Back to Journals » Vascular Health and Risk Management » Volume 21
Intensified Multifaceted Education Improves the Implementation of Standard Atrial Fibrillation Care in Elderly Patients with Atrial Fibrillation in Rural China
Authors Zhang S, Chu M, Lu D, Shen Y, Sun X ![]() , Xia Y, Yang S, Gong J, Hong L, Li M
, Xia Y, Yang S, Gong J, Hong L, Li M ![]() , Lip GYH, Chen M
, Lip GYH, Chen M
Received 19 April 2025
Accepted for publication 27 July 2025
Published 13 August 2025 Volume 2025:21 Pages 633—644
DOI https://doi.org/10.2147/VHRM.S535313
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Daniel Duprez
Shimeng Zhang,1,* Ming Chu,1,2,* Dechuan Lu,3,* Youmei Shen,1 Xingxing Sun,1 Yaodongqin Xia,1 Shu Yang,1 Jinlong Gong,3 Li Hong,3 Mingfang Li,1 Gregory YH Lip,4,5 Minglong Chen1,2
1Department of Cardiology, The First Affiliated Hospital with Nanjing Medical University, Nanjing, People’s Republic of China; 2Department of Cardiology, The Affiliated Taizhou People’s Hospital of Nanjing Medical University, Taizhou, People’s Republic of China; 3Department of Cardiology, Jiangdu People’s Hospital Affiliated to Yangzhou University, Yangzhou, People’s Republic of China; 4Liverpool Centre for Cardiovascular Science at University of Liverpool, Liverpool John Moores University and Liverpool Heart & Chest Hospital, Liverpool, UK; 5Department of Clinical Medicine, Aalborg University, Aalborg, Denmark
*These authors contributed equally to this work
Correspondence: Gregory YH Lip, Liverpool Centre for Cardiovascular Science, University of Liverpool, Liverpool John Moores University and Liverpool Heart & Chest Hospital, Liverpool, UK, Tel +44-0151-794 9020, Email [email protected] Minglong Chen, Department of Cardiology, The First Affiliated Hospital with Nanjing Medical University, 300 Guangzhou Road, Nanjing, 210029, People’s Republic of China, Tel +86-25-68303115, Fax +86-25-6813-6479, Email [email protected]
Background: Exploring an integrated care management model to effectively deliver the standardized management to atrial fibrillation (AF) elderlies in rural China.
Purpose: The objective of this study was to assess whether intensified multifaceted education (IME) targeting AF elderlies, their family members, and the village doctors (VD) can increase compliance for rural AF elderlies with integrated care based on the AF Better Care (ABC) pathway. Additionally, the capacity of VD to deliver integrated AF care was investigated.
Patients and Methods: This is a self-controlled cohort study before and after IME, including AF patients aged ≥ 65 years identified in phase-I of The Jiangsu Province Rural Community AF Project. The IME model was defined as 12 months of continuous knowledge education on integrated care management of AF based on the ABC pathway, delivered to AF patients, their family members and the village doctors. AF knowledge evaluation from VD and compliance with the ABC pathway before and after the IME model were evaluated.
Results: A total of 810 AF patients (mean age 76.1 ± 5.9 years; 51.4% women) were enrolled. After 12 months, the AF knowledge score of VD was significantly improved [(65.0 ± 13.0) scores vs (53.1 ± 9.8) scores, P < 0.001]. Although the compliance of AF patients with the ABC pathway was improved statistically (4.3% vs 1.7%, P = 0.003), the absolute increase was small.
Conclusion: Although VD have the potential to serve as AF integrated care management providers, the impact of the IME model used to improve the standard AF care in rural elderly AF population was small.
Keywords: education, atrial fibrillation, village doctors, rural, elderly
Introduction
Atrial fibrillation (AF) confers a significant public health burden due to its heightened association with mortality and morbidity from stroke, heart failure and dementia.1 The burden of AF is increasingly heavier in developing countries.2–5 China is no exception, with an increasingly higher AF incidence, multimorbidity, low disease awareness and poor adherence to management guidelines.6 Contemporary management of AF has moved towards an integrated care approach based on the Atrial fibrillation Better Care (ABC) pathway,7 avoid stroke, better symptom management and cardiovascular risk reduction, whereby adherence to the latter is associated with improved clinical outcomes,8,9 leading to its recommendation in guidelines.10–13
Rural and elderly patients were still vulnerable in chronic diseases prevention and control. By developing tailored programmes targeting specific populations to reduce inequalities in primary health care (PHC) is an important study project in rural areas. This is not only the theme for China, but a task for global health.14 Furthermore, the quality of PHC for chronic diseases in rural areas has large gaps in care continuity, provider competence, family-centeredness, and shared decision-making.15 Obviously, education is the most cost-effective intervention to enhance healthcare equity and improve chronic disease care quality.
As an integral component of AF integrated care, education is essential for mitigating AF-related adverse outcomes.8 Irrespective of the form of education or the nodes of education, AF patient education has been associated with a reduction in adverse events, improved mental well-being and quality of life.16 Nevertheless, the impact of education on the management of chronic diseases has not been as pronounced among individuals with lower educational attainment and limited economic resources.17
In our first phase of the Jiangsu Province Rural Community Atrial Fibrillation Project, elderly patients with AF in rural China was described as low educational attainment, limited health awareness, insufficient disease knowledge, and minimal access to home-based care.18 The solely medical resources they can rely on are village doctors, who have a low education level and unstandardized medical training and have been working on the frontline of primary care and public health service in rural China for decades.4 Hence, whether village doctors have the competence in chronic diseases management such as AF remains a matter of great concern. In this specific setting, we conducted intensified multifaceted education (IME) centered on the ABC pathway for rural elderly AF individuals, their family members and the village doctors and to encourage village doctors to embrace such integrated care for managing rural elderly AF patients. We aimed to assess whether IME can enhance compliance with the ABC pathway and whether village doctors possess the capacity to serve as potential implementers of standardized AF integrated care.
