health-related behaviors.13–15 However, there remains a lack of comprehensive studies specifically examining neurosurgeons’ knowledge, attitudes, and practices (KAP) regarding microvascular decompression (MVD) and how these factors might influence surgical outcomes. Existing literature is extensive on MVD techniques, long-term patient outcomes, and prognostic variables such as neurovascular conflict severity, radiological assessment, and the use of neuronavigation; however, few, if any, studies have systematically explored the impact of neurosurgeons’ KAP on procedural quality or patient results.16–19
Therefore, this study aims to explore these relationships to identify potential areas for improvement in surgical training and practice.
Materials and Methods
Study Design and Participants
This cross-sectional study was conducted between May and June 2024, involving multiple institutions across Eastern China. The hospitals involved in this study are listed in the Supplementary Materials. The participants were neurosurgeons from the region who met the following inclusion criteria: 1) currently practicing neurosurgery within Eastern China, including lead surgeons and surgical assistants; 2) having expressed willingness to participate in the study. The exclusion criteria included: 1) survey completion time under 90 seconds via WeChat, suggesting inadequate consideration of responses; and 2) incorrect answers to control questions aimed at confirming engagement. This study was approved by the Ethics Committee of the Second People’s Hospital of Liaocheng (2024–29), and all participants provided informed consent. This study was reported following the STROBE checklist.20
Questionnaire introduction
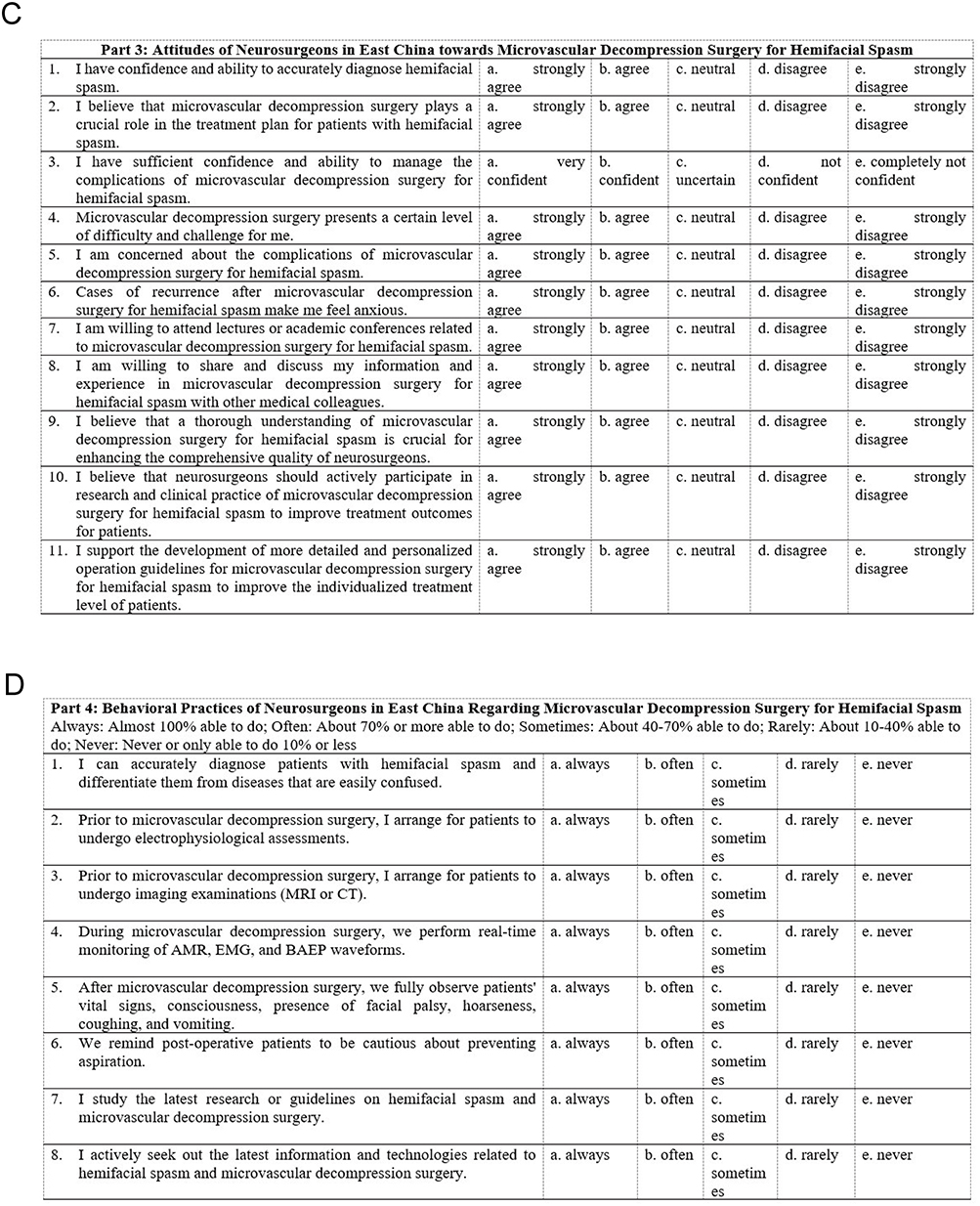
The questionnaire was initially pilot tested with a small cohort of 45 participants, achieving a reliability coefficient of 0.892. It underwent a thorough review by two statistics experts and three medical professionals. The final version of the questionnaire, administered in Chinese, included four sections (Figure 1A–D): demographic data and dimensions assessing HFS. The knowledge dimension comprised nine questions, scored as follows: “very familiar” (2 points), “heard of” (1 point), and “not familiar” (0 points), with a potential total ranging from 0 to 18 points. The attitude dimension consisted of 11 questions, evaluated using a five-point Likert scale from “strongly disagree” (1 point) to “strongly agree” (5 points), resulting in a score range of 11 to 55 points. The practice dimension included eight questions, assessed on a five-point Likert scale from “always” (5 points) to “never” (1 point), with total scores varying from 8 to 40 points. Adequate knowledge, positive attitudes, and proactive practices were defined as scores exceeding 80% of the maximum possible score in each respective dimension.21 Specifically, the cutoff values were 14.4 points for knowledge (80% of 18), 44 points for attitude (80% of 55), and 32 points for practice (80% of 40).10,22,23 Figure 1 Continued. Figure 1 Questionnaire. (A) Demographics. (B) Knowledge. (C) Attitude. (D) Practice.
