Back to Journals » International Journal of General Medicine » Volume 19
Knowledge, Attitudes, and Practices of Hypertensive Patients with Aortic Dissection and Aortic Aneurysm Towards Aortic Dissection and Its Prevention: A Mediation Analysis
Authors Zhang Y, Zhang B, Wang L, Yuan J
Received 17 March 2026
Accepted for publication 8 June 2026
Published 22 June 2026 Volume 2026:19 609862
DOI https://doi.org/10.2147/IJGM.S609862
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Redoy Ranjan
Yanda Zhang, Bo Zhang, Long Wang, Jing Yuan
Henan Provincial Chest Hospital (Affiliated Chest Hospital of Zhengzhou University), Zhengzhou, Henan, 450001, People’s Republic of China
Correspondence: Long Wang, Henan Provincial Chest Hospital (Affiliated Chest Hospital of Zhengzhou University), No. 1, Weiwu Road, Zhengzhou, Henan, 450001, People’s Republic of China, Tel +86 15639098133, Email [email protected]
Purpose: To investigate the knowledge, attitudes, and practices (KAP) of hypertensive patients with aortic dissection (AD) and aortic aneurysm regarding AD and its prevention.
Patients and Methods: This cross-sectional study was conducted at Henan Chest Hospital between September 15, 2023, and December 15, 2023. Patients with hypertension and either Stanford type A or B AD, ascending aortic aneurysm, or abdominal aortic aneurysm were invited to participate.
Results: A total of 619 participants were included, of whom 521 (84.17%) were male. Their knowledge, attitude, and practice scores were 4.12± 1.25 (range: 0– 22), 35.41± 3.92 (range: 10– 50), and 28.07± 2.96 (range: 8– 40), respectively. Mediation analysis revealed that knowledge directly influenced attitudes (β = 0.338, P = 0.010), and attitudes directly influenced practices (β = 0.458, P = 0.005). Moreover, knowledge had an indirect effect on practices through attitudes (β = 0.155, P = 0.006). In the subgroup of patients with confirmed aortic dissection (n = 605), the mediation pattern was replicated.
Conclusion: Hypertensive patients with AD and aortic aneurysm demonstrated markedly insufficient disease-related knowledge alongside relatively favorable attitudes and moderately engaged self-reported practices toward AD prevention. This imbalance suggests that certain preventive behaviors may occur despite limited disease-specific understanding, indicating a possible separation between knowledge and action. However, given the cross-sectional and self-reported nature of the data, the findings should be interpreted as descriptive patterns rather than evidence of causal relationships or intervention effectiveness.
Keywords: knowledge, attitudes, practices, hypertension, aortic dissection, cross-sectional study
Introduction
The escalating prevalence of hypertension poses a significant global health challenge, particularly due to its association with various cardiovascular diseases (CVDs). Hypertension, which becomes more prevalent with advancing age, affects approximately 70% of individuals aged 70 and above worldwide.1 It stands as the primary contributor to CVDs globally, accounting for at least 22.3% of such conditions.2 Hypertension is a leading modifiable risk factor for cardiovascular morbidity and mortality worldwide. Aortic dissection (AD) is one of the most severe complications of hypertension. AD occurs when there is a tear in the inner layer of the aorta or bleeding within the aortic wall, resulting in the separation of the layers of the aortic wall.3 This condition carries high mortality rates without prompt treatment, particularly Type A AD, which can have a 30-day mortality rate as high as 90% if left untreated.4 The incidence of AD has increased parallel to the rising prevalence of arterial hypertension in the population.5 Hypertension, along with other conditions like connective tissue disorders, cystic medial disease of the aorta, and atherosclerosis, significantly weakens the aortic wall, increasing the risk of AD.6 Notably, nearly 80% of patients who experience AD have a history of hypertension.7
Aortic aneurysm, another severe complication of hypertension, is characterized by a localized dilation of the aorta that exceeds 1.5 times its normal diameter. It is typically classified by location, including thoracic and abdominal aortic aneurysms, with the latter being more prevalent. Aneurysms often progress asymptomatically and may remain undetected until rupture, which is associated with a high fatality rate of up to 90% in cases of abdominal aortic aneurysm rupture.8 Risk factors include hypertension, smoking, male sex, family history, and age over 65 years. Effective prevention involves blood pressure control, smoking cessation, and regular imaging surveillance for early detection. Although less acute than AD, aneurysm carries substantial long-term risks and healthcare burdens, emphasizing the need for increased knowledge and preventive behaviors among at-risk populations.9 Both AD and aortic aneurysm are severe complications of hypertension, sharing overlapping risk factors such as poor blood pressure control, smoking, and genetic predisposition. While AD presents acutely, aneurysms often progress silently and can rupture without warning, carrying high mortality rates. Therefore, it is essential to assess patient understanding and behaviors toward both conditions to inform preventive strategies.
