Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Knowledge, Attitudes, and Practices Among Patients with Systemic Lupus Erythematosus Toward Disease Management and Biologic Therapy
Authors Liu X, Song Y, Wan L, Du R
Received 13 October 2023
Accepted for publication 19 January 2024
Published 2 March 2024 Volume 2024:17 Pages 937—947
DOI https://doi.org/10.2147/JMDH.S444619
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Xiaojing Liu,* You Song,* Limin Wan, Rong Du
Department of Rheumatology and Immunology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Rong Du, Department of Rheumatology and Immunology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China, Email [email protected]
Background: This study aims to investigate the knowledge, attitudes, and practices (KAP) among patients with systemic lupus erythematosus (SLE) toward disease management and biologic therapy.
Methods: This cross-sectional study was conducted between April 20, 2023, and May 5, 2023, among patients with SLE at Union Hospital Affiliated to Tongji Medical College, Huazhong University of Science and Technology. A self-designed questionnaire was developed to collect demographic information of SLE patients and assess their KAP.
Results: A total of 463 SLE patients participated. The mean scores for knowledge, attitudes, and practices were 8.52 ± 2.36 (possible range: 0– 11), 39.40 ± 3.38 (possible range: 11– 55), and 27.10 ± 6.29 (possible range: 8– 40), respectively. The path analysis demonstrated a significant and positive association between knowledge and attitudes, as indicated by a path coefficient of 0.455 (p < 0.001), and a significant and positive relationship between knowledge and practices, with a path coefficient of 0.709 (p < 0.001).
Conclusion: Patients with SLE exhibited insufficient knowledge, negative attitudes, and poor practices.
Keywords: knowledge, attitudes, practices, systemic lupus erythematosus, biologic therapy, cross-sectional study
Background
Systemic lupus erythematosus (SLE), a chronic, systemic autoimmune disease, is characterized by the presence of numerous autoantibodies in the bloodstream and multi-organ involvement. With alternating periods of remission and relapse, SLE poses a significant chronic health threat. The majority of SLE cases in China occur in young individuals. Data from the Chinese SLE Treatment and Research group (CSTAR) demonstrate an average onset age of 30.7 years, with a female-to-male ratio of 12:1.1,2
Conventional approaches for SLE involve glucocorticoids and immunosuppressive agents. However, their long-term use presents challenges due to toxic side effects. In light of advancing knowledge concerning the molecular mechanisms underlying autoimmune diseases, novel therapeutic targets have been identified, leading to the development of biologic therapy that selectively intervenes in specific targets. Biologic therapy not only demonstrates comparable or superior efficacy to traditional therapies but also exhibits fewer adverse reactions and faster onset of action.3 Despite these advantages, the high cost of biologic therapy poses a considerable financial burden for SLE patients, who already face economic challenges associated with their condition.
SLE substantially impacts patients’ lives, work, and social activities, often resulting in limited physical capabilities and job loss. A cross-sectional study evaluating the employment status of Chinese SLE patients, which included 105 patients who were employed at the time of their SLE diagnosis, demonstrated that 39 (37%) of these patients lost their ability to work due to SLE, with this occurring after an average disease duration of 10.0 ± 6.1 years.4 Another contributing factor to the limited adoption of biologic therapy is the insufficient awareness among SLE patients toward disease management and available treatment options. Several surveys investigating disease awareness among SLE patients indicate insufficient knowledge, limited access to disease-related information, and a notable lack of awareness regarding treatment medications.5,6
Both the economic burden faced by SLE patients and their limited understanding of disease management have a substantial impact on their attitudes, practices, and willingness to opt for biologic therapy as a treatment, as well as their active involvement in disease management, consequently impacting the prognosis of SLE patients.
The Knowledge, Attitude, Practice model (abbreviated as KAP) is one of the most commonly used models to explain how an individual’s knowledge and beliefs influence changes in health behavior and is one of the models for changing human health-related behaviors. It divides the process of behavior change into three continuous stages: acquiring knowledge, developing beliefs, and forming behaviors.7,8
Hence, it is crucial to explore KAP of Chinese SLE patients concerning disease management and the utilization of biologic therapy. This study adopts the KAP model to examine the associations between these variables, aiming to contribute valuable insights to future medical education endeavors promoting disease management and the utilization of biologic therapy in China.
Materials and Methods
Study Design and SLE Patients
This web-based cross-sectional study was conducted at Union Hospital Affiliated to Tongji Medical College, Huazhong University of Science and Technology between April 25, 2023, and May 5, 2023. The inclusion criteria were as follows: 1) aged between 18 and 60 years; 2) individuals who met the classification criteria for SLE according to the publications by the American College of Rheumatology (ACR) in 1997, the Systemic Lupus International Collaborating Clinics (SLICC) in 2012, or the European League Against Rheumatism (EULAR)/ACR in 2019. Those diagnosed with tuberculosis, hepatitis B, or cancer were excluded. This study was approved by the Medical Ethics Committee of Union Hospital Affiliated to Tongji Medical College, Huazhong University of Science and Technology, and informed consent was obtained from SLE patients.
Questionnaire
The questionnaire was designed with reference to the related literature review9,10 and 2020 Chinese Guidelines for the Diagnosis and Treatment of Systemic Lupus Erythematosus.11 The questionnaire was refined based on feedback from four experts and a pilot study (n = 140) demonstrated a Cronbach’s alpha coefficient of 0.765, indicating good internal reliability.
