Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Knowledge, Attitudes, and Practices Regarding PCSK9 Inhibitors Among Healthcare Professionals: Exploring Behavioral Pathways and the Intermediary Role of Attitude
Authors Zhao C ![]() , Wang N, Shen D, Zhu L, Chen G
, Wang N, Shen D, Zhu L, Chen G
Received 19 December 2025
Accepted for publication 2 June 2026
Published 8 June 2026 Volume 2026:19 590436
DOI https://doi.org/10.2147/JMDH.S590436
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jagdish Khubchandani
Chao Zhao,1,2 Nuan Wang,2 Dayong Shen,3 Laiyun Zhu,2 Guofang Chen1,4
1Suzhou Medical College of Soochow University, Suzhou, People’s Republic of China; 2Department of Neurology, The Affiliated Xuzhou Municipal Hospital of Xuzhou Medical University, Xuzhou, People’s Republic of China; 3Department of Neurology, The Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China; 4Department of Neurology, Xuzhou Central Hospital, (Clinical Medicine Postgraduate Workstation, Soochow University), Xuzhou, 221009, People’s Republic of China
Correspondence: Guofang Chen, Email [email protected]
Introduction: The aim of the current study was to assess the knowledge, attitudes, and practices (KAP) of healthcare professionals about proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors and to explicitly explore the behavioral pathways linking these domains, focusing on how attitude connects knowledge to clinical practice.
Methods: A cross-sectional study was carried out with a structured, self-complete questionnaire sent to healthcare workers of the Xuzhou area from October 2024 to July 2025. Demographic data of the respondents as well as KAP scores were obtained and compared. Knowledge, attitude, and practice interactions were analyzed with Spearman correlation and structural equation modeling.
Results: 512 usable responses for analysis. The mean scores were 10.05 ± 2.61 for knowledge, 23.78 ± 5.04 for attitude, and 31.71 ± 6.40 for practice. Knowledge, attitude, and practice were positively correlated with each other (P < 0.001). SEM analysis indicated that attitude was a mediator of the relationship between knowledge and practice in a full sense. Knowledge exerted a significant direct influence on attitude (β = 0.873, P < 0.001) and an indirect effect on practice (β = 0.702, P = 0.005), but the direct path from knowledge to practice was not significant statistically (P = 0.124).
Conclusion: Clinical practitioners demonstrated moderate levels of knowledge and self-reported practice regarding PCSK9 inhibitors that were underpinned by a generally positive attitude. Attitude was associated with practice and statistically mediated the knowledge–practice association within the proposed model. Educational activities should therefore aim not only to remedy gaps in knowledge but also to foster professional attitudes for the facilitation of the clinical use of PCSK9 inhibitors.
Keywords: PCSK9 inhibitors, knowledge, attitude, practice, healthcare professionals, structural equation model
Introduction
The emergence of proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors signifies a substantial therapeutic advance in the management of hypercholesterolemia.1–3 These agents employ a novel mechanism that involves selectively inhibiting PCSK9, which enhances the hepatic clearance of low-density lipoprotein cholesterol (LDL-C), and results in profound, sustained reductions in circulating LDL-C levels.4,5 When contrasted with traditional lipid-lowering agents, PCSK9 inhibitors provide superior efficacy through a distinct mode of action, presenting a significant opportunity for high-risk cardiovascular patients worldwide.2,6,7
While statins remain the cornerstone of lipid management, many patients encounter therapeutic challenges, including statin intolerance or failure to reach LDL-C goals despite maximal therapy.8,9 PCSK9 inhibitors address these gaps, proving particularly valuable for patients with familial hypercholesterolemia or those at very high cardiovascular risk.1,10,11 These populations often face a considerable residual risk for cardiovascular disease (CVD), which persists as a primary cause of global mortality and morbidity.8,12 PCSK9 inhibitors offers a targeted pharmacological approach to mitigate this residual cardiovascular risk and improve long-term patient outcomes and quality of life in high-risk individuals.6,10,13
The effective integration of innovative treatments like PCSK9 inhibitors into clinical settings is heavily dependent on the knowledge, attitude, and practice (KAP) of healthcare professionals.14 Healthcare professionals’ understanding and acceptance of new agents directly determine treatment uptake and efficacy. However, being a relatively new class of drugs, the adoption of PCSK9 inhibitors is met with several obstacles, including high costs and insurance coverage issues, insufficient provider familiarity with their complete clinical profile, and relevant regional consensus statements, and challenges related to long-term patient engagement,15–18 with real-world data from China indicating a 12-month adherence rate to PCSK9 monoclonal antibodies of only 31.8%.19 Moreover, the limited applicability of Western-centric guidelines to Asian populations further complicates standardized prescription practices.20 In regional healthcare settings such as Xuzhou, these barriers collectively contribute to a gap between clinical guidelines and actual practice.
