Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Impact of Pathological Grades of Metabolic Dysfunction-Associated Steatotic Liver Disease on Weight Loss Following Laparoscopic Sleeve Gastrectomy
Authors Qu YF, Wang K, Li Y, Cheng YG, Hu SY ![]() , Zhong MW
, Zhong MW
Received 2 March 2025
Accepted for publication 10 July 2025
Published 29 July 2025 Volume 2025:18 Pages 2547—2560
DOI https://doi.org/10.2147/DMSO.S523771
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Liang Wang
Yun-Fei Qu,1,* Kang Wang,1,* Yue Li,2 Yu-Gang Cheng,1,3 San-Yuan Hu,1,3 Ming-Wei Zhong1,3
1Department of General Surgery, The First Affiliated Hospital of Shandong First Medical University & Shandong Provincial Qianfoshan Hospital, Jinan, Shandong, 250000, People’s Republic of China; 2Department of General Surgery, Shandong Provincial Qianfoshan Hospital, Cheeloo College of Medicine Shandong University, Jinan, Shandong, 250000, People’s Republic of China; 3Medical Center for Digestive Diseases, The First Affiliated Hospital of Shandong First Medical University & Shandong Provincial Qianfoshan Hospital, Jinan, Shandong, 250000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: San-Yuan Hu, Email [email protected] Ming-Wei Zhong, Email [email protected]
Purpose: The impact of hepatic steatosis severity on postoperative weight loss outcomes remains unclear. This study aimed to evaluate the effect of fatty liver severity on percentage of excess weight loss (%EWL) in patients undergoing laparoscopic sleeve gastrectomy (LSG).
Methods: This retrospective cohort study included 226 patients with obesity who underwent LSG. Baseline data included liver biopsy grade (mild, moderate, or severe), body mass index (BMI), liver function, and metabolic parameters. Postoperative outcomes were assessed at 1, 3, 6, and 12 months. Statistical methods included the Pearson and Spearman correlations, chi-square test, Kruskal–Wallis test, general linear models, Kaplan–Meier analysis, and multivariate regression to identify the predictors of weight loss and cumulative rates of achieving 50% EWL and to plot the cumulative incidence curve.
Results: Baseline BMI, homeostasis model assessment for insulin resistance, free fatty acids, and A1C levels were significantly associated with steatosis severity (P < 0.05). Severe metabolic dysfunction-associated steatotic liver disease (MASLD) was associated with a lower %EWL at 1, 3, 6, and 12 months (1 month %EWL: 32.34% vs 38.59% in the mild group; P < 0.05). The Kaplan–Meier analysis showed delayed achievement of 50% EWL in the severe group (P < 0.05). Multivariate regression analysis identified MASLD severity and preoperative BMI as independent predictors of %EWL. General linear models confirmed the significant dynamic effects of MASLD severity on weight loss over time (P < 0.05).
Conclusion: MASLD severity significantly affects postoperative weight loss and delays the achievement of optimal outcomes, especially in the early postoperative period. Preoperative evaluation of liver pathology is essential for optimizing surgical outcomes in patients with obese having MASLD.
Keywords: obesity, fatty liver, bariatric surgery, insulin resistance
Introduction
The prevalence of metabolic dysfunction-associated steatotic liver disease (MASLD) has been steadily increasing worldwide,1,2 particularly in Asia and among Chinese populations,3,4 where the increase in obesity rates is more pronounced.4–6 MASLD is a hepatic condition characterized by excessive fat accumulation in hepatocytes without significant alcohol consumption. MASLD is often accompanied by inflammation and fibrosis, which may progress to cirrhosis and hepatocellular carcinoma.6 In China, the prevalence of MASLD has reached approximately 30%, primarily driven by lifestyle changes and increasing obesity rates, posing a significant public health threat.7,8 Obesity is regarded as the primary driving factor for MASLD, and its pathogenesis involves intricate interactions among hepatic steatosis, oxidative stress, and chronic inflammation. Consequently, weight management is recognized as one of the most crucial therapeutic strategies for addressing MASLD.4,9,10
Although no specific pharmacological treatment for MASLD has been identified to date, weight loss has been shown through various clinical approaches to effectively improve the pathological characteristics of MASLD.11–15
Laparoscopic sleeve gastrectomy (LSG) is among the most commonly performed bariatric procedures globally owing to its simplicity, safety, and efficacy. LSG has been shown to provide significant benefits in body weight reduction and the management of obesity-related comorbidities. LSG induces substantial weight loss by reducing gastric volume, modifying gut hormone secretion, and suppressing appetite, which collectively enhances insulin sensitivity and glycemic control.16 Additionally, LSG significantly enhances metabolic parameters, including lipid profile, liver enzyme levels, and blood glucose levels. LSG has been demonstrated to ameliorate or resolve type 2 diabetes (T2D), dyslipidemia, and hypertension in many patients.17 LSG has been shown to improve liver histology in patients with MASLD, including reduction in hepatic steatosis, inflammation, and fibrosis.18,19
These findings establish LSG as an effective therapeutic approach, not only for achieving weight loss but also for enhancing metabolic health, with sustained benefits in mitigating obesity-associated complications.20 LSG reduces gastric volume and modulates gastrointestinal hormone secretion to suppress appetite. Multiple studies have shown that LSG significantly improves hepatic steatosis and fibrosis among patients with MASLD.21 A study showed that bariatric surgery improves obesity-related metabolic parameters and can partially reverse MASLD progression.17
However, MASLD demonstrates significant pathological heterogeneity among patients, with the condition commonly classified as mild, moderate, or severe, based on liver biopsy findings. Varying degrees of MASLD severity may affect postoperative outcomes after LSG,22 although studies in this area remains limited. Some studies have suggested that the severity of fatty liver in patients with MASLD may affect postoperative weight loss and metabolic improvements; however, specific differences in outcomes among pathological grades remain poorly understood. Furthermore, obesity and MASLD are prevalent chronic conditions, and achieving a favorable postoperative prognosis is critical for these patients. Thus, preoperative evaluation of postoperative outcomes and the development of individualized therapeutic strategies are essential.
Based on these considerations, this study investigated the effect of MASLD severity, determined through pathological grading, on postoperative outcomes following LSG. By examining the differences in postoperative weight loss across various MASLD grades, this study aimed to provide robust evidence to support individualized weight management strategies for patients with MASLD in clinical practice. We hypothesized that MASLD severity significantly affects postoperative outcomes after LSG, with patients exhibiting severe MASLD experiencing more limited weight loss.20,22,23
Materials and Methods
Data Sources and Recruitment
We retrospectively included 226 patients with obesity who met the criteria for LSG and underwent the procedure at our medical center between December 2020 and August 2024. All the patients received standardized dietary counseling and follow-up protocols postoperatively, ensuring consistency in behavioral interventions across MASLD severity groups. This study was approved by the Ethics Committee of the First Affiliated Hospital of Shandong First Medical University (approval number 2025S035). Requirement for informed patient consent was waived because of the retrospective nature of the study. All patient data were anonymized and handled with strict confidentiality to ensure compliance with the Declaration of Helsinki.
Data Collection
Inclusion Criteria
(1) Age between 16 and 65 years; (2) body mass index (BMI) ≥ 32.5 kg/m² without comorbidities, or BMI ≥ 27.5 kg/m² with diabetes mellitus or other metabolic disorders; (3) those who underwent LSG with liver biopsy; and (4) availability of complete postoperative follow-up data.
Exclusion Criteria
(1) Alcoholic fatty liver disease; (2) use of obesity-inducing medications post-surgery; (3) pregnancy shortly after surgery; (4) use of weight-affecting medications (eg, metformin, insulin or GLP-1 agonists) following surgery; (5) incomplete follow-up data; and (6) patients with poor compliance were excluded to minimize confounding from postoperative behavioral factors.
