Back to Journals » Patient Preference and Adherence » Volume 20
Knowledge, Attitudes, and Practices Regarding Stroke Among Young Stroke Patients in China: A Cross-Sectional Survey
Authors Li G, Wang Z, Wang T, Cui Y, Li H, Wang W, Li J
Received 7 April 2026
Accepted for publication 10 June 2026
Published 18 June 2026 Volume 2026:20 615143
DOI https://doi.org/10.2147/PPA.S615143
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Guangling Li,1 Zhijun Wang,1 Tianzhi Wang,1 Yafang Cui,1 Haihong Li,1 Wenting Wang,2 Jieting Li1
1Department of Neurology, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Third Hospital of Shanxi Medical University, Tongji Shanxi Hospital, Taiyuan, Shanxi, People’s Republic of China; 2Department of Neurology, First People’s Hospital of Jinzhong City, Jinzhong, Shanxi, People’s Republic of China
Correspondence: Jieting Li, Department of Neurology, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Third Hospital of Shanxi Medical University, Tongji Shanxi Hospital, No. 99, Longcheng Street, Xiaodian District, Taiyuan, Shanxi, 030032, People’s Republic of China, Tel +86-13935146195, Email [email protected]
Background: Stroke remains a leading cause of death and disability, with rising incidence in young adults. This study evaluates the Knowledge, Attitudes, and Practices (KAP) regarding stroke among young stroke patients aged 18– 45 years.
Methods: A cross-sectional online survey was conducted from January 15 to June 5, 2025, in Shanxi Province, China. Data from 445 young stroke patients were analyzed. Structural equation modeling (SEM) was employed to explore the relationships among KAP domains.
Results: The average KAP scores were 23.69± 8.48, 43.71± 4.84, and 40.32± 5.68, respectively. SEM analysis revealed that knowledge directly influenced both attitudes (β=0.519, P=0.011) and practices (β=0.494, P=0.005). Furthermore, knowledge had a significant indirect effect on practices through attitudes (β=0.218, P=0.006). SEM analysis revealed that knowledge directly influenced both attitudes and practices, while attitudes partially mediated the relationship between knowledge and practice.
Conclusion: Young stroke patients demonstrated positive attitudes and moderate practices but had insufficient knowledge. This knowledge-practice gap underscores the urgent need for targeted educational interventions, such as digital health tools and community workshops, to improve secondary stroke prevention.
Keywords: stroke, young adult, health knowledge, attitude, practice, cross-sectional studies
Background
Stroke remains the second leading cause of death globally and the third leading cause of death and disability, with an increase in absolute number of incident strokes by 70%, prevalent strokes by 85%, deaths from stroke by 43%, and disability adjusted life-years (DALYs) by 32% over the last two decades (1990–2019).1 Traditionally considered a “disease of the elderly,” stroke is increasingly affecting younger populations, with incidence rates among adults under 44 years increasing from 5–17 per 100,000 person-years in the 1990s to 11–28 per 100,000 in more recent estimates.2–4 Young stroke accounts for 10–15% of total stroke patients, representing a significant public health challenge as these premature strokes have a disproportionate societal burden, curtailing productive years of life and predisposing younger adults to longer-term sequelae and complications.5,6 Consistent with widely adopted clinical and epidemiological definitions, young stroke in the present study was defined as stroke occurring between 18 and 45 years of age.7
The knowledge, attitude, and practice (KAP) model postulates that individual health behaviors are contingent upon one’s knowledge and attitudes, serving as a fundamental framework for understanding health-related decision-making processes.8 Unlike stroke in older adults, the etiological spectrum of stroke in young adults is highly heterogeneous, with cryptogenic strokes accounting for 24–53% of cases, followed by cardio-embolism (10–34%), large artery atherosclerosis (4–29%), and small vessel disease (12–26%).4,9,10 Given that young stroke patients face decades of potential recurrence risk—with 5-year risk of any recurrent vascular event reaching 12.2%—understanding their disease-related knowledge and health behaviors becomes crucial for effective secondary prevention.11
Despite the recognized importance of patient education and self-management in stroke prevention, limited research has systematically examined the KAP of young stroke patients regarding their own disease, particularly in the Chinese population. Previous studies in China have shown that overall stroke awareness and health literacy remain insufficient, especially regarding symptom recognition and risk factor identification among adults and community residents.12 In addition, disparities in health education accessibility between urban and rural populations may further influence patient understanding and self-management behaviors.13,14 However, most existing studies have focused on the general population or caregivers rather than young stroke survivors themselves. In contrast, young stroke patients represent a distinct clinical group with a prolonged risk window for recurrence and long-term disability, making their disease-related KAP particularly critical for effective secondary prevention. Shanxi Province was chosen as the research site due to its high prevalence of cardiovascular risk factors among young adults, including high rates of smoking, alcohol consumption, and rural-urban healthcare disparities, which may uniquely influence stroke risk profiles and health behaviors in this demographic.15 Specifically, Shanxi Province has been reported to have higher-than-national-average rates of major cardiovascular risk factors, including smoking prevalence, alcohol consumption, and metabolic risk profiles such as hypertension and obesity, particularly among younger adults. These indicators exceed national estimates reported in large-scale epidemiological surveys in China, thereby underscoring the increased regional burden of cardiovascular disease and the importance of targeted prevention strategies in this population. While global studies have identified substantial ethnic and regional differences in risk factors and outcomes, with patients in low and middle-income countries having almost 2.5-fold higher risk for mortality than those in high-income countries.16 Although some research has examined stroke-related knowledge, attitudes, and practices (KAP) in the general population or among caregivers, studies specifically focusing on young stroke patients themselves are scarce. Existing work has largely centered on elderly patients or caregiver knowledge, rather than the self-perceptions of young survivors. The present study addresses this gap by shifting the focus to young adults who have experienced a stroke, a group for whom KAP is critical for long-term secondary prevention. This study aims to quantify KAP levels, identify their interrelationships, and explore factors influencing the translation of knowledge into practice in this underexplored population. Structural equation modeling (SEM) was employed because it enables simultaneous evaluation of direct and indirect pathways among latent behavioral constructs, making it particularly suitable for examining the complex interrelationships within the KAP framework.17
Materials and Methods
Study Design and Participants
This cross-sectional study was conducted between January 15 and June 5, 2025, in Shanxi Province, China. The target population comprised young adults aged 18 to 45 years who had been diagnosed with stroke and were receiving medical care at hospitals within the province. Ethical approval was granted by the Medical Ethics Committee of our Hospital, and informed consent was obtained from all participants prior to enrollment.