The KAP survey model provides a structured framework for evaluating these domains to identify barriers and inform targeted interventions.21 A critical synthesis of recent KAP studies regarding novel drug adoption reveals that knowledge deficits alone do not fully explain clinical inertia; rather, cognitive and affective domains interact in complex ways. Grounded in behavioral implementation frameworks such as the Theory of Planned Behavior, understanding how professional attitudes link objective knowledge to practical implementation is essential for designing effective interventions. To date, while recent surveys have highlighted poor guideline awareness and patient-related adherence barriers in general dyslipidemia management,20 a comprehensive assessment of KAP specifically regarding PCSK9 inhibitors among healthcare providers is limited. More importantly, existing surveys traditionally treat KAP domains as isolated variables, leaving the specific behavioral pathways and interaction mechanisms largely unknown. This conceptual gap restricts the ability to target the precise intermediary factors driving clinical prescribing. Therefore, this study was designed to investigate the KAP of healthcare professionals (including physicians, nurses, pharmacists, and technicians) concerning PCSK9 inhibitors and their clinical use, and, to our knowledge, is one of the first surveys to specifically examine PCSK9 inhibitor-related KAP among healthcare professionals. We deliberately included a diverse multidisciplinary cohort because real-world PCSK9 inhibitor implementation requires collaborative care: prescribers initiate therapy, pharmacists navigate complex authorization and dispensing, nurses conduct essential patient education, and technicians facilitate lipid monitoring. Furthermore, we utilized structural equation modeling (SEM) to quantitatively explore the underlying structural relationships and mediating effects among knowledge, attitude, and practice, offering deeper insights into the specific behavioral pathways driving clinical application compared to standard regression models. By identifying knowledge gaps and elucidating the interplay between KAP domains, this research aims to provide an empirical basis for targeted educational interventions that promote the standardized clinical application of PCSK9 inhibitors.
Materials and Methods
Study Design and Participants
This multicenter, cross-sectional survey was conducted from October 1, 2024, to July 1, 2025, among healthcare professionals in the Xuzhou region. The inclusion criteria were: 1. Age (30–65 years old); 2. Professional category: Medical staff such as cardiologists, endocrinologists, neurologists, and general practitioners who may prescribe PCSK9 inhibitors; 3. Pharmacists (especially clinical pharmacists) or nursing staff (such as specialist nurses); 4. Participated in lipid management for patients with ASCVD (atherosclerotic cardiovascular disease) or familial hypercholesterolemia within the past 1 year; 5. Have prescribed or managed PCSK9 inhibitors (such as Evolocumab, Alirocumab); 6. Voluntarily participated in the survey and signed the informed consent. The target sample size was justified based on SEM requirements, which recommend 10 to 20 cases per observed variable. With 22 observed items in our KAP domains, a minimum sample size of 220 to 440 was required; thus, our final sample of 512 valid questionnaires provided sufficient statistical power.
The Exclusion Criteria Were
1. Non-clinical position medical staff (such as administrative personnel); 2. Without the prescription authority for lipid-lowering drugs or relevant patient management experience (such as only engaged in basic research); 3. Recently (within 3 months) participated in similar investigations to avoid response bias due to repetition; 4. Questionnaire incomplete (such as unanswered key questions) or logically inconsistent (such as “never used PCSK9 inhibitors” but chose “prescribe more than 10 cases per month”). The study protocol was approved by the Ethics Committee of Xuzhou First People’s Hospital, and written informed consent was obtained from all participants before completing the survey.
Questionnaire
The survey instrument was developed based on a review of existing literature and relevant clinical guidelines,15–17 and its content was validated by an expert panel. A pilot test was conducted with a small sample of healthcare professionals to ensure the clarity and appropriateness of the questions. The final Chinese version demonstrated good internal consistency, with a Cronbach’s α coefficient of 0.905. Sampling adequacy was confirmed with Kaiser-Meyer-Olkin (KMO) = 0.956 and significant Bartlett’s test of sphericity (P < 0.001). Besides, a confirmatory factor analysis (CFA) was conducted to validate the measurement model’s factor structure, with fit indices and factor loadings detailed in Supplementary Tables 1–2 and Supplementary Figure 1.
The four components of the survey were:
- Demographic Details: Included questions about gender, age, education, professional designation, department, function, years of practice, type of hospital, and prior research experience.
- Knowledge Domain: Consisted of 8 items assessing experience with PCSK9 inhibitors’ action, indications, and clinical use. These were scored on a 3-point Likert scale (“Very familiar” = 2, “Heard of it” = 1, “Unfamiliar” = 0), with the highest attainable score being 0–16. An attention-check item was embedded in the knowledge domain for data quality control and was excluded from the final knowledge score calculation.
- Attitude Domain: Consisted of 6 items scored on a 5-point Likert scale (“Strongly disagree” = 1 to “Strongly agree” = 5) with scores ranging from 6 to 30.
- Practice Domain: Consisted of 8 items scored on a 5-point Likert scale (“Never” = 1 to “Always” = 5) with scores ranging from 8 to 40. Additionally, several multiple-response questions were included strictly for descriptive baseline profiling; these items were not assigned numerical scores and were excluded from all quantitative domain score calculations and downstream analyses.
The questionnaire was distributed electronically via a QR code generated on the Wenjuanxing platform and shared through WeChat. To ensure data quality, each IP address was limited to one submission, all questions were mandatory, and submissions completed in under 90 seconds were excluded.
Statistical Analysis
SPSS software version 27.0 and AMOS software version 26.0 were used for analysis. Descriptive statistics were used to summarize participant demographics and KAP scores. Continuous variables were presented as mean ± SD, and categorical variables as frequencies and percentages (n, %). Mann–Whitney U and Kruskal–Wallis H one-way nonparametric tests were used to compare scores of KAP between demographic subgroups. Additionally, to evaluate the impact of prior research experience, the Pearson Chi-square test and Mann–Whitney U-test were applied to compare categorical demographic characteristics and continuous KAP scores, respectively, between participants with and without prior involvement in PCSK9 inhibitor-related research. Spearman rank correlation was utilized to examine correlations among total scores of practice, attitude, and knowledge. Binary logistic regression analyses were performed to identify predictors of a higher practice level. For this analysis, the practice score was dichotomized using a strict 80% cutoff of the maximum score,22 where a score >32 designated a higher level of practice and a score ≤32 designated a lower level of practice. A SEM was constructed to test the theorized relationship between practice, attitude, and knowledge. A P-value of <0.05 (two-tailed) was considered statistically significant for all tests.
