Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Influence of 5A-Based Self-Regulated Nursing Intervention on Self-Care Capability and Well-Being Among PCI Recipients with Coronary Heart Disease
Authors Wang H, Wang W, Zhang L
Received 22 September 2025
Accepted for publication 18 December 2025
Published 6 January 2026 Volume 2026:19 569413
DOI https://doi.org/10.2147/JMDH.S569413
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Veronica Swallow
Huili Wang,1,* Wenjuan Wang,1,* Lihong Zhang2
1Department of Nursing, The Eighth People’s Hospital of Jinan, Jinan, 271126, People’s Republic of China; 2Department of Critical Care Medicine, The Eighth People’s Hospital of Jinan, Jinan, 271126, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Huili Wang, Email [email protected]
Objective: This study aimed to assess the effectiveness of a 5A-based self-management nursing intervention in patients with coronary heart disease (CHD) after percutaneous coronary intervention (PCI), focusing on its impact on self-care ability and quality of life.
Methods: This retrospective study included CHD patients who underwent PCI at our hospital between September and December 2023. Based on nursing records, patients who received routine care were assigned to the control group, while those who additionally received a 5A-based self-management nursing intervention formed the intervention group. Eligible patients were identified according to predefined inclusion and exclusion criteria. Clinical indicators and patient-reported outcomes were compared between the two groups before and after the intervention.
Results: Baseline characteristics showed no significant differences between groups (P> 0.05). After the intervention period, the intervention group demonstrated significantly higher left ventricular ejection fraction (LVEF), lower serum N-terminal pro-B-type natriuretic peptide (NT-proBNP) levels, and longer distances in the 6-minute walk test (6MWT) compared with the control group (P< 0.05). Treatment adherence was also higher in the intervention group (P< 0.05). At 1, 3, and 6 months, patients in the intervention group achieved significantly better scores on the Coronary Heart Disease Self-Management Scale (CSMS), General Self-Efficacy Scale (GSES), Barthel Index (BI), and Chinese Cardiovascular Quality of Life Questionnaire (CQQC) (P< 0.05).
Conclusion: The 5A-based self-management nursing intervention appears effective for CHD patients after PCI, improving cardiac function, exercise capacity, self-management behaviors, and overall quality of life. These findings support its potential for broader clinical application.
Keywords: coronary heart disease, PCI, 5A, self-management nursing, effect, self-management, quality of life
Introduction
Coronary heart disease (CHD) remains a major global public health challenge, and percutaneous coronary intervention (PCI) is a primary strategy for revascularization in patients with acute coronary syndromes.1–3 Although PCI effectively restores coronary blood flow and improves short-term prognosis, many patients continue to experience recurrent angina, poor treatment adherence, psychological distress, and suboptimal self-management behaviors after discharge.4–6 These factors may compromise long-term outcomes and increase the risk of rehospitalization. Therefore, implementing structured and evidence-based behavioral interventions to enhance patients’ disease perception, emotional well-being, adherence, and self-management capacity is of great clinical value.
The 5A model (Assess, Advise, Agree, Assist, and Arrange) is a widely used behavioral counseling framework that emphasizes individualized goal setting, collaborative decision-making, and continuous follow-up.7–9 Previous studies suggest that the 5A model may offer benefits in chronic disease management, but evidence in cardiovascular populations remains limited and sometimes inconsistent. For example, a clinical trial in patients with heart failure found that a 5A-based self-management program significantly improved fatigue and dyspnea.10,11 Another study involving patients after myocardial infarction demonstrated that the 5A model enhanced quality of life and self-efficacy.12 However, despite these encouraging findings, its application specifically in patients with CHD after PCI is still insufficiently studied, and further validation is needed.
Given this gap, the present study retrospectively evaluated the effectiveness of a 5A-based self-management nursing intervention in CHD patients following PCI, comparing it with routine care. The aim was to provide evidence-based guidance for improving post-PCI self-management, reducing the risk of recurrent cardiovascular events, and enhancing patients’ overall health outcomes.
Objects and Methods
Research Objects
This study retrospectively included CHD patients who underwent PCI treatment at the Department of Cardiology, Jinan Eighth People’s Hospital, from September 2023 to December 2023. A total of 200 eligible patients were included after applying the inclusion and exclusion criteria. Patients were assigned to the treatment group or control group based on treatment received, rather than prospective randomization, to clarify the retrospective nature of the study. The control group (n=100) received routine treatment, while the treatment group (n=100) received the 5A self-management nursing intervention in addition to routine treatment. All interventions were conducted as per the hospital’s standard clinical practice. The study was strictly conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Jinan Eighth People’s Hospital. As patient consent for reviewing medical records was not required by the Ethics Committee, all patient data were handled with strict confidentiality, and no identifiable personal information was disclosed. Follow-up assessments were conducted at 1, 3, and 6 months post-intervention, as all patients had been treated and followed within the study timeframe (Sep–Dec 2023). Data were collected from medical records and follow-up visits. As this is a retrospective study using routine care data, no blinding of participants or evaluators was applied. Outcome assessments were based on objective medical record data and standardized scales, reducing potential bias.