Grouping Method
Liver biopsy specimens were used to assess fatty liver severity based on the following histopathological grading: (1) normal, <5% hepatocellular steatosis; (2) mild, 5–33% hepatic steatosis; (3) moderate, 34–66% hepatic steatosis; and (4) severe, >66% hepatic steatosis.
Data Collection
Perioperative data for all the patients, including sex, age, BMI, waist circumference, hip circumference, metabolic syndrome (MS), and obesity-related comorbidities (such as hypertension, T2D, and hyperlipidemia), were systematically recorded using an electronic case management system. Processing and pathological diagnosis of liver tissues were performed by experienced pathologists in the Department of Pathology at our hospital, and a final review was conducted by the Department Director. To minimize potential confounding, several strategies were implemented during study design and execution. All patients received standardized preoperative education and postoperative guidance, including structured dietary and medication counseling provided by trained clinical staff. Follow-up visits were conducted at 1, 3, 6, and 12 months postoperatively to ensure adherence and consistency of care. Patients with poor compliance or incomplete follow-up data were excluded. Furthermore, a comprehensive dataset was collected including anthropometric measures, glycemic and lipid profiles, and obesity-related comorbidities, which were incorporated into both univariate and multivariate analyses. These follow-ups included evaluating postoperative weight, conducting blood tests, assessing surgery-related complications, and monitoring the improvements in preoperative obesity-related comorbidities. To assess the effectiveness of weight loss surgery, we used percentage of excess weight loss (%EWL) as the evaluation criterion.
%TWL = (initial body weight - final body weight)/initial weight × 100%.
%EWL = ([initial body weight − final body weight]/[initial weight − ideal body weight]) × 100%.
Ideal BMI (IBMI): 25 kg/m2, ideal body weight: IBMI × (height)2.
HOMA-IR: (Fasting Glucose*Fasting Insulin)/22.5
Statistical Analyses
Continuous variables were assessed for normality using the Shapiro–Wilk test. For variables that were not normally distributed, Spearman’s rank correlation was used to assess the relationship with MASLD severity at baseline, and the Kruskal–Wallis test was used for comparisons between the three MASLD groups at specific time points. For normally distributed continuous variables, the Pearson’s correlation was used at baseline, and one-way analysis of variance (ANOVA) was employed to compare group means at each time point. Where the assumption of homogeneity of variances was violated (the Levene’s test, P < 0.05), the Welch’s ANOVA was used. Post-hoc pairwise comparisons following significant ANOVA or the Welch’s ANOVA were performed using the Games–Howell tests (for unequal variances) or least significant difference (LSD) tests (for equal variances). To account for multiple pairwise comparisons performed for %EWL between the MASLD groups at 1, 3, 6, and 12 months, the Bonferroni correction was applied, and statistical significance for the post-hoc tests was set at P < 0.05 divided by the number of comparisons at each time point (α/3 = 0.0167). Using univariate analysis to screen for significantly correlated variables and multivariate analysis to adjust for confounders, the process covered, in detail, preoperative blood biochemistry, glucose and lipid metabolism indices, and obesity comorbidities. The Kaplan–Meier curve was used to evaluate the time to achieve 50% EWL, and group differences were assessed using the Log rank test. General linear models were employed to analyze the %EWL changes at different time points across the fatty liver severity groups. All statistical analyses were performed using IBM SPSS Statistics 27.0; Plot using GraphPad Prism 9.5.0.
Results
Baseline Characteristics and Group Comparisons