Despite the growing prevalence of hypertension, the rate of adequately controlled hypertension remains disappointingly low, failing to meet expectations.10 This disparity highlights the pressing need for intensified efforts in managing and preventing hypertension, particularly considering its critical role in the development of life-threatening conditions such as AD. However, while there is extensive research on Knowledge-Attitude-Practice (KAP) related to hypertension itself, there is a notable lack of studies exploring the knowledge, attitudes, and practices of hypertensive patients towards AD and its prevention.11,12 The KAP model plays a crucial role in influencing human health behaviors and is essential for understanding and improving health literacy.13 According to this model, knowledge has a positive impact on attitudes, which, in turn, influence behaviors and practices.14 A previous KAP study on cardiovascular diseases also suggested that assessing knowledge, attitudes, and practices is useful for identifying awareness gaps and informing targeted preventive education.15 Implementing the KAP questionnaire in the healthcare field allows for a thorough assessment of the knowledge, attitudes, and practices of the target population, as well as evaluating the demand for and acceptance of relevant information.16 This approach is vital for tailoring health education programs to meet the specific needs of different populations. Most existing KAP studies have focused on general hypertension management rather than severe and potentially fatal hypertension-related complications such as aortic dissection and aortic aneurysm. Therefore, the applicability of the KAP framework in patients who have already experienced acute or life-threatening aortic diseases remains insufficiently examined. Furthermore, a critical appraisal of the current literature via PubMed reveals that existing KAP studies often rely on descriptive correlations without exploring the underlying mechanistic pathways, such as the mediating role of attitudes,17 and frequently utilize non-standardized instruments that limit cross-study comparability.18 In addition, many previous KAP studies have been cross-sectional in design, limiting their ability to clarify whether knowledge is translated into preventive behaviors through attitudes. Accordingly, limited empirical evidence is available regarding disease-specific KAP and the relationships among knowledge, attitudes, and practices in hypertensive patients with AD or aortic aneurysm. Therefore, this study aimed to investigate the KAP of hypertensive patients with AD and aortic aneurysm regarding these conditions and their prevention, and to examine the relationships among knowledge, attitudes, and practices.19
Materials and Methods
Study Design and Participants
This cross-sectional study took place at Henan Chest Hospital from September 15, 2023, to December 15, 2023. The study received approval from the Ethics Committee of Henan Chest Hospital (Approval number: #2023 08–16), and informed consent was obtained from all participants.
Patients with hypertension and Stanford A or B type AD, ascending aortic aneurysm, or abdominal aortic aneurysm, were invited to complete the study. These conditions were included because they are severe aortic diseases closely related to hypertension and require long-term prevention, blood pressure control, and follow-up management. Exclusion criteria: 1) Patients with a history of neurological damage such as stroke, cerebral hemorrhage, epilepsy, or other neurological impairments; 2) Patients displaying preoperative symptoms of coma or consciousness disorders; 3) Patients who declined to participate; 4) Patients with a history of substance abuse or prolonged use of psychotropic drugs, and those with recent significant surgical history.
Questionnaire
The questionnaire was newly developed by the research team specifically for this study, rather than adapted from an existing validated instrument. It was developed with input from three subject matter experts, including two specialists in cardiovascular surgery and one specialist in cardiovascular internal medicine. Content validity was assessed qualitatively through expert review, during which the experts evaluated whether the items were relevant, clear, and appropriate for assessing knowledge, attitudes, and practices related to aortic dissection prevention among hypertensive patients. After receiving feedback from these experts, a preliminary test was conducted with a group of 43 participants, resulting in a reliability Cronbach’s alpha of 0.832.
The final version of the questionnaire consists of four distinct sections: basic information, knowledge, attitudes, and practices. The basic information section comprises 16 items, while the knowledge section includes 11 items, the attitude section has 10 items, and the practices section contains 8 items (Supplement file). During the statistical analysis, scores were assigned based on the response options for each item. For example, in the knowledge section, scores of 2, 1, and 0 were given for complete understanding, partial understanding, and lack of understanding, respectively, with a score range from 0 to 22 points. The attitude section used a five-point Likert scale, ranging from highly positive (5 points) to highly negative (1 point), resulting in a score range of 10 to 50 points. The practices section also utilized a five-point Likert scale, ranging from highly consistent/always (5 points) to highly inconsistent/never (1 point), with a score range of 8 to 40 points. Scores exceeding 70% of the maximum score in each section were considered to reflect satisfactory knowledge, positive attitudes, and proactive practices, consistent with previous KAP research using a 70% cutoff.20
Questionnaire Distribution and Quality Control
The questionnaire was uploaded to the Wenjuanxing platform, and an electronic questionnaire link was generated. A convenience sampling method was employed to select hypertensive patients with AD or aortic aneurysm who received treatment at Henan Chest Hospital between June 2021 and December 2023. Eligible participants were approached by healthcare professionals during hospitalization, follow-up visits, or via telephone using the contact information provided during their hospital stay. The distribution of the questionnaires to participants was guided by healthcare professionals. Participants had the option to complete the questionnaire by scanning a QR code on their smartphones during hospitalization or follow-up visits. Alternatively, they could choose to complete the questionnaire via phone interviews using the contact information provided during hospitalization. The KAP assessment was conducted after diagnosis. For patients with acute aortic dissection, the questionnaire was administered after hospitalization rather than before disease onset or before diagnosis. To ensure consistency between the two data collection methods, the same questionnaire items, response options, and standardized instructions were used for both QR-code self-completion and telephone interviews. Healthcare professionals involved in data collection were instructed not to interpret or explain items beyond the standardized wording, so as to minimize interviewer-related variation. Once all data were collected, the questionnaires were checked for quality by a member of the research team. The questionnaires with obvious logical errors or a pattern of choosing the same options were considered invalid.
