Back to Journals » International Journal of General Medicine » Volume 19
Caregivers’ Knowledge, Attitudes, and Practices Regarding Risk Factors and Management of Post-Stroke Delirium Among Stroke Patients: A Cross-Sectional Study
Authors Zhao L, Xu Y, Zhang Y, Gong Q, Bao J
Received 30 August 2025
Accepted for publication 7 January 2026
Published 14 January 2026 Volume 2026:19 559169
DOI https://doi.org/10.2147/IJGM.S559169
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Woon-Man Kung
Lirong Zhao,1,* Yamin Xu,2,* Yan Zhang,3 Qing Gong,4 Jingjing Bao1
1Department of Neurology, Huadong Hospital Affiliated to Fudan University, Shanghai, 200040, People’s Republic of China; 2Day Care Chemotherapy, Huadong Hospital Affiliated to Fudan University, Shanghai, 200040, People’s Republic of China; 3Department of Geriatrics, Huadong Hospital Affiliated to Fudan University, Shanghai, 200040, People’s Republic of China; 4Shanghai Mental Health Center, Shanghai Jiao Tong University School of Medicine, Shanghai, 200030, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yan Zhang, Department of Geriatrics, Huadong Hospital Affiliated to Fudan University, Shanghai, 200040, People’s Republic of China, Tel +8618121220713, Email [email protected] Qing Gong, Shanghai Mental Health Center, Shanghai Jiao Tong University School of Medicine, Shanghai, 200030, People’s Republic of China, Email [email protected]
Objective: To investigate the knowledge, attitudes, and practices (KAP) of caregivers of stroke patients regarding the risk factors and management of post-stroke delirium.
Methods: This multicenter, cross-sectional study was conducted among caregivers of stroke patients who visited two tertiary hospitals and three community health service centers between November 2023 and January 2024. In this study, knowledge, attitude, and practice were assessed using structured scoring systems, with knowledge scored from 0– 24, attitudes from 7– 35, and practices from 9– 45.
Results: A total of 484 valid questionnaires were included, with 325 (67.1%) females respondents. The median (25th, 75th percentile) KAP scores were 9.00 (2.00, 12.00) (possible range: 0– 24), 24.00 (23.00, 26.00) (possible range: 7– 35), and 33.00 (27.00, 36.00) (possible range: 9– 45), respectively. Multivariate logistic regression analysis showed that knowledge score (OR = 1.11, 95% CI: 1.07, 1.16), attitude score (OR = 1.48, 95% CI: 1.32, 1.67), duration of stroke diagnosis > 2 years (OR = 0.47, 95% CI: 0.26, 0.83), and lack of participation in related education (OR = 0.43, 95% CI: 0.26, 0.72) were independently associated with practices. Structural equation modeling revealed that knowledge directly influenced attitudes (β = − 0.39, P < 0.001) and practice (β = 0.30, P < 0.001), while attitudes also directly influenced practices (β = − 0.51, P < 0.001). Knowledge indirectly affected practices through its effect on attitudes (β = 0.20, P < 0.001).
Conclusion: Caregivers of stroke patients exhibited inadequate knowledge, neutral attitudes and moderate practices regarding risk factors and management of post-stroke delirium. Targeted educational interventions should be implemented for caregivers, emphasizing the importance of recognizing and effectively managing post-stroke delirium.
Keywords: knowledge, attitude, practice, caregiver, stroke, post-stroke delirium, cross-sectional study
Introduction
The China Stroke Report, issued in 2020, underscores the significant public health challenge posed by stroke in China, revealing a prevalence rate of 1114.8 per 100,000 population, an annual incidence rate of 246.8 per 100,000, and a mortality rate of 149.49 per 100,000.1 Additionally, on a global scale, China has emerged as the nation with the highest lifetime risk of stroke and consequent disease burden.2 Post-stroke delirium, a consequential and potentially preventable complication of acute strokes, presents a significant clinical challenge. In China, although systematic large-scale epidemiological data on post-stroke delirium remain limited, regional studies have reported an incidence rate ranging from 12% to 30% in acute stroke patients, highlighting its relevance and the urgent need for attention in clinical settings.3 Studies have underscored its frequency, severity, and potential for prevention.4 The prevalence of post-stroke delirium varies considerably, ranging from 11% to 42%, as reported in recent literature.5 Moreover, the prognosis for patients with post-stroke delirium remains grim, with a 5-year survival rate as low as 39%.6 Furthermore, this condition is consistently associated with adverse outcomes, including increased mortality, functional disability, and the need for long-term care placement.7
Investigating the knowledge, attitudes, and practices (KAP) of caregivers of stroke patients regarding the risk factors and management of post-stroke delirium is essential to improving the quality of stroke care. Previous studies have shown that caregivers’ knowledge and attitudes significantly influence early symptom recognition, adherence to secondary prevention, and functional recovery among stroke survivors, thereby affecting overall care quality.8,9 In China, informal caregivers—primarily family members—shoulder the majority of long-term caregiving responsibilities for stroke survivors. However, studies indicate that many of these caregivers lack sufficient knowledge and training in managing stroke-related complications, particularly post-stroke delirium.10 This lack of awareness may lead to delayed recognition of symptoms, inappropriate responses, and heightened caregiver burden. The KAP model, which suggests that individual behaviors are shaped by their knowledge and attitudes, has been widely employed in public health research to understand and influence health behaviors.11 While there is existing research on KAP related to stroke,12 limited attention has been given to post-stroke delirium, an acute and often under-recognized complication that can significantly affect recovery outcomes. Given caregivers’ critical role in monitoring and managing patients at home, their understanding of post-stroke delirium directly influences early detection, timely medical intervention, and overall patient prognosis. Assessing caregivers’ KAP in this context not only provides insights into existing knowledge gaps and misconceptions but also helps healthcare providers develop targeted educational interventions. Therefore, this study aims to investigate the KAP of caregivers of stroke patients regarding risk factors and management of post-stroke delirium. Previous studies have also indicated that several caregiver- and patient-related characteristics may influence KAP outcomes in cross-sectional research. Higher educational attainment is associated with better health literacy and symptom interpretation among caregivers,13 while employed caregivers often have greater access to health information and learning resources that may enhance caregiving competence.14 Participation in delirium- or stroke-related education has been shown to significantly improve caregivers’ preparedness and understanding of stroke complications.15 In addition, uncertainty about whether a patient has experienced delirium often reflects insufficient awareness of delirium manifestations, and longer stroke duration has been linked to increasing caregiver burden and reduced engagement in recommended practices over time.16 Given the cross-sectional design, caregiver and patient characteristics may influence KAP outcomes and should be considered in interpretation.