The final version of the questionnaire was in Chinese and consisted of four dimensions: demographic information, knowledge, attitudes, and practices. The knowledge dimension comprises 11 items, while the attitude and practice dimensions include 11 and 8 items, respectively. Each correct answer for the knowledge items received a score of 1 point, while incorrect answers received 0 points, resulting in a possible score range of 0–11. The attitude and practice dimensions were assessed using a 5-point Likert scale, where responses ranged from the most positive option (5 points) to the least positive option (1 point), which resulted in possible score ranges of 11–55 for attitude and 8–40 for practice, respectively. The data were collected using an online questionnaire hosted on Sojump (http://www.sojump.com). The study disseminated the questionnaire to SLE patients through WeChat groups specifically for SLE patients and via a medical-patient management app of Union Hospital Affiliated to Tongji Medical College, Huazhong University of Science and Technology. This approach involved distributing QR codes and web links to the questionnaire through the aforementioned channels.
Statistical Analysis
STATA 17.0 (Stata Corporation, College Station, TX, USA) was used for statistical analysis. In the collected questionnaires, missing values were imputed by employing the mean value of the dataset. The continuous variables were expressed as Mean ± SD, and the categorical variables were expressed as n (%). The continuous variables conformed to a normal distribution were tested by the t-test or ANOVA. Pearson correlation was used to analyze the correlation between knowledge, attitudes, and practices. This study used the 80% of the total score of knowledge, attitudes, and practices, respectively, as the cutoff values for the three dimensions: knowledge (with a threshold score of 8.8 points), attitude (with a threshold score of 44 points), and practice (with a threshold score of 32 points). The path analysis of knowledge, attitudes, and practices among SLE patients toward disease management and biologic therapy was constructed with AMOS 24.0 (IBM, NY, United States). The model fitting was evaluated with CMIN/DF (Chi-square fit statistics/degree of freedom), RMSEA (root mean square error of approximation), IFI (incremental fix index), TLI (Tucker-Lewis index), and CFI (comparative fix index). Two-sided p < 0.05 were considered statistically significant.
Results
A total of 463 questionnaires were collected. Among the SLE patients, 421 (90.9%) of them were female, 386 of them aged between 20 and 49 years (83.4%), 311 of them were married (67.2%), 205 of them have a per capita income of 2000–5000 CNY (44.3%) and 147 diagnosed with SLE for over 10 years (31.7%) (Table 1).
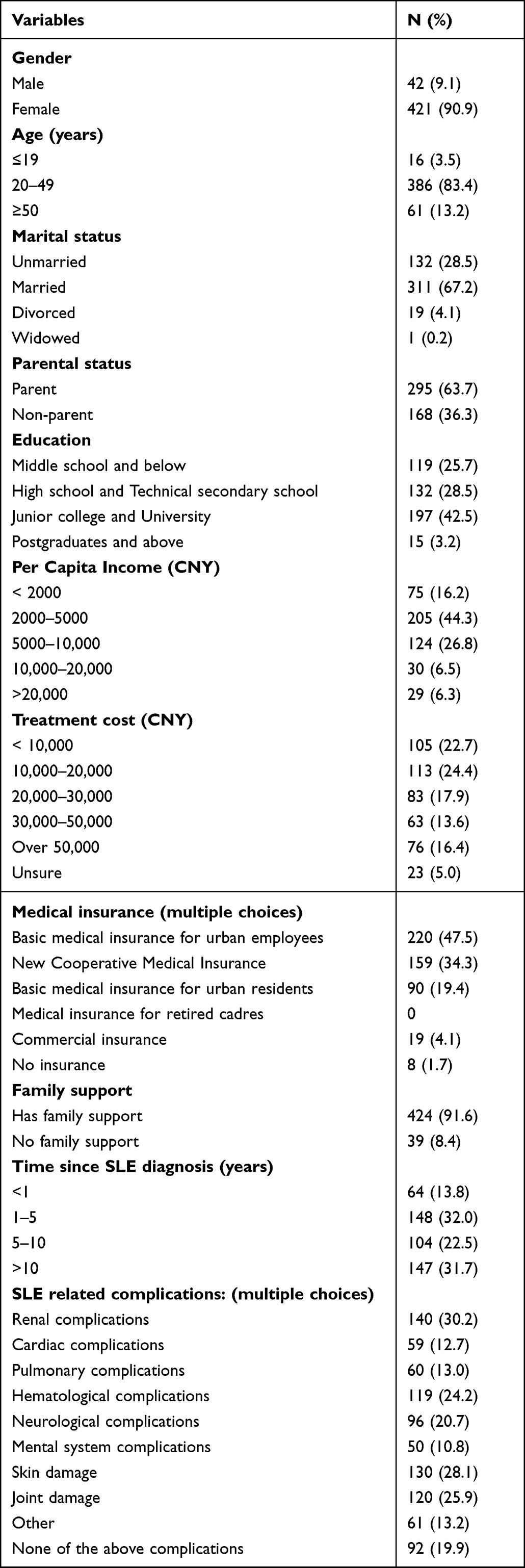 |
Table 1 Demographic Characteristics |
Meanwhile, this study investigated the prevalence of drug use among SLE patients (Table S1). In the existing treatment regimens of SLE patients, the most frequently prescribed medication is glucocorticoids (93.1%), followed by hydroxychloroquine (68.7%), immunosuppressants (58.3%), and biological agents (27.4%). The findings indicate that a majority of patients (63.9%) preferred subcutaneous injections, while 36.1% favored intravenous injections. Moreover, 41.3% of patients were both willing and able to use biologic therapy, 6.5% could afford the cost but chose not to use it, 21.6% were unable to afford the cost and therefore refrained from using it, and 30.7% found the cost to be a significant financial burden but still opted for biologic therapy as a treatment for SLE. Notably, a considerable proportion (98.7%) of SLE patients expressed the belief that incorporating biologic therapy into China’s medical insurance coverage would enhance its acceptance. Among users of biological agents (n=127), Telitacicept was used by 81.9%, Belimumab by 27.6%, and Rituximab by 2.4%. Regarding patients’ perceptions of biologic therapy, 52% felt it was both safe and effective, 39.4% believed the efficacy and adverse reactions were unclear, and 7.9% deemed the effect acceptable but experienced serious adverse reactions due to the medication (Table S1).