The questionnaires were distributed via the neurosurgeon WeChat groups of the participating hospitals. The overall Cronbach’s α coefficient for the questionnaire was 0.879, indicating good internal consistency. The distribution strategy utilized direct messaging and QR code scanning to facilitate widespread participation among the target audience. The control question was item K4 (“The capital of China is Shanghai.”), which was used only to determine whether the participants were actually reading the questions before answering. Failing item K4 automatically led to participant exclusion.
Sample Size
The sample size was determined according to Kendall’s criterion,24 which recommends a sample size of 5–10 times the number of variables. Considering that there were 28 KAP questions, the minimum sample size was determined as 140.
Statistical Analysis
Data analysis was performed using SPSS 27.0 and Amos 26.0 (IBM, Armonk, New York, USA). Descriptive statistics were used to analyze the demographic data and KAP scores of participants. Continuous variables were presented as means ± standard deviations (SD), while categorical variables and individual question responses were expressed as frequencies (percentages). The Mann–Whitney U-test was applied to compare KAP scores between two groups, and the Kruskal–Wallis H-test was used for three or more groups, both for non-normally distributed data. Spearman correlation analysis was utilized to evaluate the relationships between the scores of HFS. The cutoff value for positive practice was set at 32 points (80% of the maximum possible score of 40), following standard methodology for KAP studies. Univariate logistic regression was performed to identify factors associated with positive practice. Variables with P < 0.05 in univariate analysis were included in multivariable logistic regression to determine independent predictors of positive practice. Structural equation model (SEM) and path analysis were employed to explore the interrelationships among the KAP dimensions. Model fit was assessed using the following indices: Chi-square/degree of freedom ratio (CMIN/DF < 3 indicating good fit), root mean square error of approximation (RMSEA < 0.08 indicating acceptable fit), incremental fit index (IFI > 0.8 indicating good fit), Tucker-Lewis index (TLI > 0.8 indicating good fit), and comparative fit index (CFI > 0.8 indicating good fit).25 A two-sided P-value of less than 0.05 was considered statistically significant.
Results
Demographic Characteristics
Initially, a total of 235 questionnaires were distributed, with exclusions as follows: 1) 8 participants completed the questionnaire in less than 90 seconds, 2) 2 participants failed the trap questions, and 3) 2 individuals refused to participate. After exclusions, data from 223 participants remained valid for analysis. Among them, 218 (97.76%) were males, 122 (54.71%) were not more than 40 years of age, 120 (53.81%) had master’s degree, 128 (57.40%) had the title of associate senior or senior, 137 (61.43%) had more than 11 years of experience in neurosurgery, 198 (88.79%) had experience in the diagnosis and treatment of HFS, and 168 (75.34%) had experience in MVD surgery for HFS. The mean knowledge, attitude, and practice scores were 15.69±3.05 (possible range: 0–18), 42.57±4.03 (possible range: 11–55), and 34.58±4.71 (possible range: 8–40), respectively. By analyzing demographic characteristics, participants’ HFS scores varied across experience in diagnosis and treatment of HFS (P < 0.001, P < 0.001, P = 0.044) and experience in MVD surgery for HFS (P < 0.001, P < 0.001, P = 0.006). Differences in knowledge scores were more likely to be found among participants with different levels of education (P = 0.001), title (P < 0.001), type of hospital (P = 0.019), and presence of neurosurgical microsurgery equipment and instruments (P = 0.019). Those with a different type of hospital were more likely to have different practice scores (P = 0.037) (Table 1).
