Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Knowledge, Attitudes, and Practices of Acupuncture Physicians and Medical Students Regarding Bloodborne Occupational Exposure: A Multi-Center Cross-Sectional Study
Authors Wu Y, Wang X, Li Z, Yin T, Fang H, Fu H, Zhang M
Received 15 October 2025
Accepted for publication 11 February 2026
Published 28 February 2026 Volume 2026:19 574604
DOI https://doi.org/10.2147/JMDH.S574604
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jagdish Khubchandani
Yingjue Wu,1,* Xinyue Wang,2,* Zhaoyang Li,1 Tong Yin,3 Hao Fang,4 Hang Fu,5 Mei Zhang1
1The Affiliated Traditional Chinese Medicine Hospital, Guangzhou Medical University, Guangzhou, 510000, People’s Republic of China; 2Department of Pediatric Neurology, Dongguan Children’s hospital, Dongguan, Guangdong, 523000, People’s Republic of China; 3Guangzhou University of Chinese Medicine, Guangzhou, People’s Republic of China; 4Clinical College of Traditional Chinese and Western Medicine, Guangzhou Medical University, Guangzhou, People’s Republic of China; 5TCM Department, Dongguan Eighth People’s Hospital, Dongguan, 523000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Mei Zhang, Email [email protected] Hang Fu, Email [email protected]
Background: Bloodborne occupational exposure poses a significant risk to acupuncture physicians and medical students, yet evidence regarding their knowledge, attitudes, and practices (KAP) remains limited.
Methods: This multicenter cross-sectional study analyzed data from 224 participants recruited from hospitals in Guangzhou, Dongguan, and Shenzhen. Structural equation modeling (SEM) and logistic regression were applied to examine the associations among training, attitudes, and practice behaviors related to bloodborne occupational exposure.
Results: More than half of participants (51.4%) were healthcare providers, and most (78.6%) had received relevant training. The average scores indicated generally adequate knowledge, positive attitudes, and proactive practices. SEM demonstrated that training exerted both direct effects on practice and indirect effects mediated through attitudes, highlighting the central role of attitudes and training rather than knowledge alone in shaping safe behaviors. Gender and training were significantly associated with practice outcomes, with male participants demonstrating higher practice scores than female participants.
Conclusion: Acupuncture physicians and medical students exhibited adequate knowledge and positive attitudes toward bloodborne occupational exposure, while attitudes and training were strongly associated with proactive practice behaviors. Knowledge alone, without adequate training, was insufficient to promote safe practices. These findings underscore the importance of targeted and structured training programs to enhance proactive practices by fostering favorable attitudes and safe behaviors in clinical settings.
Keywords: acupuncture, bloodborne pathogens, occupational exposure, knowledge, attitudes, practice, healthcare personnel, infection control
Introduction
Acupuncture physicians and medical students in China face a notable risk of bloodborne occupational exposure, which can have serious health implications. Bloodborne exposure occurs when medical staff, laboratory personnel, or relevant supervisors come into contact with blood, bodily fluids, or laboratory media containing pathogens such as Human Immunodeficiency Virus (HIV), Hepatitis B Virus (HBV), and Hepatitis C Virus (HCV), during disease diagnosis, treatment, nursing, prevention, testing, or management activities.1 While bloodborne occupational exposure is a recognized concern across various healthcare settings, it poses a unique risk in acupuncture due to the need for repeated skin punctures, which inherently increase the likelihood of needlestick injuries and exposure to infectious agents.
Research indicates that needlestick injuries are common among healthcare workers, including acupuncturists, which can lead to the transmission of bloodborne pathogens such as HBV, HCV, and HIV.2 In China, a survey of 578 acupuncture practitioners across 98 hospitals in southwest China reported that 34.3% experienced at least one needlestick injury in the past three years, with approximately 46% of incidents unreported.3 The high prevalence of these injuries underscores the urgent need for robust safety protocols and effective training to reduce the risk of exposure. For example, one study found that a substantial portion of healthcare providers had experienced needlestick injuries, often during procedures involving sharp instruments, highlighting the importance of meticulous adherence to safety practices.4 Educational interventions designed to increase awareness of the risks associated with bloodborne pathogens and the critical importance of promptly reporting incidents have shown to be effective in enhancing safety within acupuncture and similar practice settings.5
The Knowledge-Attitude-Practice (KAP) model, widely applied in health behavior research, provides a comprehensive framework for understanding and influencing health-related behaviors.6 This model is typically used alongside the KAP questionnaire to assess the knowledge, attitudes, and practices within a specific population, helping gauge the demand for and acceptance of relevant training in the healthcare domain.7 Based on the premise that knowledge positively impacts attitudes, which in turn shapes practices, the KAP model serves as a foundational approach to enhance health literacy and promote safe practices.8 However, evidence from health behavior research suggests that knowledge alone is often insufficient to ensure the adoption of safe behaviors, as behavioral change is also strongly influenced by attitudes, perceived risk, motivation, and institutional or environmental support. Without positive attitudes and reinforcement through training and organizational policies, individuals may fail to translate knowledge into consistent protective practices.9,10
Despite the high relevance, current research on bloodborne occupational exposure has primarily focused on Western medical settings, with relatively little investigation into the KAP of acupuncture practitioners and students. This gap in the literature highlights the need for an in-depth exploration of their knowledge and attitudes toward bloodborne occupational exposure, as well as the factors influencing their practices. By identifying areas where knowledge may be lacking, assessing the connection between attitudes and practices, and providing targeted training, this study aims to improve the occupational safety practices of acupuncture professionals. This investigation will not only raise awareness and improve protective behaviors but also establish a scientific basis for tailored education and training programs specific to the field of acupuncture. Ultimately, the findings of this study will offer valuable insights to enhance the strategies used to address bloodborne occupational exposure in clinical practice, contributing to the overall safety and well-being of acupuncture physicians, medical students, and their patients. Specifically, this study aimed to: (1) assess the levels of knowledge, attitudes, and practices (KAP) toward bloodborne occupational exposure; (2) explore the correlations among KAP dimensions; and (3) identify demographic and training-related factors that influence practice behaviors.