Methods
Study Design and Population
The protocol for the Jiangsu Province Rural Community Atrial Fibrillation Project has previously been published.19 Participants identified with AF in the first phase (a cross-sectional study of AF screening) and all the village doctors in the two rural towns in eastern China were eligible for the present second phase (a self-controlled cohort study before and after intervention). The second phase study was conducted from May 2019 to July 2020. The exclusion criteria were not willing to participate in the IME for village doctors, and there was no exclusion criteria for AF patients and their family members.
IME was defined as the provision of continuous knowledge on the integrated care education of AF based on the ABC pathway to AF patients, their family members and the village doctors. Compliance with the ABC pathway was evaluated at baseline according to its original definition (Supplementary Table 1). Patients were categorized as “ABC pathway compliant” when compliant with all the three criteria.
The Institutional Review Board of Jiangdu People’s Hospital Affiliated to Yangzhou University granted approval for the prospective registry study (YJRY-K-2019-01), and all participants involved in the study signed consent forms to participate.
Intensified Education Targeting AF Patients and Their Family Members
The primary objective of the intensified education was to raise awareness about AF and provide knowledge regarding AF prevention and treatment for the AF patients and their family members. The key components of this intensified education included explanations of what AF is, the primary complications associated with AF, risk factors contributing to AF incidence, the relationship between AF and stroke, the significance of taking oral anticoagulants (OACs), and potential bleeding complications related to OACs usage. This intensified education employed various methods, including educational videos in the local dialect, a monograph containing AF-related information, brochures about AF, and popular science articles shared on our WeChat official accounts. WeChat is a social media and instant messaging platform primarily used by the adult children of rural elderly individuals.
In addition, face-to-face patient teaching was provided by AF specialists at 1 and 7 months and by village doctors at 2, 5, 8 and 11 months. To promote interaction with village doctors, patients and their family members were encouraged to participate in monthly group discussion held in village clinics. Face-to-face patient teaching attendance and the monthly visits of group discussion, as well as AF-related medical visits of AF patients were recorded. Feedback was gathered by identifying AF patients who had never used oral anticoagulants (OACs) or stopped using them, along with their reasons for withholding.
Tailored Training for Village Doctors in AF Integrated Care
The primary aim of tailored training from AF specialists was to enhance the village doctors’ understanding of AF integrated care, aligned with the guideline-recommended ABC pathway. The program included a series of lectures conducted by AF specialists (onsite at 1 and 7 months and online at 3 months), furthermore, AF specialists provided personalized education to address specific knowledge gaps identified in each village doctor, based on their prior knowledge assessments. All online training materials were also accessible through a specially developed online education platform (https://cunyinet.cn/#/education/continue).
Knowledge assessment involved the administration of a survey comprising 10 questions related to specific AF knowledge at both baseline and 12 months of the tailored training. In addition, door-to-door interviews for AF patients by village doctors were encouraged and recorded. Moreover, the difference in knowledge levels between village doctors who participated in our registry and those who did not was also examined.
Evaluation and Study Outcomes
Patients underwent baseline evaluations, as described in the first phase of this project.18 Final assessments were conducted at 12 months.
Compliance with ABC pathway of AF patients and AF knowledge level from village doctors were assessed. Causes of death were determined based on death certificates provided by the Health Commission of Jiangdu District.
Statistical Analysis
Continuous variables distributed normally were presented as means with standard deviation. Continuous variables distributed non-normally were presented as median (IQR) and compared using Mann–Whitney U-test or Wilcoxon test. Categorical variables were expressed as frequency (percentage) and analyzed using Fisher’s exact test or Pearson’s chi-square test. Our analysis focused on comparing ABC pathway compliance and the ABC pathway components between AF patients at baseline and 12 months. A P-value <0.05 was considered statistically significant. SPSS software version 29.0 (IBM Corporation, New York, America) was used for all the statistical analyses.
Results
Among the 18,712 residents enrolled in the first phase of the registry study, 810 (4.3%, 810/18,712) participants [mean age 76.1 (5.9) years; 51.4% women] were found to have AF. Nearly half of these AF patients (49.6%, 402/810) were aware of their AF condition based on their previous medical history. Baseline characteristics of residents without AF and those with AF were previously described.20
Over the 12-month IME, 41 (5.1%, 41/810) AF patients died of various causes, and patients who died were more likely to be older and newly detected AF (Supplementary Table 2). AF patients who died were non-compliant with the ABC pathway at baseline.
Compliance with the ABC Pathway Components
The 769 AF patients [age 76.1 (5.9) years, 50.6% women; known AF history in 51.5%] who survived at 12 months were included in the comparison of compliance with the ABC pathway before and after the IME. At 12 months, full ABC pathway compliance increased to 4.3% (33/769) as compared with baseline 1.7% (14/810), which was statistically significant (P = 0.003). No significant net increment difference in compliance with the ABC pathway was observed between patients with known AF history and newly detected AF (2.6% vs 2.4%, P = 0.766). After the 12-month of IME program, compliance with the ABC pathway in the survival patients with known AF history was numerically greater but not statistically different (6.1% vs 3.5%, P = 0.096). Specific compliance with each component of the ABC pathway is detailed in Figure 1.