The mean score of knowledge, attitude, and practice were 8.52 ± 2.36 (possible range: 0–11), 39.40 ± 3.38 (possible range: 11–55), and 27.10 ± 6.29 (possible range: 8–40), respectively. The knowledge score varied from those with different age (P = 0.033), marital status (P < 0.001), parental status (P < 0.001), education (P < 0.001), treatment cost (P = 0.001), and number of SLE-associated complications (P = 0.006). As for the attitude score, there were difference among SLE patients with different education (P = 0.004), treatment cost (P = 0.001), family support (P = 0.035), time since SLE diagnosis (P = 0.045), and number of SLE-associated complications (P = 0.060). The difference of practice score were found among patients different education (P = 0.005), treatment cost (P < 0.001) and number of SLE-associated complications (P = 0.040, Table 2).
 |
Table 2 KAP Scores |
The knowledge items with the highest correctness were “Systemic lupus erythematosus (SLE) is a systemic autoimmune disease that affects multiple organs and can result in severe and potentially fatal outcomes.” (K1), “Current pharmacological interventions for SLE encompass glucocorticoids, anti-inflammatory drugs, immunosuppressants, and biological agents.” (K6), “The etiology of SLE is multifactorial and involves a complex interplay among genetics, hormones, and environmental factors” (K2) and “SLE patients may experience various complications that affect the lungs, cardiovascular system, and nervous system.” (K4) with the correctness of 92.7%, 90.7%, 89.6%, and 