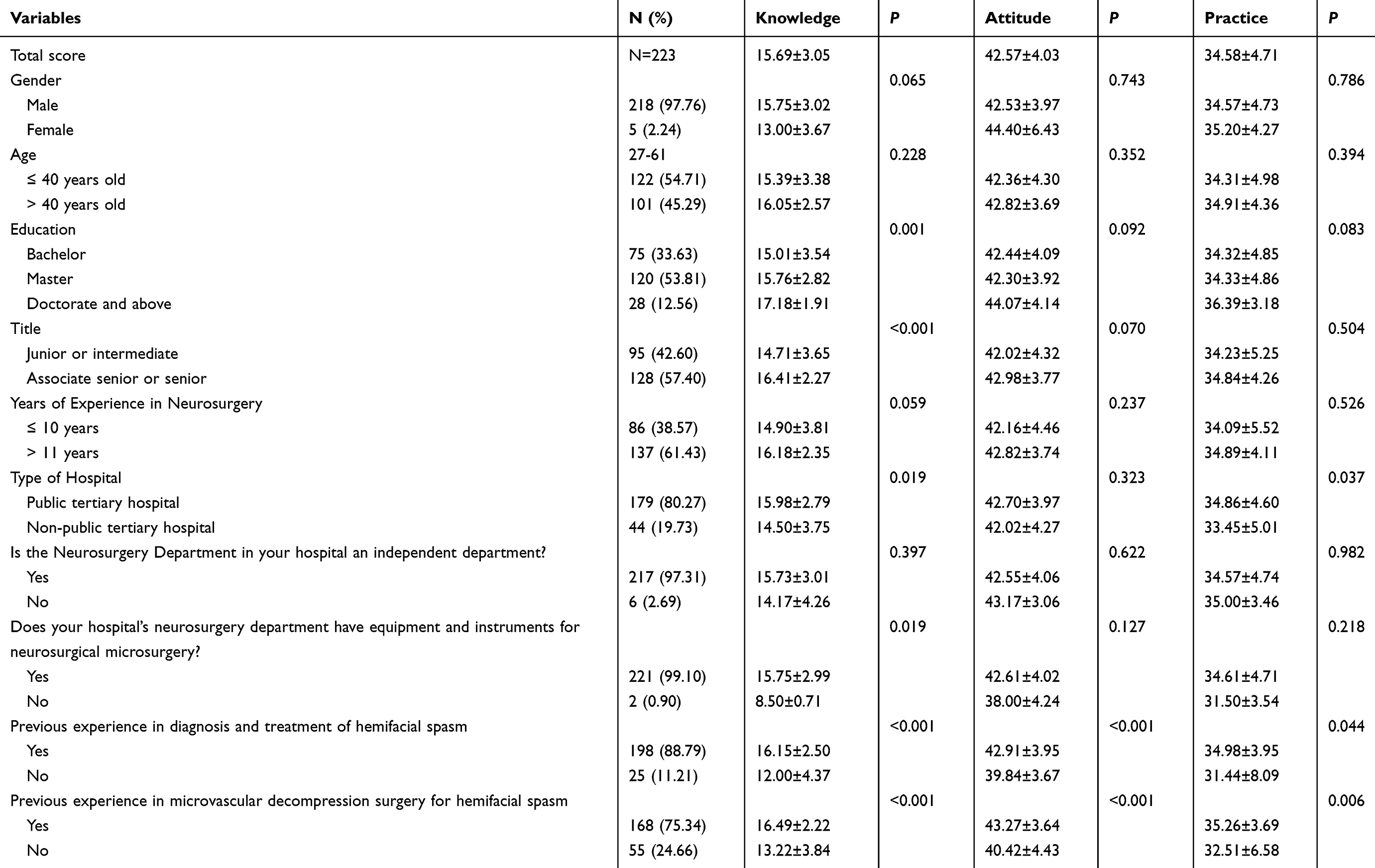 |
Table 1 Demographic Characteristics |
Knowledge, Attitude, and Practice Dimensions
The distribution of knowledge dimensions shown that the three questions with the highest number of participants choosing the “Not familiar” option were “Preoperative electrophysiological assessment aids in distinguishing HFS and objectively understanding the functional levels of the facial and vestibular nerves”. (K4) with 8.07%, “The main criteria for concluding MVD surgery are twofold” (K8) with 6.73%, and “Severe hematologic disorders or significant organ dysfunctions (heart, lungs, kidneys, or liver) are contraindications for MVD surgery.” (K7) with 3.14%. The responses for attitude showed that 30.04% strongly agreed and 47.98% agreed that the operation of MVD surgery presents some difficulty and challenges for them (A4). Meanwhile, 17.49% strongly agreed and 44.84% agreed that they were concerned about the complications of MVD surgery for HFS (A5). In addition, 19.73% strongly agreed and 50.22% agreed that cases of recurrence after MVD surgery for HFS make them feel anxious and nervous (A6). When it comes to relevant practice, a significant proportion of participants had an active practice. Notably, 14.8% rarely and 4.93% never arranged electrophysiologic assessment of patients prior to MVD (P2), and 13% rarely and 11.66% never performed real-time AMR, ZLR, and BAEP monitoring during MVD surgery (P4) (Supplementary Table 1).
Spearman Correlation Analysis
Spearman correlation analysis indicated significant positive correlations between knowledge and attitude (r = 0.517, P < 0.001), as well as practice (r = 0.478, P < 0.001). Meanwhile, there was also a correlation between attitude and practice (r = 0.448, P < 0.001) (Table 2).
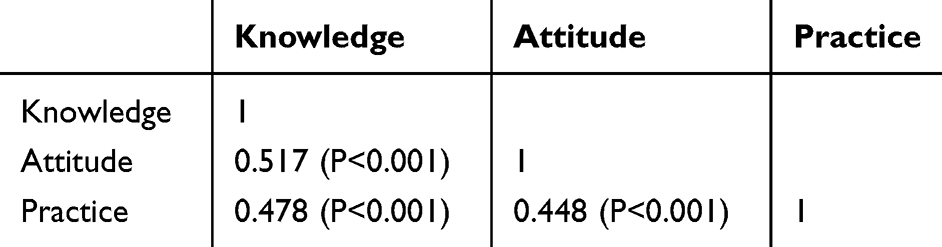 |
Table 2 Spearman Correlation Analysis |
Univariate and Multivariable Logistic Regression Analysis
Based on the established cutoff value of 32 points (80% of total practice score), 145 participants were classified as having positive practice, while 78 demonstrated negative practice. Based on the 80% cutoff value, only 35.4% of participants demonstrated adequate attitudes toward MVD surgery, indicating an insufficient overall attitude level among neurosurgeons. Univariate logistic regression identified knowledge scores (OR=1.284, 95% CI: 1.160–1.421, P<0.001), attitude scores (OR=1.273, 95% CI: 1.157–1.401, P<0.001), and prior experience in diagnosis and treatment of HFS (OR=2.671, 95% CI: 1.134–6.293, P=0.025) as factors significantly associated with positive practice. In multivariable analysis, only knowledge scores (OR=1.169, 95% CI: 1.033–1.322, P=0.013) and attitude scores (OR=1.194, 95% CI: 1.073–1.328, P=0.001) remained independently associated with positive practice after adjusting for other factors (Table 3).