Methods
Study Design and Participants
This cross-sectional study was conducted from June 10th to August 31th at hospitals in Guangzhou, Dongguan and Shenzhen. Specifically, four hospitals were involved: two in Guangzhou, one in Dongguan, and one in Shenzhen, including Guangzhou University of Chinese Medicine Affiliated Traditional Chinese Medicine Hospital, the Traditional Chinese Medicine Department of Dongguan Children’s Hospital, Shenzhen Bao’an District Hospital of Traditional Chinese Medicine, and Guangzhou Tianhe District Shipai Street Community Health Service Center. Convenience sampling was used to recruit participants due to the multicenter design and the practical constraints of accessing acupuncture physicians and students across different hospitals within a limited study period. To mitigate potential selection bias, participants were recruited from multiple hospitals of different levels in three cities, and clear inclusion and exclusion criteria were applied. In addition, standardized questionnaires, quality control measures (including trap questions and response pattern checks), and multivariate statistical analyses were used to reduce the influence of potential confounding factors. Acupuncture physicians, doctors in rotation or advanced acupuncture studies, students, and nurses were included. The exclusion criteria were: (1) Participants who withdrew from the survey without providing informed consent; (2) Questionnaires where trap questions were answered incorrectly; (3) Questionnaires with uniform responses across all items in the KAP sections. Ethical approval was obtained from the author’s Hospital, and informed consent was secured from all participants.
Questionnaire Introduction
After the initial questionnaire draft, it was reviewed by two chief acupuncture physicians and university professors, who recommended adding items on preventive measures and specific infection pathways in acupuncture. A pilot test with 34 participants yielded a Cronbach’s α coefficient of 0.8347, indicating good reliability.
The final Chinese-language questionnaire comprises four sections: demographic information, knowledge, attitude, and practice. The knowledge section includes 7 questions, with each correct response awarded 1 point and incorrect responses given 0 points. Questions 5 and 6 serve as mutually exclusive trap questions; responses indicating both “true” or both “false” render the questionnaire invalid, leading to exclusion from the analysis and scoring, resulting in a scoring range of 0–5 points. The attitude section consists of 8 questions assessed on a five-point Likert scale, from “strongly agree” (5 points) to “strongly disagree” (1 point), with scores ranging from 8 to 40 points. The practice section includes 9 questions, also on a five-point Likert scale, from “always” (5 points) to “never” (1 point), with a scoring range of 9–45 points. The final questionnaire was in Chinese (a version translated into English was attached as an Supplementary material). Scores above 70% of the maximum in each section were considered to indicate adequate knowledge, a positive attitude, and proactive practice.11 Questionnaires were distributed to participants via WeChat, Questionnaire Star, and paper surveys.
Sample Size and EPV Consideration
Sample size calculation was performed based on the “events per variable” (EPV) rule, adhering to the recommended 5–10 EPV threshold. Given that the questionnaire comprised 42 items, the minimum required sample size was calculated as 210 (42 events × 5 EPV). The final analytical cohort included 224 participants, which exceeded the minimum sample size requirement and ensured adequate statistical power.
Statistical Methods
Data analysis was conducted using R 4.3.2. The normality of score distributions for each dimension was assessed prior to analysis. For normally distributed data, results are presented as means and standard deviations (SD); for non-normally distributed data, medians, 25th, and 75th percentiles are reported. Categorical response data by demographic characteristics are expressed as n (%). Comparisons between two groups for continuous variables were performed using a t-test for normally distributed data, and the Wilcoxon-Mann–Whitney test for non-normally distributed data. For comparisons across three or more groups, analysis of variance (ANOVA) was used for normally distributed continuous variables with equal variance, while the Kruskal–Wallis test was applied to non-normally distributed data. For correlation analyses among dimension scores, Pearson correlation coefficients were used when normality assumptions were met; otherwise, Spearman correlation coefficients were applied. Both univariate and multivariate regression analyses were conducted to explore the relationships between demographic characteristics and dimension scores, with median scores used as classification thresholds. Variables with P < 0.1 in univariate analyses were included in the multivariate regression model. P values were retained to three decimal places, with a two-sided P < 0.05 considered statistically significant. The structural equation model (SEM) was employed within the Knowledge, Attitude, and Practice (KAP) theoretical framework to test whether attitudes mediated the relationship between knowledge and practice behaviors, examining the sizes of direct and indirect effects. Model fit was evaluated based on root mean square error of approximation (RMSEA) < 0.08, standardized root mean square residual (SRMR) < 0.08, Tucker-Lewis index (TLI) > 0.8, and comparative fit index (CFI) > 0.8. If model fit indices failed to meet these criteria, mediation effects were further analyzed through path analysis. SEM analysis was conducted using Stata 18.0.
Results
A total of 296 samples were initially collected. The following cases were excluded: one case without informed consent; ten cases with a response time of less than 80 seconds; two cases where participants were either under 18 years or identified as outliers; and 59 cases with inconsistencies in quality control responses. This resulted in a final valid dataset of 224 cases. In the formal study, internal consistency was good for the total scale and each subscale, with an overall Cronbach’s α coefficient of 0.8321; the coefficients for the knowledge, attitude, and practice subscales were 0.8981, 0.7703, and 0.8714, respectively. The KMO value for the total scale was 0.8911.
Demographic Information
Among the 224 participants, 115 (51.4%) were physicians or technicians/nurses, 135 (60.3%) were female, 97 (43.3%) were aged between 26–35 years, 117 (52.2%) had an associate degree or lower, 71 (31.7%) had over 10 years of experience, 98 (43.8%) held intermediate professional titles, 146 (65.2%) worked in tertiary hospitals, and 176 (78.6%) had received training related to bloodborne occupational exposure. The mean (SD) scores for knowledge, attitude, and practice were 4.88 (0.38), 30.68 (1.86), and 37.97 (5.15), respectively. Analysis of demographic differences showed no association between demographic factors and knowledge scores. However, participants with relevant training were more likely to have higher attitude scores (P = 0.019). Practice scores varied significantly by gender (P = 0.014), age (P = 0.006), residence (P = 0.045), years of experience (P = 0.027), professional title (P = 0.002), relevant training (P < 0.001), and professional category (P < 0.001) (Table 1). Specifically, male participants demonstrated higher mean practice scores than female participants, indicating a gender-related difference in proactive safety practices.