89.6%, respectively. The three items with the lowest correctness were “Infection remains the primary cause of mortality in patients with SLE.” (K5), “The administration of biological agents for SLE treatment may be accompanied by adverse effects, including gastrointestinal discomfort, diarrhea, infection, headache, and others.” (K8) and “Biological agents may exhibit particular efficacy in cases of refractory or relapsed SLE, potentially enabling a reduction in hormone dosages.” (K11) with correctness of 52.7%, 59.0%, and 71.7%, respectively. It can be inferred that SLE patients generally possess a satisfactory understanding of the disease’s characteristics and the appropriate medication regimen. However, they exhibit limited awareness regarding the high-risk complications associated with SLE, the benefits of biological therapy, and the potential adverse reactions (Table 3).
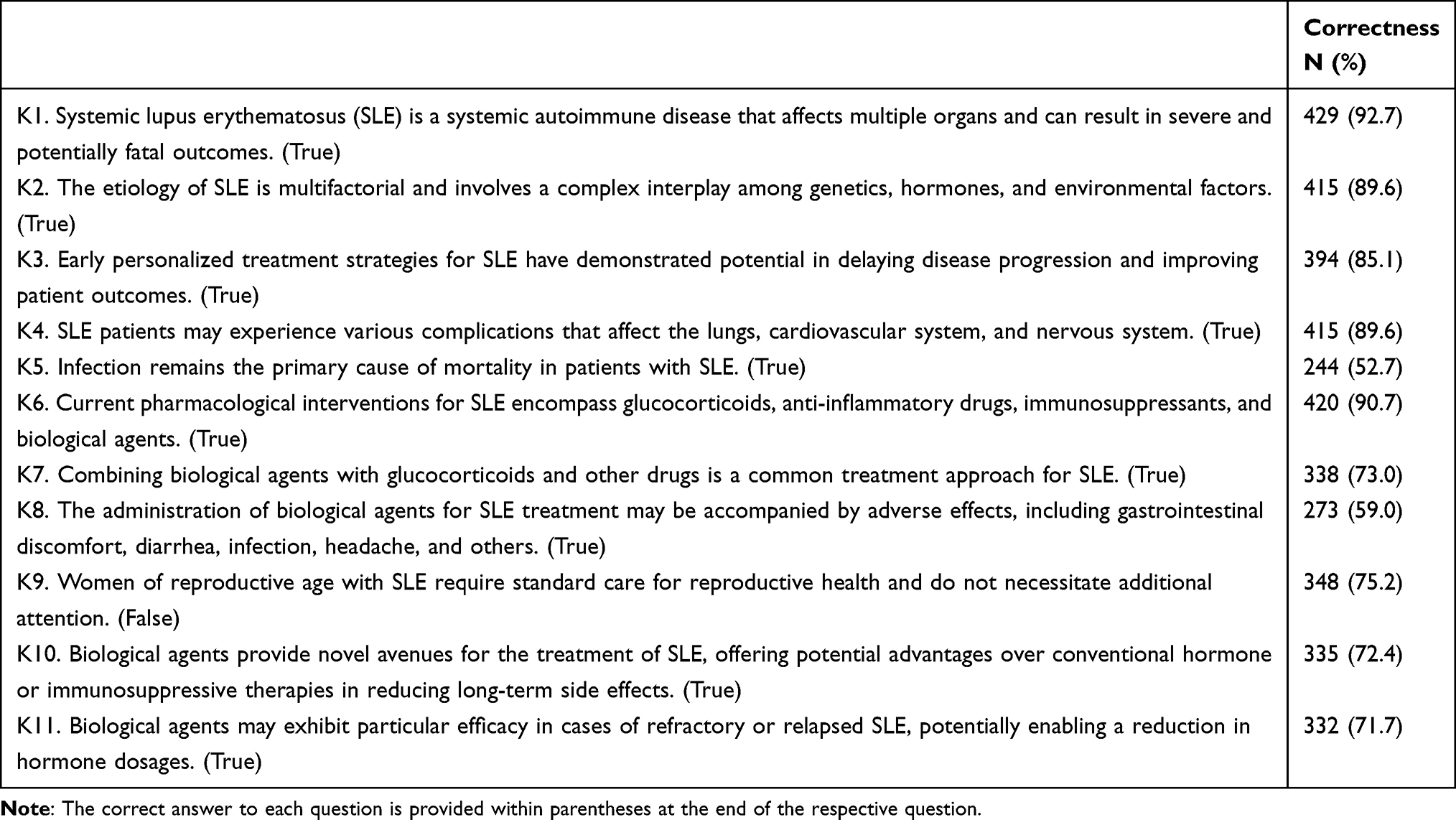 |
Table 3 Knowledge |
Regarding the attitudes of SLE patients toward disease management and biologic therapy, approximately 65.7% of the SLE patients strongly agree that it is crucial to receive early treatment for SLE in the early stages of the disease. (A3) and 60.5% strongly agreed that it is important for SLE patients to focus on their own health conditions, including the disease itself, complications, and infections, and to promptly inform the doctor if any abnormalities are detected (A6). When it comes to fertility, 58.5% strongly agree that it is crucial for female SLE patients to undergo pre-pregnancy consultations and multidisciplinary