Methods
Study Design and Participants
This cross-sectional study was conducted among caregivers of stroke patients between November 2023 and January 2024 at two tertiary hospitals and three community health service centers. Inclusion Criteria: (1) Individuals engaged in full-time caregiving for stroke patients for at least one year; (2) Home caregivers; (3) Willingness to participate in this study. Volunteers or part-time caregivers for stroke patients were excluded. Ethical approval for the study was obtained from the Ethics Committee of Fudan University Affiliated East Hospital (Approval No: 20230123). Fudan University Affiliated East Hospital served as the coordinating center for this project. In accordance with institutional collaboration agreements, the ethical approval granted by the coordinating center was recognized and accepted by the other participating tertiary hospital and the three community health service centers. All participants were informed of the study protocol and provided informed consent. All methods were performed in accordance with relevant guidelines and regulations. This study was conducted in accordance with the Declaration of Helsinki (2000) of the World Medical Association.
Questionnaire Design
The questionnaire design was informed by relevant guidelines such as the “Comprehensive Hospital Delirium Diagnosis and Treatment Chinese Expert Consensus (2021)” and the “2023 NICE Clinical Guideline: Delirium: Prevention, Diagnosis, and Management in Hospital and Long-term Care [CG103]15 “, as well as recent literature such as Yoon et al (2024), which highlights contemporary strategies for the diagnosis, prevention, and management of delirium,16 in addition to relevant literature sources.17 Content validity was evaluated by four invited experts, who assessed the clarity, relevance, and completeness of the items. A pilot test was subsequently conducted with 42 caregivers of stroke patients from one of the participating community health centers, who met the same inclusion criteria as the main study. Internal consistency reliability was calculated using Cronbach’s α, yielding a value of 0.937. Items were further refined based on pilot feedback to improve comprehension and acceptability.
The final questionnaire, developed in Chinese (A blank questionnaire translated into English was attached as (Figure S1–S4), comprised four data collection dimensions encompassing a total of 38 items. These dimensions included: Basic Information, consisting of 15 items; Knowledge Dimension, comprising 7 questions, including 4 sub-items in Question 4 and 3 sub-items in Question 7, resulting in a total of 12 scored items; Attitude Dimension, consisting of 7 items; and Practice Dimension, comprising 9 items. Scoring rules were established as follows: 1) For the Knowledge Dimension: Respondents were awarded 2 points for selecting “very familiar,” 1 point for “heard of,” and 0 points for “uncertain,” resulting in a potential score range of 0 to 24. 2) For the Attitude Dimensions: A five-point Likert scale was employed, resulting in a potential score range of 7 to 35 points. 4) For the Practice Dimension: All items (1–9) were scored as follows: a=5, b=4, c=3, d=2, e=1, with a potential score range of 9 to 45.
Questionnaire Distribution Quality Control
Five experienced nurses, all trained professionals, served as research assistants for this study. Their responsibilities included elucidating the study’s purpose and significance to participants and securing their signed consent forms. Furthermore, dedicated nurses provided participants with explanations and assessments of delirium theory and symptoms. The study participants consisted of caregivers of stroke patients and their family members recruited from two tertiary hospitals and three community health centers. This multifaceted approach facilitated thorough coverage and quality control during the data collection process.
The electronic questionnaire was hosted on Sojump (http://www.sojump.com), an online survey platform. The questionnaire link was distributed to participants via Quick Response Code or through a WeChat group. Before answering the questionnaire, participants were required to indicate informed consent by clicking the option “I agree to participate in this study” at the beginning of the electronic form. For participants with limited literacy, trained research staff were available in-person at hospital or community sites to ex the study purpose, procedures, and rights verbally, and to assist with the digital consent process as needed. All data were collected anonymously. To prevent duplication, IP restrictions were applied, allowing only one submission per device.
Sample Size
The sample size was calculated using the formula for cross-sectional studies18 with a significance level of α=0.05. Accordingly, Z1-α/2 was 1.96 when α=0.05. To maximize the required sample size, the estimated p was set at 0.5, and the allowable margin of error (δ) was set as 5%. Based on these parameters, the calculated theoretical sample size was 480, which included an additional 20% to account for potential loss to follow-up.
Statistical Analysis
Statistical analysis was conducted using SPSS 26.0 (IBM Corp., Armonk, N.Y., USA) and STATA 18.0 (StataCorp LLC, College Station, TX, USA). Continuous variables were described using median (25th percentile, 75th percentile), and between-group comparisons were performed using Wilcoxon-Mann–Whitney tests or Kruskal–Wallis analysis of variance. Categorical variables were presented as n (%). Spearman correlation analysis was employed to assess the correlations between knowledge, attitude, and practice scores. Univariate and multivariate logistic regression were performed to explore the risk factors associated with K, A, and P. Univariate variables with P<0.1 were enrolled in multivariate regression. Structural Equation Modeling (SEM) was employed to investigate the path relationships among KAP, and demographic variables. The use of SEM was guided by the theoretical framework of the KAP model, which posits directional and mediating relationships among these constructs and is thus suitable for confirmatory analysis. Given the non-normality of the data, the bootstrap resampling method (300 samples) was employed to calculate 95% confidence intervals and test the hypothesized path relationships. This non-parametric approach does not rely on distributional assumptions and is well-suited for skewed data. The approach follows recommendations by Efron and Tibshirani.19 Two-sided p<0.05 were considered statistically significant in this study.
Results
Participant Characteristics
Initially, a total of 532 questionnaires were collected in this study, and the samples in the following cases were deleted, specifically: 46 questionnaires with a response time of less than 90s were excluded, and 2 cases of non-informed consent questionnaires were excluded, resulting in a final valid data of 484 cases, with a validity rate of 90.98%. To further assess validity, Confirmatory Factor Analysis (CFA) was performed, and item loadings ranged from 0.589 to 0.876, all statistically significant (P < 0.001) (Figure S5), supporting convergent validity. The model fit indices were satisfactory (CMIN/DF = 4.016, RMSEA = 0.079, IFI = 0.909, TLI = 0.901, CFI = 0.909). In addition, the Kaiser-Meyer-Olkin (KMO) test value was 0.954 (P < 0.001), indicating strong sampling adequacy. Among all participants, 325 (67.1%) were female. The median (25%,75%) KAP scores were 9.00 [2.00, 12.00] (possible range: 0–15), 24.00 [23.00, 26.00] (possible range: 7–35), and 33.00 [27.00, 36.00] (possible range: 9–45), respectively, indicating inadequate knowledge, neutral attitudes and moderate practices. In addition, inter-group comparisons revealed several significant differences across demographic characteristics. Participants with higher education levels, particularly those with college or bachelor’s degrees, had significantly higher knowledge, attitude, and practice scores compared with those with lower educational attainment (all P<0.001). Employment status was also associated with significant differences, with employed caregivers scoring higher across all KAP dimensions (all P<0.001). Significant differences were further observed across age groups (knowledge: P<0.001; attitudes: P=0.001; practices: P<0.001), gender (knowledge: P=0.020; attitudes: P=0.015; practices: P=0.002), monthly income (knowledge: P=0.011; attitudes: P=0.009; practices: P=0.002), and several behavioral or clinical characteristics, including smoking status, drinking status, and whether the patient had experienced delirium (Table 1).
