Back to Journals » Infection and Drug Resistance » Volume 19
A Short-Course Regimen Containing Delamanid, Bedaquiline and Linezolid for the Treatment of Drug-Resistant Tuberculosis: A Retrospective Study from China
Authors Jin L, Zhang X, Jiang H, Li Q, Liu W, Wang J, Cao Z, Liu Y
Received 29 January 2026
Accepted for publication 11 May 2026
Published 10 July 2026 Volume 2026:19 596822
DOI https://doi.org/10.2147/IDR.S596822
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hemant Joshi
Long Jin, Xiaolei Zhang, Huailong Jiang, Qijian Li, Weinan Liu, Jiayao Wang, Zheyu Cao, Yuqin Liu
Department of Internal Medicine for Tuberculosis, Infectious Disease Hospital of Heilongjiang Province, Harbin, 150500, People’s Republic of China
Correspondence: Yuqin Liu, Department of Internal Medicine for Tuberculosis, Infectious Disease Hospital of Heilongjiang Province, No. 1 Jian She Street, Hulan District, Harbin, Heilongjiang, 150500, People’s Republic of China, Email [email protected]
Purpose: To assess the efficacy and safety of delamani (Dlm), bedaquiline (Bdq) and linezolid (Lzd) in multidrug-resistant tuberculosis (MDR-TB) and rifampicin-resistant tuberculosis (RR-TB).
Patients and Methods: We retrospectively analyzed the clinical data of 71 patients with MDR/RR-TB. All patients were given a 6– 9 month short-course treatment based on Dlm, Bdq and Lzd. Outcomes included treatment success, sputum culture conversion rate and time, clinical and imaging improvement, adverse events (AEs), serious adverse events (SAEs), and QTcF prolongation were recorded. Logistic regression and Cox proportional hazards models were used to identify factors associated with treatment success and time to sputum culture conversion, respectively.
Results: 57.75% of patients were male, and the median (IQR) age of all patients was 42.00 (30.50, 54.00) years. At the end of the treatment, 73.24% of patients achieved a good therapeutic outcome, 85.19% of patients achieved negative sputum culture, and the median (IQR) time for sputum culture to turn negative was 62.50 (28.00, 126.00) days. The clinical symptoms of the patients were all significantly improved (P < 0.001). 94.37% of patients showed lesion absorption, and the proportion of lesion area/volume to the whole lung was significantly reduced (P < 0.001). 36.62% of patients developed any grade AEs, the incidence of grade ≥ 3 AEs was 8.45%, and one patient (1.41%) developed SAEs, which was grade 4 anemia caused by Lzd. 12.68% of patients experienced prolonged QTcF. Previous history of tuberculosis (OR = 0.188, P = 0.015) and hepatitis B (OR = 0.150, P = 0.038) was associated with non-favorable outcomes. No baseline characteristics were associated with time to sputum culture conversion (P > 0.05).
Conclusion: The Dlm–Bdq–Lzd regimen demonstrated favorable efficacy and safety in patients with MDR/RR-TB, and may represent a mechanistically distinct, shorter-course alternative to conventional regimens, while potential risks such as prolonged QTcF need to be noted.
Keywords: tuberculosis, rifampicin-resistant TB, RR-TB, multidrug-resistant TB, MDR-TB, delamanid, bedaquiline, linezolid
Introduction
Tuberculosis (TB), a disease caused by Mycobacterium TB infection, is a serious global public health problem,1 resulting in the deaths of more than one million people per year.2 In addition to its widespread prevalence, the drug resistance of Mycobacterium TB stands as another factor contributing to the significant challenges in global TB control. Drug-resistant TB can be further classified into rifampicin-resistant TB (RR-TB) and multidrug-resistant TB (MDR-TB) that is resistant to both rifampicin and isoniazid.3 The latest research indicates that there have been 465,000 new cases of MDR/RR-TB patients worldwide. Among these patients, only 37.1% have been diagnosed and referred for treatment.4 A previous study reported that the mortality rate of patients with MDR/RR-TB reached 14.68%.5 China is one of the countries with the heaviest TB burden, and its MDR/RR-TB patients account for 13% of the total global count.6 Therefore, reducing the incidence rate and the mortality rate of MDR/RR-TB patients has gradually become the keys to the treatment of TB both in China and worldwide.
Clinical studies have shown that the treatment of TB must involve the administration of multiple drugs for several months in order to achieve effective and long-lasting therapeutic effects. However, due to the development of resistance to standard treatment drugs, the treatment of drug-resistant TB requires the administration of more than four drugs for up to 24 months, and the treatment is not standardized, which increases the burden on patients. In addition, drugs targeting drug-resistant TB may easily cause adverse reactions such as hepatotoxicity, bone marrow suppression, and peripheral neuropathy. Approximately 10% to 15% of patients discontinue treatment due to their inability to tolerate adverse reactions.7,8 These above-mentioned factors prevent drug-resistant TB patients from securing satisfactory treatment effects (cure rate < 50%).9 Hence, the development and clinical application of novel treatment are extremely crucial for curing drug-resistant TB.
In recent years, short-course regimens centered on oral drugs such as delamanid (Dlm), bedaquiline (Bdq), and linezolid (Lzd) have gradually attracted attention. Dlm belongs to the nitro-dihydroimidazolazole class of compounds.10 It is a mycotic acid biosynthesis inhibitor, which can block the production of mycolic acid, a key component of the cell wall of Mycobacterium TB.11 Dlm is active against both replicating and dormant bacilli as well as extracellular and intracellular bacilli.12 Previous studies have shown that in adult patients with MDR-TB, after two months of treatment, the sputum culture conversion rate of patients treated with Dlm combined with the optimized background protocol (OBR) was significantly higher than that of patients with placebo combined with OBR.13 Dlm has also been found to have a relatively high therapeutic effect in children with MDR-TB.14 Bdq belongs to the diarylquinoline class of compounds and is an inhibitor of mycobacterial ATP synthase. By specifically binding to the c subunit of the F0 domain of Mycobacterium TB, Bdq blocks ATP synthesis, thereby preventing the ATP energy supply of mycobacteria and exerting antibacterial effects.15 Studies have shown that adding Bdq and clofazimine to the treatment can effectively improve the prognosis of patients with MDR-TB.16 Lzd is an oxazolidinone originally approved for the treatment of gram-positive bacterial infections. Lzd binds to the peptidyl transferase center (PTC), a critical region within the 50S subunit, and interfere with tRNA binding and TB protein synthesis.17 An observational study showed that Lzd combined with the background regimen for the treatment of MDR-TB had a treatment success rate of 77.36% and a sputum culture negative conversion rate of 88.45%.18
Dlm, Bdq, and Lzd are all clinically available agents for the treatment of tuberculosis and have been incorporated into current MDR/RR-TB regimens. In 2014, the WHO issued guidelines for the use of Dlm in adults under limited conditions. Later, in the treatment guidelines for RR-TB, Dlm was classified as a Group C drug.19 From 2019 to 2022, the WHO recommended two of the most effective Group A drugs, Bdq and Lzd, for the treatment of MDR-TB.20 However, despite their inclusion in WHO-recommended regimens, real-world evidence regarding the combined use of Dlm, Bdq, and Lzd—particularly in the Chinese MDR/RR-TB population—remains limited. In addition, the clinical applicability, efficacy, and safety profile of this three-drug combination as a structured short-course regimen have not been well characterized. Therefore, this study aims to retrospectively evaluate the efficacy and safety of a Dlm–Bdq–Lzd-based regimen, and to further explore its potential clinical value as a mechanistically complementary treatment strategy.
Materials and Methods
Study Design
This study was a retrospective, single-center, cohort study. The aim was to evaluate the efficacy and safety of 6–9 month short-course treatment regimens based on Dlm, Bdq, and Lzd in the clinical treatment of patients with MDR-TB and RR-TB.