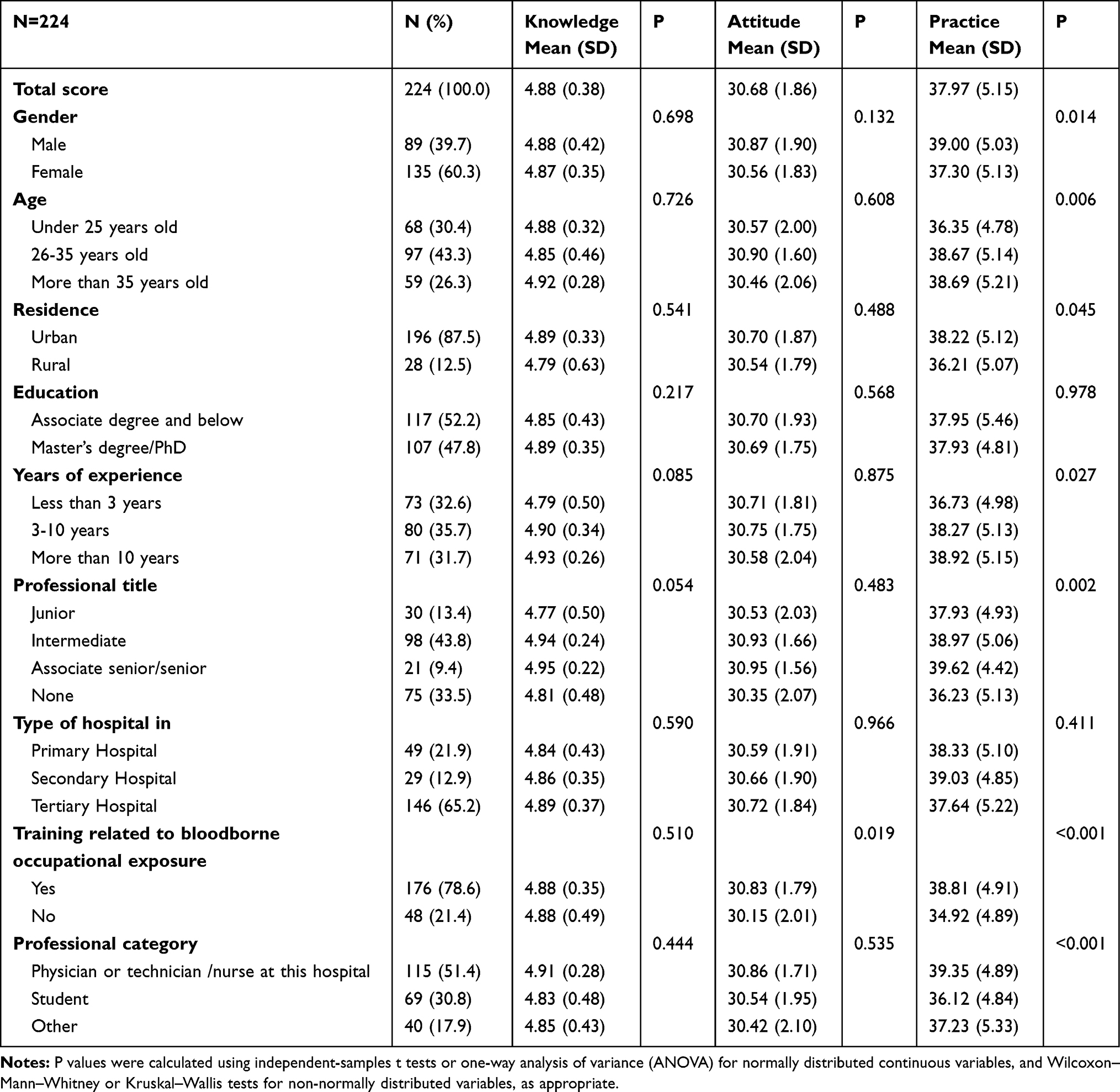 |
Table 1 Demographic Characteristics |
Participant Responses on Knowledge, Attitude, Practice, and Current Exposure Status
Responses on the knowledge dimension demonstrated high levels of awareness, with over 92.4% of participants answering all items correctly. The highest error rate (7.6%) was on the item “The risk of infection after exposure for healthcare workers is primarily determined by three factors: (1) the prevalence of bloodborne pathogens in the population, (2) the likelihood of seroconversion after exposure, and (3) the frequency of exposure” (K3). (Supplementary Figure 1). On the attitude dimension, 42% strongly agreed, 42.9% agreed, and 14.3% were neutral on the effectiveness of current post-exposure management and emergency response measures (A4). Meanwhile, 53.1% were very concerned, and 38.4% were concerned about the possibility of bloodborne occupational exposure in their work (A3) (Supplementary Figure 2). For relevant practices, 9.8% participated infrequently, and 2.7% never attended training on bloodborne occupational exposure prevention and control (P2). Additionally, 5.8% found it challenging to accurately record all occupational exposure incidents and actions taken (P2) (Supplementary Figure 3).
Regarding current bloodborne occupational exposure status, 31 participants (13.8%) reported exposure within the past year, and 12 (5.4%) were unsure. Of the 43 cases, 41 (95.3%) involved eye exposure, 35 (81.4%) occurred due to accidental injury by others, 32 (74.4%) took place in a physiotherapy room, and 22 (51.2%) were reported immediately after exposure (Supplementary Figure 4).
Correlations Between KAP
Correlation analysis revealed a significant positive correlation between attitude and practice (r = 0.406, P < 0.001). However, correlations between knowledge and both attitude and practice were not significant (Table 2).