Inclusion Criteria
Inclusion Criteria
Clinically diagnosed with CHD, based on the “Chinese Guidelines for Percutaneous Coronary Intervention (2022)”;13–16
Undergoing first-time elective PCI treatment with good surgical outcomes (TIMI flow grade 3 post-surgery) and stable vital signs post-surgery;17–19
Age of at least 18 years;
Complete clinical medical records, including baseline data and follow-up records;
Normal cognitive function and basic understanding and communication abilities.
Exclusion Criteria
Patients with comorbidities such as malignant tumors, severe liver or kidney diseases (estimated glomerular filtration rate <30 mL/min/1.73m2) or end-stage heart failure (NYHA functional classification IV);
Patients with cognitive impairments or a history of mental illness that may affect the implementation of intervention measures;
Patients with incomplete follow-up data, with missing key data exceeding 20%;
Patients with other severe complications that may affect the assessment of study results.
Intervention Plan
Control Group (Routine Care)
In-hospital care: Post-operative monitoring (ECG monitoring, puncture site observation); standardized health education (importance of oral antiplatelet medications, low-fat diet recommendations); distribution of the “PCI Post-operative Rehabilitation Manual” before discharge.
Out-of-hospital follow-up: Telephone follow-up one month post-surgery to remind patients of their follow-up appointments and medication adherence.
Treatment Group (Routine Care + 5A Self-Management Intervention)
Assessment Phase (Assess)
Within 48 hours of admission, the patient’s disease awareness, disease severity, and self-management ability are systematically assessed based on clinical data, lifestyle surveys, and surgical conditions. Individualized intervention priorities are determined using standardized assessment tools to provide a basis for setting rehabilitation goals and formulating personalized plans. A cardiac rehabilitation specialist nurse uses standardized assessment tools to systematically collect information on the patient’s lifestyle (including dietary structure, tobacco use, daily exercise levels, etc.) and conducts exercise risk assessments. For patients with acute symptoms or fluctuating conditions, assessments are postponed until clinical stability.
Health Education Phase (Advise)
Before formulating the rehabilitation plan, individualized risk factors (such as nicotine dependence, alcohol intake, abnormal glucose metabolism, and insufficient exercise) are explained to the patient through structured interviews. The clinical value of cardiac rehabilitation in improving myocardial function and promoting post-operative recovery is emphasized. Based on routine education, phased training is conducted according to the latest guidelines: at time points of days 2–3, 5–6 of admission, and the day before discharge, with a duration of 30 minutes each time. Education forms include personalized guidance, multimedia presentations, video teaching, and experience sharing among patients. The core content covers the pathological mechanism of CHD, risk factor management, medication treatment plans, key points of PCI post-operative management, and specific implementation strategies for healthy lifestyles (regular medication use, scientific diet, moderate exercise, symptom monitoring, emotional regulation, and smoking cessation and alcohol restriction).
Plan Confirmation Phase (Agree)
A rehabilitation plan is mutually agreed upon by healthcare professionals and the patient, focusing on key goals such as improving disease self-management ability, reducing the risk of recurrent cardiovascular events, and improving cardiac functional reserve. Specific behavior change goals, including smoking cessation and alcohol restriction, establishing a regular schedule, etc., are also formulated.
Rehabilitation Training Implementation (Assist)
A progressive exercise rehabilitation program is adopted:
Early post-operative period (24–48 hours): Bed joint mobility exercises (fisting, elbow flexion, etc)., 10 minutes per session, twice daily.
Intermediate post-operative period (3–4 days): Transition to bedside standing exercises and assisted walking (15–20 meters per session, twice daily).
Progressive post-operative period (4 days): Increase respiratory training frequency to five times daily and independent walking (50 meters per session, twice daily).
Intensive post-operative period (5–6 days): Further increase training intensity (eight times daily) and extend walking time to five minutes per session.
Pre-discharge period (starting from day 7): Introduce outdoor walking exercises and continue until discharge. Vital signs such as blood oxygen and blood pressure are monitored throughout the process, with no fatigue or angina symptoms as the safety threshold. The training plan is dynamically adjusted accordingly.
Continuation Management Phase (Arrange)
A three-level follow-up system is established, including pre-discharge assessment to finalize exercise ability evaluations; family member guidance on home monitoring points and emergency response procedures; and out-of-hospital follow-up with routine medication and lifestyle guidance provided by the responsible nurse, training supervision by the rehabilitation nurse (at least one remote follow-up per week), regular reminders for follow-up appointments, and adjustments to the training plan.