Results
Demographic Characteristics
514 questionnaires were returned initially. Two questionnaires that took less than 90 seconds to complete were not analyzed. The final sample was 512 valid questionnaires. The majority of participants were female (62.7%) and aged 32 years or younger (59.38%). Physicians were the most represented professional group (42.38%), followed by nurses (29.69%). Subgroup analysis revealed a statistically significant difference in practice score by level of education (P = 0.042) with Master’s degree recipients reporting higher practice scores than those with a Bachelor’s degree or below (Table 1). Furthermore, an additional subgroup analysis revealed no significant differences in Knowledge (P=0.799), Attitude (P=0.858), or Practice (P=0.484) scores between respondents who had previously participated in PCSK9 inhibitor-related research and those who had not. Demographic variables were also highly comparable between these two groups, with the only significant difference observed in Professional Title distribution (P=0.008) (Supplementary Table 3).
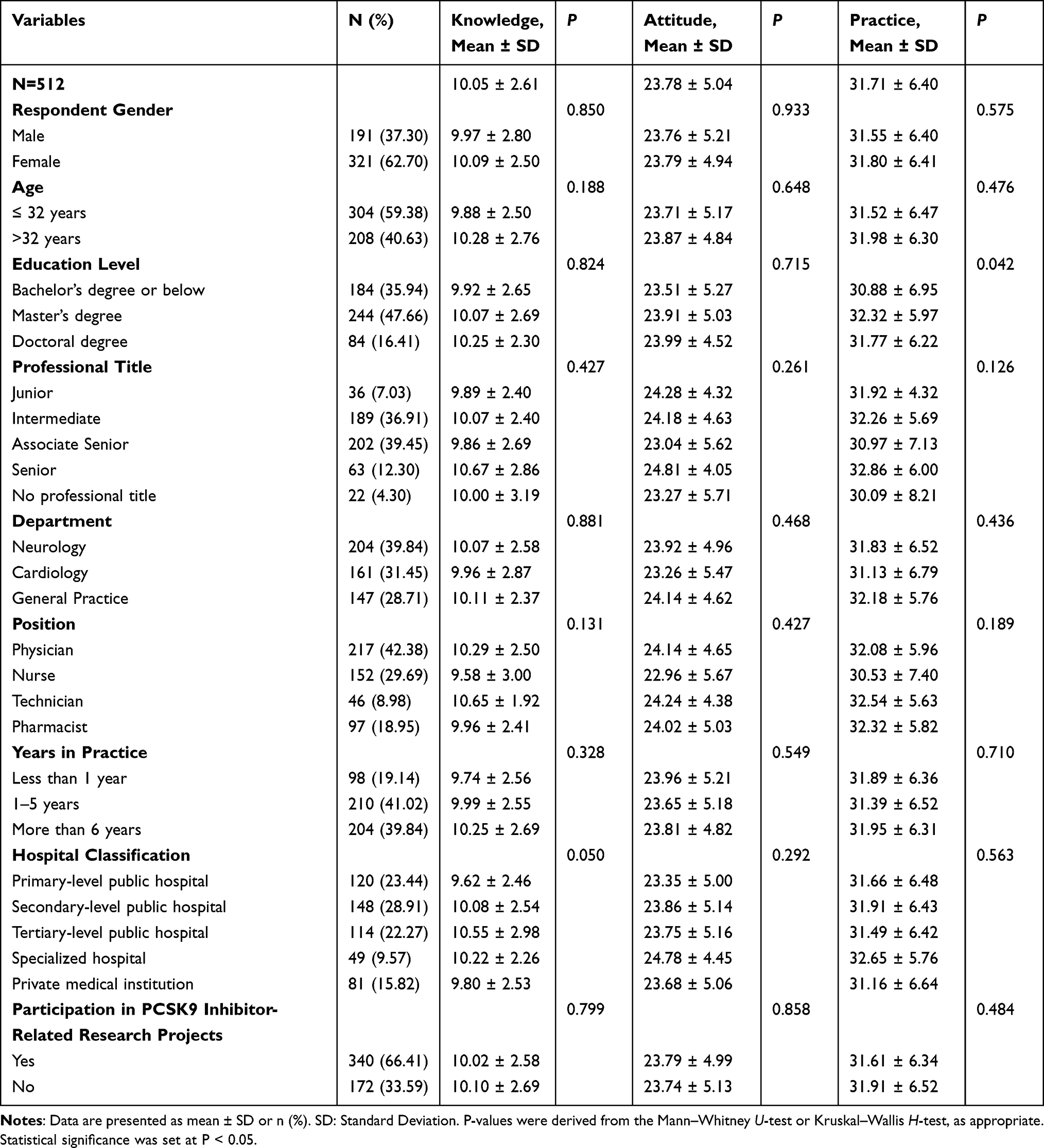 |
Table 1 Baseline Characteristics of Participants and KAP Scores |
KAP Domains
The KAP scores were 10.05 ± 2.61 for knowledge, 23.78 ± 5.04 for attitude, and 31.71 ± 6.40 for practice. For the knowledge domain, a notable trend was observed where for most questions, the highest percentage of respondents selected “Heard of it” as opposed to “Very familiar.”. For example, for mechanism of action, 46.68% were “Heard of it” only. The highest degree of familiarity was regarding general use indication when statins are insufficient (44.53% “Very familiar”). For attitudes, responses indicated a generally positive but cautious perspective. While 71.68% agreed or strongly agreed that professionals had faith in the safety and efficacy of these medicines, many also identified significant barriers. “High cost” was cited by 60.94% as the most important one, and 73.83% agreed or strongly agreed that existing clinical guidelines must be more explicitly defined. This reflects a rational paradox where positive clinical attitudes are tempered by pragmatic and systemic challenges. Within the practice domain, self-reported actions indicated a potential gap between the performance of individual patient tasks and engagement in collaborative, team-based activities. A greated proportion of respondents indicated “Always” performing independent tasks such as actively monitoring for side effects (46.88% “Always”) and checking cholesterol levels at regular intervals (42.38% “Always”). In contrast, collaborative tasks, such as attending to multidisciplinary discussions before initiating therapy, however, were reportedly performed “Always” by a smaller percentage of professionals (41.6%) (Supplementary Table 4).
