Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Knowledge, Attitudes, and Practices of Elderly Diabetic Patients and Their Families Regarding Comorbid Non-Alcoholic Fatty Liver Disease: A Structural Equation Modeling Analysis
Authors Wang Q, Zhang Y, Guo X, Zhao L
Received 20 May 2025
Accepted for publication 19 September 2025
Published 15 October 2025 Volume 2025:18 Pages 3833—3844
DOI https://doi.org/10.2147/DMSO.S541709
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Jae Woong Sull
Qian Wang,* Yingze Zhang,* Xinmiao Guo, Lin Zhao
Department of Endocrinology, Guang’anmen Hospital (Baoding) China Academy of Chinese Medical Sciences, Baoding, Hebei, 071000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qian Wang, Email [email protected]
Background: To explore the knowledge, attitudes, and practices (KAP) concerning non-alcoholic fatty liver disease (NAFLD) among elderly diabetic patients and their families.
Methods: A cross-sectional survey was conducted in the outpatient and inpatient units of the Endocrinology Department at Baoding First Hospital of Traditional Chinese Medicine between September, 2023, and March, 2024. Data and KAP scores were collected using a self-designed questionnaires.
Results: The survey yielded 511 valid responses. Of these respondents, 361 (70.65%) were patients, and 177 (34.64%) were diagnosed with NAFLD. The mean scores for knowledge, attitudes, and practices among patients were 5.20 ± 3.37, 37.98 ± 3.96, and 41.85 ± 5.92, respectively, while the scores among patients’ family members were 6.42 ± 4.22, 37.72 ± 4.46, and 41.31 ± 7.02, respectively. Structural equation modeling (SEM) demonstrated significant direct and indirect influences on knowledge, attitude, and practice. Education level (β = 0.71, P < 0.001) were direct determinants of knowledge. Directly, knowledge (β = 0.42, P < 0.001), use of antidiabetic medications (β = − 1.8, P < 0.001), and body mass index (BMI) (β = 0.11, P = 0.011) influenced attitude, while knowledge (β = 0.33, P < 0.001), attitude (β = 0.64, P < 0.001), and NAFLD (β = − 1.2, P < 0.001) affected practice. Indirectly, education level (β = 0.30, P < 0.001) influenced attitude; education level (β = 0.43, P < 0.001), BMI (β = 0.07, P = 0.013), and use of antidiabetic medications (β = − 1.1, P = 0.001) impacted practice.
Conclusion: Despite elderly diabetic patients and their families showing a general lack of in-depth knowledge about NAFLD, they exhibit positive attitudes and proactive practices toward managing the condition. Healthcare providers should focus on enhancing educational interventions targeted at this demographic to improve knowledge, which is crucial for sustaining positive attitudes and effective practices in NAFLD management.
Keywords: knowledge, attitude, practice, non-alcoholic fatty liver disease, diabetes, cross-sectional study
Background
Diabetes patients frequently experience dysregulated lipid metabolism, characterized by increased levels of plasma triglycerides and low-density lipoproteins.1 The deposition of these abnormal lipid metabolites in the liver intensifies hepatic fat accumulation, thereby accelerating the onset and progression of non-alcoholic fatty liver disease (NAFLD).2 There is a strong correlation between the development of NAFLD and diabetes.3 Insulin resistance (IR), commonly observed in diabetic individuals, significantly contributes to this association, with diabetic patients exhibiting a 4.7-fold higher prevalence of NAFLD compared to their non-diabetic counterparts.4 Furthermore, while the prevalence of NAFLD in the general population stands at 33.7%, this figure rises dramatically to 74.9% among subjects with diabetes.5,6 NAFLD and type 2 diabetes mellitus (T2DM) often coexist and synergistically interact, thereby escalating the risk of adverse clinical outcomes, both hepatic and extra-hepatic. Notably, T2DM is also one of the most significant risk factors for the rapid progression of NAFLD to non-alcoholic steatohepatitis, advanced fibrosis, or cirrhosis.7
The Knowledge-Attitude-Practice (KAP) model, foundational to health literacy, is essential in shaping human health behaviors.8 Previous studies have indicated that patients with NAFLD often show gaps in disease knowledge and encounter significant barriers in implementing health behavior changes, despite awareness of the importance of lifestyle modifications.9 This model operates on the principle that improved knowledge positively influences attitudes, which in turn, dictate individual practices.10 In the healthcare domain, the KAP model is frequently utilized along with a tailored questionnaire to thoroughly assess the knowledge, attitudes, and practices of a targeted population, also evaluating their demand and acceptance of pertinent information.11 This study focuses on the KAP concerning NAFLD among elderly diabetic patients and their families. Aging populations and the soaring prevalence of diabetes mellitus12,13 coupled with evidence that older patients with NAFLD are at a higher risk of developing advanced fibrosis than their younger counterparts,14 underscore the urgency and significance of this research. Additionally, in Chinese societies, elderly care predominantly provided by family members,15 amplifies the complexity and health risks due to the interplay of age and chronic diseases. Understanding and enhancing this group’s awareness of NAFLD can lead to more effective disease management and preventive measures, reducing complications and improving quality of life. Furthermore, since family members play a crucial role in the daily health management of patients, examining their attitudes and behaviors is critical. This not only enhances health outcomes for the individuals but also provides healthcare providers with data to design targeted and culturally sensitive interventions. Therefore, this study aims to explore the KAP regarding NAFLD among elderly diabetic patients and their families, and to identify factors influencing these KAP dimensions.