Quality Control Measures
Standardized assessment scales are used to ensure data consistency.
A symptom warning mechanism is established to ensure training safety.
Digital platforms are utilized for real-time recording of follow-up data.
The intervention period for both groups is one year, with follow-up periods at one month, three months, and six months.
Observation Indicators
Intervention Effect
Cardiac function and exercise tolerance are assessed using left ventricular ejection fraction (LVEF) measured by the XFl20.A cardiac function hemodynamics detector (Changsha Xiongfei Technology); serum NT-proBNP concentration detected using the DxI800 Access fully automated chemiluminescence immunoassay analyzer (Beckman Coulter) after fasting venous blood collection (3 mL, centrifuged at 3000 r/min for 15 minutes); and the 6-minute walk test (6MWT) to record the maximum walking distance in six minutes on a flat corridor.
Treatment Adherence Evaluation
Assessed by dedicated nurses using the following criteria:
Complete adherence: Autonomously and regularly completing the entire training plan.
Partial adherence: Completing the main training content with supervision.
Non-adherence: Failing to adhere to the established training plan.
Calculation method: Adherence rate = (Number of completely adherent patients + number of partially adherent patients) / Total number of patients × 100%.
Self-Management Ability
Assessed using the Coronary Heart Disease Self-management Behavior Scale (CSMS), which includes three dimensions (emotional management, daily life management, and disease medical management) with 27 items. The total score ranges from 0 to 135, with higher scores indicating better self-management.
Self-Efficacy
Assessed using the General Self-Efficacy Scale (GSES), where the score is positively correlated with the level of self-efficacy.
Daily Living Ability
Assessed using the Barthel Index (BI), which evaluates six basic activities including personal hygiene, dressing, and toileting. The total score is 100, with higher scores indicating stronger self-care ability.
Quality of Life
Evaluated using the Chinese Cardiovascular Quality of Life Questionnaire (CQQC), which covers six dimensions including physical strength, illness, and psychosocial factors. The total score ranges from 0 to 154, with higher scores indicating better quality of life.
Statistical Methods
GraphPad Prism 8 was used for image processing.
SPSS 26.0 software was used for data organization and statistical analysis.
Measurement data are presented as mean ± standard deviation (±s) and compared using t-tests.
Count data are presented as rates (%) and compared using chi-square tests (χ2).
P<0.05 indicates statistically significant differences.
Results
General Information
This study included 200 PCI post-operative patients, with 100 patients in each group. The baseline characteristics of the two groups were balanced: the treatment group had an average age of 55.74±7.23 years, with 55 males (55.00%); the control group had an average age of 56.01±7.18 years, with 53 males (53.00%). In terms of disease duration, the treatment group had 3.32±1.01 years, and the control group had 3.28±1.12 years. There were no significant differences in age (t=0.265, P=0.791), gender (χ2=0.081, P=0.776), or disease duration (t=0.265, P=0.791) between the two groups (Table 1).
 |
Table 1 General Information of Patients in Both Groups (±s) |
Intervention Effect
Cardiac Function
After intervention, the cardiac function of the treatment group was significantly better than that of the control group: LVEF increased from 52.3±5.1% to 58.7±4.8% in the treatment group compared to 52.1±5.3% to 54.9±5.0% in the control group (inter-group difference t=4.92, P<0.001); NT-proBNP decreased from 856.4±152.7 pg/mL to 324.6±98.5 pg/mL in the treatment group, a 62.1% reduction, which was significantly better than the reduction in the control group (856.8±155.2 to 498.3±120.1 pg/mL, t=5.67, P<0.001) (Figure 1).
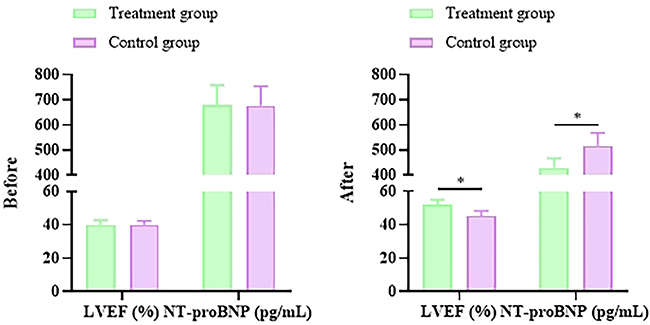 |
Figure 1 Comparison of Cardiac Function Indicators LVEF and NT-proBNP Between the Two Groups Before and After Intervention. *Indicates statistically significant differences between the two groups (P<0.05). |
Exercise Tolerance
The 6-minute walk test (6MWT) showed that the exercise tolerance of the treatment group improved more significantly: the walking distance increased from 328.5±45.2 meters to 412.7±38.6 meters (an increase of 84.2 meters) in the treatment group compared to 326.8±44.9 meters to 376.3±40.1 meters (an increase of 49.5 meters) in the control group (inter-group difference t=6.34, P<0.001) (Figure 2).