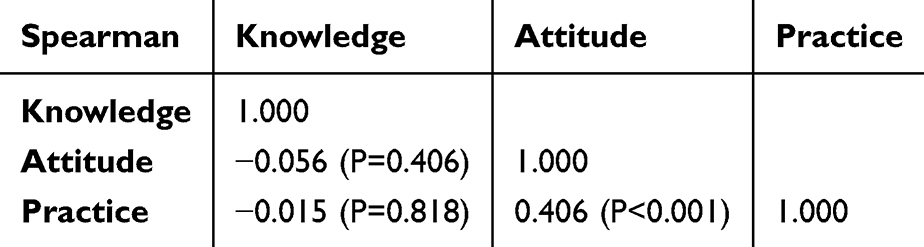 |
Table 2 Spearman Correlation Analysis |
Univariate and Multivariate Logistic Regression Analysis for Practice
The median of practice scores was used as the cut-off value, and the number of participants above the cut-off value was 118 (52.68%). Multivariate logistic regression analysis revealed that both attitude and training were significant independent predictors of proactive practice behavior. Specifically, for each one-point increase in attitude score, the odds of demonstrating proactive practice increased by 42% (OR = 1.419, 95% CI: [1.185, 1.699], P < 0.001). Participants without relevant training had 61% lower odds of proactive practice compared to those with training (OR = 0.391, 95% CI: [0.182, 0.843], P = 0.017) (Table 3).
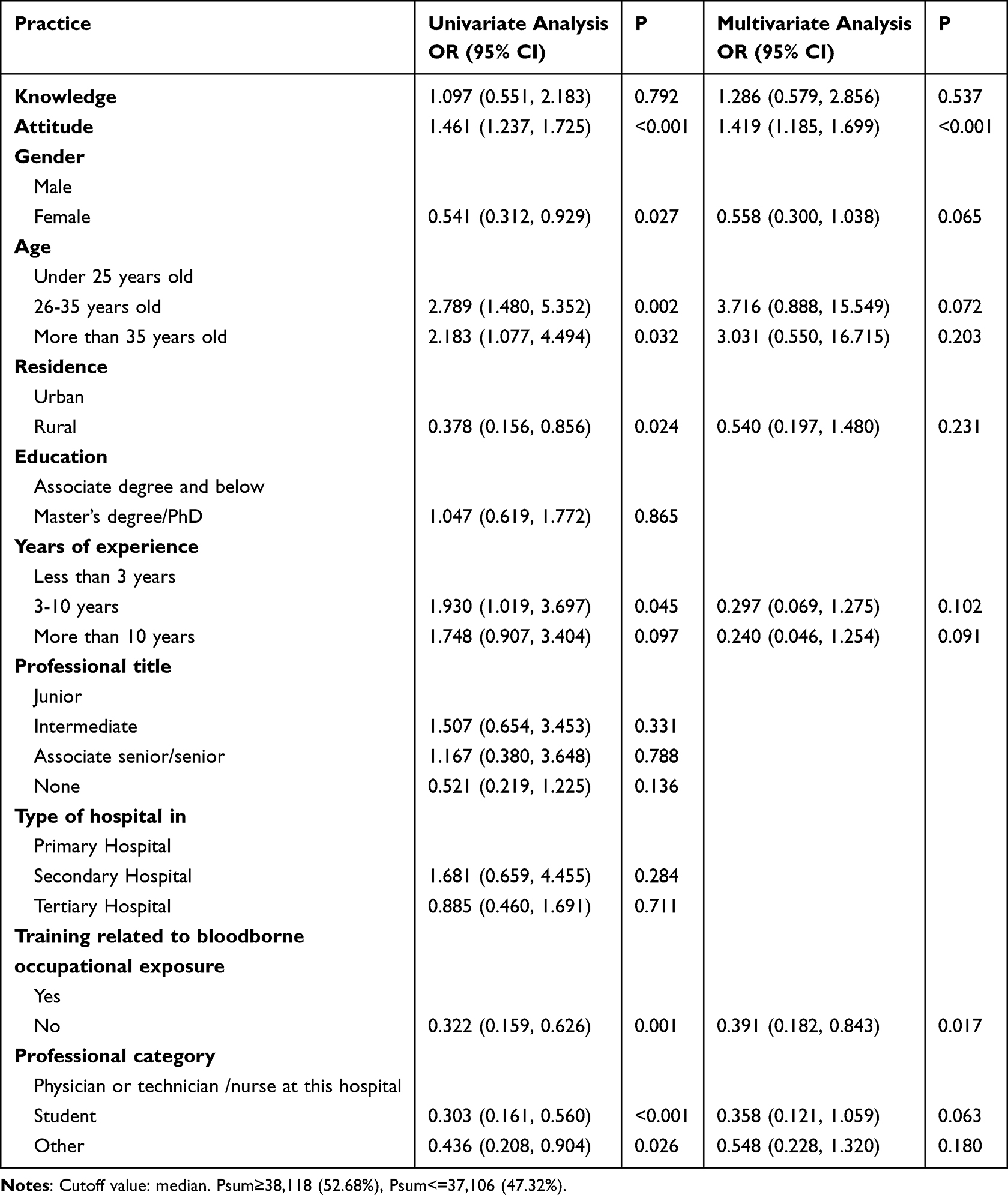 |
Table 3 Univariate and Multivariate Logistic Regression Analysis for Practice |
SEM Analysis and Path Analysis
The structural model fit indices (RMSEA = 0.051; SRMR = 0.023; TLI = 0.933; CFI = 0.990) surpassed threshold values, indicating a satisfactory fit of the data to the model (Supplementary Table 1). Structural equation modeling (SEM) further supported the strong influence of attitude and training on practice behaviors. Attitude had a significant direct effect on practice (β = 0.345, 95% CI: [0.228, 0.461], P < 0.001), indicating that more positive attitudes were associated with safer practice behaviors. Similarly, training had both a direct effect on practice (β = −0.263, 95% CI: [−0.379, −0.147], P < 0.001) and an indirect effect via attitude (β = −0.052, 95% CI: [−0.100, −0.004], P = 0.033), confirming its central role in influencing both attitudes and practices. Moreover, training also significantly improved attitude itself (β = −0.151, 95% CI: [−0.281, −0.022], P = 0.022) (Table 4 and Figure 1).
