Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Parental Knowledge, Attitudes, and Practices Regarding Low-Temperature Plasma Adenotonsillectomy for Pediatric Obstructive Sleep Apnea Syndrome: A Structural Equation Modeling Analysis
Authors Shi B, Mao R, Fang J, Wu Y ![]() , Liu F, Xiang S, Xia S
, Liu F, Xiang S, Xia S
Received 24 October 2025
Accepted for publication 4 March 2026
Published 28 March 2026 Volume 2026:19 576607
DOI https://doi.org/10.2147/JMDH.S576607
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Linda Yoder
Bowen Shi,1,* Ruotong Mao,1,* Jianjing Fang,2,* Yixin Wu,3 Fanli Liu,1 Songjie Xiang,1 Siwen Xia1
1Department of Otolaryngology Head & Neck Surgery, The Second Affiliated Hospital and Yuying Children’s Hospital, Wenzhou Medical University, Wenzhou, Zhejiang, 325027, People’s Republic of China; 2Department of Ultrasonography, Wuma Street Community Health Service Center of Lucheng District, Wenzhou, Zhejiang, 325000, People’s Republic of China; 3Alberta Institute, Wenzhou Medical University, Wenzhou, Zhejiang, 325035, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Siwen Xia, Email [email protected]
Background: To investigate parental knowledge, attitudes, and practices (KAP) regarding low-temperature plasma adenotonsillectomy for children with obstructive sleep apnea syndrome (OSAS).
Methods: This cross-sectional study employed a self-administered KAP questionnaire for data collection from parents of children with OSAS at the Second Affiliated Hospital of Wenzhou Medical University, spanning August, 2023, to August, 2024.
Results: A total of 415 parents were included, with 83.86% were female and 84.34% being primary caregivers. The knowledge, attitude, and practice scores were 14.91 ± 2.40 (total score: 18 points), 31.87 ± 3.12 (total score: 35 points), and 32.01 ± 3.15 (total score: 35 points), respectively. Knowledge positively correlated with attitude (r = 0.365, P < 0.001), and practices (r = 0.336, P < 0.001). Attitude correlated with practice (r = 0.745, P < 0.001). Structural equation modelling revealed that knowledge influenced attitude (β = 0.490, P < 0.001), and attitude strongly impacted practice (β = 0.729, P < 0.001).
Conclusion: Parents demonstrated adequate knowledge, positive attitudes, and proactive practices regarding low-temperature plasma surgery. This underscores the clinical value of incorporating structured parental education and counseling into perioperative care to support adherence and improve recovery in children with OSAS. These findings warrant continued, targeted health education focused on knowledge gaps to further enhance treatment compliance and optimize postoperative outcomes for children with OSAS.
Keywords: obstructive sleep apnea syndrome, tonsillectomy, adenoidectomy, knowledge, attitudes, practice, cross-sectional study
Introduction
Pediatric obstructive sleep apnea syndrome (OSAS), a prevalent disorder, is characterized by recurrent partial or complete upper airway obstruction during sleep, resulting in abnormal ventilation and fragmented sleep.1 Its prevalence, estimated at 1% to 5.8%, is projected to increase due to the ongoing obesity epidemic.2,3 Since adenotonsillar or adenoid hypertrophy is the most prominent etiology, adenotonsillectomy remains the first-line treatment.4 Low-temperature plasma radiofrequency ablation, also referred to as low-temperature plasma adenotonsillectomy, represents a minimally invasive surgical technique that has been increasingly applied in the treatment of OSAS. Operating at a temperature range of 40–70°C, this approach minimizes thermal damage to surrounding healthy tissues, aligning with the principles of minimally invasive surgery while offering advantages such as precise excision and reduced intraoperative bleeding.2 These attributes make low-temperature plasma surgery an effective and safe option for pediatric patients.
Despite the advantages of low-temperature plasma surgery, postoperative complications such as bleeding and infection may still occur. Effective parental involvement in postoperative care plays a critical role in reducing these risks; however, existing caregiver education remains limited and inconsistent. The knowledge, attitude, and practice (KAP) model postulates that individual’s practice are influenced by their knowledge and attitudes. KAP surveys are widely used to assess knowledge, perceptions, and practices, thereby offering insights into health-related behaviors and decision-making processes.5,6 Within the context of pediatric OSAS, parental KAP is particularly important, as parents serve as the primary caregivers and are directly responsible for adhering to preoperative and postoperative care protocols. Their understanding and engagement have a profound impact on the surgical outcomes and long-term health of their children.
Despite the importance of this topic, to our knowledge, no studies have specifically examined the KAP of parents regarding low-temperature plasma adenotonsillectomy for the treatment of pediatric OSAS. This study aims to evaluate parental KAP and to analyze the relationships and influencing factors among these components.
Methods
Study Design and Subjects
This cross-sectional study investigated the parental KAP regarding low-temperature plasma adenotonsillectomy in children with OSAS. The study was conducted at the Second Affiliated Hospital and Yuying Children’s Hospital, Wenzhou Medical University from August, 2023, to August, 2024. The study was approved by the Medical Ethics Committee of the Second Affiliated Hospital and Yuying Children’s Hospital, Wenzhou Medical University, and informed consent was obtained from all participants. Parents were included if their child: 1) was aged 1–18 years; 2) was hospitalized with an OSAS diagnosis; and 3) was undergoing low-temperature plasma adenotonsillectomy. The diagnosis of pediatric OSAS in this study was established based on overnight polysomnography, in accordance with current clinical practice guidelines. Patients were excluded if they were over 18 years of age; were undergoing coblation surgery for conditions unrelated to OSAS; had other chronic diseases or acute upper respiratory infections; or were unable to complete scheduled postoperative follow-up visits.