Participants were eligible for inclusion if they met the following criteria: aged between 18 and 45 years, clinically diagnosed with stroke, clinically stable at the time of recruitment, and attending follow-up appointments at least one month post-discharge. A convenience sampling technique was employed to recruit eligible young stroke patients attending follow-up clinics across participating hospitals in Shanxi Province. Individuals were excluded if they had cognitive impairments that interfered with their ability to comprehend and complete the questionnaire (such as intellectual disability or dementia), a history of severe psychiatric disorders (including major depressive disorder or schizophrenia), coexisting serious medical conditions (such as malignant tumors or end-stage renal disease), or if they failed to provide complete responses to key survey items. Duplicate submissions were restricted using mobile phone number, WeChat account, IP address, and backend submission records. Questionnaires with abnormal values, such as implausible age entries of 150 or 180 years, were excluded. A trap question, “15 × 2 = 40,” was included to assess response attentiveness; questionnaires selecting “correct” for this item were excluded. Initially, a total of 519 questionnaires were collected. After excluding 19 questionnaires from individuals who did not consent to participate, 8 from individuals outside the 18–45 age range, 41 with abnormal values, and 6 with incorrect answers to trap questions, 445 valid questionnaires remained, resulting in a valid response rate of 85.74%.
Questionnaire
The questionnaire was designed with reference to the 2023 edition of the National Clinical Guideline for Stroke by the United Kingdom.18 Following its initial formulation, the instrument underwent expert review and iterative revision based on feedback from five clinical specialists across neurology, psychiatry, and gastroenterology. A pilot test was subsequently conducted among 43 individuals to assess the instrument’s reliability. The resulting Cronbach’s alpha coefficient was 0.887, reflecting a high level of internal consistency. The Kaiser–Meyer–Olkin (KMO) measure was 0.912 (p < 0.001), indicating sampling adequacy. Model fit indices demonstrated acceptable fit (Chi-square Minimum/Degrees of Freedom ratio (CMIN/DF) = 4.345, Root Mean Square Error of Approximation (RMSEA) = 0.071, Incremental Fit Index (IFI) = 0.895, Tucker–Lewis Index (TLI) = 0.901, and Comparative Fit Index (CFI) = 0.901), confirming convergent validity (Figure S1 and Tables S1–S3). After the pilot test, participants were asked about their subjective experience in completing the questionnaire. None reported that the items were difficult to understand or confusing. As the questionnaire also showed good internal consistency, no further item modification was made after the pilot test.
The finalized questionnaire consisted of four sections: demographic characteristics, KAP. The knowledge section contained 11 questions, with a total of 24 items. The first question was scored as 2 points for “Yes” and 0 points for “No”. For the remaining questions, responses of “very familiar,” “heard of,” and “not clear” were assigned 2, 1, and 0 points, respectively, allowing for a total score ranging from 0 to 48. The attitude section also included 11 items, evaluated using a five-point Likert scale from “strongly agree” (5 points) to “strongly disagree” (1 point), resulting in a total score between 11 and 55. The practice section focused on five questions, with questions 1, 2, and 5 included in the scoring. These items utilized a five-point Likert scale, where responses ranged from “always” to “never,” scored from 5 to 1, respectively. P5 further evaluated six rehabilitation-related behaviors. Specifically, sub-items P5.1 through P5.4 applied only to participants currently undergoing stroke rehabilitation. In contrast, P5.5 and P5.6 focused on dietary management and follow-up behaviors relevant to all respondents. Therefore, only P5.5 and P5.6 received assigned values. The overall score range for the practice dimension was also 11 to 55. Consistent with common practice in KAP studies,19 a score exceeding 70% of the maximum possible in any given domain was considered indicative of sufficient knowledge, a favorable attitude, or active engagement in stroke-related health behaviors.