Methods
Study Design and Participants
This cross-sectional study was conducted from September 2023 to March 2024, at the outpatient and inpatient units of the Endocrinology Department at Baoding First Hospital of Traditional Chinese Medicine. Inclusion Criteria: 1) Patients with a medical record of T2DM and their family members. 2) Patients aged 55 to 80 years and family members aged 18 to 80 years. 3) Participants who were conscious, verbally responsive, and free from cognitive or communicative impairments. 4) Individuals capable of independent behavior and comprehension of the questionnaire. 5) Participants who willingly volunteered, cooperated with survey procedures, and provided informed consent. Exclusion Criteria: 1) Patients under severe stress, those who had recently undergone surgery, or were experiencing acute complications of diabetes that prevented them from completing the questionnaire. 2) Patients suffering from severe acute illnesses or in the acute exacerbation phase of chronic conditions, including diseases of the heart, liver, lungs, or kidneys. 3) Individuals with severe cognitive impairments, mental disorders, a history of substance abuse or alcoholism, or those facing significant communication challenges. 4) Participants who were unwilling or unable to cooperate with the study protocols. Dropout and Removal Criteria: 1) Individuals incorrectly included who did not meet the set inclusion criteria. 2) Patients or family members who were non-cooperative or unable to complete the questionnaire as required. 3) Questionnaires that were incomplete or filled out inaccurately without honest responses.
Ethical approval was granted by the Medical Ethics Committee of Baoding First Hospital of Traditional Chinese Medicine (bdsdyzyy-IRB-20230825-001), and all participants provided written informed consent before inclusion in the study.
Questionnaire
The design of the questionnaire was informed by the “Expert Consensus on the Management of NAFLD in Chinese Adults with Type 2 Diabetes” (2021). Initially drafted with input from this guideline, the questionnaire underwent revisions based on feedback from three experts. Following these modifications, it was piloted with a small sample of 40 participants, yielding 33 valid responses for final analysis. The reliability of the questionnaire was confirmed by a Cronbach’s α coefficient of 0.889, indicating good internal consistency.
The final version of the questionnaire, written in Chinese, consisted of four dimensions, encompassing a total of 44 items: 16 items collected basic information, while the knowledge, attitude, and practice dimensions comprised 9, 9, and 10 items respectively. Among the basic variables, “tumor status” referred to any self-reported history of malignant or benign tumors. “Daily alcohol consumption” was defined as the average self-reported intake in milliliters per day, without distinguishing beverage type, and “ever consumed more than 2500 mL of alcohol in total” described estimated lifetime intake among former drinkers. Scoring for the knowledge dimension allowed respondents to self-rate as “very knowledgeable” (2 points), “heard of it” (1 point), or “not clear” (0 points), yielding a potential score range from 0 to 18 points. Both the attitude and practice dimensions employed a five-point Likert scale, with options ranging from very positive (5 points) to very negative (1 point). The scoring for the attitude dimension was straightforward for items 1–5 and 7–9; however, item 6 was scored inversely to capture differing perceptions. The practice dimension followed a direct scoring approach, and included 9 items, with a total possible score ranging from 9 to 45 points. The final questionnaire was in Chinese (a version translated into English was attached as an Appendix). To further clarify the scoring implications, the knowledge dimension defined scores of 0–10 as indicating insufficient knowledge and 11–18 as sufficient. For the attitude dimension, scores of 9–22 represented a negative attitude, 23–32 a neutral attitude, and 33–45 a positive attitude. In the practice dimension, scores were categorized into negative practice behavior (10–25), moderate practice behavior (26–35), and positive practice behavior (36–50).
Data Collection and Quality Control
From September 2023 to March 2024, questionnaires were collected one-on-one by trained members of the research team, which included the principal investigator and two research assistants. These were distributed to patients or their family members who met the inclusion criteria. Participants were provided with standardized explanations and detailed instructions for completing the questionnaires, facilitating face-to-face collection to immediately address any questions or uncertainties. For those patients who were unable to complete the questionnaire independently due to illiteracy or poor vision, researchers filled out the questionnaires based on the patients’ verbal responses. Laboratory and functional test results were meticulously recorded from participants’ examination reports, and the completed questionnaires were collected on-site. To protect participants’ privacy, all data were anonymized, and personal identifiers were removed prior to analysis. To ensure the authenticity, rigor, and scientific integrity of the data, the entire process was meticulously managed by the uniformly trained research team under strict quality control measures.