Procedures
The questionnaire was designed based on relevant guidelines and literature, with modifications made after consultation with five experts specializing in otolaryngology and throat and neck conditions. Following the initial draft, the questionnaire underwent three rounds of pilot testing and iterative adjustments. The final pilot yielded a Cronbach’s α of 0.870, confirming good internal consistency. The finalized version comprised four sections: demographic data (including basic information about the children and their families), a knowledge dimension, an attitude dimension, and a practice dimension.
The questionnaire is provided in Figure S1. The knowledge dimension included two subcategories with a total of 9 questions. Correct answers were awarded 2 points, while incorrect or unclear responses received 0 points, resulting in a total possible score ranging from 0 to 18 points. The attitude dimension consisted of 7 questions assessed on a five-point Likert scale, ranging from very positive (5 points) to very negative (1 point), with a total score range of 7–35 points. Similarly, the practice dimension included 7 questions, also rated on a five-point Likert scale, ranging from always (5 points) to never (1 point), yielding a total score range of 7–35 points.
Our self-designed questionnaire was imported into the SoJump platform (SoJump.com; wjx.cn) to create its electronic version, and a QR code was generated for convenient access. Two extensively trained senior nurses served as research assistants to facilitate the distribution of the questionnaire. The link to the questionnaire and its QR code were disseminated to participants through WeChat groups, display boards, and consultation rooms. Participants could access the questionnaire by scanning the QR code, and each IP address was restricted to a single submission to ensure that each participant submitted only once. The questionnaire was completed anonymously, and participants were informed that there were no right or wrong answers and that their responses would be used solely for research purposes, in order to minimize social desirability and response bias. Additionally, members of the research team reviewed all submissions for completeness, internal consistency, and logical coherence.
Sample Size Calculation
We determined the minimum required sample size (n) using the standard formula for cross-sectional studies:

The value of p was set to 0.5 because it yields the maximum variance and therefore provides a conservative estimate to ensure adequate sample size when the true population proportion is unknown. The Type I error (α) was set to 0.05, corresponding to a Z-score of 1.96 (for a 95% confidence level). The standard error (δ) was set at 0.05. Substituting these values yields a required sample size of 384. Assuming an effective questionnaire recovery rate of 90%, the final target is to collect at least 430 completed questionnaires. In addition, the final sample size of 415 also satisfied the recommended sample size requirements for Structural Equation Modeling (SEM), which generally suggest a minimum of 200 participants or a sample size equivalent to 10–20 times the number of estimated parameters.
Statistical Analysis
Data analysis was conducted using SPSS 27.0 (IBM, Armonk, NY, USA) and AMOS 26.0 (IBM, Armonk, NY, USA). Descriptive statistics were used to analyze demographic data and KAP (knowledge, attitude, and practice) scores. Continuous variables were tested for normality using the Shapiro–Wilk test. As the knowledge, attitude, and practice scores did not follow a normal distribution (all P < 0.001), continuous variables are presented as medians and interquartile ranges (IQR), while categorical variables are expressed as n (%). Differences in KAP scores among respondents with different demographic characteristics were analyzed using the Mann–Whitney U-test for comparisons between two groups and the Kruskal–Wallis H-test for comparisons among three or more groups. Spearman rank correlation analysis was performed to assess the relationships among the knowledge, attitude, and practice dimensions. These relationships were further validated using structural equation modeling (SEM). The scores for each dimension were dichotomized into high and low groups based on a cutoff of 80% of the maximum score and used as the dependent variable for the logistic regression analysis. Variables demonstrating statistical significance in the univariate analysis (P<0.05) were subsequently included in multivariable logistic regression analysis. A two-sided P-value less than 0.05 was considered statistically significant.
Results
Demographic Information
After excluding 124 invalid questionnaires, the final analysis included 415 valid questionnaires, achieving a total effective response rate of 77.0% (Figure S2). The majority of parents 348 (83.86%) were female, 275 (66.27%) were aged 30–39 years, 350 (84.34%) were the primary caregiver for the patient after surgery, with the majority residing in urban or suburban areas 229 (57.35%), 186 (44.82) lived in rural, 209 (50.36%) held an associate/bachelor’s degree or higher, and 137 (33.01%) had previous experience caring for children after tonsil or adenoid surgery. Among the children, 262 (63.13%) were boys, 229 (55.18%) were over 7 years old, 237 (57.11%) were firstborns, 320 (77.11%) experienced postoperative sore throat, and 222 (53.49%) had postoperative fever. The mean duration of fever was 2.55 ± 2.85 days, with a mean maximum temperature of 38.29 ± 1.15°C (Table 1).