 |
Figure 2 Comparison of 6MWT Distances Between the Two Groups Before and After Intervention.*Indicates statistically significant differences between the two groups (P<0.05). |
Treatment Adherence
The adherence rate of the treatment group (95.00%) was significantly higher than that of the control group (80.00%) (χ2=10.23, P=0.001). Specifically: complete adherence was observed in 78 cases (78.00%) in the treatment group versus 52 cases (52.00%) in the control group; partial adherence was observed in 17 cases (17.00%) in the treatment group versus 28 cases (28.00%) in the control group; and non-adherence was observed in 5 cases (5.00%) in the treatment group versus 20 cases (20.00%) in the control group (Figure 3).
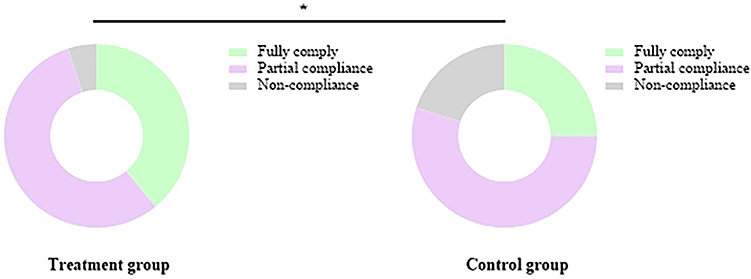 |
Figure 3 Comparison of Adherence Rates Between the Two Groups. *Indicates statistically significant differences between the two groups (P<0.05). |
Self-Management
The Coronary Heart Disease Self-management Scale (CSMS) scores showed continuous improvement in self-management ability in the treatment group: 1 month: 89.5±10.2 points in the treatment group vs 76.8±9.7 points in the control group (t=8.12, P<0.001); 3 months: 102.3±11.5 points in the treatment group vs 85.4±10.8 points in the control group (t=10.45, P<0.001); 6 months: 118.7±12.1 points in the treatment group vs 92.6±11.3 points in the control group (t=14.67, P<0.001) (Figure 4).
 |
Figure 4 Comparison of CSMS Scores Between the Two Groups. *Indicates statistically significant differences between the two groups (P<0.05). |
Self-Efficacy
Changes in General Self-Efficacy Scale (GSES) scores: 1 month: 25.7±3.8 points in the treatment group vs 20.3±3.5 points in the control group (t=9.23, P<0.001); 3 months: 29.4±4.1 points in the treatment group vs 22.6±3.9 points in the control group (t=11.56, P<0.001); 6 months: 33.8±4.5 points in the treatment group vs 24.9±4.2 points in the control group (t=13.89, P<0.001) (Figure 5).
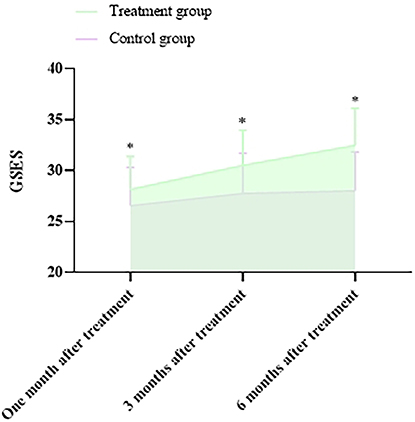 |
Figure 5 Comparison of GSES Scores Between the Two Groups. *Indicates statistically significant differences between the two groups (P<0.05). |
Self-Care Ability
The Barthel Index (BI) showed better self-care ability in the treatment group: 1 month: 75.3±8.6 points in the treatment group vs 65.2±7.9 points in the control group (t=7.89, P<0.001); 3 months: 86.7±9.2 points in the treatment group vs 72.4±8.5 points in the control group (t=10.34, P<0.001); 6 months: 94.5±9.8 points in the treatment group vs 80.1±9.0 points in the control group (t=10.34, P<0.001) (Figure 6).