Sample Size Calculation
The required sample size was estimated using Cochran’s formula for cross-sectional studies n0 = (Z2 × p × (1 - p)) / e2,21,22 where Z is the standard normal variate at a 95% confidence level (1.96), p is the estimated proportion of the population with adequate knowledge (assumed to be 50% in the absence of prior data), and e is the margin of error (set at 5%). This yielded a minimum sample size of 384 participants. Allowing for a 10% attrition rate, the target sample size was set at 480. Ultimately, 619 participants were included, exceeding the calculated requirement and ensuring sufficient statistical power and reliability of the results.
Statistical Analysis
Data analysis was performed using Stata 14.0 (Stata Corporation, College Station, TX, USA). Prior to statistical analysis, data were screened for invalid responses and assessed for distributional assumptions. Normality of continuous variables was evaluated using the Kolmogorov–Smirnov test, and homogeneity of variance was assessed before conducting parametric analyses. Continuous variables were presented as mean and standard deviation (SD). If the data followed a normal distribution, a t-test was utilized for group comparisons. In cases where normal distribution was not observed, the Wilcoxon Mann–Whitney test was employed to compare two groups. For three or more groups with continuous variables displaying normal distribution and homogeneity of variance, analysis of variance (ANOVA) was used. Alternatively, the Kruskal–Wallis analysis of variance was applied when normal distribution was not met. Categorical variables were presented as frequencies and percentages. Mediation analysis was conducted to explore both direct and indirect effects among the variables: knowledge (K), attitudes (A), and practices (P). The model structure was based on the hypothesized KAP framework, with standardized path coefficients reported. Indirect effects were evaluated using a bias-corrected bootstrap procedure with 1000 resamples. Statistical significance of mediation effects was determined using the 95% bootstrap confidence intervals. Subgroup analysis was performed among participants who reported a confirmed diagnosis of aortic dissection. Within this subgroup, KAP scores were compared across demographic and clinical characteristics using the same statistical tests described above. In addition, mediation analysis based on the KAP framework was repeated in this subgroup to examine whether the relationships among knowledge, attitudes, and practices were consistent with those observed in the overall sample. In this study, statistical significance was determined by a two-sided p-value <0.05.
Results
Basic Characteristics
Initially, the total sample consisted of 628 cases. During data cleaning, 9 cases containing invalid responses were excluded. These invalid responses included selections that did not correspond to the predefined response categories for demographic variables (eg, non-existent response options for gender, marital status, or place of residence). Consequently, a final valid sample of 619 cases was retained for analysis, yielding a validity rate of 98.57%. Among the respondents, 336 (54.28%) participants were aged 46–65 years, and 521 (84.17%) were male. The knowledge, attitude, and practice scores were 4.12±1.25 (range: 0–22), 35.41±3.92 (range: 10–50), and 28.07±2.96 (range: 8–40), respectively (Table 1).
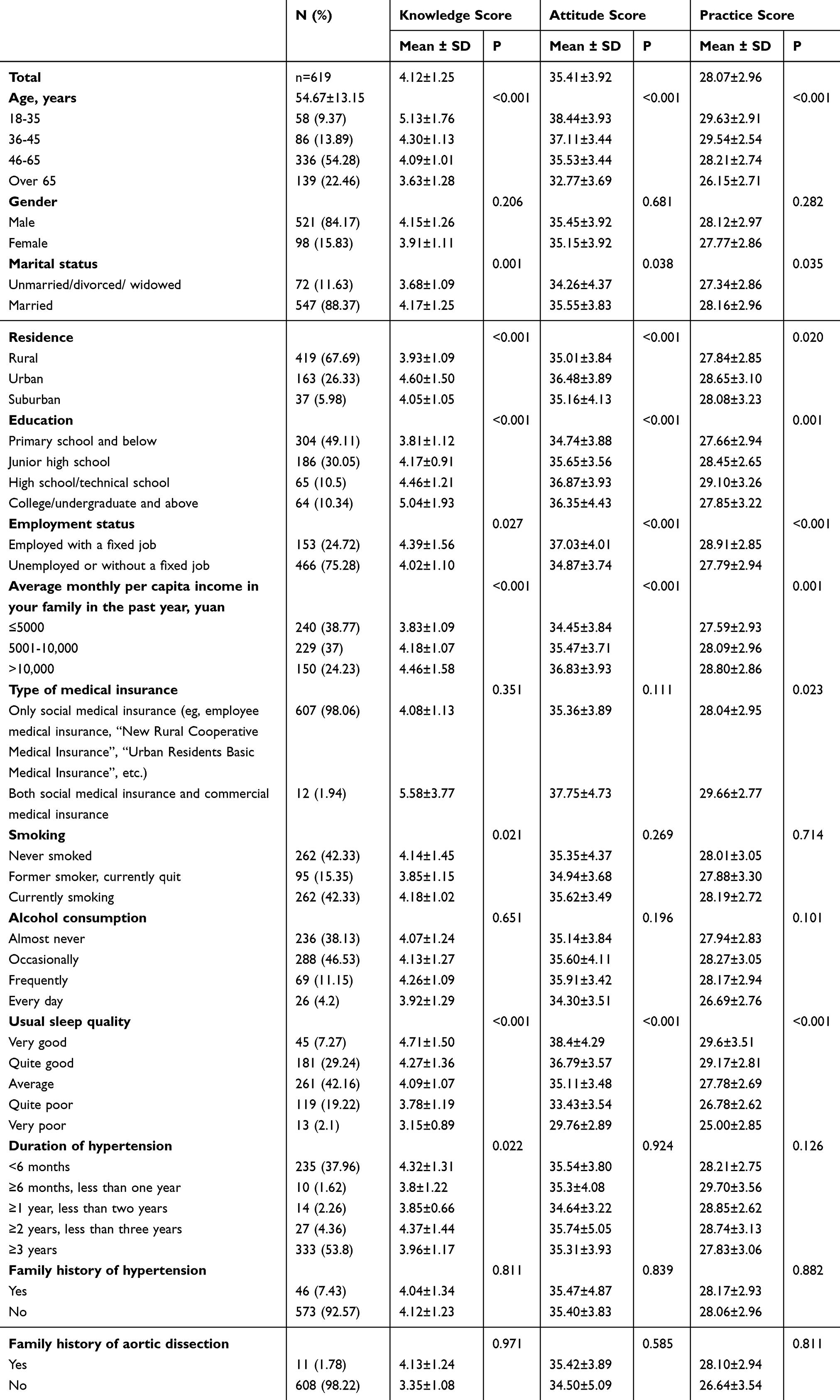 |
Table 1 Basic Characteristics of All Participants |
Distribution of Knowledge, Attitudes, and Practices
The distribution of knowledge dimensions indicated that even after surgery and recovery, complications such as new dissections, organ ischemia, aneurysm formation, or rupture may occur (K11) with 86.59%. Conversely, the two questions with the highest proportion of respondents choosing the “Heard of it but not familiar or have little understanding” option were “Hypertensive patients need to undergo long-term antihypertensive treatment and maintain blood pressure below the target level (140/90 mmHg), which is an important measure to prevent AD (K4)” with 58.64%, and “Besides hypertension, other risk factors for AD include smoking, atherosclerosis, and family inheritance” (K3) with 54.6% (Table 2).