Participants
71 patients with MDR-TB and RR-TB who received Dlm, Bdq, and Lzd as the basis treatment at the Infectious Disease Hospital of Heilongjiang Province from March 12, 2023 to August 6, 2024 were selected. All patients were informed and signed the informed consent form. This study was approved by the Ethics Committee of the Infectious Disease Hospital of Heilongjiang Province (Approval No. 2025019).
Inclusion criteria: 1) Patients diagnosed with MDR/RR-TB; 2) Age of patients ≥ 18 years; 3) Patients who have received treatment with Bdq, Dlm, and Lzd-based regimens for at least one week.
Exclusion criteria: 1) Patients who have received Dlm, Bdq, or Lzd regimens for more than one month in the past or are known to be resistant to any of these drugs; 2) Patients who have participated in any other clinical trials of drugs or medical devices within two months prior to the screening; 3) Patients who are deemed unsuitable to participate in the trial by the researchers.
Treatment Regimens
All the enrolled patients received treatment regimens based on Dlm, Bdq and Lzd for 6 to 9 months. Among them:
Dlm: 100 mg each time, orally, twice a day;
Bdq: 400 mg each time, orally, once a day for 2 weeks, then 200 mg, three times a week. There should be at least a 48-hour interval between the two administrations;
Lzd: 600 mg each time, orally, once a day. When intolerance occurs, the dosage will be reduced to 300 mg once a day or discontinued.
The treatment lasts for 6 months. If the bacteriological tests remain positive after 4 months of treatment and the clinical response improves, the course can be extended to 9 months. If the clinical response is unsatisfactory after 6 months and the bacteriology remain positive, the possibility of treatment failure should be considered. If treatment failure is determined, sputum culture and drug sensitivity test (DST) are required, and an individualized remedial treatment plan should be formulated based on the DST results.
Clinicians decide whether to incorporate additional drugs other than Dlm, Bdq, and Lzd, and formulate a treatment plan based on the actual diagnosis and treatment outcomes.
Patient Monitoring
During the treatment period, the patient should undergo at least one systematic laboratory test every month, including routine blood test, blood biochemistry tests (liver and kidney function), electrolyte panel test, and thyroid function test. Chest imaging examinations and other examinations required according to actual clinical conditions are conducted. Baseline electrocardiogram tests should be conducted at the beginning of the treatment, every two weeks during the first three months of treatment, and once a month thereafter. The QTc interval (corrected using the Fridericia formula (QTcF)) is calculated by the attending clinician.21 Repeat the electrocardiogram examination only when QTcF is abnormal. Bacteriological tests, including sputum smears and sputum cultures (on solid or liquid media), are conducted once a month until the end of the course of treatment, and additional DST is applied to first-line and second-line drugs when positive culture results are obtained.
Study Outcomes
Primary Endpoints
Effectiveness: 1) Percentage of patients achieving treatment success (cured+treatment completed) at the end of treatment (Patient outcomes are defined by WHO criteria, including cured, treatment completed, treatment failure, lost to follow-up, and death).22 2) The negative conversion rate of sputum culture in patients. 3) The median time for sputum culture to turn negative.
Safety: Percentage of serious adverse events (SAEs) at the end of treatment.
Secondary Endpoints
Effectiveness: 1) The percentage of improvement in patients’ symptoms (cough, expectoration, hemoptysis, chest pain, dyspnea, fatigue, weight loss, fever) at the completion of treatment. 2) The improvement of the patient’s imaging (lesions, cavities) at the completion of treatment.
Safety: 1) Percentage of adverse events (AEs) at the end of treatment. 2) The percentage of QTcF extension during treatment (QTcF interval ≥ 500 ms or any QTcF interval extended by more than 60 ms from baseline).
Statistical Analysis
Categorical variables were described by frequencies and percentages n (%), while continuous variables were described by mean and standard deviations (SD) (for normally distributed variables) or median and interquartile range (IQR) (for non-normally distributed variables). Intra-group comparisons before and after treatment were conducted using McNemar’s test (for categorical variables) or Wilcoxon signed-rank test (for non-normally distributed continuous variables). The median time and 95% confidence interval (CI) of the time for sputum culture to turn negative were calculated using the Kaplan-Meier method. Univariate and multivariate analyses were performed using logistic regression (for treatment success) and Cox proportional-hazards model (for time to sputum culture conversion).
Analyses were conducted using R software (version 4.4.1; R Core Team, Vienna, Austria). Two-sided P values of < 0.05 were considered to be statistically significant.
Results
Baseline Characteristics of the Participants
A total of 71 patients with MDR/RR-TB were included in this study, among whom 57.75% (41/71) were male patients. The median age of the patients was 42.00 years. The baseline Karnofsky performance score (KPS) of the patient was 90.00. The baseline QTcf of the patient was 403.74ms. In terms of medical history, 59.15% (42/71) of the patients had a previous history of TB, and 18.31% (13/71) of the patients had a history of diabetes. At baseline, 97.18% (69/71) of the patients presented with TB-related clinical symptoms, including cough (87.32%), expectoration (71.83%), fatigue (47.89%), fever (33.80%), dyspnea (26.76%), weight loss (25.35%), chest pain (22.54%), and hemoptysis (11.27%). The bacteriological results indicated that 76.06% (54/71) of the patients had positive sputum cultures at baseline, and 39.44% (28/71) of the patients had positive sputum smears. Imaging results indicated that 71.83% (51/71) of the patients had pulmonary cavities at the baseline period. Among them, 53.52% (38/71) of the patients had no more than 2 cavities, and 45.07% (32/71) of the patients had 3 to 6 cavities. 97.18% of the patients (69/71) had lesions involving both lungs, and the median lesion area/volume accounted for 20.00% of the whole lung area.
The treatment regimens for the patients were as follows: Dlm, Bdq, and Lzd were used in all patients (during the treatment process, contezolid was used instead of Lzd in two patients). The number of anti-TB drugs in the protocol was 4.52 (1.53). Concomitant drugs included moxifloxacin (32.39%), amikacin (29.58%), cycloserine (21.13%), clofazimine (15.49%), pyrazinamide (15.49%), para-aminosalicylic acid (9.86%), ethambutol (8.45%), protionamide (7.04%), levofloxacin (5.63%), rifampicin (1.41%), and isoniazid (1.41%). 40.85%, 4.23% and 1.41% of the patients had one, two and three types of QT interval prolonging drugs (moxifloxacin, levofloxacin and clofazimine) added to their treatment regimens, respectively. The specific baseline characteristics of the patients are shown in Table 1.