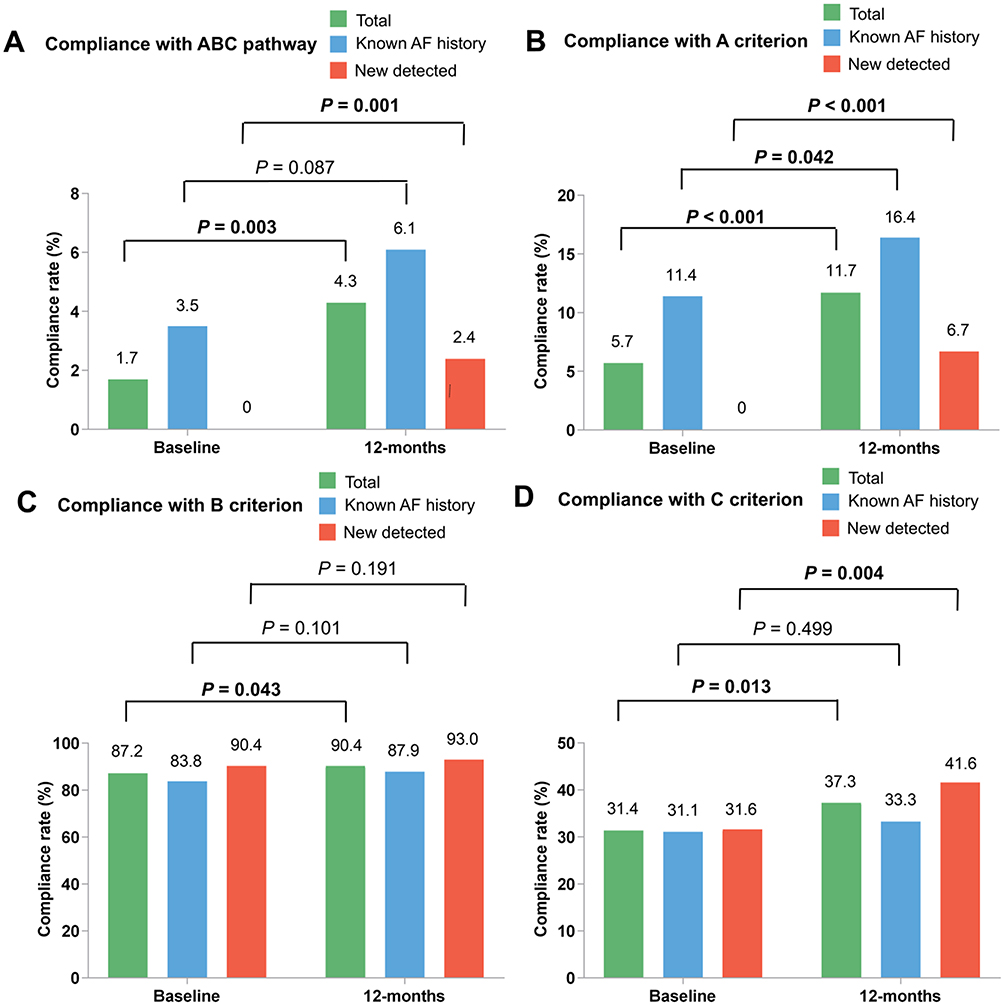 |
Figure 1 Compliance with ABC pathway in atrial fibrillation before and after intensified multifaceted education. (A) Compliance with ABC pathway; (B) Compliance with A criterion; (C) Compliance with B criterion; (D) Compliance with C criterion. A criterion, avoid stroke; B criterion, better symptoms control; C criterion, cardiovascular risk and comorbidity optimization. Abbreviations: ABC, atrial fibrillation better care; AF, atrial fibrillation. |
Patient, Relative and Village Doctor Interactions
During the IME process, the participation rates for patients at the 2 health education activities by AF specialists were 84.8% and 73.1%, respectively; but was only 37.2% (IQR: 25.5–53.1%) for the 4 health education activities by village doctors (Supplementary Figure 1A and B).
A median of 9.4% (IQR: 3.6–14.3%) patients or their family members visited the village doctor’s clinic monthly to engage in the educational sessions and interactions with the village doctors (Supplementary Figure 1C), while during the 12-month IME program, 15.2% (123/810) of patients sought medical attention at various levels due to AF related events. Within this period, 78.9% (97/123) of these patients presented with worsening of AF-related symptoms and 84.6% (104/123) directly visited secondary or tertiary hospitals.
Of the 744 patients at high risk for stroke at baseline, 95.2% (708/744) survived at 12 months, and only 11.7% (83/708) were using OACs, with the majority opting for warfarin (89.2%, 74/83) (Figure 2). An additional 33 patients (4.7%, 33/708) had previously OACs use, but discontinued. The remaining 592 patients (83.6%, 592/708) had never used OACs.
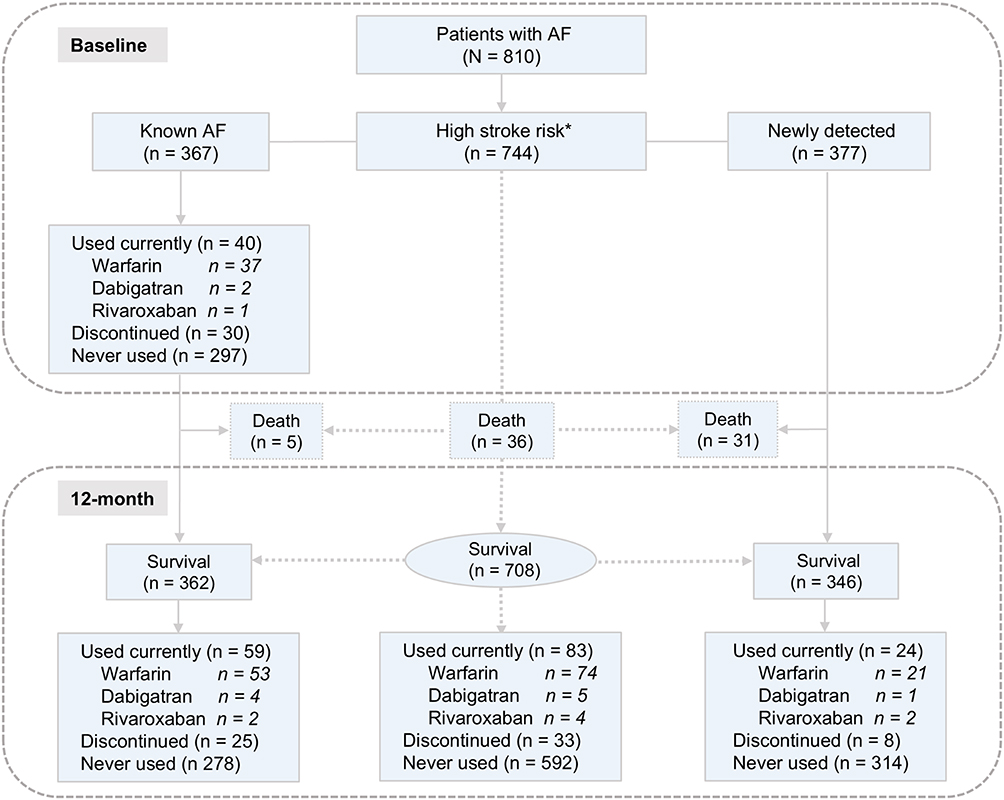 |
Figure 2 The flow chart of anticoagulation in patients with atrial fibrillation. *High stroke risk AF was defined AF of CHA2DS2-VASc ≥ 2 (men) or 3 (women). Abbreviation: AF, atrial fibrillation. |
No significant difference in the proportions of never users was observed between the baseline and the 12-month (80.9% vs 83.6%, P = 0.269). Similar results were observed in AF patients with known AF at high risk of stroke (P = 0.104).
