Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Inflammation Mediates the Relationship Between Serum Uric Acid and New-Onset Diabetes Risk in Patients with Coronary Heart Disease: Results from a Multicenter Cohort Study
Authors Song S, Cai X, Xu T, Cui P, Zou Z, Zhao J ![]() , Liu Y, Wang K
, Liu Y, Wang K
Received 11 February 2026
Accepted for publication 31 May 2026
Published 18 June 2026 Volume 2026:19 602643
DOI https://doi.org/10.2147/DMSO.S602643
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hillary Keenan
Shuaiwei Song,1 Xintian Cai,2 Tuo Xu,3 Penghui Cui,4 Ziliang Zou,5 Junjie Zhao,6 Yazhe Liu,7 Kaiyu Wang8
1Department of Endocrinology and Metabolism, Shanghai Tenth People’s Hospital, School of Medicine, Tongji University, Shanghai, People’s Republic of China; 2Heart, Lung and Vessels Center, Sichuan Provincial People’s Hospital, University of Electronic Science and Technology of China, Chengdu, Sichuan, People’s Republic of China; 3Department of Critical Care Medicine, Xinxiang Central Hospital, Xinxiang, Henan, People’s Republic of China; 4Department of Cardiology, Changzhi People’s Hospital, Changzhi, Shanxi, People’s Republic of China; 5Department of Cardiology, Sixth Affiliated Hospital of Kunming Medical University, Yuxi, Yunnan, People’s Republic of China; 6Emergency and Critical Care Center, Department of Emergency Medicine, Zhejiang Provincial People’s Hospital (Affiliated People’s Hospital), Hangzhou Medical College, Hangzhou, Zhejiang, People’s Republic of China; 7Department of Cardiology, Yunyang County People’s Hospital, Yunyang, Chongqing, People’s Republic of China; 8Department of Critical Care Medicine, The Quzhou Affiliated Hospital of Wenzhou Medical University, Quzhou People’s Hospital, Quzhou, Zhejiang, People’s Republic of China
Correspondence: Kaiyu Wang, Department of Critical Care Medicine, The Quzhou Affiliated Hospital of Wenzhou Medical University, Quzhou People’s Hospital, Quzhou, Zhejiang, 324000, People’s Republic of China, Email [email protected]
Background: Serum uric acid (SUA), a key metabolite in purine metabolism, has been linked to various metabolic disturbances. However, its specific role in the development of new-onset diabetes among patients with coronary heart disease (CHD) remains unclear.
Methods: This multi-center study included 5141 CHD patients. To assess the relationship between SUA and diabetes, we used Cox regression and generalized additive models, along with gender-stratified threshold analyses to explore the dose–response pattern. Additionally, the incremental predictive value of SUA was evaluated by calculating the integrated discrimination improvement (IDI) and net reclassification improvement (NRI). Lastly, mediation analysis was performed to examine the potential role of inflammatory markers in the observed association.
Results: Elevated SUA levels were significantly associated with an increased risk of diabetes in CHD patients, showing a clear nonlinear relationship. We identified risk thresholds at SUA levels of > 345 μmol/L for females and > 350.5 μmol/L for males. SUA levels improved diabetes risk prediction, with NRI=0.033 and IDI=0.003. Furthermore, mediation analysis revealed that inflammatory markers partially mediated the association between SUA and diabetes risk, with the highest proportion of mediation reaching 32.27%.
Conclusion: Elevated SUA is an independent risk factor for new-onset diabetes in CHD patients, with gender-specific risk thresholds. This association is partially mediated through inflammation. Monitoring and managing SUA levels may help reduce the risk of diabetes in this high-risk group. Moreover, the mediating role of inflammation provides an important basis for future in-depth mechanistic studies.
Keywords: serum uric acid, coronary heart disease, diabetes, inflammation, insulin resistance
Introduction
Diabetes is a chronic metabolic condition chiefly defined by inadequate insulin secretion or reduced insulin sensitivity, with sustained hyperglycemia representing its hallmark feature.1,2 Prolonged hyperglycemia not only triggers systemic metabolic disturbances but also significantly increases the risk of multi-system complications, including those related to the heart, kidneys, retina, and peripheral nerves.3–6 As modern lifestyles have evolved, especially with the widespread adoption of high-sugar diets, the prevalence of diabetes has risen dramatically, making it one of the most significant chronic diseases threatening public health.7,8
Coronary heart disease (CHD), the most common and fatal form of cardiovascular disease, also represents a major global health burden.9 Notably, there is a close pathophysiological link between diabetes and CHD.10–12 Diabetes-induced dyslipidemia, vascular endothelial dysfunction, and chronic inflammatory states significantly accelerate atherosclerosis, substantially increasing the risk of CHD onset and progression.12,13 When diabetes and CHD coexist, they exacerbate each other’s effects, leading to further vascular and multi-organ damage and a marked increase in patient mortality risk.14–16 Therefore, early identification of diabetes risk and proactive intervention are critical in CHD patients to break this vicious cycle and improve long-term prognosis.
The occurrence of diabetes in patients with CHD has traditionally been linked to unhealthy diets, lifestyles, obesity, and associated metabolic disturbances, such as hyperlipidemia, insulin resistance, and chronic inflammation.17–20 However, the role of serum uric acid (SUA) in diabetes development has often been overlooked. SUA has long been viewed primarily as the end product of purine metabolism, with clinical significance related mainly to gout, joint injury, kidney damage, and certain cardiovascular events (including heart failure, hypertension, and cardiovascular death).21–25 Its impact on glucose metabolism has received less attention. Recent research, however, has gradually recognized SUA’s role in metabolism.26,27 Elevated SUA levels are associated with obesity and contribute to insulin resistance, lipid metabolism disorders, and chronic low-grade inflammation—mechanisms central to diabetes pathophysiology.28–30 As a result, the link between SUA and diabetes is supported by both theoretical and empirical evidence. Moreover, SUA has been shown to cause endothelial dysfunction, promote oxidative stress, and accelerate atherosclerosis, increasing cardiovascular risk, including CHD.31,32 Thus, a complex network emerges between SUA, diabetes, and CHD, where hyperuricemia contributes to CHD development and, through metabolic pathways (insulin resistance, pancreatic β-cell dysfunction, chronic inflammation and lipid metabolism disorders), increases diabetes risk.30,33 When both conditions coexist, they disrupt SUA metabolism, creating a vicious cycle.
In light of these factors, this study aims to investigate, through a multicenter design, the impact of SUA on the risk of diabetes in CHD patients. This approach not only expands the traditional understanding of metabolic risk factors but also provides a novel perspective on disease progression in this high-risk population. It holds promise for the early identification and comprehensive intervention of diabetes in CHD patients, with the potential to clarify the complex relationships among SUA, diabetes, and CHD, offering important implications for improving patient prognosis and enabling more targeted metabolic management.
MaterialS and Methods
Study Population
This study is a multicenter research project that included a total of 9412 patients with CHD from five centers in China: Changzhi People’s Hospital, Sichuan Provincial People’s Hospital, the Sixth Affiliated Hospital of Kunming Medical University, Xinxiang Central Hospital, and Yunyang County People’s Hospital.
Initially, we excluded 529 patients who lacked SUA data. Subsequently, taking into account the potential impact of certain diseases and medications, we further excluded patients who had diabetes at baseline, severe renal dysfunction, were taking any medications that may affect SUA metabolism at baseline (Febuxostat, Benzbromarone, Allopurinol, Diuretics, and Various weight-loss drugs), or had malignant tumors. Lastly, patients who were lost to follow-up were also excluded from the study. After applying these strict exclusion criteria, a total of 5141 CHD patients ultimately met the final research requirements. Figure 1 illustrates the detailed screening process of the study population.
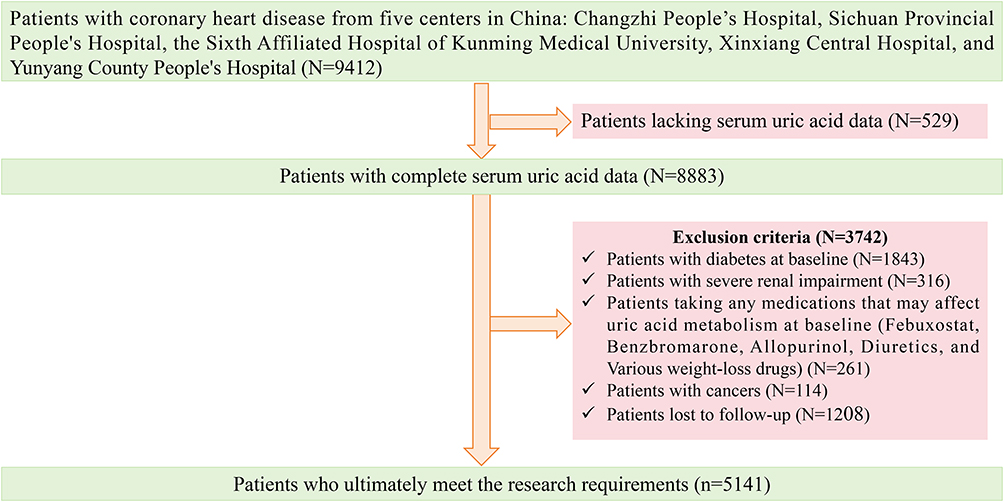 |
Figure 1 Screening process of study participants. |
The entire process of the study followed the Helsinki Declaration and obtained approval from the ethics committees of the five hospitals involved: Changzhi People’s Hospital (CZX20180213), Sichuan Provincial People’s Hospital (CRC2024-0512), the Sixth Affiliated Hospital of Kunming Medical University (XKY20200806), Xinxiang Central Hospital (NXCH20230911), and Yunyang County People’s Hospital (Yy20200419). All participants provided written informed consent prior to enrollment.