Statistical Analysis
Data analysis was conducted using SPSS 22.0 (IBM, Armonk, NY, USA). The reliability of the questionnaire was confirmed with a Cronbach’s alpha of 0.826. Descriptive analysis included demographic data and KAP scores, with continuous variables expressed as Mean ± SD and categorical variables as n(%). For continuous variables, normally distributed data were compared between two groups using the t-test and among three or more groups using ANOVA with homogeneity of variance assumed. For data not conforming to a normal distribution, the Mann–Whitney U-test was applied for comparisons between two groups. Pearson correlation analysis assessed relationships between knowledge, attitude, and practice dimensions. The Pearson correlation coefficient, ranging from −1 to +1, indicates the strength and direction of correlations. Structural equation modeling (SEM) was performed using Amos 26.0 to examine direct and indirect effects of demographic and clinical factors on knowledge, attitude, and practice.16,17 Based on the KAP model framework, knowledge, attitude, and practice were defined as latent variables, each measured by corresponding questionnaire items. Observed variables included age, education level, body mass index (BMI), diabetes medication use, and NAFLD status. An initial model was constructed, and non-significant paths were removed to obtain the final adjusted model. Model fit was evaluated using the root mean square error of approximation (RMSEA), standardized root mean square residual (SRMR), comparative fit index (CFI), and Tucker-Lewis index (TLI). Variables included in the path analysis model were selected based on theoretical rationale and supported by observed associations, rather than solely relying on statistical significance, to avoid potential double testing. An adjusted model was then constructed after removing non-contributory paths. All analyses were two-sided, with P values less than 0.05 regarded as statistically significant.
Results
Basic Characteristics
In this study, we initially collected 519 samples. Exclusions were made for samples under specific conditions: one participant declined to answer, and eight participants completed the survey in less than 90 seconds. Consequently, the analysis proceeded with 511 valid samples, yielding an effective response rate of 98.46%. The participants’ mean age was 55.52 ± 14.73 years, and the mean BMI was 25.81 ± 3.86 kg/m². Of these participants, 361 (70.65%) were patients, and 165 (32.29%) had received a junior high school level education. Currently, 107 (20.94%) participants were smokers, with 35 (32.71%) of them smoking more than 20 cigarettes per day. Additionally, 72 (14.09%) participants reported current alcohol consumption, with 46 (63.89%) consuming less than 100mL per day. A total of 302 (59.10%) participants reported having underlying or chronic diseases; 177 (34.64%) were diagnosed with NAFLD, and 443 (86.69%) were on medication for diabetes.
KAP Scores and Related Factors
The mean scores for knowledge, attitudes, and practices were 5.56 ± 3.68, 37.91 ± 4.12, and 41.70 ± 6.26, respectively. Participants’ knowledge scores were more likely to vary depending on: who they are (patient or patient’s family member) (P = 0.001), education level (P < 0.001), type of residence (P < 0.001), employment status (P < 0.001), hypertension status (P < 0.001), tumors status (P = 0.003), and NAFLD status (P < 0.001). Meanwhile, their attitude scores were more likely to vary across daily alcohol consumption (P = 0.013), hyperlipidemia status (P = 0.019), tumors status (P = 0.016), NAFLD status (P < 0.001), and medication status (P = 0.001). Furthermore, their practice scores were more likely to vary depending on: type of residence (P = 0.019), smoke status (P = 0.007), whether ever consumed more than 2500mL of alcohol in total (P = 0.003), daily alcohol consumption (P = 0.044), tumors status (P = 0.025), NAFLD status (P < 0.001), and medication status (P = 0.005) (Table 1).