The patients were classified into normal (n=0), mild (n=73), moderate (n=86), and severe (n=67) groups based on the pathological grading of MASLD. As indicated in Table 1, BMI, waist-to-hip ratio (WHR), serum uric acid, triglycerides, total cholesterol, A1C, and homeostasis model assessment for insulin resistance (HOMA-IR) were significantly associated with MASLD severity (P < 0.05). Group differences were denoted by superscript letters (a/b) (P < 0.05). Fatty liver severity was significantly correlated with WHR (r = 0.156, P = 0.020). Significant differences were observed between the mild and moderate groups and between the moderate and severe groups (F = 5.933, P = 0.003; mild vs moderate, P < 0.001; mild vs severe, P = 0.022; moderate vs severe, P = 0.367). Uric acid, total cholesterol, and high-density lipoprotein levels were significantly associated with the severity of fatty liver disease (P < 0.005); however, no significant group differences were found among the mild, moderate, and severe groups (H < 5.991, P > 0.05). Triglyceride was significantly correlated with fatty liver severity (r = 0.188, P = 0.005), with significant differences observed between the mild and severe groups (H = −30.974, P = 0.015). A1C (mild vs severe group, H = −33.116, P = 0.008) and HOMA-IR (mild vs severe group, H = −39.916, P = 0.001) were also significantly different. Aspartate transaminase/alanine transaminase (mild vs severe group, H = 46.988, P < 0.001; mild vs moderate group, H = 45.330, P < 0.001) and low-density lipoprotein (mild vs severe group, H = −32.023, P = 0.01) exhibited similar trends. Metabolic diseases, such as T2D, were notably more prevalent in the severe MASLD group (53.7%) than those in the mild group (28.8%), indicating a significant association between MASLD severity and metabolic diseases (P = 0.011). MASLD severity, as reflected by the degree of hepatic steatosis (DHS), significantly affected weight loss outcomes following LSG. Univariate analysis (Table S1) revealed that higher DHS grades were negatively correlated with percentage of total weight loss (%TWL) at 3 months (r = −0.184, P = 0.006), indicating that advanced hepatic steatosis impaired early postoperative weight loss.
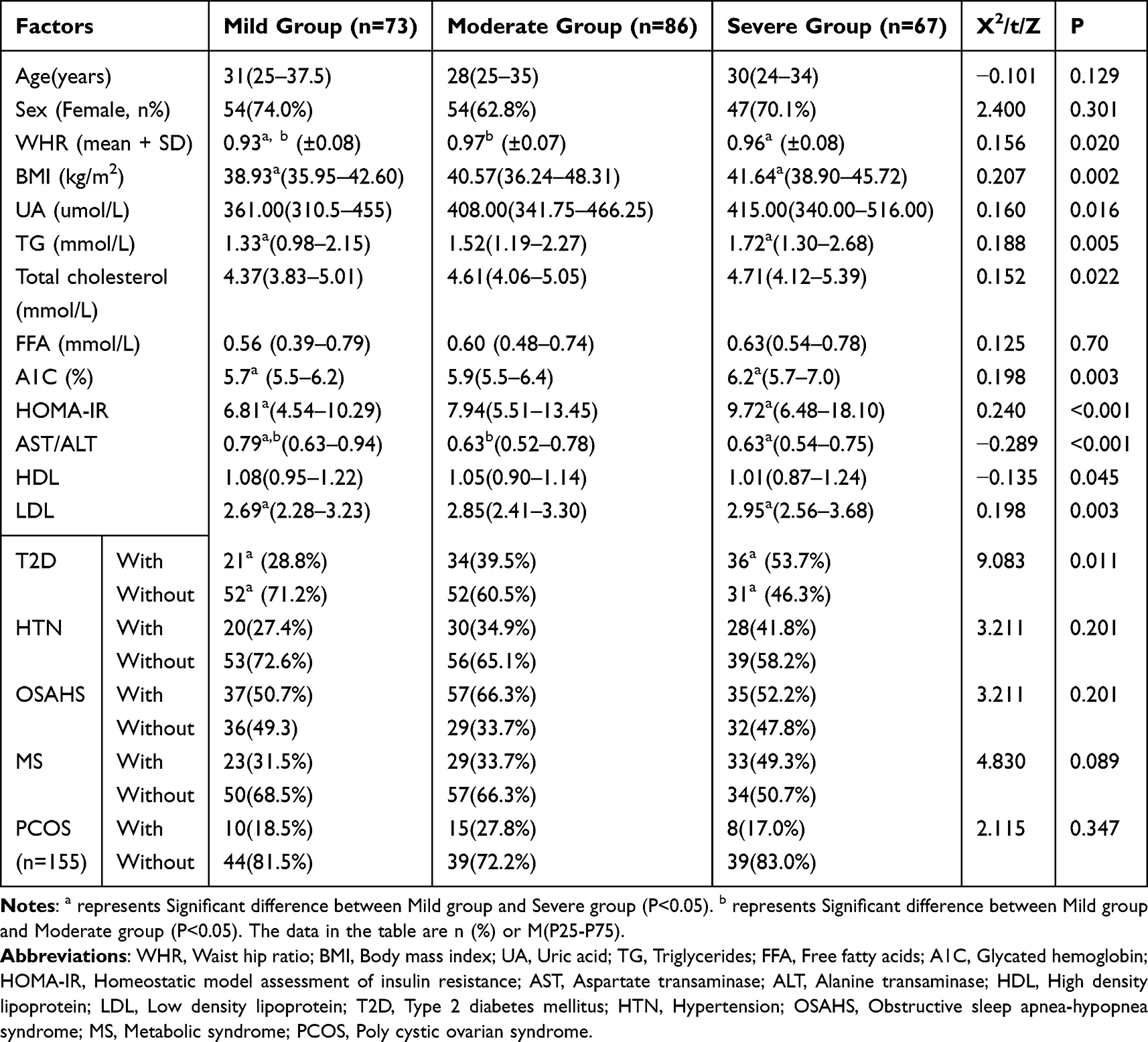 |
Table 1 Preoperative Baseline Information |
At 1 month postoperatively, age, sex, and WHR were significantly correlated with %EWL. BMI and the DHS also showed strong associations (Table 2). The DHS and BMI had the most substantial effect on %EWL at all time points, with a consistent negative correlation observed over time (P < 0.05). At 3, 6, and 12 months, significant associations were observed between %EWL and several metabolic factors, including free fatty acids (FFAs), A1C, and HOMA-IR. Specifically, fatty liver severity continued to show a significant negative correlation with %EWL across all follow-up periods (P < 0.05). Additionally, the effect of metabolic syndrome and obstructive sleep apnea-hypopnea syndrome (OSAHS) on weight loss was less pronounced, showing no significant changes across the time points. Although this association was weakened by 6 months (r = −0.059, P = 0.451), multivariate regression (Table S2) identified DHS as an independent negative predictor of %TWL both at 1 (β = −0.159, p = 0.036) and 12 (β = −0.167, P = 0.040) months, suggesting persistent detrimental effects in patients with severe MASLD. In contrast, baseline BMI transitioned from an initial inverse correlation (1 month: r = −0.134, P = 0.044) to a dominant positive predictor of long-term success (12 months: β = 0.521, P < 0.001). These findings underscore that although elevated BMI drives sustained weight loss, MASLD severity, mediated by DHS, imposes early- and late-phase barriers to optimal %TWL, highlighting its clinical relevance in personalized postoperative management.
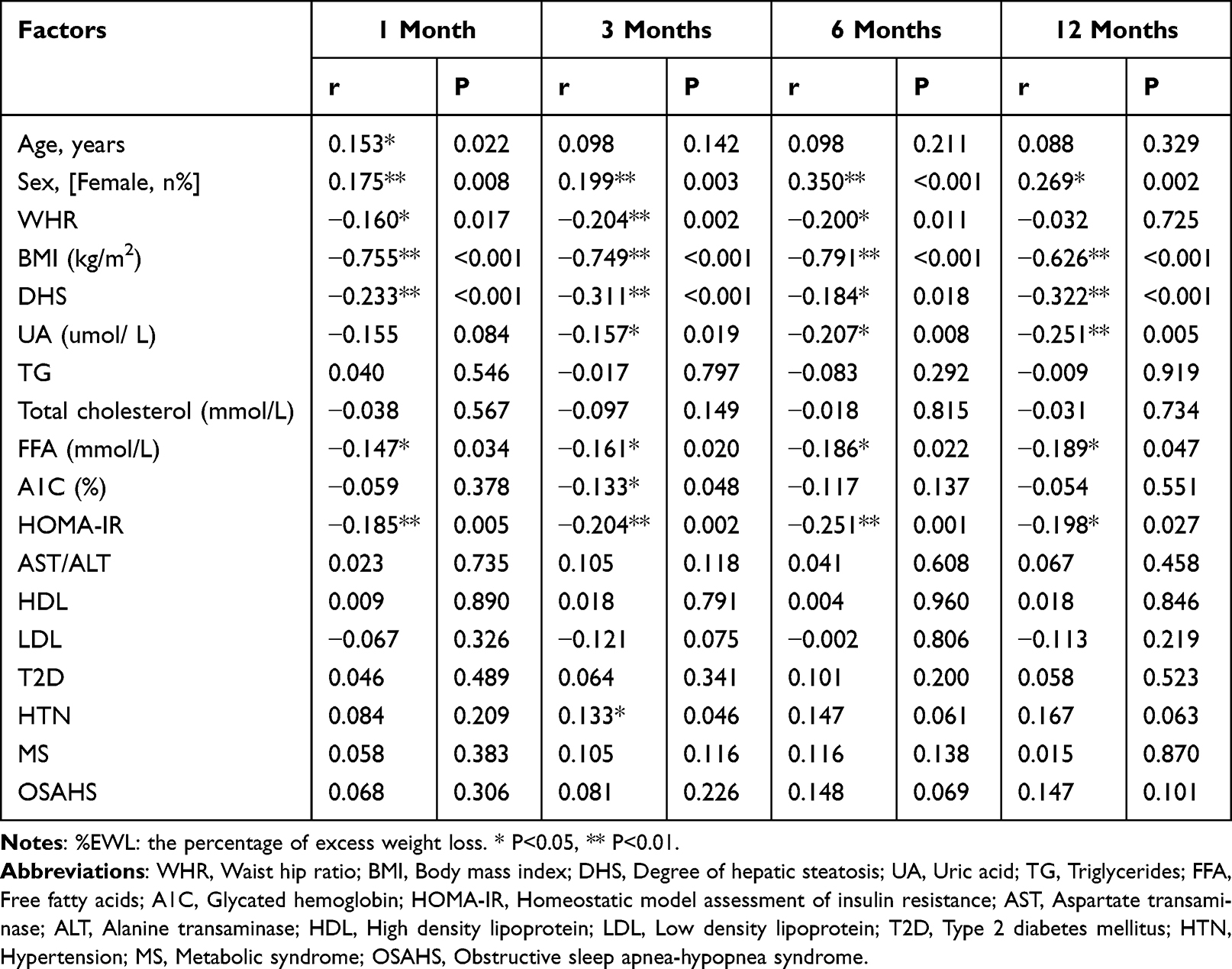 |
Table 2 Factors Affecting %EWL |
The analysis identified preoperative DHS and BMI as primary independent predictors of %EWL (Table 3). A significant negative association was observed between DHS and %EWL at 1, 3, and 12 months postoperatively, indicating that greater fatty liver severity was linked to poorer weight loss outcomes, as shown in Table 3. At 1 month, the DHS showed a significant effect (B = −0.023, P = 0.010), with similar trends at 3 (B = −0.052, P < 0.001) and 12 (B = −0.090, P = 0.001) months. Although DHS did not reach statistical significance at 6 months (P = 0.065), the effect reemerged at 12 months, highlighting its long-term effect on weight loss. Preoperative BMI was consistently a significant negative predictor of %EWL across all time points (P < 0.05), with a higher BMI correlating with reduced postoperative weight loss outcomes. Other variables, such as sex, WHR, uric acid, FFA, and HOMA-IR, were not significantly associated with %EWL at any time point. The models demonstrated strong explanatory power for %EWL variation, with adjusted R² values between 0.396–0.524 across different time points. These findings underscore the critical role of preoperative fatty liver severity and BMI in shaping postoperative weight loss outcomes, and emphasize the importance of preoperative optimization strategies.