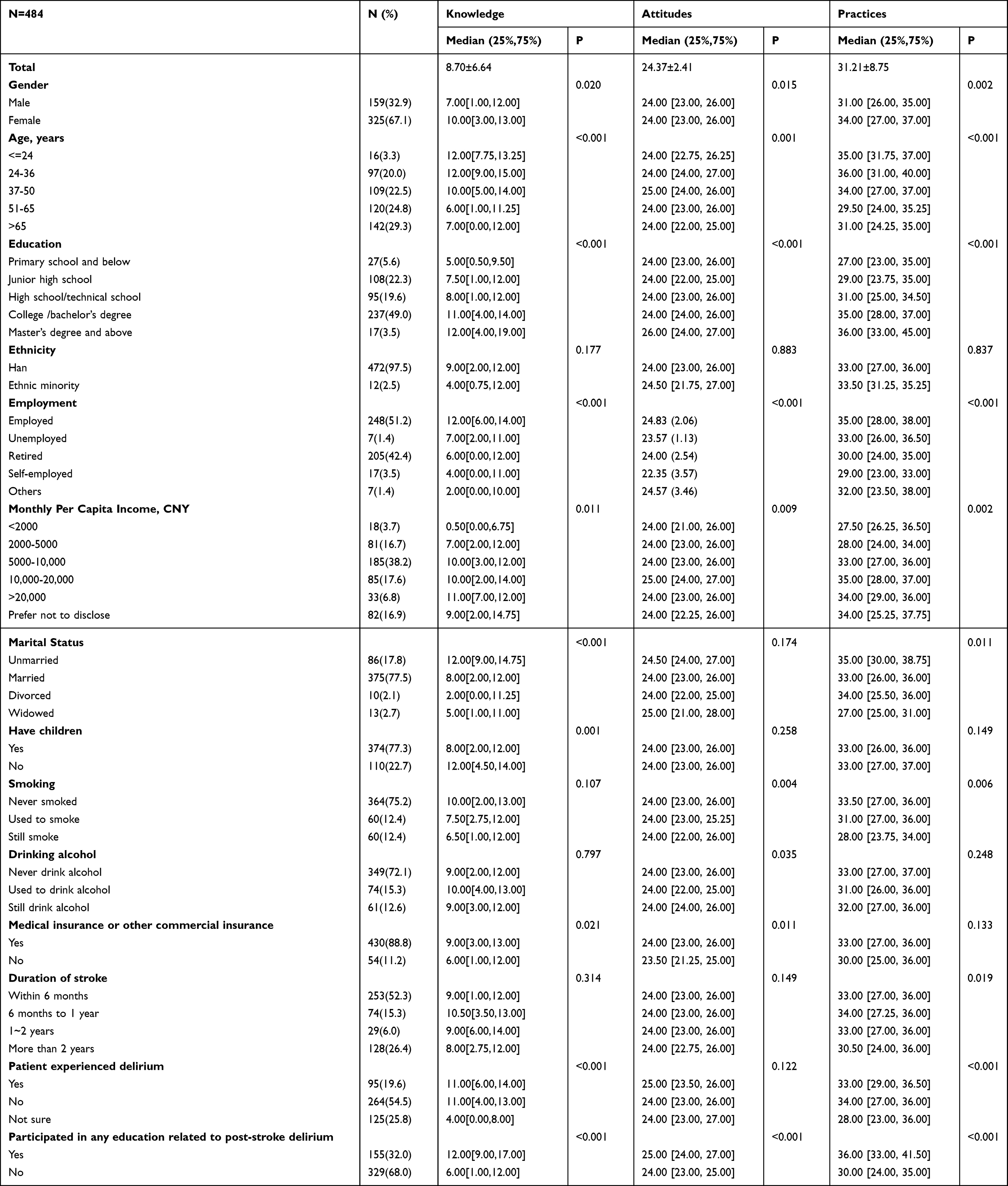 |
Table 1 Demographic Characteristics and KAP Scores |
Item-Level Performance in KAP Dimensions
Regarding knowledge, only a minority of caregivers were very familiar with key symptoms and risk factors, with notable uncertainty about specific clinical factors such as lesion location (Table S1). Attitudes toward post-stroke delirium were generally positive, with most caregivers supporting regular assessment and increased support from healthcare professionals (Table S2). In terms of practice, while most caregivers reported frequently engaging in supportive behaviors, such as seeking professional help or encouraging rehabilitation, active learning about delirium management remained limited (Table S3).
Correlations Among Knowledge, Attitudes, and Practices
In the correlation analyses, significant positive correlations were found between knowledge and attitude (r = 0.1539, P < 0.001), knowledge and practice (r = 0.4270, P < 0.001), as well as attitude and practice (r = 0.4416, P < 0.001), respectively (Table 2).
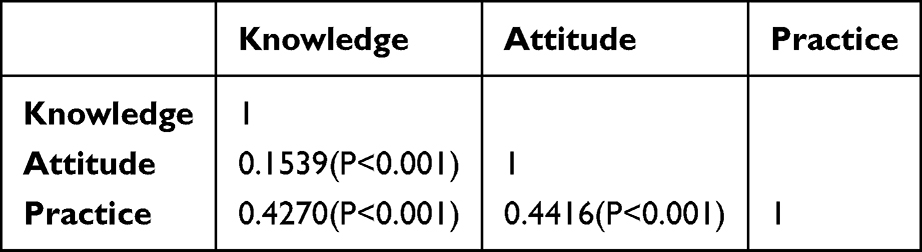 |
Table 2 Correlation Analysis |
Factors Associated with Knowledge, Attitudes, and Practices
Multivariate analysis results showed that being unsure whether the patient had delirium (OR = 0.30, 95% CI: [0.10,0.94], P = 0.038), which suggests a 70% lower likelihood of sufficient knowledge, and not participating in related education (OR = 0.23, 95% CI: [0.12,0.46], P < 0.001), indicating a 77% reduction in the odds of having sufficient knowledge, were independently associated with poor knowledge (Table 3). Concurrently, not participated in related education (OR = 0.56, 95% CI: [0.33,0.95], P = 0.033) was independently associated with negative attitude (Table 4). Furthermore, knowledge score (OR = 1.11, 95% CI: [1.07,1.16], P < 0.001), indicating that a one-point increase in knowledge score was associated with an 11% increase in the odds of better caregiving practices; attitude score (OR = 1.48, 95% CI: [1.32,1.67], P < 0.001), suggesting that a one-point increase in attitude score was associated with a 48% increase in the odds of better practices; patient diagnosed with stroke for more than 2 years (OR = 0.47, 95% CI: [0.26,0.83], P = 0.009), indicating a 53% decrease in the odds of better practices; and not participated in related education (OR = 0.43, 95% CI: [0.26,0.72], P = 0.001), suggesting a 57% lower likelihood of better practices, were independently associated with caregiving practices (Table 5).