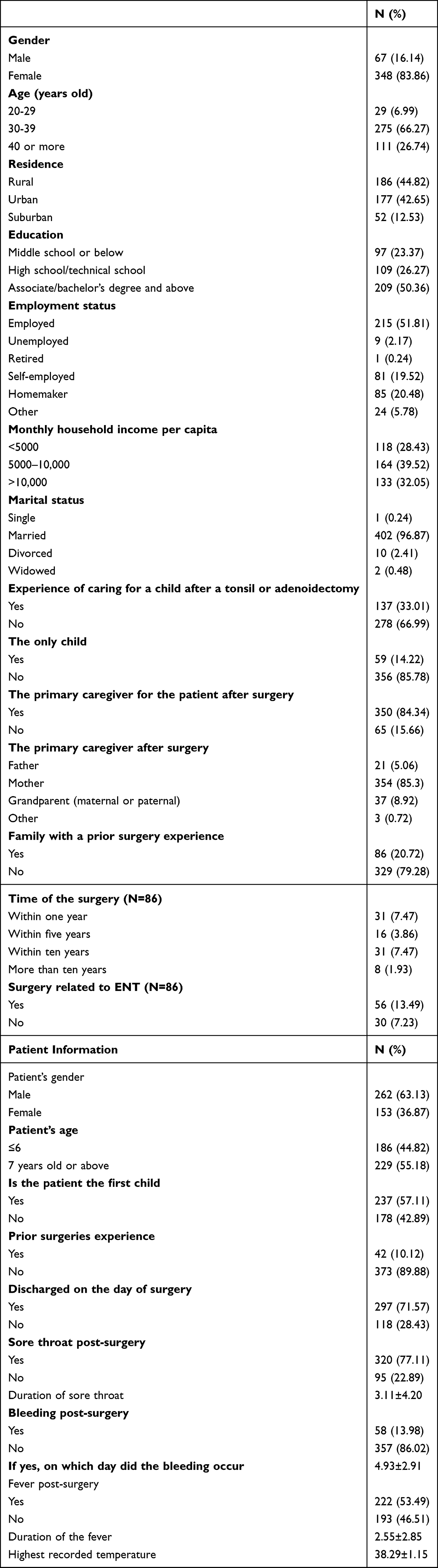 |
Table 1 Basic Information of Participants |
Parents demonstrated adequate knowledge (median: 16.00, IQR: 14.00–16.00), positive attitudes (median: 33.00, IQR: 29.00–35.00), and proactive practices (median: 33.00, IQR: 28.00–35.00) regarding low-temperature plasma surgery (Table 2).
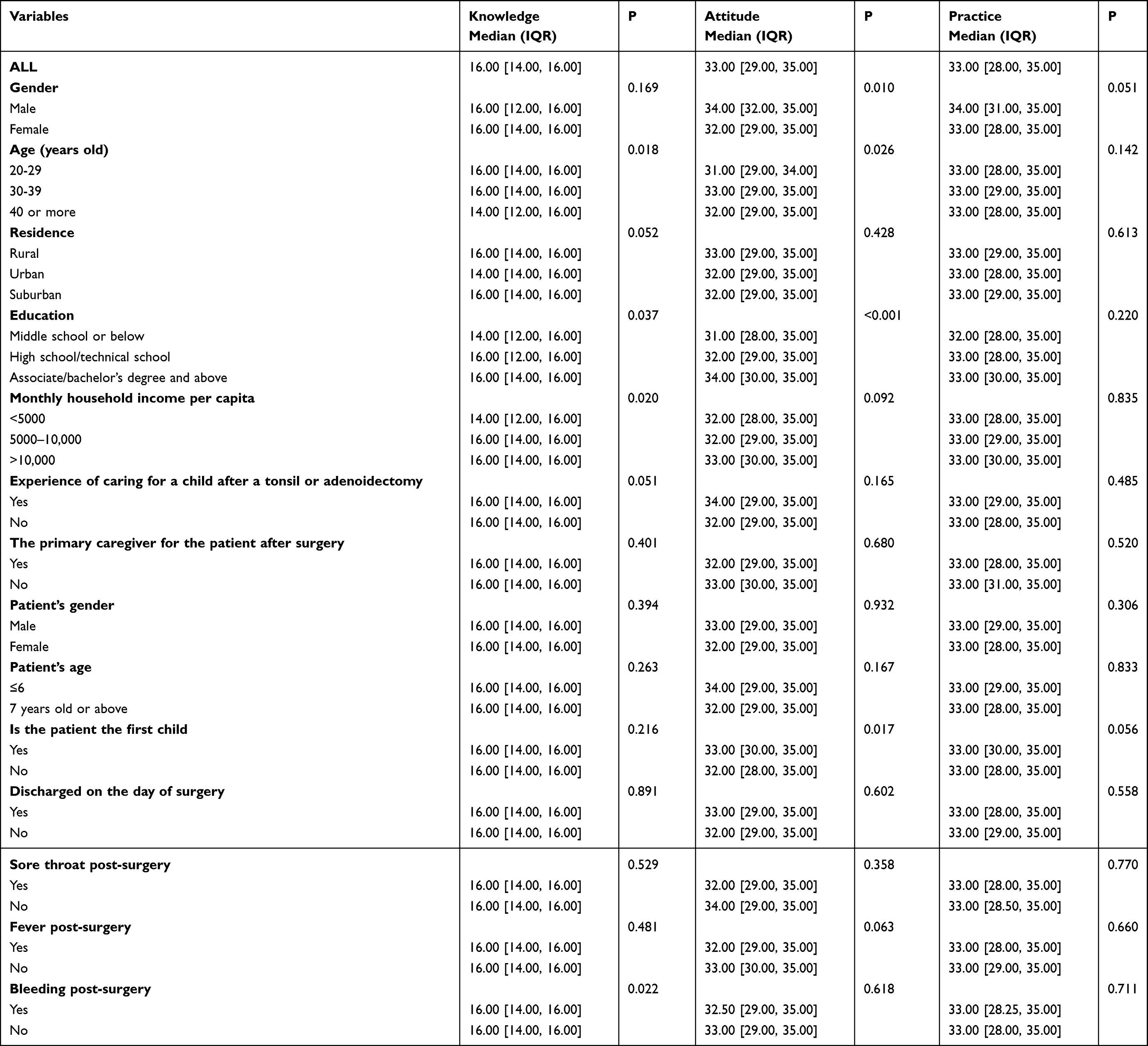 |
Table 2 KAP Score of the Participants |
Knowledge, Attitude, and Practice Distribution
In the knowledge dimension, the lowest correctness rates were observed for: “Surgery can be performed during the acute phase of tonsillitis, upper respiratory infections, or other infectious diseases” (K4, 27.71%) and “Tonsil and adenoid hypertrophy may cause swallowing difficulties, leading to nutritional deficiencies and unclear speech” (K2, 57.83%). In the attitude dimension, 7.71% of participants were neutral about satisfaction with their child’s postoperative recovery process (A5), and 5.78% were neutral about their optimism regarding recovery prospects. In the practice dimension, within 14 days post-surgery, 11.81% of children were not consistently having their temperature monitored (P2), and 9.64% were not adhering daily to a semi-liquid diet (Table S1).