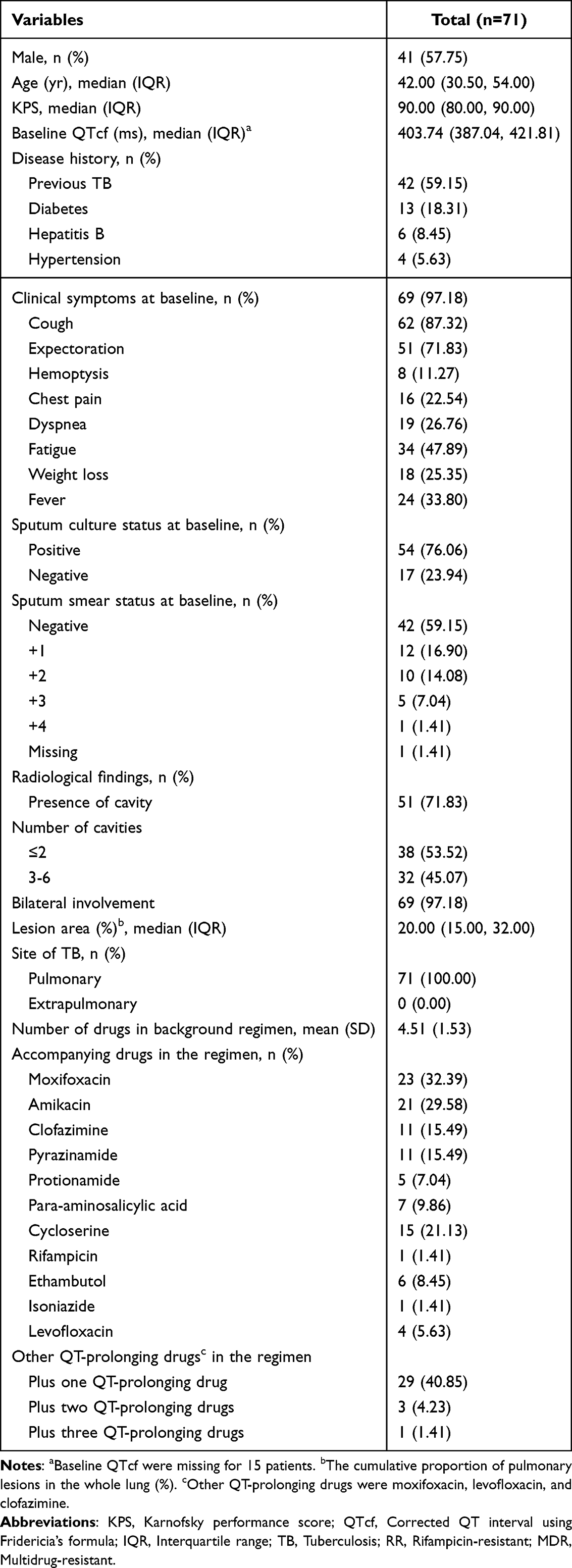 |
Table 1 Baseline Characteristics of Participants |
Efficacy
The Treatment Outcomes and the Results of Sputum Culture Conversion
73.24% (52/71) of the patients achieved the good outcome as defined by the WHO at the end of the treatment, among which 71.83% (51/71) were cured and 1.41% (1/71) completed the treatment. 85.19% (46/54) of the patients achieved negative sputum culture conversion (SCC) at the end of the treatment. The median time for sputum culture to turn negative was 62.50 days. As shown in Table 2 and Figure 1.
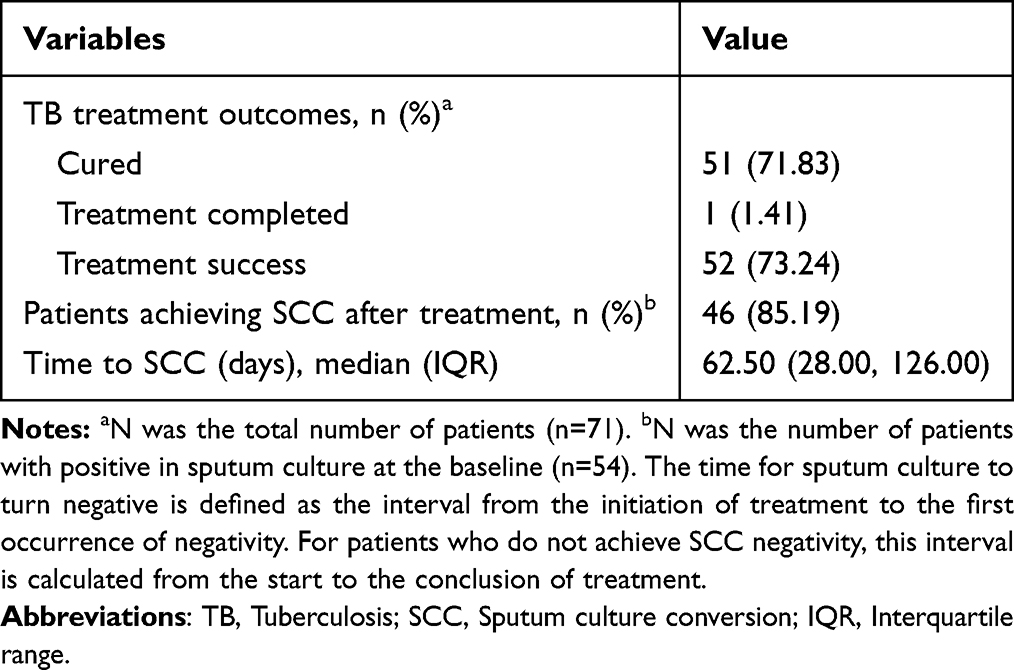 |
Table 2 The Treatment Outcomes and the Results of Sputum Culture Conversion |
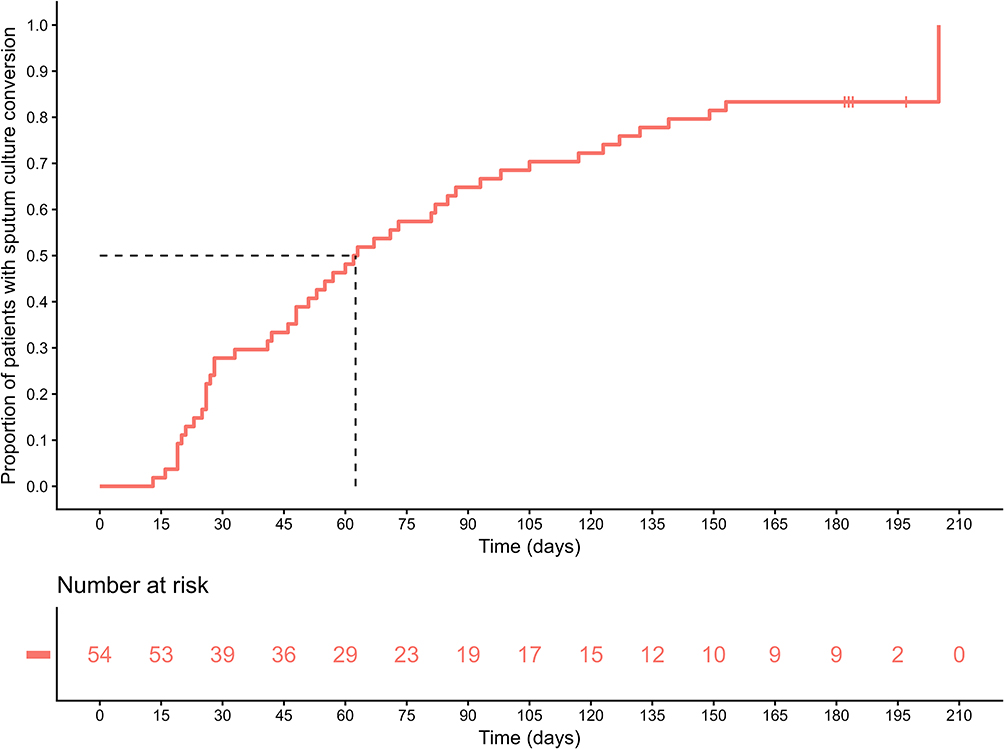 |
Figure 1 The time for sputum culture to turn negative. |
The Improvement in Clinical Symptoms
At the end of the treatment, the clinical symptoms related to TB improved significantly (Cough: 87.32% vs. 5.71%, P < 0.001; Expectoration: 71.83% vs. 2.86%, P < 0.001; Hemoptysis: 11.27% vs. 0.00%, P < 0.001; Chest pain: 22.54% vs. 2.86%, P < 0.001; Dyspnea: 26.76% vs. 0.00%, P < 0.001; Fatigue: 47.89% vs. 7.14%, P < 0.001; Weight loss: 25.35% vs. 0.00%, P < 0.001; Fever: 33.80% vs. 0.00%, P < 0.001). As shown in Table 3 and Figure 2.
