Back to Journals » Infection and Drug Resistance » Volume 19
Interim Effectiveness and Safety of Prolonged Bedaquiline Use in Comparison to Standard 24-Week Treatment for MDR-TB: A Multicenter Cohort Study in China
Authors Hu X, Gao M, Liu Y ![]() , Pei Y, Du J, Wu G, Wang A, Li L, Gao J
, Pei Y, Du J, Wu G, Wang A, Li L, Gao J
Received 7 November 2025
Accepted for publication 26 February 2026
Published 10 March 2026 Volume 2026:19 572423
DOI https://doi.org/10.2147/IDR.S572423
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hemant Joshi
Xinyang Hu,1,* Mengqiu Gao,2,* Yuhong Liu,3,* Yi Pei,4,* Juan Du,5,* Guihui Wu,6,* Aidi Wang,7,* Liang Li,3 Jingtao Gao1
1GCP Administration Office, Beijing Chest Hospital, Capital Medical University/Beijing Tuberculosis & Thoracic Tumor Research Institute, Beijing, People’s Republic of China; 2Department of Tuberculosis, Beijing Chest Hospital, Capital Medical University/Beijing Tuberculosis and Thoracic Tumor Research Institute, Beijing, People’s Republic of China; 3Clinical Center on TB, Beijing Chest Hospital, Capital Medical University/Beijing Tuberculosis & Thoracic Tumor Research Institute, Beijing, People’s Republic of China; 4Department of Tuberculosis, Changsha Central Hospital, Changsha, People’s Republic of China; 5Department of Tuberculosis, Wuhan Pulmonary Hospital, Wuhan, People’s Republic of China; 6Department of Tuberculosis, Chengdu Public Health Clinical Centre, Chengdu, People’s Republic of China; 7Department of Tuberculosis, Shenyang Chest Hospital, Shenyang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jingtao Gao, Beijing Chest Hospital, Capital Medical University/Beijing Tuberculosis & Thoracic Tumor Research Institute, GCP Administration Office, No. 9 Beiguan Street, Tongzhou District, Beijing, 101149, People’s Republic of China, Email [email protected] Liang Li, Beijing Chest Hospital, Capital Medical University/Beijing Tuberculosis & Thoracic Tumor Research Institute, Clinical Center on TB, No. 9 Beiguan Street, Tongzhou District, Beijing, 101149, People’s Republic of China, Email [email protected]
Purpose: Limited evidence exists regarding impacts of prolonged bedaquiline use in the treatment of multidrug-resistant (MDR) tuberculosis (TB). This study evaluated the effectiveness and safety of prolonged bedaquiline use (> 24 weeks) compared to the standard 24-week in MDR/extensively drug-resistant (XDR)-TB treatment with longer regimen.
Patients and Methods: This retrospective study analysed a prospective cohort of drug-resistant pulmonary TB patients treated with bedaquiline provided by the Global Drug Facility in China. Patients were enrolled from February 2018 to April 2020 across 21 hospitals under the New Drug Introduction and Protection Program. Prolonged use decisions were made by a central expert committee based on individual treatment responses. Effectiveness was assessed through cumulative culture conversion rates and time; safety was evaluated by monitoring adverse events (AEs).
Results: Of 481 patients, 421 received standard bedaquiline treatment, and 60 received prolonged treatment. Median culture conversion time was 4 weeks in both groups (P = 0.443), with one patient in the prolonged group achieving culture conversion after 24 weeks. Rates of QT prolongation (30.0% vs 28.5%), deaths (0% vs 2.1%), and other AEs were comparable. During the first 24 weeks, the prolonged group had a lower AE rate overall (35.0% vs 51.3%), including serious AEs (1.7% vs 13.8%), grade > 3 AEs (13.3% vs 30.4%), AEs leading to death (0% vs 2.1%), bedaquiline-related AEs (16.7% vs 26.6%), and AEs leading to bedaquiline discontinuation (0% vs 5.7%).
Conclusion: Prolonged bedaquiline use is effective and well-tolerated without significantly increased toxicity, potentially benefitting bedaquiline-tolerant patients with positive sputum cultures after the standard 6-month treatment.
Keywords: tuberculosis, multidrug resistant, bedaquiline, culture conversion, safety
Introduction
An estimated 450,000 cases of multidrug-resistant/rifampicin-resistant tuberculosis (MDR/RR-TB) emerged globally in 2021, including 33,000 cases in China, accounting for 7.3% of the global incidence.1 Despite a 60% treatment success rate, MDR/RR-TB caused approximately 191,000 deaths worldwide in 2021.1 Although cure rates are steadily improving, MDR/RR-TB remains a significant public health challenge, underscoring the need for more effective treatment options. While promising therapies like delamanid and pretomanid1–6 show potential, access to these drugs in China was limited at that time.
Bedaquiline (BDQ), a diarylquinoline anti-mycobacterial drug, is a cornerstone of MDR/RR-TB treatment regimens.6 Accelerated approval was granted in 2012 by the US Food and Drug Administration based on phase 2b TMC207-C208 trial results.7 The World Health Organisation (WHO) subsequently recommended including BDQ in MDR/RR-TB regimens in its guidance document The Use of Bedaquiline in the Treatment of Multidrug-Resistant Tuberculosis: Interim Policy Guidance, initially with a conditional recommendation based on limited evidence.8 Subsequent studies demonstrated that BDQ shortened the time to sputum conversion, increases sustained negative culture rates, and improves long-term survival.8,9 WHO now classifies BDQ as a Group A drug, recommending its inclusion in all long-term MDR/RR-TB treatment regimens, with potential use beyond the standard 6-month course.6
Some patients fail to achieve sputum conversion within 24 weeks of BDQ treatment, raising questions about whether its use should be extended. Current evidence indicates that QT-interval prolongation associated with extended bedaquiline therapy occurs predominantly within the first 6 months of treatment, with the most pronounced risk occurring within the initial 12 weeks.10,11 Moreover, several clinical trials conducted under rigorous surveillance have permitted prolonged BDQ use. A French cohort of 33 patients receiving prolonged BDQ therapy achieved a favorable outcome rate of 81.8%.12 A multicentre, open-label, non-inferiority randomized controlled trial conducted in China (n = 231) showed no statistically significant difference in favourable outcome rates or safety between a 9-month BDQ-containing short regimen and an 18–20-month long regimen; the incidence of QTcF prolongation was 22.6% versus 24.1%, and the proportions of evaluable unfavourable outcomes were 16.5% versus 22.4%, respectively.13 Two additional multicentre cohort studies found no statistically significant differences in sputum conversion, cavity closure, or treatment success between 6-month and >6-month regimens, and prolonged therapy did not increase the incidence of adverse events.14,15
Although prolonging the BDQ course beyond six months has not significantly improved treatment success rates,16 long-term administration has demonstrated a favorable safety profile.17 Limited alternative drug options for MDR/RR-TB patients prone to relapse after treatment completion; and prevalent off-label drug use in MDR/RR-TB treatment.18 Caminero et al suggested BDQ use for at least 13–15 months, and WHO guidelines leave treatment duration beyond the standard 24 weeks to physician discretion.18,19 While current data support the overall safety of prolonged BDQ therapy, its risk–benefit ratio requires further validation through high-quality evidence.
