")
Back to Journals » Infection and Drug Resistance » Volume 16
In vitro and Intracellular Antibacterial Activity of Sudapyridine (WX-081) Against Tuberculosis
Authors Xiao H, Yu X, Shang Y, Ren R, Xue Y, Dong L, Zhao L, Jiang G, Huang H
Received 17 September 2022
Accepted for publication 20 December 2022
Published 10 January 2023 Volume 2023:16 Pages 217—224
DOI https://doi.org/10.2147/IDR.S390187
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Hua Xiao,* Xia Yu,* Yuanyuan Shang, Ruyan Ren, Yi Xue, Lingling Dong, Liping Zhao, Guanglu Jiang, Hairong Huang
National Clinical Laboratory on Tuberculosis, Beijing Key Laboratory for Drug Resistant Tuberculosis Research; Beijing Chest Hospital, Capital Medical University, Beijing Tuberculosis and Thoracic Tumor Institute, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hairong Huang, Beijing Key Laboratory for Drug-Resistant Tuberculosis Research, Beijing Chest Hospital, Capital Medical University, No. 97 Ma Chang, Tongzhou District, Beijing, 101149, People’s Republic of China, Tel +86-10-89509159, Fax +86-10-89509160, Email [email protected]
Background: Sudapyridine (WX-081) has exhibited equivalent efficacy than its counterpart parent drug bedaquiline (BDQ) but better safety profile against Mycobacterium tuberculosis (Mtb). Our study was aimed to evaluate in vitro activity of WX-081 against the clinical isolates of Mtb with different drug-resistance profiles and the intracellular bactericidal activity against the reference strain.
Methods: The minimum inhibitory concentrations (MICs) of WX-081 and BDQ were tested against 114 Mtb clinical isolates. The intracellular activity of WX-081 and BDQ against the Mtb reference strain H37Rv in THP-1 cells was also evaluated in parallel.
Results: The MICs for WX-081 of the enrolled isolates ranged from 0.0156 μg/mL to 1 μg/mL. The MIC50 and MIC90 of WX-081 were, respectively, 0.25 μg/mL and 0.5 μg/mL, with 95.6% of the enrolled strains having MICs ≤ 0.25 μg/mL. For a given strain, the MIC value of WX-081 was generally equivalent to or 2-fold than MIC of BDQ. The intracellular bacterial killing was acquired with the tested drug concentrations that were presumed attainable during clinical usage.
Conclusion: WX-081 exhibited potent efficacy against the clinical isolates in vitro. The intracellular killing effect of sudapyridine against the reference strain supports its potential efficacy in treating TB patients.
Keywords: tuberculosis, sudapyridine, bedaquiline, antibacterial activity
Introduction
Tuberculosis, (TB) a chronic infectious disease caused by Mycobacterium tuberculosis (Mtb), remains one of the leading causes of global deaths. According to the Global tuberculosis report (2021), the estimated TB incidence was 59 per 100,000 population while the mortality rate was 2.1/100,000 in China.1 One of the major challenges that currently hinder the national TB program of China is drug resistance. Multiple drug-resistant tuberculosis (MDR-TB) and MDR-TB plus additional resistance to fluoroquinolone and second-line injectable reagent (once named extensively drug-resistant (XDR) TB, and herein called Pre-XDR TB according to the new concept of WHO) render the treatment arduous and unsatisfactory. This is mostly due to unavailability of potent drugs and the lengthy and complicated treatment course which deteriorates the overall treatment outcomes.2–5 Developing new, safe, high-efficiency anti-TB drugs is the mainstay to cope with the seriousness of drug resistance.
Bedaquiline (BDQ) is among the first anti-TB drugs, with a novel mechanism, that has been approved since 1962. It works by inhibiting the proton pump of ATP synthesis and has demonstrated potent bactericidal activities in vitro and in vivo.6,7 Several studies have proved the high efficacy of BDQ in treating drug-resistant TB.8–10 Due to its potent efficacy, BDQ was listed as the first-line choice drug for long-term treatment of MDR/rifampicin resistant (RR)-TB by WHO in 2018. Meanwhile, the major disadvantages of using BDQ include prolongation of the QT interval, cardiotoxicity, hepatotoxicity, and cross-resistance between BDQ and clofazimine.11,12 Hence, the analogs of BDQ with similar efficacy but lesser side effects are pursued.