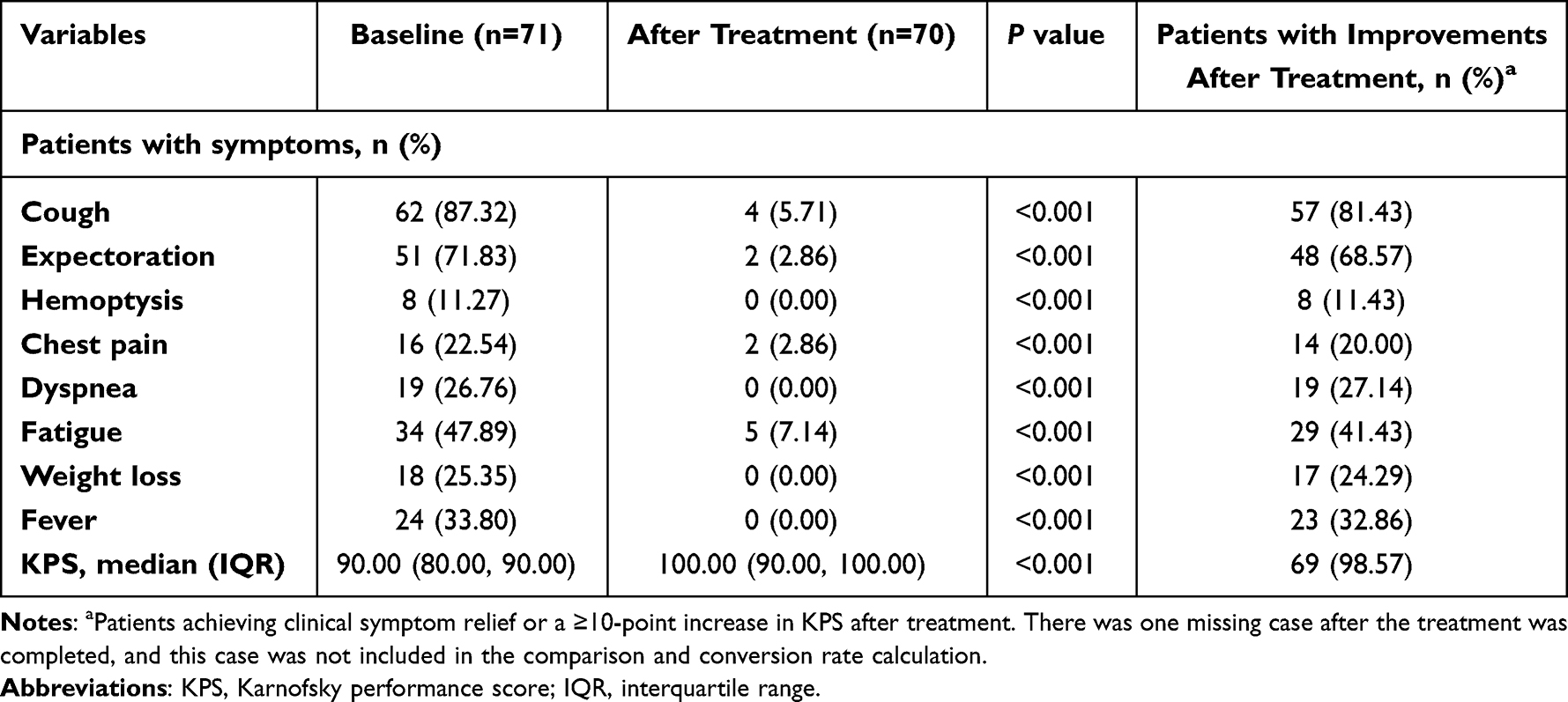 |
Table 3 The Improvements in Clinical Symptoms |
 |
Figure 2 The improvement of clinical symptoms. (A) The propotion of patients with symptoms at baseline and after treatment. (B) The proportion of patients whose symptoms improved after treatment. |
The Improvements in Radiological Results
After the treatment, 94.37% (67/71) of the patients showed TB lesion absorption. 5.63% (4/71) of the patients showed slight TB lesion absorption. 39.44% (28/71) of the patients showed shrinkage of TB cavity. 54.93% (39/71) of the patients showed shrinkage and calcification of TB cavity. 4.23% (3/71) of the patients showed slight shrinkage of TB cavity (Table 4). After treatment, the proportion of lesion area/volume in the entire lung of the patients decreased significantly (P < 0.001) (Figure 3).
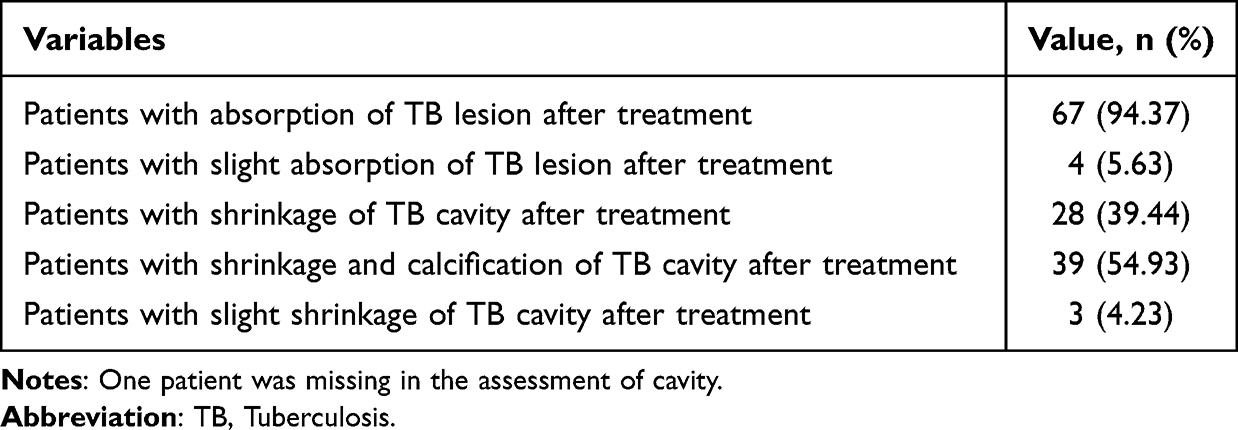 |
Table 4 The Improvements in Radiological Results |
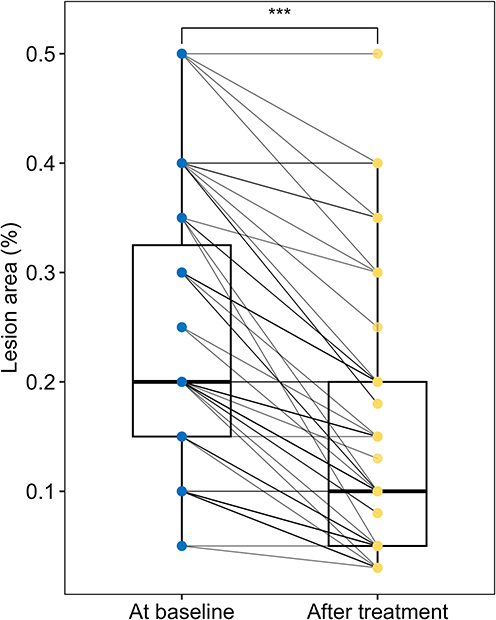 |
Figure 3 The improvements in pulmonary lesion. ***P<0.001. |
Safety
36.62% (26/71) of the patients experienced AEs. The incidence of grade ≥3 AEs was 8.45% (6/71), and one patient (1.41%) experienced SAE, which was grade 4 anemia caused by Lzd. Prolonged QTcF occurred in 12.68% (9/71) of the patients (Table 5). After the treatment, the patients’ QTcFs were significantly longer than the baseline (P < 0.001) (Figure 4).
