Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 17
Comparing Lifestyle and Behavior of Post-Bariatric Surgery and Participants with Obesity: A Community-Based Cross-Sectional Study
Authors Althumiri NA, BinDhim NF, Aldabaeab AE, AlMousa N, Aljabbary RA, Alumran A ![]()
Received 14 September 2023
Accepted for publication 28 December 2023
Published 3 January 2024 Volume 2024:17 Pages 31—44
DOI https://doi.org/10.2147/DMSO.S440209
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Konstantinos Tziomalos
Nora A Althumiri,1,2 Nasser F BinDhim,1,2 Abdulaziz E Aldabaeab,3 Norah AlMousa,2 Ruqayah Ahmed Aljabbary,2 Arwa Alumran4
1Scientific Department, Informed Decision Making (IDM), Riyadh, Saudi Arabia; 2Scientific Department, Sharik Association for Research and Studies, Riyadh, Saudi Arabia; 3Obesity Department, King Fahad Hospital of the Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 4Health Information Management and Technology Department, College of Public Health, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
Correspondence: Nora A Althumiri, Email [email protected]
Background: There is a paucity of research dedicated to exploring behavioral change in patients following bariatric surgery. However, there is a need for comparison analysis of individuals with obesity who have received surgical treatment and those who have not opted for any surgical procedures for weight loss. This study is designed to scrutinize the lifestyle choices, behavioral patterns, psychological elements, and eating habits of individuals who have undergone bariatric surgery, in contrast to those with obesity who have not undergone such a procedure.
Methods: This study is a secondary analysis from Sharik Diet and Health National Survey (SDHNS) dataset, which is a cross-sectional investigation covering the period from 2020 to 2022. The study focused on demographic factors like age, gender, educational attainment, and monthly earnings. Furthermore, other variables such as physical activity, leisure and workplace sitting habits, smoking patterns, strategies for managing weight, and eating and consumption behaviors were also examined.
Results: Out of the initial 15,980 participants reached, 4,069 satisfied the study’s inclusion criteria. Bariatric surgery was reported by 806 participants (19.8%). Upon comparing three obesity status groups - The participants who underwent bariatric surgery with or without obesity, those with obesity who did not opt for any surgical weight loss measure, the analysis found that the three obesity status groups were significantly different in 21 variables from a total of 26. Moreover, a logistic regression analysis revealed that 11 variables influenced persistent obesity in the post-surgery phase, as opposed to those who successfully lost weight. These variables included advanced age, limited education, being female, lower income, waterpipe smoking habits, and the consumption of carbonated drinks.
Conclusion: This study showed that inability to lose weight after bariatric surgery are linked to poor lifestyle choices and behavior compared to those who were able to lose weight after the surgery.
Keywords: bariatric surgery, obesity, weight recurrence, weight loss, weight loss intervention
Introduction
The escalating issue of obesity is generating significant public health concerns, and the complications associated with it are leading to a considerable decline in both the quality and expectancy of life.1 As of 2020, the occurrence rate of obesity, defined by a Body Mass Index (BMI) of 30 or higher, in Saudi Arabia was recorded at 21.7%.2 In Saudi Arabia, a significant correlation has been observed in previous study between obesity and several health disorders such as Type 2 Diabetes Mellitus (T2DM), high cholesterol, high blood pressure, pulmonary diseases, rheumatoid arthritis, sleep disorders, colon-related diseases, and thyroid problems.2 The economic burden linked to obesity management in Saudi Arabia is also substantial, constituting about 2.4% of its total GDP, which is approximately 19 billion USD.3 This cost is projected to escalate to 4.1% of the GDP by 2060, amounting to USD 78 billion, if no measures are implemented to address the issue.3
In the last decade many global strategies for weight loss were initiated such as behavioral, therapeutical, and surgical interventions.4 These interventions are administered within a multidisciplinary framework, involving collaborative efforts from a team comprising dietitians, physiotherapists, endocrinologists, and in certain cases, surgeons.4 Nevertheless, the government of Saudi Arabia, in partnership with the Quality-of-Life Program 2020, is initiating various efforts focused on obesity management. These efforts encompass the Obesity Control Program, the Child Obesity Control Program, initiatives to boost physical activity levels among women, promotion of women’s participation in sports clubs, and the establishment of academic degrees and programs specializing in sports. Collectively, these initiatives aim to achieve a 3% reduction in obesity rates by the year 2030.5
Nevertheless, weight loss surgery, also referred to as bariatric or metabolic surgery, stands as the most effective and enduring method for treating obesity.4,6 Weight loss surgeries, encompassing procedures like sleeve gastrectomy, gastric bypass, duodenal switch, and gastric band, have demonstrated beneficial outcomes in managing conditions such as diabetes, hypertension, hypercholesterolemia, OSA syndrome among various other diseases.6,7 In Saudi Arabia, there are around 20 accredited public obesity centers dedicated to performing weight loss surgeries.8 In the year 2021, these obesity centers in Saudi Arabia carried out over 30,000 weight loss surgeries, with the average cost per surgery ranging between USD 6,600 and USD 10,000. The total expenditure for these procedures surpassed USD 100 million.8 These surgical procedures constitute 10% of the annual budget of the Ministry of Health.3 Additionally, in late 2022, the Saudi Council of Health Insurance (SCHI) implemented a new policy requiring all private health insurance companies to include coverage for bariatric surgery for individuals with a Body Mass Index (BMI) of 30 or higher. The coverage is capped at a maximum cost of USD 5,000, with a deductible of 20%.9 However, there were no valuable data regarding the number of surgeries conducted within private hospitals or centers.