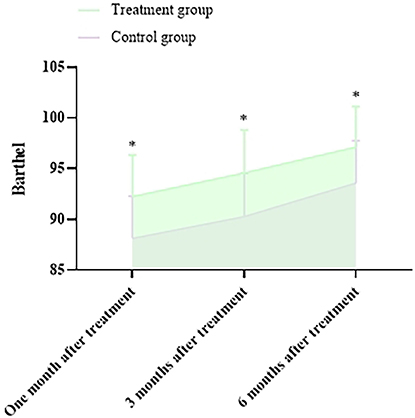 |
Figure 6 Comparison of Barthel Index Scores Between the Two Groups. *Indicates statistically significant differences between the two groups (P<0.05). |
Quality of Life
Scores on the Chinese Cardiovascular Quality of Life Questionnaire (CQQC): 1 month: 98.6±12.3 points in the treatment group vs 85.7±11.8 points in the control group (t=7.45, P<0.001); 3 months: 115.2±13.5 points in the treatment group vs 95.4±12.7 points in the control group (t=10.12, P<0.001); 6 months: 132.8±14.1 points in the treatment group vs 105.3±13.2 points in the control group (t=13.78, P<0.001) (Figure 7).
 |
Figure 7 Comparison of CQQC Scores Between the Two Groups. *Indicates statistically significant differences between the two groups (P<0.05). |
Discussion
Self-management refers to the process by which individuals actively participate in health decisions and adopt a series of behaviors to maintain or improve their health status during disease management. For PCI post-operative patients, good self-management abilities include regular medication, reasonable diet, moderate exercise, smoking cessation and alcohol restriction, regular follow-up, and psychological adjustment.20–22 However, clinical observations have shown that many patients lack systematic health education and continuous nursing support, leading to poor self-management abilities, which in turn results in suboptimal post-operative rehabilitation outcomes and even increased readmission risks. Therefore, exploring effective nursing intervention models to improve patients’ self-management abilities is of significant clinical importance.
Currently, domestic research on PCI post-operative nursing has mostly focused on routine health education or short-term follow-ups, lacking systematic and structured long-term self-management intervention programs. Moreover, existing studies have paid less attention to cardiac function indicators (such as left ventricular ejection fraction, LVEF, and NT-proBNP) and exercise tolerance (such as the 6-minute walk test, 6MWT), which are crucial for assessing the rehabilitation outcomes of PCI post-operative patients. Therefore, this study aimed to explore the impact of the 5A self-management nursing intervention on coronary heart disease PCI post-operative patients, with a focus on analyzing its effects on cardiac function, exercise tolerance, self-management abilities (using the CSMS and GSES), and quality of life (using the BI and CQQC), in order to provide more scientific evidence for clinical nursing practice.
This study retrospectively analyzed clinical data from 200 coronary heart disease PCI post-operative patients and systematically evaluated the impact of the 5A self-management nursing intervention on patients’ cardiac function, exercise tolerance, self-management abilities, and quality of life. The results showed that compared with routine care, the treatment group exhibited significant advantages in physiological indicators such as LVEF, NT-proBNP, and 6MWT, as well as in psychosocial indicators such as CSMS, GSES, BI, and CQQC, verifying the effectiveness of the 5A model in PCI post-operative rehabilitation. The following discussion combines the study results with existing evidence from three aspects: mechanism exploration, clinical significance, and limitations.
First, the significant increase in LVEF and the decrease in NT-proBNP levels in the treatment group suggest that the 5A intervention may improve cardiac remodeling and neuroendocrine activation through multiple pathways. On the one hand, individualized exercise prescriptions (such as aerobic combined with resistance training) can enhance myocardial contractility and reduce cardiac afterload, while strict fluid management (for patients with high NT-proBNP levels) reduces the risk of volume overload. This is consistent with previous clinical studies23–25 which concluded that structured exercise rehabilitation can increase LVEF by 3–5% in PCI post-operative patients. On the other hand, continuous medication adherence supervision (such as pillbox counting) may optimize the therapeutic effects of antiplatelet medications and statins, thereby inhibiting the progression of atherosclerosis and reducing the release of myocardial injury markers. Additionally, the significant increase in 6MWT distance in the treatment group (approximately 50 meters more than the control group) reflects an overall improvement in exercise tolerance. This result is closely related to the “assist” component of the 5A model: by providing fitness trackers to monitor real-time heart rate and step count, patients can safely execute their exercise plans and avoid overexertion; meanwhile, success stories shared during online group counseling may enhance patients’ confidence and promote their active participation in exercise training. Studies have confirmed that every 30-meter increase in 6MWT distance can reduce cardiovascular mortality risk by approximately 8%, suggesting that this intervention may have long-term prognostic benefits. Moreover, previous studies have applied cardiac rehabilitation interventions based on the 5A model and have demonstrated significant improvements in LVEF, exercise tolerance, and treatment adherence.26 These findings are highly consistent with the results of the present study and further support the effectiveness of this model across different countries and healthcare systems.