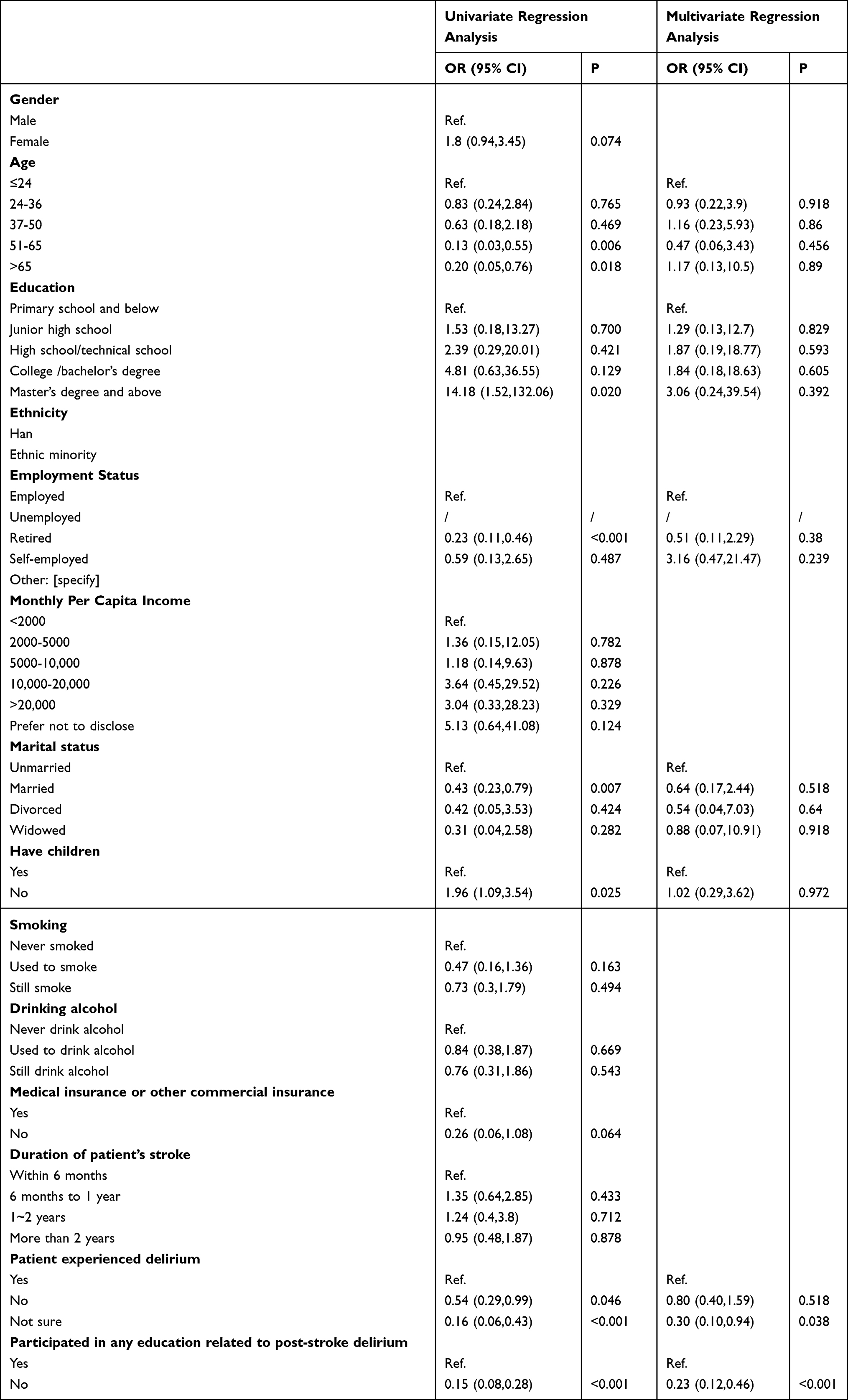 |
Table 3 Univariate and Multivariate Regression Analysis for Knowledge Dimension |
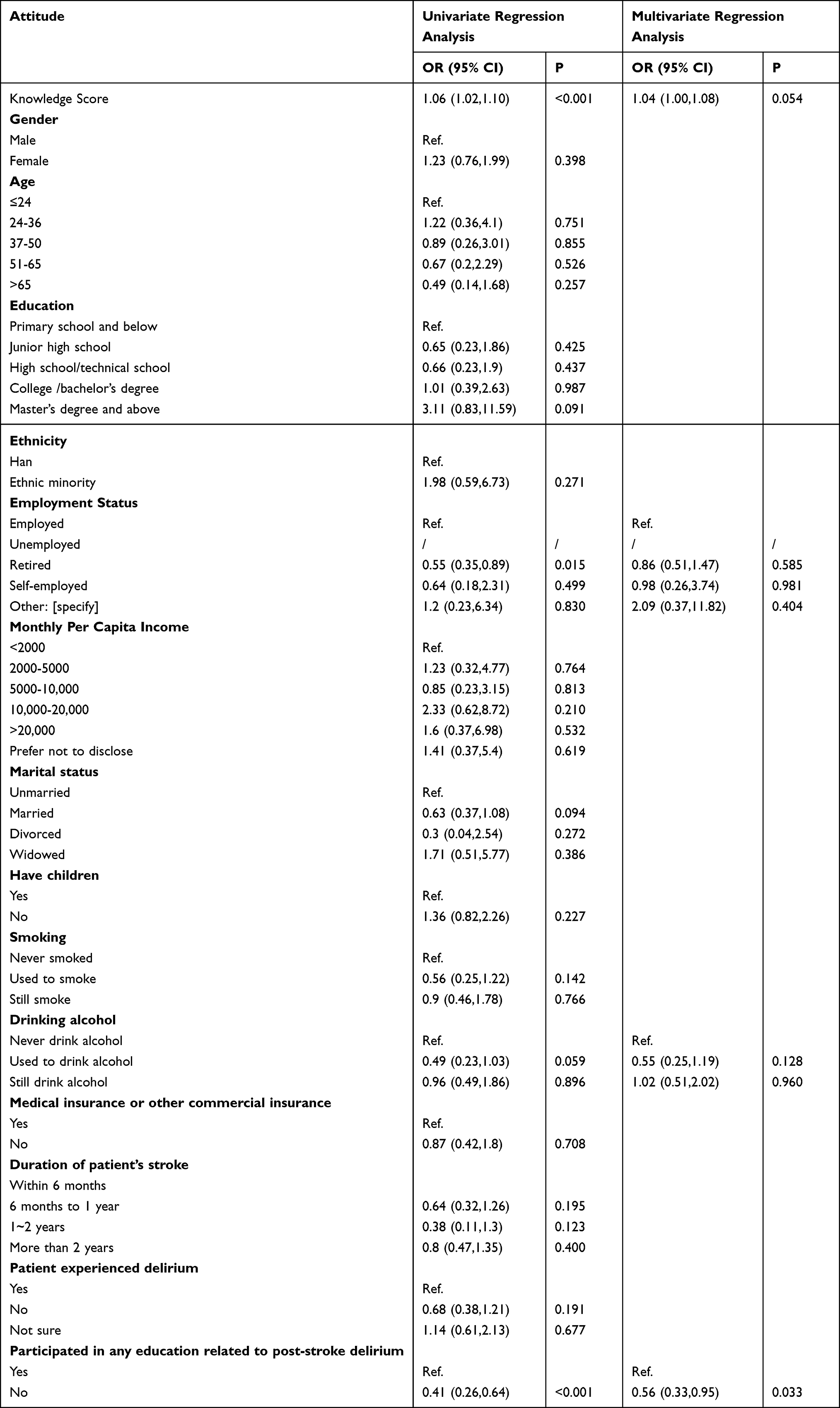 |
Table 4 Univariate and Multivariate Regression Analysis for Attitude Dimension |
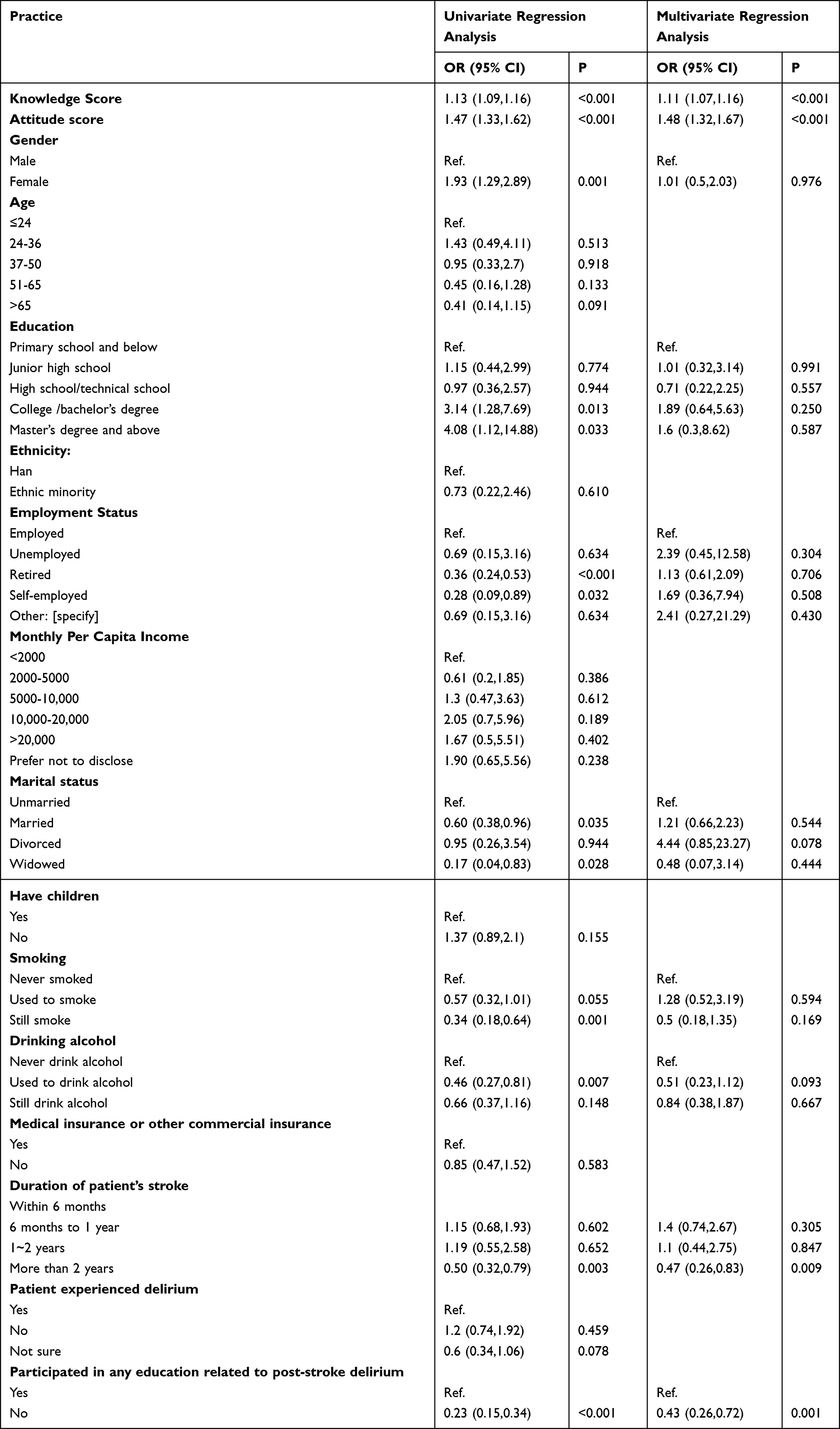 |
Table 5 Univariate and Multivariate Regression Analysis for Practice Dimension |
SEM Results
The SEM demonstrate a highly favorable model fit indices, suggesting a well-fitting model (Table S4), and shown that knowledge had direct effects on attitude (β = −0.39, P < 0.001) and practice (β = 0.30, P < 0.001). Moreover, attitudes have a direct impact on practice (β = −0.51, P < 0.001). Additionally, knowledge has an indirect effect on practice through attitude (β = 0.20, P < 0.001) (Table 6 and Figure 1).