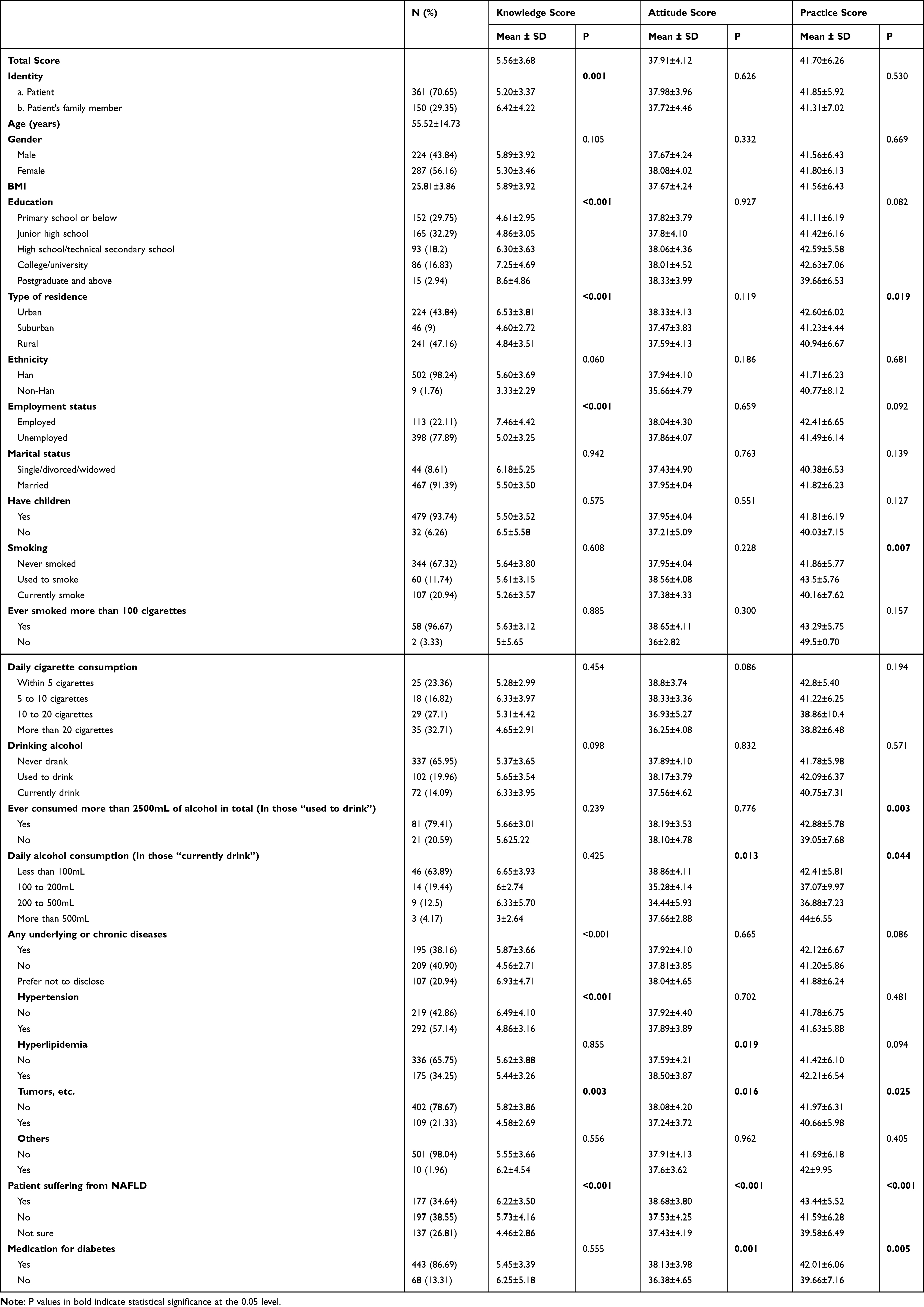 |
Table 1 Demographic Characteristics and KAP Scores |
The distribution of knowledge dimensions shown that the three questions with the highest number of participants choosing the “Unclear” option were (K8) with 85.13%, “For T2DM patients with combined NAFLD, empagliflozin is recommended for liver disease treatment.” (K6) with 81.02%, and “Ultrasound (US) is a common diagnostic method for detecting NAFLD.” (K7) with 53.82% (Table S1).
Responses to the attitude dimension showed that participants’ attitudes were positive, with more than 90% choosing “strongly agree” or “agree”, except for A6, where 23.29% felt very anxious and very worried about combining NAFLD and also 24.27% felt anxious and worried about it (Table S2). When it comes to related practices, 25.24% sometimes and 12.52% rarely would (urge patients to) cooperate with weight loss (P9), 21.53% sometimes and 5.28% rarely would (urge patients to) actively monitor the NAFLD status of older patients with diabetes (P2) (Table S3).
Correlation Analysis of KAP Dimensions
Correlation analysis indicated significant positive correlations between knowledge and attitude (r = 0.3622, P < 0.001), as well as practice (r = 0.4227, P < 0.001), and between attitude and practice (r = 0.5091, P < 0.001) (Table 2).
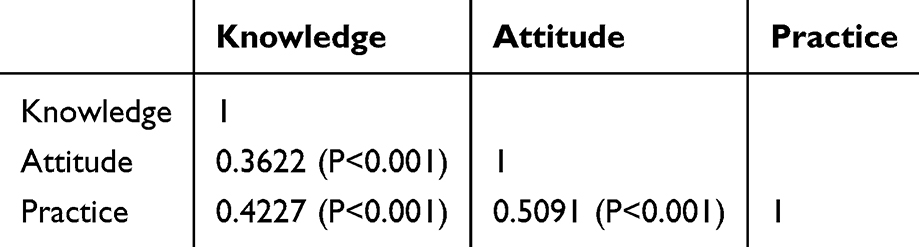 |
Table 2 Correlation Analysis |
SEM Analysis
The adjusted SEM (The unadjusted SEM were showed in Tables S4 and S5) achieved a good fit with an RMSEA value of 0.062, SRMR value of 0.045, TLI value of 0.904, and CFI value of 0.947 (Table 3). Path coefficient analysis revealed that education level (β = 0.71, P < 0.001) and age (β = 0.03, P = 0.009) directly influenced knowledge. Knowledge (β = 0.42, P < 0.001), use of antidiabetic medications (β = −1.8, P < 0.001), and BMI (β = 0.11, P = 0.011) directly influenced attitude. Knowledge (β = 0.33, P < 0.001), attitude (β = 0.64, P < 0.001), and NAFLD (β = −1.2, P < 0.001) directly affected practice.