Among AF patients who had never used OACs, the majority (97.2%, 622/640) refused to use OACs. The main reasons were as follows: 81.5% (507/622) patients believed that OACs were unnecessary, and 13.7% (85/622) were concerned about potential side effects (Figure 3A). Among 39 AF patients who had previously used OACs, main reasons of discontinued: 17.9% (7/39) felt that the treatment was ineffective, 17.9% (7/39) were not willing to undergo frequent blood tests, 17.9% (7/39) reported improved symptoms, and 15.4% (6/39) had concerns about side effects (Figure 3B).
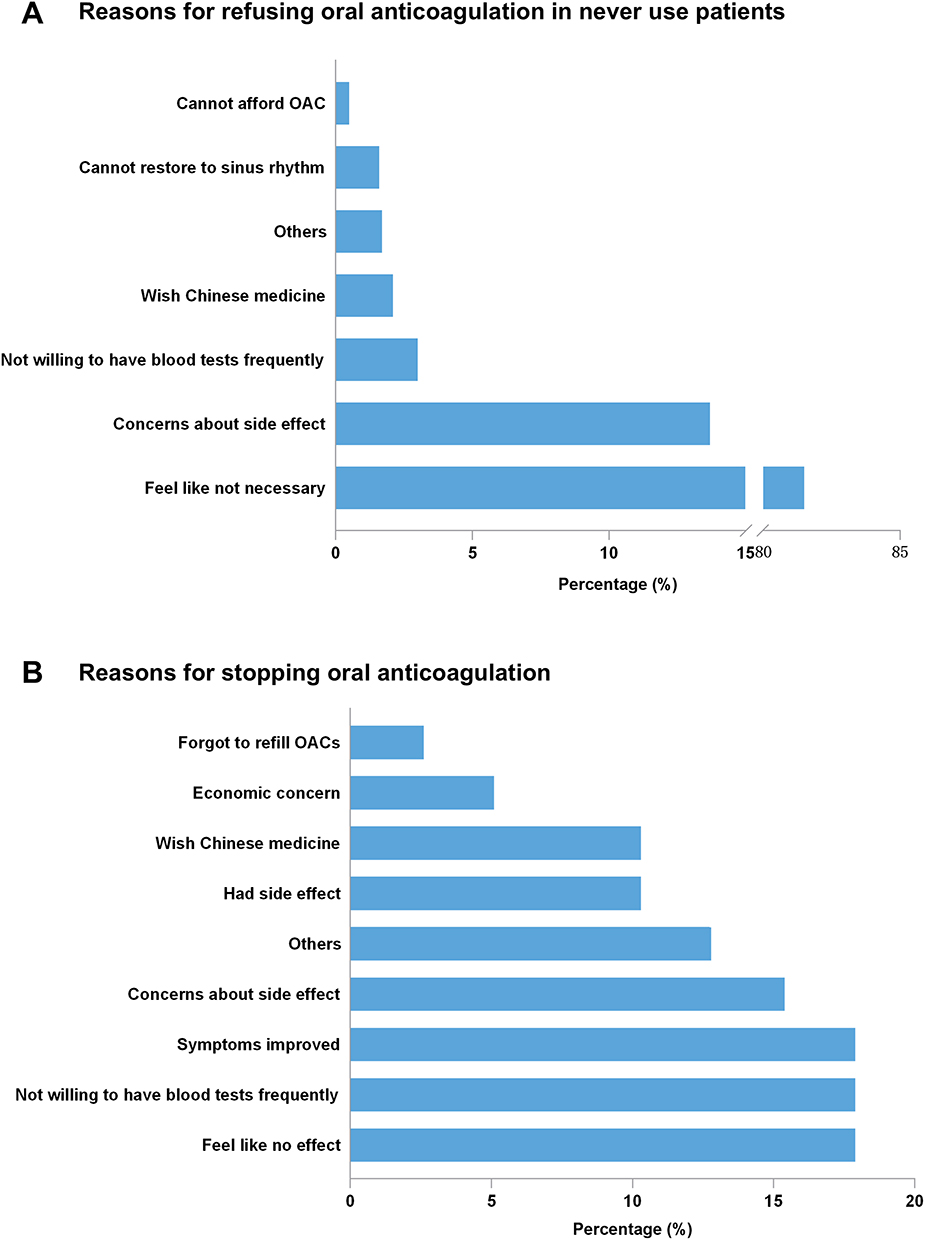 |
Figure 3 Reasons for withholding oral anticoagulation therapy in atrial fibrillation patients. (A) Reasons for refusing oral anticoagulation in never use patients; (B) Reasons for stopping oral anticoagulation. Abbreviation: OACs, oral anticoagulants. |
Feedback from Village Doctors
A dedicated training program on AF was provided to all the 125 village doctors in these two towns. The participation rates of village doctors in onsite training and online training were all 100%.