Questionnaire Distribution and Quality Control
A dedicated research team was formed, consisting of clinical nursing professionals with over a decade of experience in patient care and clinical research. Before data collection began, all team members participated in standardized training that covered the questionnaire’s content and administration protocol. This training focused on the study’s objectives, inclusion and exclusion criteria, and methods to ensure methodological consistency and data reliability. Participants were recruited from neurology inpatient wards and outpatient follow-up clinics of the participating hospitals. Potentially eligible patients were identified from discharge records and outpatient follow-up lists, and all consecutively eligible patients were contacted by designated members of the research team during the study period. Data collection involved follow-up telephone interviews with eligible participants who had been discharged from the hospital for at least one month. Trained researchers adhered to a standardized script to introduce the study, explain its significance, and provide clear instructions for completing the questionnaire. After obtaining informed consent, participants were invited to join a designated WeChat contact to access the electronic version of the questionnaire. For respondents who could not complete the survey independently, researchers read each question aloud and recorded the responses accordingly. Throughout this process, care was taken to avoid leading or suggestive language. All interviews were conducted individually to preserve the integrity of the responses and minimize potential bias, thereby enhancing the validity of the collected data.
Statistical Analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS) version 27.0 (IBM Corp., Armonk, NY, USA) and Analysis of Moment Structures (AMOS) version 26.0 (IBM Corp., Armonk, NY, USA). Continuous variables are presented as means with standard deviations (SD), while categorical variables are expressed as frequencies and percentages (n, %). The normality of continuous variables was assessed prior to comparison. For normally distributed variables, independent sample t-tests were used for comparisons between two groups, and analysis of variance (ANOVA) was applied for comparisons among three or more groups. For variables that did not follow a normal distribution, the Wilcoxon–Mann–Whitney test was used for two-group comparisons, and the Kruskal–Wallis test was used for comparisons involving multiple groups. Correlation analysis was conducted using either Pearson’s correlation coefficient for normally distributed data or Spearman’s rank correlation coefficient for non-normally distributed data. To further examine the interrelationships among knowledge, attitude, and practice (KAP), SEM was employed. The SEM framework was constructed to test the following hypothesized pathways: (1) knowledge directly influences attitude; (2) attitude directly influences practice; and (3) knowledge influences practice both directly and indirectly through attitude. Model fit was evaluated using multiple indices, including the root mean square error of approximation (RMSEA), incremental fit index (IFI), Tucker–Lewis index (TLI), and comparative fit index (CFI). The adequacy of the sample size was also examined to ensure robustness of the SEM analysis. According to the commonly accepted guideline that the sample size should be at least 5–10 times the number of observed variables, consistent with recommendations from previous methodological studies.20 Given that the model contained 46 observed variables, a minimum of 230–460 participants would be required. The final sample of 445 met this criterion, supporting the sufficiency of the sample size for SEM. All statistical analyses were two-tailed, and a P-value less than 0.05 was considered to indicate statistical significance.
Results
Demographic Characteristics and KAP Scores
A total of 445 young stroke patients were included, with a mean age of 37.67 ± 6.68 years. Most participants were male (66.29%), married (79.10%), and 43.60% held a bachelor’s degree or higher. Nearly half had never smoked (49.44%) or consumed alcohol (37.98%), while 45.62% occasionally stayed up late. In response to stroke symptoms, panic levels varied, with most reporting moderate panic (Figure 1). The KAP scores were 23.69 ± 8.48 for knowledge, 43.71 ± 4.84 for attitude, and 40.32 ± 5.68 for practice. KAP scores were significantly associated with multiple sociodemographic and lifestyle factors including education, income, medical insurance, BMI, and health behaviors. Participants with dual medical insurance, higher socioeconomic status, and healthier habits had more favorable KAP scores. Notably, females showed significantly higher practice scores than males (P<0.05) (Table S4).
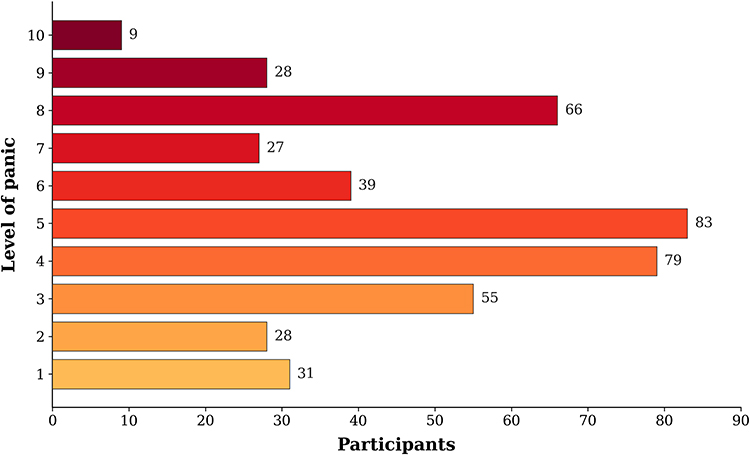 |
Figure 1 Level of Panic When Experiencing Symptoms (1–10 points, with 1 indicating no panic and 10 indicating extreme panic). |
KAP
In the Knowledge domain, young stroke patients demonstrated critical gaps. Over 65% were unaware of the stroke risk linked to obstructive sleep apnea, 59% lacked knowledge of hyperhomocysteinemia, and 64% did not recognize gender as a relevant factor. Only 6.97% knew psychological counseling is relevant for secondary prevention. Symptom recognition was poor: merely 14.38% could identify the BE FAST components, and only 20.45% understood transient ischemic attacks require urgent care. Furthermore, just 18.88% knew professional rehabilitation should continue in the post-acute recovery phase.