 |
Table 2 Response Distribution for Knowledge Dimension |
Patients’ attitudes towards questions related to AD exhibited variation, with 38.45% agreeing that AD is a very dangerous disease and that hypertensive patients should take active measures to prevent it, while 42.81% were neutral on this point (A1). Additionally, 45.72% recognized the importance of maintaining a good, positive mindset in controlling blood pressure and preventing AD (A7). Conversely, 46.2% disagreed that the effectiveness of measures to prevent AD was uncertain (A3), and 47.17% strongly disagreed with the statement “Taking medication for hypertension every day is troublesome, and it creates an economic burden for the family, so I am unwilling to undergo drug treatment” (A5) (Table 3).
 |
Table 3 Response Distribution for Attitude Dimension |
The distribution of responses on the practice dimension revealed that, regarding quitting smoking or avoiding exposure to second-hand smoke (P3), 30.53% were more aware, 25.69% were less aware, and 29.56% were not concerned. It is also notable that patients did not frequently measure their blood pressure (P6), with 35.06% doing so sometimes and even 23.26% never (Table 4).
 |
Table 4 Response Distribution for Practice Dimension |
Mediation Analysis
Mediation analysis demonstrated that knowledge directly influenced attitudes (β = 0.338, P = 0.010). Attitudes also had direct effects on practices (β = 0.458, P = 0.005, respectively). Moreover, knowledge had an indirect effect on practices through attitudes (β = 0.155, P = 0.006) (Table 5 and Figure S1). The mediation model was saturated (just-identified) with degrees of freedom equal to zero (DF = 0). In such models, the chi-square statistic is necessarily zero, and global fit indices, including the Comparative Fit Index (CFI), the Tucker–Lewis Index (TLI), and the Root Mean Square Error of Approximation (RMSEA), are mathematically constrained (eg, CFI = 1, TLI = 1, RMSEA = 0). Therefore, these indices do not provide evaluative information regarding model fit, and interpretation should instead rely on the significance and magnitude of the estimated path coefficients rather than global model fit statistics. This should be distinguished from latent-variable SEM, in which such ideal fit indices are generally not expected.
 |
Table 5 Direct and Indirect Effects of Path Analysis |
Subgroup Analysis
Subgroup analysis was conducted among participants who reported a confirmed diagnosis of AD (n = 605). The mean knowledge, attitude, and practice scores were 4.13 ± 1.24, 35.43 ± 3.89, and 28.11 ± 2.94, respectively (Supplementary Table 1). Significant differences in KAP scores were observed across age groups, with younger participants demonstrating higher knowledge, more positive attitudes, and better practices than older participants (all P < 0.001). Education level, employment status, residence, monthly household income, and sleep quality were also associated with significant variations in KAP scores (all P < 0.05). In contrast, gender, smoking status, alcohol consumption, family history of hypertension, and family history of aortic dissection were not significantly associated with KAP scores in this subgroup (Supplementary Table 1).
Path analysis indicated that knowledge had a significant direct effect on attitudes (β = 0.328, P < 0.001), while attitudes exerted a strong direct effect on practices (β = 0.451, P < 0.001). Knowledge did not show a significant direct effect on practices (β = 0.038, P = 0.323), but had a significant indirect effect on practices through attitudes (β = 0.148, P < 0.001), indicating a full mediation effect (Supplementary Table 2 and Supplementary Figure 2).