Spearman Correlation Analysis
Spearman correlation analysis revealed that there were significant positive correlations between all three KAP domains. The strongest correlation was that between attitude and practice (r = 0.571, P < 0.001), followed by knowledge and practice (r = 0.384, P < 0.001), and knowledge and attitude (r = 0.348, P < 0.001) (Table 2).
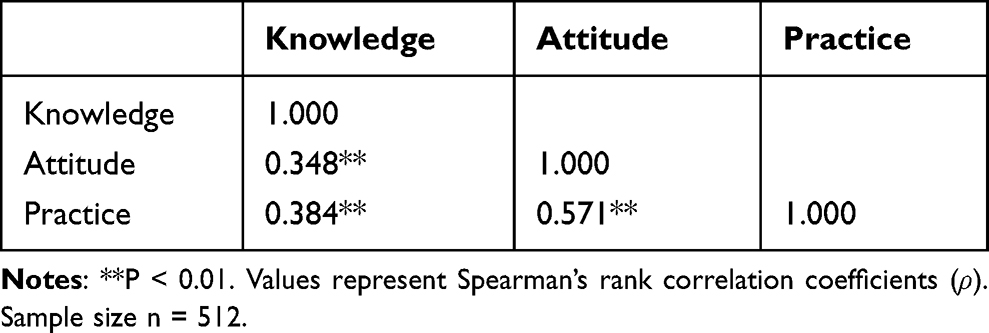 |
Table 2 Spearman Correlation Matrix for KAP Scores |
Multivariate Logistic Regression Analyses
Based on cutoff of 80% of the maximum possible score, 327 participants were classified as having a higher level of practice, whereas 185 were classified as having a lower level of practice. Univariate and multivariate logistic regression analyses found that increased scores for Knowledge (OR = 1.468, P < 0.001) and Attitude (OR = 1.434, P < 0.001) in the univariate analysis were positively associated with the higher level of practice (defined as a score >32). No demographic or professional factors were found to be significant predictors. For the multivariate analysis below, both Attitude and Knowledge scores were significant independent predictors of practice level. Specifically, higher Knowledge score (OR = 1.213, P < 0.001) and positive Attitude score (OR = 1.393, P < 0.001) independently increased the odds of a high practice score (Table 3).
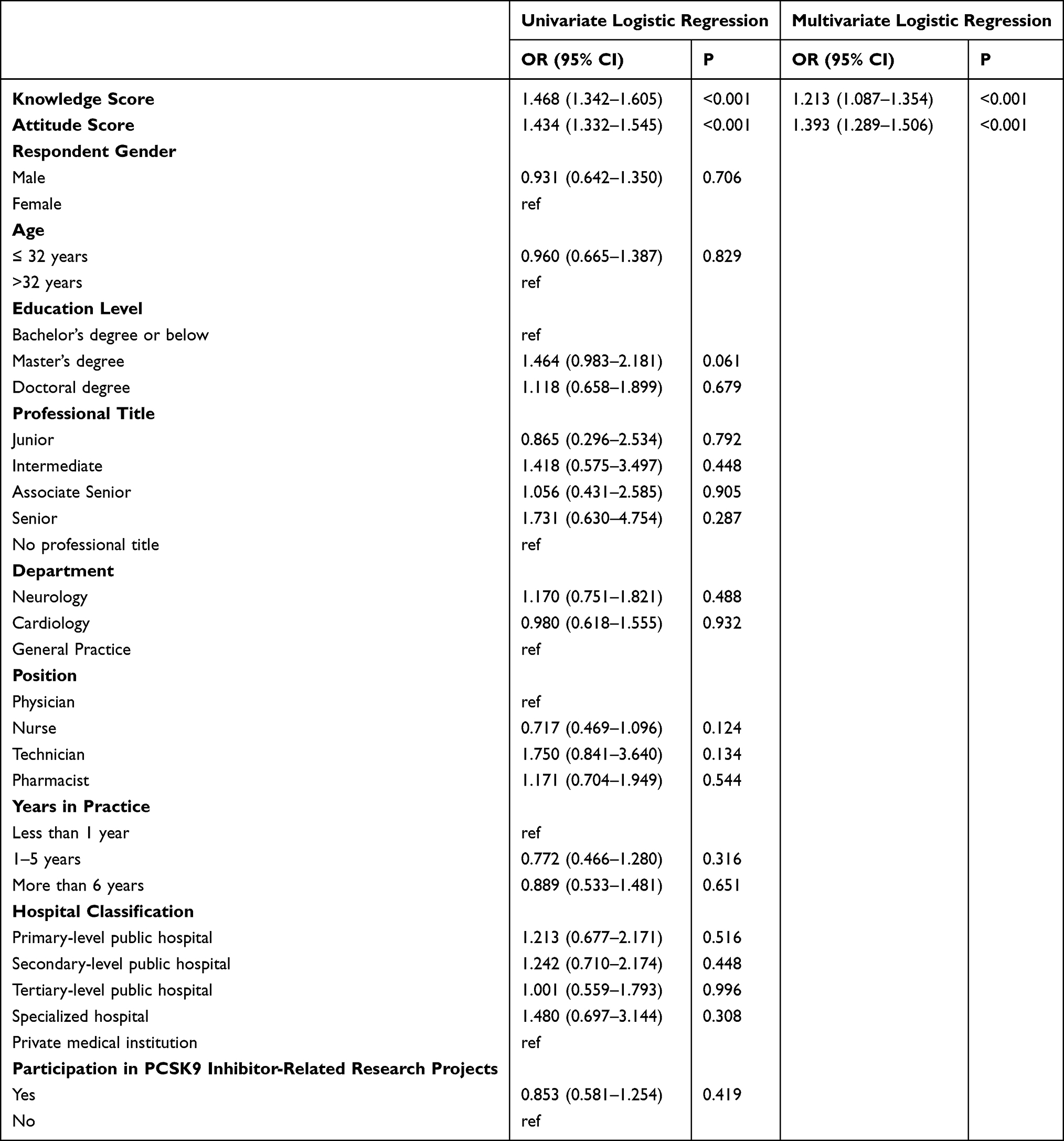 |