Data Collection and Definitions
Data, including patient demographics, physical examination findings, medical history, and laboratory test results, were collected via telephone interviews, in-person visits, electronic medical records, and medical insurance documentation. Measurements such as height, weight, and blood pressure (BP) were taken by professional nurses using standardized methods, as detailed in the Supplementary Materials.
Laboratory tests were conducted using fully automated biochemical analyzers. The biochemical indicators measured included complete blood count, liver function, C-reactive protein (CRP), total cholesterol (TC), triglycerides (TG), fasting blood glucose (FBG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and SUA. The specific measurement instruments and methods can be found in the Supplementary Materials. SUA levels were measured in all patients at baseline enrollment, with blood samples collected by professionally trained nurses using standardized procedures and subjected to standardized measurement. Medication use, including lipid-lowering drugs, antiplatelet drugs, diuretics, beta-blockers, and ACEIs/ARBs, was also collected and recorded.
The diagnoses of CHD, hypertension, and hyperlipidemia were made according to current clinical guidelines, with specific diagnostic criteria detailed in the Supplementary Materials.
Outcome
The primary endpoint of this research was the development of new-onset diabetes in the CHD cohort. The diagnosis of diabetes adhered strictly to contemporary clinical standards,34–36 as defined by any of the following: 1) characteristic symptoms (e.g., polydipsia, polyuria, polyphagia, or unexplained weight loss) accompanied by a random venous plasma glucose level of ≥11.1 mmol/L; 2) a fasting venous plasma glucose level ≥7.0 mmol/L after ≥8 hours of fasting; 3) a 2-hour plasma glucose level ≥11.1 mmol/L during a 75-g oral glucose tolerance test; or 4) a glycated hemoglobin value ≥6.5%.
Endpoint data were collected from multiple sources, including medical visit records, health insurance data, and periodic follow-ups (both face-to-face and via telephone). Follow-up began at baseline enrollment (with the earliest enrolled patient in February 2018) and continued until the earliest of the following three time points: (1) the date of first diabetes diagnosis; (2) the date of the patient’s last follow-up; or (3) the overall study end date (February 1, 2026). Thus, “the date of the last follow-up” refers to the actual date on which an individual patient completed follow-up (possibly due to early withdrawal), while “the overall study end date” is the fixed termination point of the entire study.
Statistical Analysis
Participants were divided into four groups based on quartiles of SUA levels. To assess multicollinearity, variance inflation factors were computed for all predictors; each was found to be below 5, confirming the absence of substantial collinearity (Table S1). Additionally, the proportional hazards assumption test confirmed that the assumptions of the Cox proportional hazards model were satisfied (Figure S1). Subsequently, multivariable-adjusted Cox proportional hazards regression models were employed to assess the association between SUA levels and incident diabetes in patients with CHD. Cumulative diabetes incidence across SUA strata was visualized using Kaplan-Meier (KM) curves. To investigate the dose–response relationship, a generalized additive model (GAM) was fitted, and subgroup analyses were stratified by sex. Furthermore, based on an inflection point identified by the GAM, a two-piecewise regression model was applied to characterize the association pattern in detail.
To evaluate the predictive ability of SUA for diabetes, several metrics were employed: the C-index, net reclassification improvement (NRI), integrated discrimination improvement (IDI), and the Boruta algorithm for variable importance ranking. Finally, a mediation analysis was performed to identify potential mediating factors in the relationship between SUA and diabetes onset. Detailed descriptions of the statistical analysis can be found in the Supplementary Materials.
All analyses were performed in R (version 4.2.2), with statistical significance defined as a two-sided P-value < 0.05.
Results
Baseline Characteristics of the Study Population
This study included 5141 patients from five centers, with a median follow-up duration of 4.15 years. During the follow-up period, 1592 participants were diagnosed with diabetes. We divided the patients into four groups based on the quartiles of their SUA levels, with Table 1 presenting the baseline characteristics of each group.
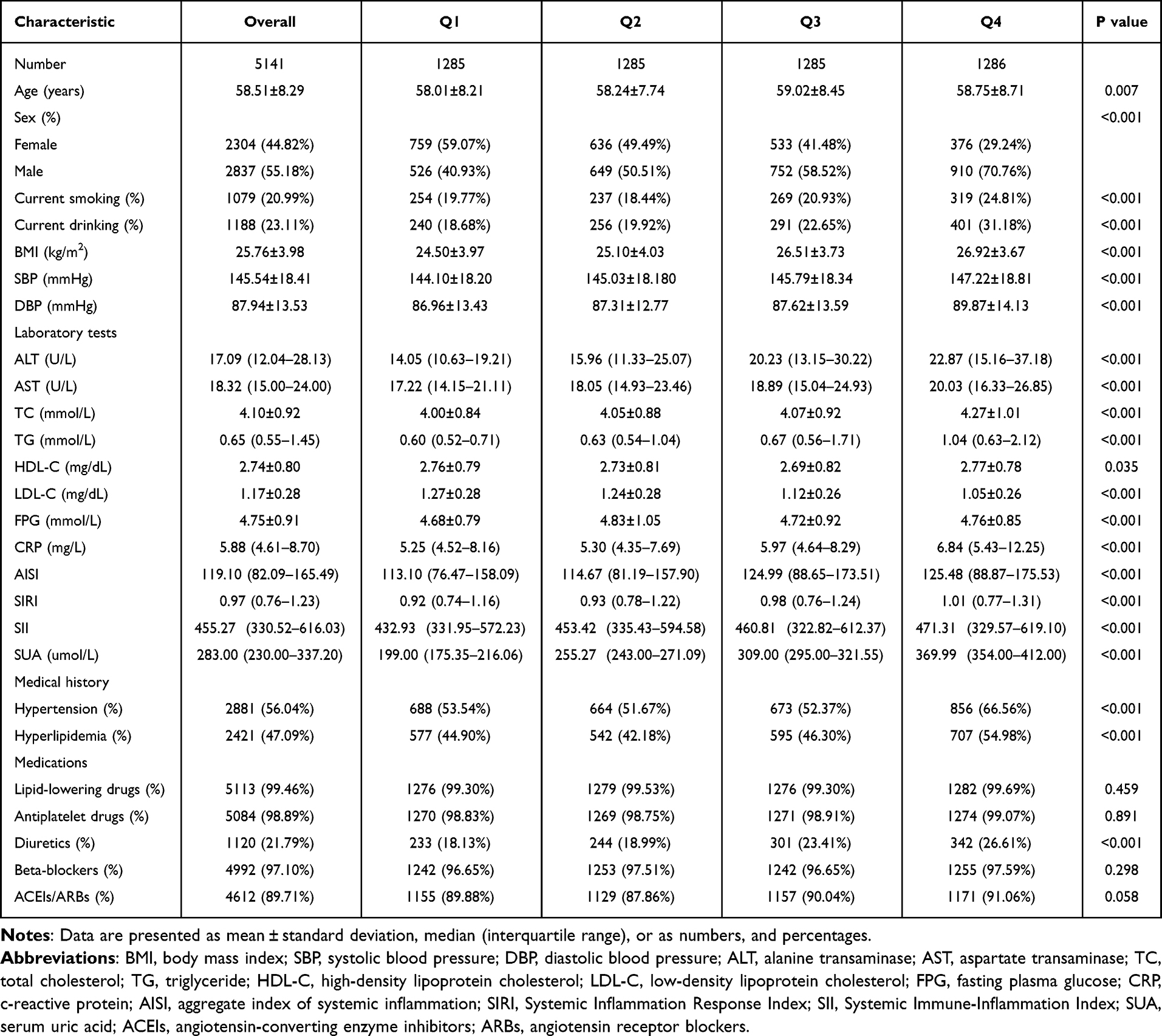 |
Table 1 Baseline Characteristics of the Study Participants |
Compared to the lower-SUA quartiles, participants in the higher SUA quartile demonstrated several distinct clinical and demographic features. These patients tended to be older and were more frequently male. They also reported higher rates of smoking and alcohol consumption. Additionally, this group exhibited elevated body mass index (BMI) and BP. In terms of laboratory test results, the higher SUA group had elevated liver enzyme levels, as well as higher levels of blood lipids, TC, TG, and LDL-C. Furthermore, their FPG, CRP, and SUA levels were significantly higher. In terms of medical history and medication use, a greater proportion had hypertension and hyperlipidemia, and diuretic use was more common. More importantly, the prevalence of diabetes among the four groups showed a stepwise increase, rising progressively from Q1 to Q4 (Figure 2).
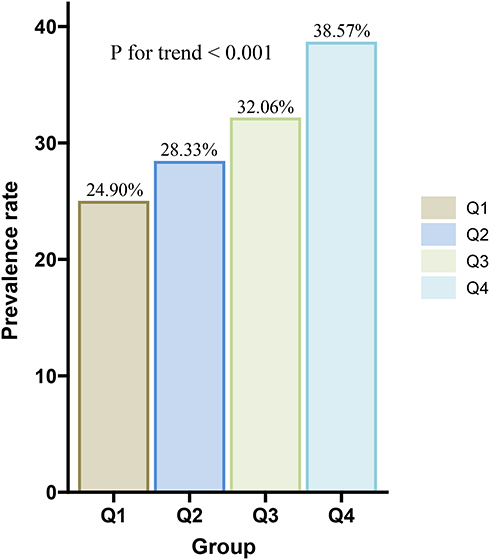 |
Figure 2 Prevalence rates of diabetes among the four groups of people. |
SUA and New-Onset Diabetes Risk in CHD Patients
To evaluate the incidence of diabetes across different SUA groups, we calculated the incidence rate per 100 person-years. The results demonstrated a gradual increase in diabetes incidence with rising SUA levels, with the highest incidence observed in the Q4 group (highest SUA quartile) (Figure 3).