Of the group, 95.2% (119/125) village doctors completed our survey at 12 months. AF knowledge level of village doctors exhibited a significant improvement after the 12-month training program [baseline 50 (IQR: 50–60) scores vs 12-month 70 (IQR 60–70) scores, P < 0.001] (Figure 4).
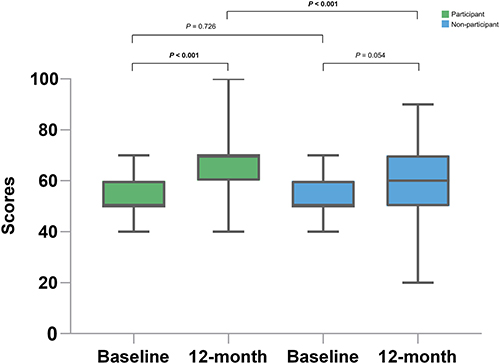 |
Figure 4 Atrial fibrillation knowledge level of village doctors before and after intensified multifaceted education. |
Additionally, 97 village doctors from other towns in Jiangdu District also participated in the same survey. At 12 months, compared to village doctors not participate in the tailored training, AF knowledge levels of participating village doctors increased significantly [10.0 (IQR: 0.0–20.0) scores vs 0.0 (IQR: −10.0–10.0) scores, P < 0.001].
Discussion
This is the first study focused on rural elderly AF patients as education recipients and village doctors as both recipients and implementers. This new IME model was designed for AF patients, their family members and the village doctors, which aimed to increase compliance with the ABC pathway for rural elderly AF patients. Our results showed a statistically significant improvement in AF knowledge amongst village doctors as well as the compliance with the ABC pathway of AF patients at 12 months, but the absolute increase was minimal.
Compliance with the ABC pathway among AF patients can substantially diminish the risks of all-cause mortality, cardiovascular mortality, rehospitalization, stroke, and major bleeding.8,9,21–23 Such a holistic approach is important given the clinical complexity in AF patients, with high prevalence of multimorbidity, polypharmacy and frailty.24–26 Hence, given the improvement in clinical outcomes with ABC pathway adherence, even in complex patients,27–29 this approach has been recommended in recent guidelines.10–13 The latest ESC guideline for AF management has established the “CARE” pathway to further optimize the integrated management of patients with AF, emphasizing a patient-centered approach involving comorbidity and risk factor management, avoiding stroke and thromboembolism, reducing symptoms by rate and rhythm control, and evaluation and dynamic reassessment. As an upgraded version of the ABC pathway, besides affirming the importance a multi-disciplinary management approach covering primary care, cardiology, pharmacy, nursing and home care, evaluation and dynamic reassessment was first emphasized. Regularly re-evaluation of medical history and the results of any tests could address the dynamic nature of comorbidities and risk factors, as a result, dynamic care and treatment adherence could be promoted. Regrettably, our study only focused on the compliance with the ABC pathway before and after the completion of the 12-month IME.30
Despite the association between ABC pathway compliance and improved clinical outcomes have been affirmed, the present study is the first study to assess whether IME model can improve ABC pathway compliance in rural areas. Numerous studies have consistently demonstrated the benefits of education in terms of enhancing treatment adherence, mitigating severe adverse events, and fostering improved mental health and quality of life among AF patients.16 The IMPACT-AF study showed a significant increase in use of OACs at one year in AF patients at high risk of stroke through a multifaceted and multilevel educational program.31 The mAFA-II trial showed improved OACs compliance and clinical outcomes in the intervention arm.32 A targeted nurse-led educational program led to a 50% reduction in the composite endpoint of death, cardiovascular hospitalization, and AF-related emergency department visits.33
Our study reveals that, although the improvement of the ABC pathway compliance was statistical significantly improved following 12-month IME, this was substantially lower compared to prior AF studies (ranging from 7.0% to 63.0%).34,35 Although clinical outcomes were not assessed, the poor ABC pathway compliance is of great concern. This obviously is determined by the education level of the recipients. Unlike IMPACT-AF and mAFA-II, which were targeting on mid and high education recipients, the education level of rural elderly in our study is very low. Hence, the impact of this IME model in elderly AF patients residing in rural areas in China may be somewhat limited.
AF care in more experienced centers demonstrated greater reductions in the primary endpoints of major cardiovascular adverse events.36 Thus, adequate training and continuous skill development for healthcare professionals are imperative for delivering integrated care to AF patients. In rural China, village doctors take on the responsibility of overseeing the health and chronic disease management of rural residents,4 and whether village doctors have the competence in management of chronic diseases remains a matter of great concern. The CRHCP trial showed that village doctor-led multifaceted intervention resulted in statistically significant improvements in blood pressure control,37 and the primary outcome and secondary outcomes were reduced among rural residents in China.38
The ability of village doctors in improving AF care, which is perhaps more comprehensive given the clinical complexity associated with these patients, remains unknown. In the present study, after 12 months of integrated care education rooted in the ABC pathway, there was a significant improvement in the knowledge level of village doctors regarding AF management, suggesting that village doctors have the potential to serve as AF integrated care providers. However, this improvement was primarily confined to AF knowledge, and there was no substantial overall enhancement in the ABC pathway compliance. Hence, there may be challenges in effectively translating the elevated knowledge level of village doctors into improved AF management capabilities.
In our study, the interaction between AF patients and their family members and village doctors was limited. First, only a median of 9.4% AF patients or their family members visited the village doctor’s clinic monthly to participate in the group discussion. Most (78.9%) AF patients sought help only when symptoms exacerbated and the overwhelming majority (84.6%) of them sought assistance from higher-level hospitals instead of village doctors. These findings suggest that AF patients possess low health awareness and lack trust in village doctors. Second, none of the village doctors provided AF management-related home visits, resulting in insufficient motivation. The tenuous link between AF patients and village doctors made education implementation challenging in elderly patients in rural China. The distrust of village doctors among AF patients and the inability of village doctors to translate AF knowledge into AF management capability indicates that the capacity of village doctors to provide AF integrated care necessitates better support from higher-level hospitals or specialists.