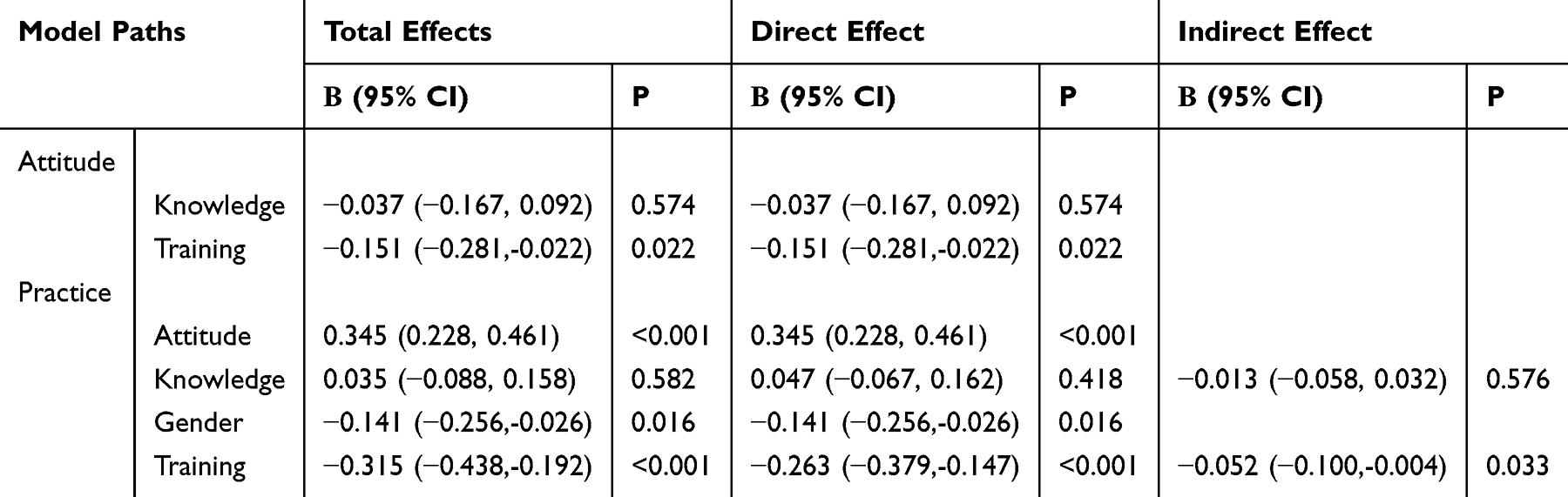 |
Table 4 Path Analysis |
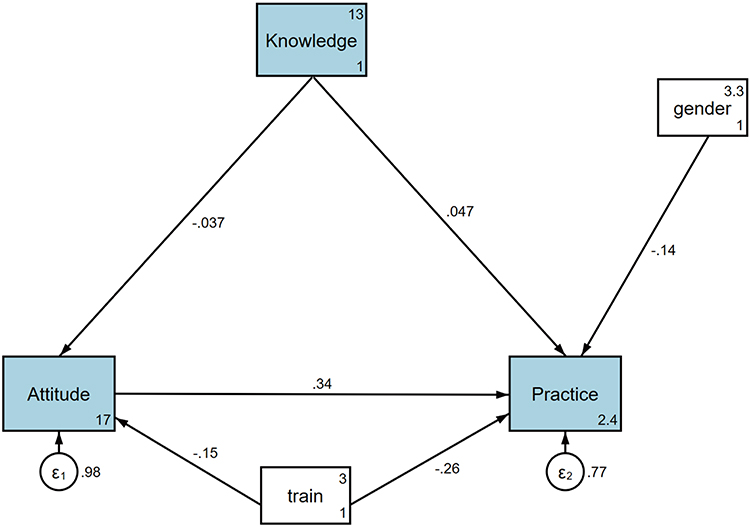 |
Figure 1 Structural equation model (SEM) illustrating the associations among knowledge, attitude, training, and practice regarding bloodborne occupational exposure. Standardized path coefficients are shown. Solid lines indicate statistically significant paths. |
Discussion
Acupuncture physicians and medical students demonstrated adequate knowledge, positive attitudes, and proactive practices regarding bloodborne occupational exposure. Enhancing training programs focusing on bloodborne exposure could further improve preventive practices in clinical settings.
Despite this overall positivity, there were specific areas where KAP appeared less robust, potentially contributing to ongoing challenges in full compliance with bloodborne safety protocols. These findings are in line with earlier observations by Subramanian et al and Edlich et al,1,2 who emphasized the inherent risk of bloodborne exposures in clinical procedures, particularly among healthcare workers using sharp instruments. Our study reaffirms that acupuncture, due to its skin-penetrating nature, presents similar risks. Grimmond and Good4 also noted that many exposures occurred during needle disposal and handling—patterns similarly observed in our data, where 58.1% of reported exposures occurred during the disposal stage. Furthermore, Wen et al5 found that structured training significantly improved nursing students’ awareness and responses to exposure events. Our findings extend this by showing that training is positively associated with more favorable attitudes and proactive practice behaviors. These results are also consistent with those of Alsaeed et al and Rahmani et al,12,13 who reported that although healthcare providers often have basic knowledge and positive attitudes toward occupational risks, actual adherence to safety protocols can be inconsistent. Alsaeed et al found that emergency responders in Saudi Arabia demonstrated strong awareness of infection control practices, but lacked uniform implementation in real scenarios. Similarly, Rahmani et al observed that nursing staff during the COVID-19 pandemic showed psychological stress and irregular compliance with safety procedures. Our study also identified this discrepancy—knowledge did not significantly predict practice, while attitude and training played more substantial roles, suggesting that positive perceptions and institutional reinforcement may be more effective drivers of safe behaviors than knowledge alone.