In the Attitude dimension, misconceptions were notable A large majority (87.19%) believed stroke primarily affects older adults, underestimating personal risk. Furthermore, 56.4% held neutral or negative views on the preventive importance of quitting smoking and limiting alcohol. In the Practice dimension, engagement was suboptimal. Only 41.57% were undergoing rehabilitation. Among them, participation in specific therapies was low, with only 13.49% in cognitive and 17.31% in speech rehabilitation. Physical activity was inconsistent, as 51.01% never practiced Tai Chi and 25.84% never jogged. (Table S5).
Correlation Analysis
Correlation analysis showed that there were significant positive correlations between knowledge and attitude (r = 0.396, P < 0.001) as well as practice (r = 0.559, P < 0.001). Also, there was a correlation between attitude and practice (r = 0.339, P < 0.001) (Table 1).
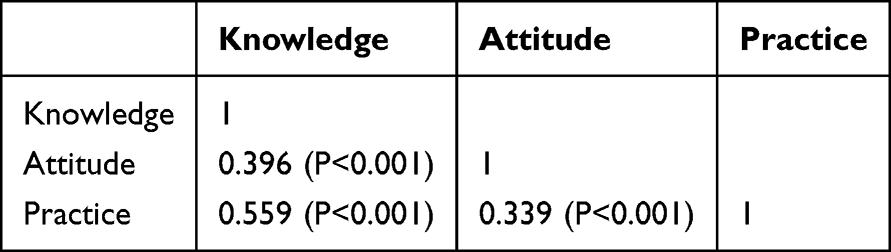 |
Table 1 KAP Correlation Analysis |
SEM Analysis
The SEM demonstrate an acceptable overall model fit (CMIN/DF value: 4.620, RMSEA value: 0.078, IFI value: 0.832, TLI value: 0.808, and CFI value: 0.830), which falls within the range considered adequate in comparable behavioral and psychological models.21,22 Although the CFI and TLI values are slightly below the conventional 0.90 threshold, they are still regarded as acceptable when factor loadings exceed 0.80 and model parsimony is prioritized. Therefore, the model was considered reasonably well-fitting for examining the hypothesized pathways (Table 2). The results of mediation effect analysis showed that knowledge had direct effects on attitude (β = 0.519, P = 0.011) and practice (β = 0.494, P = 0.005). Meanwhile, attitude had a direct impact on practice (β = 0.421, P = 0.016). Furthermore, knowledge indirectly affected practice through attitude (β = 0.218, P = 0.006) (Table 3 and Figure 2).
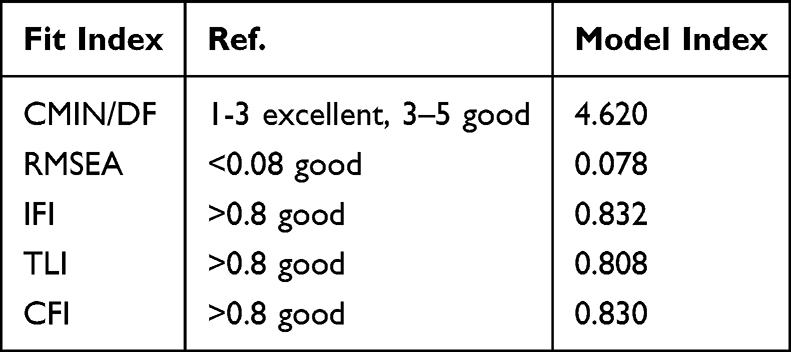 |
Table 2 Structural Equation Model Fit Indices |
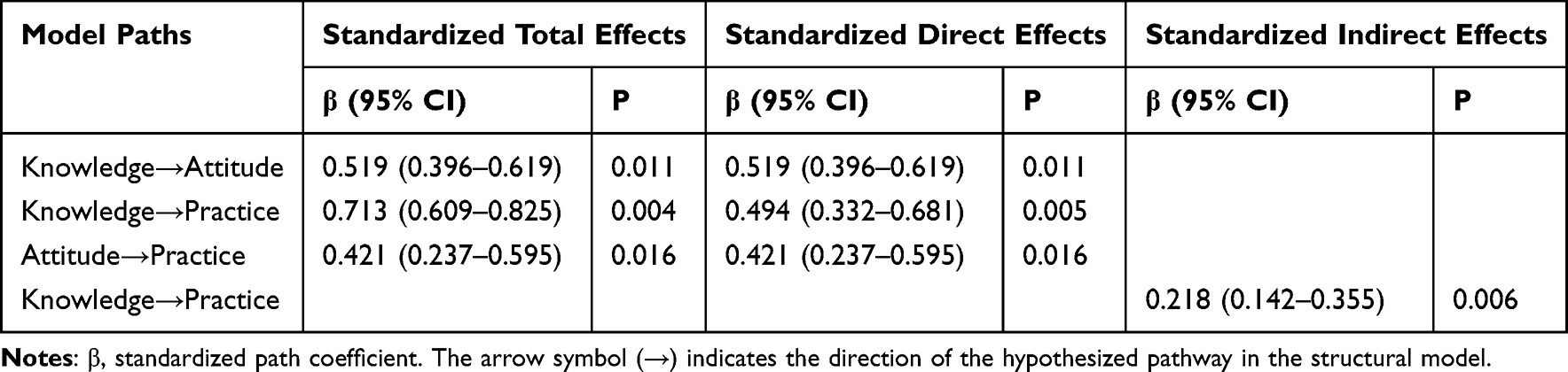 |
Table 3 Mediation Effects in the Structural Model Verified by the Bootstrap Method |
 |
Figure 2 The relationship between knowledge, attitude and practice using structural equation model. |
Discussion
A key finding is the mismatch between low stroke-related knowledge and the relatively positive attitudes and practices among young survivors. This paradox, directly relevant to secondary prevention, suggests that beneficial behaviors may be unsustainable without a deeper understanding of the disease. The discrepancy may stem from contextual factors. In China, family-centered and collectivist norms encourage adherence to health advice from physicians or family, even with limited personal knowledge. Social desirability may also lead to overreporting of positive behaviors. Furthermore, structured discharge education and community health programs in the region may promote proactive practices independently of knowledge levels. Future qualitative research is needed to explore these psychosocial and systemic determinants. Overall, the findings highlight the urgent need for targeted educational interventions to enhance foundational knowledge, thereby reinforcing and sustaining positive long-term health behaviors in this high-risk group.