A recent study proved that compared to patients in township hospitals with median management intensity, patients in high-intensity townships have 4.8% increment PHC visits, 5.2% decrement specialist visits, and 11.7% lower likelihood of having an inpatient admission. The main results are derived from better medication adherence and better control of blood pressure.39 In disease management practice in rural China, the exploration of innovative management and educational approaches is essential for enhancing the knowledge base of village doctors. This is more pounced when delivering integrating AF management skills into their overall care capabilities, thereby bridging the gap between AF patients and village doctors. While patient education is highly valued by healthcare professionals, providing optimal face-to-face patient education often faces challenges due to constraints such as limited time and insufficient staffing. Innovative educational programs including video-based resources, informational reminders, and interactive modules to supplement or even replace in-person patient counseling may be needed. The mAFA-II trial was delivered through a mobile phone app-emphasized self-monitoring and educational content delivered through videos, games, and other materials.29 The intervention clusters showed a 61% reduction in the primary composite outcome covering major cardiovascular events after 1 year.32,40
Although video or online education could improve increased patient-knowledge of AF,41 many online resources lack patient-specific materials, and some patients, particularly those with low e-health knowledge, may struggle to use smart devices or access the internet.42 Indeed, mobile or online education may be less applicable in elderly patients in rural China given the low smartphone ownership and application. Village doctors play a pivotal role as the primary healthcare providers in rural China, and our study has affirmed their capacity for education and potential in chronic disease management. Hence, there is a compelling need to proactively explore a standardized and integrated care model for AF led by village doctors to enhance management compliance and improve the prognosis of patients with AF in rural regions.43,44
Our study has certain limitations. First, within the group of patients with known AF, there was an insufficient number of patients who fully adhered to the ABC pathway. As a result, it was difficult to conduct a meaningful comparison of clinical endpoints between groups based on baseline ABC pathway adherence after 12 months. Additionally, exploring the factors influencing adherence to the ABC pathway was also hindered by the low number of adherent patients. Furthermore, while village doctors’ knowledge significantly improved, the direct impact on patient health outcomes, such as stroke prevention, anticoagulation adherence, and mortality reduction, remains unclear. Further studies should be designed to evaluate the impact of improving the professional competence of village doctors on the clinical outcomes of patients. Moreover, our current educational program consisted of a relatively short duration of only 12 months. The potential effects of a more extended period of education have not been further investigated within this population. Finally, the results observed in the present study are specific to socioeconomic and healthcare conditions in rural China, and it is necessary to replicate the study in diverse rural settings across different regions or countries to assess the generalizability of the findings and identify context-specific factors influencing the effectiveness of the intervention.
Conclusion
Although village doctors had the potential to serve as AF integrated care providers, the rural elderly AF population were poor responders to IME program. The absolute impact of the IME model used to improve the standard AF care in this specific setting was small. There is a pressing need to explore an integrated care model linking AF patients, frontline healthcare providers and the specialists to deliver standard integrated care to AF patients in rural China.
Abbreviations
AF, atrial fibrillation; IME, intensified multifaceted education; VD, village doctors; ABC, Atrial fibrillation Better Care; PHC, primary health care; OAC, oral anticoagulants.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study was approved by Institutional Review Board of Jiangdu People’s Hospital Affiliated to Yangzhou University (YJRY-K-2019-01). Informed consent was obtained from all individual participants included in the study. All participants provided informed consent to participate before enrollment.
Acknowledgments
We thank the participants, project staff, and Health Commission of Jiangdu District and its regional offices for access to death and disease registries. The Chinese National Health Insurance scheme provides electronic linkage to all hospital treatment.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grant BE2017750 from Key Clinical Study Project of Jiangsu Province. The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
Minglong Chen reported receiving lecture fee from Boehringer Ingelheim. All other authors declare no competing interests for this work.
References
1. Burdett P, Lip GYH. Atrial fibrillation in the UK: predicting costs of an emerging epidemic recognizing and forecasting the cost drivers of atrial fibrillation-related costs. Eur Heart J Qual Care Clin Outcomes. 2022;8(2):187–194. doi:10.1093/ehjqcco/qcaa093
2. Chen X, Giles J, Yao Y, et al. The path to healthy ageing in China: a Peking University-Lancet Commission. Lancet. 2022;400(10367):1967–2006. doi:10.1016/S0140-6736(22)01546-X