 |
Table 3 Univariate and Multivariable Logistic Regression Analysis of Practice |
Structural Equation Model
The fitting index of the SEM outperformed the respective threshold value (CMIN/DF = 2.101, RMSEA = 0.070; IFI = 0.944; TLI = 0.895; CFI = 0.942), signifying that the data satisfactorily fit the structural model (Supplementary Table 2), the path analysis showed that presence of neurosurgical microsurgery equipment and instruments (β = −3.980, P = 0.025), title (β = 1.189, P < 0.001), past experience in diagnosis and treatment of HFS (β = −2.200, P < 0.001), and past experience in MVD surgery for HFS (β = −1.794, P < 0.001) had direct effects on knowledge. At the same time, knowledge (β = 0.629, P < 0.001) had a direct effect on attitude. Further, knowledge (β = 0.547, P < 0.001) and attitude (β = 0.322, P < 0.001) had direct effects on practice (Table 4 and Figure 2).
 |
Table 4 Path Analysis |
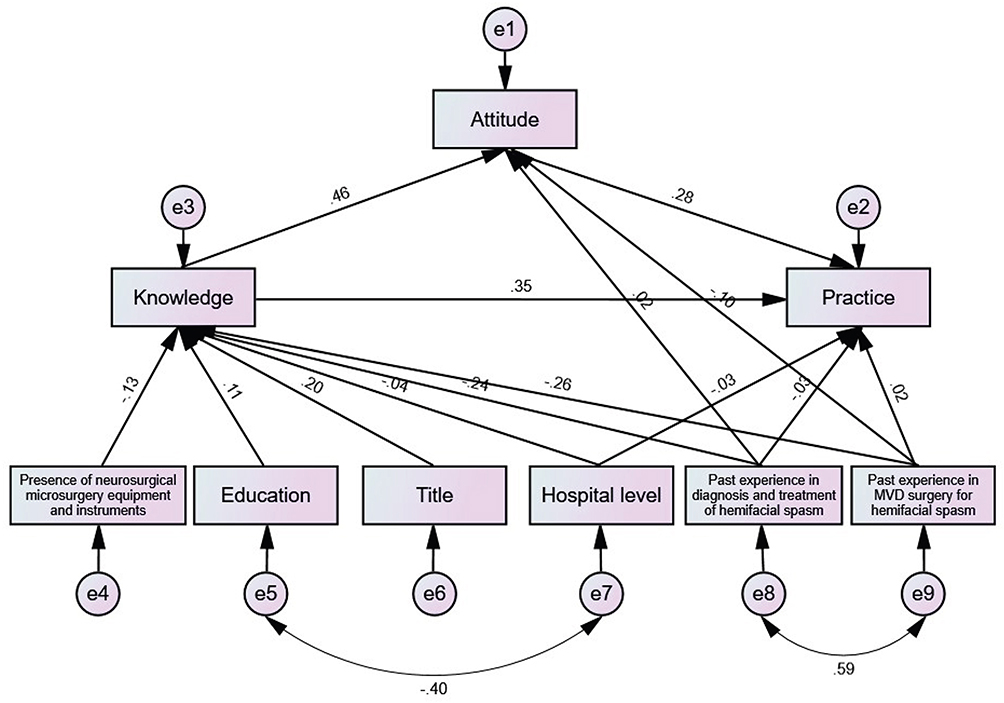 |
Figure 2 Path analysis. 1) Graphic shape: The latent variables are represented by ellipses or circles, observed variables are depicted as rectangles or squares, and error terms are illustrated by small circles connected to the corresponding observed variables. 2) Arrows: The arrows and coefficients among the three KAP constructs indicate both the direction and strength of the relationships between the latent variables. The small circles associated with A and P represent the residual terms. A unidirectional arrow signifies the direction of causation, specifically from cause to effect. When an arrow points from one latent variable to another, it indicates that the former exerts a direct effect on the latter. Conversely, if the latent variable is directed from the observed variable, it signifies that the latent variable is represented by that observed variable. 3) Number: The numerical value on the arrow connecting the latent variable to the observed variable signifies the factor loading, which reflects the strength of the association between the observed variable and the latent variable, specifically the regression coefficient of the observed variable with respect to the latent variable. A positive value indicates a positive correlation, suggesting that as the latent variable increases, the observed variable also tends to increase; conversely, a negative value indicates a negative correlation, implying that as the latent variable increases, the observed variable tends to decrease. |
Discussion
Our findings demonstrate that neurosurgeons’ knowledge, attitudes, and practices regarding MVD are significantly interrelated, with knowledge serving as a fundamental driver of both attitudes and practices. Specifically, the multivariable analysis revealed that higher knowledge scores and attitude scores independently predicted positive surgical practices, highlighting the crucial role of comprehensive education and training.