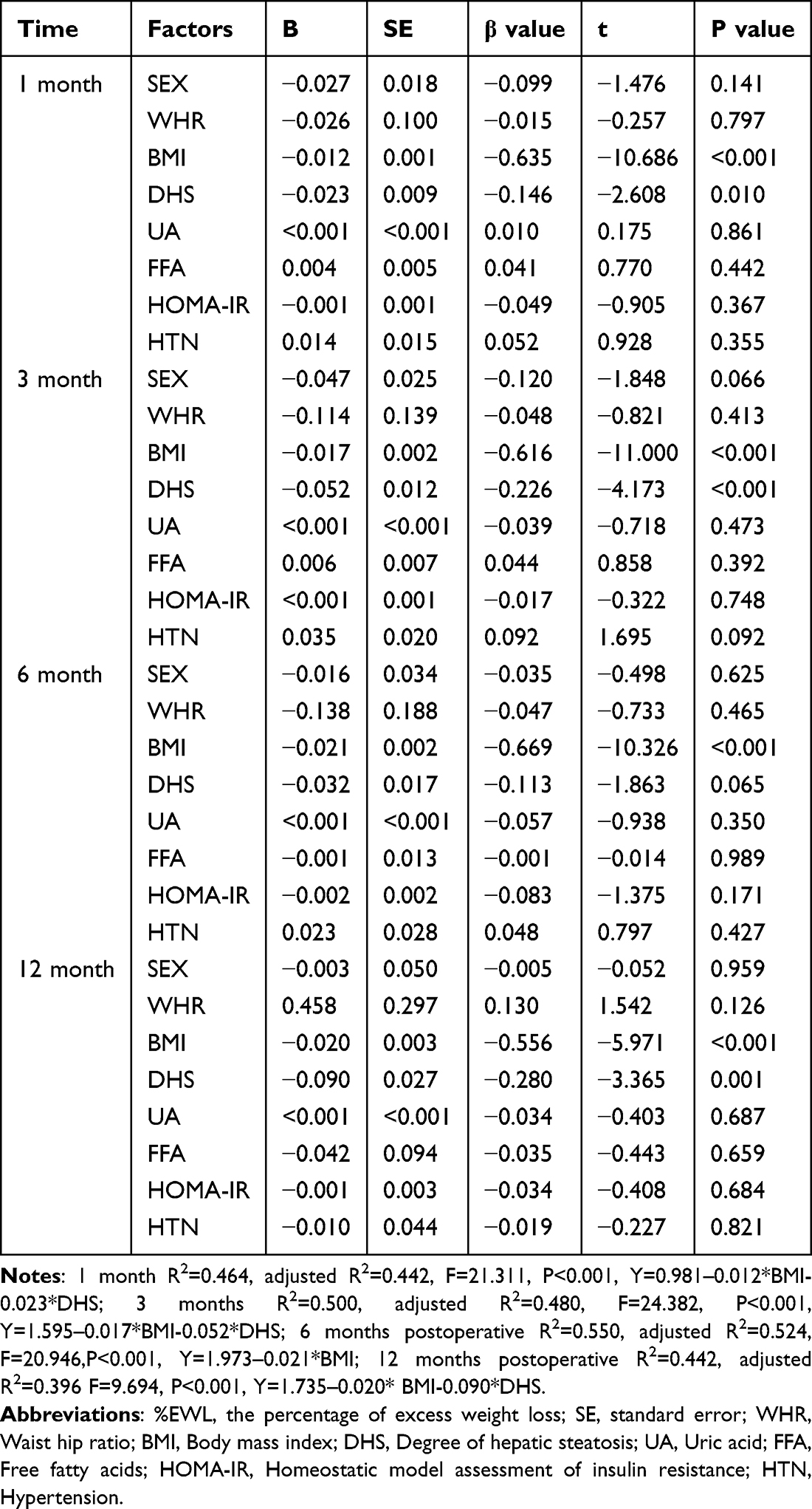 |
Table 3 Multiple Linear Regression Affecting Postoperative %EWL |
Postoperative %EWL significantly increased in all MASLD groups over time (1, 3, 6, and 12 months). Correlation analysis demonstrated a significant negative association between MASLD severity and %EWL at each time point: 1 month (r = −0.233, P < 0.001), 3 months (r = −0.330, P < 0.001), 6 months (r = −0.218, P = 0.005), and 12 months (r = −0.287, P = 0.001), suggesting that greater steatosis severity was associated with attenuated weight loss (Table 4).
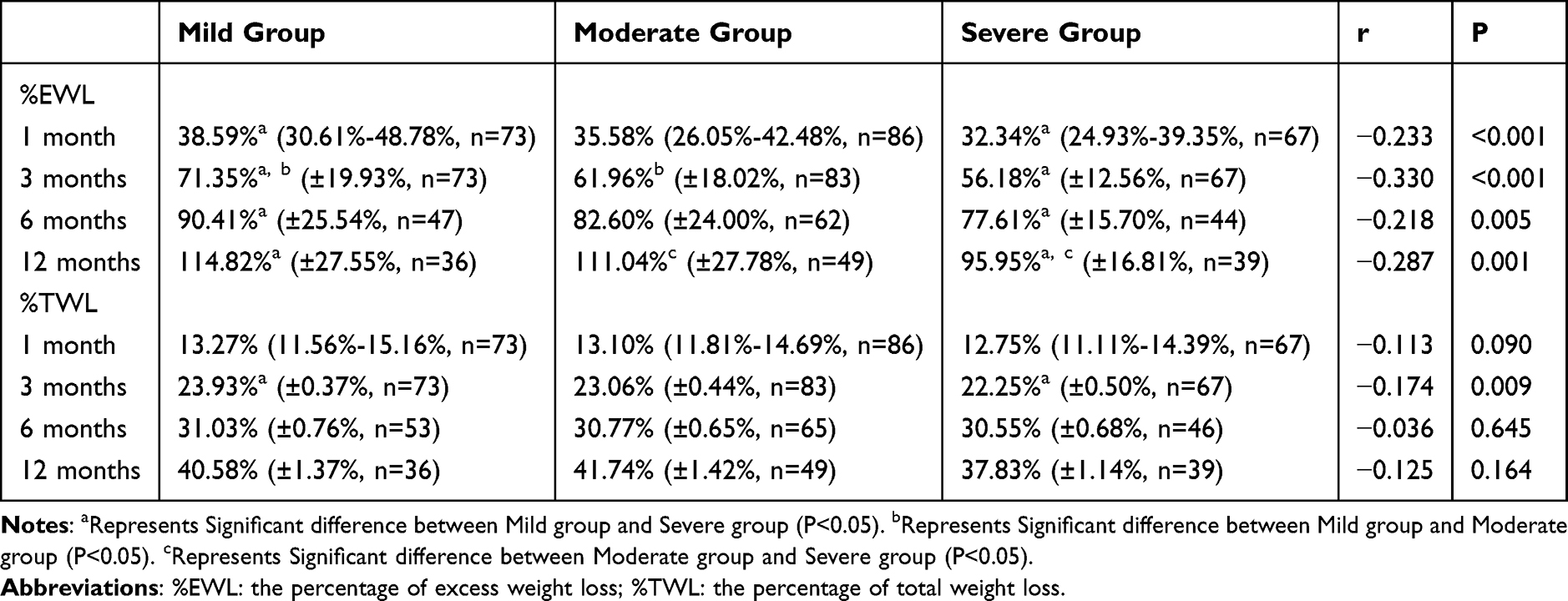 |
Table 4 Postoperative Excess Weight Loss Percentage |
According to the Shapiro–Wilk test, the %EWL and %TWL values at 1 month postoperatively were not normally distributed (P < 0.05). Therefore, the Kruskal–Wallis test was used to compare the three MASLD groups. A significant difference in %EWL was found (H = 22.861, P < 0.001). Bonferroni-corrected post-hoc comparisons showed that the median %EWL in the mild group was significantly higher than both the moderate and severe groups (mild vs severe: F = 51.577, P < 0.001; mild vs moderate: F = 32.341, P = 0.020). No significant difference was observed in %TWL among the groups at 1 month (H = 3.019, P = 0.221).