Sudapyridine (WX-081), an innovative diarylpyridinated drug formed by substituting the bromoquinoline of BDQ with a 5-phenylpyridine, was introduced to clinical development stage in 2018.13 In vivo animal studies have shown that WX-081 had higher lung tissue concentration, greater safety, and lower risk of QT interval prolongation than BDQ.14 Furthermore, the drug did not manifest any effect on heart rate, electrocardiograph (ECG) morphology, or blood pressure in animal models.14 A phase III clinical trial (CTR20221162) is ongoing after a successful phase II clinical trial (data is ready for publication).
The recent first publication on WX-081 presented the in vitro inhibitory outcomes of this drug candidate against few clinical isolates and the in vitro time-kill activity assay.13 In order to better understand its therapeutic potential on TB, we measured the MICs of WX-081 and BDQ against 114 clinical Mtb isolates, including sensitive strains, MDR strains, and Pre-XDR strains. Moreover, we also evaluated the bactericidal activity of WX-081 against Mtb in macrophages. The purpose of this study is to expand current information on sudapyridine and its anti-TB activity.
Materials and Methods
Ethics Statement
As the study only involved laboratory testing of mycobacterial strains without the direct involvement of human subjects, ethical approval was not sought, and Biosafety Level 3 precautions and laboratory conditions were adhered to and maintained.
Compounds
BDQ was purchased from Liye-Pharmaceutical (Nanjing, China) Co., Ltd. and WX-081 was provided by Shanghai Jiatan Biotech Ltd.
Reference Strains and Clinical Isolates
The reference strain of Mtb H37Rv (ATCC 27294) and 114 clinical isolates were collected from the Bio-bank of Beijing Chest Hospital (Beijing, China). The isolates were firstly cultured positive on Löwenstein-Jensen (LJ) medium, and then classified as tuberculosis preliminarily with negative results using p-nitrobenzoic acid-containing medium (500 µg/mL). All the strains were identified to tuberculosis by the alignments of 16S rRNA, rpoB, hsp65, 16–23S rRNA internal transcribed spacer sequence genes.15 The clinical isolates including 41 sensitive strains (S-TB), 35 MDR strains, and 38 Pre-XDR strains were determined by drug susceptibility testing (proportion method) using LJ medium. These clinical strains were identified as Mtb by using the p-nitrobenzoic acid-containing medium (500 μg/mL).
Minimal Inhibitory Concentration (MIC) Testing
BDQ and WX-081 were dissolved in Dimethyl sulfoxide (DMSO) at a stock concentration of 8 mg/mL and stored at −80°C. MIC detection was performed according to the Clinical and Laboratory Standards Institute (CLSI) guidelines.16 Briefly, the MICs of BDQ and WX-081were determined by 7H9 medium using 2-fold dilutions ranging from 0.0039 to 2.0 μg/mL. Bacterial suspension was prepared using the 1 McFarland turbidity standard, diluted at 1:20, and added to a 96-well plate. The plates were incubated at 37°C for 7 days for Mtb. The color change was assessed after re-incubating at 37°C for an additional 24 h after adding 20 μL Alamar Blue and 50 μL Tween 80 (5%) solutions in each well. The pink or purple color indicated mycobacterial growth. MIC was defined as the lowest drug concentration that prevented a color change from blue to pink or purple.
Tentative Epidemiological Cut-off (ECOFF) Determination
ECOFF was determined from the distribution curve of MIC values. For the unimodal MIC distribution curve, ECOFF was defined as the concentration capable of inhibiting more than 95% of the bacterial population. In contrast, for the bimodal MIC distribution curve, the ECOFF was set between the two populations.