Correlation Analysis
Correlation analysis revealed significant positive associations between knowledge and attitude (r = 0.365, P < 0.001), and between knowledge and practice (r = 0.336, P < 0.001). A strong correlation was also observed between attitude and practice (r = 0.745, P < 0.001) (Table 3).
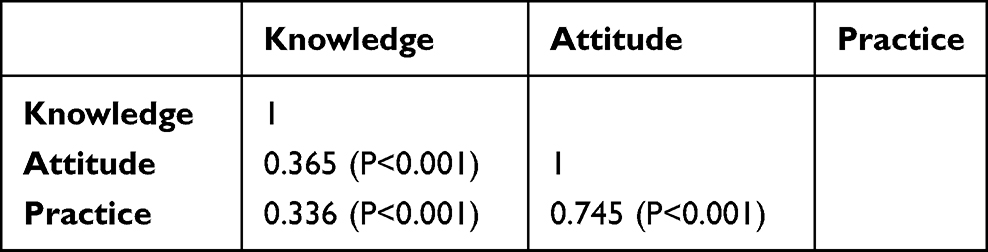 |
Table 3 Correlation Analysis |
Structural Equation Modeling Analysis
SEM demonstrated excellent model fit (CMIN/DF = 2.591, RMSEA = 0.062, IFI = 0.902, TLI = 0.888, CFI = 0.901) (Table 4). The results indicated that knowledge directly influenced attitude (β = 0.490, P < 0.001), and attitude had a direct impact on practice (β = 0.729, P < 0.001) (Table 5 and Figure 1).
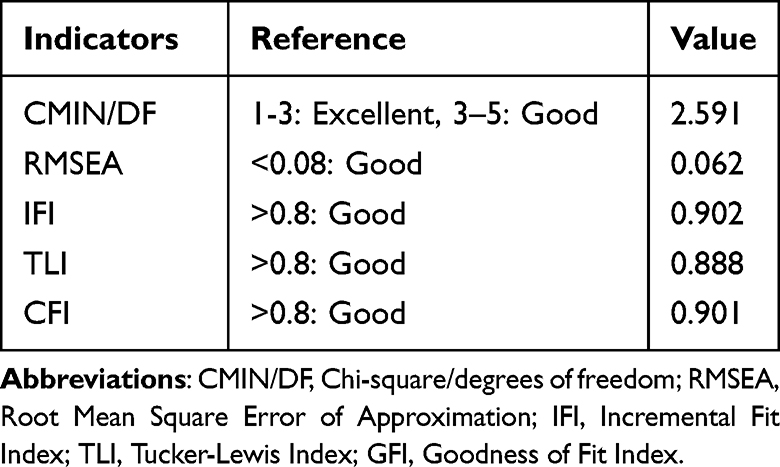 |
Table 4 Structural Equation Modeling Fit Indices |
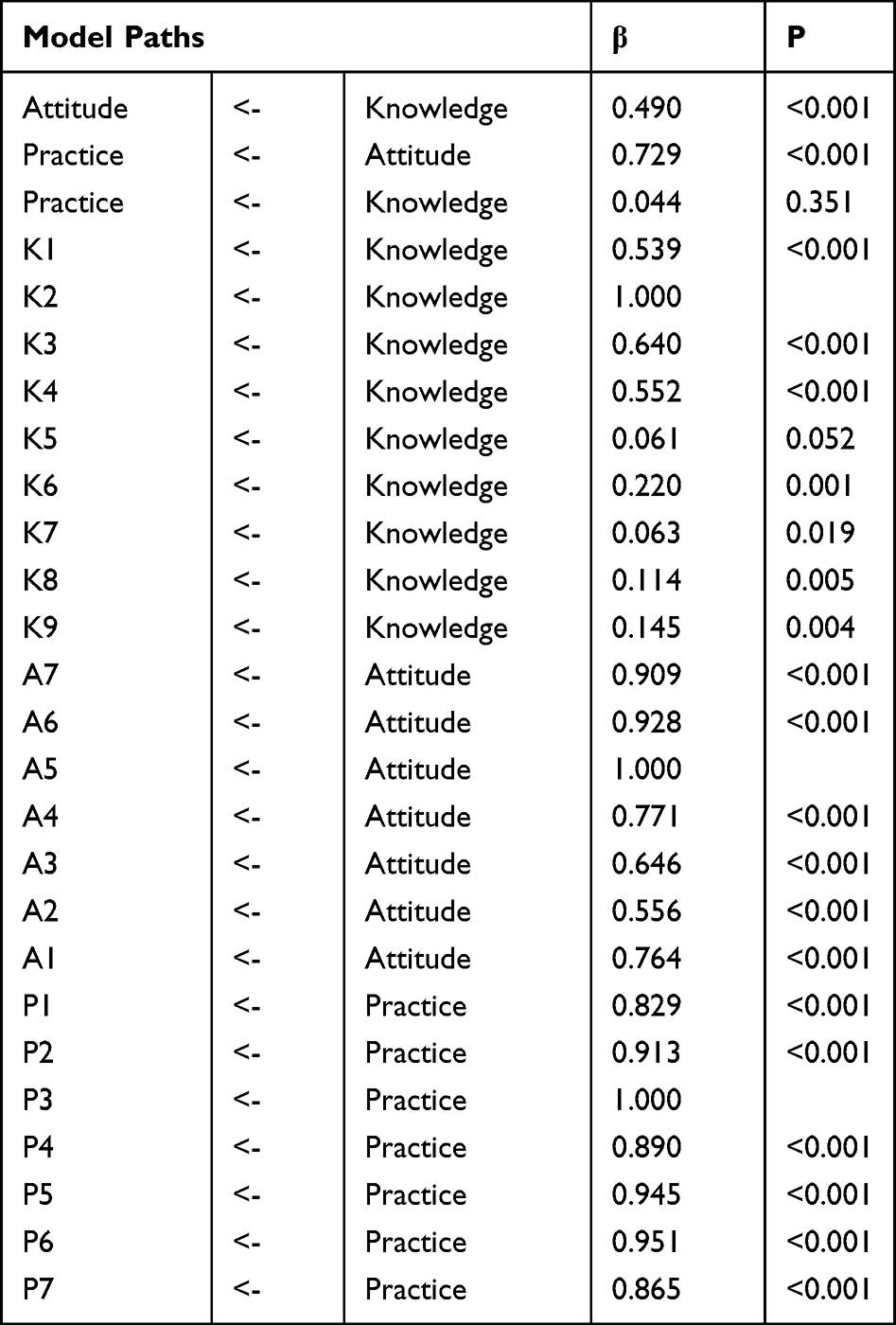 |
Table 5 Structural Equation Modeling Results |
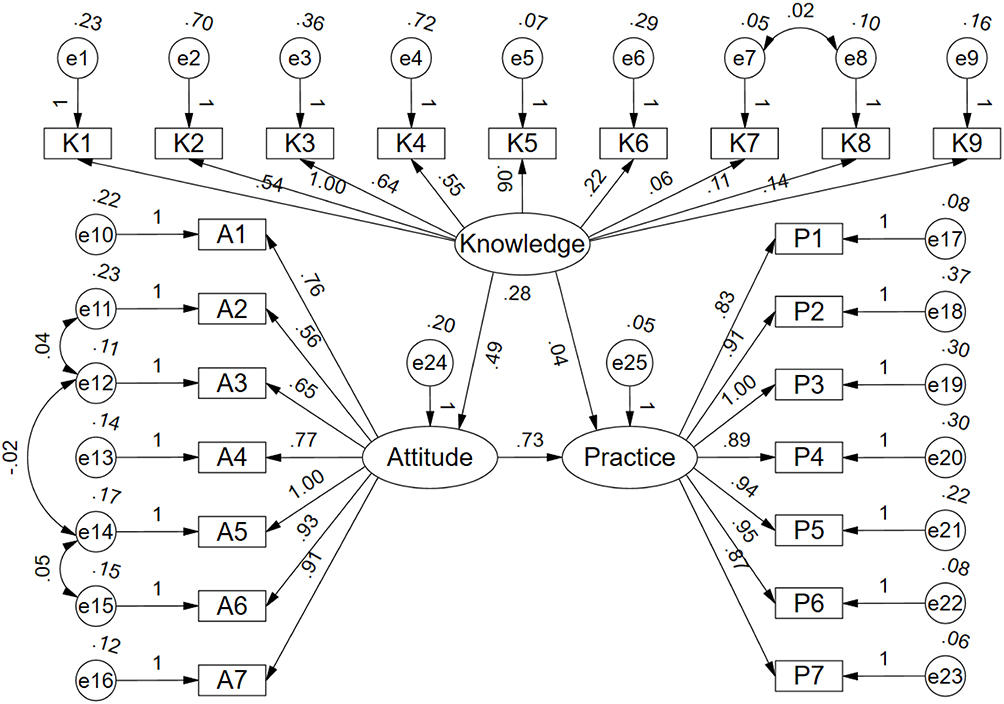 |
Figure 1 Structural Equation Model (SEM) illustrating the relationships among knowledge, attitude, and practice. Rectangles represent observed variables (questionnaire items), ellipses represent latent variables, and circles indicate error terms or residuals. Single-headed arrows denote hypothesized directional pathways between variables, with standardized path coefficients shown along each path. |
Multivariable Logistic Regression Analysis
Multivariable logistic regression showed that aged 40 years or more (OR = 0.304, 95% CI: [0.122, 0.760], P = 0.011), urban (OR = 0.537, 95% CI: [0.347, 0.831], P = 0.005), and associate/bachelor’s degree and above (OR = 1.779, 95% CI: [1.066, 2.971], P = 0.028) were independently associated with knowledge (Table S2). Meanwhile, knowledge score (OR = 1.284, 95% CI: [1.156, 1.427], P < 0.001) and associate/bachelor’s degree and above (OR = 2.748, 95% CI: [1.383, 5.460], P = 0.004) were independently associated with positive attitude (Table S3). Moreover, attitude score (OR = 1.993, 95% CI: [1.712, 2.320], P < 0.001) was independently associated with proactive practice (Table S4).