The International Federation for the Surgery of Obesity and Metabolic Disorders recorded a total of 278,581 initial bariatric surgeries and 32,860 follow-up revision surgeries globally in the year 2022.10 The United States accounted for the majority, with an estimated 149,520 procedures.10 Notably, the report highlights the absence of data from Saudi Arabia, as it is not listed among the registered countries within IFSO countries. However, within Middle Eastern countries, only Kuwait is registered and has reported 24 bariatric surgery procedures, of which a significant majority (96%) were sleeve gastrectomy.10 The report also predict that 100% of bariatric surgery performed in Saudi Arabia is sleeve gastrectomy.10 However, in 2018, the (IFSO) reported a total of 4,231 bariatric surgery procedures, as documented by only three centers in Saudi Arabia.10 This accounts for merely 10% of all the centers performing bariatric surgeries in Saudi Arabia.10
The rate of surgical revisions after initial obesity surgery differs widely, from 5% for Biliary Pancreatic Diversion (BPD) to as much as 50% for Laparoscopic Gastric Band (LAGB). Procedures like Laparoscopic Sleeve Gastrectomy (LSG) and Roux-en-Y Gastric Bypass (RYGB) see revision frequencies that are intermediate, particularly within a timeframe of 3 to 5 years. Factors contributing to this include genetic predispositions, unhelpful eating habits, and suboptimal initial surgical choices, among others.11 Moreover, surgeries for revision or conversion tend to have a higher rate of complications compared to the initial obesity surgeries.11 Studies on post-bariatric surgery have predominantly centered on aspects such as comorbidity and morbidity, recurrence of weight, recovery time, progression in percentage of weight loss, performance, and both short- and long-term complications.
However, there has been limited research on the behavioral changes in individuals who have undergone such surgery, particularly in comparison with individuals with obesity who have not undergone surgical intervention. One study published data comparing lifestyle behaviors and dietary intake among individuals who were obese and non-obese, following bariatric surgery.12 The study found that factors such as age, reduced consumption of fresh juices and chicken, and current tobacco use were significantly associated with persistent obesity.12
Therefore, the aim of this research is to explore the lifestyle attributes, psychological health aspects, and dietary patterns of individuals following bariatric surgery. This analysis is to be compared with similar factors in individuals with obesity who have not undergone any weight-loss surgery.
Methodology
Study Design
This research project is a secondary analysis of data obtained from the nationwide Sharik Diet and Health National Survey (SDHNS),13 an annual, cross-sectional survey launched in Saudi Arabia in 2020. The survey collects data through Arabic telephone interviews. For this specific study, we used data covering the period from 2020 to 2022, which included more than 15,000 research entries. The thorough scientific approach of the SDHNS is elaborated on in a different publication by the Sharik Association for Research & Studies.13
Sampling and Sample Size
The SDHNS used a quota sampling strategy to ensure a balanced sample, distinguished by age, gender, and geographical location within the 13 administrative divisions of Saudi Arabia. Participants were divided into two age cohorts, with the dividing line set at the median adult age in Saudi Arabia, which is 36 years. The size of the sample was determined to accommodate the desired level of sub-analysis, which entailed comparing different age and sex cohorts across various regions. The aim was to target a medium effect size of roughly 0.26, with a statistical power of 80% and a confidence interval of 95%.14
The proportional sample method is automated, managed by data collection, ZDataCloud ® governance system without human intervention, which further decreases sampling bias.15 Since this research utilized ZdataCloud® as data collection, no missing values were present. To explain this point, (SDHNS) is structured around a telephone interview process conducted by trained interviewers. Concurrently, managing a database of participants is another operation within the organization. This operation is aimed at registering potential research participants and educating them about the importance of research participation, adherence to research ethics, and the significance of data quality. Established in 2015, Sharik currently maintains a database with more than 200,000 potential research participants, accurately representing the population of Saudi Arabia. Additionally, the ZDataCloud system includes a feature for data integrity validation. This feature, serving as a protective measure, aims to prevent any erroneous data entry by the data collectors and to reduce the occurrence of missing data.15
Inclusion Criteria
For this study, we included only the records of individuals who are with obesity (BMI ≥ 30) and those who have undergone bariatric surgery.