The findings of this study highlight a consistent yet complex pattern in the cognitive and behavioral profiles of young individuals with a history of stroke. The SEM demonstrated that knowledge exerted a strong direct effect on both attitudes and practices, with an additional indirect path to practice mediated through attitudes. This layered relationship affirms that while cognitive awareness can shape behavioral outcomes, its influence is also contingent upon the affective stance individuals hold toward stroke prevention. Such mechanisms suggest that simply disseminating information may be insufficient unless accompanied by interventions that also foster emotional engagement and belief in the value of preventive action.8,23
The strength of the knowledge-practice link was further supported by the observed positive correlations among all three KAP domains. In particular, the strong association between knowledge and practice underscores the role of informational access and comprehension in enabling proactive health behaviors. This finding aligns with previous work in chronic disease management, which has similarly noted that individuals who possess greater disease-specific knowledge tend to engage more consistently in health-preserving practices.23,24 However, the observed knowledge deficits in key areas such as symptom recognition, risk factor awareness, and rehabilitation measures indicate a disconnect between general health attitudes and specific content retention. Many participants were unable to identify transient ischemic attack symptoms or distinguish preventable from non-preventable risk factors, revealing gaps that may undermine timely and effective responses to stroke events.
The SEM pathway between attitude and practice, though somewhat weaker than the direct influence of knowledge, remained statistically significant and meaningful. The attitudinal dimension likely reflects a more motivational substrate that reinforces or inhibits the translation of knowledge into behavior. This is especially relevant in a younger population who may not yet perceive themselves at imminent risk and thus require additional motivational cues to act on their knowledge. Related research in cardiovascular risk perception supports the idea that behavioral activation is often contingent upon both self-relevance and perceived severity, particularly in younger cohorts.25,26
Sociodemographic variation in KAP outcomes offers further insight into modifiable disparities. Urban residents, individuals with higher educational attainment, and those with commercial medical insurance generally displayed better knowledge scores and more consistent engagement in preventive practices. These findings are consistent with prior studies linking healthcare literacy and resource access with improved chronic disease outcomes.27,28 In contrast, rural residency, lower income, and limited insurance coverage appeared to correlate with both cognitive and behavioral vulnerability, indicating a need for targeted outreach in these groups. It is noteworthy that even among participants receiving care at tertiary hospitals, a substantial proportion remained uninformed about essential aspects of stroke management, suggesting that clinical encounters may not always suffice as educational interventions.