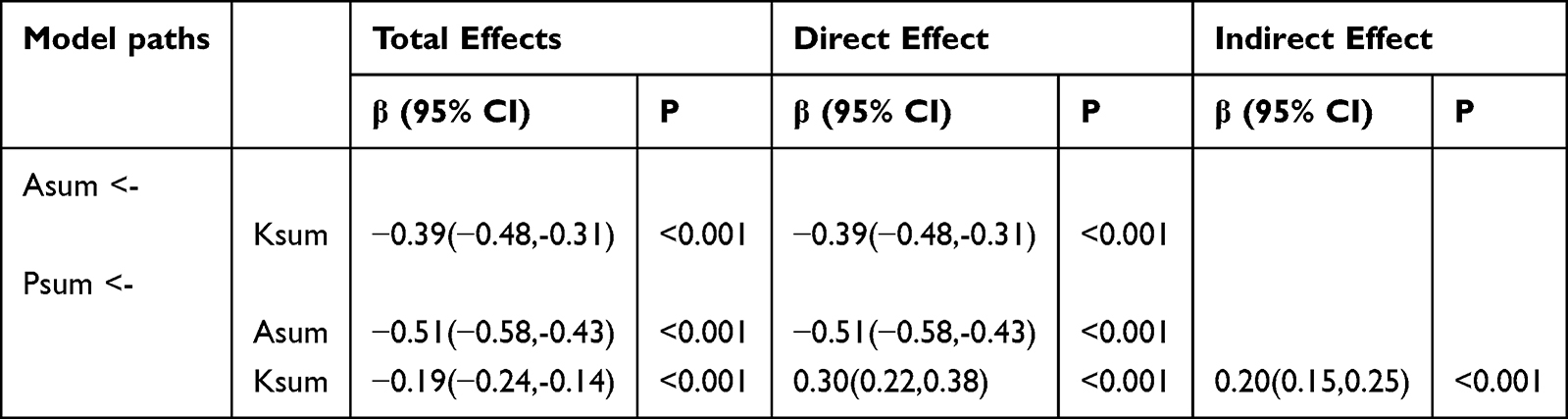 |
Table 6 Analysis of Direct and Indirect Effects |
 |
Figure 1 SEM model. |
Discussion
This study demonstrated that caregivers of stroke patients have inadequate knowledge, neutral attitudes, and moderate practices concerning the identification and management of post-stroke delirium. In addition to the overall KAP performance, several caregiver- and patient-related characteristics were identified as associated factors influencing these outcomes. Lower educational attainment, retirement status, lack of participation in delirium-related education, uncertainty about whether the patient had experienced delirium, and caring for patients with stroke duration longer than two years were all related to poorer performance in one or more KAP dimensions. The findings add new insight by identifying key caregiver- and patient-related factors linked to KAP outcomes and by demonstrating the direct and indirect pathways among knowledge, attitudes, and practices through SEM. This study provides new evidence by quantitatively illustrating how caregiver knowledge exerts both direct and indirect effects on attitudes and practices, offering a clearer explanation of the behavioral mechanisms involved in post-stroke delirium care. It is recommended that healthcare providers prioritize educational interventions targeting caregivers to enhance their knowledge, attitudes, and practices regarding post-stroke delirium management, thereby improving patient outcomes and reducing the burden on healthcare systems.
Several associated factors identified in this study warrant further explanation. Caregivers with lower educational attainment showed poorer KAP performance, consistent with evidence that limited education reduces health literacy and symptom recognition.13 Employed caregivers demonstrated better outcomes, which may relate to greater access to health-related information and resources.14 In addition, caregivers who had not participated in delirium-related education exhibited significantly poorer knowledge and attitudes, supporting findings that structured caregiver training improves preparedness in managing stroke-related complications.15 Caregivers who were unsure whether the patient had experienced delirium showed markedly lower knowledge levels, reflecting insufficient awareness of delirium symptoms and the challenges of recognizing delirium at home.20 Moreover, caring for patients with stroke duration longer than two years was associated with poorer practices, aligning with literature showing that long-term caregiving burden may diminish vigilance and reduce caregiving capability.16 These findings highlight the need for targeted, individualized educational interventions.
The findings of this study reveal concerning disparities in knowledge, attitude, and practice among caregivers of stroke patients regarding the identification and management of post-stroke delirium. In comparing the results from inter-group comparisons and the multivariate logistic regression, one notable common result is the significant association between education levels and caregiver knowledge, attitude, and practice. The inter-group comparisons revealed that participants with higher education, particularly those with college/bachelor’s degrees and above, demonstrated superior scores across all domains compared to those with lower educational attainment. This finding aligns with existing literature highlighting the positive correlation between education levels and health literacy.13 Moreover, the multivariate logistic regression also identified not participating in related education as independently associated with poor knowledge and negative attitude among caregivers. This suggests that educational interventions play a crucial role in shaping caregivers’ understanding and attitudes towards post-stroke delirium management.
Another common finding between the two analyses is the association between employment status and caregiver outcomes. The inter-group comparisons revealed that employed individuals scored significantly higher in knowledge, attitude, and practice compared to other employment categories. Similarly, the multivariate logistic regression identified employment status as a significant predictor of caregiving practices, with employed caregivers demonstrating better practices. This finding may be attributed to employed individuals having access to resources, such as workplace-based educational programs or greater financial stability, which could positively influence their ability to provide care effectively.14
However, there are instances where results from the multivariate logistic regression analysis reveal additional insights not captured by inter-group comparisons. For example, the regression analysis identified patient duration of stroke diagnosis of more than 2 years as independently associated with poorer caregiving practices, whereas this association was not evident in the inter-group comparisons. This discrepancy may be due to the complex interplay of factors affecting caregiving practices, including the progression of stroke-related symptoms over time and the evolving needs of patients and caregivers.21 Future research could explore the longitudinal effects of stroke duration on caregiving practices to better understand this relationship. This finding suggests that age may interact with other variables, such as educational attainment or caregiving experience, to influence caregiver knowledge levels.