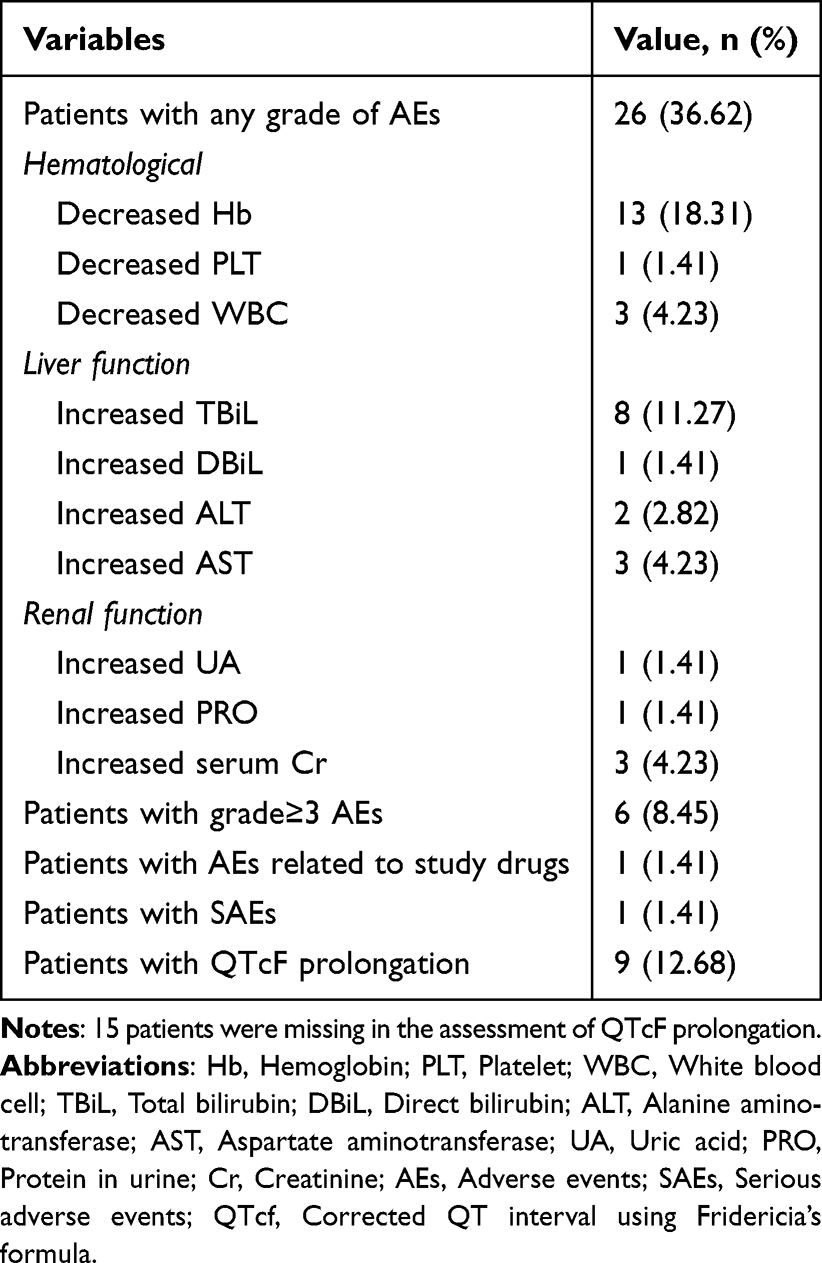 |
Table 5 Overall Safety During Treatment Period |
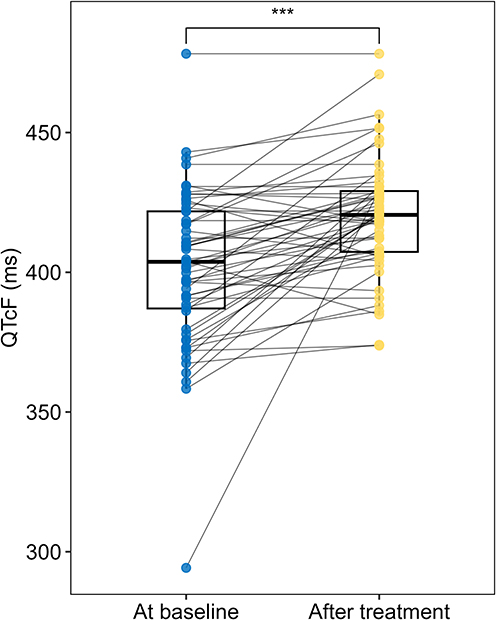 |
Figure 4 Changes in QTcF of patients at baseline and after treatment. ***P<0.001. |
Factors Associated with Treatment Success and Time to Sputum Culture Conversion
Univariate analysis showed that a previous history of TB (OR = 0.188, 95% CI = 0.040–0.646, P = 0.015) and a previous history of hepatitis B (OR = 0.150, 95% CI = 0.019–0.845, P = 0.038) were associated with a lower likelihood of achieving treatment success. However, in the multivariate analysis, only a previous history of TB remained independently associated with treatment success (OR = 0.204, 95% CI: 0.036–0.831, P = 0.040), while hepatitis B showed a non-significant trend (P = 0.085). Other baseline characteristics, including gender, age, KPS score, history of diabetes, history of hypertension, sputum smear results, presence of cavities, and the number of cavities, were not significantly associated with treatment success (P > 0.05) (Table 6).
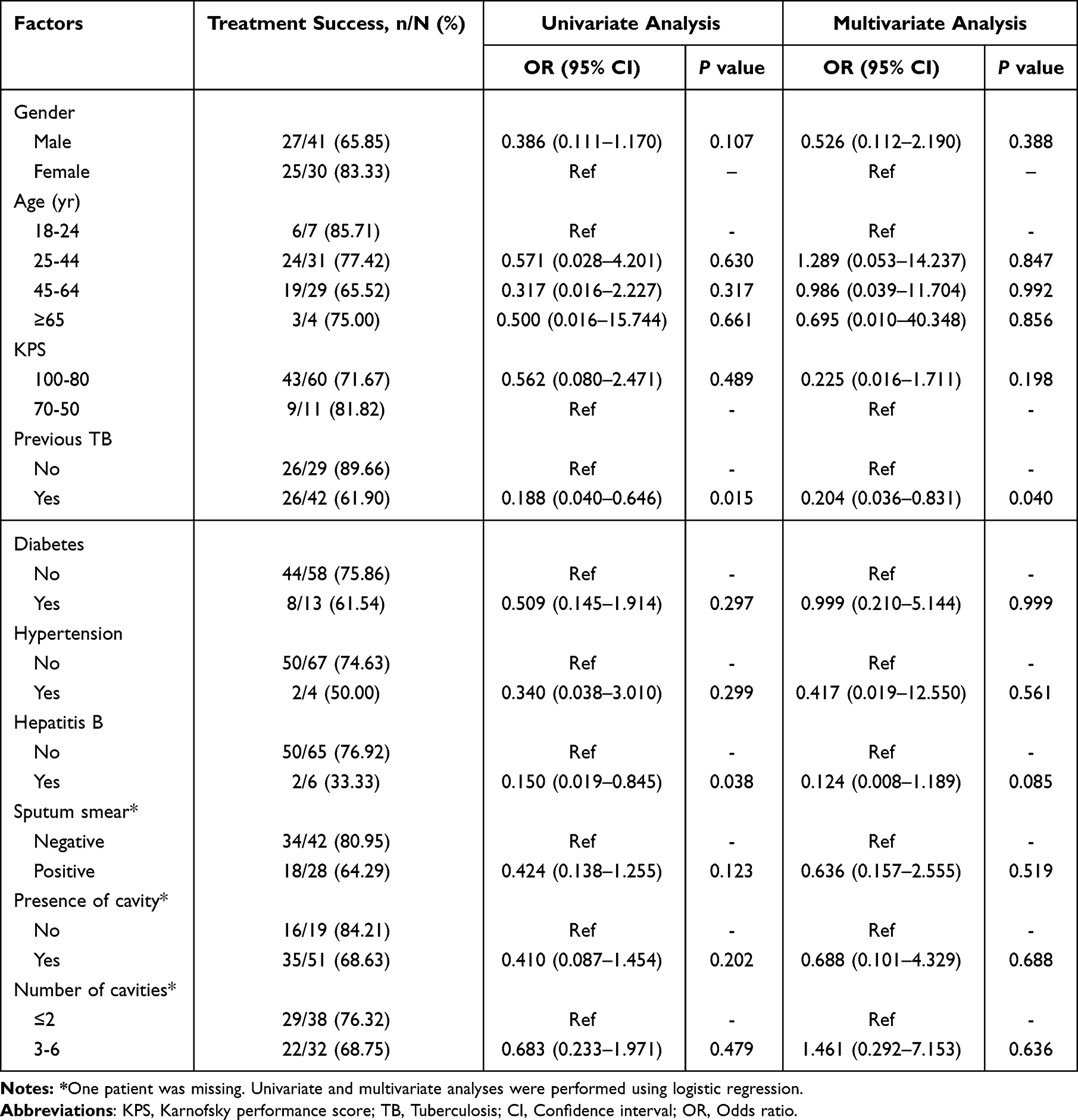 |
Table 6 Factors Associated with Treatment Success |
The factors, including gender, age, KPS score, history of TB, history of diabetes, history of hypertension, sputum smear results, presence or absence of cavities, and the number of cavities, were not significant associated with time to sputum culture conversion in either univariate or multivariate Cox regression analyses (P > 0.05) (Table 7).