The bar chart illustrating panic levels upon symptom onset revealed an interesting psychological profile: the highest concentration of responses clustered around moderate panic levels, with a noticeable drop-off at both extremes. This distribution may reflect partial symptom awareness coupled with uncertainty about appropriate action, rather than complete ignorance or overconfidence. It highlights a latent tension between knowledge and perceived control, which may shape whether individuals respond promptly or hesitate during acute episodes. Addressing this tension requires more than factual correction; it demands confidence-building measures that enhance self-efficacy in symptom interpretation and response.29,30
Although overall attitudes toward stroke prevention were generally positive, a closer inspection of practice patterns revealed several inconsistencies. While lifestyle modifications such as dietary improvement and smoking cessation were relatively common, rehabilitation practices were notably underutilized. Participation in structured physical therapy, occupational training, and speech therapy remained low, even among those actively recovering. Similar patterns have been reported in Chinese stroke populations, where post-stroke rehabilitation utilization remains suboptimal due to financial burden, limited accessibility of rehabilitation facilities, and insufficient patient awareness regarding the long-term benefits of rehabilitation, particularly outside tertiary urban centers.31 National and regional studies from China have shown that high out-of-pocket costs, uneven distribution of rehabilitation resources between urban and rural areas, and inadequate rehabilitation education after hospital discharge are major barriers to sustained rehabilitation engagement among stroke survivors.32 The underutilization of rehabilitation services observed in this study may stem from multiple factors. First, economic burden remains a critical barrier, as post-stroke rehabilitation often involves out-of-pocket expenses not fully covered by insurance, particularly for younger patients who are less likely to qualify for long-term disability benefits. Second, disparities in the availability of specialized rehabilitation facilities, especially in less urbanized areas of Shanxi Province, limit accessibility. Third, inadequate awareness of the importance of ongoing rehabilitation and misconceptions that functional recovery plateaus shortly after discharge may discourage sustained engagement. Together, these findings suggest that the low utilization of rehabilitation services among young stroke patients reflects a combination of structural constraints and insufficient rehabilitation awareness, underscoring the need for integrated policy, educational, and service-delivery interventions. To further support the generalizability of the present findings, evidence from large-scale epidemiological studies in China has consistently demonstrated a clear north–south gradient in cardiovascular risk profiles. A nationally representative study reported significantly higher prevalence of hypertension in northern China compared with southern regions, along with higher levels of key behavioral risk factors such as smoking and elevated blood pressure.33 These geographic differences have been observed across multiple population-based surveys and are considered a stable feature of cardiovascular epidemiology in China. More recent analyses based on large-scale national datasets further confirmed substantial regional variation in clustered cardiovascular risk factors, with northern provinces showing a relatively higher burden of hypertension and related behavioral risks.34 These findings suggest that the risk environment in Shanxi Province is representative of a broader northern China pattern, thereby supporting the applicability of the present results to other similar high-risk populations. The underuse of these services may reflect barriers beyond knowledge or belief, such as logistical constraints, financial limitations, or misperceptions about the utility of rehabilitative care. Other work in neurological rehabilitation contexts suggests that uptake is often sensitive to both social support and the clarity of professional guidance provided during discharge planning.28,35
Several recommendations arise from these findings. Educational strategies must go beyond the mere provision of information, emphasizing tailored messaging that considers the emotional and contextual realities of younger stroke survivors. Interactive formats, community-based peer engagement, and digital platforms could help increase accessibility and resonance. Additionally, integrating rehabilitation guidance into standard care transitions may help mitigate the observed practice gaps, particularly if accompanied by follow-up support. Policy initiatives aimed at expanding insurance coverage and enhancing service availability in rural areas could further reduce structural inequities that constrain knowledge acquisition and behavioral compliance.36,37
This study has several limitations. First, its cross-sectional design precludes the establishment of causal relationships between KAP. Second, the use of an online self-reported questionnaire may have introduced response bias, particularly in the assessment of lifestyle behaviors and rehabilitation practices. Third, as the study was conducted in a single province with a specific age group and healthcare setting, the generalizability of the findings to other regions or populations may be limited. Because all participants were recruited from hospitals within Shanxi Province, the findings may reflect regional characteristics in stroke awareness and health-seeking behavior. Differences in socioeconomic context, healthcare access, and health education across provinces could introduce regional bias, further limiting external validity. Additionally, selection bias may have occurred, as individuals more engaged in follow-up care were more likely to participate. Although the questionnaire demonstrated high internal consistency, further validation across broader populations and longitudinal settings is needed to ensure measurement reliability. Moreover, due to regional socioeconomic and healthcare disparities, findings may not be fully representative of all young stroke patients in China.
Conclusions
In conclusion, young patients with a history of stroke demonstrated insufficient disease-related knowledge despite exhibiting generally positive attitudes and relatively proactive health practices, with knowledge significantly influencing both attitudes and behaviors through direct and indirect pathways relevant to secondary prevention. These findings highlight the need for targeted educational interventions to enhance disease-specific knowledge, which may further strengthen attitudes and translate into sustained improvements in stroke-related self-management among young patients.