Discussion
Parents of children with OSAS demonstrated adequate knowledge, positive attitudes, and proactive practices toward low-temperature plasma adenotonsillectomy. Enhancing educational efforts targeting parents, particularly those with lower educational attainment, older parents, and parents in families with multiple children may further improve practices and optimize postoperative outcomes in pediatric OSAS management.
Notable deficiencies in specific aspects of knowledge and practice highlight areas for improvement. For instance, many parents lacked understanding of the risks of performing surgery during acute infections and the nutritional implications of tonsil and adenoid hypertrophy. These findings are consistent with previous studies that demonstrated similar knowledge gaps among caregivers in surgical and pediatric contexts.7,8 Such deficiencies are critical, as inadequate knowledge has been linked to lower adherence to postoperative care protocols and delayed medical intervention.9,10 These gaps may partly explain why some children continue to experience prolonged recovery periods or suboptimal health outcomes despite advances in surgical techniques.
The correlation analysis and SEM results demonstrated strong interconnections among the KAP dimensions. Knowledge directly influenced attitudes, which, in turn, had a substantial impact on practices. This mediating role of attitudes has been emphasized in previous studies, which suggest that attitudes often serve as the bridge between knowledge and practice.11,12 The absence of a significant direct effect of knowledge on practice in the SEM model further supports the notion that cultivating positive attitudes is essential to translating knowledge into actionable practices. This pattern is consistent with the classical KAP theoretical framework, which emphasizes attitude as a critical mediating pathway through which knowledge is transformed into sustained behavioral change, as has been demonstrated in previous health behavior study.13 For example, parents with greater confidence in their child’s recovery process were more likely to adhere to postoperative guidelines, a pattern documented in similar studies of parental caregiving in pediatric surgery.14,15 These findings underscore the importance of integrating attitude-focused interventions, such as counseling or peer support, into educational programs.
Significant differences in KAP scores were observed across demographic variables, with Multivariable analysis supporting the role of age, residence, and education in shaping knowledge and attitudes. Older parents (≥40 years) had lower knowledge scores compared to younger parents, potentially due to less exposure to contemporary health education resources or lower familiarity with digital health tools. This trend aligns with studies suggesting that older caregivers may face barriers in accessing up-to-date medical information.16,17 Urban parents also demonstrated lower knowledge scores compared to rural parents, a finding that contrasts with conventional assumptions about urban populations having greater access to healthcare resources. One possible explanation is that rural caregivers might rely more heavily on direct communication with healthcare providers, leading to better knowledge retention.
Higher education levels were consistently associated with better knowledge and attitudes, highlighting the critical role of formal education in fostering health literacy. This finding is consistent with numerous studies linking educational attainment to improved health practices and outcomes.18,19 Interestingly, gender differences were observed in attitudes but not in knowledge or practice. Mothers generally reported more positive attitudes than fathers, which may reflect their primary caregiving role and closer emotional engagement with their child’s health.20,21 However, the lack of gender differences in knowledge and practice suggests that both parents receive similar exposure to postoperative instructions, possibly due to standardized communication by healthcare providers. These patterns indicate that while standardized education benefits both parents, tailored interventions may be needed to further engage fathers and older caregivers.
Parental knowledge demonstrated strong awareness of routine postoperative care, specifically dietary guidelines and activity restriction. However, understanding was deficient regarding surgical risks during acute infections and the long-term developmental impact of tonsil/adenoid hypertrophy. Other studies document similar gaps, where caregivers prioritize immediate postoperative concerns over long-term implications.22,23 In adherence to key recommendations, such as temperature monitoring and a semi-liquid diet, was inconsistent. These shortcomings may reflect logistical challenges, such as balancing caregiving responsibilities with work, or a lack of perceived importance for certain recommendations. Research on postoperative care in pediatric contexts has similarly identified practical barriers as significant contributors to non-adherence.24,25
Educational materials must be redesigned to specifically target the identified knowledge deficits.26 Preoperative consultations should include distributing brief, illustrated handouts or videos that explain the necessity of deferring surgery during acute infections and detail the developmental risks of untreated OSAS. These materials must also provide actionable postoperative care tips, including clear instructions for temperature monitoring and dietary management. To improve attitudes, providers should implement group counseling sessions where parents share experiences and receive emotional support. Incorporating testimonials from successful family cases can enhance parental confidence and optimism, thereby facilitating adherence to care protocols. Additionally, tailored workshops or campaigns specifically targeting fathers to emphasize their role in caregiving could improve family health outcomes.27,28 Automated reminders via text or mobile applications can promote consistent temperature monitoring and dietary adherence. Furthermore, providers can introduce postoperative care checklists for parents to track compliance. For families facing logistical challenges, offering home-based follow-up visits or telemedicine consultations provides crucial support.29,30 Finally, interventions must consider demographic disparities: health education for older caregivers may require incorporating user-friendly digital tools or in-person workshops, while urban caregivers, despite proximity to services, may benefit from personalized counseling to enhance engagement with medical advice. In addition, regional healthcare infrastructure, hospital management practices, and local cultural attitudes toward pediatric surgery may influence parental behaviors and care patterns, which should be considered when extrapolating these findings to other clinical settings or healthcare systems.