Minimum Bactericidal Concentrations (MBCs) Determination
MBC of BDQ and WX-081 were determined by killing 99.9% of the initial inoculum according to the CLSI guidelines.17 MBCs against M. tuberculosis H37Rv and 6 Mtb clinical isolates that were randomly chosen, including two strains from S-TB, MDR-TB, and Pre-XDR group, were determined by conventional CFU counts in 96 well plates. The treatment concentration of WX-081 and BDQ ranged from 0.0625×MIC to 32×MIC. After 7 days of incubation with BDQ or WX-081 at different concentrations, 100 μL medium from each well was plated on 7H9 medium with 10% OADC. The CFU on the plates was calculated after 3–4 weeks of incubation at 37°C. The MBC was defined as the lowest effective drug concentration that had an effect not less than a 3 log10 decrease in CFU compared to the initial CFU. When the MBC/MIC ratio was ≤32, the tested drug was categorized as a bactericidal agent, otherwise categorized as a bacteriostatic agent.14
Intracellular Killing Assay
THP-1 was purchased from the Wuhan Procell Life Science & Technology Co., Ltd. Cells were seeded into 96-well plates at a density of 5×105 cells/well and differentiated into macrophages with phorbol myristate acetate (PMA) at a final concentration of 200 ng/mL at 37°C. After 48 h incubation, the differentiated THP-1 cells were infected with Mtb H37Rv at a multiplicity of infection (MOI) of 5:1 for 4 h. Then, the plates were washed 3 times with 1×PBS. Subsequently, the culture medium was replaced with RPMI-1640 medium containing different concentrations of BDQ and WX-081 for the assay, the medium containing vehicle (DMSO) was used as control. At days 0, 1, 3 and 5, the cells were washed once with PBS and lysed with Triton X-100 (0.1% (v/v)). One hundred microliters of 10-fold serial dilutions of the cell lysate was plated on 7H10 agar and incubated at 37°C to determine the CFU counts. A CFU count curve was drawn over time to characterize the effect of BDQ or WX-081 in different treatment concentrations.
Statistical Analysis
Data analysis was performed using SPSS 26.0 software and GraphPad Prism 8.0. Correlation between BDQ MIC and WX-081 MIC for the clinical isolates was assessed using the Spearman’s correlation. For intracellular bactericidal assay, t-test was used to determine significant differences between the groups. Differences were considered to be statistically significant for P value of <0.05.
Results
MICs Distributions and ECOFFs of BDQ and WX-081
The MIC of BDQ and WX-081 against the Mtb reference strain (ie, H37Rv) was 0.062 μg/mL and 0.125 μg/mL, respectively. The MIC distributions of the 114 clinical isolates are presented in Figure 1. The MICs of WX-081 ranged from 0.0156 μg/mL to 1 μg/mL. The MIC50 and MIC90 of WX-081 were, respectively, at 0.25 μg/mL and 0.5 μg/mL, whereas 95.6% of the enrolled strains had MICs ≤0.25 μg/mL. Stratification according to the drug susceptibility to other anti-TB drugs, ie, the S-TB, MDR-TB and Pre-XDR did not present any significant difference (data not shown). In contrast, the MICs of BDQ ranged from 0.0078 μg/mL to 0.5 μg/mL, with MIC50=0.125 μg/mL and MIC90=0.25 μg/mL, respectively. For a given strain, the MIC of WX-081 was generally equivalent to or 2-fold more than BDQ. ECOFFs for BDQ and WX-081 were 0.25 μg/mL and 0.5 μg/mL in the tested isolates, respectively.
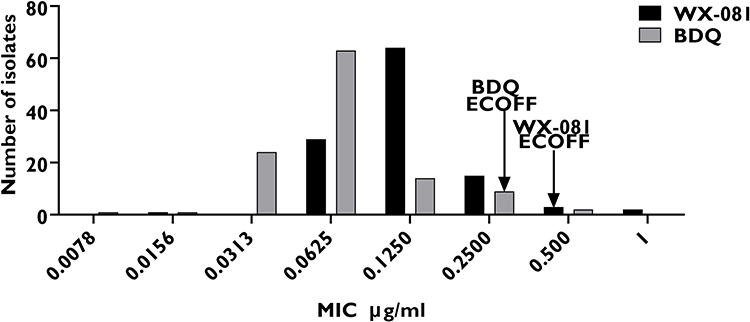 |
Figure 1 The MIC distributions of BDQ and WX-081 against Mtb clinical isolates. |
Spearman’s rank correlation coefficient revealed a significant correlation between the MIC of BDQ and WX-081 in the tested Mtb clinical strains (Figure 2A) (n = 114, Spearman’s q = 0.764, two tailed, P < 0.001. Correlation was considered significant at the 0.01). For S-TB strains, BDQ and WX-081 had a good correlation (n = 41, Spearman’s q = 0.840, two tailed, P< 0.001, Figure 2B). For MDR-TB strains, correlation of MIC between BDQ and WX-081 was also strong (n = 35, Spearman’s q = 0.773, P < 0.001, Figure 2C). Significant correlation was also detected in Pre-XDR strains (n = 38, Spearman’s q = 0.854, P<0.001, Figure 2D).