Our prior study compared the safety and efficacy of a 24-week BDQ-containing regimen in patients with MDR/XDR-TB with and without diabetes.20 Building on the same cohort, the current study further evaluated the effectiveness and safety of prolonged BDQ therapy (>24 weeks) versus the standard 24-week regimen for long-course treatment of MDR/RR-TB. The findings will guide the better use of BDQ in managing longer MDR/RR-TB treatment.
Materials and Methods
Patients
This study retrospectively analysed data from a prospective cohort of patients with drug-resistant pulmonary TB treated with BDQ donated by the Global Drug Facility (GDF) in China.20 Patients were enrolled across 21 centres between February 24, 2018 and April 1, 2020. All TB cases were culture-confirmed. This study was approved by the ethics committee of Beijing Chest Hospital, and informed consent was obtained from all patients.
Inclusion criteria were: 1) laboratory-confirmed diagnosis of MDR/XDR-TB (This study was conducted from 2018 to 2020, when the definitions of MDR/XDR-TB had not yet been updated; therefore, all references to MDR/XDR-TB in this article follow the WHO previous definitions); 2) No prior initiation of MDR/XDR-TB treatment or cases where further intensive treatment was required; 3) age ≥18 years; 4) patients requiring BDQ as part of an effective regimen following WHO therapeutic principles for MDR-TB, including patients with XDR-TB, pre-XDR-TB, MDR-TB with previous treatment failure, or MDR-TB where fluoroquinolones or injectables were unsuitable;8,21 and 5) no respiratory failure, cardiac failure, clinically significant arrhythmia, or corrected QT interval with Fridericia’s formula (QTcF) ≥450 ms.
Exclusion criteria were: 1) allergy to BDQ; 2) participation in other clinical trials within the last 3 months; or 3) high-risk cardiac comorbidities or factors predisposing to QT prolongation, including: a. QTcF ≥450 ms on screening ECG (patients could undergo re-evaluation during screening for eligibility); b. Pathologic Q wave (>40 ms or depth >0.4–0.5 mV); c. Evidence of ventricular preexcitation (eg, Wolff-Parkinson-White syndrome); d. Complete or clinically significant incomplete bundle branch block; e. Grade II or III heart block; f. QRS duration >120 ms; g. Bradycardia (sinus heart rate <50 bpm); h. History of long QT syndrome, symptomatic or asymptomatic arrhythmia (excluding sinus arrhythmia), cardiogenic syncope, or other heart disease; i. Risk factors for torsades de pointes (eg, heart failure, hypokalemia, or hypomagnesemia).
Treatment
Individualised background regimens were developed by local physicians following WHO guidelines Based on drug susceptibility testing results, MDR-TB treatment regimens should consist of at least four second-line anti-TB drugs which are likely to be effective, including an injectable anti-TB agent.8,21 BDQ was administered alongside individualised background regimens based on each patient’s previous anti-TB treatment history and tolerance. For patients with definite drug susceptibility testing results, BDQ was used in combination with at least three drugs. Baseline culture was performed within 30 days prior to BDQ treatment initiation. For patients without definite drug susceptibility testing results, BDQ was used in combination with at least four drugs. The patients received oral BDQ 400 mg once daily for 2 weeks, then 200 mg three times a week (with at least a 48-h interval between doses) for 22 weeks.
At the end of the 24-week BDQ treatment period, the local expert panel evaluated whether an additional 12-week prolonged BDQ treatment was needed and submitted applications to a central expert committee for approval. Prolonged BDQ use (>24 weeks) was determined by an independent expert committee based on: (1) persistent culture positivity at Week 24, (2) inadequate clinical or radiographic response, and (3) absence of QTc prolongation >500 ms or other serious adverse events. Patients meeting criteria were uniformly extended to 36 weeks. Upon completion of bedaquiline treatment, patients continued their background regimens and were followed for an additional 12 weeks. For analysis, patients were grouped into standard BDQ treatment (24 weeks) or prolonged treatment (>24 weeks).
Evaluation
Patients were followed biweekly during the first month and monthly thereafter, with sputum culture performed at each follow-up visit. Evaluations included sputum culture, ECG, symptom assessment, and imaging. Outcomes assessed were: cumulative culture conversion rate based on two consecutive negative sputum cultures ≥25 days apart following a positive baseline culture; time to culture conversion defined as the time from baseline to the first negative sputum culture in patients achieving conversion; adverse events (AEs), including abnormal QTcF intervals, recorded throughout the treatment period and graded using Division of AIDS Guidelines for Grading the Severity of Adult and Pediatric Adverse Events, version 2.1.22
Statistical Analysis
Continuous variables were assessed for normality using the Kolmogorov–Smirnov test. As they were non-normally distributed, results are presented as medians with interquartile ranges [IQR]. Comparisons between groups were conducted using the Mann–Whitney U-test. Categorical variables were expressed as frequencies (percentages) and analysed using chi-square or Fisher’s exact tests, as appropriate. Factors associated with time to culture conversion were identified using univariable and multivariable Cox proportional hazard models, which estimate the hazard ratio (HR) as a measure of the relative risk of an event occurring at any given time point between groups. The results are presented with 95% confidence intervals (95% CI), indicating the range within which the true HR is expected to lie with 95% certainty. Statistical analyses were performed using SPSS 22.0 (IBM, Armonk, NY, USA). P-values <0.05 were considered statistically significant.
Results
Patient Characteristics
In this study of 481 patients, 421 received the standard 24-week BDQ treatment and 60 received the prolonged BDQ treatment (Table 1). The median ages of patients were 43.5 years (IQR, 33–51.5) in the prolonged group and 44 years (IQR, 32–52) in the standard group (P = 0.932). The majority of patients in both groups were male (71.7% in the prolonged group and 76.2% in the standard group, P = 0.439). The proportions of patients with MDR-TB, pre-XDR-TB, and XDR-TB were similarly distributed between the groups (P = 0.209). Among the patients, 9 (15.0%) in the prolonged group and 66 (15.7%) in the standard group were previously untreated (P = 0.892). Comorbidities were present in 11 (18.3%) and 74 (17.6%) patients in the prolonged and standard groups, respectively (P = 0.886). Most patients (81.7% in the prolonged group and 80.3% in the standard group) received five to six anti-TB drugs throughout their treatment, including BDQ, its combination drugs, and those used post-BDQ treatment (P = 0.414, Table 1).