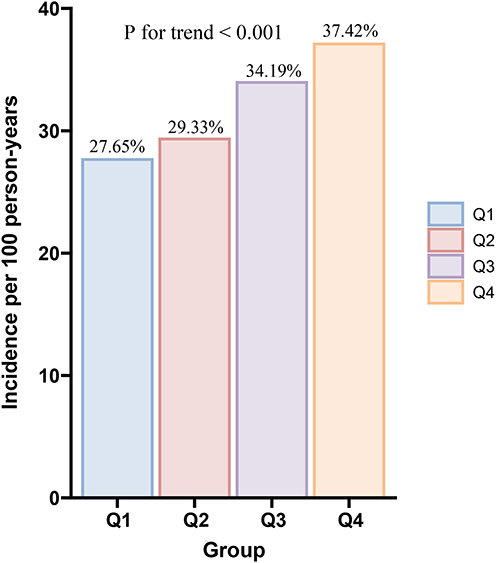 |
Figure 3 Incidence of diabetes per 100 person-years among the four groups. |
The association between SUA and diabetes risk was evaluated through progressively adjusted Cox regression models. In the unadjusted Model 1, each 10 μmol/L increase in SUA and each standard deviation (SD) increase were associated with a 5.2% and 49.6% increased risk of diabetes, respectively (Table 2). In the fully adjusted Model 5, these associations remained significant, with hazard ratios (HRs) of 1.042 [(95% confidence interval (CI): 1.035–1.049)] and 1.391 (95% CI: 1.319–1.464), respectively (Table 2). When analyzing SUA as a categorical variable by quartiles, the Q2, Q3, and Q4 groups showed progressively higher risks of diabetes compared with the Q1 group (lowest quartile), with HRs of 1.213 (95% CI: 1.041–1.413), 1.277 (95% CI: 1.098–1.485), and 1.700 (95% CI: 1.463–1.976), respectively (Table 2). The KM cumulative risk curves confirmed these findings, showing a stepwise increase in cumulative diabetes risk across ascending SUA quartiles (Figure 4).
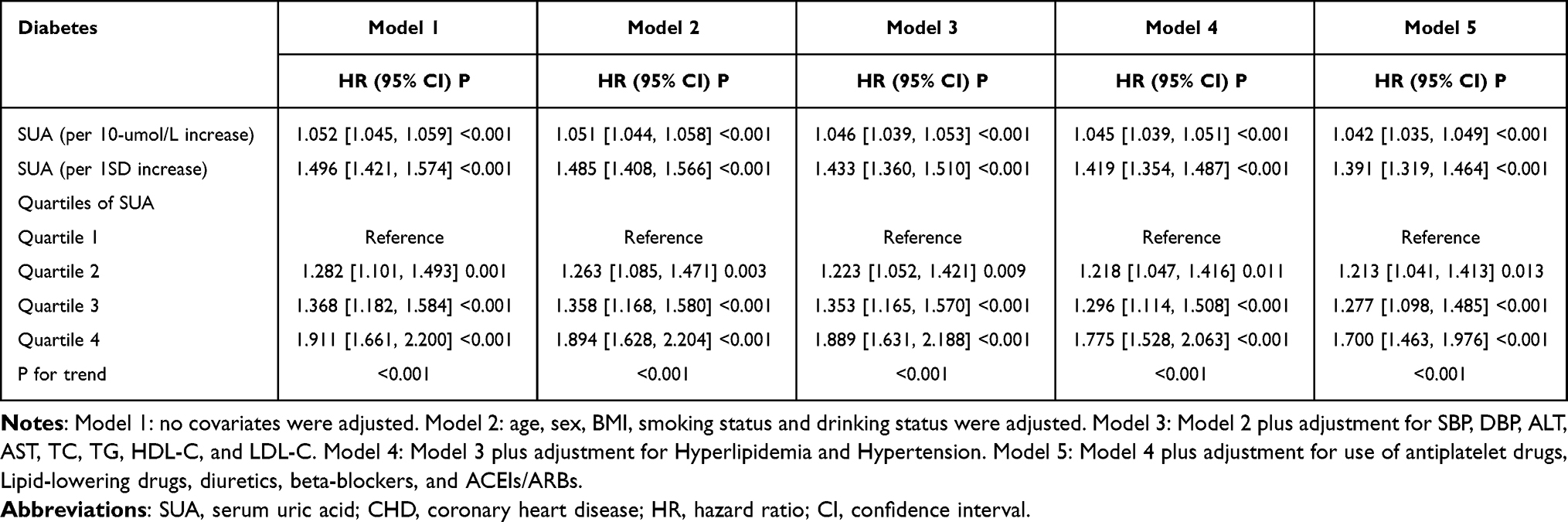 |
Table 2 Relationship Between Between SUA and New-Onset Diabetes in Patients with CHD |
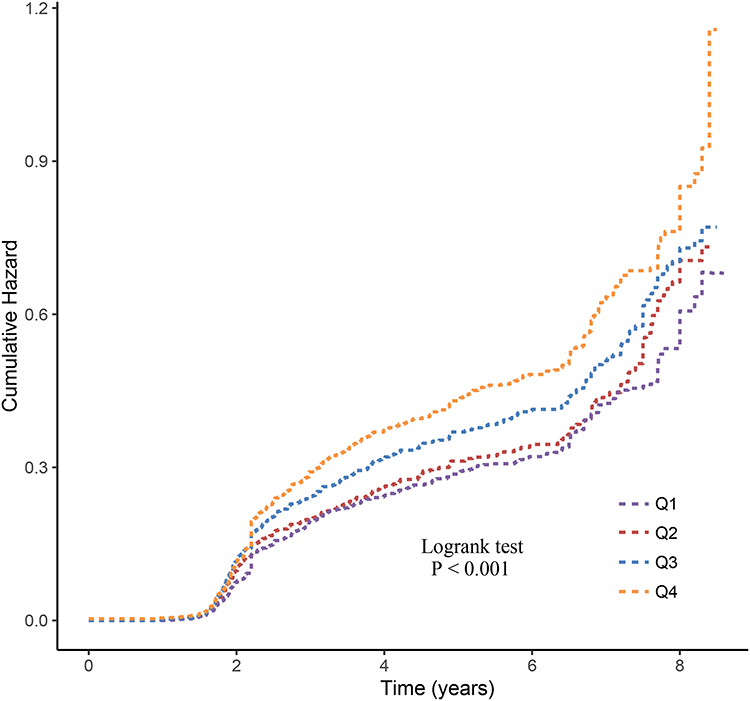 |
Figure 4 Kaplan-Meier cumulative risk curve for new-onset diabetes across the four groups. |
Furthermore, to account for physiological differences between sexes, we conducted sex-stratified analyses. The results indicated that elevated SUA levels, whether analyzed as a continuous or categorical variable, remained associated with a higher risk of diabetes in both males and females (Table 3).
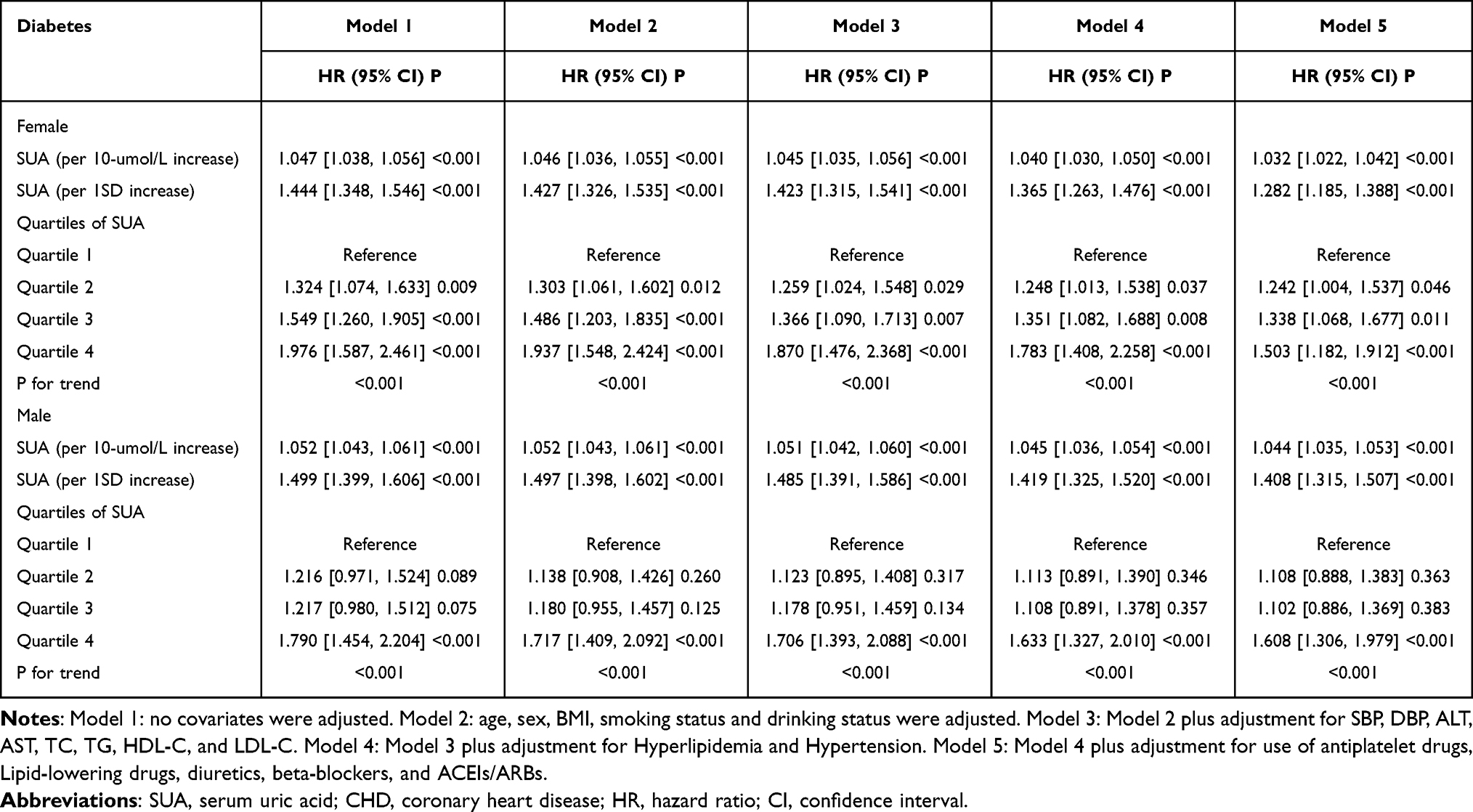 |
Table 3 Association Between SUA and New-Onset Diabetes in Patients with CHD, Stratified by Sex |
Dose-Response Relationship of SUA with New-Onset Diabetes in CHD Patients
Next, a GAM was applied to examine the dose-response relationship between SUA levels and incident diabetes. In the overall population, the risk of new-onset diabetes increased continuously with rising SUA levels, with a more pronounced increase observed when SUA exceeded 346.4 μmol/L (Figure 5 and Table 4). Specifically, among participants with SUA levels ≤ 346.4 μmol/L, each 10 μmol/L increase and each SD increase in SUA were associated with a 2.6% and 22.8% higher risk of diabetes, respectively (Table 4). In contrast, among those with SUA levels > 346.4 μmol/L, the corresponding increases in risk were significantly greater, reaching 7.7% and 80.1%, respectively (Table 4). Similar nonlinear patterns were observed in sex-stratified analyses (Figure 6 and Table 5). Among females, the inflection point was identified at 345.0 μmol/L, while among males, it was identified at 350.5 μmol/L (Figure 6 and Table 5). In both sexes, the association between elevated SUA and diabetes risk intensified significantly once SUA exceeded these respective thresholds (Table 5).