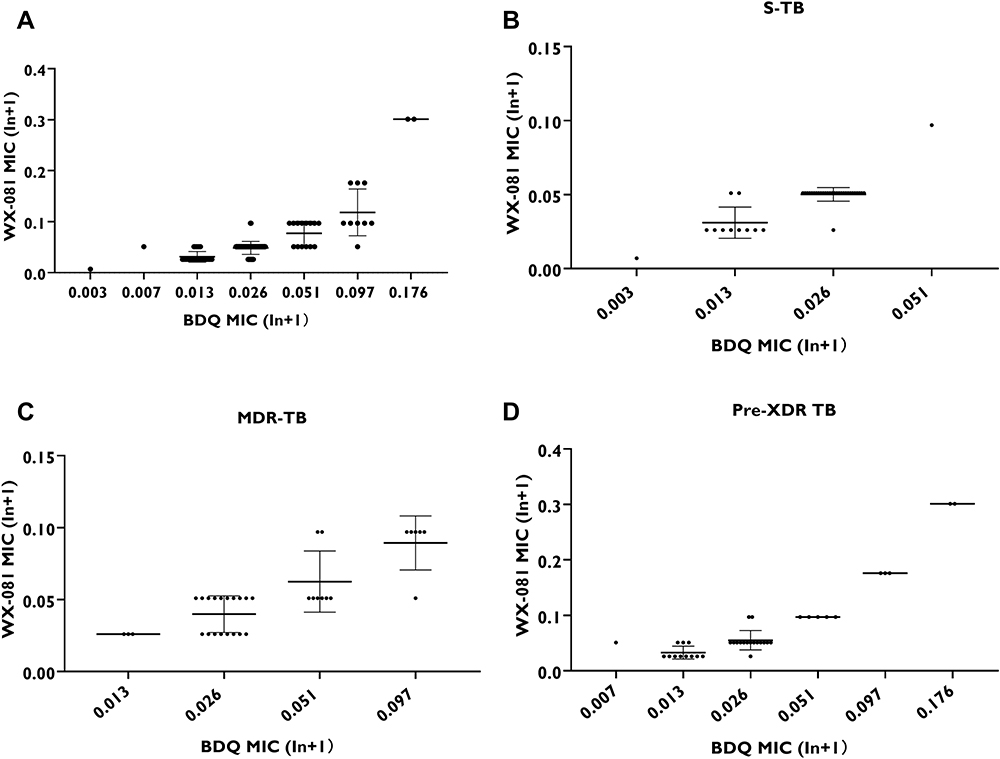 |
Figure 2 The correlation between BDQ MIC and WX-081 MIC against M. tuberculosis clinical isolates: (A) All the strains; (B) S-TB strains; (C) MDR-TB strains; (D) Pre-XDR TB strains; indicates P<0.001. |
MBC Determination
For the H37Rv and 6 randomly selected clinical isolates, the MBCs of WX-081 ranged from 0.5 μg/mL to 8 μg/mL, while BDQ ranged from 0.0625 μg/mL to 2 μg/mL (Table 1). Furthermore, the MBC/MIC ratio of BDQ ranged from 8 to 32, and that of WX-081 ranged from 16 to 64. The MBCs of WX-081 and BDQ against M. tuberculosis were not greater than 32×MICs, except for one MDR strain which was 64×MICs to WX-081. Therefore, just like BDQ, WX-081 should also be considered to possess antibacterial activity against most of the tested strains.