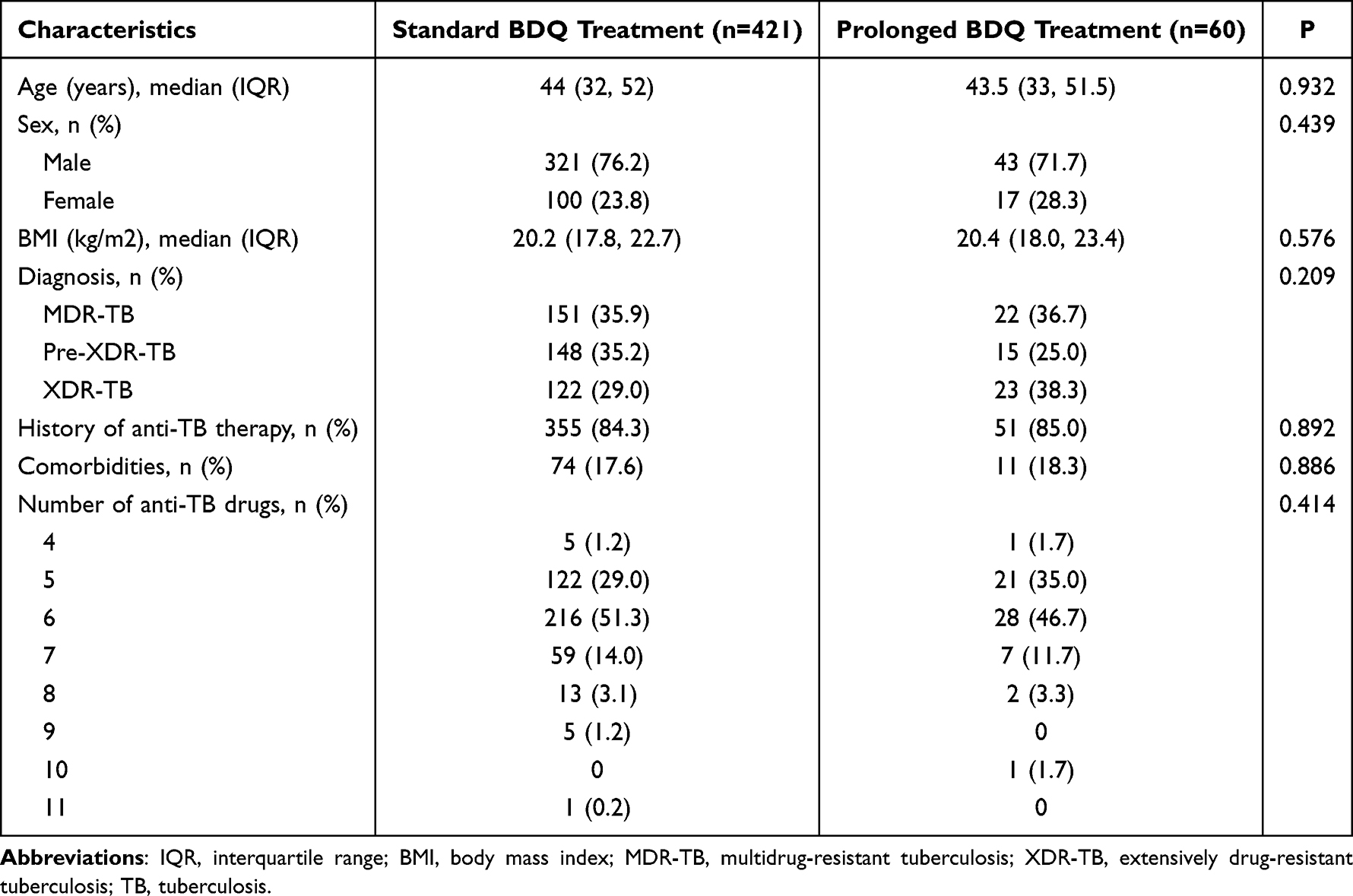 |
Table 1 Baseline Characteristics in Standard BDQ Treatment Group and Prolonged BDQ Treatment Group |
Anti-TB Drugs Before and After BDQ Treatment
Table 2 summarises the background regimen drugs. There were no significant differences between the two groups in the use of Group A and B drugs, either before or after BDQ treatment. However, differences were observed in Group C drugs, with lower use of pyrazinamide in the prolonged group compared to the standard group during BDQ treatment (13.3% vs 25.2%, P = 0.044) and after BDQ treatment (8.3% vs 20.9%, P = 0.021). Conversely, para-aminosalicylic acid was used more frequently in the prolonged group during BDQ treatment (51.7% vs 34.9%, P = 0.012) and after BDQ treatment (48.3% vs 32.5%, P = 0.016).