For follow-up data at 3, 6, and 12 months, both %EWL and %TWL were normally distributed (P > 0.05). Levene’s test revealed that the assumption of homogeneity of variances was violated for %EWL at 3 and 6 months (3 months: F = 3.592, P = 0.029; 6 months: F = 4.276, P = 0.016). Therefore, Welch’s ANOVA was performed and showed significant group differences (3 months: F = 13.998, P < 0.001; 6 months: F = 3.833, P = 0.025). Post-hoc analysis using the Games–Howell test indicated that at 3 months, the mild MASLD group had significantly higher %EWL than both the moderate (P = 0.005, mean difference = 7.10% ± 2.21%, 95% CI: 1.86–12.33%) and severe groups (P < 0.001, mean difference = 11.17% ± 2.11%, 95% CI: 6.18–16.17%). At 6 months, only the mild vs severe comparison remained significant (P = 0.018, mean difference = 8.91% ± 3.21%, 95% CI: 1.27–16.55%).
At 12 months, Levene’s test indicated equal variances (F = 2.411, P = 0.094), and one-way ANOVA revealed a significant difference in %EWL between the MASLD groups (F = 6.247, P = 0.003). LSD post-hoc tests showed that the severe group had significantly lower %EWL than the mild (P = 0.002, mean difference = 14.07% ± 4.33%, 95% CI: 5.49–22.65%) and moderate (P = 0.005, mean difference = 11.69% ± 4.05%, 95% CI: 3.67–19.72%) groups.
For %TWL at 3 months, both normality and equal variances were confirmed (Levene’s test: F = 2.144, P = 0.120), allowing for one-way ANOVA. The analysis revealed significant differences among groups (F = 3.450, P = 0.033). LSD post-hoc comparison showed that the mild group had significantly higher %TWL than the severe group (P = 0.009, mean difference = 1.68% ± 0.64%, 95% CI: 0.42–2.94%). No significant differences in %TWL were found among the MASLD groups at 6 and 12 months postoperatively.
%EWL values for patients in the three MASLD groups were evaluated across four postoperative time points (1, 3, 6, and 12 months) using a general linear model (GLM) with repeated measures, assessing the main effects of time and group, as well as their interaction.
A significant main effect of time was observed (F[2,148] = 780.650, P < 0.001), indicating substantial changes in %EWL across follow-up. The main effect of MASLD group was also significant (F[2,149] = 5.197, P = 0.007), suggesting that fatty liver severity influences overall weight loss outcomes. Importantly, a significant time × group interaction was found (F[2,149] = 5.926, P = 0.003), indicating that the %EWL trajectory over time differed depending on MASLD severity.
In light of this significant interaction, simple effects analyses were conducted using pairwise comparisons at each time point. Where appropriate, Bonferroni correction was applied to account for multiple comparisons. At 1 month, only the mild vs severe group comparison reached significance (P = 0.026, mean difference = 6.8% ± 2.5%). At 3 months, the mild group had significantly higher %EWL than both the moderate (P = 0.030, mean difference = 8.6% ± 3.3%) and severe (P < 0.001, mean difference = 13.7% ± 3.6%) groups. At 6 months, a significant difference was maintained between mild and severe groups (P = 0.016, mean difference = 12.8% ± 4.5%). At 12 months, both the mild vs severe (P = 0.004, mean difference = 18.9% ± 5.7%) and moderate vs severe (P = 0.016, mean difference = 15.1% ± 5.3%) comparisons were significant.
No significant differences were observed between the moderate and severe groups at 1–6 months, or between the mild and moderate groups at 12 months.
To facilitate interpretation, the results were illustrated in Figure 1, with significance values labeled directly on the graph. All post-hoc p-values are two-tailed, and where not otherwise specified, results are reported with a significance threshold of α < 0.05.
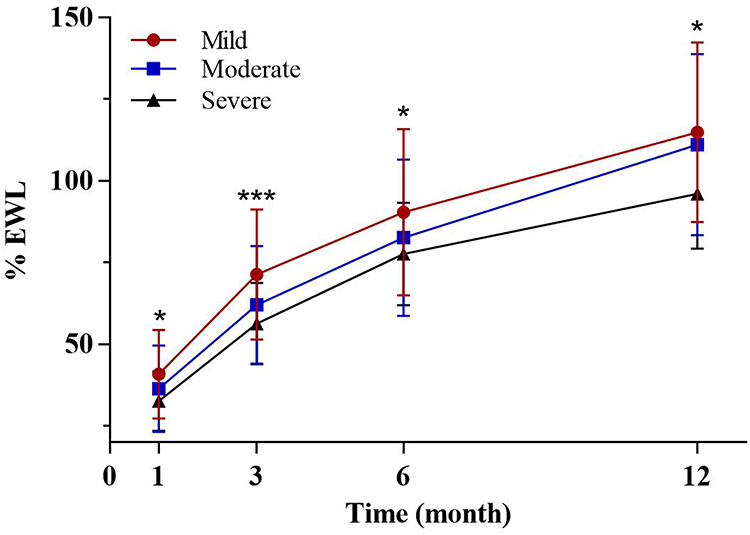 |
Figure 1 General Linear Model Analysis of %EWL Changes Over Time by MASLD Severity. Abbreviation: %EWL, the percentage of excess weight loss. Notes: *P<0.05, ***P<0.001. |
To investigate the differences in the time required to achieve satisfactory weight loss following surgery among patients with varying degrees of fatty liver disease, satisfactory weight loss was defined as reaching 50% EWL, and the cumulative incidence of this event was examined using postoperative follow-up data. A significant difference was observed in the rate of achieving 50% EWL among the MASLD severity groups over the 12 months postoperative follow-up period (P < 0.05, Figure 2B). Across all time points, the mild MASLD group consistently demonstrated the highest proportion of patients achieving 50% EWL, indicating superior weight-loss outcomes. Conversely, the severe MASLD group exhibited a significantly lower rate of attainment and slower increase in weight loss during the early postoperative period. This was supported by post-operative data showing that at 1 month, 28.8% of patients in the mild group achieved 50% EWL compared with 11.6% in the moderate group, while only 2.6% of patients in the severe group reached this threshold. At 3 months, the mild group maintained a significant advantage, with 91.8% of patients achieving 50% EWL compared with 75.6% and 64.7% in the moderate and severe groups, respectively. At 6 months, the differences between the groups diminished, and all the groups showed significant improvement (98.4%, 97.7%, and 92.6% in the mild, moderate, and severe groups, respectively). At 12 months, nearly similar results were observed in all the groups (98.4%, 98.8%, and 97.5%, respectively), indicating that the cumulative incidence converged over time. Although patients in the severe group had worse weight loss results than those in the moderate and mild groups, 97.5% of patients in this group achieved satisfactory weight loss within 1 year of bariatric surgery.