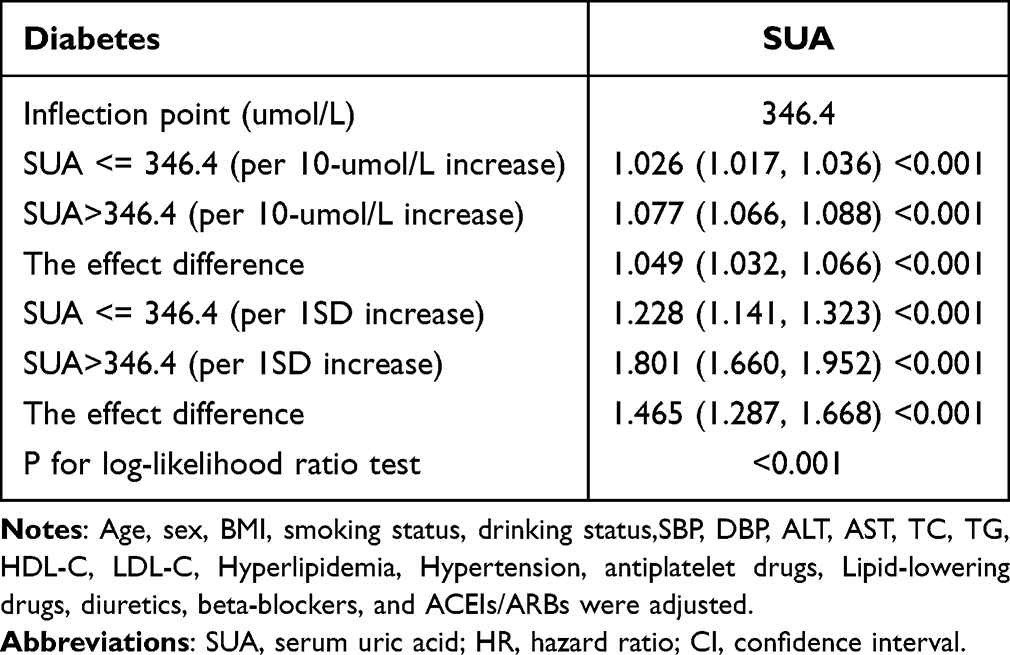 |
Table 4 Association Between SUA and Risk of New-Onset Diabetes Based on Threshold Grouping |
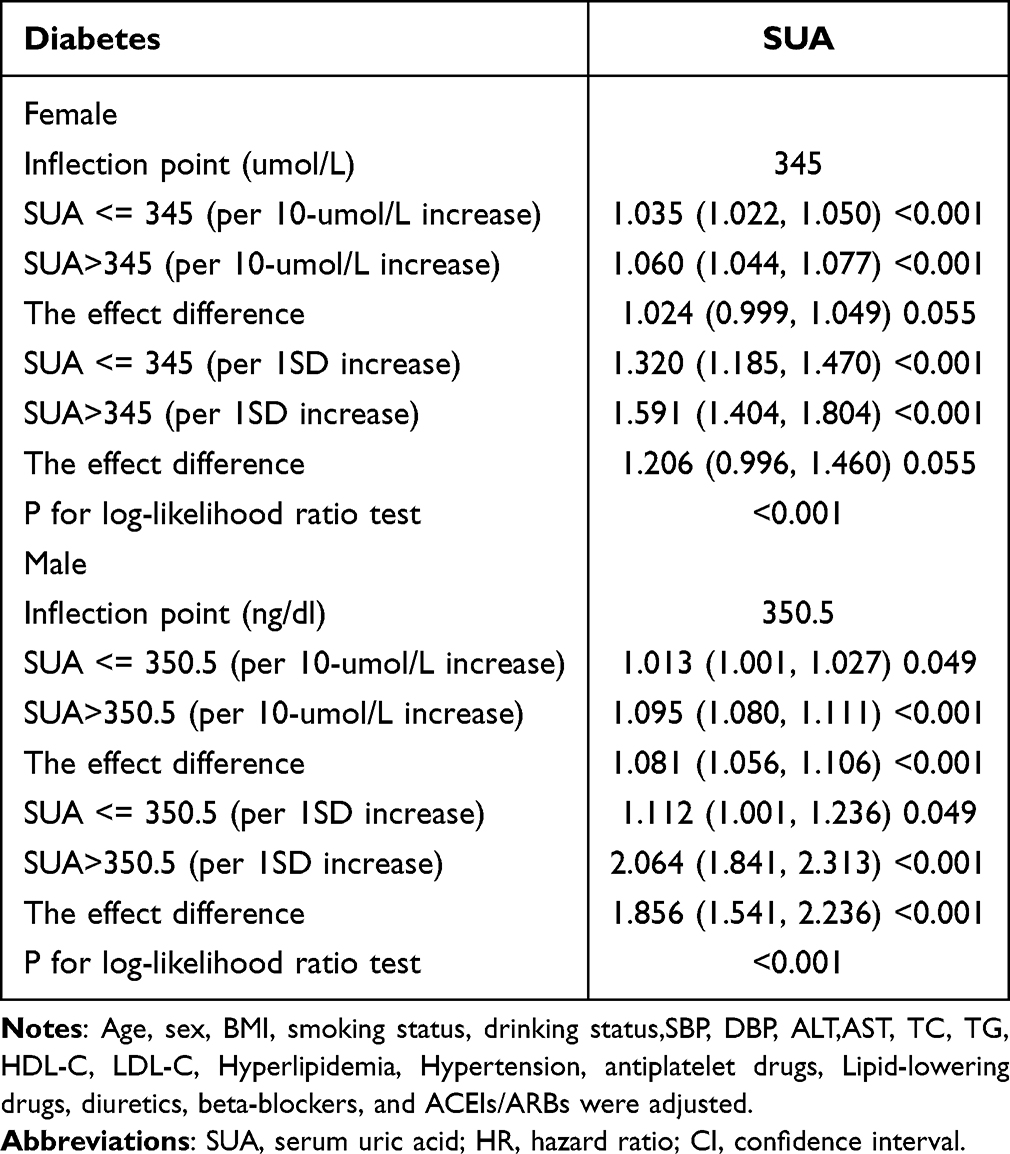 |
Table 5 Association Between SUA and Risk of New-Onset Diabetes According to Sex-Specific Threshold Groups |
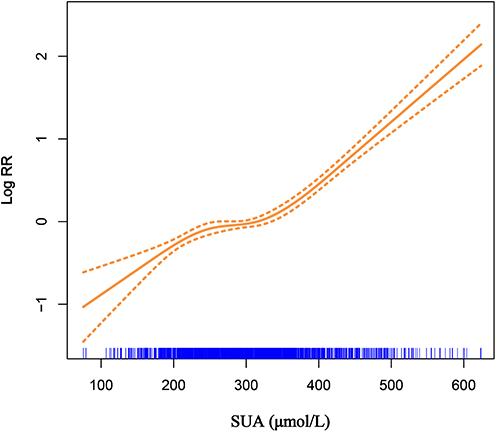 |
Figure 5 Dose-response relationship between SUA and new-onset diabetes risk in patients with CHD Solid line represents the fitted curve between the variables. The area between the dashed lines indicates the 95% confidence interval of the fitted result. |
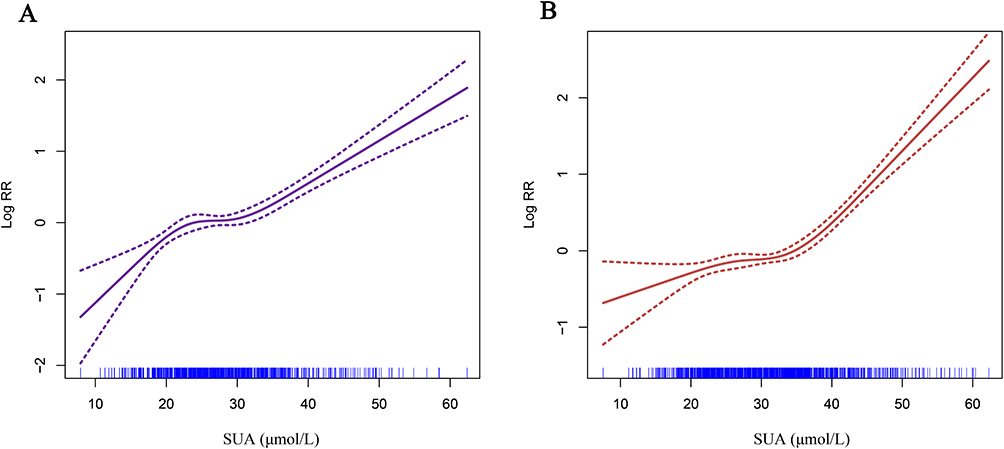 |
Figure 6 Dose-response relationship between SUA and new-onset diabetes risk in patients with CHD, stratified by sex (A), Female; (B), Male Solid line represents the fitted curve between the variables. The area between the dashed lines indicates the 95% confidence interval of the fitted result. |
Subgroup Analysis
To assess the potential impact of baseline characteristics, comorbidities, and medication use, we conducted subgroup analyses (Table 6 and Figure 7).