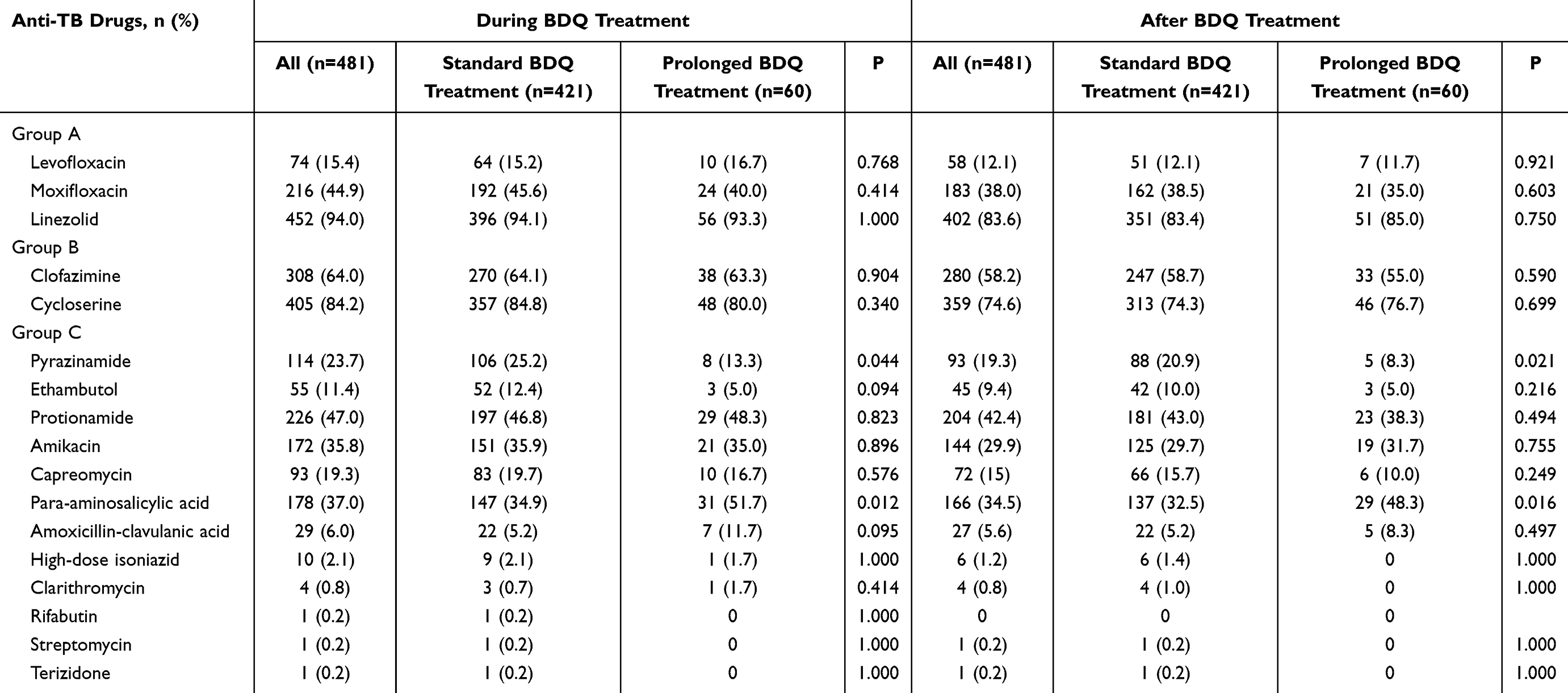 |
Table 2 Background Regimen in Two Groups |
Culture Conversion
The median time to culture conversion was 4 weeks in both groups (Figure 1), with no significant difference between them (P = 0.443). One patient in the prolonged group achieved culture conversion after 24 weeks. Multivariable logistic regression analysis revealed that prolonged BDQ use was not associated with time to culture conversion (HR = 0.901, 95% CI: 0.670–1.212, P = 0.489). Age was the only factor independently associated with a shorter time to culture conversion (HR = 0.990, 95% CI: 0.982–0.998, P = 0.017, Table 3).
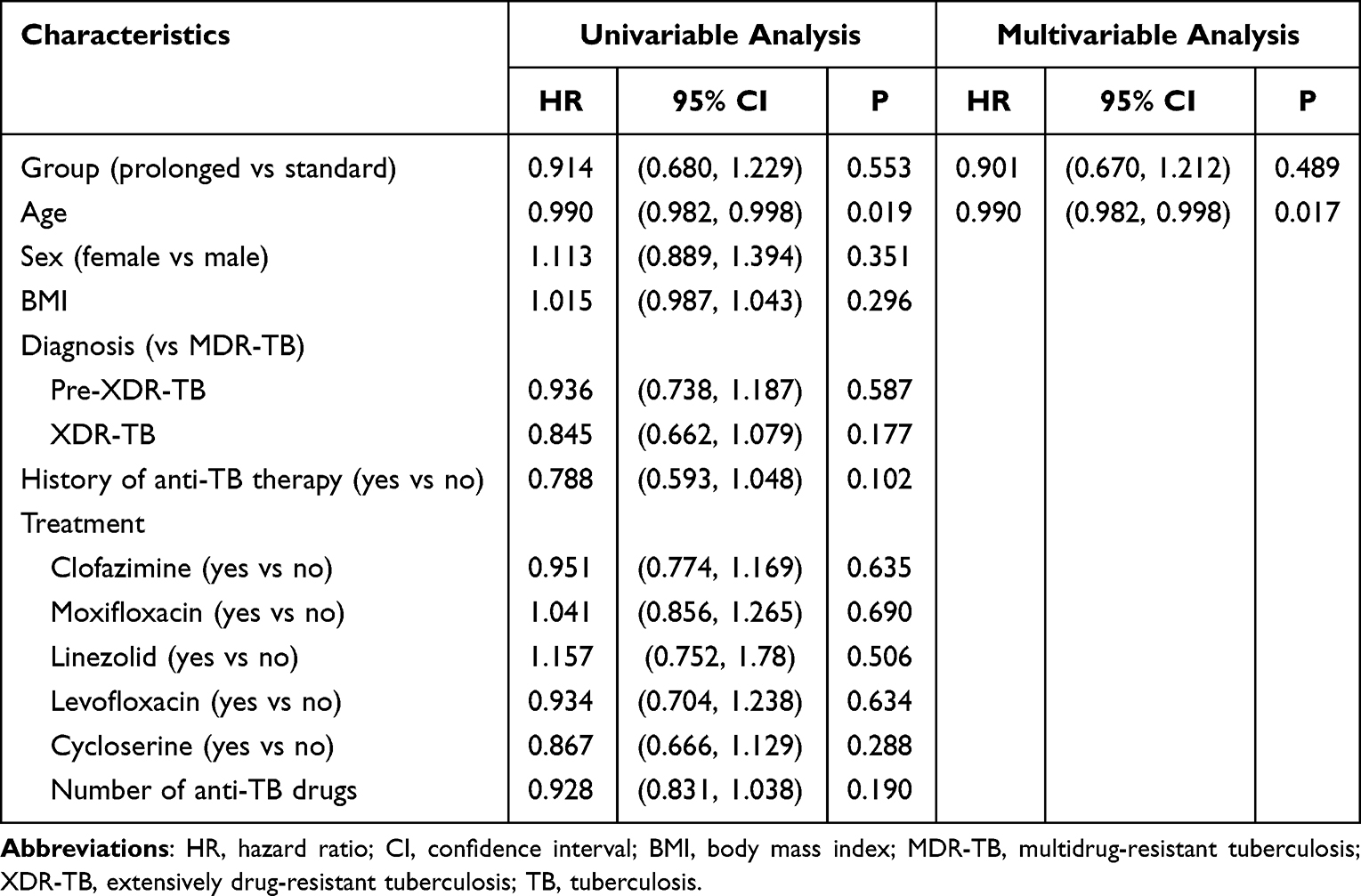 |
Table 3 Cox Regression Analysis for Time to Confirmed Culture Conversion |
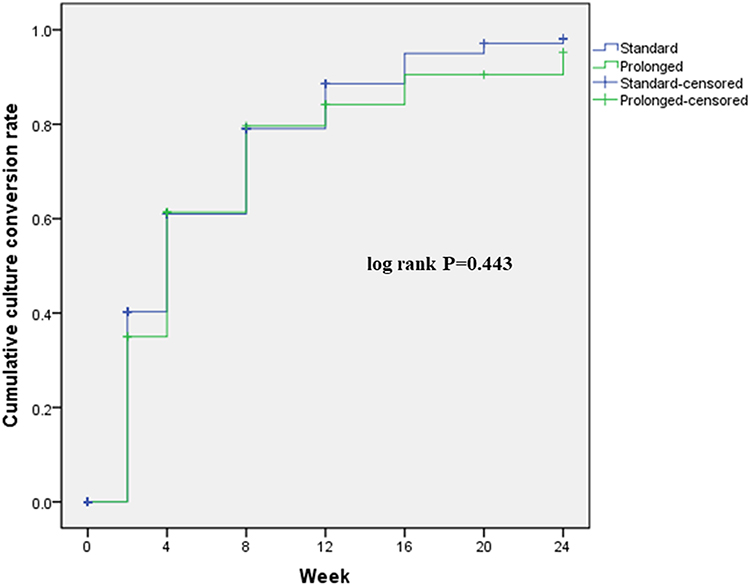 |
Figure 1 Kaplan-Meier plot for time to confirmed culture conversion in two groups. |
The cumulative culture conversion rate in the prolonged group was comparable to the standard group at 4 weeks (60.0% vs 55.6%, P = 0.267). From 8 weeks (85.7% vs 68.5%, P = 0.520) to 24 weeks (83.3% vs 84.1%, P = 0.874), the prolonged group demonstrated slightly higher rates, though the differences were not statistically significant (Figure 2).