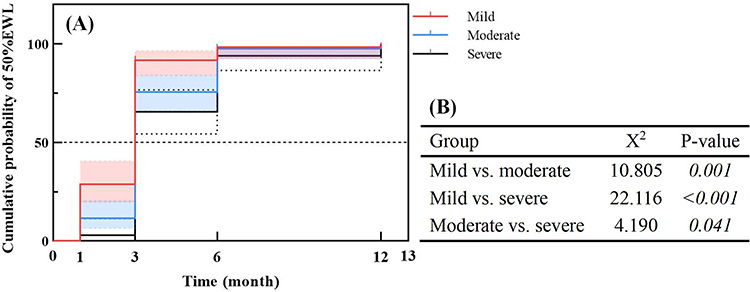 |
Figure 2 (A) Kaplan-Meier Analysis of 50%EWL Achievement Rate by MASLD Severity. (B) The Log rank test was employed to undertake a pair-wise comparison of the data, Italic formatting in the figure indicates P<0.05, reflecting statistically significant differences. Abbreviation: %EWL, the percentage of excess weight loss. |
Discussion
Although the existing literature suggests that bariatric surgery produces positive outcomes for weight loss and metabolic improvement in patients with MASLD, only a few studies have evaluated the effect of different baseline stages of MASLD on postoperative weight loss,24,25 and the specific impact of pathology-based hepatic steatosis on postoperative outcomes remains underexplored. Existing literature on MASLD/NAFLD and bariatric outcomes has produced heterogeneous findings. For example, Abdalla et al (2023) and Goh et al (2020) reported no significant associations between histological severity and weight loss, while Rheinwalt et al (2020) and Montoro et al (2022) found that steatosis or fibrosis negatively affected surgical outcomes.24–26 One major difference lies in the assessment modality: several previous studies relied on imaging-based NAFLD scores or non-standardized pathology reviews. In contrast, our study incorporated intraoperative liver biopsies, enabling a more granular classification of steatosis severity. Furthermore, our use of repeated longitudinal follow-up (%EWL at 1, 3, 6, and 12 months) adds to the literature by tracking dynamic trends in weight loss over time. Moreover, most previous studies were conducted in Western populations with distinct metabolic phenotypes. To our knowledge, this is one of the first biopsy-based MASLD studies in an Asian bariatric cohort, providing important context for populations with different fat distribution, insulin resistance patterns, and MASLD presentation. By integrating steatosis-based pathology, metabolic markers, and prospective weight loss dynamics, this study adds novel evidence to support the role of hepatic steatosis as a risk stratifier in clinical bariatric practice.
Consistent with previous findings, our study further validated that preoperative fatty liver severity is significantly associated with glycolipid metabolism.27 Additionally, we found that preoperative HOMA-IR and FFA levels were significantly associated with %EWL in a univariate analysis. However, after including BMI, fatty liver severity, HOMA-IR, and FFA in the multifactorial analysis, only BMI and fatty liver severity were significantly associated with %EWL; HOMA-IR and FFA did not show statistical significance. This suggests that the predictive value of glycolipid metabolism indices for postoperative %EWL may be limited when other factors, such as BMI and fatty liver severity, are considered. Therefore, multiple factors should be considered when predicting the effects of weight loss, as well as glycolipid metabolism indices. This study also confirmed that preoperative fatty liver severity and BMI were independent risk factors for predicting %EWL; that is, the effect of fatty liver severity was independent of BMI and vice versa. Therefore, both factors should be considered when evaluating postoperative weight loss outcomes to develop a more precise treatment plan.
Although indicators of glucose and lipid metabolism (eg, HOMA-IR and FFA) may co-vary with other variables in multifactorial models, their effects might be masked by stronger predictors (eg, DHS and BMI), leading to reduced or non-significant statistical outcomes. The liver serves as the central organ for metabolism, where glucose (eg, insulin resistance, IR) and lipid (eg, FFA) metabolisms play critical roles in the development of hepatic steatosis.28 The reduced postoperative weight loss cannot be solely attributed to hepatic steatosis because, first, hepatic fat accumulation can impair insulin signaling, increase insulin resistance,29 and disrupt glucose metabolism. Second, elevated FFA levels associated with hepatic steatosis lead to lipid peroxidation and oxidative stress, further compromising liver function. Finally, the inflammatory response induced by steatosis can impair liver metabolic function and exacerbate metabolic disturbances. These factors may collectively contribute to poorer postoperative weight loss observed in patients with severe hepatic steatosis. The negative association between severe MASLD (reflected by DHS) and early weight loss may reflect its role as a marker of advanced metabolic dysfunction, which could indirectly hinder weight loss through mechanisms such as insulin resistance or altered energy metabolism.
Figure 1 demonstrates that the severity of MASLD significantly affects the trajectory of postoperative weight loss. Patients with severe MASLD exhibited 18.9% greater mean %EWL at 12 months than those with mild MASLD. The Kaplan–Meier analysis (Figure 2) confirmed delayed achievement of higher %EWL levels in the severe MASLD group during the early postoperative period (1–3 months), although the outcomes converged by 12 months. This suggests that although patients with severe MASLD can achieve satisfactory weight loss after sleeve gastrectomy, it occurs more gradually and with less overall %EWL than those with mild or moderate MASLD. Optimizing MASLD severity preoperatively may improve early postoperative weight loss trajectories.
Early impaired weight loss in patients with severe MASLD may be due to systemic metabolic disorders caused by severe steatosis, such as increased lipid toxicity, insulin resistance, and chronic inflammation, all of which compromise energy metabolism postoperatively.30 Severe hepatic steatosis exacerbates these conditions by impairing mitochondrial function and promoting systemic inflammation, which impedes insulin signaling and oxidative capacity, critical to postoperative metabolic improvement.28,31,32
The liver plays a central role in metabolism, and its condition may be a key indicator of weight loss after bariatric surgery. Our findings identified preoperative MASLD severity as an independent predictor of postoperative weight loss. Severe hepatic steatosis, associated with insulin resistance, chronic inflammation, and mitochondrial dysfunction, impairs metabolic flexibility and diminishes the early efficacy of bariatric surgery, aligning with previous studies.33 Preoperative interventions targeting insulin resistance and hepatic steatosis, such as dietary modification, physical activity,34 and pharmacological agents like GLP-1 receptor agonists,35 may improve surgical outcomes.
Although our study focused on the percentage of hepatic steatosis as the primary marker of MASLD severity, we acknowledge the pathophysiological complexity of MASLD, which includes necroinflammation (MASH) and fibrosis. However, several evidences suggest that steatosis plays a dominant role in metabolic dysregulation and weight loss. Recent studies have shown that baseline hepatic fat content, rather than fibrosis stage, independently predicts postoperative weight loss after bariatric surgery.25 Furthermore, in a biopsy-based cohort of patients undergoing sleeve gastrectomy, steatosis severity was more strongly associated with attenuated weight loss than with fibrosis or inflammation.24,26 This aligns with our findings that steatosis severity exhibits time-dependent correlations with %TWL, even after adjusting for metabolic confounders. Although we did not analyze the MASH score or fibrosis owing to sample size constraints, our results emphasize the clinical relevance of quantifying steatosis as a key driver of metabolic dysfunction in MASLD. Nevertheless, it is important to acknowledge that steatosis is only one component of MASLD pathology. The lack of data on inflammatory activity and fibrosis prevents comprehensive staging (eg, using SAF or NAS scores), which could further refine prognostic modeling. This simplification may have led to underestimation of the role of necroinflammation or fibrosis in patients with MASH or advanced disease. While steatosis alone was significantly predictive of postoperative weight loss in our cohort, future studies should incorporate full histological staging or validated non-invasive markers of liver fibrosis (eg, transient elastography, MRI-PDFF) to capture the multidimensional burden of MASLD.