The correlation analyses and SEM results provide additional insights into the relationships between knowledge, attitude, and practice among caregivers. The positive correlations observed between knowledge and attitude, knowledge and practice, as well as attitude and practice, underscore the interconnected nature of these variables, supporting the idea that enhancing knowledge can positively influence attitudes and subsequent practices.22 Although SEM results showed negative paths from knowledge to attitude and from attitude to practice, this does not contradict the positive correlations seen in bivariate analysis. The SEM was based on latent variables from item-level data, while correlations used total scores. One possible explanation is that increased knowledge may raise awareness of challenges in delirium care, leading to more cautious or critical attitudes. Furthermore, the SEM analysis demonstrates that knowledge directly impacts both attitude and practice, with attitude also directly influencing practice, highlighting the importance of fostering positive attitudes alongside improving knowledge levels. The indirect effect of knowledge on practice through attitude suggests that interventions aimed at modifying caregivers’ attitudes may have a significant impact on their actual caregiving behaviors.
Among caregivers, knowledge regarding post-stroke delirium varied across different aspects. Notably, while there was a relatively high level of awareness about delirium occurrence after stroke, specific knowledge regarding its symptoms and management appeared to be less robust. For instance, items related to recognizing the symptoms of delirium, such as attention disorders, consciousness content disorders, and cognitive function disorders, received relatively lower scores compared to items addressing general concepts. To address the gaps in knowledge regarding post-stroke delirium, targeted educational programs should be developed. These programs should go beyond general definitions and provide in-depth training on symptom recognition and management strategies.23 Interactive workshops and training sessions led by healthcare professionals can enhance caregivers’ understanding of delirium symptoms and equip them with practical skills to identify and manage these symptoms effectively. Additionally, the development of educational materials such as brochures, videos, and online resources tailored to caregivers’ needs can serve as valuable tools for ongoing education and reference.
Caregivers demonstrated varying attitudes towards post-stroke delirium management, reflecting their perceptions and beliefs regarding the condition. Notably, caregivers expressed strong concern and a sense of responsibility towards delirium management, as evidenced by the majority agreeing on the importance of specialized training for caregivers. However, despite the recognition of the importance of non-pharmacological interventions, a significant proportion of caregivers expressed belief in the effectiveness of medication therapy for managing delirium. This finding suggests a potential gap between caregivers’ attitudes and evidence-based recommendations advocating for non-pharmacological approaches as the cornerstone of delirium management.15 Educational initiatives aimed at promoting evidence-based practices in delirium management should be implemented. These initiatives should focus on dispelling misconceptions surrounding delirium and emphasizing the importance of non-pharmacological interventions. Workshops, seminars, and support groups led by healthcare professionals can provide caregivers with firsthand knowledge and experiences to challenge preconceived notions and foster a positive attitude towards delirium prevention and management. Moreover, fostering collaborative relationships between caregivers and healthcare professionals through mentorship programs or peer support networks can facilitate ongoing guidance and reinforcement of positive attitudes towards delirium management.20
Caregivers’ practices regarding post-stroke delirium management encompassed a range of proactive behaviors, yet certain areas showed room for improvement. While caregivers demonstrated willingness to engage in learning activities and seek professional advice, challenges were evident in consistently implementing preventive measures and participating in formal educational activities. Moreover, despite recognizing the importance of prompt action in seeking assistance from healthcare professionals when delirium symptoms arise, a substantial proportion of caregivers reported uncertainty or inconsistency in observing delirium symptoms and participating in screening activities. Practical interventions should be implemented to facilitate caregivers’ engagement in preventive measures and educational activities. This could involve providing caregivers with access to screening tools and resources for regular delirium risk assessments. Healthcare institutions can offer training sessions on how to use these tools effectively and integrate them into daily caregiving routines. Additionally, the development of caregiver support programs, including respite care services and peer support groups, can alleviate caregiver burden and promote consistent engagement in delirium prevention practices. Furthermore, implementing technology-based solutions such as mobile applications or telehealth platforms can facilitate remote access to educational resources and consultations, particularly for caregivers in remote or underserved areas.24 From a clinical perspective, the findings suggest several practical applications. Healthcare providers may incorporate brief caregiver-focused delirium education into routine stroke follow-up care to strengthen early recognition and response. Simple observation checklists or screening tools can be distributed to caregivers to facilitate daily monitoring at home. Integrating delirium-related education into hospital discharge planning and community rehabilitation programs may further enhance continuity of care and reduce delays in symptom detection.
This study had several limitations. Firstly, the cross-sectional design employed limits the ability to establish causal relationships between variables. Secondly, the reliance on self-reported data via questionnaires may introduce response bias and potential inaccuracies. Thirdly, the study’s sample was drawn from specific healthcare settings, potentially limiting the generalizability of the findings to broader caregiver populations. In addition, the use of self-reported questionnaires may be subject to social desirability bias, as participants might respond in ways they perceive as favorable or expected. The sample, primarily drawn from urban tertiary hospitals and affiliated community health centers, may not fully represent caregivers in rural or lower-resource settings, introducing potential selection bias. Furthermore, the cross-sectional nature of the study limits inference on the directionality or causality of the relationships observed, underscoring the need for longitudinal research in future studies.
In conclusion, caregivers of stroke patients demonstrated inadequate knowledge, neutral attitudes, and moderate practices concerning the risk factors and management of post-stroke delirium. Given these findings, it is imperative for healthcare providers to implement targeted educational interventions aimed at enhancing caregivers’ understanding of post-stroke delirium. Recommended strategies may include interactive workshops to improve recognition and response to delirium symptoms, mobile applications for accessible caregiver education and real-time symptom monitoring, and policy-level integration of caregiver training programs into stroke care pathways. These measures could collectively enhance caregiver capacity and patient outcomes in both hospital and home settings.