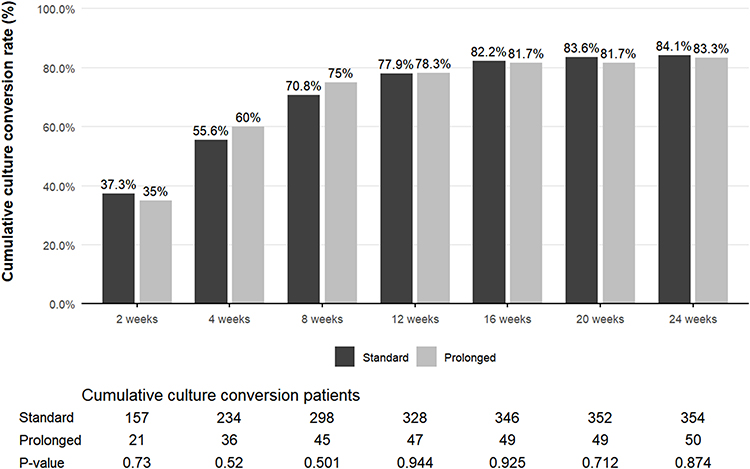 |
Figure 2 Cumulative culture conversion rate during the 24-week BDQ treatment period in two groups. |
Safety
Table 4 details the combinations of drugs known to prolong the QT interval. Frequently used QT-prolonging drugs in combination with BDQ included clofazimine (prolonged: 15.0%; standard: 20.2%), clofazimine plus moxifloxacin (prolonged: 25.0%; standard: 25.0%), and moxifloxacin (prolonged: 38.3%; standard: 39.2%).
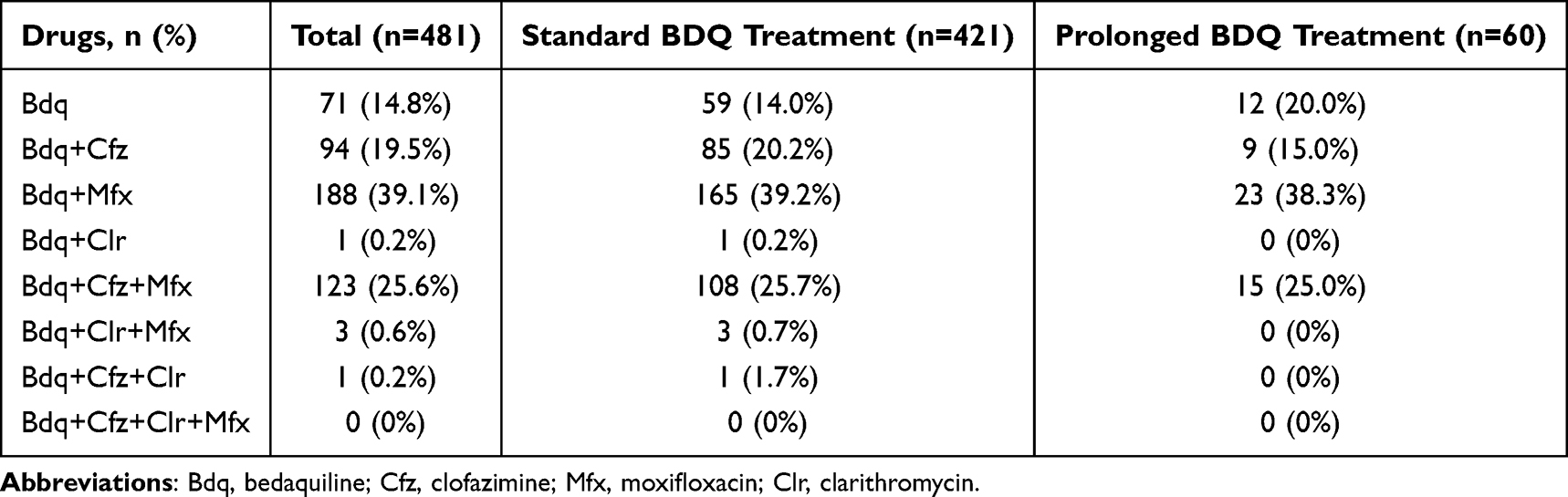 |
Table 4 The Use of QT-Prolonging Drugs During the Whole Treatment Period |
The overall incidence of any AE was 46.7% (28/60) in the prolonged group and 51.3% (216/421) in the standard group (p=0.501). Serious AEs and grade ≥3 AEs occurred less frequently in the prolonged group (1.7% and 18.3%) compared to the standard group (13.8% and 30.4%). BDQ-related AEs were reported in 25.0% of the prolonged group and 26.6% of the standard group, while AEs leading to BDQ withdrawal occurred in 1.7% and 5.7% of patients, respectively. No deaths occurred in the prolonged group, whereas nine patients (2.1%) in the standard group died due to AEs.