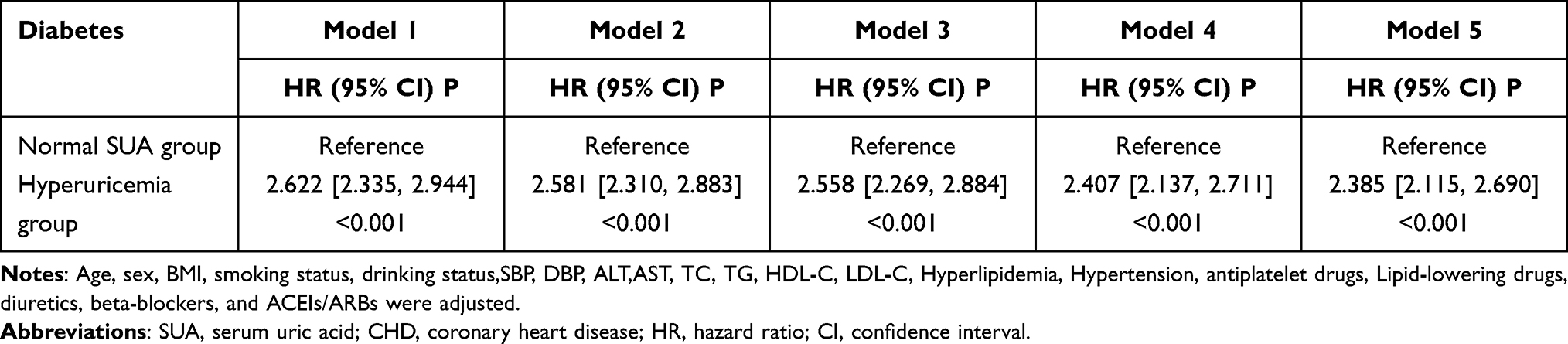 |
Table 6 Association Between Hyperuricemia and New-Onset Diabetes Risk in Patients with CHD |
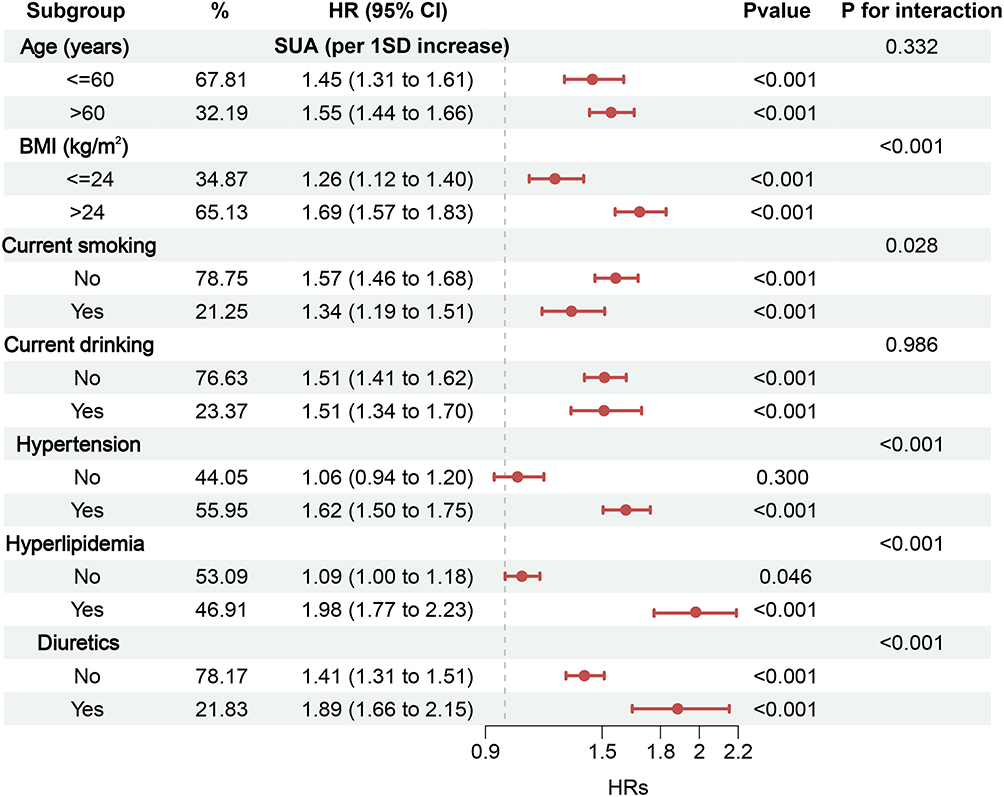 |
Figure 7 Association between SUA and new-onset diabetes across various stratified analyses. |
First, participants were first classified as having hyperuricemia or normal SUA levels based on clinical criteria. The hyperuricemia group exhibited a significantly higher diabetes risk (HR = 2.385, 95% CI: 2.115–2.690) than the normal-SUA group (Table 6). Further stratification by age, BMI, smoking status, alcohol consumption, hypertension, hyperlipidemia, and diuretic use consistently demonstrated a positive association between elevated SUA and diabetes risk across most subgroups (Figure 7). Notably, this association appeared stronger in participants with BMI > 24 kg/m2, non-smokers, and those with hypertension, hyperlipidemia, or diuretic use (Figure 7). These results suggest that such populations may be more vulnerable to SUA-associated diabetes risk, highlighting the importance of monitoring and maintaining lower SUA levels in these groups for diabetes prevention.
Predictive Performance of SUA for New-Onset Diabetes
To evaluate the predictive ability and clinical value of SUA for new-onset diabetes, a series of comparative analyses were conducted. First, incremental predictive performance analysis showed that adding SUA to the basic model (Model 5) significantly improved risk stratification. Specifically, the IDI and NRI increased by 0.003 (95% CI: 0.001–0.005) and 0.033 (95% CI: 0.017–0.081), respectively (Table 7). Meanwhile, the C-index improved from 0.645 to 0.663, with an increase of 0.018 after incorporating SUA (Table 7). To further assess SUA’s relative importance compared to other variables in predicting diabetes risk, variable importance ranking was performed using the Boruta algorithm. The results indicated that SUA was more important in predicting diabetes risk than traditional predictors (Figure 8).
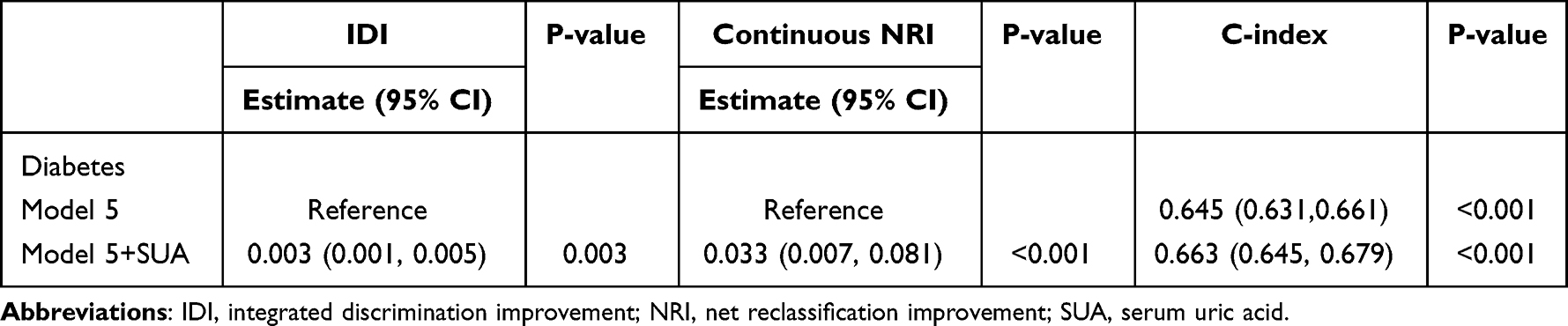 |
Table 7 Incremental Predictive Value of SUA for New-Onset Diabetes |
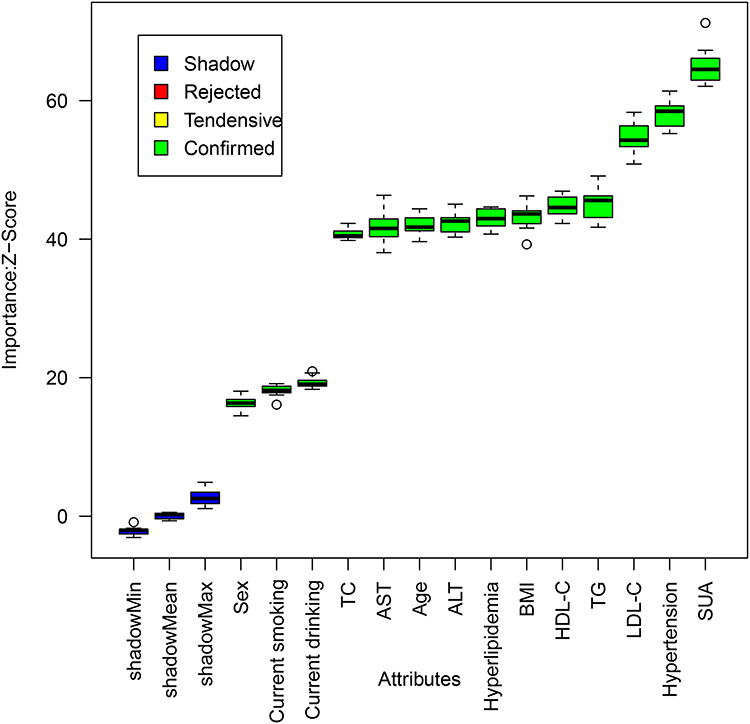 |
Figure 8 Variable importance ranking for predicting new-onset diabetes based on the Boruta algorithm. |
Collectively, the results indicate that SUA serves as an independent predictor for incident diabetes in CHD patients, underscoring its potential clinical utility.