 |
Table 3 Fit Indices for Adjusted SEM (Excluding Variables with No Statistical Significance from the First Round of SEM) |
Additionally, the mediation analysis based on the adjusted SEM showed that education level (β = 0.30, P < 0.001) and age (β = 0, P = 0.011) indirectly influenced attitude. Knowledge (β = 0.27, P < 0.001), use of antidiabetic medications (β = −1.1, P = 0.001), education level (β = 0.43, P < 0.001), age (β = 0, P = 0.012), and BMI (β = 0.07, P = 0.013) also indirectly affected practice (Tables 4, 5 and Figure 1). Higher education level was associated with better knowledge, which in turn predicted more favorable attitudes and behaviors. Similarly, knowledge and attitude served as mediators between demographic factors and practice.
 |
Table 4 Total Path Coefficients for Adjusted SEM |
 |
Table 5 Mediation Analysis Based on the Adjusted SEM |
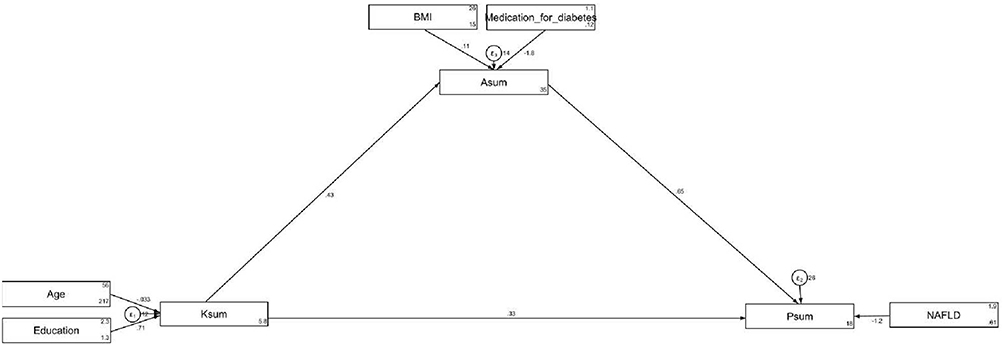 |
Figure 1 Adjusted SEM Path. |
Discussion
The study reveals that elderly diabetic patients and their families generally possess inadequate knowledge of NAFLD, yet exhibit positive attitudes and proactive practices toward managing the disease. Enhancing educational interventions to improve the knowledge of NAFLD among elderly diabetic patients and their families could potentially strengthen their already positive attitudes and proactive practices, thereby improving health outcomes. These findings highlight the importance of separately investigating patients and their family members, as their knowledge levels and roles in disease management differ significantly.
Surprisingly, no significant differences in attitudes were observed, potentially due to a uniform perception or collective familial response to managing the disease.18,19 The findings of this study underscore significant relationships between KAP concerning NAFLD among elderly diabetic patients and their families. Correlation analysis revealed a positive association between knowledge and attitudes, as well as between knowledge and practices. These correlations were further supported by the structural equation model, which confirmed that knowledge significantly influenced both attitudes and practices, while attitude itself acted as a strong mediator toward behavioral outcomes. Additionally, demographic and clinical factors—such as age, education level, NAFLD status, BMI, and medication use—exerted direct or indirect effects on the KAP dimensions through these pathways. Literature supports the interdependence of these elements, suggesting that improved knowledge can lead to better attitudes and more proactive health practices.20,21 The direct impact of knowledge on attitude, and the combined effect of knowledge and attitude on practice, underline the potential benefits of educational interventions. Furthermore, SEM revealed that knowledge and attitude served as key mediators in transmitting the effects of demographic characteristics—particularly age and education—onto health practices. Particularly, knowledge acts as a crucial mediator in improving attitudes towards NAFLD management, even as negative effects from use of antidiabetic medications suggest complexities in patient medication experiences impacting their attitudes. Age directly influenced knowledge, with older patients typically having less familiarity with specific health conditions, possibly due to cognitive decline or less exposure to newer health education methods.22
BMI directly influenced attitudes minimally and had a negligible indirect effect on practices. This modest impact suggests that while physical health status affects how individuals feel about their health, it does not significantly alter their health practices in a chronic care context, possibly due to established routines. This finding aligns with literature indicating that urban residents often have better access to health information and services, which can enhance both knowledge and the ability to apply it in daily practices.23,24 The lack of significant differences in attitudes could be due to a universal value placed on health irrespective of geographic location.