The most common AEs (>5% of patients) were QT prolongation (30.0% in the prolonged group vs 28.5% in the standard group), pulmonary infection (18.3% vs 16.6%), and gastrointestinal bleeding (8.3% vs 8.6%) (Table 5). AEs in the prolonged group were categorised as occurring within 24 weeks and after 24 weeks (Table 5). During the first 24 weeks, the prolonged group exhibited lower frequencies of any AE (35.0% vs 51.3%), serious AEs (1.7% vs 13.8%), grade >3 AEs (13.3% vs 30.4%), AEs leading to death (0% vs 2.1%), BDQ-related AEs (16.7% vs 26.6%), and AEs leading to BDQ discontinuation (0% vs 5.7%) compared to the standard group. The three most frequent AEs (QT prolongation, pulmonary infection, and gastrointestinal bleeding) occurred at comparable rates during the first 24 weeks of treatment (QT prolongation: 20.0% vs 28.5%; pulmonary infection: 13.3% vs 16.6%; gastrointestinal bleeding: 8.3% vs 8.6%) (Table 5).
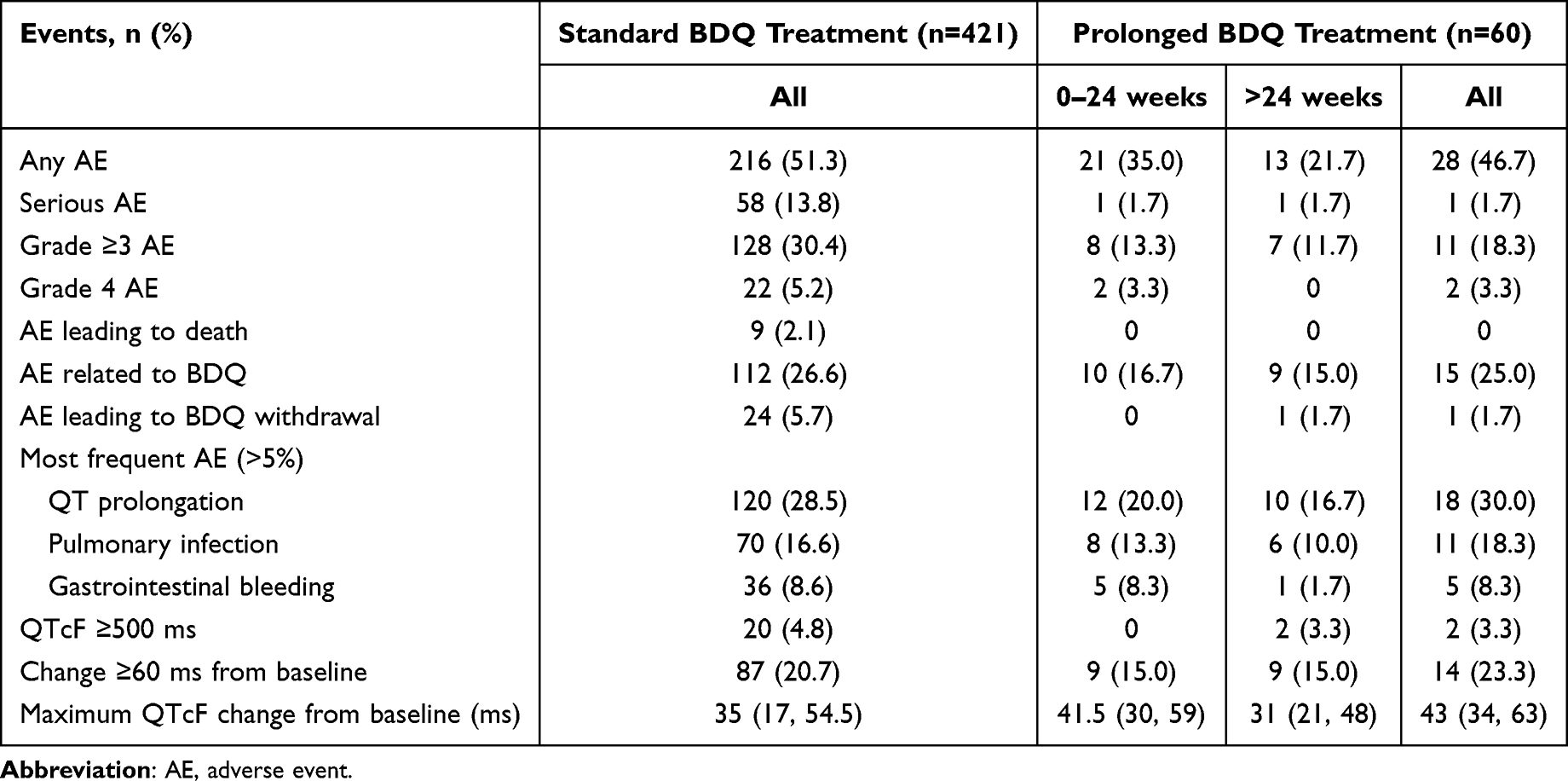 |
Table 5 Adverse Events in Two Groups |
Discussion
We report successful outcomes in 83.3% of MDR-TB patients treated with prolonged BDQ regimens, along with a lower rate of AEs compared to the standard group. Limited evidence exists regarding the effectiveness and safety of prolonged BDQ treatment for MDR-TB, but the WHO has suggested that prolonged BDQ use is safe in patients with appropriate baselines and close follow-up.1 This study aimed to examine the effectiveness and safety of prolonged BDQ use (>24 weeks) compared to the standard 24-week for MDR-TB and XDR-TB longer regimen. No significant differences in overall effectiveness or safety were observed between groups (p=0.442 and p=0.501).
The study was based on earlier guidelines, and the background regimens used were primarily aligned with the 2020 WHO guidance;6,8,21 meanwhile, the BPaLM regimen is now the preferred option.23 Concerns about QT prolongation limited the use of the Group A drug moxifloxacin (44.9% during BDQ treatment, 38.0% after BDQ treatment) and the Group B drug clofazimine (64.0% during BDQ treatment, 58.2% after BDQ treatment), necessitating routine ECG monitoring. Clarithromycin was rarely prescribed (0.8% during BDQ treatment and after BDQ treatment). Pyrazinamide was used more frequently in the standard group (25.2% vs 13.3% during BDQ treatment; 20.9% vs 8.3% after BDQ treatment), while para-aminosalicylic acid was more commonly prescribed in the prolonged group (51.7% vs 34.9% during BDQ treatment; 48.3% vs 32.5% after BDQ treatment).