Table 3 Univariate and Multivariate Analysis |
Structural Equation Modeling
The fit indices for the proposed SEM, indicated a good fit to the data (CMIN/DF = 1.223, RMSEA = 0.021, CFI = 0.986) (Supplementary Table 5). The standardized path coefficients are shown in. The model indicated that knowledge had a significant positive direct effect on attitude (β = 0.873, P < 0.001). Attitude had a significant positive direct effect on practice (β = 0.803, P < 0.001), whereas knowledge did not. The direct effect from knowledge to practice was not statistically significance (β = 0.212, P = 0.124). However, knowledge had a significant indirect effect on practice through the statistical intermediary role of attitude (Standardized indirect effect β = 0.702, P = 0.005) (Figure 1 and Table 4).
 |
Table 4 Sem |
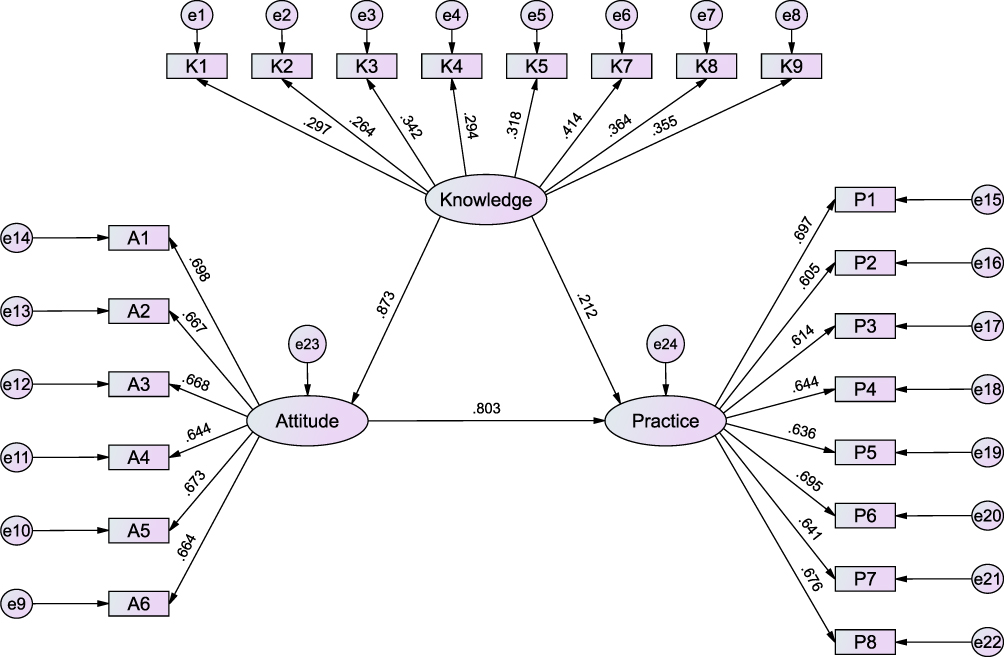 |
Figure 1 Structural Equation Model of Knowledge, Attitude and Practice. |
Discussion
The current research is a systematic analysis of knowledge, attitude, and practice of healthcare professionals toward PCSK9 inhibitors, applying SEM to describe the complex interaction among these constructs. Our main result is that professional attitude might mediate the associations between knowledge and clinical practice, showing that only being knowledgeable is insufficient for fostering its use without the presence of a good professional attitude.