assessments involving obstetrics and gynecology (A7) and 66.9% strongly agree/agree that it leads to anxiety about reproductive issues caused by the disease (A5). Moreover, the results showed a lack of recognition of adverse drug reactions among SLE patients, with only 16.4% strongly agreeing that among adverse drug reactions, it causes anxiety regarding potential adverse reactions such as nausea, vomiting, and infusion reactions caused by biologics and other medications (A11) (Table 4).
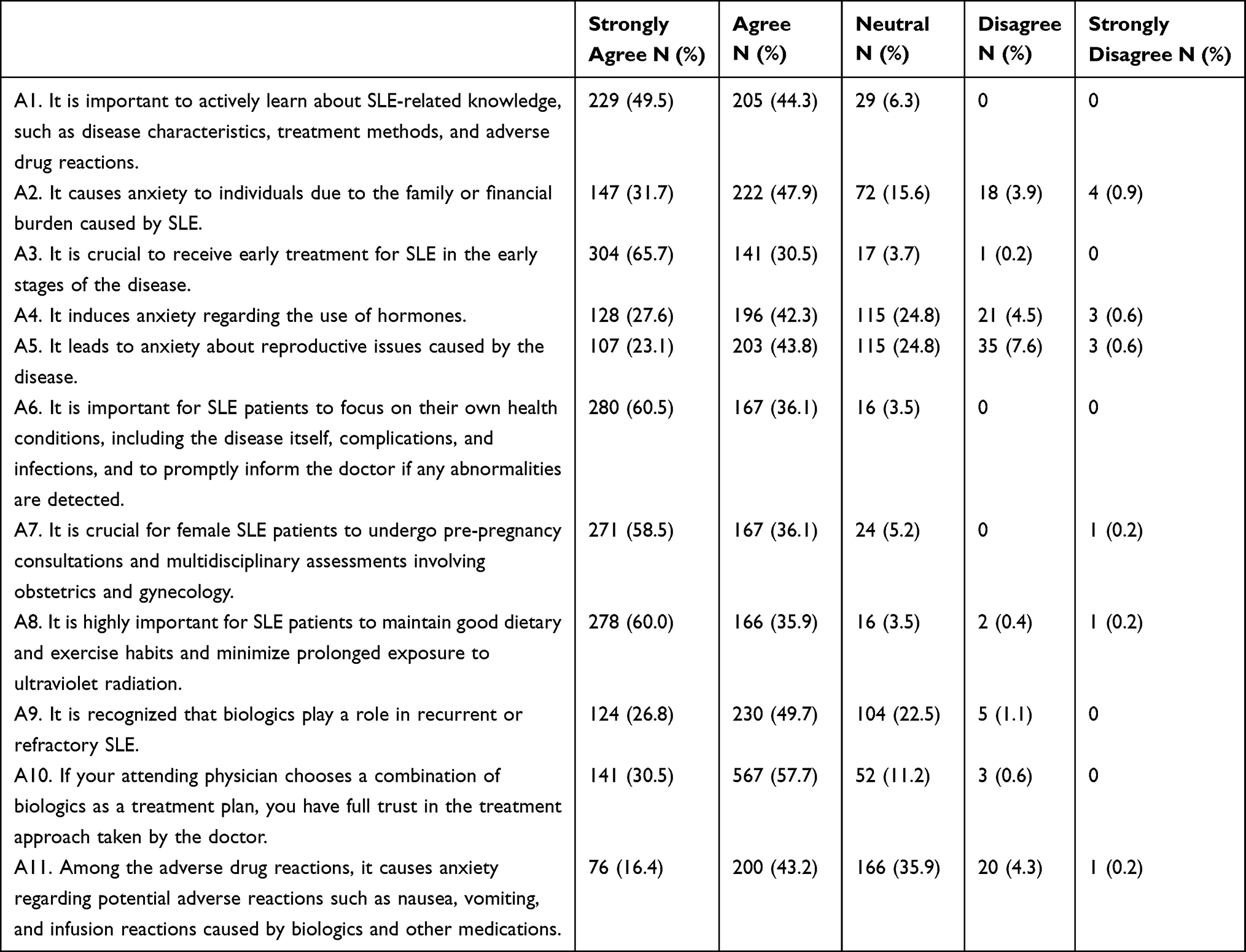 |
Table 4 Attitudes |
Regarding the practice, it was shown that only 10.4% of the SLE patients actively acquire knowledge about SLE (P1) and only 8.9% of them seek psychological support, such as confiding in family and friends or participating in psychological counseling (P5). Nevertheless, 59.8% always/often engage in skincare for SLE or take proactive measures to avoid prolonged exposure to ultraviolet radiation (P7) and 68.7% report a high adherence toward medical advice regarding the timely and proper use of medications (P8) (Table 5).
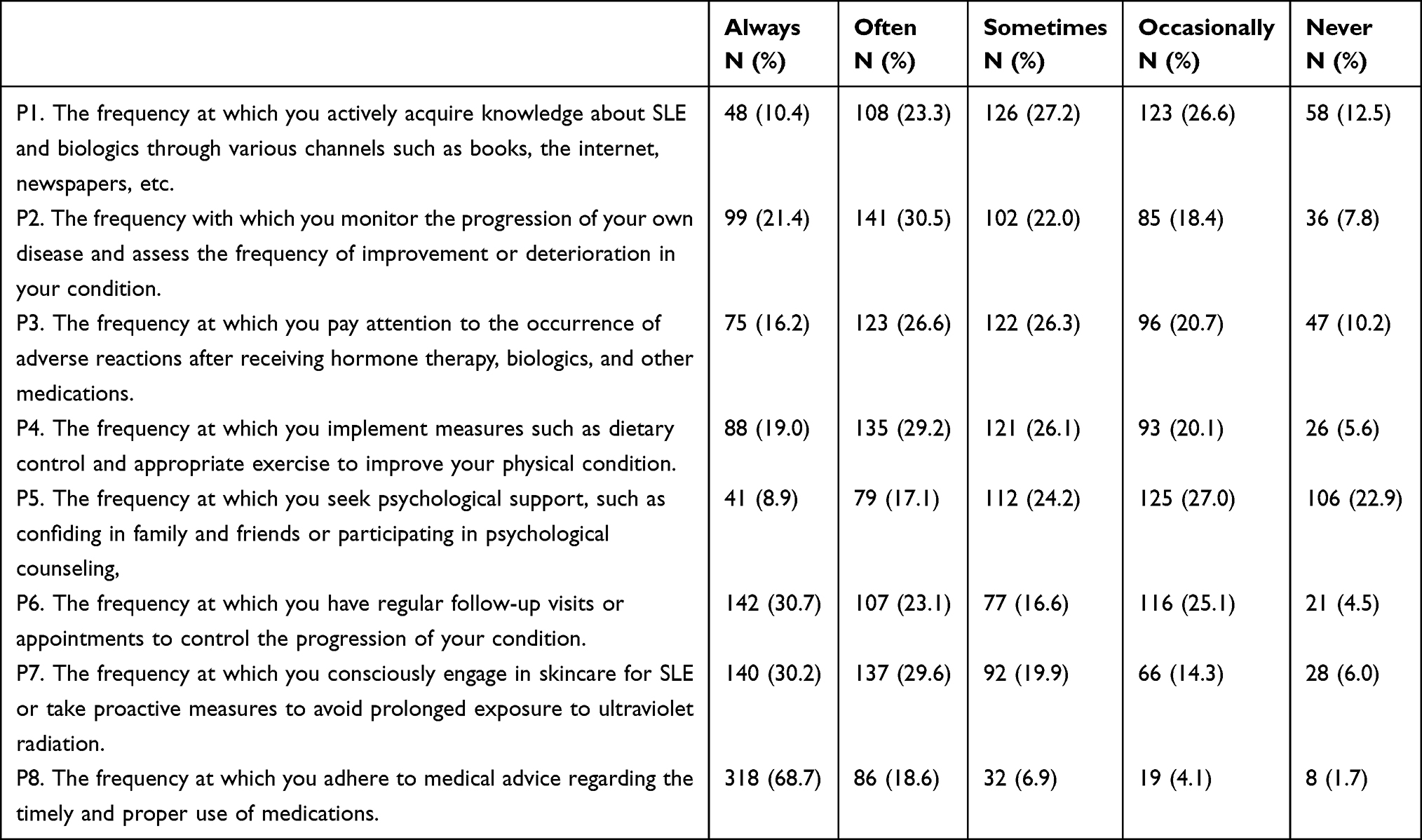 |
Table 5 Practices |
A correlation analysis was performed to assess the relationship between knowledge, attitudes, and practices. It was shown that the knowledge and the attitudes were positively correlated (r = 0.327, P < 0.001), and knowledge and practices were also positively correlated (r = 0.269, P < 0.001). Additionally, there was a positive correlation between attitude and practice scores (r = 0.102, P < 0.001) (Table S2).