The cumulative culture conversion rate was high (84.0%) at 24 weeks, consistent with prior studies showing the effectiveness of BDQ-containing regimens.12,14,17,24–28 Median time to culture conversion was similar between the groups, though one patient in the prolonged group achieved conversion only after 24 weeks, suggesting potential benefits of extended BDQ use in select cases.6 These findings align with studies reporting higher culture conversion rates and comparable safety profiles for prolonged regimens versus standard treatment.12,27 Given limited treatment options for MDR/XDR-TB, the 24-week standard regimen may not suffice for all patients, potentially resulting in missed culture conversion or increased relapse risk. This underscores the need for individualised approaches, particularly when WHO-recommended drugs (eg, fluoroquinolones, linezolid, clofazimine) are used off-label for MDR-TB.6,29 Collaborative decision-making between physicians and patients is crucial to tailoring effective regimens.30
The safety profile of BDQ observed in this study is consistent with previous findings,12,14,17,24–26,28,31,32 including evidence that QTcF elevation typically peaks at 8–12 weeks and that extending BDQ treatment beyond 24 weeks does not increase QTcF elevation rates.12,27 In this study, prolonged BDQ use was not associated with higher risks of QT prolongation, death, or other AEs. Changes in QTcF were comparable between the groups, offering reassurance for both physicians and patients considering prolonged BDQ regimens. Notably, the prolonged group experienced fewer AEs during the first 24 weeks compared to the standard group. Moreover, AEs occurring after 24 weeks in the prolonged group were manageable and did not raise significant safety concerns. For patients who fail to achieve sputum-culture conversion within the standard 24-week treatment, remain susceptible to BDQ, exhibit good drug tolerance during the first 24 weeks, and have a low burden of cardiac comorbidities, BDQ treatment may be prolonged.
This study has limitations. First, despite being a multicentre study, the sample size was still relatively small, limiting the power to detect differences between the standard and prolonged groups. Second, the lack of a control group not receiving BDQ limits broader comparisons. Finally, comorbidities such as diabetes, hypertension, hepatitis, or AIDS were not assessed, nor were subgroup analyses conducted for special populations, limiting the generalisability of our results to these groups. Future studies should address these limitations by expanding the sample size, conducting subgroup analyses, and including patients with comorbidities to provide robust evidence on the efficacy and safety of prolonged BDQ regimens across diverse populations. Long-term follow-up should be conducted to assess durable outcomes, and baseline or early-treatment transcriptomic and proteomic biomarkers predictive of delayed sputum-culture conversion should be prospectively validated to enable precision-guided decisions regarding BDQ prolongation.
Conclusion
Tolerance to BDQ is a critical factor for physicians when considering extended treatment in MDR/XDR-TB patients. The effectiveness and safety of prolonged BDQ use are acceptable, with no significant increase in toxicity. Prolonged BDQ treatment may benefit patients who tolerate BDQ and whose sputum culture remains positive after six months of standard treatment. Future research should increase the sample size, include patients with comorbidities, and conduct long-term follow-up to assess the efficacy and safety of prolonged BDQ regimens. Biomarkers predictive of delayed sputum-culture conversion should be validated to enable precision-guided decisions regarding BDQ prolongation.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author Jingtao Gao on reasonable request.
Ethics Approval
This clinical study was conducted in accordance with the principles of the Declaration of Helsinki. This study was approved the Beijing Chest Hospital Ethics Committee (ethical approval number: 2018-05-03). Informed consent was obtained from all individual participants included in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Xinyang Hu, Mengqiu Gao, Yuhong Liu, Yi Pei, Juan Du, Guihui Wu and Aidi Wang are the co-first authors and contributed equally to this study.
Funding
This work was supported by the Bill & Melinda Gates Foundation.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Global tuberculosis report 2022. Geneva: World Health Organization; 2022.
2. Liu Y, Matsumoto M, Ishida H, et al. Delamanid: from discovery to its use for pulmonary multidrug-resistant tuberculosis (MDR-TB). Tuberculosis. 2018;111:20–11. doi:10.1016/j.tube.2018.04.008
3. Xavier AS, Lakshmanan M. Delamanid: a new armor in combating drug-resistant tuberculosis. J Pharmacol Pharmacother. 2014;5(3):222–224. doi:10.4103/0976-500X.136121
4. Tweed CD, Dawson R, Burger DA, et al. Bedaquiline, moxifloxacin, pretomanid, and pyrazinamide during the first 8 weeks of treatment of patients with drug-susceptible or drug-resistant pulmonary tuberculosis: a multicentre, open-label, partially randomised, phase 2b trial. Lancet Respir Med. 2019;7(12):1048–1058. doi:10.1016/S2213-2600(19)30366-2
5. McKenna L, Furin J. Are pretomanid-containing regimens for tuberculosis a victory or a victory narrative? Lancet Respir Med. 2019;7(12):999–1000. doi:10.1016/S2213-2600(19)30363-7
6. WHO consolidated guidelines on drug-resistant tuberculosis treatment. Geneva: World Health Organization; 2020.
7. Diacon AH, Pym A, Grobusch MP, et al. Multidrug-resistant tuberculosis and culture conversion with bedaquiline. N Engl J Med. 2014;371(8):723–732. doi:10.1056/NEJMoa1313865
8. World Health Organization. The Use of Bedaquiline in the Treatment of Multidrug-Resistant Tuberculosis: Interim Policy Guidance. World Health Organization; 2013.
9. Conradie F, Diacon AH, Ngubane N, et al. Treatment of highly drug-resistant pulmonary tuberculosis. N Engl J Med. 2020;382(10):893–902. doi:10.1056/NEJMoa1901814
10. Khan U, Rich M, Franke MF, et al. The frequency and incidence of QT prolongation with extended use of bedaquiline or delamanid in a large, multi-country multidrug-resistant/rifampicin-resistant tuberculosis cohort. Clin Infect Dis. 2025;81(1):153–158. doi:10.1093/cid/ciae601
11. van Beek SW, Tanneau L, Meintjes G, et al. Model-predicted impact of ECG monitoring strategies during bedaquiline treatment. Open Forum Infect Dis. 2022;9(8):ofac372. doi:10.1093/ofid/ofac372
12. Guglielmetti L, Jaspard M, Le Dû D, et al. Long-term outcome and safety of prolonged bedaquiline treatment for multidrug-resistant tuberculosis. Eur Respir J. 2017;49(3).