Employed individuals showed higher knowledge and practice scores, which SEM supported. Employment may correlate with better health literacy and active engagement in health-promoting behaviors due to socioeconomic stability and access to resources like workplace wellness programs.25,26 This could indicate that while negative health behaviors correlate with poorer health practices, they do not necessarily alter personal attitudes toward disease management, which might be more strongly influenced by intrinsic values and overall health awareness.
The distribution of responses across the knowledge, attitude, and practice dimensions concerning NAFLD among elderly diabetic patients reveals varied levels of engagement and understanding. In the knowledge dimension, there is a notable deficiency, particularly in understanding the relationship between diabetes and NAFLD, dietary recommendations, and specific treatments for T2DM patients with NAFLD, with most respondents either answering incorrectly or indicating uncertainty. This gap in fundamental disease understanding mirrors previous findings, which noted similar challenges in diabetic patient education.27 Attitudinally, while there is a strong belief in the importance of understanding diabetes and NAFLD for effective management, there is also noticeable anxiety about having NAFLD. Practically, while many respondents report often engaging in recommended practices for managing NAFLD, such as monitoring liver health and maintaining a healthy diet, efforts toward weight management and emotional regulation are less frequently adhered to, highlighting potential areas for improvement in daily disease management. These less consistent practices reflect trends seen in broader study, which emphasize the need for ongoing patient support.28
Unlike most previous KAP studies focusing solely on patients, this study included both elderly diabetic patients and their family members. This design offers a more comprehensive perspective on disease management, given the supportive role of family in reinforcing health behaviors. The findings underscore the value of incorporating family-based educational strategies into MASLD care.
To address these deficiencies, targeted educational interventions are essential. One specific recommendation would be the development of tailored educational programs that leverage both digital media and traditional workshops to enhance understanding.29–31 These should focus on the critical areas where knowledge is lacking, such as the importance of diet (particularly the Mediterranean diet), the risks associated with alcohol consumption in NAFLD-cirrhosis, and the use of medications like empagliflozin and diagnostics like Magnetic Resonance Spectroscopy (MRS). Moreover, given the significant role of family members in patient management, educational interventions should also involve family members to ensure a supportive home environment that reinforces correct practices. For instance, cooking classes for families could be an effective method to encourage adherence to the Mediterranean diet. Additionally, healthcare providers should be encouraged to initiate regular discussions and check-ins about NAFLD during routine visits. This could be facilitated by integrating reminders into electronic health record systems that prompt healthcare professionals to discuss NAFLD risks and management strategies with patients, particularly those who are diabetic. Finally, considering the role of socioeconomic factors highlighted by the significant differences in knowledge based on education and residence type, community-based outreach programs could be beneficial. These programs could be tailored to different community needs, focusing on rural areas with less access to healthcare information and lower educational levels, utilizing local community centers or even mobile health units to disseminate information and resources effectively.32,33
This study has several limitations that should be considered when interpreting the results. First, the cross-sectional design limits our ability to establish causal relationships between the variables of knowledge, attitudes, and practices concerning NAFLD. Second, the study population was confined to two hospitals in a specific region, which may not reflect the broader demographic and cultural differences present in larger, more diverse populations. Finally, self-reported data from questionnaires are subject to response bias, which might have influenced the accuracy of the reported knowledge, attitudes, and practices.
Conclusions
In conclusion, elderly diabetic patients and their families exhibit a significant gap in knowledge about NAFLD, yet they maintain positive attitudes and proactive practices towards managing the condition. It is recommended that healthcare providers implement targeted educational interventions for elderly diabetic patients and their families to enhance knowledge, which is shown to positively influence attitudes and practices towards NAFLD management.