Measurement
The SDHNS published an English-translated copy of the code-book including all the variables and questions used in the survey.13
Demographics
Information regarding demographics, including age, gender, educational attainment, and monthly income, was sourced from the SDHNS database. Obesity was defined as a Body Mass Index (BMI) of 30 kg/m^2 or more, based on self-reported height and weight data.
Regarding bariatric surgery, data was gathered by inquiring if participants had undergone the surgery and the time elapsed since the operation. Responses about the surgery’s duration were limited to single-choice options: within the last three months, between 3–6 months, 6–9 months, and over one year.
Lifestyle and Eating Behavior
The primary variables examined included physical activity, leisure sitting, office sitting, smoking, weight management practices, and dietary and consumption habits. Physical activity levels were determined through self-reports, focusing on the frequency of weekly engagement in physical activities. Using the World Health Organization (WHO) standards, physical activity was classified as moderate (involving at least 150 minutes of moderate physical activity per week) or vigorous (comprising at least 75 minutes of vigorous physical activity per week).16 The variable of physical activity was categorized into either an acceptable level of physical activity (ALPA) if it met either of the criteria, or a low level of physical activity (LLPA) if it met neither. The degree of a sedentary lifestyle was assessed based on the daily hours spent sitting for leisure, like watching TV or playing video games, or sitting during office work. This was divided into two groups: (1) sitting for 4 hours or less per day; (20 sitting for more than 4 hours/day.
Self-Rated Health and Mental Health
The study assessed the participants’ perception of their health status using a 5-point Likert scale, with 1 indicating ‘poor’ and 5 indicating ‘excellent’. The prevalence of a high risk for depression and anxiety within the study group was evaluated using the Patient Health Questionnaire (PHQ-9) with cut-off score > 10 and the Generalized Anxiety Disorder (GAD-7) with cut-off score ≥ 10.17
Statistical Analysis
The analysis of the data was carried out using frequencies and percentages to outline the study variables. The bivariate analysis was facilitated by the chi-square (χ2) test. As data collection was electronic, there was no missing data. SPSS version 22 was used for the statistical analysis. A backward maximum likelihood multivariate logistic regression model, including all variables, was used to identify factors significantly linked to bariatric surgery. All tests were conducted at a 95% confidence level to evaluate significance. The communication of results followed the guidelines set by the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) for cross-sectional studies.
Ethical Considerations
The study was approved by the ethics committee of the Sharik Association for Health Research (Approval no.06-2021), in compliance with national research ethics guidelines. Informed consent from participants was obtained verbally during telephone interviews and appropriately documented in our data collection system. This method not only ensured informed consent but also aligned with the study’s methodology. We affirm that this study is conducted in accordance with the Declaration of Helsinki.
Results
From the SDHNS data spanning 2020 to 2022, out of 15,980 potential respondents, 4,069 qualified for inclusion in the study. Among them, 56.9% were female. The mean age was 40.67 years with a standard deviation of 12.84. Notably, 55.9% had an education level below a bachelor’s degree. More than 60% reported a monthly income not exceeding SAR 8000. Regarding bariatric surgery 806 (19.8%) participants had the surgery, 10.2% underwent the procedure in the last 3 months, 11.9% between 3 and 6 months ago, 9.8% between 6 and 9 months ago, and the majority, 68.1%, had their surgery over a year ago.
Three Groups Comparison (Bariatric Surgery with Obesity, Bariatric Surgery Without Obesity, Participants with Obesity)
In this section, we compared three groups based on their obesity status - those who underwent bariatric surgery (both with and without obesity), and those suffering from obesity but have not had surgery. The comparison was made across various domains, including sociodemographic factors, lifestyle habits, attitudes, mental health elements, and dietary habits.