Discussion
Knowledge–Attitude–Practice Discordance in Hypertensive Patients
The findings indicate a marked discordance in the KAP pattern among hypertensive patients with AD, characterized by extremely low knowledge scores (mean 4.12 out of 22, representing less than 20% of the maximum score) alongside comparatively higher attitude and practice scores. This striking contrast represents one of the central observations of the present study. Beyond potential measurement-related factors such as social desirability bias or interviewer effects, this pattern may also reflect a phenomenon of “knowledge–behavior separation”. In clinical settings, patients may adhere to prescribed treatments or lifestyle recommendations primarily due to strong medical advice, routine follow-up requirements, or perceived authority of healthcare providers, without fully understanding the underlying disease mechanisms or preventive rationale. For example, antihypertensive medication adherence may occur as a passive response to physician instruction rather than as a knowledge-driven preventive behavior. Because the KAP assessment was conducted after diagnosis, the findings may reflect post-diagnosis understanding rather than baseline knowledge before disease onset. This also raises the possibility of reverse causality, as disease experience, treatment, hospitalization, and repeated interactions with healthcare providers may have shaped patients’ knowledge, attitudes, and practices after diagnosis. Such partial or externally motivated compliance could result in relatively favorable self-reported practices despite limited disease-specific knowledge. This dissociation between understanding and action has important clinical implications, as behaviors not grounded in comprehension may be less sustainable and more vulnerable to discontinuation when supervision decreases.
The main findings of our study underscore a significant gap in understanding AD and its prevention among hypertensive patients with AD. It is also noteworthy that a considerable proportion of participants expressed neutral attitudes toward certain attitude items, particularly regarding the perceived severity of AD and the necessity of preventive measures. A neutral response may reflect uncertainty, limited confidence in personal understanding, or ambivalence toward disease-related information rather than firm disagreement. This pattern further suggests that although overtly negative attitudes were not dominant, a substantial proportion of patients may lack strong conviction or clarity regarding AD prevention, which could influence the consistency of preventive behaviors. Despite showing positive attitudes and proactive practices towards managing AD, there is a notable lack of knowledge. Consistent with our results, a study noted a limited knowledge of risk factors beyond hypertension and inadequate knowledge of preventive measures among hypertensive patients.23 Although aortic aneurysm differs in clinical presentation from AD, it also represents a life-threatening complication of hypertension, especially when rupture occurs. The low knowledge scores observed in our study may also reflect inadequate knowledge of aneurysm-related risks and the importance of imaging surveillance, blood pressure control, and smoking cessation in preventing aneurysm expansion or rupture. Therefore, education on both AD and aneurysm prevention should be integrated into patient care.
Sociodemographic Variations in KAP Profiles
Descriptive and subgroup analyses revealed notable variations in KAP scores across several demographic and socioeconomic characteristics. In particular, younger participants tended to demonstrate higher knowledge scores and more favorable attitudes and practices compared with older individuals. Similar patterns were observed across levels of education, employment status, residence, household income, and sleep quality. These findings highlight heterogeneity in KAP profiles within the hypertensive population and suggest that differences in information exposure, health literacy, and daily living conditions may contribute to observed variations, without implying independent effects or causal relationships. The identification of lifestyle factors such as smoking status and sleep quality as correlates adds a nuanced perspective to the interaction between lifestyle choices and health literacy. This complexity is not unique to our findings; similar trends have been observed in other studies. For instance, a previous study found that poor sleep quality was significantly linked to higher risks of cardiovascular diseases and hypertension, suggesting a direct influence on health outcomes.24 Similarly, the connection between smoking and cardiovascular health is well-documented, with smoking cessation known to decrease the risk of developing aortic diseases.25 These similarities suggest that lifestyle-related factors may be associated with health management and outcomes among hypertensive patients. These results echo guidelines that emphasize the detrimental effects of poor lifestyle choices on health outcomes in hypertensive patients.26 Such evidence underscores the critical need to address both informational gaps and lifestyle factors in comprehensive interventions.
Mediating Role of Attitudes and Implications for Health Education
Additionally, our mediation analysis results highlighted the important mediating role of attitudes in translating knowledge into practices. Importantly, this mediating structure was replicated in the aortic dissection subgroup, supporting the internal consistency of the KAP framework within patients who had experienced the disease. Although knowledge directly influenced attitudes but had no statistically significant direct effect on practices, attitudes showed a strong direct effect on practices and also mediated the indirect effect of knowledge on practices. Accordingly, this pattern was interpreted as full mediation rather than partial mediation. This finding suggests that merely improving patients’ knowledge about AD may not be sufficient to change their preventive behaviors. Attitudes may represent an important component in understanding how knowledge relates to self-reported practices. This mediating mechanism aligns with the KAP theoretical framework and underscores the importance of comprehensive, multi-level health education strategies.27