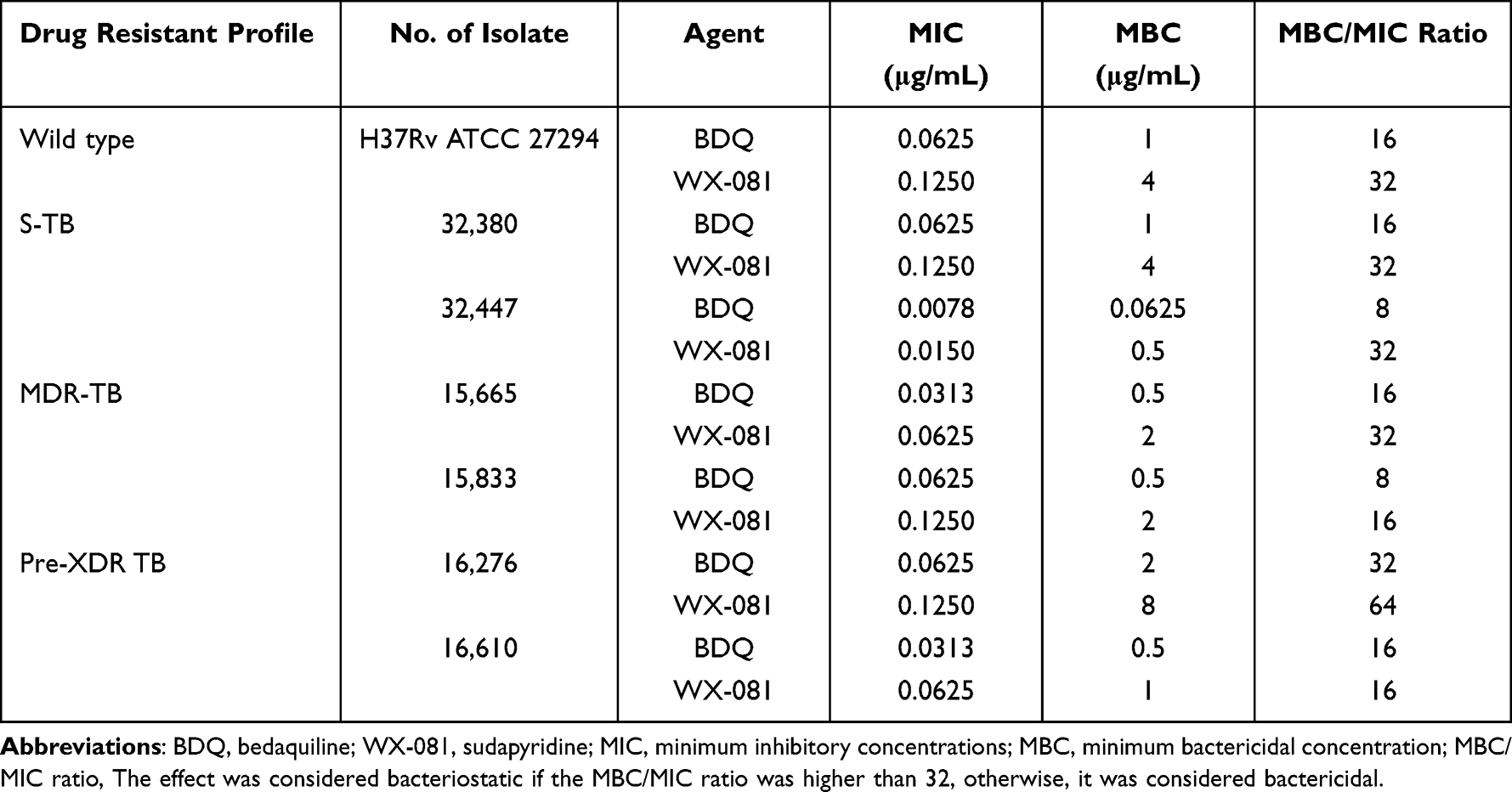 |
Table 1 The MBC/MIC Ratio of the Reference and Clinical Strains of M. tuberculosis |
Intracellular Bactericidal Activity of BDQ and WX-081
At MOI=5:1, the curves showed killing effect in all of the tested concentrations of BDQ and WX-081 during the 5-day exposure period (Figure 3). Both BDQ and WX-081 showed earlier bactericidal effect with no initial static phase against intracellular Mtb. The reduction of bacterial load was within 1.5 to 2 log10 CFU mL−1 in the exposure groups, obvious concentration-dependent killing activity was also observed for both BDQ and WX-081. Notably, on day 1, when incubated with WX-081 (1.86 μM) or BDQ (0.45 μM), the bacterial viability decreased to about 35.8% in contrast with day 0. Exposure to the highest concentrations of BDQ (3.60 μM) and WX-081 (14.90 μM), resulted in decrease of viability to 17.2%. Surprisingly, the differences in the concentration of the two drugs were marginal, while the growth curves of different groups were hardly indiscernible in Figure 3 except WX-081 at 14.90 μM, which presented the strongest kill effect among all tested groups.