Our results, indicating moderate levels of knowledge with favorable but cautious and pragmatic attitudes, are consistent with existing literature on the uptake of other novel medical therapies.23 That the majority of professionals had only “heard of” salient features of PCSK9 inhibitors is a common pattern seen when a medical innovation is first diffusing. For instance, a study of DOACs knowledge among pharmacists revealed precisely the same knowledge gaps, primarily in terms of dosing modification and monitoring algorithms.24 This suggests a superficial level of awareness rather than in-depth knowledge regarding PCSK9 inhibitors among most respondents. Such limited deep mastery is particularly critical given the substantial vascular benefits of adding high-intensity lipid-lowering therapies like PCSK9 inhibitors in atherosclerotic patients, particularly in promoting vulnerable plaque stabilization and atheroma regression,25 which highlights the urgent need to bridge the gap between clinical efficacy and provider awareness. Likewise, supported by our result that 71.68% of respondents agreed on the safety and efficacy of these agents, clinical effectiveness is highly valued by professionals, although this is tempered by concerns for undue cost. Furthermore, it is important to acknowledge that the uptake of innovative new products is not solely dependent on provider KAP. It is also significantly influenced by the active role of pharmaceutical manufacturers in providing continuing medical education, facilitating patient access programs, and encouraging clinical adoption—external drivers that warrant consideration in real-world settings. A qualitative study examining PCSK9 inhibitor prescribing obstacles in the US identified cost and rigorous insurance authorization processes as the prevailing discouragement to cardiologists, even when believing the drugs were clinically suitable.26,27 This suggests that the tension among perceived clinical value and economic limitation is a system issue insinuating the take-up of expensive, new drugs in many healthcare systems.28,29
Moreover, the extreme positive correlation reported between KAP dimensions and the mediating effect of attitude provide empirical evidence for the theoretical KAP model of new drug adoption. This concurs with findings of a study on antimicrobial stewardship that also highlighted the importance of professional attitude in bringing about the translation of knowledge into appropriate prescribing habits.29,30 Nevertheless, although professional experience has been correlated with improved attitudes and practices in some research, such as the study on the working environment of pediatric nurses,31 our research did not establish a high correlation between years of practice and KAP scores. This could mean that with such a highly specialized and fast-evolving therapy as PCSK9 inhibitors, regular education and CME may prove stronger than just total years of practice.32 Experienced clinicians would become more familiar with habitual statin-driven regimens, while recent trainees would be better tuned into fresh evidence-based guidelines incorporating new drugs.33
Furthermore, it is important to clarify the apparent methodological distinction between our regression and SEM findings. While knowledge emerged as a significant independent predictor of practice in the multivariate logistic regression, its direct path became non-significant within the structural equation model. This occurs because logistic regression evaluates the overall association, whereas SEM partitions these structural pathways. The loss of direct significance in SEM indicates full statistical mediation, suggesting that the impact of knowledge on clinical practice is primarily actualized through the formation of appropriate professional attitudes.
The inference that attitude fully mediates the relationship between knowledge and practice has extremely robust policy and educational intervention implications. Presenting raw facts with traditional didactic methods is unlikely to change clinical practice. What emerges from our study is the need for interventions to also aim at the attitudinal domain, shaping the perception, beliefs, and professional horizon of healthcare professionals. For example, educational programs could move from simple knowledge transfer to more complex, case-based scenarios in which clinicians have to go through the very problems (eg., cost, guideline ambiguity) they had reported were barriers.34 Workshops and continuing education emphasizing the practical value proposition of PCSK9 inhibitors in high-risk patients can prompt a bolder professional response.35 Support from institutions also is critical. Healthcare systems may encourage good attitudes by establishing streamlined prior authorization procedures, clear institutional guidelines, and making decision-support tools within electronic health records available to reduce administrative burdens and inspire prescribing these drugs.36,37
Regarding the demographic profile of our cohort, it is noteworthy that while physicians comprised the largest professional group (42.38%), only 16.41% of the total sample held a doctoral degree. This distribution accurately reflects the current multi-tiered medical education system in China. Unlike healthcare systems where a doctoral degree (M.D. or Ph.D.) is a universal prerequisite for medical practice, the primary pathways for clinical licensure in China are the 5-year bachelor’s program and the “5+3” integrated master’s program. Consequently, doctoral degrees are predominantly pursued by clinician-scientists in elite academic centers, whereas the vast majority of frontline patient care across regional and secondary hospitals is delivered by highly experienced practitioners holding bachelor’s or master’s degrees.38 Therefore, our sample closely aligns with the real-world clinical workforce demographic in regional settings like Xuzhou.
This research has some limitations that have to be stated initially. Firstly, the cross-sectional design prevents the setting up of causal associations, and secondly, self-report questionnaire data may create bias through social desirability and recall bias,39 which may not reflect objective, real-world prescribing behaviors; thirdly, the regional convenience sampling from one area in China (Xuzhou) restricts generalizability to actual prescribers in other healthcare systems or cultures;40 fourthly, multi-center cross-validation of the questionnaire remains incomplete, and quantitative assessments of content validity, such as a Content Validity Index (CVI), were not formally performed prior to implementation.
Conclusion
Our regional, cross-sectional study demonstrates that knowledge, attitudes, and self-reported practices regarding PCSK9 inhibitors were positively associated among healthcare workers in the Xuzhou area, with attitude showing a statistically important intermediary role in the proposed SEM. Rather than acting as a definitive causal factor, appropriate professional attitude serves as a vital statistical link between knowledge and self-reported actions. Future initiatives to make optimal use of these potent lipid-lowering drugs need to adopt a twofold approach, which not only disseminates technical knowledge but also establishes desirable professional mindsets and transcends perceived barriers to care.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Review Committee of the First People’s Hospital of Xuzhou City (xyyl1[2024]073), I confirm that all methods were performed in accordance with the relevant guidelines. All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments, and informed consent was obtained from all participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Affiliated Hospital of Xuzhou Medical University (XYFY202316). The funding bodies had no role in the design of the study, the collection, analysis, and interpretation of data, and the writing of the manuscript.
Disclosure
All authors declare that they have no conflicts of interest in this work.