This study has several limitations. First, detailed information regarding previous non-surgical treatments for pediatric OSAS (such as medication use, nasal corticosteroids, or continuous positive airway pressure therapy) was not systematically collected, which may have influenced parental perceptions and behaviors. However, children with a history of prior adenotonsillectomy were excluded to reduce potential confounding effects related to previous surgical treatment. Second, as a cross-sectional study, it cannot establish causal relationships between knowledge, attitudes, and practices, or the factors influencing them. Third, the data were collected from a single hospital, which may limit the generalizability of the findings to other settings or populations. In particular, regional differences in healthcare infrastructure, hospital management practices, and access to postoperative support services may introduce potential geographic bias. Moreover, cultural beliefs regarding pediatric surgery and variations in healthcare delivery systems may influence parental decision-making and caregiving behaviors, which should be considered when applying these findings to other regions or countries. Fourth, the self-reported nature of the questionnaire may introduce response bias, as participants might overestimate their knowledge or report socially desirable practices rather than actual practices. In addition, clinical symptom indicators such as daytime sleepiness, cognitive impairment, or functional and behavioral disturbances related to OSAS were not systematically assessed, which may have influenced parental perceptions and responses to the questionnaire. Although anonymity, standardized Likert-scale items, and neutral questionnaire instructions were used to reduce this potential bias, it cannot be completely eliminated. Future studies should address these limitations by incorporating longitudinal designs, expanding the study population, and using objective measures of parental practices.
Parents of children with OSAS demonstrated adequate knowledge, positive attitudes, and proactive practices regarding low-temperature plasma adenotonsillectomy, with clear interrelationships among the KAP dimensions. Targeted educational interventions focusing on enhancing parental knowledge and fostering positive attitudes may further improve postoperative care practices, particularly in populations with lower educational attainment or limited prior experience. Although this study was conducted at a single center, the findings provide practical clinical insights that may inform parental education strategies in similar pediatric surgical settings.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
This study was approved by the ethic committee of the Second Affiliated Hospital and Yuying Children’s Hospital, Wenzhou Medical University (2023-K-102-1), I confirm that all methods were performed in accordance with the relevant guidelines. All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments, and obtain written informed consent from all participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Fundamental Research Project of Wenzhou City (Y20240051).
Disclosure
All authors declare that they have no conflicts of interest in this work.
References
1. Bitners AC, Arens R. Evaluation and management of children with obstructive sleep apnea syndrome. Lung. 2020;198(2):257–13. doi:10.1007/s00408-020-00342-5
2. Chinese M. Clinical practice guidelines for standardized low-temperature plasma radiofrequency ablation tonsillectomy and adenoidectomy in children. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2021;35(3):193–199. doi:10.13201/j.issn.2096-7993.2021.03.001
3. Tsukada E, Kitamura S, Enomoto M, et al. Prevalence of childhood obstructive sleep apnea syndrome and its role in daytime sleepiness. PLoS One. 2018;13(10):e0204409. doi:10.1371/journal.pone.0204409
4. Di Mauro P, Cocuzza S, Maniaci A, et al. The effect of adenotonsillectomy on children’s behavior and cognitive performance with obstructive sleep apnea syndrome: state of the art. Children. 2021;8(10). doi:10.3390/children8100921
5. Tahani B, Manesh SS. Knowledge, attitude and practice of dentists toward providing care to the geriatric patients. BMC Geriatr. 2021;21(1):399. doi:10.1186/s12877-021-02343-2
6. Tousif K, Saeed S, Hamid S, et al. The relationship between knowledge, attitude, and practice of plasma donation with age and gender as moderators: a cross-sectional survey. Ann Med Surg Lond. 2023;85(5):1594–1600. doi:10.1097/MS9.0000000000000121
7. Markiewicz-Gospodarek A, Kozioł M, Tobiasz M, Baj J, Radzikowska-Büchner E, Przekora A. Burn wound healing: clinical complications, medical care, treatment, and dressing types: the current state of knowledge for clinical practice. Int J Environ Res Public Health. 2022;19(3):1338. doi:10.3390/ijerph19031338
8. Morgan RW, Kirschen MP, Kilbaugh TJ, Sutton RM, Topjian AA. Pediatric in-hospital cardiac arrest and cardiopulmonary resuscitation in the United States: a review. JAMA Pediatr. 2021;175(3):293–302. doi:10.1001/jamapediatrics.2020.5039
9. Di Nardo M, Tikkanen J, Husain S, et al. Postoperative management of lung transplant recipients in the intensive care unit. Anesthesiology. 2022;136(3):482–499. doi:10.1097/ALN.0000000000004054
10. Gizaw MA, Negawo MK, Bala ET, Daba DB. Knowledge, practice, and associated factors towards postoperative wound care among nurses working in public hospitals in Ethiopia: a multicenter cross-sectional study in low resource setting area. Health Sci Rep. 2022;5(4):e677. doi:10.1002/hsr2.677