Given the cross-sectional and self-reported nature of the data, the present findings primarily describe observed patterns in KAP rather than providing evidence for specific behavioral change mechanisms or intervention effectiveness. The pronounced imbalance between limited knowledge and comparatively favorable attitudes and practices remains a clinically relevant finding that warrants careful consideration in future patient education strategies. Participants demonstrated varying levels of understanding regarding different aspects of AD. However, the coexistence of very low knowledge scores with comparatively favorable attitudes and self-reported practices suggests that attitude and practice measures may not solely reflect actual behavioral competence or informed decision-making. Participants may endorse socially expected attitudes or report desirable practices without a corresponding depth of disease-specific knowledge. This phenomenon may be further amplified by telephone-based data collection, which is known to increase social desirability bias and acquiescent responding. As a result, attitudes and practices may be overestimated relative to objective knowledge. Therefore, the observed discrepancy between low knowledge and relatively favorable attitudes and practices should be interpreted not only as a possible knowledge–behavior separation, but also as a pattern that may have been partly influenced by response bias. It is striking that even among patients who had experienced a life-threatening condition such as AD or aneurysm, understanding of the disease remained limited. Several potential factors may explain this phenomenon. First, there may be insufficient post-discharge health education, as patients often do not receive structured follow-up information about disease management and secondary prevention.28 Second, some patients may face cognitive limitations due to age, comorbidities, or low educational attainment, making it difficult for them to process complex medical information.29 Third, psychological trauma associated with critical illness may lead to emotional avoidance or denial, hindering engagement with preventive knowledge.30 While some participants showed knowledge of certain key concepts related to AD, such as risk factors and preventive measures, others exhibited limited familiarity with the condition. This disparity underscores the need for targeted educational efforts to improve patients’ understanding of AD and its prevention. Specifically, recommendations include developing community-based workshops or online resources that offer accessible and comprehensive information about AD, its risk factors, symptoms, and preventive measures. Collaborating with healthcare providers and local organizations can enhance the reach and effectiveness of these educational efforts, ensuring individuals from diverse backgrounds receive the necessary knowledge to recognize and respond to AD promptly.31,32 Our findings reinforce the importance of patient education and information dissemination as fundamental components of preventive care. Previous studies have emphasized that improving knowledge and understanding of cardiovascular risk factors can significantly contribute to reducing morbidity and mortality associated with aortic aneurysms and dissections.33 Moreover, global trends indicate that increased healthcare expenditure, particularly on preventive care and education, is associated with a decline in mortality from aortic aneurysms and dissections. In Europe, a shift in healthcare investment toward prevention and public knowledge has significantly contributed to improved outcomes.33 While specific data on China’s preventive care expenditure are limited, our findings support the notion that prioritizing education and preventive measures is essential for reducing the burden of aortic diseases.
Participants exhibited varying levels of adherence to recommended practices for preventing and managing AD. While some were willing to engage in proactive behaviors like seeking immediate medical attention for symptoms, others encountered difficulties in implementing lifestyle modifications such as dietary changes. This may involve structured lifestyle modification programs delivered through community centers or healthcare facilities, providing guidance on dietary changes, regular exercise, and stress management techniques. Moreover, integrating telemedicine services can improve access to healthcare professionals for ongoing monitoring and support. By addressing practical challenges and offering continuous support, individuals can develop sustainable habits that decrease their risk of AD and enhance their overall cardiovascular health.34
Limitations and Methodological Considerations
This study had several limitations. Firstly, the data were collected from a single institution, which limits the generalizability of the findings to broader populations. As convenience sampling was used rather than true random sampling, there remains a risk of selection bias. Patients who were more health-conscious, cooperative, or more willing to engage with follow-up may have been overrepresented, which may limit the generalizability of the findings to all hypertensive patients with AD or aortic aneurysm. While this strengthens the internal validity of our findings for our specific center, caution should still be exercised when generalizing results to other healthcare settings or geographical regions with different patient demographics or treatment protocols. Secondly, the cross-sectional design restricts our ability to establish causality or capture temporal relationships between variables. Thirdly, reliance on self-reported measures, such as questionnaire responses, may introduce response bias or inaccuracies due to recall or social desirability biases, potentially influencing the validity of our results. Furthermore, the use of two different data collection methods, mobile phone QR code self-completion and telephone interviews, may have introduced systematic measurement bias. The presence of an interviewer during telephone surveys could increase social desirability bias, particularly for items assessing attitudes and self-reported practices. Participants may have been more likely to provide responses perceived as socially acceptable or consistent with medical advice when interacting directly with healthcare staff. This potential mode effect could partly explain the comparatively high attitude and practice scores observed despite extremely low knowledge levels. As the study did not formally compare responses across data collection modes, the extent of this bias cannot be quantified, and future studies should consider using uniform administration methods or conducting mode-specific analyses to minimize such systematic differences. Finally, although both abdominal aortic aneurysm and acute AD share a common association with hypertension, these conditions differ in their clinical presentation and progression. The small number of patients with abdominal aortic aneurysm (only 14 cases) in our study limited our ability to analyze these groups separately. In addition, the inclusion of patients with different medical conditions—namely Stanford type A and B AD, ascending aortic aneurysm, and abdominal aortic aneurysm—may have introduced clinical heterogeneity. Patients with acute AD may have experienced sudden symptoms, hospitalization, or surgical/interventional treatment, which could increase their exposure to disease-related information and influence their KAP responses. In contrast, patients with aortic aneurysm may have a more chronic or asymptomatic disease course, and their risk perception and preventive behaviors may differ from those of patients with acute AD. Because the KAP assessment was performed after diagnosis, the observed KAP scores may partly reflect post-event disease experience, treatment history, hospitalization, or exposure to health education rather than baseline understanding before disease onset. Due to the limited number of patients with aortic aneurysm and the lack of detailed data on disease severity, treatment history, and exposure to health education, we were unable to conduct stratified analyses or adjust for these factors; therefore, the relationships between KAP and clinical conditions should be interpreted cautiously, and the generalizability of the findings to the broader hypertensive population may be limited.