Despite early postoperative challenges, all the groups showed significant improvements in liver function and glycemic control by 6 months, consistent with the benefits of bariatric surgery, such as reduced visceral adiposity and systemic inflammation. These improvements indicate that LSG can reverse metabolic dysfunction, in patients with advanced liver fat disease.36
Patients with severe MASLD should be considered for targeted preoperative interventions, including GLP-1 receptor agonists, sodium-glucose linked transporter 2 inhibitors, or structured weight loss programs, to improve liver function and metabolic flexibility.37 Additionally, enhanced follow-up schedules focused on liver function, glycemic control, and weight loss, which are critical for early identification and management of suboptimal outcomes. Integrating imaging tools, such as magnetic resonance imaging-based proton density fat fraction (PDFF) or ultrasound-derived fat fraction (UDFF), could provide precise longitudinal monitoring of liver fat resolution and inform personalized management strategies.38
Clinical Implications
The observed differences in early postoperative %EWL between MASLD groups—particularly the 13.7% and 18.9% gaps at 3 and 12 months—surpass thresholds often regarded as clinically meaningful in bariatric literature (ie, 10% %EWL difference). These differences may delay the achievement of weight-related targets such as glycemic control, blood pressure reduction, or medication de-escalation. In particular, our Kaplan–Meier analysis revealed that <3% of patients in the severe MASLD group achieved 50% EWL at 1 month, compared to nearly 29% in the mild group. This suggests that MASLD severity can identify patients at risk for early suboptimal response and help guide early intervention. From a clinical perspective, incorporating MASLD grading—through either biopsy or non-invasive surrogates—into preoperative workups could support more personalized postoperative plans. For example, severe MASLD patients may benefit from early introduction of GLP-1 receptor agonists, intensive dietary coaching, or more frequent follow-up visits during the first 3–6 months post-surgery.
Strengths and Limitations
This study has several notable strengths. First, it provides a detailed histopathological evaluation of MASLD severity through intraoperative liver biopsies, ensuring precise grading of hepatic steatosis (mild, moderate, and severe) rather than relying on non-invasive surrogates. Second, the inclusion of longitudinal follow-up data (up to 12 months postoperatively) and multivariate adjustments for key metabolic confounders (eg, BMI and A1c) strengthened the validity of the observed associations. Third, the use of standardized surgical protocols and postoperative care minimizes the variability in clinical management and enhances internal consistency.
As this was a retrospective, single-center study conducted in a Chinese cohort, its findings may not be generalizable to other ethnic populations with differing metabolic profiles or MASLD pathophysiologies. The 12-month follow-up period precludes conclusions regarding long-term weight maintenance or potential late-phase divergence in the outcomes. Additionally, although histopathology focused on steatosis grading, critical features, such as inflammation (MASH) and fibrosis, were not analyzed because of sample size constraints, limiting insights into their potential roles. Unmeasured behavioral factors (eg, dietary adherence and physical activity) and postoperative medical management (eg, antidiabetic medications) could confound weight loss trajectories, but were not systematically assessed. Finally, the absence of postoperative liver biopsies hindered the exploration of dynamic histological changes after LSG.
Prospective multicenter studies with extended follow-up periods (>5 years) are required to validate these findings in diverse populations. Future studies should integrate comprehensive histological staging (steatosis, inflammation, and fibrosis) and behavioral assessments to disentangle their individual contributions. Additionally, exploring the effect of perioperative metabolic interventions (eg, GLP-1 agonists) in patients with severe MASLD could refine personalized management strategies.
Conclusion
The severity of MASLD, defined by intraoperative hepatic steatosis, significantly affected both %EWL and %TWL following laparoscopic sleeve gastrectomy. Patients with severe MASLD exhibited a mean of 18.9% lower %EWL at 12 months compared to those with mild disease, particularly during the early postoperative phase. These findings remained robust after adjustment for key metabolic confounders such as BMI and HOMA-IR, suggesting an independent role of MASLD in shaping weight loss trajectories. Given that full histological assessment including inflammation and fibrosis was not feasible, and only steatosis grade was consistently available, our conclusions should be interpreted in light of this limitation. Nevertheless, hepatic steatosis may serve as a readily identifiable marker of metabolic risk and poor postoperative responsiveness. Routine preoperative liver pathology assessment may help identify patients at risk for delayed weight loss, guiding the implementation of intensified follow-up protocols, nutritional support, or pharmacological adjuncts (eg, GLP-1 receptor agonists). However, the invasive nature of liver biopsy limits its widespread use. Future research should therefore explore non-invasive stratification tools (eg, imaging biomarkers) and evaluate the efficacy of preoperative metabolic interventions in patients with suspected or confirmed advanced MASLD. Incorporating MASLD severity into perioperative decision-making may help optimize individualized treatment strategies and improve surgical outcomes.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. San-Yuan Hu and Ming-Wei Zhong should be considered joint senior author.
Funding
This work was supported by the National Science Foundation of China (82270914, 82070869).
Disclosure
The authors declare that they have no competing interests.
References
1. Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease—meta‐analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64(1):73–84. doi:10.1002/hep.28431
2. Ng M, Fleming T, Robinson M, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the global burden of disease study 2013. Lancet. 2014;384(9945):766–781. doi:10.1016/S0140-6736(14)60460-8
3. Wang Y, Zhao L, Gao L, Pan A, Xue H. Health policy and public health implications of obesity in China. Lancet Diabetes Endocrinol. 2021;9(7):446–461. doi:10.1016/S2213-8587(21)00118-2
4. Godoy-Matos AF, Silva WS, Valerio CM. NAFLD as a continuum: from obesity to metabolic syndrome and diabetes. Diabetol Metab Syndr. 2020;12(1):60. doi:10.1186/s13098-020-00570-y
5. Teng ML, Ng CH, Huang DQ, et al. Global incidence and prevalence of nonalcoholic fatty liver disease. Clin Mol Hepatol. 2023;29(Suppl):S32–S42. doi:10.3350/cmh.2022.0365
6. Wong RJ, Ahmed A. Obesity and non-alcoholic fatty liver disease: disparate associations among Asian populations. World J Hepatol. 2014;6(5):263–273. doi:10.4254/wjh.v6.i5.263
7. Lu R, Liu Y, Hong T. Epidemiological characteristics and management of nonalcoholic fatty liver disease/nonalcoholic steatohepatitis in China: a narrative review. Diabetes Obes Metab. 2023;25(1):13–26. doi:10.1111/dom.15014
8. Lou TW, Yang RX, Fan JG. The global burden of fatty liver disease: the major impact of China. Hepatobiliary Surg Nutr. 2024;13(1):119–123. doi:10.21037/hbsn-23-556
9. Vancells Lujan P, Vinas Esmel E, Sacanella Meseguer E. Overview of Non-Alcoholic Fatty Liver Disease (NAFLD) and the role of sugary food consumption and other dietary components in its development. Nutrients. 2021;13(5):1442. doi:10.3390/nu13051442
10. Romero-Gomez M, Zelber-Sagi S, Trenell M. Treatment of NAFLD with diet, physical activity and exercise. J Hepatol. 2017;67(4):829–846. doi:10.1016/j.jhep.2017.05.016
11. Koutoukidis DA, Astbury NM, Tudor KE, et al. Association of weight loss interventions with changes in biomarkers of nonalcoholic fatty liver disease: a systematic review and meta-analysis. JAMA Intern Med. 2019;179(9):1262–1271. doi:10.1001/jamainternmed.2019.2248
12. Vilar-Gomez E, Martinez-Perez Y, Calzadilla-Bertot L, et al. Weight loss through lifestyle modification significantly reduces features of nonalcoholic steatohepatitis. Gastroenterology. 2015;149(2):367–378e365;quize314–365. doi:10.1053/j.gastro.2015.04.005
13. Hashem A, Khalouf A, Acosta A. Management of obesity and nonalcoholic fatty liver disease: a literature review. Semin Liver Dis. 2021;41(4):435–447. doi:10.1055/s-0041-1731704
14. Brunner KT, Henneberg CJ, Wilechansky RM, Long MT. Nonalcoholic fatty liver disease and obesity treatment. Curr Obes Rep. 2019;8(3):220–228. doi:10.1007/s13679-019-00345-1
15. Koutoukidis DA, Koshiaris C, Henry JA, et al. The effect of the magnitude of weight loss on non-alcoholic fatty liver disease: a systematic review and meta-analysis. Metabolism. 2021;115:154455. doi:10.1016/j.metabol.2020.154455
16. Elyasinia F, Jalali SM, Zarini S, Sadeghian E, Sorush A, Pirouz A. The effect of laparoscopic sleeve gastrectomy and gastric bypass surgery on non-alcoholic steatohepatitis in Iranian patients with obesity. Middle East J Dig Dis. 2021;13(3):200–207. doi:10.34172/mejdd.2021.226
17. Cabre N, Luciano-Mateo F, Fernandez-Arroyo S, et al. Laparoscopic sleeve gastrectomy reverses non-alcoholic fatty liver disease modulating oxidative stress and inflammation. Metabolism. 2019;99:81–89. doi:10.1016/j.metabol.2019.07.002
18. Gluszynska P, Lukaszewicz A, Diemieszczyk I, et al. The effect of laparoscopic sleeve gastrectomy on the course of non-alcoholic fatty liver disease in morbidly obese patients during one year of follow up. J Clin Med. 2023;12(12):4122. doi:10.3390/jcm12124122
19. Cabre N, Gil M, Amigo N, et al. Laparoscopic sleeve gastrectomy alters (1)H-NMR-measured lipoprotein and glycoprotein profile in patients with severe obesity and nonalcoholic fatty liver disease. Sci Rep. 2021;11(1):1343. doi:10.1038/s41598-020-79485-7
20. Gluszynska P, Lemancewicz D, Dzieciol JB, Razak Hady H. Non-alcoholic fatty liver disease (NAFLD) and bariatric/metabolic surgery as its treatment option: a review. J Clin Med. 2021;10(24):5721. doi:10.3390/jcm10245721
21. Eisenberg D, Shikora SA, Aarts E, et al. 2022 American Society for Metabolic and Bariatric Surgery (ASMBS) and International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO): indications for metabolic and bariatric surgery. Surg Obes Relat Dis. 2022;18(12):1345–1356.