Abbreviations
KAP, Knowledge, attitudes, and practices; NAFLD, Non-alcoholic fatty liver disease; SEM, Structural equation modeling; T2DM, Type 2 diabetes mellitus; SD, Standard deviations; BMI, Body mass index; RMSEA, Root mean square error of approximation; SRMR, Standardized root mean square residual; CFI, Comparative fit index; TLI, Tucker-Lewis index.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics Approval and Consent to Participate
Ethical approval was granted by the Medical Ethics Committee of Baoding First Hospital of Traditional Chinese Medicine (now known as Guang’anmen Hospital (Baoding) China Academy of Chinese Medical Sciences; bdsdyzyy-IRB-20230825-001), and all participants provided written informed consent before inclusion in the study. I confirm that all methods were performed in accordance with the relevant guidelines. All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Luciani L, Pedrelli M, Parini P. Modification of lipoprotein metabolism and function driving atherogenesis in diabetes. Atherosclerosis. 2024;394:117545. doi:10.1016/j.atherosclerosis.2024.117545
2. Younossi ZM, Golabi P, Price JK, et al. The global epidemiology of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis among patients with type 2 diabetes. Clin Gastroenterol Hepatol. 2024;22(10):1999–2010.e8. doi:10.1016/j.cgh.2024.03.006
3. Dwivedi DK, Jena GB. NLRP3 inhibitor glibenclamide attenuates high-fat diet and streptozotocin-induced non-alcoholic fatty liver disease in rat: studies on oxidative stress, inflammation, DNA damage and insulin signalling pathway. Naunyn Schmiedebergs Arch Pharmacol. 2020;393(4):705–716. doi:10.1007/s00210-019-01773-5
4. Almahmoud MH, Al Khawaja NM, Alkinani A, Khader Y, Ajlouni KM. Prevalence of fatty liver disease and its associated factors among Jordanian patients with type 2 diabetes mellitus: a cross-sectional study. Ann Med Surg. 2021;68:102677. doi:10.1016/j.amsu.2021.102677
5. Ciardullo S, Ballabeni C, Trevisan R, Perseghin G. Liver fibrosis assessed by transient elastography is independently associated with albuminuria in the general United States population. Dig Liver Dis. 2021;53(7):866–872. doi:10.1016/j.dld.2021.02.010
6. Ciardullo S, Perseghin G. Statin use is associated with lower prevalence of advanced liver fibrosis in patients with type 2 diabetes. Metabolism. 2021;121:154752. doi:10.1016/j.metabol.2021.154752
7. Targher G, Corey KE, Byrne CD, Roden M. The complex link between NAFLD and type 2 diabetes mellitus - mechanisms and treatments. Nat Rev Gastroenterol Hepatol. 2021;18(9):599–612. doi:10.1038/s41575-021-00448-y
8. Tan J, Luo L, Zhang M, et al. A Chinese and western medication adherence scale in patients with chronic kidney disease. Patient Prefer Adherence. 2019;13:1487–1495. doi:10.2147/ppa.S207693
9. Tincopa MA, Wong J, Fetters M, Lok AS. Patient disease knowledge, attitudes and behaviours related to non-alcoholic fatty liver disease: a qualitative study. BMJ Open Gastroenterol. 2021;8(1):e000634. doi:10.1136/bmjgast-2021-000634
10. Khalid A, Haque S, Alvi S, et al. Promoting health literacy about cancer screening among Muslim immigrants in Canada: perspectives of imams on the role they can play in community. J Prim Care Community Health. 2022;13:21501319211063051. doi:10.1177/21501319211063051
11. Li L, Zhang J, Qiao Q, Wu L, Chen L. Development, reliability, and validity of the “Knowledge-Attitude-Practice” questionnaire of foreigners on traditional Chinese medicine treatment. Evid Based Complement Alternat Med. 2020;2020:8527320. doi:10.1155/2020/8527320
12. Ogura S, Jakovljevic MM. Editorial: global population aging - health care, social and economic consequences. Front Public Health. 2018;6:335. doi:10.3389/fpubh.2018.00335
13. Sinclair A, Saeedi P, Kaundal A, Karuranga S, Malanda B, Williams R. Diabetes and global ageing among 65–99-year-old adults: findings from the International Diabetes Federation Diabetes Atlas, 9(th) edition. Diabet Res Clin Pract. 2020;162:108078. doi:10.1016/j.diabres.2020.108078
14. Noureddin M, Yates KP, Vaughn IA, et al. Clinical and histological determinants of nonalcoholic steatohepatitis and advanced fibrosis in elderly patients. Hepatology. 2013;58(5):1644–1654. doi:10.1002/hep.26465
15. Lin W. The relationship between formal and informal care among Chinese older adults: based on the 2014 CLHLS dataset. BMC Health Serv Res. 2019;19(1):323. doi:10.1186/s12913-019-4160-8
16. Liao Y, Yang J. Status of nutrition labeling knowledge, attitude, and practice (KAP) of residents in the community and structural equation modeling analysis. Front Nutr. 2023;10:1097562. doi:10.3389/fnut.2023.1097562