11. Halloy A, Simon E, Hejoaka F. Defining patient’s experiential knowledge: who, what and how patients know. A narrative critical review. Sociol Health Illn. 2023;45(2):405–422. doi:10.1111/1467-9566.13588
12. Sobeck J, Smith-Darden J, Gartner D, et al. Antibiotic knowledge, beliefs, and behaviors: testing competing hypotheses using an urban community sample. Health Commun. 2022;37(7):862–871. doi:10.1080/10410236.2021.1875557
13. Zhang X, Zhang M, Li T, et al. Knowledge, attitudes, and practice (KAP) of old age mental health among Chinese medical undergraduate students: a cross-sectional study. BMC Med Educ. 2025;25(1):814. doi:10.1186/s12909-025-07363-9
14. Bach Q, Thomale UW, Müller S. Parents’ and children’s decision-making and experiences in pediatric epilepsy surgery. Epilepsy Behav. 2020;107:107078. doi:10.1016/j.yebeh.2020.107078
15. Wu JM, Tam MT, Page PM, et al. Pain management communication between parents and nurses after pediatric outpatient surgery. J Pediatr Nurs. 2022;65:e87–e92. doi:10.1016/j.pedn.2022.03.008
16. Hall S, Rohatinsky N, Holtslander L, Peacock S. Caregivers to older adults require support: a scoping review of their priorities. Health Soc Care Community. 2022;30(6):e3789–e3809. doi:10.1111/hsc.14071
17. Petrovic M, Gaggioli A. Digital mental health tools for caregivers of older Adults-A scoping review. Front Public Health. 2020;8:128. doi:10.3389/fpubh.2020.00128
18. Kondirolli F, Sunder N. Mental health effects of education. Health Econ. 2022;31 Suppl 2(Suppl 2):22–39. doi:10.1002/hec.4565
19. Stormacq C, Van den Broucke S, Wosinski J. Does health literacy mediate the relationship between socioeconomic status and health disparities? Integrative review. Health Promot Int. 2019;34(5):e1–e17. doi:10.1093/heapro/day062
20. Augustine JM. Mothers’ out-of-sequence postsecondary education and their health and health behaviors. J Health Soc Behav. 2021;62(1):2–18. doi:10.1177/0022146520979664
21. Hydery T, Shields S, Hen E, Rizzo P, Sullivan K, Savageau JA. The impact of local education and resource distribution on maternal health behaviors. Matern Child Health J. 2022;26(8):1676–1688. doi:10.1007/s10995-022-03416-3
22. Giordano CN, Mori S, Navarrete-Dechent C, et al. Patient concerns in the immediate postoperative period after Mohs micrographic surgery. Dermatol Surg. 2020;46(4):514–518. doi:10.1097/DSS.0000000000002116
23. Zhou K, Wang W, Zhao W, et al. Benefits of a WeChat-based multimodal nursing program on early rehabilitation in postoperative women with breast cancer: a clinical randomized controlled trial. Int J Nurs Stud. 2020;106:103565. doi:10.1016/j.ijnurstu.2020.103565
24. Floridis J, Barbour R. Postoperative weakness and anesthetic-associated rhabdomyolysis in a pediatric patient: a case report and review of the literature. J Med Case Rep. 2022;16(1):387. doi:10.1186/s13256-022-03629-8
25. Guerriero RM, Guilliams KP. Pediatric Neurocritical Care: from Field to Follow-Up. Pediatr Neurol. 2020;108:1–2. doi:10.1016/j.pediatrneurol.2019.09.006
26. Shenoy VS, Samanth R, Parvathareddy N, Apoorva KV. Pediatric oronasopharyngeal stricture- a rare surgical complication of adeno-tonsillectomy abstract. Indian J Otolaryngol Head Neck Surg. 2023;75(3):2352–2354. doi:10.1007/s12070-023-03694-5
27. Fisher SD, Glangeaud-Freudenthal N. Fathers as assets to support maternal mental health and family wellbeing. Arch Womens Ment Health. 2023;26(1):87–88. doi:10.1007/s00737-023-01292-6
28. Latomme J, Morgan PJ, Chastin S, Brondeel R, Cardon G. Effects of a family-based lifestyle intervention on co-physical activity and other health-related outcomes of fathers and their children: the ‘Run Daddy Run’ intervention. BMC Public Health. 2023;23(1):342. doi:10.1186/s12889-023-15191-z
29. Noroozzadeh M, Amiri M, Farhadi-Azar M, Ramezani Tehrani F. Bone health in women with polycystic ovary syndrome: a narrative review. J Clin Densitom. 2022;25(4):606–614. doi:10.1016/j.jocd.2022.02.005
30. Zhou S, Jin CY, Guo J, et al. The relationship between online courses and mental health among Chinese children. BMC Psychiatry. 2022;22(1):328. doi:10.1186/s12888-022-03976-2
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Psychiatric Nurses’ Knowledge, Attitudes, and Practice Regarding Physical Restraint in China: A Multicentre Cross-Sectional Study
Chong Y, Wang C, Zhi T, Fang S, Min H, Zhang L, Wu X, Wang Y
Journal of Multidisciplinary Healthcare 2023, 16:1475-1489
Published Date: 29 May 2023
Assessing the Knowledge, Attitudes, and Vaccination Practices Towards COVID-19 Vaccination Among Mainland Chinese Nursing Students and Interns: A Multicenter Cross-Sectional Study

Qin Z, Ye X, Liu H, Tao Y, Zheng X, Zhong Y, Chen D, Ye W, Zhan C
Infection and Drug Resistance 2023, 16:4717-4728
Published Date: 20 July 2023
Knowledge, Attitudes and Practices Towards Psoriasis Among Patients and Their Family Members
Zhang X, Du H, Liu X, Liu L, Zhang T
Clinical, Cosmetic and Investigational Dermatology 2024, 17:769-782
Published Date: 3 April 2024
Knowledge, Attitude and Practice of Radiologists Regarding Artificial Intelligence in Medical Imaging
Huang W, Li Y, Bao Z, Ye J, Xia W, Lv Y, Lu J, Wang C, Zhu X
Journal of Multidisciplinary Healthcare 2024, 17:3109-3119
Published Date: 4 July 2024
Family Members’ Perspectives on Integrative Chinese-Western Medicine in Cancer Care
Sun T, Wang T, Xia F, Xia L, Sun X, Jiang H, Xu P, Li P
Journal of Multidisciplinary Healthcare 2025, 18:2361-2373
Published Date: 28 April 2025