References
1. Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk: the task force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur Heart J. 2019;41(1):111–11.
2. Chaudhary R, Garg J, Shah N, Sumner A. PCSK9 inhibitors: a new era of lipid lowering therapy. World J Cardiol. 2017;9(2):76–91. doi:10.4330/wjc.v9.i2.76
3. Rosenson RS, Hegele RA, Fazio S, Cannon CP. The evolving future of PCSK9 inhibitors. J Am College Cardiol. 2018;72(3):314–329. doi:10.1016/j.jacc.2018.04.054
4. Jeswani BM, Sharma S, Rathore SS, Nazir A, Bhatheja R, Kapoor K. PCSK9 inhibitors: the evolving future. Health Sci Rep. 2024;7(11):e70174. doi:10.1002/hsr2.70174
5. Warden BA, Fazio S, Shapiro MD. The PCSK9 revolution: current status, controversies, and future directions. Trend Cardiovasc Med. 2020;30(3):179–185. doi:10.1016/j.tcm.2019.05.007
6. Guedeney P, Giustino G, Sorrentino S, et al. Efficacy and safety of alirocumab and evolocumab: a systematic review and meta-analysis of randomized controlled trials. Eur Heart J. 2022;43(7):e17–e25. doi:10.1093/eurheartj/ehz430
7. Sabatine MS, Giugliano RP, Keech AC, et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. 2017;376(18):1713–1722. doi:10.1056/NEJMoa1615664
8. Bytyçi I, Penson PE, Mikhailidis DP, et al. Prevalence of statin intolerance: a meta-analysis. Eur Heart J. 2022;43(34):3213–3223. doi:10.1093/eurheartj/ehac015
9. Qian LJ, Gao Y, Zhang YM, Chu M, Yao J, Xu D. Therapeutic efficacy and safety of PCSK9-monoclonal antibodies on familial hypercholesterolemia and statin-intolerant patients: a meta-analysis of 15 randomized controlled trials. Sci Rep. 2017;7(1):238. doi:10.1038/s41598-017-00316-3
10. Auer J, Berent R. Alirocumab as add-on therapy to statins: current evidence and clinical potential. Ther Adv Cardiovasc Dis. 2018;12(7):191–202.
11. Raal FJ, Hovingh GK, Catapano AL. Familial hypercholesterolemia treatments: guidelines and new therapies. Atherosclerosis. 2018;277:483–492. doi:10.1016/j.atherosclerosis.2018.06.859
12. Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–1222.
13. Durairaj A, Sabates A, Nieves J, Moraes B, Baum S. Proprotein convertase subtilisin/kexin type 9 (PCSK9) and its inhibitors: a review of physiology, biology, and clinical data. Curr Treat Options Cardiovasc Med. 2017;19(8):58.
14. Ajzen I. The theory of planned behaviour. Organizat Behav Human Decis Proc. 1991;50(2):179–211.
15. Altschmiedová T, Todorovová V, Šnejdrlová M, Šatný M, Češka R. PCSK9 inhibitors in real-world practice: analysis of data from 314 patients and 2 years of experience in a center of preventive cardiology. Curr Atheroscler Rep. 2022;24(5):357–363. doi:10.1007/s11883-022-01008-8
16. Ye X, Zhang S, Zhong X, et al. Real-World assessment of the association between PCSK9i adherence and LDL reduction and variability in a Chinese clinical practice. Clin Epidemiol. 2025;17:537–546. doi:10.2147/CLEP.S507761
17. Nguy J, Hitchen SA, Lan NS, et al. Barriers to prescribing proprotein convertase subtilisin‐kexin type 9 inhibitors after coronary revascularisation. Internal Med J. 2023;53(6):994–1001. doi:10.1111/imj.15700
18. Gallego-Colon E, Daum A, Yosefy C. Statins and PCSK9 inhibitors: a new lipid-lowering therapy. Eur J Pharmacol. 2020;878:173114. doi:10.1016/j.ejphar.2020.173114
19. Zheng X, Jin Y, Fan M, Cui H, Zhu S. Multilevel factors predict medication adherence and efficacy within 12 months in patients receiving PCSK9 monoclonal antibodies: the findings from a real-world analysis in China. J Atheroscler Thromb. 2025;32(11):1375–1389. doi:10.5551/jat.65624
20. Bhandari R, Ganachari M. Patient and healthcare professional perspective on challenges in lipid profile management in dyslipidemia patients: two separate cross-sectional surveys. J Appl Pharmaceut Sci. 2024;14(12):180–186.
21. Launiala A. How much can a KAP survey tell us about people’s knowledge, attitudes and practices? Some observations from medical anthropology research on malaria in pregnancy in Malawi. Anthropol Matters. 2009;11(1).