17. Collier J. Applied structural equation modeling using AMOS: basic to advanced techniques. 2020.
18. Illum LRH, Forman A, Melgaard A, et al. Temporal and regional differences in the incidence of hospital-diagnosed endometriosis: a Danish population-based study. Acta Obstet Gynecol Scand. 2022;101(7):737–746. doi:10.1111/aogs.14364
19. Nebout A, Cavillon M, Ventelou B. Comparing GPs’ risk attitudes for their own health and for their patients’: a troubling discrepancy? BMC Health Serv Res. 2018;18(1):283. doi:10.1186/s12913-018-3044-7
20. Dauda Goni M, Hasan H, Naing NN, et al. Assessment of knowledge, attitude and practice towards prevention of respiratory tract infections among Hajj and Umrah Pilgrims from Malaysia in 2018. Int J Environ Res Public Health. 2019;16(22):4569. doi:10.3390/ijerph16224569
21. Gatulytė I, Verdiņa V, Vārpiņa Z, Lublóy Á. Level of health literacy in Latvia and Lithuania: a population-based study. Arch Public Health. 2022;80(1):166. doi:10.1186/s13690-022-00886-3
22. Marek-Jozefowicz L, Lemanowicz A, Grochocka M, et al. Cognitive functions associated with brain imaging markers in patients with psoriasis. Int J Environ Res Public Health. 2022;19(9):5687. doi:10.3390/ijerph19095687
23. Hao H, Nicholas S, Xu L, Leng A, Sun J, Han Z. Productivity losses due to diabetes in Urban Rural China. Int J Environ Res Public Health. 2022;19(10):5873. doi:10.3390/ijerph19105873
24. Zhu J, Sun K, Wang J, et al. Clinicopathological and surgical comparisons of differentiated thyroid cancer between China and the USA: a multicentered hospital-based study. Front Public Health. 2022;10:974359. doi:10.3389/fpubh.2022.974359
25. Okan O, Bollweg TM, Berens EM, Hurrelmann K, Bauer U, Schaeffer D. Coronavirus-related health literacy: a cross-sectional study in adults during the COVID-19 infodemic in Germany. Int J Environ Res Public Health. 2020;17(15):5503. doi:10.3390/ijerph17155503
26. Zhang Y, Li M, Jiang H, et al. Development and validation of a Chinese parental health literacy questionnaire for caregivers of children 0 to 3 years old. BMC Pediatr. 2019;19(1):293. doi:10.1186/s12887-019-1670-9
27. Ye H, Xin D, Hu X. The nursing effect of PRECEDE management on occupational exposure to surgical smoke: based on a randomized controlled study. Comput Math Methods Med. 2022;2022:8610517. doi:10.1155/2022/8610517
28. Gyuk P, Vassányi I, Kósa I. Blood glucose level prediction for diabetics based on nutrition and insulin administration logs using personalized mathematical models. J Healthc Eng. 2019;2019:8605206. doi:10.1155/2019/8605206
29. Chatterjee S, Davies MJ, Heller S, Speight J, Snoek FJ, Khunti K. Diabetes structured self-management education programmes: a narrative review and current innovations. Lancet Diabetes Endocrinol. 2018;6(2):130–142. doi:10.1016/s2213-8587(17)30239-5
30. Nassar CM, Montero A, Magee MF. Inpatient diabetes education in the real world: an overview of guidelines and delivery models. Curr Diab Rep. 2019;19(10):103. doi:10.1007/s11892-019-1222-6
31. Ruszkiewicz K, Jagielski P, Traczyk I. Glycemic control and awareness among diabetic patients of nutrition recommendations in diabetes. Rocz Panstw Zakl Hig. 2020;71(2):191–196. doi:10.32394/rpzh.2020.0116
32. Peng H, Pan L, Ran S, et al. Prediction of MAFLD and NAFLD using different screening indexes: a cross-sectional study in U.S. adults. Front Endocrinol. 2023;14:1083032. doi:10.3389/fendo.2023.1083032
33. Semmler G, Datz C, Reiberger T, Trauner M. Diet and exercise in NAFLD/NASH: beyond the obvious. Liver Int. 2021;41(10):2249–2268. doi:10.1111/liv.15024
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Managing Pain in Low Resource Settings: Healthcare Professionals’ Knowledge, Attitude and Practice Regarding Pain Management in Western Nepal
Thapa P, KC B, Lee SWH, Dujaili JA, Gyawali S, Mohamed Ibrahim MI, Alrasheedy AA
Journal of Pain Research 2022, 15:1587-1599
Published Date: 2 June 2022
Knowledge, Attitudes, and Practices Regarding Ergonomic Hazards Among Healthcare Workers in a Saudi Government Hospital

ALHazim SS, Al-Otaibi ST, Herzallah NH
Journal of Multidisciplinary Healthcare 2022, 15:1771-1778
Published Date: 24 August 2022
Critical Care Nurses’ Knowledge, Attitudes, and Practices Regarding Pressure Injury Treatment: A Nationwide Cross-Sectional Survey
Li J, Zhu C, Liu Y, Song B, Jin J, Liu Y, Wen X, Cheng S, Wu X
Risk Management and Healthcare Policy 2022, 15:2125-2134
Published Date: 16 November 2022
Self-Medication Prevalence and Factors Associated with Knowledge and Attitude Towards Self-Medication Among Undergraduate Health Science Students at GAMBY Medical and Business College, Bahir Dar, Ethiopia
Siraj EA, Yayehrad AT, Kassaw AT, Kassahun D, Solomon E, Abdela H, Gizachew G, Awoke E
Patient Preference and Adherence 2022, 16:3157-3172
Published Date: 5 December 2022
Dermatologists’ Knowledge, Attitude, and Practice Pattern Toward Low-Dose Oral Minoxidil in Hair Loss in Saudi Arabia
Altalhab S
Clinical, Cosmetic and Investigational Dermatology 2024, 17:653-662
Published Date: 15 March 2024