3. Li X, Krumholz HM, Yip W, et al. Quality of primary health care in China: challenges and recommendations. Lancet. 2020;395(10239):1802–1812. doi:10.1016/S0140-6736(20)30122-7
4. Li X, Lu J, Hu S, et al. The primary health-care system in China. Lancet. 2017;390(10112):2584–2594. doi:10.1016/S0140-6736(17)33109-4
5. Mahipala P, Dorji G, Tisocki K, Rani M. A critical review of addressing cardiovascular and other non-communicable diseases through a primary health care approach in the South-East Asia Region. Cardiovasc Diagn Ther. 2019;9(2):150–157. doi:10.21037/cdt.2018.09.03
6. Du X, Guo L, Xia S, et al. Atrial fibrillation prevalence, awareness and management in a nationwide survey of adults in China. Heart. 2021;107(7):535–541. doi:10.1136/heartjnl-2020-317915
7. Lip GYH. The ABC pathway: an integrated approach to improve AF management. Nat Rev Cardiol. 2017;14(11):627–628. doi:10.1038/nrcardio.2017.153
8. Romiti GF, Pastori D, Rivera-Caravaca JM, et al. Adherence to the ‘Atrial Fibrillation Better Care’ pathway in patients with atrial fibrillation: impact on clinical outcomes-a systematic review and meta-analysis of 285,000 patients. Thromb Haemost. 2022;122(3):406–414. doi:10.1055/a-1515-9630
9. Stevens D, Harrison SL, Kolamunnage-Dona R, Lip GYH, Lane DA. The Atrial Fibrillation Better Care pathway for managing atrial fibrillation: a review. Europace. 2021;23(10):1511–1527. doi:10.1093/europace/euab092
10. Hindricks G, Potpara T, Dagres N, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the task force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42(5):373–498. doi:10.1093/eurheartj/ehaa798
11. Chao TF, Joung B, Takahashi Y, et al. 2021 focused update consensus guidelines. of the Asia Pacific Heart Rhythm Society on stroke prevention in atrial fibrillation: executive summary. Thromb Haemost. 2022;122(1):20–47. doi:10.1055/s-0041-1739411
12. Wang Y, Guo Y, Qin M, et al. 2024 Chinese Expert Consensus Guidelines on the diagnosis and Treatment of Atrial Fibrillation in the Elderly, Endorsed by Geriatric Society of Chinese Medical Association (Cardiovascular Group) and Chinese Society of Geriatric Health Medicine (Cardiovascular branch): executive Summary. Thrombosis Haemostasis. 2024;2024:1. doi:10.1055/a-2325-5923
13. Lip GYH, Banerjee A, Boriani G, et al. Antithrombotic therapy for atrial fibrillation: CHEST guideline and expert panel report. Chest. 2018;154(5):1121–1201. doi:10.1016/j.chest.2018.07.040
14. Zhou Y, Wu Q, Li C, Meng P, Ding L. Inequalities in non-communicable disease management in China and progress toward universal health coverage: an analysis of nationwide household survey data from 2004 to 2018. Lancet Reg Health West Pac. 2023;44:100989. doi:10.1016/j.lanwpc.2023.100989
15. Li M, Zhang X, Tang H, et al. Quality of primary health care for chronic diseases in low-resource settings: evidence from a comprehensive study in rural China. PLoS One. 2024;19(7):e0304294. doi:10.1371/journal.pone.0304294
16. Palm P, Qvist I, Rasmussen TB, Christensen SW, Håkonsen SJ, Risom SS. Educational interventions to improve outcomes in patients with atrial fibrillation-a systematic review. Int J Clin Pract. 2020;74(11):e13629. doi:10.1111/ijcp.13629
17. Rosengren A, Smyth A, Rangarajan S, et al. Socioeconomic status and risk of cardiovascular disease in 20 low-income, middle-income, and high-income countries: the Prospective Urban Rural Epidemiologic (PURE) study. Lancet Glob Health. 2019;7(6):e748–e760. doi:10.1016/S2214-109X(19)30045-2
18. Li S, Liu Z, Joseph P, et al. Modifiable risk factors associated with cardiovascular disease and mortality in China: a PURE substudy. Eur Heart J. 2022;43(30):2852–2863. doi:10.1093/eurheartj/ehac268
19. Li M, Shi J, Chu M, et al. Screening for atrial fibrillation by village doctors in rural areas of China: the Jiangsu Province Rural Community AF Project. Vasc Health Risk Manag. 2022;18:757–766. doi:10.2147/VHRM.S379182
20. Li M, Chu M, Zhang S, et al. Is it the high time to leave the chronic disease care of rural older people on village doctors in China: deep insight from a population-based atrial fibrillation screening study. Curr Probl Cardiol. 2024;49(10):102759. doi:10.1016/j.cpcardiol.2024.102759
21. Wang YF, Jiang C, He L, et al. Integrated care of atrial fibrillation using the ABC (Atrial fibrillation Better Care) pathway improves clinical outcomes in Chinese population: an analysis from the Chinese Atrial Fibrillation Registry. Front Cardiovasc Med. 2021;8:762245. doi:10.3389/fcvm.2021.762245
22. Yoon M, Yang P-S, Jang E, et al. Improved population-based clinical outcomes of patients with atrial fibrillation by compliance with the simple ABC (Atrial Fibrillation Better Care) pathway for integrated care management: a nationwide cohort study. Thromb Haemost. 2019;119(10):1695–1703. doi:10.1055/s-0039-1693516
23. Vitolo M, Proietti M, Malavasi VL, et al. Adherence to the “Atrial fibrillation Better Care” (ABC) pathway in patients with atrial fibrillation and cancer: a report from the ESC-EHRA EURObservational Research Programme in atrial fibrillation (EORP-AF) General Long-Term Registry. Eur J Intern Med. 2022;105:54–62. doi:10.1016/j.ejim.2022.08.004
24. Romiti GF, Proietti M, Bonini N, et al. Clinical complexity domains, anticoagulation, and outcomes in patients with atrial fibrillation: a report from the GLORIA-AF Registry Phase II and III. Thromb Haemost. 2022;122(12):2030–2041. doi:10.1055/s-0042-1756355
25. Lip GYH, Genaidy A, Tran G, Marroquin P, Estes C, Sloop S. Improving stroke risk prediction in the general population: a comparative assessment of common clinical rules, a new multimorbid index, and machine-learning-based algorithms. Thromb Haemost. 2022;122(1):142–150. doi:10.1055/a-1467-2993