Second, the significant increase in CSMS and GSES scores in the treatment group indicates that the 5A model effectively enhances patients’ self-management behaviors and self-efficacy through a systematic assessment-feedback loop. Self-efficacy refers to the ability of individuals to regulate their own behaviors based on the external environment; the stronger the confidence, the stronger the ability to regulate and change one’s own behaviors, thereby better coping with stress and challenges. Low self-efficacy, on the other hand, can lead to an undervaluation of oneself and a decreased ability to cope with disease and setbacks.27–31 From the baseline of the 5A nursing model intervention, it is evident that patients’ self-management behaviors were suboptimal, with significantly low self-management scores, which is consistent with previous related studies. After implementing the 5A model intervention, patients’ self-management behaviors showed significant advantages over the control group. Specifically, the “assess” phase provided an accurate identification of patients’ baseline abilities (such as identifying weaknesses in diet control through CSMS), providing a scientific basis for subsequent personalized recommendations (such as formulating a modified Mediterranean diet plan). Furthermore, “reaching agreement” may have enhanced patients’ sense of responsibility through a psychological contract mechanism, whereby goal setting and successful experiences accumulate, gradually increasing patients’ confidence in their own abilities and thereby promoting the long-term maintenance of healthy behaviors.32–34 Meanwhile, cultural and regional factors may influence patient adherence. For example, older patients in China tend to rely more on family members for decision-making, and the lower usage of smart devices in rural areas may also affect the implementation of the 5A model. Future studies should consider how to further optimize this model within different cultural contexts to enhance its generalizability.
In terms of quality of life, the improvement in BI and CQQC scores in the treatment group suggests that the 5A intervention not only focuses on physiological rehabilitation but also on the restoration of psychosocial functions. For instance, the “PCI Rehabilitation Mutual Aid Group” in the “assist” phase provided patients with a social support network, alleviating the loneliness brought about by their illness. Meanwhile, anxiety screening (such as the SAS scale) and targeted psychological counseling during regular follow-ups may have reduced the negative impact of depressive emotions on daily activities. Moreover, studies have shown that poor treatment adherence in PCI post-operative patients, such as failing to actively cooperate with medication, lifestyle improvements, and follow-up appointments, can lead to recurrent angina pectoris, myocardial infarction, and cardiogenic death. This study found that the 5A self-management nursing model can improve treatment adherence and strengthen medication compliance in PCI post-operative patients, enhancing rehabilitation outcomes and improving quality of life, which also explains why the BI index and CQQC scores in the observation group were significantly higher than those in the control group.
The innovative aspects of this study are twofold: firstly, it is the first time the 5A model has been combined with PCI post-operative nursing, and a comprehensive assessment of intervention effects was conducted using multidimensional outcome indicators (covering physiological, behavioral, psychological, and social functions); secondly, NT-proBNP and 6MWT were introduced as objective quantitative indicators of cardiac function and exercise tolerance, making up for the deficiency of previous studies that relied excessively on subjective scales. These findings provide empirical evidence for the update of cardiac rehabilitation guidelines, suggesting, for example, the inclusion of the 5A model in the standardized nursing pathway for PCI post-operative care. However, this study has the following limitations: firstly, as a single-center retrospective study, although stringent exclusion criteria were used to reduce confounding bias, selection bias could not be completely avoided (such as the possibility that included patients had higher health awareness); secondly, the intervention effect may be influenced by differences in regional medical resources (such as the coverage of WeChat mini-programs among the elderly population), and future multi-center prospective studies are needed to further verify the universality of the conclusions. In addition, the follow-up period in this study was limited to six months. Although significant improvements were observed in cardiac function, exercise tolerance, and self-management ability, evidence is still insufficient to determine whether these benefits can be sustained for 12 months or longer. Future work will involve prospective studies with extended follow-up to evaluate the long-term impact of the 5A model on key clinical endpoints, such as readmission rates, in-stent restenosis, major adverse cardiovascular events (MACE), and cardiovascular mortality, thereby providing a more comprehensive assessment of its clinical value. Furthermore, future research may explore integrating the 5A model with digital follow-up platforms, wearable device monitoring, and artificial intelligence–assisted decision-making systems. Such integration could enhance patient adherence, enable continuous management, and improve the model’s applicability across diverse regions and healthcare settings, ultimately extending its utility and scalability.