Most research focuses on clinical results (eg, success rates, complication profiles, and technical innovations), consistently demonstrating that MVD is effective and generally safe for conditions like trigeminal neuralgia. Technical factors such as surgeon experience, meticulous preoperative imaging, and advanced intraoperative techniques, like endoscope or neuronavigation assistance, are associated with improved outcomes. However, underlying KAP variables (such as individual surgeon beliefs about optimal techniques, attitudes toward technology adoption, or patterns in intraoperative decision-making) are not directly measured or connected to surgical success in published series.18,26–28 Bibliometric analyses and systematic reviews show that highly cited studies in MVD focus on technical innovation and long-term efficacy, with almost no direct assessment of clinical decision-making frameworks, learning curves, or educational backgrounds as they relate to patient outcomes. This represents a critical knowledge gap that could be addressed by future KAP-based research within neurosurgical cohorts.19,29 Hence, despite robust literature on MVD outcomes and technical variation, there are currently no comprehensive studies directly linking neurosurgeons’ knowledge, attitudes, and practices to observed surgical results in this domain. Future research explicitly designed to capture KAP data is warranted to inform best practices and optimize MVD outcomes.18,19 The findings of this study indicate that neurosurgeons in Eastern China possess strong knowledge but insufficient attitudes towards MVD for HFS, which may impact their clinical practices. These results are consistent with similar studies that have emphasized the significance of high knowledge levels and positive attitudes in fostering effective clinical practices.30,31
Barriers to the application of MVD in developing countries such as China include multiple systemic, technical, and economic factors.32–34 Resource constraints limit the availability of advanced surgical equipment, intraoperative monitoring, and high-resolution imaging necessary for safe and effective MVD procedures. Cost barriers also impact access to quality operating room environments and postoperative care.34 There is a scarcity of neurosurgeons highly trained in MVD, particularly in rural and less developed regions. The complexity of the procedure demands extensive experience, which is often concentrated in urban tertiary centers.34 Access to high-quality MRI and angiography is sometimes limited, leading to suboptimal preoperative planning and less accurate identification of neurovascular conflicts, thereby affecting patient outcomes.34 The absence of standardized academic and practical training programs for MVD, allied with insufficient surgeon training opportunities, reduces procedural uptake and success rates in lower-resource settings.32,34 High costs and limited availability of standard synthetic materials (such as Teflon) sometimes necessitate using alternative materials like autologous muscle grafts, the long-term outcomes of which are less well-established in these settings.32 Disparities in access to neurosurgical services, especially pronounced in vast countries like China, mean that many patients in rural areas cannot benefit from specialized treatments like MVD.34 Constraints on intensive care capabilities and rehabilitation services can lead to increased complication rates and difficulties in managing adverse events after surgery, further limiting MVD’s widespread adoption.34 Both patients and primary healthcare providers may have limited awareness of MVD as a treatment option, leading to delayed referrals and more advanced disease at presentation.32 Technological complexity and rising costs can act as barriers, particularly in terms of acquiring and maintaining surgical instruments or employing newer techniques such as full endoscopy or neuronavigation.35 These challenges highlight the need for global health initiatives, increased training, innovation in cost-effective surgical materials, and better healthcare infrastructure to improve MVD accessibility and outcomes in developing regions like China.
Significant variables such as education, title, and previous experience show varying influences on knowledge, attitudes, and practices. For instance, higher education levels, specifically doctorates, are associated with better knowledge and practice scores, which might be attributed to the more rigorous training and exposure received during advanced studies.36 Similarly, those with higher professional titles exhibit more substantial knowledge and slightly better practices, possibly due to the cumulative experience and responsibilities that come with seniority.37 This underscores the importance of tailored training programs that build on existing educational foundations while addressing gaps in specific skill sets, particularly for early-career neurosurgeons. However, despite differences in education and title, the variations in attitudes were not as pronounced, suggesting that while knowledge and experience enrich technical competence, attitudes might be influenced more by personal or systemic factors rather than educational attainment alone.
The type of hospital also presented differences in practice scores, with public tertiary hospitals showing significantly better practices than non-public ones. This could be attributed to the better resources and more frequent exposure to complex cases in public tertiary settings.38,39 Surprisingly, no significant differences were observed in attitude based on hospital type, suggesting that individual attitudes towards procedures may be less influenced by the working environment and more by personal or professional factors.
The logistic regression results showed that knowledge and attitude scores remained the strongest predictors of positive surgical practices even after adjusting for demographic and institutional factors. This suggests that while experience and resources are important, fundamental understanding of MVD procedures and positive attitudes toward continuous learning are crucial for maintaining high practice standards. The pathway analysis revealed several key determinants of surgical competence. Professional title and specialized equipment availability significantly influenced knowledge levels, while knowledge had direct effects on both attitudes and practices. These findings suggest that institutional support and career development play crucial roles in building surgical expertise. Correlation and SEM analyses consistently demonstrated strong links between knowledge, attitude, and practice dimensions. Knowledge was a critical predictor of both attitude and practice, confirming the integral role of education and continuous professional development in fostering proactive clinical behaviors.40 The presence of equipment and prior experience, particularly in the diagnosis and treatment of HFS, was also crucial, significantly impacting knowledge levels. Neurosurgeons with greater surgical experience were more likely to report higher confidence and proficiency, highlighting the need for training programs that integrate hands-on workshops, mentorship, and simulation-based learning to bridge the gap for less experienced surgeons. This also emphasizes the importance of incorporating real-world clinical scenarios in training to ensure the practical applicability of knowledge.