The relationships between KAP dimensions in this study offer interesting insights. Although structural equation modeling was applied to examine the hypothesized pathways among knowledge, attitudes, training, and practices, the cross-sectional design of this study does not allow for causal inference. The SEM results should therefore be interpreted as associations that are consistent with the proposed theoretical framework, rather than evidence of temporal or causal relationships. Longitudinal or interventional studies are required to further verify the causal directions suggested by the model. Both correlation analyses and SEM identified a significant positive correlation between attitude and practice, underscoring that a favorable attitude is strongly associated with proactive safety behaviors. This finding is consistent with prior research, which also emphasizes the role of positive attitudes in translating knowledge into effective practice behaviors.14,15 For instance, healthcare workers who believe in the efficacy of standard precautions are more likely to consistently apply them in practice. However, knowledge did not significantly correlate with attitude or practice, which mirrors findings in similar studies where knowledge alone was not a sufficient driver of behavior change without corresponding attitudes or reinforcement through training.16,17 This suggests that while foundational knowledge is essential, it may not fully drive compliance without active reinforcement of positive attitudes and practice-oriented training.
Significant differences were noted in practice scores across demographic factors, particularly gender, age, residence, and training. Multivariate analysis reinforced these findings, revealing that male participants, individuals with prior training, and those with longer professional experience demonstrated higher practice scores. This finding suggests that practice behaviors may differ by gender and professional experience, and such differences have been variably reported across healthcare safety research.18,19 Training on bloodborne occupational exposure significantly impacted both attitudes and practices, highlighting its role in fostering a culture of safety. These findings support targeted interventions, as tailored training sessions that reinforce both knowledge and attitudes could bridge the gap for those who lack direct experience or prior training.
Education level, however, was not associated with differences in practice scores. This result suggests that in healthcare settings with standardized protocols, practical experience and hands-on training may outweigh formal education in influencing safety practices. Studies have similarly found that standardized procedures and ongoing training have a more substantial impact on compliance than initial education level, emphasizing the need for regular refresher courses and practical skills assessments in workplace safety training programs.20,21
The detailed analysis of responses sheds light on specific areas of knowledge, attitude, and practice. While participants generally demonstrated a strong understanding of bloodborne exposure concepts, including the necessity of preventive measures, some specific knowledge items, like the factors influencing infection risk, had relatively higher error rates. This finding is echoed in similar studies, which have reported that while basic knowledge is usually well understood, complex or less frequently addressed aspects often exhibit gaps.22,23 Attitudinal responses were largely positive, with most participants recognizing the importance of preventive measures. However, a notable proportion expressed anxiety regarding the risk of exposure and concerns about the adequacy of post-exposure procedures. These concerns, reported in other studies as well, can undermine confidence and lead to inconsistent practice behaviors.24,25
Practice-related responses pointed to certain areas needing improvement. For instance, participation in training, consistent PPE checks, and accurate documentation of exposure incidents were all less frequently reported. Studies have shown that routine retraining and reinforcement of documentation practices can significantly improve these behaviors, as consistent training fosters habit formation and raises awareness of procedural details.26,27 Specifically, regular training sessions incorporating hands-on simulations can enhance familiarity with emergency response measures, improving both accuracy in practice and confidence in managing exposure incidents.28,29
To address the identified gaps in practice, the following interventions are recommended: 1) Mandatory annual training on bloodborne occupational exposure prevention, especially focusing on high-error knowledge areas (eg, infection risk factors), to reinforce understanding and risk awareness;26 2) Simulation-based exercises to familiarize staff with emergency response procedures and enhance confidence in incident management;27 3) Peer mentoring systems, where experienced staff guide junior practitioners in safe practices, reinforcing positive attitudes and reducing anxiety; 4) Routine performance feedback and PPE use monitoring to improve consistency and accountability in protective behaviors; 5) Streamlined reporting systems and reminder protocols to encourage timely and complete reporting of exposure incidents.30,31
Given that a substantial proportion of exposure events occurred during needle disposal and handling, additional targeted measures are warranted to further reduce occupational risks, particularly among highly vulnerable practitioners. The use of protective devices, such as needle guards or protective shields during needle removal and disposal, may help minimize accidental injuries. Emerging technological approaches, including robotic-assisted procedures, may also reduce direct hand–needle contact in high-risk settings. In addition, noninvasive acupuncture-related techniques, such as laser acupuncture, transcutaneous electrical acupoint stimulation (TEAS), or other needle-free modalities, could be considered as complementary alternatives in selected populations to reduce exposure risk while maintaining therapeutic effectiveness.
To enhance the practical applicability of these suggestions, tailored approaches based on specific demographic needs may be effective. For example, experienced staff may benefit more from advanced training modules or leadership roles in safety initiatives, while newer or younger healthcare workers could gain from more foundational training focusing on basic practices and procedures. Integrating such structured and demographic-specific approaches has shown success in improving compliance in similar occupational health contexts.32,33 Similarly, for those working in rural versus urban settings, localized training adaptations that account for available resources and environmental factors can further promote adherence to best practices.34,35
The findings of this study have several important implications for clinical practice, training, and future research. From a practical perspective, the results highlight that improving safety behaviors among acupuncture practitioners cannot rely on knowledge dissemination alone. Structured and continuous training programs that actively reinforce positive attitudes toward bloodborne exposure prevention are essential, particularly for high-risk procedures such as needle handling and disposal. Incorporating simulation-based training, standardized operating procedures, and regular refresher courses may help translate awareness into consistent safe practices.
In terms of policy and education, institutions may consider integrating targeted occupational exposure training into routine professional development and clinical supervision, with particular attention to vulnerable groups such as junior practitioners and trainees. For future research, longitudinal or interventional studies are warranted to further examine the causal pathways suggested by the current findings and to evaluate the effectiveness of specific training strategies or technological interventions in reducing bloodborne occupational exposure in acupuncture settings.
This study has several limitations. First, the cross-sectional design restricts the ability to draw causal inferences between knowledge, attitudes, practices, and training. Second, self-reported data may be subject to recall bias or social desirability bias, potentially influencing participants’ responses about their practices. Finally, the study was conducted in a limited geographic area, focusing on a tertiary hospital in Guangzhou and surrounding cities, which may limit the generalizability of the findings to other regions or healthcare settings. In addition, the relatively small sample size (n = 224) may have reduced the statistical power for subgroup analyses and increased the potential for type II errors, thus affecting the robustness of some associations.