Path analysis was established to further investigate whether SLE patients’ knowledge and attitude toward disease management and biologic therapy affect their practice, whether attitude plays an intermediary role between knowledge and practice, and whether knowledge can directly affect their practice according to the KAP theory. It also investigated the effect of other factors including “parental status “family support “time since SLE diagnosis” and “per capital income” on the three dimensions mentioned above (Figure 1).
Hypothesis 1: The path coefficient from knowledge to attitudes is 0.455 (P < 0.001), which indicates that SLE patients’ knowledge level is positively and significantly associated with their attitudes. Hypothesis 2: The path coefficient from knowledge to practice is 0.709 (P < 0.001), which indicates that their knowledge level is positively and significantly associated with their practices. Hypothesis 3: The path coefficient from attitude to practice is 0.049 (P = 0.580), indicating that the patients’ attitude was positively associated with practice, however the path coefficient was not significant. Hypothesis 4: The path coefficient from family support to attitude is −1.187 (P = 0.025), indicating that family support was inversely related to attitude. Hypothesis 5: The path coefficient from time since SLE diagnosis to attitude is 0.330 (P = 0.018), which indicates that time since SLE diagnosis will impact patients’ attitude toward disease management and biologic therapy. Hypothesis 6: The path coefficient from parental status to knowledge is 0.591 (P = 0.009), which indicates that parental status positively and significantly associated with their knowledge. Hypothesis 7: The path coefficient from time since SLE diagnosis to practice is −0.817 (P = 0.002), which indicates that time since SLE diagnosis was inversely related to attitude (Figure 1, Table S3).
 |
Figure 1 The KAP path analysis. |
The fitting index of the structural model (CMIN/DF = 1.533; RMSEA = 0.034; IFI = 0.948; TLI = 0.902; CFI = 0.944) outperformed the respective threshold value, signifying that the data fit the structural model satisfactorily (Table S4).
Discussion
Patients with SLE exhibited insufficient knowledge, negative attitudes, and poor practices toward disease management and biologic therapy. The present study aligns with the findings of the CSTAR survey and previous cross-sectional investigations on SLE patients.
SLE patients showed suboptimal awareness of the potential adverse effects of biologic therapy. This finding is consistent with previous studies that have reported low levels of disease-specific knowledge among SLE patients. An online survey of the Spanish Lupus Patient Association (FELUPUS) reported that 73% of Spanish SLE patients perceived a lack of knowledge about the disease at the time of diagnosis, with 92% of patients having a low level of SLE knowledge.12 Similarly, a study analyzed SLE patients’ knowledge and health-related quality of life found very low baseline levels of SLE knowledge among Iranian SLE patients, with a significant impact on patients’ health-related quality of life.13 A recent qualitative investigation has highlighted the inadequate provision of clear and consistent information to patients with SLE at the time of diagnosis, leading to further distress and confusion among this population.14 Hence, it is critical to improve patient education regarding SLE and biologic therapy, particularly with regard to the potential adverse effects of these therapies. Moreover, this study found that SLE patients who spent 30,000–50,000 CNY on treatment and those who had more complications exhibited higher knowledge scores. It is plausible that these patients have a greater disease burden and consequently have a greater inclination to seek information about SLE and its associated treatments compared to those who spent less and took fewer medications.15,16
In terms of attitude, patients receiving biological therapy were always found to have a high level of perceived necessity for medication but also a significant concern for potential adverse consequences.17 This anxiety may arise from the insecurity and distrust that stems from inadequate knowledge of systemic autoimmune diseases and their responses to symptoms.18 Therefore, it is crucial to address such concerns by providing comprehensive information and addressing related problems, including the financial burden of biologic therapy and its potential side effects. Moreover, in the precious study, 66.9% of the SLE patients thought that it leads to anxiety about reproductive issues caused by the SLE. Notably, a recent investigation focusing on the childbearing decisions of Korean women diagnosed with SLE revealed a higher prevalence of opting not to have children compared to healthy individuals, primarily attributed to health-related apprehensions.19 Similarly, a study conducted in South Africa examining fertility, pregnancy, and sexuality among women with SLE reported participants expressing a sense of entitlement deprivation, one participant in her twenties shared that upon evaluating her condition, she realized her self-care limitations also meant an inability to care for children. This realization led to significant distress.20 These findings collectively emphasize the significance of acknowledging the influence of SLE on fertility pressures and the subsequent adverse psychological impact experienced by women of reproductive age. Such considerations should not be underestimated.