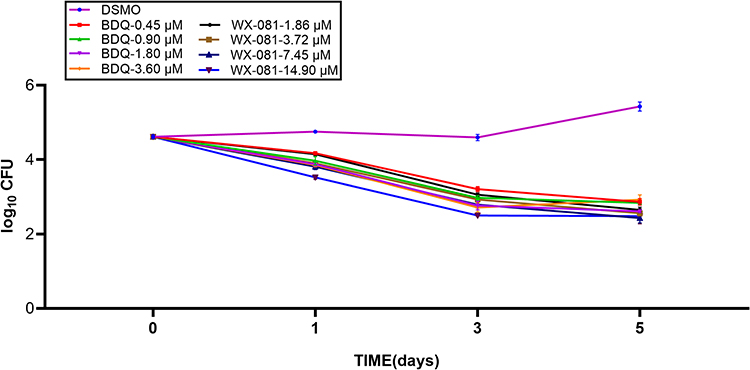 |
Figure 3 The antibacterial effect of BDQ and WX-081 against intracellular Mtb reference strain H37Rv. All data are shown as the means ± SD (n = 3); P<0.05. |
Discussion
The development of a novel anti-TB drug is expensive, time-consuming and often less successful. Therefore, re-structuring a used drug with the purpose of keeping the efficacy and overcoming its flaws becomes a feasible and practical strategy. WX-081 was developed by introducing structural modification in BDQ for acquiring an analog drug with equivalent anti-TB efficacy but better safety.
In this study, the in vitro and intracellular activity evaluation demonstrated strong anti-TB activities of WX-081. Additionally, WX-081 exhibited comparable activity against sensitive as well as drug-resistant clinical isolates, including MDR and Pre-XDR isolates. Compared with BDQ, the MIC value of WX-081 was generally equivalent to or marginally higher than BDQ. The pharmacokinetic study of BDQ demonstrated that Cmax was 1.715 μg/mL,18 which is dozens of folds higher than common MIC values of the clinical isolates, and was usually much higher than the target effective plasma concentration, ie, 0.6 μg/mL.19 Multiple species study with mouse and rat demonstrated that evidently higher serum concentrations and lung tissue concentrations were acquired for WX-081 than BDQ, despite being administered at the same dosage. After oral administration of WX-081/BDQ at doses of 6.25 mg/kg in Mice, the Cmax of WX-081 was 503 ng/mL, which was slightly lower than BDQ (608 ng/mL), and AUC0-last of WX-081 was 10,155 ng×h/m, which was nearly twice of that of BDQ (6038 ng/mL). Similar trend in PK parameters was seen in rat after oral administration of WX-081/BDQ.14 Specifically, the preclinical PK study showed that a few folds higher lung tissue concentration was obtained for WX-081 than BDQ. Lung Concentration of BDQ and WX-081 at the same oral dose after 96h time point in mice was 135 ng/g and 857 ng/g, respectively.13 Therefore, equivalent in vivo efficacy could be reasonably expected between the two drugs. The unblended outcomes of the Phase II clinical trial of WX-081, which will be released soon, would validate the above speculation.