Conclusions
In conclusion, acupuncture physicians and medical students demonstrated adequate knowledge, positive attitudes, and proactive practices regarding bloodborne occupational exposure. A positive attitude was significantly associated with proactive practices, and relevant training was strongly associated with more favorable attitudes and proactive practices. These findings indicate that knowledge of occupational exposure risks alone, without adequate and structured training, is insufficient to foster positive attitudes or ensure safe practice behaviors. To enhance proactive practices in clinical settings, targeted training on bloodborne exposure prevention should be expanded, particularly emphasizing its role in shaping positive attitudes and safe practices.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article. Additional data are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study was approved by Ethics Committee of the Affiliated Traditional Chinese Medicine Hospital (2024NK69). All participants were informed about the study protocol and provided written informed consent to participate in the study. I confirm that all methods were performed in accordance with the relevant guidelines. All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The Clinical College of Traditional Chinese and Western Medicine of Guangzhou Medical University announced the teaching and cultivation project of traditional Chinese and Western clinical medicine in 2023 (20230053).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Subramanian GC, Arip M, Saraswathy Subramaniam TS. Knowledge and risk perceptions of occupational infections among health-care workers in Malaysia. Saf Health Work. 2017;8(3):246–11. doi:10.1016/j.shaw.2016.12.007
2. Edlich RF, Rhoads SK, Buck LR, Gubler KD, Long WB, Zura RB. The failure of the Food and Drug Administration to protect operating room personnel from the spread of deadly blood-borne infections. Ann Plast Surg. 2011;66(4):421. doi:10.1097/SAP.0b013e3182152ed7
3. Jiang W, Liu Y, Cao L, Zhou P, Dai A, Tang J. Needle stick injury and associated factors among acupuncture practitioners: a cross-sectional study in China. Front Public Health. 2024;12:1515889. doi:10.3389/fpubh.2024.1515889
4. Grimmond T, Good L. Exposure survey of trends in occupational practice (EXPO-S.T.O.P.) 2015: a national survey of sharps injuries and mucocutaneous blood exposures among health care workers in US hospitals. Am J Infect Control. 2017;45(11):1218–1223. doi:10.1016/j.ajic.2017.05.023
5. Wen H, Zhang R, Zhou Z, et al. Comparison of lecture-based learning with presentation-assimilation-discussion method in occupational bloodborne exposure education of nursing students, a randomised trial. BMC Nurs. 2024;23(1):702. doi:10.1186/s12912-024-02365-2
6. Tan J, Luo L, Zhang M, et al. A Chinese and western medication adherence scale in patients with chronic kidney disease. Patient Prefer Adherence. 2019;13:1487–1495. doi:10.2147/PPA.S207693
7. Li L, Zhang J, Qiao Q, Wu L, Chen L. Development, reliability, and validity of the”knowledge-attitude-practice” questionnaire of foreigners on traditional chinese medicine treatment. Evid Based Complement Alternat Med. 2020;2020:8527320. doi:10.1155/2020/8527320
8. Khalid A, Haque S, Alvi S, et al. Promoting health literacy about cancer screening among Muslim immigrants in canada: perspectives of imams on the role they can play in community. J Prim Care Community Health. 2022;13:21501319211063051. doi:10.1177/21501319211063051
9. Guerin RJ, Toland MD. An application of a modified theory of planned behavior model to investigate adolescents’ job safety knowledge, norms, attitude and intention to enact workplace safety and health skills. J Safety Res. 2020;72:189–198. doi:10.1016/j.jsr.2019.12.002
10. Alves FR. The relationship between health-related knowledge and attitudes and health risk behaviours among Portuguese university students. Global Health Promotion. 2024;31(1):36–44. doi:10.1177/17579759231195561
11. Lee F, Suryohusodo AA. Knowledge, attitude, and practice assessment toward COVID-19 among communities in East Nusa Tenggara, Indonesia: a cross-sectional study. Front Public Health. 2022;10:957630. doi:10.3389/fpubh.2022.957630
12. Alsaeed SA, Alkarani AS. Factors affects the performance of red crescent paramedics, Bisha, Saudi Arabia. J Family Med Prim Care. 2022;11(2):715–719. doi:10.4103/jfmpc.jfmpc_2060_21
13. Rahmani F, Hosseinzadeh M, Gholizadeh L. Complicated grief and related factors among nursing staff during the Covid-19 pandemic: a cross-sectional study. BMC Psychiatry. 2023;23(1):73. doi:10.1186/s12888-023-04562-w
14. Koroma JM, Wang Y, Guo X, et al. A cross-sectional survey on the malaria control and prevention knowledge, attitudes, and practices of caregivers of children under-5 in the western area of Sierra Leone. Trop Med Infect Dis. 2022;7(7). doi:10.3390/tropicalmed7070120
15. Sinuraya RK, Kusuma ASW, Pardoel ZE, Postma MJ, Suwantika AA. Parents’ knowledge, attitude, and practice on childhood vaccination during the COVID-19 pandemic in Indonesia. Patient Prefer Adherence. 2022;16:105–112. doi:10.2147/PPA.S339876
16. Alqassim MY, Kresnye KC, Siek KA, Lee J, Wolters MK. The miscarriage circle of care: towards leveraging online spaces for social support. BMC Womens Health. 2022;22(1):23. doi:10.1186/s12905-022-01597-1
17. Bitta MA, Kariuki SM, Gona J, Abubakar A, Newton C. Priority mental, neurological and substance use disorders in rural Kenya: traditional health practitioners’ and primary health care workers’ perspectives. PLoS One. 2019;14(7):e0220034. doi:10.1371/journal.pone.0220034