Several studies suggested encouraging SLE patients to better understand their condition and treatment options can help facilitate shared decision-making.21–23 Moreover, most patients exhibited a preference for subcutaneous injections of biologic therapy in this study. Therefore, physicians should initiate a discussion with patients regarding medication administration preferences during the treatment plan discussion to ensure that the patient is comfortable with the injection method. In cases where patients express discomfort with self-injection.24 The implementation of a shared decision-making model has the potential to facilitate greater patient engagement and proactive involvement in the management of disease.
Last but not least, this study demonstrated that biologic therapy imposed a financial burden on around half of the SLE patients, and many of them did not receive the treatment as a consequence. This finding echoes the previous study on the financial costs of biologic therapy.25 Including biologic therapy in national health insurance coverage would greatly ease the financial burden on SLE patients with their families.
This study has several limitations. Firstly, this study was conducted in a single province in China, and the results might not be generalized to the whole country. Secondly, a positive correlation was observed between attitude and practice in the previous study, while the path coefficient did not reach statistical significance. This outcome was likely attributed to the impact of a relatively small sample size on the results of the path analysis adopted in this study.
However, the study remains clinically relevant as it examines the KAP of SLE patients towards the disease and its biologic therapy. The investigation of this study can assist in recognizing deficiencies in patient knowledge, attitudes, and practices, thus enabling health-care providers to enhance the quality of care rendered to SLE patients by utilizing these insights. Future research may delve deeper into the relationship between KAP scores and the prognosis of SLE patients. For example, this will involve employing regression analysis to adjust for variables such as age, gender, and treatment modalities, elucidating the correlation between KAP scores and patient-reported outcomes, such as quality of life.
Conclusions
Patients with SLE exhibited insufficient knowledge, moderate attitudes, and inactive practices toward disease management and biologic therapy. There is a pressing need for the development and implementation of educational programs and interventions aimed at enhancing their comprehension and behaviors related to SLE management.
Abbreviations
KAP, Knowledge, attitudes, and practices; SLE, Systemic lupus erythematosus; CSTAR, Chinese SLE Treatment and Research group; ACR, American College of Rheumatology; SLICC, Systemic Lupus International Collaborating Clinics; EULAR, European League Against Rheumatism.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics Approval and Consent to Participate
This study was approved by the Medical Ethics Committee of Union Hospital Affiliated to Tongji Medical College, Huazhong University of Science and Technology ([2023]NO.0133-01), and written informed consent was obtained from the SLE patients. I confirm that all methods were performed in accordance with the relevant guidelines. All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval for the version to be published, and agree to be accountable for all aspects of the work.
Funding
This work was supported by National Natural Science Foundation of China [81900497].
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Zhang SQ, Han JW, Sun LD, et al. A single-nucleotide polymorphism of the TNFSF4 gene is associated with systemic lupus erythematosus in Chinese Han population. Rheumatol Int. 2011;31(2):227–231. doi:10.1007/s00296-009-1247-2
2. Zhang Y, Yang J, Zhang J, et al. Genome-wide search followed by replication reveals genetic interaction of CD80 and ALOX5AP associated with systemic lupus erythematosus in Asian populations. Ann Rheum Dis. 2016;75(5):891–898. doi:10.1136/annrheumdis-2014-206367
3. Harvey PR, Gordon C. B-cell targeted therapies in systemic lupus erythematosus: successes and challenges. BioDrugs. 2013;27(2):85–95. doi:10.1007/s40259-013-0015-8
4. Mok CC, Cheung MY, Ho LY, Yu KL, To CH. Risk and predictors of work disability in Chinese patients with systemic lupus erythematosus. Lupus. 2008;17(12):1103–1107. doi:10.1177/0961203308094280
5. Maheswaranathan M, Eudy AM, Barr AC, et al. Association of health literacy and numeracy with lupus knowledge and the creation of the lupus knowledge assessment test. J Rheumatol. 2022;49(6):585–591. doi:10.3899/jrheum.210708
6. Katz P, Dall’Era M, Trupin L, et al. Impact of limited health literacy on patient-reported outcomes in systemic lupus erythematosus. Arthritis Care Res. 2021;73(1):110–119. doi:10.1002/acr.24361
7. Aldhamy H, Maniatopoulos G, McCune VL, Mansi I, Althaqafy M, Pearce MS. Knowledge, attitude and practice of infection prevention and control precautions among laboratory staff: a mixed-methods systematic review. Antimicrob Resist Infect Control. 2023;12(1):57. doi:10.1186/s13756-023-01257-5
8. Tahani B, Manesh SS. Knowledge, attitude and practice of dentists toward providing care to the geriatric patients. BMC Geriatr. 2021;21(1):399. doi:10.1186/s12877-021-02343-2
9. Grisaru-Tal S, Itan M, Klion AD, Munitz A. A new Dawn for eosinophils in the tumour microenvironment. Nat Rev Cancer. 2020;20(10):594–607. doi:10.1038/s41568-020-0283-9
10. Gomez A, Parodis I. Do biological agents improve health-related quality of life in patients with systemic lupus erythematosus? Results from a systematic search of the literature. Autoimmun Rev. 2022;21(11):103188. doi:10.1016/j.autrev.2022.103188
11. Zeng X, Chen Y. 2020 Chinese guidelines for the diagnosis and treatment of systemic lupus erythematosus. Chin J Intern Med. 2020;1(3):172–185.