Mediation Effect Between SUA and Diabetes
Mediation analyses were performed to explore potential mechanisms linking elevated SUA to incident diabetes. According to the basic premise of mediation analysis, a mediating variable must show statistically significant associations with both the exposure factor (SUA) and the outcome (diabetes) to be considered valid.
Results showed that CRP, as an indicator of inflammatory status, significantly mediated the SUA–diabetes association, accounting for 32.27% of the effect (P < 0.001) (Figure 9). Given that CRP may not fully capture systemic inflammation and immune activity, we further evaluated the mediating roles of novel immune-inflammatory markers: the aggregate index of systemic inflammation (AISI), systemic inflammatory response index (SIRI), and systemic immune-inflammation index (SII). The results showed that all three markers also exhibited significant mediating effects, with mediation proportions of 12.97% (P < 0.001), 5.82% (P = 0.020), and 3.68% (P = 0.025), respectively (Figure 9).
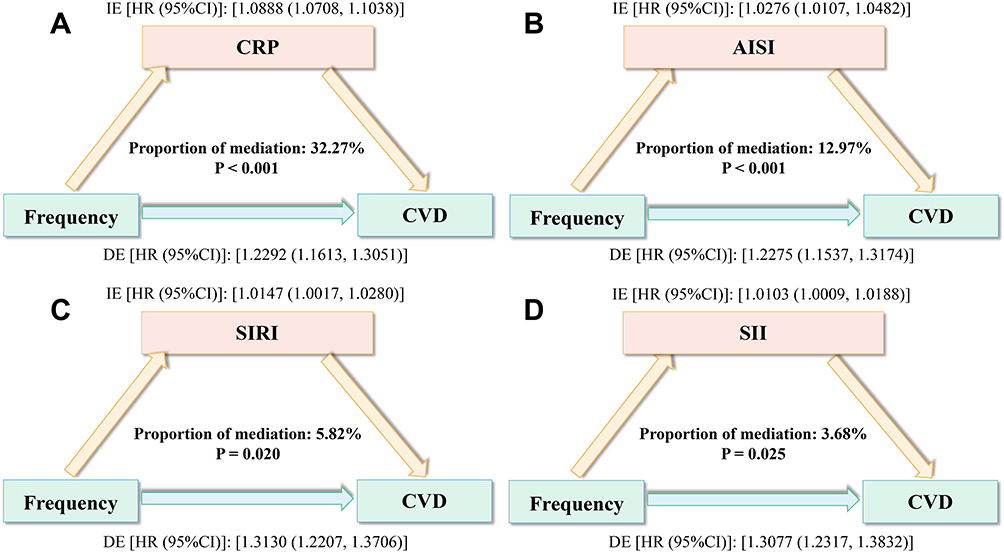 |
Figure 9 Mediation analysis of the association between SUA and new-onset diabetes (A), CRP; (B), AISI; (C), SIRI; (D),SII. |
In conclusion, this study suggests that chronic hyperuricemia may activate inflammatory responses and immune reactions in the body, and these inflammatory and immune states play a critical mediating role in the development of diabetes induced by SUA. These findings provide important clues and research directions for further elucidating the pathological mechanisms linking SUA to diabetes.
Discussion
Although SUA is a key end product of purine metabolism, its relationship with diabetes has often been overlooked. This large, multicenter cohort study is the first to establish a clear and significant link between SUA levels and incident diabetes in patients with CHD. The results show a clear correlation between elevated SUA and increased diabetes risk, particularly when SUA exceeded 345 μmol/L in women and 350.5 μmol/L in men. Our findings indicate that SUA is a critical risk factor for diabetes in CHD patients, especially in those with a BMI > 24 kg/m2, non-smokers, and those with hypertension, hyperlipidemia, or diuretic use. Furthermore, mediation analysis identified inflammatory status as a significant mediator of the SUA–diabetes association, offering mechanistic insight into this relationship. In conclusion, this study provides a new perspective on preventing and managing diabetes in CHD patients, with important clinical implications for improving prognosis and guiding personalized metabolic management strategies.
Diabetes is a widespread chronic systemic metabolic condition that involves multiple organ systems and can lead to extensive tissue damage.1,37–39 It not only causes vascular endothelial injury, laying a critical pathological foundation for the development of atherosclerosis, but also contributes to dyslipidemia and promotes the formation of arterial plaques.38–40 Additionally, diabetes-induced insulin resistance often coexists with a series of metabolic abnormalities, such as hypertension, obesity, and hyperlipidemia.41,42 These factors collectively exacerbate the progression of cardiovascular diseases and significantly increase mortality risk.38,41,42 Patients with CHD already exhibit established vascular damage and luminal stenosis. The coexistence of diabetes in such individuals leads to a synergistic worsening effect, accelerating vascular deterioration, promoting plaque progression, and intensifying luminal obstruction.40,43 Consequently, this not only substantially increases the healthcare burden and impairs quality of life but also further elevates the risk of mortality. Therefore, systematically identifying diabetes risk factors in patients with CHD and implementing proactive interventions to reduce the likelihood of diabetes onset are critical clinical priorities.
In recent years, increasing interest has focused on the role of SUA in diabetes pathogenesis. However, existing evidence is mainly derived from specific populations or limited settings.44–47 For example, a Shanghai-based cohort study of pregnant women identified a significant dose-response relationship between SUA levels and gestational diabetes risk, which strengthened once SUA exceeded 300 µmol/L.46 Another single-center observational study from Fudan University further indicated that elevated SUA before 24 weeks of gestation could predict subsequent gestational diabetes, suggesting a potential intervention window prior to 18 weeks of pregnancy.45 Additionally, research on diabetes complications has suggested that poorly controlled SUA may exacerbate the progression of microvascular complications, such as diabetic retinopathy.47 A study in a Korean adult population also found a synergistic effect between SUA and CRP in increasing diabetes risk, indirectly supporting the hypothesis that SUA influences glucose metabolism through inflammatory pathways.44
However, previous studies have several limitations: they primarily focused on gestational diabetes mellitus, lacked systematic investigation in high-risk cardiovascular populations, and were mainly single-center studies with limited representativeness. They also provided insufficient analysis of gender and subgroup differences and lacked adequate evidence on mechanistic pathways, particularly regarding inflammatory mediation. In contrast, through a large multicenter cohort design, the present study is the first to systematically characterize the dose‑response relationship between SUA and incident diabetes in CHD patients, establishing sex‑specific risk thresholds (>345 µmol/L in women, >350.5 µmol/L in men). Moreover, mediation analysis provides empirical support for the critical role of systemic inflammation as a mediator. Thus, this work not only addresses key gaps in prior research but also offers novel insights for early diabetes prevention and management in the CHD population.
In patients with CHD, hyperuricemia may promote diabetes development through several interconnected pathophysiological pathways. The core pathways are outlined below: First, SUA contributes to insulin resistance and pancreatic β-cell dysfunction.30,48,49 It inhibits insulin signaling in peripheral tissues, reduces the membrane translocation of the glucose transporter GLUT4, and impairs glucose uptake. Additionally, SUA directly damages β-cells, reducing insulin synthesis and secretion.48,49 Second, SUA also promotes chronic inflammation and immune dysregulation.50,51 Through NLRP3 inflammasome activation, it induces the release of pro-inflammatory cytokines including IL-1β, IL-6, and TNF-α, which disrupt insulin signaling and intensify insulin resistance.50,52,53 Consistently, our study found that both CRP and composite inflammatory markers (AISI, SIRI, and SII) exhibited significant mediating effects in the development of diabetes. These findings align well with previous basic research and continue to support the role of inflammation in the development of diabetes in patients with CHD. Furthermore, SUA is associated with oxidative stress and endothelial dysfunction.31,54,55 It enhances reactive oxygen species production and reduces nitric oxide bioavailability, contributing to vascular endothelial damage.54–56 Given the pre-existing vascular injury in CHD, this further aggravates glucose metabolism disorders. Additionally, Diabetes and CHD share multiple common pathophysiological pathways at the cellular level.57 Meanwhile, the sympathetic nervous system plays an indispensable regulatory role in glucose homeostasis in patients with CHD, which may interact synergistically with SUA to increase the risk of diabetes.58 Finally, SUA disrupts adipokine secretion by interfering with normal adipocyte function, decreasing adiponectin levels, increasing leptin resistance, promoting visceral fat accumulation, and amplifying systemic inflammation and metabolic disturbances.59–61 In summary, these mechanisms do not operate in isolation; instead, they interact and synergize, collectively worsening insulin resistance and disrupting glucose homeostasis, ultimately significantly increasing the risk of new-onset diabetes in patients with CHD.