26. Zheng Y, Lip GYH, Guo L, Zhu W. Effect of oral anticoagulants in atrial fibrillation patients with polypharmacy: a meta-analysis. Thromb Haemost. 2023;2023:2. doi:10.1055/s-0043-1770724
27. Treewaree S, Lip GYH, Krittayaphong R. Non-vitamin K antagonist oral anticoagulant, warfarin, and ABC pathway adherence on hierarchical outcomes: win ratio analysis of the COOL-AF Registry. Thromb Haemost. 2024;124(1):69–79. doi:10.1055/s-0043-1772773
28. Krittayaphong R, Treewaree S, Wongtheptien W, Kaewkumdee P, Lip GYH. Clinical phenotype classification to predict risk and optimize the management of patients with atrial fibrillation using the Atrial fibrillation Better Care (ABC) pathway: a report from the COOL-AF registry. QJM. 2023;2023:hcad219. doi:10.1093/qjmed/hcad219
29. Romiti GF, Guo Y, Corica B, et al. Mobile health-technology-integrated care for atrial fibrillation: a win ratio analysis from the mAFA-II randomized clinical trial. Thromb Haemost. 2023;123(11):1042–1048. doi:10.1055/s-0043-1769612
30. Van Gelder IC, Rienstra M, Bunting KV, et al. 2024 ESC Guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2024;45(36):3314–3414. doi:10.1093/eurheartj/ehae176
31. Vinereanu D, Lopes RD, Bahit MC, et al. A multifaceted intervention to improve treatment with oral anticoagulants in atrial fibrillation (IMPACT-AF): an international, cluster-randomised trial. Lancet. 2017;390(10104):1737–1746. doi:10.1016/S0140-6736(17)32165-7
32. Guo Y, Lane DA, Wang L, et al. Mobile health technology to improve care for patients with atrial fibrillation. J Am Coll Cardiol. 2020;75(13):1523–1534. doi:10.1016/j.jacc.2020.01.052
33. Wijtvliet EPJP, Tieleman RG, van Gelder IC, et al. Nurse-led vs. usual-care for atrial fibrillation. Eur Heart J. 2020;41(5):634–641. doi:10.1093/eurheartj/ehz666
34. Rivera-Caravaca JM, Roldán V, Martínez-Montesinos L, Vicente V, Lip GYH, Marín F. The Atrial Fibrillation Better Care (ABC) pathway and clinical outcomes in patients with atrial fibrillation: the prospective Murcia AF Project Phase II Cohort. J Gen Intern Med. 2023;38(2):315–323. doi:10.1007/s11606-022-07567-5
35. Proietti M, Romiti GF, Olshansky B, Lane DA, Lip GYH. Comprehensive management with the ABC (Atrial Fibrillation Better Care) pathway in clinically complex patients with atrial fibrillation: a post hoc ancillary analysis from the AFFIRM trial. J Am Heart Assoc. 2020;9(10):e014932. doi:10.1161/JAHA.119.014932
36. Hendriks JM, de Wit R, Crijns HJ, et al. Nurse-led care vs. usual care for patients with atrial fibrillation: results of a randomized trial of integrated chronic care vs. routine clinical care in ambulatory patients with atrial fibrillation. Eur Heart J. 2012;33(21):2692–2699. doi:10.1093/eurheartj/ehs071
37. Sun Y, Mu J, Wang DW, et al. A village doctor-led multifaceted intervention for blood pressure control in rural China: an open, cluster randomised trial. Lancet. 2022;399(10339):1964–1975. doi:10.1016/S0140-6736(22)00325-7
38. He J, Ouyang N, Guo X, et al. Effectiveness of a non-physician community health-care provider-led intensive blood pressure intervention versus usual care on cardiovascular disease (CRHCP): an open-label, blinded-endpoint, cluster-randomised trial. Lancet. 2023;401(10380):928–938. doi:10.1016/S0140-6736(22)02603-4
39. Ding H, Chen Y, Yu M, et al. The Effects of Chronic Disease Management in Primary Health Care: evidence from Rural China. J Health Econ. 2021;80:102539. doi:10.1016/j.jhealeco.2021.102539
40. Guo Y, Guo J, Shi X, et al. Mobile health technology-supported atrial fibrillation screening and integrated care: a report from the mAFA-II trial Long-term Extension Cohort. Eur J Intern Med. 2020;82:105–111. doi:10.1016/j.ejim.2020.09.024
41. McIntyre D, Kovoor JG, Chow CK, et al. Clinician-created video education for patients with AF: a randomized clinical trial. JAMA Network Open. 2023;6(12):e2345308. doi:10.1001/jamanetworkopen.2023.45308
42. Middeldorp ME, Lyrtzis E, Heath K, Hall T, Kadhim K, Sanders P. Assessment of available online educational resources for patients with atrial fibrillation. Heart Rhythm. 2022;4(3):187–192. doi:10.1016/j.hroo.2022.12.013
43. Li M, Chu M, Shen Y, et al. A Novel Model of Integrated Care of Older Patients with Atrial Fibrillation in Rural China. JACC: Asia. 2024;4(10):764–773. doi:10.1016/j.jacasi.2024.07.006
44. Chu M, Zhang S, Gong J, et al. Telemedicine-based integrated management of atrial fibrillation in village clinics: a cluster randomized trial. Nat Med. 2025;31(4):1276–1285. doi:10.1038/s41591-025-03511-2
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Screening for Atrial Fibrillation by Village Doctors in Rural Areas of China: The Jiangsu Province Rural Community AF Project
Li M, Shi J, Chu M, Shen Y, Zhang S, Sun X, Zhang H, Yan Q, Gong J, Lip GYH, Chen M
Vascular Health and Risk Management 2022, 18:757-766
Published Date: 15 September 2022
Adherence to Atrial Fibrillation Better Care (ABC) Pathway Management of Chinese Community Elderly Patients with Atrial Fibrillation: A Cross-Sectional Study
Zhang X, Huang J, Weng F, Wen Y, Wang X, Jiang J, Xue Y, Li K
Patient Preference and Adherence 2023, 17:1813-1823
Published Date: 25 July 2023
Prognosis of Older Adult Patients Suffering from Atrial Fibrillation and Hypokalemia
Wang XD, Wang Y, Liu J, Yao JW, Zhang J, Zhang YN
Clinical Interventions in Aging 2023, 18:1363-1371
Published Date: 17 August 2023
Exercise, Ethnicity, and Quality of Life in Older Adults with Persistent Nonvalvular Atrial Fibrillation: A Multicenter Cross-Sectional Study
Xu Y, Zhao X, Zheng X, Shi S, Lv F, Dong R, Liu K
Clinical Interventions in Aging 2026, 21:599331
Published Date: 15 May 2026