Conclusion
In conclusion, this study describes a distinct KAP profile among hypertensive patients with AD, characterized by markedly limited disease-related knowledge alongside relatively favorable attitudes and self-reported practices. This imbalance suggests that certain preventive behaviors may occur in the absence of adequate disease-specific understanding, highlighting a potential separation between knowledge and action. However, this pattern may also be partly influenced by measurement bias, including social desirability bias and the self-reported nature of attitude and practice measures. In addition, clinical heterogeneity between acute aortic dissection and more chronic aortic aneurysm conditions may have influenced patients’ disease experience, risk perception, and KAP responses.
These findings underscore the presence of substantial knowledge gaps and heterogeneity in KAP patterns within this population. However, given the cross-sectional and self-reported nature of the data, the results should be interpreted as descriptive rather than indicative of causal relationships or intervention effects. Future studies using longitudinal designs and objective behavioral measures are warranted to further clarify how knowledge, attitudes, practices, disease experience, and healthcare interactions influence one another in this clinical context.
Data Sharing Statement
All data generated or analyzed during this study are included in this article and supplementary information files.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Henan Provincial Chest Hospital (Approval number: #2023 08-16). All participants were informed about the study protocol and provided written informed consent to participate in the study I confirm that all methods were performed in accordance with the relevant guidelines. All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Key Clinical Specialty Construction Project of China.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Cho EJ, Sung KC, Kang SM, Shin MS, Joo SJ, Park JB. Fimasartan reduces clinic and home pulse pressure in elderly hypertensive patients: a K-MetS study. PLoS One. 2019;14(4):e0214293. doi:10.1371/journal.pone.0214293
2. Yusuf S, Joseph P, Rangarajan S, et al. Modifiable risk factors, cardiovascular disease, and mortality in 155 722 individuals from 21 high-income, middle-income, and low-income countries (PURE): a prospective cohort study. Lancet. 2020;395(10226):795–14. doi:10.1016/S0140-6736(19)32008-2
3. Nienaber CA, Clough RE, Sakalihasan N, et al. Aortic dissection. Nat Rev Dis Primers. 2016;2(1):16053. doi:10.1038/nrdp.2016.53
4. Ahlsson A, Wickbom A, Geirsson A, et al. Is there a weekend effect in surgery for type A dissection?: results from the nordic consortium for acute type A aortic dissection database. Ann Thorac Surg. 2019;108(3):770–776. doi:10.1016/j.athoracsur.2019.03.005
5. Lu J, Li P, Ma K, et al. OPG/TRAIL ratio as a predictive biomarker of mortality in patients with type A acute aortic dissection. Nat Commun. 2021;12(1):3401. doi:10.1038/s41467-021-23787-5
6. Chewcharat A, Hamaya R, Thongprayoon C, Cato LD, Mao MA, Cheungpasitporn W. The association between simple renal cyst and aortic diseases: a systematic review and meta-analysis of observational studies. J Evid Based Med. 2020;13(4):265–274. doi:10.1111/jebm.12385
7. Hagan PG, Nienaber CA, Isselbacher EM, et al. The international registry of acute aortic dissection (IRAD): new insights into an old disease. JAMA. 2000;283(7):897–903. doi:10.1001/jama.283.7.897
8. Kent KC. Clinical practice. Abdominal aortic aneurysms. N Engl J Med. 2014;371(22):2101–2108. doi:10.1056/NEJMcp1401430
9. Sakalihasan N, Limet R, Defawe OD. Abdominal aortic aneurysm. Lancet. 2005;365(9470):1577–1589. doi:10.1016/S0140-6736(05)66459-8
10. Shaw JE; NCD Risk Factor Collaboration. Worldwide trends in blood pressure from 1975 to 2015: a pooled analysis of 1479 population-based measurement studies with 19·1 million participants. Lancet. 2017;389(10064):37–55. doi:10.1016/S0140-6736(16)31919-5
11. Abdalla AA. Knowledge, attitude and practice towards therapeutic lifestyle changes in the management of hypertension in Khartoum State. Cardiovasc J Afr. 2021;32(4):198–203. doi:10.5830/CVJA-2021-011
12. Chen L, Liu Y, Xi X. Study of knowledge, attitude and practice regarding patient education in hypertension among community pharmacists in China. BMC Health Serv Res. 2022;22(1):1295. doi:10.1186/s12913-022-08686-9
13. Tan J, Luo L, Zhang M, et al. A Chinese and Western medication adherence scale in patients with chronic kidney disease. Patient Prefer Adherence. 2019;13:1487–1495. doi:10.2147/PPA.S207693
14. Khalid A, Haque S, Alvi S, et al. Promoting health literacy about cancer screening among Muslim immigrants in Canada: perspectives of imams on the role they can play in community. J Prim Care Community Health. 2022;13:21501319211063051. doi:10.1177/21501319211063051
15. Machaalani M, Fakhry B, Zwaideh M, et al. Knowledge, attitude, and practice toward cardiovascular diseases in the Lebanese population. Glob Heart. 2022;17(1):47. doi:10.5334/gh.1138