Conclusion
In summary, the 5A self-management nursing intervention for patients with coronary heart disease following PCI demonstrated clear benefits. It significantly improved cardiac function, exercise tolerance, self-management ability, and overall quality of life compared with routine care. These findings suggest that the 5A model may serve as an effective and feasible nursing strategy in the postoperative management of PCI patients. However, given the retrospective design and single-center nature of the study, further multicenter prospective studies are warranted to validate and extend these results.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Khamis RY, Ammari T, Mikhail GW. Gender differences in coronary heart disease. Heart. 2016;102(14):1142–12. doi:10.1136/heartjnl-2014-306463
2. Ulbricht TL, Southgate DA. Coronary heart disease: seven dietary factors. Lancet. 1991;338(8773):985–992. doi:10.1016/0140-6736(91)91846-M
3. Wirtz PH, von Känel R. Psychological stress, inflammation, and coronary heart disease. Curr Cardiol Rep. 2017;19(11):111. doi:10.1007/s11886-017-0919-x
4. Akbari T, Al-Lamee R. Percutaneous coronary intervention in multi-vessel disease. Cardiovasc Revasc Med. 2022;44:80–91. doi:10.1016/j.carrev.2022.06.254
5. Angiolillo DJ, Galli M, Collet J-P, et al. Antiplatelet therapy after percutaneous coronary intervention. EuroIntervention. 2022;17(17):e1371–e1396. doi:10.4244/EIJ-D-21-00904
6. Bhatt DL. Percutaneous coronary intervention in 2018. JAMA. 2018;319(20):2127–2128. doi:10.1001/jama.2018.5281
7. Sherson EA, Jimenez EY, Katalanos N. A review of the use of the 5 A’s model for weight loss counselling: differences between physician practice and patient demand. Fam Pract. 2014;31(4):389–398. doi:10.1093/fampra/cmu020
8. Fisher EB, Brownson CA, O’Toole ML, et al. Ecological approaches to self-management: the case of diabetes. Am J Public Health. 2005;95(9):1523–1535. doi:10.2105/AJPH.2005.066084
9. Xu Y, Yang J. The effect of 5A nursing combined with psychological nursing on the immune function, cancer-related fatigue and complications of patients undergoing radical resection of colorectal cancer. Cell Mol Biol. 2022;68(1):169–176. doi:10.14715/cmb/2022.68.1.21
10. Hajmohamadi M, Imani-Goghary Z, Jahani Y, Sabzevari S. Investigating the effectiveness of self-management program based on 5A model on fatigue and dyspnea in patients with heart failure. Bratisl Lek Listy. 2023;124(11):821–826. doi:10.4149/BLL_2023_126
11. Zhao S, Xu H, Liu F, Guo X, Zhang Y. Application of early multi-dimensional cardiac rehabilitation nursing in percutaneous coronary intervention and Its effects on adverse events and patients’ adherence to medication. J Mod Nurs Pract Res. 2022;2(4):16. doi:10.53964/jmnpr.2022016
12. Aloghareh SB, Salehi Tali S, Hasanpour Dehkordi A, Gangi H, Sedehi M. The effects of a self-management program based on 5 A`s model on the quality of life and self-efficacy in the myocardial infarction patients. Przegl Epidemiol. 2021;75(4):556–563. doi:10.32394/pe.75.52
13. Tian Y, Deng P, Li B, et al. Treatment models of cardiac rehabilitation in patients with coronary heart disease and related factors affecting patient compliance. Rev Cardiovasc Med. 2019;20(1):27–33. doi:10.31083/j.rcm.2019.01.53
14. Di Angelantonio E, Thompson A, Wensley F, et al. Coronary heart disease. IARC Sci Publ. 2011;163:363–386.
15. Wang Z, Zhang Y, Wang Y, et al. Kinesiophobia and its associated factors in patients with coronary heart disease: a cross-sectional study based on latent feature analysis. BMJ Open. 2023;13(7):e072170. doi:10.1136/bmjopen-2023-072170
16. Cobble M. Coronary heart disease in women. J Fam Pract. 2014;63(2 Suppl):S9–14.
17. Finch W, Lee MS. Percutaneous coronary intervention for coronary bifurcation lesions. Rev Cardiovasc Med. 2017;18(2):59–66. doi:10.3909/ricm0868
18. Banning AP, Baumbach A, Blackman D, et al. Percutaneous coronary intervention in the UK: recommendations for good practice 2015. Heart. 2015;101(Suppl 3):1–13. doi:10.1136/heartjnl-2015-307821
19. Rinfret S, Baron SJ, Cohen DJ. Percutaneous coronary intervention: finally mature enough. J Am Coll Cardiol. 2015;65(23):2508–2510. doi:10.1016/j.jacc.2015.04.041
20. Allegrante JP, Wells MT, Peterson JC. Interventions to support behavioral self-management of chronic diseases. Annu Rev Public Health. 2019;40:127–146. doi:10.1146/annurev-publhealth-040218-044008
21. van Smoorenburg AN, Hertroijs DFL, Dekkers T, et al. Patients’ perspective on self-management: type 2 diabetes in daily life. BMC Health Serv Res. 2019;19(1):605. doi:10.1186/s12913-019-4384-7
22. Duggal HS. Self-Management of depression: beyond the medical model. Perm J. 2019;23.
23. He M, Tong L, Zou Y, et al. Effect of 5A nursing mode combined with fine nursing management on perioperative self-efficacy and living quality of hysteromyoma. Am J Transl Res. 2021;13(9):10737–10743.