The present study offers several strengths. Its multicenter cohort design and relatively large sample improve the representativeness and generalizability of the findings. By focusing on the high‑risk CHD population, systematic subgroup analyses further identified individuals at heightened risk—such as those with elevated BMI, hypertension, hyperlipidemia, or diuretic use—which is important for targeted screening and early clinical intervention. Additionally, the robustness of the results was confirmed through multiple statistical approaches, and mediation analysis suggests a potential inflammatory pathway underlying the SUA–diabetes association, offering direction for future mechanistic and translational research.
Several limitations should also be noted. First, as an observational study, although temporal associations were observed and major confounders were adjusted, causality between SUA and diabetes cannot be conclusively established. Second, the analysis relied on baseline SUA measurements only; dynamic changes in SUA over follow‑up were not captured. Future studies should examine how SUA variability influences diabetes risk. Third, information on the use of urate-lowering medications during follow-up was not collected, which may influence the interpretation of SUA levels. Fourth, despite adjusting for a range of covariates, unmeasured confounding factors may still exist.
Conclusion
This study provides the first evidence that SUA level is an independent risk factor for incident diabetes in CHD patients, exhibiting a clear dose–response relationship with sex‑specific thresholds. Mediation analysis further indicates a significant role of inflammation in mediating this association. These results underscore the value of integrating SUA monitoring and management into CHD care, offering a new clinical approach for early diabetes prevention and improved patient prognosis. However, as an observational cohort study, causality cannot be definitively established. Future prospective mechanistic or interventional studies are necessary to confirm and further advance these findings.
Institutional Review Board Statement
The entire process of the study followed the Helsinki Declaration and obtained approval from the ethics committees of the five hospitals involved: Changzhi People’s Hospital (CZX20180213), Sichuan Provincial People’s Hospital (CRC2024-0512), the Sixth Affiliated Hospital of Kunming Medical University (XKY20200806), Xinxiang Central Hospital (NXCH20230911), and Yunyang County People’s Hospital (Yy20200419). All participants provided written informed consent prior to enrollment.
Data Sharing Statement
The data analyzed in this study are available from the corresponding author upon reasonable request.
Author Contributions
Shuaiwei Song: Conceptualization, Methodology, Investigation, Data Curation, Formal Analysis, Writing – Original Draft, Writing – review and editing. Xintian Cai: Methodology, Data Curation, Investigation, Formal Analysis, Validation Writing – Original Draft. Tuo Xu: Methodology, Writing – Review and Editing, Investigation, Visualization. Penghui Cui: Methodology, Investigation, Data Curation, Formal Analysis, Writing – review and editing. Ziliang Zou: Data Curation, Investigation, Writing – review and editing. Junjie Zhao: Methodology, Formal Analysis, Investigation, Supervision, Writing – review and editing. Yazhe Liu: Methodology, Data Curation, Writing – review and editing. Kaiyu Wang: Conceptualization, Methodology, Investigation, Supervision, Data Curation, Writing – Original Draft, Writing – review and editing. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that no funding was received for this study.
Disclosure
The authors declare that there are no conflicts of interest in this study.
References
1. Vijan S. Type 2 diabetes. Ann Intern Med. 2015;163(4):322. doi:10.7326/L15-5122-2
2. Brody H. Diabetes. Nature. 2012;485(7398):S1. doi:10.1038/485s1a
3. Rav Acha M, Glikson M. Type 2 diabetes mellitus association with atrioventricular block. Eur Heart J. 2023;44(9):762–17. doi:10.1093/eurheartj/ehac755
4. Chang E, Abe J-I. Kinase-SUMO networks in diabetes-mediated cardiovascular disease. Metabolism. 2016;65(5):623–633. doi:10.1016/j.metabol.2016.01.007
5. Anders H-J, Huber TB, Isermann B, et al. CKD in diabetes: diabetic kidney disease versus nondiabetic kidney disease. Nat Rev Nephrol. 2018;14(6):361–377. doi:10.1038/s41581-018-0001-y
6. Eid SA, Rumora AE, Beirowski B, et al. New perspectives in diabetic neuropathy. Neuron. 2023;111(17):2623–2641. doi:10.1016/j.neuron.2023.05.003
7. Wu Y, Fu R, Lei C, et al. Estimates of type 2 diabetes mellitus burden attributable to particulate matter pollution and its 30-year change patterns: a systematic analysis of data from the global burden of disease study 2019. Front Endocrinol. 2021;12:689079. doi:10.3389/fendo.2021.689079
8. Schmidt AM. Highlighting diabetes mellitus: the epidemic continues. Arterioscler Thromb Vasc Biol. 2018;38(1):e1–e8. doi:10.1161/ATVBAHA.117.310221
9. Dalen JE, Alpert JS, Goldberg RJ, et al. The epidemic of the 20th century: coronary heart disease. Am J Med. 2014;127(9):807–812. doi:10.1016/j.amjmed.2014.04.015
10. Goodarzi MO, Rotter JI. Genetics insights in the relationship between type 2 diabetes and coronary heart disease. Circ Res. 2020;126(11):1526–1548. doi:10.1161/CIRCRESAHA.119.316065
11. Zhao W, Rasheed A, Tikkanen E, et al. Identification of new susceptibility loci for type 2 diabetes and shared etiological pathways with coronary heart disease. Nat Genet. 2017;49(10):1450–1457. doi:10.1038/ng.3943
12. Beckman JA, Paneni F, Cosentino F, et al. Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: part II. Eur Heart J. 2013;34(31):2444–2452. doi:10.1093/eurheartj/eht142
13. Beckman JA, Creager MA. Vascular complications of diabetes. Circ Res. 2016;118(11):1771–1785. doi:10.1161/CIRCRESAHA.115.306884
14. Kadowaki S, Okamura T, Hozawa A, et al. Relationship of elevated casual blood glucose level with coronary heart disease, cardiovascular disease and all-cause mortality in a representative sample of the Japanese population. NIPPON DATA80. Diabetologia. 2008;51(4):575–582. doi:10.1007/s00125-007-0915-6
15. Matsumoto K, Sera Y, Abe Y, et al. Inflammation and insulin resistance are independently related to all-cause of death and cardiovascular events in Japanese patients with type 2 diabetes mellitus. Atherosclerosis. 2003;169(2):317–321. doi:10.1016/s0021-9150(03)00198-9
16. Frye RL, August P, BARI 2D Study Group. A randomized trial of therapies for type 2 diabetes and coronary artery disease. N Engl J Med. 2009;360(24):2503–2515. doi:10.1056/NEJMoa0805796
17. Ulbricht TL, Southgate DA. Coronary heart disease: seven dietary factors. Lancet. 1991;338(8773):985–992. doi:10.1016/0140-6736(91)91846-m
18. Jensen JC, Dardari ZA, Blaha MJ, et al. Association of body mass index with coronary artery calcium and subsequent cardiovascular mortality: the coronary artery calcium consortium. Circ Cardiovasc Imaging. 2020;13(7):e009495. doi:10.1161/CIRCIMAGING.119.009495
19. Lv J, Pan C, Cai Y, et al. Plasma metabolomics reveals the shared and distinct metabolic disturbances associated with cardiovascular events in coronary artery disease. Nat Commun. 2024;15(1):5729. doi:10.1038/s41467-024-50125-2
20. Danesh J, Whincup P, Walker M, et al. Low grade inflammation and coronary heart disease: prospective study and updated meta-analyses. BMJ. 2000;321(7255):199–204. doi:10.1136/bmj.321.7255.199
21. Xia X, Luo Q, Li B, et al. Serum uric acid and mortality in chronic kidney disease: a systematic review and meta-analysis. Metabolism. 2016;65(9):1326–1341. doi:10.1016/j.metabol.2016.05.009
22. Song S, Cai X, Hu J, et al. Serum uric acid and bone health in middle-aged and elderly hypertensive patients: a potential U-shaped association and implications for future fracture risk. Metabolites. 2025;15(1):15. doi:10.3390/metabo15010015
23. Song S, Cai X, Hu J, et al. Plasma aldosterone concentrations elevation in hypertensive patients: the dual impact on hyperuricemia and gout. Front Endocrinol. 2024;15:1424207. doi:10.3389/fendo.2024.1424207
24. Li N, Li Y, Cui L, et al. Uric acid and risk of incident heart failure in individuals with cardiovascular disease. Nutr Metab Cardiovasc Dis. 2024;34(12):2763–2770. doi:10.1016/j.numecd.2024.09.012
25. Borghi C, Agnoletti D, Cicero AFG, et al. Uric acid and hypertension: a review of evidence and future perspectives for the management of cardiovascular risk. Hypertension. 2022;79(9):1927–1936. doi:10.1161/HYPERTENSIONAHA.122.17956
26. Ahmadnezhad M, Arefhosseini SR, Parizadeh MR, et al. Association between serum uric acid, high sensitive C-reactive protein and pro-oxidant-antioxidant balance in patients with metabolic syndrome. Biofactors. 2018;44(3):263–271. doi:10.1002/biof.1424
27. Du L, Zong Y, Li H, et al. Hyperuricemia and its related diseases: mechanisms and advances in therapy. Signal Transduct Target Ther. 2024;9(1):212. doi:10.1038/s41392-024-01916-y
28. Adnan E, Rahman IA, Faridin HP. Relationship between insulin resistance, metabolic syndrome components and serum uric acid. Diabetes Metab Syndr. 2019;13(3):2158–2162. doi:10.1016/j.dsx.2019.04.001
29. Zhang Q, Ma X, Xing J, et al. Serum uric acid is a mediator of the association between obesity and incident nonalcoholic fatty liver disease: a prospective cohort study. Front Endocrinol. 2021;12:657856. doi:10.3389/fendo.2021.657856
30. McCormick N, O’Connor MJ, Yokose C, et al. Assessing the causal relationships between insulin resistance and hyperuricemia and gout using bidirectional mendelian randomization. Arthritis Rheumatol. 2021;73(11):2096–2104. doi:10.1002/art.41779
31. Taher R, Sara JD, Prasad M, et al. Elevated serum uric acid is associated with peripheral endothelial dysfunction in women. Atherosclerosis. 2019;290:37–43. doi:10.1016/j.atherosclerosis.2019.07.013
32. Prasad M, Matteson EL, Herrmann J, et al. Uric acid is associated with inflammation, coronary microvascular dysfunction, and adverse outcomes in postmenopausal women. Hypertension. 2017;69(2):236–242. doi:10.1161/HYPERTENSIONAHA.116.08436
33. Wheeler JG, Juzwishin KDM, Eiriksdottir G, et al. Serum uric acid and coronary heart disease in 9,458 incident cases and 155,084 controls: prospective study and meta-analysis. PLoS Med. 2005;2(3):e76. doi:10.1371/journal.pmed.0020076
34. Harreiter J, Roden M. Diabetes mellitus: definition, classification, diagnosis, screening and prevention (update 2023). Wien Klin Wochenschr. 2023;135(Suppl S1):7–17. doi:10.1007/s00508-022-02122-y German.