Abbreviations
KAP, Knowledge, Attitudes, and Practices; SEM, Structural Equation Modeling; DALYs, Disability-Adjusted Life Years; TIA, Transient Ischemic Attack; BE FAST, Balance, Eyes, Face, Arm, Speech, Time.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
The study was approved by the Medical Ethics Committee of Shanxi Bethune Hospital (Approval No: YXLL-2025-014). All participants were informed about the study protocol and provided written informed consent to participate in the study. I confirm that all methods were performed in accordance with the relevant guidelines. All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported by Special Project of Science and Technology Strategy Research of Shanxi Province (project number: 202404030401171).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Feigin VL, Stark BA, Johnson CO. Global. regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021;20(10):795–10. doi:10.1016/S1474-4422(21)00252-0
2. Boot E, Ekker MS, Putaala J, Kittner S, De Leeuw FE, Tuladhar AM. Ischaemic stroke in young adults: a global perspective. J Neurol Neurosurg Psychiatry. 2020;91(4):411–417. doi:10.1136/jnnp-2019-322424
3. Madsen TE, Khoury JC, Leppert M, et al. Temporal trends in stroke incidence over time by sex and age in the GCNKSS. Stroke. 2020;51(4):1070–1076. doi:10.1161/STROKEAHA.120.028910
4. Smajlović D. Strokes in young adults: epidemiology and prevention. Vasc Health Risk Manag. 2015;11:157–164. doi:10.2147/VHRM.S53203
5. Maaijwee NA, Rutten-Jacobs LC, Schaapsmeerders P, Van Dijk EJ, de Leeuw FE. Ischaemic stroke in young adults: risk factors and long-term consequences. Nat Rev Neurol. 2014;10(6):315–325. doi:10.1038/nrneurol.2014.72
6. Putaala J, Yesilot N, Waje-Andreassen U, et al. Demographic and geographic vascular risk factor differences in European young adults with ischemic stroke: the 15 cities young stroke study. Stroke. 2012;43(10):2624–2630. doi:10.1161/STROKEAHA.112.662866
7. Ekker MS, Boot EM, Singhal AB, et al. Epidemiology, aetiology, and management of ischaemic stroke in young adults. Lancet Neurol. 2018;17(9):790–801. doi:10.1016/S1474-4422(18)30233-3
8. Li D, Guo H, Sun Y, Zhang Z, Liu H. Knowledge, attitude, and practice of stroke patients’ family members towards stroke rehabilitation: a cross-sectional study. J Stroke Cerebrovascular Dis. 2025;34(2):108177. doi:10.1016/j.jstrokecerebrovasdis.2024.108177
9. Van Alebeek ME, Arntz RM, Ekker MS, et al. Risk factors and mechanisms of stroke in young adults: the FUTURE study. J Cereb Blood Flow Metab. 2018;38(9):1631–1641. doi:10.1177/0271678X17707138
10. Yahya T, Jilani MH, Khan SU, et al. Stroke in young adults: current trends, opportunities for prevention and pathways forward. Am J Prev Cardiol. 2020;3:100085. doi:10.1016/j.ajpc.2020.100085
11. Verburgt E, Hilkens NA, Ekker MS, et al. Short-Term and long-term risk of recurrent vascular event by cause after ischemic stroke in young adults. JAMA Network Open. 2024;7(2):e240054. doi:10.1001/jamanetworkopen.2024.0054
12. Luan S, Yang Y, Huang Y, McDowell M. Public knowledge of stroke and heart attack symptoms in China: a cross-sectional survey. BMJ Open. 2021;11(1):e043220. doi:10.1136/bmjopen-2020-043220
13. Zhang M, Shi Y, Zhou B, et al. Prevalence, awareness, treatment, and control of hypertension in China, 2004-18: findings from six rounds of a national survey. BMJ. 2023;380:e071952. doi:10.1136/bmj-2022-071952
14. Tian X, Di Z, Cheng Y, et al. Study on the development of an infectious disease-specific health literacy scale in the Chinese population. BMJ Open. 2016;6(8):e012039. doi:10.1136/bmjopen-2016-012039
15. Li X, Wu C, Lu J, et al. Cardiovascular risk factors in China: a nationwide population-based cohort study. Lancet Public Health. 2020;5(12):e672–e681. doi:10.1016/S2468-2667(20)30191-2
16. Jacob MA, Ekker MS, Allach Y, et al. Global differences in risk factors, etiology, and outcome of ischemic stroke in young adults-a worldwide meta-analysis: the GOAL initiative. Neurology. 2022;98(6):e573–e588. doi:10.1212/WNL.0000000000013195
17. McDonald RP, Ho MH. Principles and practice in reporting structural equation analyses. Psychol Methods. 2002;7(1):64–82. doi:10.1037/1082-989X.7.1.64
18. Crow J, Smith A. National clinical guideline for stroke for the United Kingdom and ireland: Part I–an overview of the updated recommendations. Br J Occup Ther. 2023;86(10):661–664. doi:10.1177/03080226231188020
19. Lee F, Suryohusodo AA. Knowledge, attitude, and practice assessment toward COVID-19 among communities in East Nusa Tenggara, Indonesia: a cross-sectional study. Front Public Health. 2022;10:957630. doi:10.3389/fpubh.2022.957630
20. Naqvi AA, Hassali MA, Rizvi M, et al. Validation of the general medication adherence scale in pakistani patients with rheumatoid arthritis. Front Pharmacol. 2020;11:1039. doi:10.3389/fphar.2020.01039
21. Goretzko D, Siemund K, Sterner P. Evaluating model fit of measurement models in confirmatory factor analysis. Educ Psychol Meas. 2024;84(1):123–144. doi:10.1177/00131644231163813