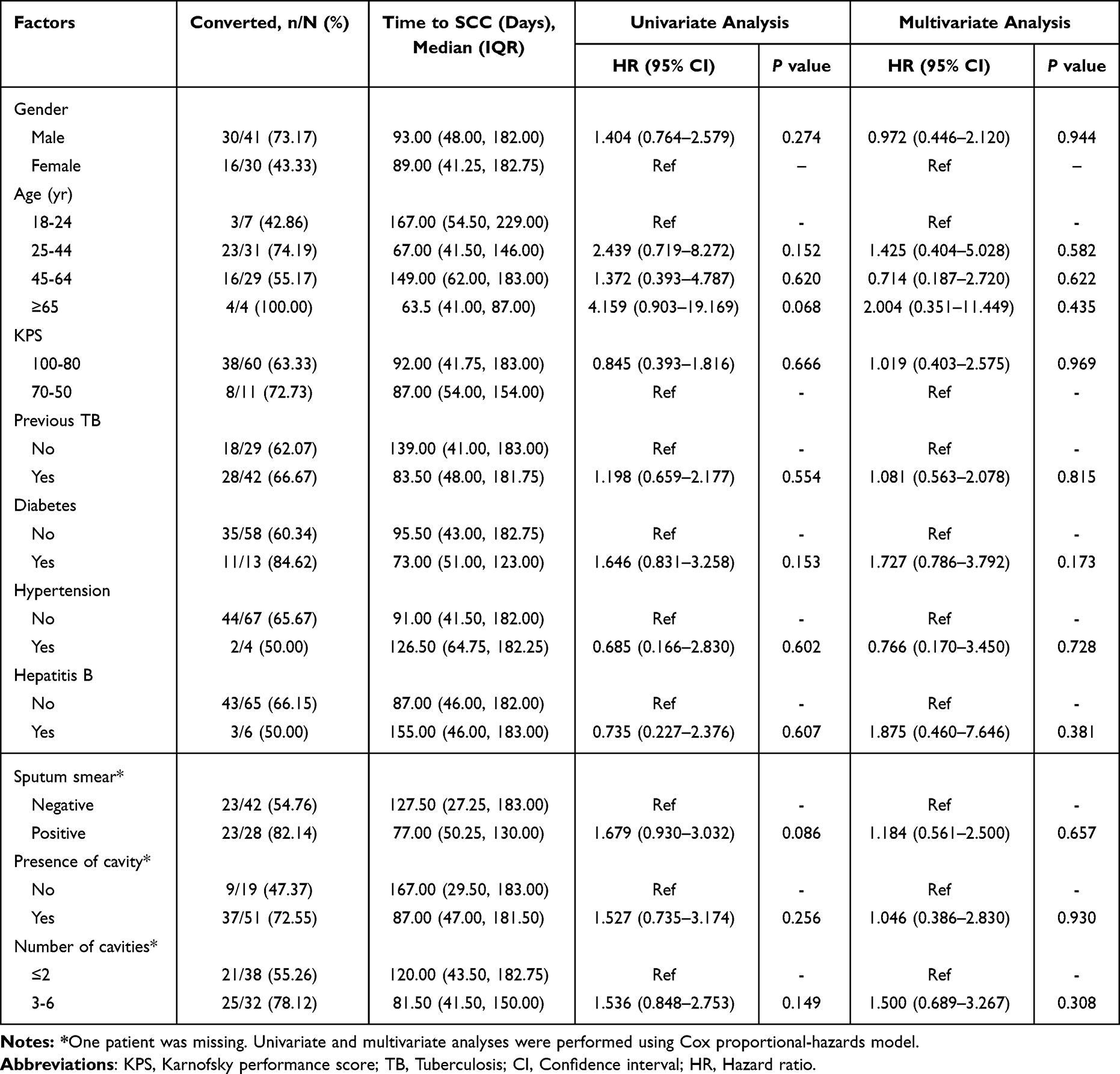 |
Table 7 Factors Associated with Time to Sputum Culture Conversion |
Discussion
This study systematically evaluated the therapeutic efficacy and safety of treatment regimens based on Dlm, Bdq, and Lzd in patients with MDR/RR-TB. The results showed that after treatment with Dlm, Bdq and Lzd, 73.24% of the patients achieved the good outcome defined by WHO, and 85.19% of the patients achieved negative sputum culture at the end of the treatment. What’s more, the patient’s TB-related clinical symptoms, including cough, expectoration, hemoptysis, chest pain, dyspnea, fatigue, weight loss and fever all improved significantly. Imaging results indicated that after the treatment, both the absorption and cavity of the TB lesion improved, and the proportion of the lesion area/volume to the whole lung area of the patient was significantly reduced. In terms of safety, 36.62% of patients experienced AEs, the incidence of grade ≥3 AEs was 8.45%, and one patient developed SAE, which was grade 4 anemia caused by Lzd. 12.68% of the patients showed prolonged QTcF, and the QTcF of the patients after treatment was significantly longer than the baseline. Based on the above results, the regimens based on Dlm, Bdq and Lzd have shown good efficacy and high safety in patients with MDR/RR-TB.
These favorable clinical outcomes may be attributed to the complementary and multi-target mechanisms of the three core drugs. Bdq targets ATP synthase and disrupts energy metabolism, particularly in dormant bacilli, while Dlm inhibits mycolic acid synthesis and compromises cell wall integrity.23,24 Lzd, by interfering with protein synthesis, further enhances antibacterial activity.25 Together, these agents exert activity against Mycobacterium tuberculosis across different metabolic states, potentially enhancing bactericidal activity and contributing to the observed clinical improvements, including symptom relief and radiographic lesion absorption. Taken together, these findings highlight the Dlm-Bdq-Lzd regimen as a mechanistically complementary, multi-target strategy that is distinct from existing regimens.
According to the latest WHO report, the global treatment success rate for MDR/RR-TB is approximately 68%.1 In our study, 73.24% of the patients achieved the favorable outcomes defined by the WHO at the end of the treatment after receiving the Dlm-Bdq-Lzd-based regimen, suggesting a relatively high treatment success rate compared with previously reported data. Both the clinical symptoms and imaging results demonstrated good therapeutic effects.
Compared with conventional long-course MDR/RR-TB regimens requiring 18–24 months of treatment and associated with substantial toxicity, the regimen used in this study appears to offers the potential advantages of a shorter duration and improved tolerability. In addition, Previous studies have demonstrated that regimens containing Bdq or Lzd are associated with improved treatment outcomes in patients with MDR/RR-TB, and their combined use has shown synergistic effects in enhancing therapeutic success.26,27 The inclusion of Dlm in the present regimen may provide additional benefits through complementary mechanisms. However, cross-study comparisons should be interpreted with caution due to differences in study design and patient characteristics.