12. Monte TCS, Mateo PF, Izquierdo MG, et al. An online survey of the Spanish Lupus Patient Association (FELUPUS): patient perceptions and experiences. Clin Rheumatol. 2023;42(5):1259–1265. doi:10.1007/s10067-023-06500-3
13. Sahebalzamani M, Farahani H, Jamarani MT, Faezi ST, Moradi K, Paragomi P. Effects of a continuous care model on patients’ knowledge and health-related quality of life in systemic lupus erythematosus. Rehabil Nurs. 2017;42(6):E9–E18. doi:10.1002/rnj.283
14. Waldron N, Brown S, Hewlett S, Elliott B, McHugh N, McCabe C. ‘It’s more scary not to know’: a qualitative study exploring the information needs of patients with systemic lupus erythematosus at the time of diagnosis. Musculoskeletal Care. 2011;9(4):228–238. doi:10.1002/msc.221
15. Scalzi LV, Ballou SP, Park JY, Redline S, Kirchner HL. Cardiovascular disease risk awareness in systemic lupus erythematosus patients. Arthritis Rheum. 2008;58(5):1458–1464. doi:10.1002/art.23419
16. Bin Haikel KA, Al Tulaihi B. Awareness of systemic lupus erythematosus among primary health care patients in Riyadh, Saudi Arabia. Saudi Med J. 2019;40(2):177–182. doi:10.15537/smj.2019.2.23920
17. Barton JL. Patient preferences and satisfaction in the treatment of rheumatoid arthritis with biologic therapy. Patient Prefer Adherence. 2009;3:335–344. doi:10.2147/ppa.s5835
18. Sloan M, Naughton F, Harwood R, et al. Is it me? The impact of patient-physician interactions on lupus patients’ psychological well-being, cognition and health-care-seeking behaviour. Rheumatol Adv Pract. 2020;4(2):rkaa037. doi:10.1093/rap/rkaa037
19. Kim IJ, Kim HA, Suh CH, et al. Impact of childbearing decisions on family size of Korean women with systemic lupus erythematosus. J Korean Med Sci. 2016;31(5):729–734. doi:10.3346/jkms.2016.31.5.729
20. Phuti A, Hodkinson B, Tikly M, Schneider M. “The feeling of not being entitled to something”: fertility, pregnancy, and sexuality among women with systemic lupus erythematosus in South Africa. Scand J Rheumatol. 2020;49(3):214–220. doi:10.1080/03009742.2019.1657492
21. Ilchmann-Diounou H, Menard S. Psychological stress, intestinal barrier dysfunctions, and autoimmune disorders: an overview. Front Immunol. 2020;11:1823. doi:10.3389/fimmu.2020.01823
22. Moraleda V, Prados G, Martinez MP, Sanchez AI, Sabio JM, Miro E. Sleep quality, clinical and psychological manifestations in women with systemic lupus erythematosus. Int J Rheum Dis. 2017;20(10):1541–1550. doi:10.1111/1756-185X.13081
23. Shen B, Tan W, Feng G, et al. The correlations of disease activity, socioeconomic status, quality of life, and depression/anxiety in Chinese patients with systemic lupus erythematosus. Clin Dev Immunol. 2013;2013:270878. doi:10.1155/2013/270878
24. Miyokawa R, Kivler C, Louie S, Godor D, Tan L, Kenyon N. Self-administered mepolizumab in the management of severe asthma: usability and patient acceptance. Patient Prefer Adherence. 2020;14:1669–1682. doi:10.2147/PPA.S227465
25. Ding Q, Shiltz D, Hossami D, Konieczny AM. The economic burden of biologic disease-modifying antirheumatic drugs in rheumatoid arthritis patients in the United States. Expert Rev Pharmacoecon Outcomes Res. 2022;22(8):1231–1241. doi:10.1080/14737167.2022.2117690
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge, Attitudes, and Practices Among Community Populations Toward Long COVID in China
He N, Tunala S, Wu R, Zhao C, Wuren T, Hushuud C
International Journal of General Medicine 2024, 17:4455-4463
Published Date: 1 October 2024
Knowledge, Attitudes, and Practices Regarding Swallowing Disorders Among General Practitioners
Zou M, Zhu X, Li J, Yu H, Guo P
International Journal of General Medicine 2025, 18:1555-1567
Published Date: 18 March 2025
Knowledge, Attitudes and Practices Toward Hypotension During Hemodialysis Among Nephrology and Hemodialysis Medical Staff: A Multi-Center Cross-Sectional Study
Cheng D, Xie L, Chu X, Bai Y, He T
Journal of Multidisciplinary Healthcare 2025, 18:5359-5369
Published Date: 28 August 2025
Knowledge, Attitudes, and Practices Toward Microvascular Decompression for Hemifacial Spasm Among Neurosurgeons: A Multicenter Cross-Sectional Study
Xu Y, Dong S, Zhao R, Liu J, Han P, Guo Y, Jiang R
Journal of Multidisciplinary Healthcare 2025, 18:8277-8291
Published Date: 27 December 2025
Knowledge, Attitudes, and Practices of Hypertensive Patients with Aortic Dissection and Aortic Aneurysm Towards Aortic Dissection and Its Prevention: A Mediation Analysis
Zhang Y, Zhang B, Wang L, Yuan J
International Journal of General Medicine 2026, 19:609862
Published Date: 22 June 2026