22. Phuyal P, Kramer IM, Kuch U, et al. The knowledge, attitude and practice of community people on dengue fever in Central Nepal: a cross-sectional study. BMC Infect Dis. 2022;22(1):454. doi:10.1186/s12879-022-07404-4
23. Dearing JW, Cox JG. Diffusion of innovations theory, principles, and practice. Health Affairs. 2018;37(2):183–190. doi:10.1377/hlthaff.2017.1104
24. Vakili Z, Heydarpour F, Shahbazi F. Survey of knowledge and attitude of pharmacists about direct oral anticoagulants: a Cross-Sectional Study. J Pharm Care. 2021. doi:10.18502/jpc.v9i3.7369
25. Biccirè FG, Gatto L, La Porta Y, Pignatelli P, Prati F, Pastori D. Effects of lipid lowering therapies on vulnerable plaque features: an updated narrative review of the literature. J Cardiovasc Dev Dis. 2023;10(6). doi:10.3390/jcdd10060260
26. Cohen JD, Cziraky MJ, Jacobson TA, Maki KC, Karalis DG. Barriers to PCSK9 inhibitor prescriptions for patients with high cardiovascular risk: results of a healthcare provider survey conducted by the National Lipid Association. J Clin Lipidol. 2017;11(4):891–900. doi:10.1016/j.jacl.2017.04.120
27. Doshi JA, Li P, Puckett JT, et al. Trends and factors associated with insurer approval of proprotein convertase subtilisin/kexin type 9 inhibitor prescriptions. Value Health. 2020;23(2):209–216. doi:10.1016/j.jval.2019.08.011
28. Kazi DS, Moran AE, Coxson PG, et al. Cost-effectiveness of PCSK9 inhibitor therapy in patients with heterozygous familial hypercholesterolemia or atherosclerotic cardiovascular disease. JAMA. 2016;316(7):743–753. doi:10.1001/jama.2016.11004
29. Mercep I, Strikic D, Hrabac P, Pecin I, Reiner Ž. PCSK9 inhibition: from effectiveness to cost-effectiveness. Front Cardiovascul Med. 2024;11:1339487. doi:10.3389/fcvm.2024.1339487
30. Musoke D, Lubega GB, Obeng MB, et al. Knowledge, perceptions and practices on antimicrobial resistance in humans and animals in Wakiso district, Uganda: a cross sectional study. PLOS Glob Public Health. 2023;3(12):e0002701. doi:10.1371/journal.pgph.0002701
31. Buckley L, Berta W, Cleverley K, Widger K. The relationships amongst pediatric nurses’ work environments, work attitudes, and experiences of burnout. Front Pediatr. 2021;9:807245. doi:10.3389/fped.2021.807245
32. Cervero RM, Gaines JK. The impact of CME on physician performance and patient health outcomes: an updated synthesis of systematic reviews. J Contin Educ Health Prof. 2015;35(2):131–138. doi:10.1002/chp.21290
33. Dixon DL, Sharma G, Sandesara PB, et al. Therapeutic inertia in cardiovascular disease prevention: time to move the bar. J Am College Cardiol. 2019;74(13):1728–1731. doi:10.1016/j.jacc.2019.08.014
34. Fromke EJ, Jordan SG, Awan OA. Case-based learning: its importance in medical student education. Acad Radiol. 2022;29(8):1284–1286. doi:10.1016/j.acra.2021.09.028
35. Forsetlund L, Bjørndal A, Rashidian A, et al. Continuing education meetings and workshops: effects on professional practice and health care outcomes. Cochrane Database Syst Rev. 2009;2009(2):Cd003030. doi:10.1002/14651858.CD003030.pub2
36. Corrigan-Curay J, Sacks L, Woodcock J. Real-world evidence and real-world data for evaluating drug safety and effectiveness. JAMA. 2018;320(9):867–868. doi:10.1001/jama.2018.10136
37. Irwin R, Stokes T, Marshall T. Practice-level quality improvement interventions in primary care: a review of systematic reviews. Primary Health Care Res Develop. 2015;16(6):556–577. doi:10.1017/S1463423615000274
38. Ling T, Shen Y, Zhang Y, Tang J, Zhao E. Medical education reform in China in the 21st century: a literature review. Adv Med Educ Pract. 2024;15:1313–1324. doi:10.2147/AMEP.S489903
39. Althubaiti A. Information bias in health research: definition, pitfalls, and adjustment methods. J Multidiscip Healthc. 2016;211–217. doi:10.2147/JMDH.S104807
40. Tsang S, Royse CF, Terkawi AS. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi Anaesthesia. 2017;11(Suppl 1):S80–S89. doi:10.4103/sja.SJA_203_17
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Managing Pain in Low Resource Settings: Healthcare Professionals’ Knowledge, Attitude and Practice Regarding Pain Management in Western Nepal
Thapa P, KC B, Lee SWH, Dujaili JA, Gyawali S, Mohamed Ibrahim MI, Alrasheedy AA
Journal of Pain Research 2022, 15:1587-1599
Published Date: 2 June 2022
Knowledge, Attitudes, and Practices Regarding Ergonomic Hazards Among Healthcare Workers in a Saudi Government Hospital

ALHazim SS, Al-Otaibi ST, Herzallah NH
Journal of Multidisciplinary Healthcare 2022, 15:1771-1778
Published Date: 24 August 2022
Self-Medication Prevalence and Factors Associated with Knowledge and Attitude Towards Self-Medication Among Undergraduate Health Science Students at GAMBY Medical and Business College, Bahir Dar, Ethiopia
Siraj EA, Yayehrad AT, Kassaw AT, Kassahun D, Solomon E, Abdela H, Gizachew G, Awoke E
Patient Preference and Adherence 2022, 16:3157-3172
Published Date: 5 December 2022
Dermatologists’ Knowledge, Attitude, and Practice Pattern Toward Low-Dose Oral Minoxidil in Hair Loss in Saudi Arabia
Altalhab S
Clinical, Cosmetic and Investigational Dermatology 2024, 17:653-662
Published Date: 15 March 2024
Knowledge, Attitude, and Practice Toward Breast Reconstruction Among Breast Surgery Healthcare Professionals in China
Duan Q, Sun M, Kong D, Liu J, Liu B, Li K
Journal of Multidisciplinary Healthcare 2025, 18:5701-5712
Published Date: 11 September 2025