When compared to the current WHO-recommended 6-month BPaLM (Bdq, pretomanid, Lzd, moxifloxacin) regimen, this Dlm-based combination provides a critical alternative for patients who may not tolerate or have access to pretomanid in real-world clinical settings.28 Moreover, in the past, patients with MDR/RR-TB received the 18–24-month regimen based on anti-TB drugs were prone to adverse reactions such as hepatotoxicity and neuritis. Patients endured the pain of long-term medication and a high economic burden, which also greatly tested their compliance and affected the therapeutic effect. The treatment duration of this study is relatively short, and good therapeutic effects can be achieved within 6 to 9 months.
The study showed that half of the patients experienced adverse reactions such as decreased hemoglobin levels, and one patient developed grade 4 anemia related to Lzd. This result is consistent with previous studies.29 Hematotoxicity is one of the common adverse reactions of Lzd. Lzd inhibits TB by binding to mitochondrial ribosomes, disrupting the expression and biosynthesis of mitochondrial proteins encoded by the mitochondrial genome, and blocking the action of cytochrome C-oxidase and mitochondrial oxidative activity. Similarly, mitochondrial dysfunction can lead to bone marrow suppression, resulting in anemia, leukopenia and thrombocytopenia.30 In addition to blood toxicity, this study also found that nine patients experienced prolonged QTcF, but no serious adverse cardiovascular reactions caused by prolonged QTcF occurred. A previous retrospective clinical study demonstrated that during the treatment of MDR/RR-TB, when Dlm was combined with Bdq, QTcF prolongation also occurred, but it was only cumulative and did not cause grade 3 or 4 QT interval prolongation.31 In addition, some patients in this study received combined treatment with moxifloxacin, levofloxacin, and clofazimine, which might have led to QTcF prolongation.
A previous history of TB and hepatitis B was associated with a lower likelihood of achieving treatment success. Some studies have shown that some MDR-TB patients have a history of TB,32,33 and those with a history of TB have an increased risk of developing MDR-TB.34 Another study illustrated that previously treated TB patients were 8.1 times more likely to develop MDR-TB infection compared to newly diagnosed TB patients.35 The cause of this phenomenon is that previously treated TB patients are usually exposed to a drug that inhibits the growth of drug-sensitive bacilli but promotes the proliferation of other drug-resistant mutant TB bacilli.36 Although the correlation between HBV history and drug-resistant TB is still unknown at present, existing studies have shown that drug-induced liver injury (DILI) is an adverse outcome of the current TB treatment regimens, leading to non-compliance, poor treatment effects, and the emergence of drug-resistant TB.37 Therefore, liver injury caused by HBV may lead to poor treatment and adverse outcomes, Hence, the treatment outcomes of Dlm, Bdq and Lzd for MDR/RR-TB patients can be affected by the history of TB and hepatitis B. Caution is required when formulating treatment plans for such patients.
This study evaluated the efficacy and high safety of treatment regimens based on Dlm, Bdq and Lzd in patients with MDR/RR-TB in China for the first time. This study provides a novel therapeutic idea for the clinical treatment of MDR/RR-TB and lays the foundation for the clinical promotion and application of Dlm, Bdq and Lzd. However, limitations still exist. First, the relatively small sample size and single-center design may introduce potential bias and thereby limit the generalizability of the findings. Second, this study adopts retrospective design, so there may be bias. Moreover, both the analysis of factors associated with outcomes and the evaluation of adverse events were limited by the relatively small sample size. In addition, the follow-up duration was insufficient for long-term assessment of patient outcomes. Therefore, the results of this study should be validated in large-scale prospective multicenter studies, extended follow-up is required to evaluate long-term treatment efficacy and safety.
Conclusions
This study suggests that the regimens based on Dlm, Bdq and Lzd demonstrate promising efficacy and an acceptable safety profile in patients with MDR/RR-TB. This treatment regimen has high clinical value and provides a new option for the clinical treatment of TB. However, given the retrospective design and limited sample size, these findings should be interpreted with caution. Further studies are warranted to identify the subpopulation of patients with TB who may benefit most from this regimen, in order to optimize treatment efficacy while minimizing potential risks.
Abbreviations
TB, Tuberculosis; MDR-TB, Multidrug-resistant tuberculosis; RR-TB, Rifampicin-resistant tuberculosis; Dlm, Delamani; Bdq, Bedaquiline; Lzd, Linezolid; AE, Adverse event; SAE, Serious adverse event; QTcF, Corrected QT Interval using Fridericia’s formula.
Data Sharing Statement
The data sets generated during and/or analysed during the current study are available from the corresponding authors on reasonable request.
Ethics Approval and Consent to Participate
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of the Infectious Disease Hospital of Heilongjiang Province (Approval No. 2025019). Written informed consent was obtained from all participants prior to participation in the study.
Funding
This study was supported by Research Project of the Heilongjiang Provincial Health Commission (2020-165).
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. World Health Organization. Global tuberculosis report 2024. World Health Organization; 2024.
2. Jacobs WR. A world without tuberculosis: moving from imagination to reality. J Clin Invest. 2022;132(18). doi:10.1172/JCI162688
3. Wulandari DA, Hartati YW, Ibrahim AU, Pitaloka DAE, Irkham. Multidrug-resistant tuberculosis. Clin Chim Acta. 2024;559:119701. doi:10.1016/j.cca.2024.119701
4. World Health Organization. Global tuberculosis report 2022. World Health Organization; 2022.
5. Hu S, Guo J, Chen Z, Gong F, Yu Q. Nutritional indices predict all cause mortality in patients with multi-/rifampicin-drug resistant tuberculosis. Infect Drug Resist. 2024;17:3253–15. doi:10.2147/IDR.S457146
6. Lu J, Xu Y, Li Z, Chen X, Lin H, Zhao Q. Diagnosis and treatment pathway of MDR/RR-TB in Taizhou, Zhejiang Province, China. Trop Med Infect Dis. 2023;8(2). doi:10.3390/tropicalmed8020079
7. Esmail A, Sabur NF, Okpechi I, Dheda K. Management of drug-resistant tuberculosis in special sub-populations including those with HIV co-infection, pregnancy, diabetes, organ-specific dysfunction, and in the critically ill. J Thorac Dis. 2018;10(5):3102–3118. doi:10.21037/jtd.2018.05.11
8. Singla R, Sarin R, Khalid UK, et al. Seven-year DOTS-Plus pilot experience in India: results, constraints and issues. Int J Tuberc Lung Dis. 2009;13(8):976–981.
9. Seung KJ, Keshavjee S, Rich ML. Multidrug-resistant tuberculosis and extensively drug-resistant tuberculosis. Cold Spring Harb Perspect Med. 2015;5(9):a017863. doi:10.1101/cshperspect.a017863
10. Guo Y, Yang J, Wang W, et al. Bedaquiline, delamanid, linezolid, clofazimine, and capreomycin MIC distributions for drug resistance mycobacterium tuberculosis in Shanghai, China. Infect Drug Resist. 2023;16:7587–7595. doi:10.2147/IDR.S440711
11. Matsumoto M, Hashizume H, Tomishige T, et al. OPC-67683, a nitro-dihydro-imidazooxazole derivative with promising action against tuberculosis in vitro and in mice. PLoS Med. 2006;3(11):e466.