24. Zhang X, Lai M, Wu D, et al. The Effect of 5A nursing intervention on living quality and self-care efficacy of patients undergoing chemotherapy after hepatocellular carcinoma surgery. Am J Transl Res. 2021;13(6):6638–6645.
25. Rim D, Shin H, Jeon H, et al. Creating the 5A nursing response model for the emerging pandemic: a qualitative, theory-generating study. J Adv Nurs. 2025;81(9):6011–6021. doi:10.1111/jan.16746
26. Yamaoka K, Katsumata Y, Kohsaka S, et al. Patient-centered medical tools for sustained motivation in cardiac rehabilitation of patients with heart failure: protocol of a multicenter randomized controlled trial (EXERCISE-HF trial). Contemp Clin Trials Commun. 2025;47:101522. doi:10.1016/j.conctc.2025.101522
27. van Riel P, Zuidema RM, Vogel C, et al. Patient self-management and tracking: a European experience. Rheum Dis Clin North Am. 2019;45(2):187–195. doi:10.1016/j.rdc.2019.01.008
28. van Dongen SI, de Nooijer K, Cramm JM, et al. Self-management of patients with advanced cancer: a systematic review of experiences and attitudes. Palliat Med. 2020;34(2):160–178. doi:10.1177/0269216319883976
29. Peng S, He J, Huang J, et al. Self-management interventions for chronic kidney disease: a systematic review and meta-analysis. BMC Nephrol. 2019;20(1):142. doi:10.1186/s12882-019-1309-y
30. Goldberg JI, Schulman-Green D, Hernandez M, et al. Self-Management interventions for psychological distress in adult cancer patients: a systematic review. West J Nurs Res. 2019;41(10):1407–1422. doi:10.1177/0193945919845104
31. Cuthbert CA, Farragher JF, Hemmelgarn BR, et al. Self-management interventions for cancer survivors: a systematic review and evaluation of intervention content and theories. Psychooncology. 2019;28(11):2119–2140. doi:10.1002/pon.5215
32. Keivan S, Shariati A, Miladinia M, et al. Role of self-management program based on 5A nursing model in quality of life among patients undergoing hemodialysis: a randomized clinical trial. BMC Nephrol. 2023;24(1):58. doi:10.1186/s12882-023-03108-2
33. Xu P, Zheng W, Zhu Y. Effect analysis of lung rehabilitation training in 5A nursing mode for elderly patients with COPD based on X-Ray. Comput Math Methods Med. 2022;2022:1963426. doi:10.1155/2022/1963426
34. Shieh C, Hardin HK, Doerstler MD, et al. Integration of the 5A’s framework in research on obesity and weight counseling: systematic review of literature. Am J Lifestyle Med;2024. 15598276241306351. doi:10.1177/15598276241306351
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Health-Related Quality of Life and Influencing Factors in Coronary Heart Disease Based on the Scale QLICD-CHD (V2.0): A Cross-Sectional Study
Rao S, Xu C, Wan C, Huang Z, Huang X, Chen S
International Journal of General Medicine 2023, 16:5119-5129
Published Date: 6 November 2023
Banxia Gualou Xiebai Tang and Qishen Yiqi Dropping Pills Combined Therapy for Qi Deficiency, Phlegm, and Blood Stasis Syndrome in Post-PCI Coronary Heart Disease Patients
Fan M, Du L, Jiang W, Ding T, Yang X, Peng Z
International Journal of General Medicine 2025, 18:1795-1805
Published Date: 31 March 2025
Effectiveness of Community Nurse-Led Intervention in Managing Older Adults with Multimorbidity: A Systematic Review of Randomized Controlled Trials
Rahmat R, Haroen H, Juniarti N, Sari SP, Rinawan FR
Journal of Multidisciplinary Healthcare 2025, 18:6373-6389
Published Date: 3 October 2025
Analysis Impact of Positive Psychological Capital on Quality of Life Among Patients Post Percutaneous Coronary Intervention: A Cross-Sectional Study
Kudelati Z, Yin S, Chen S, Han S, Yuan S, Wang H
Journal of Multidisciplinary Healthcare 2025, 18:7413-7421
Published Date: 11 November 2025
The Effectiveness of a Self-Management-Based Nutritional Promotion Program on Food Consumption Knowledge, Behaviors, and Quality of Life of Patients Undergoing Hemodialysis
Maytharit B, Wungrath J, Ong-artborirak P, Chautrakarn S
Journal of Multidisciplinary Healthcare 2026, 19:591842
Published Date: 14 April 2026