18. Cho OH, Lee D, Hwang KH. Patient safety awareness, knowledge and attitude about fire risk assessment during time-out among perioperative nurses in Korea. Nurs Open. 2022;9(2):1353–1361. doi:10.1002/nop2.1180
19. Rubasinghe S, Priyadarshani K, Wijesundara P, et al. Knowledge of nosocomial infections, standard precautions, and source of information among physiotherapy undergraduates in Sri Lanka; an observational study. Antimicrob Resist Infect Control. 2023;12(1):45. doi:10.1186/s13756-023-01248-6
20. Kam AJ, Gonsalves CL, Nordlund SV, et al. Implementation and facilitation of post-resuscitation debriefing: a comparative crossover study of two post-resuscitation debriefing frameworks. BMC Emerg Med. 2022;22(1):152. doi:10.1186/s12873-022-00707-4
21. Malik AA, Khan RS, Khan RN, et al. Lack of awareness among surgeons regarding safe use of electrosurgery. A cross sectional survey of surgeons in Pakistan. Ann Med Surg Lond. 2020;50:24–27. doi:10.1016/j.amsu.2019.11.017
22. Nelsen DR, David EM, Harty CN, Hector JB, Corbit AG. Risk assessment and the effects of refuge availability on the defensive behaviors of the southern unstriped scorpion (Vaejovis carolinianus). Toxins. 2020;12(9):534. doi:10.3390/toxins12090534
23. Peolsson A, Peterson G, Hermansen A, Ludvigsson ML, Dedering Å, Löfgren H. Physiotherapy after anterior cervical spine surgery for cervical disc disease: study protocol of a prospective randomised study to compare internet-based neck-specific exercise with prescribed physical activity. BMJ Open. 2019;9(2):e027387. doi:10.1136/bmjopen-2018-027387
24. Casey AN, Islam MM, Schütze H, et al. GP awareness, practice, knowledge and confidence: evaluation of the first nation-wide dementia-focused continuing medical education program in Australia. BMC Fam Pract. 2020;21(1):104. doi:10.1186/s12875-020-01178-x
25. Koffman J, Yorganci E, Yi D, et al. Managing uncertain recovery for patients nearing the end of life in hospital: a mixed-methods feasibility cluster randomised controlled trial of the AMBER care bundle. Trials. 2019;20(1):506. doi:10.1186/s13063-019-3612-0
26. Iqbal J, Asghar MZ, Ashraf MA, Yi X. The impacts of emotional intelligence on students’ study habits in blended learning environments: the mediating role of cognitive engagement during COVID-19. Behav Sci. 2022;12(1):14.
27. Marín-Marín JA, Soler-Costa R, Moreno-Guerrero AJ, López-Belmonte J. Effectiveness of diet habits and active life in vocational training for higher technician in dietetics: contrast between the traditional method and the digital resources. Nutrients. 2020;12(11):3475. doi:10.3390/nu12113475
28. Nantanda R, Kayingo G, Jones R, van Gemert F, Kirenga BJ. Training needs for Ugandan primary care health workers in management of respiratory diseases: a cross sectional survey. BMC Health Serv Res. 2020;20(1):402. doi:10.1186/s12913-020-05135-3
29. Prat Vigué G, Cano Prieto I, Del Río Sáez R, Vilanova Masana R, Simó Algado S. Training peer support workers in mental health care: a mixed methods study in central catalonia. Front Psychiatry. 2022;13:791724. doi:10.3389/fpsyt.2022.791724
30. Lee JB, Choi JS. Epidemiology of occupational exposure to blood-borne viruses, postexposure prophylaxis and seroconversion over 10 years among healthcare workers. J Hosp Infect. 2023;135:18–27. doi:10.1016/j.jhin.2023.02.003
31. Zhang L, Li Q, Guan L, et al. Prevalence and influence factors of occupational exposure to blood and body fluids in registered Chinese nurses: a national cross-sectional study. BMC Nurs. 2022;21(1):298. doi:10.1186/s12912-022-01090-y
32. Yu X, Gan T, Zhu Y, Wang M, Qian L, Lu Y. Management of occupational bloodborne pathogen exposure among medical personnel: a 4-year prospective study. Jpn J Infect Dis. 2023;76(5):289–294. doi:10.7883/yoken.JJID.2022.492
33. Zhang Y, Zhang H, Li L, Li J. A survey of bloodborne occupational exposure protection behavior among qualified Chinese midwives: a cross-sectional study. Heliyon. 2023;9(11):e21288. doi:10.1016/j.heliyon.2023.e21288
34. Han A, Henderson DK. Postexposure prophylaxis for occupational exposure to selected pathogens for healthcare personnel. Curr Opin Infect Dis. 2024;37(4):296–303. doi:10.1097/QCO.0000000000001029
35. Pierce A. Management of occupational exposure to blood and body fluids in primary care. Aust Prescr. 2024;47(4):113–118. doi:10.18773/austprescr.2024.037
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Psychiatric Nurses’ Knowledge, Attitudes, and Practice Regarding Physical Restraint in China: A Multicentre Cross-Sectional Study
Chong Y, Wang C, Zhi T, Fang S, Min H, Zhang L, Wu X, Wang Y
Journal of Multidisciplinary Healthcare 2023, 16:1475-1489
Published Date: 29 May 2023
Assessing the Knowledge, Attitudes, and Vaccination Practices Towards COVID-19 Vaccination Among Mainland Chinese Nursing Students and Interns: A Multicenter Cross-Sectional Study

Qin Z, Ye X, Liu H, Tao Y, Zheng X, Zhong Y, Chen D, Ye W, Zhan C
Infection and Drug Resistance 2023, 16:4717-4728
Published Date: 20 July 2023
Knowledge, Attitudes, and Practices Among Middle-Aged and Elderly Population Towards Ultrasound Screening for Strokes
Wang W, Peng Y, Tang K, Zheng Z, He L, Yang S
Journal of Multidisciplinary Healthcare 2024, 17:147-157
Published Date: 9 January 2024
Knowledge, Attitude, and Practice of Anesthetists in Managing Severe Craniocerebral Trauma in China: A Cross-Sectional Study
Zha C, Che X, Xiong L, Ji Y, Zhang G
International Journal of General Medicine 2025, 18:1035-1046
Published Date: 25 February 2025
Family Members’ Perspectives on Integrative Chinese-Western Medicine in Cancer Care
Sun T, Wang T, Xia F, Xia L, Sun X, Jiang H, Xu P, Li P
Journal of Multidisciplinary Healthcare 2025, 18:2361-2373
Published Date: 28 April 2025