12. He W, Liu C, Liu D, et al. Prevalence of Mycobacterium tuberculosis resistant to bedaquiline and delamanid in China. J Glob Antimicrob Resist. 2021;26:241–248. doi:10.1016/j.jgar.2021.06.007
13. Gler MT, Skripconoka V, Sanchez-Garavito E, et al. Delamanid for multidrug-resistant pulmonary tuberculosis. N Engl J Med. 2012;366(23):2151–2160. doi:10.1056/NEJMoa1112433
14. Garcia-Prats AJ, Frias M, van der Laan L, et al. Delamanid added to an optimized background regimen in children with multidrug-resistant tuberculosis: results of a phase I/II clinical trial. Antimicrob Agents Chemother. 2022;66(5):e0214421. doi:10.1128/aac.02144-21
15. Ofori-Anyinam B, Hamblin M, Coldren ML, et al. Catalase activity deficiency sensitizes multidrug-resistant Mycobacterium tuberculosis to the ATP synthase inhibitor bedaquiline. Nat Commun. 2024;15(1):9792. doi:10.1038/s41467-024-53933-8
16. Yao G, Zhu M, Nie Q, et al. Improved outcomes following addition of bedaquiline and clofazimine to a treatment regimen for multidrug-resistant tuberculosis. J Int Med Res. 2023;51(1):3000605221148416. doi:10.1177/03000605221148416
17. Kadura S, King N, Nakhoul M, et al. Systematic review of mutations associated with resistance to the new and repurposed Mycobacterium tuberculosis drugs bedaquiline, clofazimine, linezolid, delamanid and pretomanid. J Antimicrob Chemother. 2020;75(8):2031–2043. doi:10.1093/jac/dkaa136
18. Agyeman AA, Ofori-Asenso R. Efficacy and safety profile of linezolid in the treatment of multidrug-resistant (MDR) and extensively drug-resistant (XDR) tuberculosis: a systematic review and meta-analysis. Ann Clin Microbiol Antimicrob. 2016;15(1):41. doi:10.1186/s12941-016-0156-y
19. Zou Y, de Jager V, Hesseling AC, et al. Relative bioavailability of delamanid 50 mg tablets dispersed in water in healthy adult volunteers. Br J Clin Pharmacol. 2025;91(4):957–967. doi:10.1111/bcp.15672
20. Hasan T, Medcalf E, Nyang’wa B-T, et al. The safety and tolerability of linezolid in novel short-course regimens containing bedaquiline, pretomanid, and linezolid to treat rifampicin-resistant tuberculosis: an individual patient data meta-analysis. Clin Infect Dis. 2024;78(3):730–741. doi:10.1093/cid/ciad653
21. Li R, Ma J-B, Yang H, et al. Effects of bedaquiline combined with fluoroquinolone and/or clofazimine on QT interval in patients with multidrug-resistant tuberculosis: a Retrospective Study. Microbiol Spectr. 2023;11(4):e0104823. doi:10.1128/spectrum.01048-23
22. Linh NN, Viney K, Gegia M, et al. World Health Organization treatment outcome definitions for tuberculosis: 2021 update. Eur Respir J. 2021;58(2). doi:10.1183/13993003.00804-2021
23. Islam MM, Alam MS, Liu Z, et al. Molecular mechanisms of resistance and treatment efficacy of clofazimine and bedaquiline against mycobacterium tuberculosis. Front Med. 2024;10:1304857. doi:10.3389/fmed.2023.1304857
24. Khoshnood S, Taki E, Sadeghifard N, et al. Mechanism of action, resistance, synergism, and clinical implications of delamanid against multidrug-resistant mycobacterium tuberculosis. Front Microbiol. 2021;12:717045. doi:10.3389/fmicb.2021.717045
25. Hashemian SMR, Farhadi T, Ganjparvar M. Linezolid: a review of its properties, function, and use in critical care. Drug Des Devel Ther. 2018;12:1759–1767. doi:10.2147/DDDT.S164515
26. Zhang S-J, Yang Y, Sun -W-W, et al. Effectiveness and safety of bedaquiline-containing regimens for treatment on patients with refractory RR/MDR/XDR-tuberculosis: a retrospective cohort study in East China. BMC Infect Dis. 2022;22(1):715. doi:10.1186/s12879-022-07693-9
27. Cheraghi M, Amiri M, Andarzgoo S, et al. Bedaquiline and linezolid regimens for multidrug-resistant tuberculosis: a systematic review and meta-analysis. J Bras Pneumol. 2025;51(1):e20240391. doi:10.36416/1806-3756/e20240391
28. Otto-Knapp R, Edwards S, Kuchukhidze G, et al. Availability of drugs for the treatment of multidrug-resistant/rifampicin-resistant tuberculosis in the World Health Organization European Region, October 2023. Euro Surveill. 2024;29(17). doi:10.2807/1560-7917.ES.2024.29.17.2400211
29. Imperial MZ, Nedelman JR, Conradie F, Savic RM. Proposed linezolid dosing strategies to minimize adverse events for treatment of extensively drug-resistant tuberculosis. Clin Infect Dis. 2022;74(10):1736–1747. doi:10.1093/cid/ciab699
30. Oehadian A, Santoso P, Menzies D, Ruslami R. Concise clinical review of hematologic toxicity of linezolid in multidrug-resistant and extensively drug-resistant tuberculosis: role of mitochondria. Tuberc Respir Dis. 2022;85(2):111–121. doi:10.4046/trd.2021.0122
31. Nyang’wa B-T, Berry C, Kazounis E, et al. Short oral regimens for pulmonary rifampicin-resistant tuberculosis (TB-PRACTECAL): an open-label, randomised, controlled, phase 2B-3, multi-arm, multicentre, non-inferiority trial. Lancet Respir Med. 2024;12(2):117–128. doi:10.1016/S2213-2600(23)00389-2
32. Dean AS, Cox H, Zignol M. Epidemiology of Drug-Resistant Tuberculosis. In: Gagneux S, editor. Strain Variation in the Mycobacterium Tuberculosis Complex: Its Role in Biology, Epidemiology and Control. Springer International Publishing; 2017:209–220.
33. Ali MH, Alrasheedy AA, Hassali MA, Kibuule D, Godman B. Predictors of Multidrug-Resistant Tuberculosis (MDR-TB) in Sudan. Antibiotics. 2019;8(3). doi:10.3390/antibiotics8030090
34. Ketema DB, Muchie KF, Andargie AA. Time to poor treatment outcome and its predictors among drug-resistant tuberculosis patients on second-line anti-tuberculosis treatment in Amhara region, Ethiopia: retrospective cohort study. BMC Public Health. 2019;19(1):1481. doi:10.1186/s12889-019-7838-2
35. Eshetie S, Gizachew M, Dagnew M, et al. Multidrug resistant tuberculosis in Ethiopian settings and its association with previous history of anti-tuberculosis treatment: a systematic review and meta-analysis. BMC Infect Dis. 2017;17(1):219. doi:10.1186/s12879-017-2323-y
36. Colijn C, Cohen T, Ganesh A, Murray M. Spontaneous emergence of multiple drug resistance in tuberculosis before and during therapy. PLoS One. 2011;6(3):e18327. doi:10.1371/journal.pone.0018327
37. Bakshi S, Kaur M, Verma A, Sharma S. Molecular and cellular remodeling of HepG2 cells upon treatment with antitubercular drugs. J Biochem Mol Toxicol. 2023;37(8):e23386. doi:10.1002/jbt.23386
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
In vitro and Intracellular Antibacterial Activity of Sudapyridine (WX-081) Against Tuberculosis
Xiao H, Yu X, Shang Y, Ren R, Xue Y, Dong L, Zhao L, Jiang G, Huang H
Infection and Drug Resistance 2023, 16:217-224
Published Date: 10 January 2023
Clinical Utility of Contezolid-Containing Regimens in 25 Cases of Linezolid-Intolerable Tuberculosis Patients
Wang J, Nie W, Ma L, Li Q, Geng R, Shi W, Chu N
Infection and Drug Resistance 2023, 16:6237-6245
Published Date: 19 September 2023
Contezolid Harbored Equivalent Efficacy to Linezolid in Tuberculosis Treatment in a Prospective and Randomized Early Bactericidal Activity Study
Jiang G, Liu R, Xue Y, Ge Q, Nie L, Lv Z, Kong Z, Shi J, Chen H, Li H, Wu X, Xie L, Song Y, Huang H, Gao M
Infection and Drug Resistance 2025, 18:261-268
Published Date: 13 January 2025
Interim Effectiveness and Safety of Prolonged Bedaquiline Use in Comparison to Standard 24-Week Treatment for MDR-TB: A Multicenter Cohort Study in China
Hu X, Gao M, Liu Y, Pei Y, Du J, Wu G, Wang A, Li L, Gao J
Infection and Drug Resistance 2026, 19:572423
Published Date: 10 March 2026