22. Abu-Rumaileh M, Haddad RA, Yosef M, et al. Impact of Nonalcoholic Fatty Liver Disease (NAFLD) on weight loss after bariatric surgery. Obes Surg. 2023;33(12):3814–3828. doi:10.1007/s11695-023-06865-z
23. Billmann F, Shishtawi SE, Bruckner T, ElSheikh M, Muller-Stich BP, Billeter A. Combined non-alcoholic fatty liver disease and type 2 diabetes in severely obese patients-medium term effects of sleeve gastrectomy versus Roux-en-Y-gastric bypass on disease markers. Hepatobiliary Surg Nutr. 2022;11(6):795–807. doi:10.21037/hbsn-21-71
24. Martínez-Montoro JI, Arranz-Salas I, Gutiérrez-Repiso C, et al. Weight loss after sleeve gastrectomy according to metabolic dysfunction-associated steatotic liver disease stage in patients with obesity: a liver biopsy-based prospective study. Nutrients. 2024;16(22):3857. doi:10.3390/nu16223857
25. Rheinwalt KP, Drebber U, Schierwagen R, et al. Baseline presence of NAFLD predicts weight loss after gastric bypass surgery for morbid obesity. J Clin Med. 2020;9(11).
26. Abdalla TSA, Giannou AD, Abdalla ASA, et al. The effect of non‐alcoholic fatty liver disease on weight loss and resolution of obesity‐related disorders after bariatric surgery. World J Surg. 2023;47(12):3281–3288. doi:10.1007/s00268-023-07153-8
27. Mantovani A, Byrne CD, Bonora E, Targher G. Nonalcoholic fatty liver disease and risk of incident type 2 diabetes: a meta-analysis. Diabetes Care. 2018;41(2):372–382. doi:10.2337/dc17-1902
28. Ziolkowska S, Binienda A, Jablkowski M, Szemraj J, Czarny P. The interplay between insulin resistance, inflammation, oxidative stress, base excision repair and metabolic syndrome in nonalcoholic fatty liver disease. Int J Mol Sci. 2021;22(20):11128. doi:10.3390/ijms222011128
29. Mathurin P, Gonzalez F, Kerdraon O, et al. The evolution of severe steatosis after bariatric surgery is related to insulin resistance. Gastroenterology. 2006;130(6):1617–1624. doi:10.1053/j.gastro.2006.02.024
30. Chen Z, Yu R, Xiong Y, Du F, Zhu S. A vicious circle between insulin resistance and inflammation in nonalcoholic fatty liver disease. Lipids Health Dis. 2017;16(1):203. doi:10.1186/s12944-017-0572-9
31. Sabench F, Rusu EC, Clavero-Mestres H, et al. Metabolic-associated fatty liver disease and weight loss after bariatric surgery: a systematic review and meta-analysis. Obes Surg. 2024;34(12):4459–4471. doi:10.1007/s11695-024-07585-8
32. Gehrke N, Schattenberg JM. Metabolic inflammation-a role for hepatic inflammatory pathways as drivers of comorbidities in nonalcoholic fatty liver disease? Gastroenterology. 2020;158(7):1929–1947e1926. doi:10.1053/j.gastro.2020.02.020
33. Armstrong MJ, Gaunt P, Aithal GP, et al. Liraglutide safety and efficacy in patients with non-alcoholic steatohepatitis (LEAN): a multicentre, double-blind, randomised, placebo-controlled Phase 2 study. Lancet. 2016;387(10019):679–690. doi:10.1016/S0140-6736(15)00803-X
34. Beygi M, Ahi S, Zolghadri S, Stanek A. Management of metabolic-associated fatty liver disease/metabolic dysfunction-associated steatotic liver disease: from medication therapy to nutritional interventions. Nutrients. 2024;16(14):2220. doi:10.3390/nu16142220
35. Elshaer A, Chascsa DMH, Lizaola-Mayo BC. Exploring varied treatment strategies for Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD). Life. 2024;14(7).
36. Nogueira JP, Cusi K. Role of insulin resistance in the development of nonalcoholic fatty liver disease in people with type 2 diabetes: from bench to patient care. Diabetes Spectr. 2024;37(1):20–28. doi:10.2337/dsi23-0013
37. Shen K, Singh AD, Modaresi Esfeh J, Wakim-Fleming J. Therapies for non-alcoholic fatty liver disease: a 2022 update. World J Hepatol. 2022;14(9):1718–1729. doi:10.4254/wjh.v14.i9.1718
38. De Robertis R, Spoto F, Autelitano D, et al. Ultrasound-derived fat fraction for detection of hepatic steatosis and quantification of liver fat content. Radiol Med. 2023;128(10):1174–1180. doi:10.1007/s11547-023-01693-8
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Insight on Semaglutide for Chronic Weight Management in Adults: Patient Selection and Special Considerations
Chao AM, Tronieri JS, Amaro A, Wadden TA
Drug Design, Development and Therapy 2022, 16:4449-4461
Published Date: 29 December 2022
Baseline Serum BCAAs are Related to the Improvement in Insulin Resistance in Obese People After a Weight Loss Intervention
Zhang C, Wang S, Wu Y, Guo Y, Wang X
Diabetes, Metabolic Syndrome and Obesity 2023, 16:179-186
Published Date: 19 January 2023
The Evaluation of Serum Endocan, Interleukin-6, and CRP Levels Following Sleeve Gastrectomy
Turkmen Sariyildiz G, Cicek Demir C, Demir ME, Arslan Aİ, Banli O, Dursun AD
International Journal of General Medicine 2023, 16:4737-4744
Published Date: 19 October 2023
Comparing Lifestyle and Behavior of Post-Bariatric Surgery and Participants with Obesity: A Community-Based Cross-Sectional Study
Althumiri NA, BinDhim NF, Aldabaeab AE, AlMousa N, Aljabbary RA, Alumran A
Diabetes, Metabolic Syndrome and Obesity 2024, 17:31-44
Published Date: 3 January 2024
Assessing the Impact of Bariatric Surgery on Quality of Life in the Saudi Population: A Systematic Review
Alqhtani H
Diabetes, Metabolic Syndrome and Obesity 2026, 19:572545
Published Date: 13 February 2026