While the majority of neurosurgeons demonstrated familiarity with HFS and its treatment via MVD, areas of concern emerged regarding the specifics of preoperative assessments and the distinctions between typical and atypical HFS. Notably, a significant number lacked full familiarity with the preoperative electrophysiological assessments necessary for distinguishing between HFS and other conditions, with around 8% unfamiliar with these techniques. To address these deficits, targeted educational interventions could be beneficial. Workshops and continuing education programs that focus on the latest diagnostic technologies, like electrophysiology, could enhance the surgeons’ diagnostic accuracy. Additionally, incorporating case-based discussions and interactive sessions during professional conferences could provide practical exposure to complex diagnostic challenges, fostering a deeper understanding of these nuances. Further, incorporating these assessments into standard preoperative protocols and ensuring they are discussed at professional conferences could standardize care and improve outcomes.41,42
While the majority of neurosurgeons demonstrated familiarity with HFS and its treatment via MVD, their attitudes were found to be insufficient based on the 80% criterion. This insufficiency was particularly evident in areas such as confidence in managing complications and concerns about surgical challenges. Approximately 17% are concerned about the complications, reflecting a potential lack of confidence in managing adverse outcomes, a critical aspect of surgical competence. This suggests that training programs should prioritize simulation-based training and complication management to build surgeons’ confidence and preparedness. Moreover, establishing a mentorship program where less experienced surgeons can learn directly from seasoned experts in MVD could enhance confidence levels. Regular case review sessions where surgical complications are discussed openly could also help in demystifying the complexities and variabilities of these surgical procedures.43,44
While a high percentage of surgeons regularly conduct necessary imaging and assessments before MVD, there is variability in the adoption of real-time monitoring during surgery. The practice of conducting intraoperative monitoring, such as auditory brainstem response (ABR), brainstem auditory evoked potential (BAEP), and electromyography (EMG), was less consistently performed, with about 24% not regularly incorporating these practices. Given the critical role that intraoperative monitoring plays in the success of MVD and the minimization of surgical risks, enhancing the use of these technologies is essential. One approach could be the integration of standardized operating procedures that include mandatory intraoperative monitoring for all MVD surgeries. Further, hospital-based workshops that teach the technical aspects and interpretation of intraoperative monitoring data could address gaps in its implementation. Additionally, providing access to the latest monitoring technologies through hospital investments and training on how to effectively use these tools could ensure more consistent implementation across all surgical cases.45,46
Based on our findings, we propose several key clinical recommendations: (1) Healthcare institutions should prioritize establishing comprehensive neuromonitoring facilities, as the regular use of intraoperative monitoring showed significant variability among respondents; (2) A structured mentorship program should be implemented, pairing less experienced surgeons with seasoned experts in MVD procedures; (3) Regular case review sessions focusing on complication management should be conducted, particularly addressing concerns about postoperative complications that were expressed by 17.49% of respondents; and (4) Standardized preoperative assessment protocols, including mandatory electrophysiological testing and imaging evaluations, should be established across institutions. Additionally, we recommend developing regional training networks to ensure equitable access to high-quality training opportunities, particularly for neurosurgeons in lower-tier hospitals where resources and exposure to complex cases may be limited.
Several practical strategies should be adopted to ensure methodological rigor and clinical relevance to enhance research on the KAP relating to facial decompression in future studies. KAP questionnaires that are validated for surgical or neurological contexts should be used. Quantitative questionnaires with qualitative methods, such as in-depth interviews or focus groups, should be used. It would allow more nuanced insights into the barriers and facilitators affecting neurosurgeons’ practice and belief systems around facial decompression. KAP findings should be paired with objective measures of clinical practice, such as adherence to surgical protocols, rehabilitation engagement, and patient outcomes. It may reveal practical links between KAP domains and real-world practice. Future studies should not only involve neurosurgeons, but also anesthesiologists, nurses, rehabilitation specialists, and patients to map out comprehensive practice patterns and identify points of educational need. Online survey tools and digital platforms should be employed to facilitate broad, efficient participation, especially in large or geographically diverse populations. Future research should be designed with sensitivity to known obstacles, such as time constraints, low response rates, and possible social desirability bias. By adopting these strategies, researchers should be able to generate high-quality evidence to inform future educational interventions, training programs, and clinical guidelines for facial decompression surgery.
However, this study had several limitations. First, its cross-sectional design limits the ability to establish causality between the observed factors and the KAP scores among neurosurgeons. Second, the sample is confined to neurosurgeons in Eastern China, which may not be representative of neurosurgeons in other regions or countries, potentially affecting the generalizability of the findings. Third, the participant exposure or training with MVD was not assessed. Lastly, the reliance on self-reported data may introduce response bias, as participants might have overestimated their knowledge or practices due to social desirability or other factors.
Conclusion
This study demonstrates that both knowledge and attitude independently predict neurosurgeons’ practice quality in MVD procedures. These findings emphasize the importance of targeting areas for improvement in surgical training and practice standards. To address identified gaps, it is recommended that structured, competency-based training programs be established (particularly for junior doctors and neurosurgeons working in lower-tier hospitals) to systematically enhance KAP levels. Healthcare institutions should implement and sustain comprehensive professional development initiatives, with a dual emphasis on advanced technical skills and updated theoretical knowledge specific to MVD. Such efforts are essential for optimizing surgical performance and patient outcomes, thereby ensuring continual improvement in neurosurgical care.
Data Sharing Statement
All data generated or analyzed during this study are included in this article and supplementary information files.
Ethics Approval and Consent to Participate
The authors confirm that all methods were performed in accordance with the relevant guidelines. This work has been carried out in accordance with the Declaration of Helsinki (2000) of the World Medical Association. This study was approved by the Ethics Committee of the Second People’s Hospital of Liaocheng (2024-29), and all participants provided written informed consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the Journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (No. 82271394 and No. 82311530117).
Disclosure
The authors declare that they have no competing interests.