35. Davidson KW, Barry MJ, Mangione CM, et al; US Preventive Services Task Force. Screening for prediabetes and type 2 diabetes: US preventive services task force recommendation statement. JAMA. 2021;326(8):736–743. doi:10.1001/jama.2021.12531
36. Keen H, Jarrett RJ, Alberti KG. Diabetes mellitus: a new look at diagnostic criteria. Diabetologia. 1979;16(5):283–285. doi:10.1007/BF01223616
37. Mitchell JD. Personalizing risk assessment in diabetes mellitus and metabolic syndrome. JACC Cardiovasc Imaging. 2021;14(1):230–232. doi:10.1016/j.jcmg.2020.11.002
38. Wong ND, Sattar N. Cardiovascular risk in diabetes mellitus: epidemiology, assessment and prevention. Nat Rev Cardiol. 2023;20(10):685–695. doi:10.1038/s41569-023-00877-z
39. Khan AW, Jandeleit-Dahm KAM. Atherosclerosis in diabetes mellitus: novel mechanisms and mechanism-based therapeutic approaches. Nat Rev Cardiol. 2025;22(7):482–496. doi:10.1038/s41569-024-01115-w
40. Bartoli-Leonard F, Wilkinson FL, Schiro A, et al. Loss of SIRT1 in diabetes accelerates DNA damage-induced vascular calcification. Cardiovasc Res. 2021;117(3):836–849. doi:10.1093/cvr/cvaa134
41. Accili D, Deng Z, Liu Q. Insulin resistance in type 2 diabetes mellitus. Nat Rev Endocrinol. 2025;21(7):413–426. doi:10.1038/s41574-025-01114-y
42. Jia G, Sowers JR. Hypertension in diabetes: an update of basic mechanisms and clinical disease. Hypertension. 2021;78(5):1197–1205. doi:10.1161/HYPERTENSIONAHA.121.17981
43. Mondesir FL, Brown TM, Muntner P, et al. Diabetes, diabetes severity, and coronary heart disease risk equivalence: rEasons for geographic and racial differences in stroke (REGARDS). Am Heart J. 2016;181:43–51. doi:10.1016/j.ahj.2016.08.002
44. Lee KW, Shin D. Concurrent presence of high serum uric acid and inflammation is associated with increased incidence of type 2 diabetes mellitus in Korean adult population. Sci Rep. 2022;12(1):11000. doi:10.1038/s41598-022-15176-9
45. Yue C, Ying C, Li X. Elevated serum uric acid is associated with gestational diabetes mellitus: an observational cohort study. J Clin Endocrinol Metab. 2023;108(7):e480–e486. doi:10.1210/clinem/dgac760
46. Zhao Y, Zhao Y, Fan K, et al. Serum uric acid in early pregnancy and risk of gestational diabetes mellitus: a cohort study of 85,609 pregnant women. Diabetes Metab. 2022;48(3):101293. doi:10.1016/j.diabet.2021.101293
47. Zhu Q, Wang H, Qu Y, et al. Association between long-term serum uric acid variability and diabetic retinopathy: a prospective study in patients with Type 1 and Type 2 diabetes. Diabet Res Clin Pract. 2025;226:112306. doi:10.1016/j.diabres.2025.112306
48. Li M, Gu L, Yang J, et al. Serum uric acid to creatinine ratio correlates with β-cell function in type 2 diabetes. Diabetes Metab Res Rev. 2018;34(5):e3001. doi:10.1002/dmrr.3001
49. Volpe A, Ye C, Hanley AJ, et al. Changes over time in uric acid in relation to changes in insulin sensitivity, beta-cell function, and glycemia. J Clin Endocrinol Metab. 2020;105(3):e651–9. doi:10.1210/clinem/dgz199
50. Shen S, He F, Cheng C, et al. Uric acid aggravates myocardial ischemia–reperfusion injury via ROS/NLRP3 pyroptosis pathway. Biomed Pharmacother. 2021;133:110990. doi:10.1016/j.biopha.2020.110990
51. Li D, Yuan S, Deng Y, et al. The dysregulation of immune cells induced by uric acid: mechanisms of inflammation associated with hyperuricemia and its complications. Front Immunol. 2023;14:1282890. doi:10.3389/fimmu.2023.1282890
52. Feng L, Chen C, Xiong X, et al. PS-MPs promotes the progression of inflammation and fibrosis in diabetic nephropathy through NLRP3/Caspase-1 and TGF-β1/Smad2/3 signaling pathways. Ecotoxicol Environ Saf. 2024;273:116102. doi:10.1016/j.ecoenv.2024.116102
53. Vandanmagsar B, Youm Y-H, Ravussin A, et al. The NLRP3 inflammasome instigates obesity-induced inflammation and insulin resistance. Nat Med. 2011;17(2):179–188. doi:10.1038/nm.2279
54. Zhao H, Lv J, Chen B, et al. RAGE deficiency obstructs high uric acid-induced oxidative stress and inflammatory response. Int Immunopharmacol. 2025;151:114316. doi:10.1016/j.intimp.2025.114316
55. Strazzullo P, Puig JG. Uric acid and oxidative stress: relative impact on cardiovascular risk? Nutr Metab Cardiovasc Dis. 2007;17(6):409–414. doi:10.1016/j.numecd.2007.02.011
56. Han F, Yu C, Hu F, et al. Association between serum uric acid levels and peripheral artery disease in Chinese adults with hypertension. Front Endocrinol. 2023;14:1197628. doi:10.3389/fendo.2023.1197628
57. Ktenopoulos N, Anagnostopoulou L, Apostolos A, et al. Cellular and molecular pathways in diabetes-associated heart failure: emerging mechanistic insights and therapeutic opportunities. Curr Issues Mol Biol. 2025;47(11):886. doi:10.3390/cimb47110886
58. Koutra E, Dimitriadis K, Pyrpyris N, et al. Unravelling the effect of renal denervation on glucose homeostasis: more questions than answers? Acta Diabetol. 2023;61(3):267–280. doi:10.1007/s00592-023-02208-7
59. Su M, Sun L, Li W, et al. Metformin alleviates hyperuricaemia-induced serum FFA elevation and insulin resistance by inhibiting adipocyte hypertrophy and reversing suppressed white adipose tissue beiging. Clin Sci. 2020;134(12):1537–1553. doi:10.1042/CS20200580
60. Yang L, Yin R, Shan Z, et al. Adipocyte-secreted ANGPTL2 promotes hyperuricemia through inhibiting AKT/ABCG2 signaling. Free Radic Biol Med. 2025;233:209–225. doi:10.1016/j.freeradbiomed.2025.03.048
61. D’Elia L, Giaquinto A, Cappuccio FP, et al. Circulating leptin is associated with serum uric acid level and its tubular reabsorption in a sample of adult middle-aged men. J Endocrinol Invest. 2020;43(5):587–593. doi:10.1007/s40618-019-01140-4
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Relationship Between Four Non-Insulin-Based Indexes of Insulin Resistance and Serum Uric Acid in Patients with Type 2 Diabetes: A Cross-Sectional Study
Han R, Zhang Y, Jiang X
Diabetes, Metabolic Syndrome and Obesity 2022, 15:1461-1471
Published Date: 9 May 2022
Platelet-Activating Factor Promotes the Development of Non-Alcoholic Fatty Liver Disease
Yin H, Shi A, Wu J
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2003-2030
Published Date: 8 July 2022
Gender Differences in Relation to Body Composition, Insulin Resistance, and Islet Beta Cell Function in Newly Diagnosed Diabetic or Pre-Diabetic Patients
Ma M, Jiang T, Wen Z, Zhang D, Xiu L
Diabetes, Metabolic Syndrome and Obesity 2023, 16:723-732
Published Date: 10 March 2023
The Association Between Sarcopenia and Diabetes: From Pathophysiology Mechanism to Therapeutic Strategy
Chen H, Huang X, Dong M, Wen S, Zhou L, Yuan X
Diabetes, Metabolic Syndrome and Obesity 2023, 16:1541-1554
Published Date: 30 May 2023
Obesity-Related Insulin Resistance Indices and CKD Risk in Patients with Diabetes and Coronary Heart Disease: A Multicenter Cohort Analysis
Zhang J, Zhang Z, He Y, Liu S, Zhao J, Ge X
Diabetes, Metabolic Syndrome and Obesity 2026, 19:610602
Published Date: 26 June 2026