The MIC50, MIC90 and ECOFFs of WX-081 and BDQ are very consistent with the MIC distribution patterns. All of these parameters for WX-081 were one-fold higher than BDQ. Therefore, it was not surprising to see a significant correlation between MICs of BDQ and WX-081 in Mtb clinical strains, as suggested by the Spearman’s rank correlation coefficient at a Spearman value of 0.764. Stratification of the isolates according to the drug susceptibility profiles showed that the MDR-TB group had a relatively lower correlation coefficient than other groups, but this value was still indicative of a very strong correlation between the MICs of the two drugs. These outcomes were very reasonable because the two drugs shared the same antibacterial mechanism. Two Pre-XDR strains harbored the highest MIC to BDQ at 0.5 μg/mL and had MIC to WX-081 at 1 μg/mL, which was also the highest MIC value to WX-081 among all the tested isolates.
The MBC test showed that both drugs possessed certain level of bactericidal activities. However, both MBC ranges had a wide concentration distribution. The MBCs of WX-081 ranged from 0.5 μg/mL to 8 μg/mL and ranged from 0.0625 μg/mL to 2 μg/mL for BDQ. The higher concentrations in these ranges for both drugs were much greater than the ECOFFs defined in this study, ie, for BDQ at 0.25 μg/mL and for WX-081 at 0.5 μg/mL. ECOFF is generally set up for breakpoint definition. Additionally, the higher concentrations in BDQ range overlapped the Cmax of plasma concentration, which could possibly be the case for WX-081 as well. Therefore, for some isolates the MBC might not be attainable in real practice.
In this study, we evaluated the killing effect of WX-081 against the Mtb H37Rv in macrophages and compared it with BDQ.13,14 We simulated the possible plasma concentrations of the two drugs when administered to patients at the recommended dosages. Both drugs demonstrated time-concentration dependent killing effects, which are mainly caused by their mechanism of action. However, our outcomes seemed better than the study performed directly on bacteria in vitro with WX-081, even the lowest tested concentration (1.86 μM) manifested killing effects. Since these drugs have high protein binding rate (>99%) and very long elimination half-life,13,20 a plausible explanation for killing effect could be partly caused by the accumulation of drug in the cells. Compared with the in vitro study, the intracellular killing curves were consistent between different concentrations, and manifested a gentle declining tendency. This phenomenon might also reflect the gradual accumulation of drug in the cells.
The efficacy of WX-081 against TB remains well proven only in vitro, in macrophages and in animal models. A clinical trial (currently ongoing) is expected to characterize the results of its efficacy in treating patients soon. Further clinical studies and should be performed and synergistic effects of WX-081 with other compounds should be determined for better understanding its usage as a new anti-TB reagent.
This study has some limitations. Firstly, all the tested M. tuberculosis isolates were collected from a single hospital, Beijing chest hospital, a designated clinical center on tuberculosis; thus, the activity of WX-081 need further validation against clinical isolates of tuberculosis from different countries. Secondly, the antimicrobial activity in animal models and macrophages does not always reflect the drug response in human; therefore, more clinical trials are warranted to prove our findings in this study.
In conclusion, WX-081 exhibited high antibacterial activity against M. tuberculosis in vitro and in macrophages. Sudapyridine may be a promising candidate drug for the treatment of tuberculosis, especially drug-resistant tuberculosis.
Funding
This work was supported by the Natural Science Fund of China (82072328), the Beijing Hospitals Authority Youth Programme (QML20211602), the Tongzhou Science and technology Project (KJ2022CX041), and the Beijing Hospitals Authority’ Ascent Plan (DFL20221401).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. World Health Organization. Global tuberculosis report 2021; 2021. Available from: https://www.who.int/teams/global-tuberculosis-programme/data.