References
1. Kim YG, Kim MH, Kim GE, Cho D. Early-Onset insomnia among patients with hemifacial spasm in South Korea: a nationwide cohort study. J Pers Med. 2023;13(2):197. doi:10.3390/jpm13020197
2. Kim YG, Chang WS, Jung HH, Chang JW. The long-term effects of microvascular decompression on social phobia and health-related quality of life in patients with hemifacial spasm: a 3-year prospective study. Acta Neurochir. 2019;161(10):2035–2042. doi:10.1007/s00701-019-04023-y
3. Kim YG, Jung NY, Kim M, Chang WS, Jung HH, Chang JW. Benefits of microvascular decompression on social anxiety disorder and health-related quality of life in patients with hemifacial spasm. Acta Neurochir. 2016;158(7):1397–1404. doi:10.1007/s00701-016-2822-4
4. Tambasco N, Filidei M, Nigro P, Parnetti L, Simoni S. Botulinum toxin for the treatment of hemifacial spasm: an update on clinical studies. Toxins. 2021;13(12):881. doi:10.3390/toxins13120881
5. Terasaka S, Asaoka K, Yamaguchi S, Kobayashi H, Motegi H, Houkin K. A significant correlation between delayed cure after microvascular decompression and positive response to preoperative anticonvulsant therapy in patients with hemifacial spasm. Neurosurg Rev. 2016;39(4):607–613. doi:10.1007/s10143-016-0729-4
6. Sindou M, Mercier P. Microvascular decompression for hemifacial spasm: outcome on spasm and complications. A review. Neurochirurgie. 2018;64(2):106–116. doi:10.1016/j.neuchi.2018.01.001
7. Lee S, Han J, Park SK, Lee JA, Joo BE, Park K. Involvement of the vertebral artery in hemifacial spasm: clinical features and surgical strategy. Sci Rep. 2021;11(1):4915. doi:10.1038/s41598-021-84347-x
8. Baldauf J, Rosenstengel C, Schroeder HWS. Nerve compression syndromes in the posterior cranial fossa. Dtsch Arztebl Int. 2019;116(4):54–60. doi:10.3238/arztebl.2019.0054
9. Lee S, Park SK, Lee JA, Joo BE, Park K. Missed culprits in failed microvascular decompression surgery for hemifacial spasm and clinical outcomes of redo surgery. World Neurosurg. 2019;129:e627–e633. doi:10.1016/j.wneu.2019.05.231
10. Andrade C, Menon V, Ameen S, Kumar Praharaj S. Designing and conducting knowledge, attitude, and practice surveys in psychiatry: practical guidance. Indian J Psychol Med. 2020;42(5):478–481. doi:10.1177/0253717620946111
11. World Health Organization. Advocacy, communication and social mobilization for TB control: a guide to developing knowledge, attitude and practice surveys. Available from: http://whqlibdoc.who.int/publications/2008/9789241596176_eng.pdf.
12. Zarei F, Dehghani A, Ratansiri A, et al. ChecKAP: a checklist for reporting a knowledge, attitude, and practice (KAP) study. Asian Pac J Cancer Prev. 2024;25(7):2573–2577. doi:10.31557/APJCP.2024.25.7.2573
13. Aerts C, Revilla M, Duval L, et al. Understanding the role of disease knowledge and risk perception in shaping preventive behavior for selected vector-borne diseases in Guyana. PLoS Negl Trop Dis. 2020;14(4):e0008149. doi:10.1371/journal.pntd.0008149
14. Liao L, Feng H, Jiao J, Zhao Y, Ning H. Nursing assistants’ knowledge, attitudes and training needs regarding urinary incontinence in nursing homes: a mixed-methods study. BMC Geriatr. 2023;23(1):39. doi:10.1186/s12877-023-03762-z
15. Mumena WA. Maternal knowledge, attitude and practices toward free sugar and the associations with free sugar intake in children. Nutrients. 2021;13(12):4403. doi:10.3390/nu13124403
16. Zhong J. The simpler the better: a personal philosophy of microvascular decompression surgery. Chin Med J. 2021;134(4):410–412. doi:10.1097/CM9.0000000000001233
17. Legninda Sop FY, D’Ercole M, Izzo A, et al. The impact of neuronavigation on the surgical outcome of microvascular decompression for trigeminal neuralgia. World Neurosurg. 2021;149:80–85. doi:10.1016/j.wneu.2021.02.063
18. Fareed A, Iftikhar Z, Haider R, et al. Awake neurosurgery: advancements in microvascular decompression for trigeminal neuralgia. Surg Neurol Int. 2024;15:215. doi:10.25259/SNI_286_2024
19. Wolff Fernandes F, Krauss JK. Microvascular decompression: a bibliometric analysis of the 100 most cited articles. World Neurosurg. 2022;164:e67–e81. doi:10.1016/j.wneu.2022.03.128
20. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. 2007;335(7624):806–808. doi:10.1136/bmj.39335.541782.AD
21. Hebo HJ, Gemeda DH, Abdusemed KA. Hepatitis B and C viral infection: prevalence, knowledge, attitude, practice, and occupational exposure among healthcare workers of jimma university medical center, Southwest Ethiopia. Scientific World J. 2019;2019:9482607. doi:10.1155/2019/9482607
22. Bloom BS. Learning for mastery. instruction and curriculum. regional education laboratory for the carolinas and virginia, topical papers and reprints, number 1. Evaluation Comment. 1968;1(2):n2.
23. Kaliyaperumal K. Guideline for conducting a knowledge, attitude and practice AECS Illumination. 2004;4:7–9.
24. Kendall MG. A new measure of rank correlation. Biometrika. 1938;30(1/2):81–93. doi:10.1093/biomet/30.1-2.81
25. Bachelet VC, Osorio R, Silva-Villalobos D, Urzúa-álvarez C, Navarrete MS. Exploring physicians’ perception of diagnostic information in clinical practice. Medwave. 2023;23(1):e2665. doi:10.5867/medwave.2023.01.2665
26. Loayza R, Wikström J, Grabowska A, Semnic R, Ericson H, Abu Hamdeh S. Outcome after microvascular decompression for trigeminal neuralgia in a single center-relation to sex and severity of neurovascular conflict. Acta Neurochir. 2023;165(7):1955–1962. doi:10.1007/s00701-023-05642-2
27. Nurimanov C, Mammadinova I, Menlibayeva K, Kaliyev A, Makhambetov Y, Akshulakov S. The outcomes of microvascular decompression for primary trigeminal neuralgia: insights from a single-center experience and technical advancements. Front Surg. 2024;11. doi:10.3389/fsurg.2024.1378717
28. Liu J, Wu G, Xiang H, et al. Long-Term retrospective analysis of microvascular decompression in patients with recurrent trigeminal neuralgia. Front Neurol. 2020;11:11–2020. doi:10.3389/fneur.2020.00011
29. Nova CV, Zakrzewska JM, Baker SR, Riordain RN. Treatment outcomes in trigeminal neuralgia–A systematic review of domains, dimensions and measures. World Neurosurg. 2020;6:100070.