16. Li L, Zhang J, Qiao Q, Wu L, Chen L. Development, reliability, and validity of the “knowledge-attitude-practice” questionnaire of foreigners on traditional Chinese medicine treatment. Evid Based Complement Alternat Med. 2020;2020(1):8527320. doi:10.1155/2020/8527320
17. McAnally K, Hagger MS. Health literacy, social cognition constructs, and health behaviors and outcomes: a meta-analysis. Health Psychol. 2023;42(4):213–234. doi:10.1037/hea0001266
18. Mallah N, Rodríguez-Cano R, Figueiras A, Takkouche B. Design, reliability and construct validity of a knowledge, attitude and practice questionnaire on personal use of antibiotics in Spain. Sci Rep. 2020;10(1):20668. doi:10.1038/s41598-020-77769-6
19. Zhang K, Gao S, Zhou C, et al. Knowledge, attitude and practice towards postoperative management among patients with type A aortic dissection or their relatives: a cross-sectional study in China. BMJ Open. 2024;14(12):e086623. doi:10.1136/bmjopen-2024-086623
20. Wang D, Pan X, Wang J. Skin care knowledge, attitudes and practices: a comparative study between patients with atopic dermatitis and healthy individuals. BMC Public Health. 2025;25(1):3898. doi:10.1186/s12889-025-25264-w
21. Monti CB, Ambrogi F, Sardanelli F. Sample size calculation for data reliability and diagnostic performance: a go-to review. Eur Radiol Exp. 2024;8(1):79. doi:10.1186/s41747-024-00474-w
22. Wang X, Ji X. Sample size estimation in clinical research: from randomized controlled trials to observational studies. Chest. 2020;158(1s):S12–s20. doi:10.1016/j.chest.2020.03.010
23. Okai DE, Manu A, Amoah EM, Laar A, Akamah J, Torpey K. Patient-level factors influencing hypertension control in adults in Accra, Ghana. BMC Cardiovasc Disord. 2020;20(1):123. doi:10.1186/s12872-020-01370-y
24. Grandner MA, Jackson NJ, Pak VM, Gehrman PR. Sleep disturbance is associated with cardiovascular and metabolic disorders. J Sleep Res. 2012;21(4):427–433. doi:10.1111/j.1365-2869.2011.00990.x
25. Wong ND. Epidemiological studies of CHD and the evolution of preventive cardiology. Nat Rev Cardiol. 2014;11(5):276–289. doi:10.1038/nrcardio.2014.26
26. Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European society of hypertension (ESH) and of the European society of cardiology (ESC). J Hypertens. 2013;31(7):1281–1357. doi:10.1097/01.hjh.0000431740.32696.cc
27. Nutbeam D, Lloyd JE. Understanding and responding to health literacy as a social determinant of health. Annu Rev Public Health. 2021;42(1):159–173. doi:10.1146/annurev-publhealth-090419-102529
28. Jack BW, Chetty VK, Anthony D, et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med. 2009;150(3):178–187. doi:10.7326/0003-4819-150-3-200902030-00007
29. Wolf MS, Gazmararian JA, Baker DW. Health literacy and functional health status among older adults. Arch Intern Med. 2005;165(17):1946–1952. doi:10.1001/archinte.165.17.1946
30. Davydow DS, Gifford JM, Desai SV, Needham DM, Bienvenu OJ. Posttraumatic stress disorder in general intensive care unit survivors: a systematic review. Gen Hosp Psychiatry. 2008;30(5):421–434. doi:10.1016/j.genhosppsych.2008.05.006
31. Jiang Y, Tang X, Wang Y, et al. Serum oxylipin profiles identify potential biomarkers in patients with acute aortic dissection. Metabolites. 2022;12(7):587. doi:10.3390/metabo12070587
32. Lu N, Ma X, Xu T, et al. Optimal blood pressure control for patients after thoracic endovascular aortic repair of type B aortic dissection. BMC Cardiovasc Disord. 2019;19(1):124. doi:10.1186/s12872-019-1107-2
33. Sterpetti AV, Gabriele R, Iannone I, Sapienza P, Marzo LD. The role of education and information to prevent trends towards increase of cardiovascular mortality rates in Europe from 2015 TO 2019. Curr Probl Cardiol. 2024;49(3):102415. doi:10.1016/j.cpcardiol.2024.102415
34. Lian G, Li X, Zhang L, et al. Macrophage metabolic reprogramming aggravates aortic dissection through the HIF1α-ADAM17 pathway(✰). EBioMedicine. 2019;49:291–304. doi:10.1016/j.ebiom.2019.09.041
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge, Attitudes, and Practices Among Patients with Systemic Lupus Erythematosus Toward Disease Management and Biologic Therapy
Liu X, Song Y, Wan L, Du R
Journal of Multidisciplinary Healthcare 2024, 17:937-947
Published Date: 2 March 2024
Knowledge, Attitudes, and Practices Among Community Populations Toward Long COVID in China
He N, Tunala S, Wu R, Zhao C, Wuren T, Hushuud C
International Journal of General Medicine 2024, 17:4455-4463
Published Date: 1 October 2024
Knowledge, Attitudes, and Practices Regarding Swallowing Disorders Among General Practitioners
Zou M, Zhu X, Li J, Yu H, Guo P
International Journal of General Medicine 2025, 18:1555-1567
Published Date: 18 March 2025
Knowledge, Attitudes and Practices Toward Hypotension During Hemodialysis Among Nephrology and Hemodialysis Medical Staff: A Multi-Center Cross-Sectional Study
Cheng D, Xie L, Chu X, Bai Y, He T
Journal of Multidisciplinary Healthcare 2025, 18:5359-5369
Published Date: 28 August 2025
Knowledge, Attitudes, and Practices Toward Microvascular Decompression for Hemifacial Spasm Among Neurosurgeons: A Multicenter Cross-Sectional Study
Xu Y, Dong S, Zhao R, Liu J, Han P, Guo Y, Jiang R
Journal of Multidisciplinary Healthcare 2025, 18:8277-8291
Published Date: 27 December 2025