2. Fellous S, Rkain H, Tahiri L, Bouraqadi A, Nassar I, Allali F. Pre-extensively drug-resistant tuberculosis spondylodiscitis in an immunocompetent patient: a case report. Pan Afr Med J. 2020;36:165. doi:10.11604/pamj.2020.36.165.21689
3. Garg RK, Rizvi I, Malhotra HS, Uniyal R, Kumar N. Management of complex tuberculosis cases: a focus on drug-resistant tuberculous meningitis. Expert Rev Anti Infect Ther. 2018;16:813–831. doi:10.1080/14787210.2018.1540930
4. Kherabi Y, Fréchet-Jachym M, Rioux C, et al. Revised definitions of tuberculosis resistance and treatment outcomes, France, 2006–2019. Emerg Infect Dis. 2022;28:1796–1804. doi:10.3201/eid2809.220458
5. Lange C, Chesov D, Heyckendorf J, Leung CC, Udwadia Z, Dheda K. Drug-resistant tuberculosis: an update on disease burden, diagnosis and treatment. Respirology. 2018;23:656–673. doi:10.1111/resp.13304
6. Andries K, Verhasselt P, Guillemont J, et al. A diarylquinoline drug active on the ATP synthase of Mycobacterium tuberculosis. Science. 2005;307:223–227. doi:10.1126/science.1106753
7. Li Y, Sun F, Zhang W. Bedaquiline and delamanid in the treatment of multidrug-resistant tuberculosis: promising but challenging. Drug Dev Res. 2019;80:98–105. doi:10.1002/ddr.21498
8. Ardhianto D, Suharjono S, Fatmawati U, Fatmawati U. Analysis of the side effect of QTc interval prolongation in the bedaquiline regimen in drug resistant tuberculosis patients. J Basic Clin Physiol Pharmacol. 2021;32:421–427. doi:10.1515/jbcpp-2020-0415
9. Saeed DK, Shakoor S, Razzak SA, et al. Variants associated with Bedaquiline (BDQ) resistance identified in Rv0678 and efflux pump genes in Mycobacterium tuberculosis isolates from BDQ naïve TB patients in Pakistan. BMC Microbiol. 2022;22:62. doi:10.1186/s12866-022-02475-4
10. Wu SH, Chan HH, Hsiao HC, Jou R. Primary bedaquiline resistance among cases of drug-resistant tuberculosis in Taiwan. Front Microbiol. 2021;12:754249. doi:10.3389/fmicb.2021.754249
11. Patel H, Pawara R, Pawara K, Ahmed F, Shirkhedkar A, Surana S. A structural insight of bedaquiline for the cardiotoxicity and hepatotoxicity. Tuberculosis. 2019;117:79–84. doi:10.1016/j.tube.2019.06.005
12. Nguyen TVA, Anthony RM, Bañuls AL, Nguyen TVA, Vu DH, Alffenaar JC. Bedaquiline resistance: its emergence, mechanism, and prevention. Clin Infect Dis. 2018;66:1625–1630. doi:10.1093/cid/cix992
13. Huang Z, Luo W, Xu D, et al. Discovery and preclinical profile of sudapyridine (WX-081), a novel anti-tuberculosis agent. Bioorg Med Chem Lett. 2022;71:128824. doi:10.1016/j.bmcl.2022.128824
14. Yao R, Wang B, Fu L, et al. Sudapyridine (WX-081), a novel compound against Mycobacterium tuberculosis. Microbiol Spectr. 2022;10:e0247721. doi:10.1128/spectrum.02477-21
15. Pang Y, Zheng H, Tan Y, Song Y, Zhao Y. In vitro activity of bedaquiline against nontuberculous mycobacteria in China. Antimicrob Agents Chemother. 2017;61. doi:10.1128/AAC.02627-16
16. Clinical and Laboratory Standards Institute. Susceptibility Testing of Mycobacteria, Nocardia, and Other Aerobic Actinomycetes; Approved Standard.
17. Clinical and Laboratory Standards Institute. M26-A: Methods for Determining Bactericidal Activity of Antimicrobial Agents. Clinical and Laboratory Standards Institute; 1999.
18. Ngwalero P, Brust JCM, van Beek SW, et al. Relationship between plasma and intracellular concentrations of bedaquiline and its M2 metabolite in South African Patients with rifampin-resistant tuberculosis. Antimicrob Agents Chemother. 2021;65:e0239920. doi:10.1128/AAC.02399-20
19. Perrineau S, Lachâtre M, Lê MP, et al. Long-term plasma pharmacokinetics of bedaquiline for multidrug- and extensively drug-resistant tuberculosis. Int J Tuberc Lung Dis. 2019;23:99–104. doi:10.5588/ijtld.18.0042
20. Kempker RR, Smith AGC, Avaliani T, et al. Cycloserine and linezolid for tuberculosis meningitis: pharmacokinetic evidence of potential usefulness. Clin Infect Dis. 2021;72(7):1244–1246. doi:10.1093/cid/ciaa877
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.