30. Park H, Cho H. Effects of a self-directed clinical practicum on self-confidence and satisfaction with clinical practicum among South Korean nursing students: a mixed-methods study. Int J Environ Res Public Health. 2022;19(9).
31. Xing H, Zhu S, Liu S, et al. Knowledge, attitudes and practices of ICU nurses regarding subsyndromal delirium among 20 hospitals in China: a descriptive cross-sectional survey. BMJ Open. 2022;12(9):e063821. doi:10.1136/bmjopen-2022-063821
32. Alasta A, Al Naggar AM, Al-Saidy A, Al Wesabi F. Microvascular decompression for trigeminal neuralgia using autologous muscle grafting: a retrospective analysis in a resource-limited setting. Cureus. 2025;17(3):e81362. doi:10.7759/cureus.81362
33. Adidharma P, Prasetya M, Sulistyanto A, et al. Single-surgeon approach in microvascular decompression for trigeminal neuralgia: lessons from an Indonesian tertiary-level neurological center. J Clin Neurosci. 2023;115:53–59. doi:10.1016/j.jocn.2023.07.017
34. Okon II, Menon SS, Osama M, et al. Microvascular decompression: a contemporary update. BMC Surg. 2025;25(1):20. doi:10.1186/s12893-025-02762-7
35. Liu J, Zhang Y, Tao X, Wang B. Application of multimodal reconstruction technology and 3D printing technology in MVD surgery. J Craniofac Surg. 2024;35(8):2360–2363. doi:10.1097/SCS.0000000000010612
36. Agbeno EK, Osarfo J, Owusu GB, et al. Knowledge of hypertensive disorders of pregnancy among pregnant women attending antenatal clinic at a tertiary hospital in Ghana. SAGE Open Med. 2022;10:20503121221088432. doi:10.1177/20503121221088432
37. Ju C, Zhang S. Influencing factors of continuous use of web-based diagnosis and treatment by patients with diabetes: model development and data analysis. J Med Internet Res. 2020;22(9):e18737. doi:10.2196/18737
38. Harrison-Bernard LM, Augustus-Wallace AC, Souza-Smith FM, Tsien F, Casey GP, Gunaldo TP. Knowledge gains in a professional development workshop on diversity, equity, inclusion, and implicit bias in academia. Adv Physiol Educ. 2020;44(3):286–294. doi:10.1152/advan.00164.2019
39. Mncube LS, Mthethwa LC. Potential ethical problems in the creation of open educational resources through virtual spaces in academia. Heliyon. 2022;8(6):e09623. doi:10.1016/j.heliyon.2022.e09623
40. Glover K, Bodzin A. Learner analysis to inform the design and development of a serious game for nongaming female emerging health care preprofessionals: qualitative sample study. JMIR Serious Games. 2020;8(1):e16003. doi:10.2196/16003
41. Lee S, Joo KM, Park K. Challenging microvascular decompression surgery for hemifacial spasm. World Neurosurg. 2021;151:e94–e99. doi:10.1016/j.wneu.2021.03.133
42. Zheng X, Zhang B, Shao D, et al. Fully endoscopic microvascular decompression for hemifacial spasm: a clinical study and analysis. Neurosurg Rev. 2024;47(1):83. doi:10.1007/s10143-024-02311-5
43. Lee HY, Park I, Luu MP, et al. Interrater reliability of motor severity scales for hemifacial spasm. J Neural Transm. 2023;130(10):1269–1279. doi:10.1007/s00702-023-02667-w
44. Rangwala HS, Fatima H, Rangwala BS. Letter to the editor: fully endoscopic microvascular decompression for hemifacial spasm: a clinical study and analysis. Neurosurg Rev. 2024;47(1):97. doi:10.1007/s10143-024-02332-0
45. Matmusaev M, Kumar RS, Yamada Y, et al. Endoscopic microvascular decompression for hemifacial spasm. Asian J Neurosurg. 2020;15(4):833–838. doi:10.4103/ajns.AJNS_152_20
46. Zhao Z, Chai S, Xiao D, et al. Microscopic versus endoscopic microvascular decompression for the treatment of hemifacial spasm in China: a meta-analysis and systematic review. J Clin Neurosci. 2021;91:23–31. doi:10.1016/j.jocn.2021.06.034
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge, Attitudes, and Practices Among Patients with Systemic Lupus Erythematosus Toward Disease Management and Biologic Therapy
Liu X, Song Y, Wan L, Du R
Journal of Multidisciplinary Healthcare 2024, 17:937-947
Published Date: 2 March 2024
Knowledge, Attitudes, and Practices Among Community Populations Toward Long COVID in China
He N, Tunala S, Wu R, Zhao C, Wuren T, Hushuud C
International Journal of General Medicine 2024, 17:4455-4463
Published Date: 1 October 2024
Knowledge, Attitudes, and Practices Regarding Swallowing Disorders Among General Practitioners
Zou M, Zhu X, Li J, Yu H, Guo P
International Journal of General Medicine 2025, 18:1555-1567
Published Date: 18 March 2025
Knowledge, Attitudes and Practices Toward Hypotension During Hemodialysis Among Nephrology and Hemodialysis Medical Staff: A Multi-Center Cross-Sectional Study
Cheng D, Xie L, Chu X, Bai Y, He T
Journal of Multidisciplinary Healthcare 2025, 18:5359-5369
Published Date: 28 August 2025
Knowledge, Attitudes, and Practices of Hypertensive Patients with Aortic Dissection and Aortic Aneurysm Towards Aortic Dissection and Its Prevention: A Mediation Analysis
Zhang Y, Zhang B, Wang L, Yuan J
International Journal of General Medicine 2026, 19:609862
Published Date: 22 June 2026