22. Stone BM. The ethical use of fit indices in structural equation modeling: recommendations for psychologists. Front Psychol. 2021;12:783226. doi:10.3389/fpsyg.2021.783226
23. Melak AD, Wondimsigegn D, Kifle ZD. Knowledge, prevention practice and associated factors of stroke among hypertensive and diabetic patients–a systematic review. Risk Manage Healthc Polic. 2021;14:3295–3310. doi:10.2147/RMHP.S324960
24. Naga MS, Bedier NA, Salem MA, Ahmed HAM, Elhfnawy AM. Effect of competency based program on nurses’ knowledge, skills and attitude toward the care of patients with stroke. Alexandria Sci Nurs J. 2021;23(2):10–21. doi:10.21608/asalexu.2021.219098
25. Low MA, Power E, McGrath M. Sexuality after stroke: exploring knowledge, attitudes, comfort and behaviours of rehabilitation professionals. Ann Phys Rehabil Med. 2022;65(2):101547. doi:10.1016/j.rehab.2021.101547
26. Syed W, Qadhi OA, Barasheed A, AlZahrani E, Basil A, Al-Rawi M. Evaluation of knowledge of risk factors and warning signs of stroke–An observational study among future health care professionals. Front Public Health. 2023;11:1131110. doi:10.3389/fpubh.2023.1131110
27. Saade S, Hallit S, Salameh P, Hosseini H. Knowledge and response to stroke among Lebanese adults: a population-based survey. Front Public Health. 2022;10:891073. doi:10.3389/fpubh.2022.891073
28. Xiang R, Zhai X, Zhang Q, Wang Z. Relationship between dietary knowledge, socioeconomic status, and stroke among adults involved in the 2015 China health and nutrition survey. Front Nutri. 2021;8:728641. doi:10.3389/fnut.2021.728641
29. Al-Obaidi H, Khidhair Z, Jirjees F, et al. Factors associated with knowledge and awareness of stroke in the Iraqi population: a cross-sectional study. Front Neurol. 2023;14:1144481. doi:10.3389/fneur.2023.1144481
30. Kiær C, Lundquist CB, Brunner I. Knowledge and application of upper limb prediction models and attitude toward prognosis among physiotherapists and occupational therapists in the clinical stroke setting. Topic Stroke Rehabilitat. 2021;28(2):135–141. doi:10.1080/10749357.2020.1783915
31. Liu M, Wu Z, Liu GG, Xiao L, Li S. Barriers and facilitators for stroke patients’ adherence to rehabilitation in China: a qualitative study based on medical experts. Sci Rep. 2025;15(1):31525. doi:10.1038/s41598-025-12795-w
32. Zeng S, Wu M, Xu L, et al. Challenges in accessing community-based rehabilitation and long-term care for older adult stroke survivors and their caregivers: a Qualitative Study. J Multidiscipl Healthc. 2024;17(null):4829–4838. doi:10.2147/JMDH.S476993
33. Reynolds K, Gu D, Muntner P, et al. Geographic variations in the prevalence, awareness, treatment and control of hypertension in China. J Hypertens. 2003;21(7):1273–1281. doi:10.1097/00004872-200307000-00014
34. Wu J, Cheng X, Qiu L, et al. Prevalence and clustering of major cardiovascular risk factors in china: a recent cross-sectional survey. Medicine. 2016;95(10):e2712. doi:10.1097/MD.0000000000002712
35. Yang H, Huang X, Yang C, et al. Time window for acute stroke management: a cross-sectional study among community healthcare practitioners in primary care. Int J Gene Med. 2022;15:4483–4493. doi:10.2147/IJGM.S361189
36. Moore JL, Virva R, Henderson C, et al. Applying the knowledge-to-action framework to implement gait and balance assessments in inpatient stroke rehabilitation. Arch Phys Med Rehabil. 2022;103(7):S230–S245. doi:10.1016/j.apmr.2020.10.133
37. Widjaja KK, Chulavatnatol S, Suansanae T, et al. Knowledge of stroke and medication adherence among patients with recurrent stroke or transient ischemic attack in Indonesia: a multi-center, cross-sectional study. Int J Clin Pharm. 2021;43:666–672. doi:10.1007/s11096-020-01178-y
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge, Attitudes, and Practices Regarding Ergonomic Hazards Among Healthcare Workers in a Saudi Government Hospital

ALHazim SS, Al-Otaibi ST, Herzallah NH
Journal of Multidisciplinary Healthcare 2022, 15:1771-1778
Published Date: 24 August 2022
Dynamics of Patient-Based Benefit-Risk Assessment of Medicines in Chronic Diseases: A Systematic Review
EL Masri H, McGuire TM, van Driel ML, Benham H, Hollingworth SA
Patient Preference and Adherence 2022, 16:2609-2637
Published Date: 20 September 2022
Self-Medication Prevalence and Factors Associated with Knowledge and Attitude Towards Self-Medication Among Undergraduate Health Science Students at GAMBY Medical and Business College, Bahir Dar, Ethiopia
Siraj EA, Yayehrad AT, Kassaw AT, Kassahun D, Solomon E, Abdela H, Gizachew G, Awoke E
Patient Preference and Adherence 2022, 16:3157-3172
Published Date: 5 December 2022
Dermatologists’ Knowledge, Attitude, and Practice Pattern Toward Low-Dose Oral Minoxidil in Hair Loss in Saudi Arabia
Altalhab S
Clinical, Cosmetic and Investigational Dermatology 2024, 17:653-662
Published Date: 15 March 2024
Caregivers’ Knowledge, Attitudes, and Practices Regarding Risk Factors and Management of Post-Stroke Delirium Among Stroke Patients: A Cross-Sectional Study
Zhao L, Xu Y, Zhang Y, Gong Q, Bao J
International Journal of General Medicine 2026, 19:559169
Published Date: 14 January 2026