Abbreviations
KAP, knowledge, attitudes, and practices; SEM, Structural Equation Modeling.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics Approval and Consent to Participate
Ethical approval for the study was obtained from the Ethics Committee of Fudan University Affiliated East Hospital (Approval No: 20230123), and All participants were informed about the study protocol and provided written informed consent to participate in the study. I confirm that all methods were performed in accordance with the relevant guidelines. This work has been carried out in accordance with the Declaration of Helsinki (2000) of the World Medical Association.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Fosun Research Foundation of Fudan University.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Wang YJ, Li ZX, Gu HQ, et al. China stroke statistics 2019: a report from the national center for healthcare quality management in neurological diseases, china national clinical research center for neurological diseases, the chinese stroke association, national center for chronic and non-communicable disease control and prevention, chinese center for disease control and prevention and institute for global neuroscience and stroke collaborations. Stroke Vasc Neurol. 2020;5(3):211–16. doi:10.1136/svn-2020-000457
2. Global. regional, and national age-sex specific mortality for 264 causes of death, 1980-2016: a systematic analysis for the global burden of disease study 2016. Lancet. 2017;390(10100):1151–1210. doi:10.1016/S0140-6736(17)32152-9
3. Zhang GB, Li HY, Yu WJ, et al. Occurrence and risk factors for post-stroke delirium: a systematic review and meta-analysis. Asian J Psychiatr. 2024;99:104132. doi:10.1016/j.ajp.2024.104132
4. Boßelmann C, Zurloh J, Stefanou MI, et al. delirium screening in aphasic patients with the Intensive Care Delirium Screening Checklist (ICDSC): a prospective cohort study. Front Neurol. 2019;10:1198. doi:10.3389/fneur.2019.01198
5. Girard TD, Thompson JL, Pandharipande PP, et al. Clinical phenotypes of delirium during critical illness and severity of subsequent long-term cognitive impairment: a prospective cohort study. Lancet Respir Med. 2018;6(3):213–222. doi:10.1016/S2213-2600(18)30062-6
6. Neufeld KJ, Thomas C. Delirium: definition, epidemiology, and diagnosis. J Clin Neurophysiol. 2013;30(5):438–442. doi:10.1097/WNP.0b013e3182a73e31
7. Miu DK, Yeung JC. Incidence of post-stroke delirium and 1-year outcome. Geriatr Gerontol Int. 2013;13(1):123–129. doi:10.1111/j.1447-0594.2012.00871.x
8. Bakas T, Clark PC, Kelly-Hayes M, King RB, Lutz BJ, Miller EL. Evidence for stroke family caregiver and dyad interventions. Stroke. 2014;45(9):2836–2852. doi:10.1161/STR.0000000000000033
9. King RB, Hartke RJ, Houle TT. Patterns of relationships between background characteristics, coping, and stroke caregiver outcomes. Top Stroke Rehabil. 2010;17(4):308–317. doi:10.1310/tsr1704-308
10. Liu Y, Chen H, Zhao K, He W, Lin S, He J. High levels of plasma fibrinogen are related to post-stroke cognitive impairment. Brain Behav. 2019;9(10):e01391. doi:10.1002/brb3.1391
11. Dostovic Z, Smajlovic D, Ibrahimagic OC, Dostovic A. Mortality and functional disability of poststroke delirium. Mater Sociomed. 2018;30(2):95–97. doi:10.5455/msm.2018.30.95-97
12. Pasińska P, Wilk A, Kowalska K, Szyper-Maciejowska A, Klimkowicz-Mrowiec A. The long-term prognosis of patients with delirium in the acute phase of stroke: pRospective Observational Polish Study (PROPOLIS). J Neurol. 2019;266(11):2710–2717. doi:10.1007/s00415-019-09471-1
13. Shen J, Xia Y, Cao S, et al. Knowledge, attitude, and practice regarding atrial fibrillation among neurologists in central China: a cross-sectional study. Clin Cardiol. 2020;43(6):639–646. doi:10.1002/clc.23361
14. Wanichanon W, Ananchaisarp T, Buathong N, Choomalee K. Knowledge and attitude towards stroke among the population of one rural community in southern Thailand: a survey. BMJ Open. 2024;14(2):e080269. doi:10.1136/bmjopen-2023-080269
15. Lin S, Wang C, Wang Q, et al. The experience of stroke survivors and caregivers during hospital-to-home transitional care: a qualitative longitudinal study. Int J Nurs Stud. 2022;130:104213. doi:10.1016/j.ijnurstu.2022.104213
16. Hu P, Yang Q, Kong L, Hu L, Zeng L. Relationship between the anxiety/depression and care burden of the major caregiver of stroke patients. Medicine. 2018;97(40):e12638. doi:10.1097/MD.0000000000012638
17. Aerts C, Revilla M, Duval L, et al. Understanding the role of disease knowledge and risk perception in shaping preventive behavior for selected vector-borne diseases in Guyana. PLoS Negl Trop Dis. 2020;14(4):e0008149. doi:10.1371/journal.pntd.0008149
18. Liao L, Feng H, Jiao J, Zhao Y, Ning H. Nursing assistants’ knowledge, attitudes and training needs regarding urinary incontinence in nursing homes: a mixed-methods study. BMC Geriatr. 2023;23(1):39. doi:10.1186/s12877-023-03762-z
19. Bradley E, T RJ. An Introduction to the Bootstrap. New York: Chapman & Hall/CRC; 1993.
20. McManus J, Pathansali R, Stewart R, Macdonald A, Jackson S. Delirium post-stroke. Age Ageing. 2007;36(6):613–618. doi:10.1093/ageing/afm140
21. National Institute for Health and Care Excellence. Copyright © NICE. Guidelines. Delirium: Prevention, Diagnosis and Management in Hospital and Long-Term Care. National Institute for Health and Care Excellence (NICE); London. 2023.
22. Yoon I, Galarneau D, Winslow M, et al. Diagnosis, prevention and management of delirium: spot it, stop it, treat it. BJPsych Advances. 2024;1–12.
23. Makin SD, Wardlaw J. Predicting delirium after a stroke. J Neurol Neurosurg Psychiatry. 2014;85(4):357. doi:10.1136/jnnp-2013-305379
24. Charan J, Biswas T. How to calculate sample size for different study designs in medical research? Indian J Psychol Med. 2013;35(2):121–126. doi:10.4103/0253-7176.116232
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge, Attitudes and Practices Towards Psoriasis Among Patients and Their Family Members
Zhang X, Du H, Liu X, Liu L, Zhang T
Clinical, Cosmetic and Investigational Dermatology 2024, 17:769-782
Published Date: 3 April 2024
Knowledge, Attitudes and Practices Toward Physical Literacy Among the College Students During COVID-19 School Closure
Ma C, Yue M, Zhu X
Journal of Multidisciplinary Healthcare 2024, 17:1629-1640
Published Date: 15 April 2024
Knowledge, Attitude and Practice of Radiologists Regarding Artificial Intelligence in Medical Imaging
Huang W, Li Y, Bao Z, Ye J, Xia W, Lv Y, Lu J, Wang C, Zhu X
Journal of Multidisciplinary Healthcare 2024, 17:3109-3119
Published Date: 4 July 2024
Knowledge, Attitude, and Practice Toward Varicocele in Patients with Varicoceles: A Cross-Sectional Study in Chinese Patients
Gong P, Shen J, Yang Y, Xue D, Lu H, Zhuang Q, Wang X, Tian Z, Chen Y, Chen C, Cao Y
International Journal of General Medicine 2024, 17:3423-3432
Published Date: 7 August 2024
Knowledge, Attitude, and Practice Towards Rehabilitation in Patients with Breast Cancer: A Cross-Sectional Study
Zhou Y, Lu Q, Yu X
Journal of Multidisciplinary Healthcare 2025, 18:1483-1492
Published Date: 12 March 2025