13. Song Y, Shu W, Pei Y, et al. Nine months of bedaquiline, linezolid, levofloxacin, clofazimine, and cycloserine chemotherapy for rifampicin/multidrug-resistant tuberculosis: a multicenter, randomized, open-label non-inferiority trial in China. BMC Med. 2024;22(1):401. doi:10.1186/s12916-024-03633-3
14. Yu Y, Cao J, Pan H, et al. Real-world effectiveness and safety of prolonged bedaquiline course in the treatment of drug-resistant tuberculosis-a multi-center retrospective cohort study in a country with a high burden of drug-resistant tuberculosis. Microbiol Spectr. 2025;13(8):e0009725. doi:10.1128/spectrum.00097-25
15. Ke H, Gui X, Sun W, et al. The safety and efficacy of prolonged use of bedaquiline for the treatment of patients with pulmonary multi-drug resistant/rifampin-resistant tuberculosis: a prospective, cohort study in China. Infect Drug Resist. 2023;16:5055–5064. doi:10.2147/IDR.S419996
16. Trevisi L, Hernán MA, Mitnick CD, et al. Effectiveness of bedaquiline use beyond six months in patients with multidrug-resistant tuberculosis. Am J Respir Crit Care Med. 2023;207(11):1525–1532. doi:10.1164/rccm.202211-2125OC
17. Zhurkin D, Gurbanova E, Campbell JR, et al. Safety of prolonged treatment with bedaquiline in programmatic conditions. ERJ Open Res. 2022;8(2):00685–2021. doi:10.1183/23120541.00685-2021
18. Furin J, Lessem E, Cox V. Recommending prolonged bedaquiline use for the treatment of highly resistant strains of tuberculosis. Eur Respir J. 2017;50(5):1701552. doi:10.1183/13993003.01552-2017
19. Frequently asked questions about the use of bedaquiline according to the WHO guidelines and evidence from its early use in selected countries. 2017. Available from: https://www.who.int/docs/default-source/documents/tuberculosis/faqs-bedaquiline.pdf?sfvrsn=ab0053b6_2.
20. Shi L, Gao J, Gao M, et al. Interim effectiveness and safety comparison of bedaquiline-containing regimens for treatment of diabetic versus non-diabetic MDR/XDR-TB patients in China: a multicenter retrospective cohort study. Infect Dis Ther. 2021;10(1):457–470. doi:10.1007/s40121-021-00396-9
21. Companion Handbook to the WHO guidelines for the programmatic management of drug-resistant tuberculosis. Geneva: World Health Organization; 2014.
22. U.S. Department of Health and Human Services, National Institutes of Health, National Institute of Allergy and Infectious Diseases, AIDS Do. Division of AIDS (DAIDS) table for grading the severity of adult and pediatric adverse events, corrected version 2.1. Bethesda: National Institutes of Health; 2017. Available from: https://rsc.niaid.nih.gov/sites/default/files/daidsgradingcorrectedv21.pdf.
23. Global tuberculosis report 2024. Geneva: World Health Organization; 2024.
24. Mase S, Chorba T, Parks S, et al. Bedaquiline for the treatment of multidrug-resistant tuberculosis in the United States. Clin Infect Dis. 2020;71(4):1010–1016. doi:10.1093/cid/ciz914
25. Borisov SE, D’Ambrosio L, Centis R, et al. Outcomes of patients with drug-resistant-tuberculosis treated with bedaquiline-containing regimens and undergoing adjunctive surgery. J Infect. 2019;78(1):35–39. doi:10.1016/j.jinf.2018.08.003
26. Yates TA. Effect of bedaquiline on mortality in South African patients with drug-resistant tuberculosis. Lancet Respir Med. 2018;6(12):e56. doi:10.1016/S2213-2600(18)30453-3
27. Ndjeka N, Schnippel K, Master I, et al. High treatment success rate for multidrug-resistant and extensively drug-resistant tuberculosis using a bedaquiline-containing treatment regimen. Eur Respir J. 2018;52(6):1801528. doi:10.1183/13993003.01528-2018
28. Khan A, Khan AH, Ahmad N, et al. Effectiveness of bedaquiline containing all oral longer regimens in treating multidrug/rifampicin resistant tuberculosis in Pakistan. J Infect Public Health. 2024;17(9):102522. doi:10.1016/j.jiph.2024.102522
29. D’Ambrosio L, Centis R, Sotgiu G, et al. New anti-tuberculosis drugs and regimens: 2015 update. ERJ Open Res. 2015;1(1). doi:10.1183/23120541.00010-2015
30. Lessem E, Cox H, Daniels C, et al. Access to new medications for the treatment of drug-resistant tuberculosis: patient, provider and community perspectives. Int J Infect Dis. 2015;32:56–60. doi:10.1016/j.ijid.2014.12.012
31. Borisov SE, Dheda K, Enwerem M, et al. Effectiveness and safety of bedaquiline-containing regimens in the treatment of MDR- and XDR-TB: a multicentre study. Eur Respir J. 2017;49(5):1700387. doi:10.1183/13993003.00387-2017
32. Nguyen TMP, Nguyen BH, Hoang TTT, et al. Safety and effectiveness of all-oral and injectable-containing, bedaquiline-based long treatment regimen for pre-XDR tuberculosis in Vietnam. Front Pharmacol. 2022;13:1023704. doi:10.3389/fphar.2022.1023704
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
In vitro and Intracellular Antibacterial Activity of Sudapyridine (WX-081) Against Tuberculosis
Xiao H, Yu X, Shang Y, Ren R, Xue Y, Dong L, Zhao L, Jiang G, Huang H
Infection and Drug Resistance 2023, 16:217-224
Published Date: 10 January 2023
Clinical Utility of Contezolid-Containing Regimens in 25 Cases of Linezolid-Intolerable Tuberculosis Patients
Wang J, Nie W, Ma L, Li Q, Geng R, Shi W, Chu N
Infection and Drug Resistance 2023, 16:6237-6245
Published Date: 19 September 2023
Clinical and Microbiological Characteristics of Klebsiella pneumoniae Co-Infections in Pulmonary Tuberculosis: A Retrospective Study
Liu J, Zhang Y, Cai J, Shao L, Jiang X, Yin X, Zhao X, Wang S
Infection and Drug Resistance 2023, 16:7175-7185
Published Date: 8 November 2023
Advances in the Treatment and Clinical Management Strategies of Tuberculous Meningitis
Li R, Yin R, Li Y, Wei Y, Zhao B, Ge C
International Journal of General Medicine 2025, 18:3267-3276
Published Date: 19 June 2025
A Short-Course Regimen Containing Delamanid, Bedaquiline and Linezolid for the Treatment of Drug-Resistant Tuberculosis: A Retrospective Study from China
Jin L, Zhang X, Jiang H, Li Q, Liu W, Wang J, Cao Z, Liu Y
Infection and Drug Resistance 2026, 19:596822
Published Date: 10 July 2026