Table 1 in the report offers a comparative analysis of participant demographics across the three obesity status groups. The analysis revealed significant differences among the groups in terms of age, education level, and income.
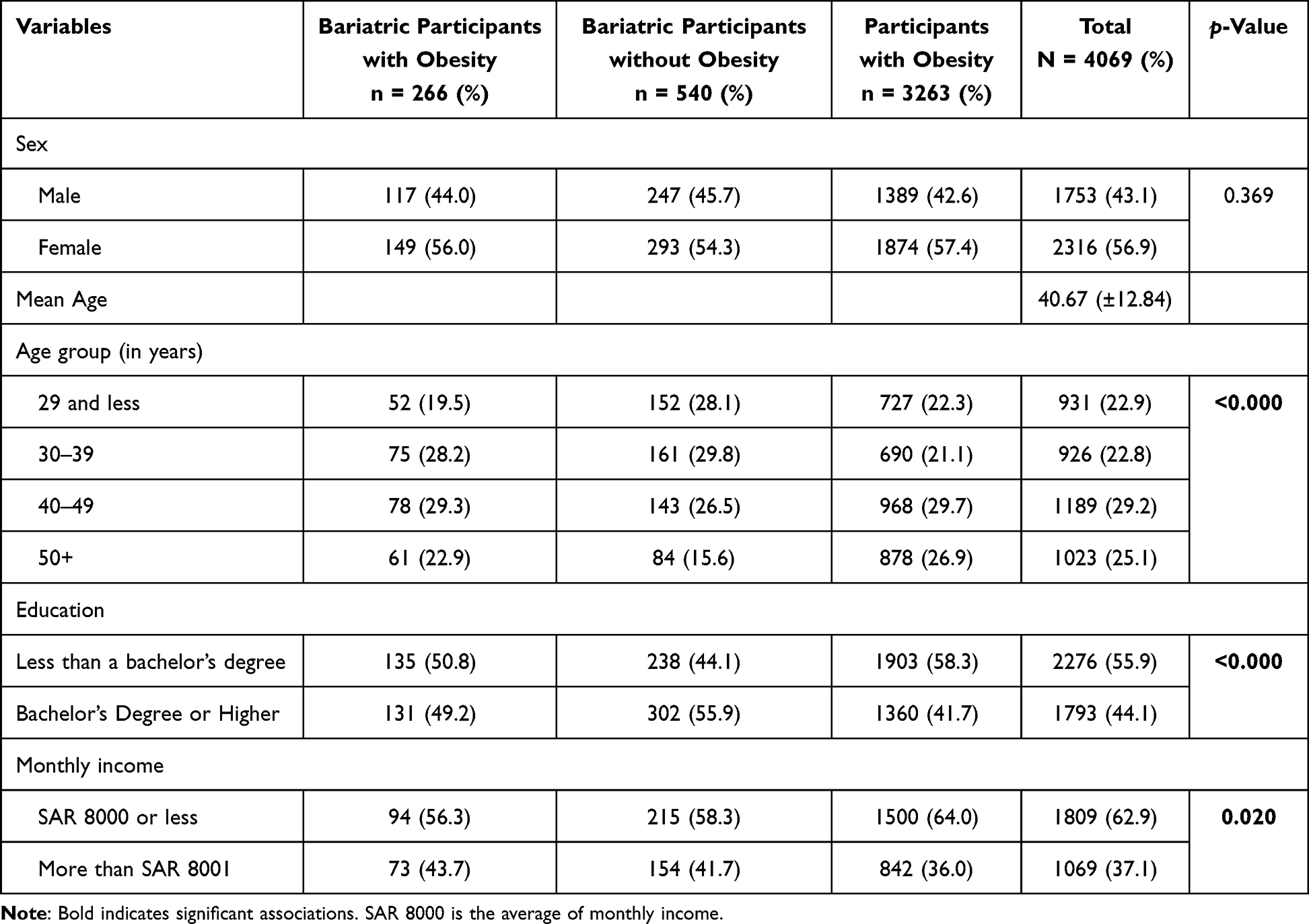 |
Table 1 Participant Sociodemographic Characteristics |
Table 2 shows the lifestyle habits of the different groups studied, covering aspects such as the intensity of physical activity, duration of sedentary behaviors, smoking habits, and frequency of eating out. The analysis found significant differences among the three obesity status groups in terms of their physical activity, current cigarette smoking, current waterpipe smoking, efforts toward weight management, consumption of pre-prepared food (in the past week), and frequency of breakfast meals. (in the past week)
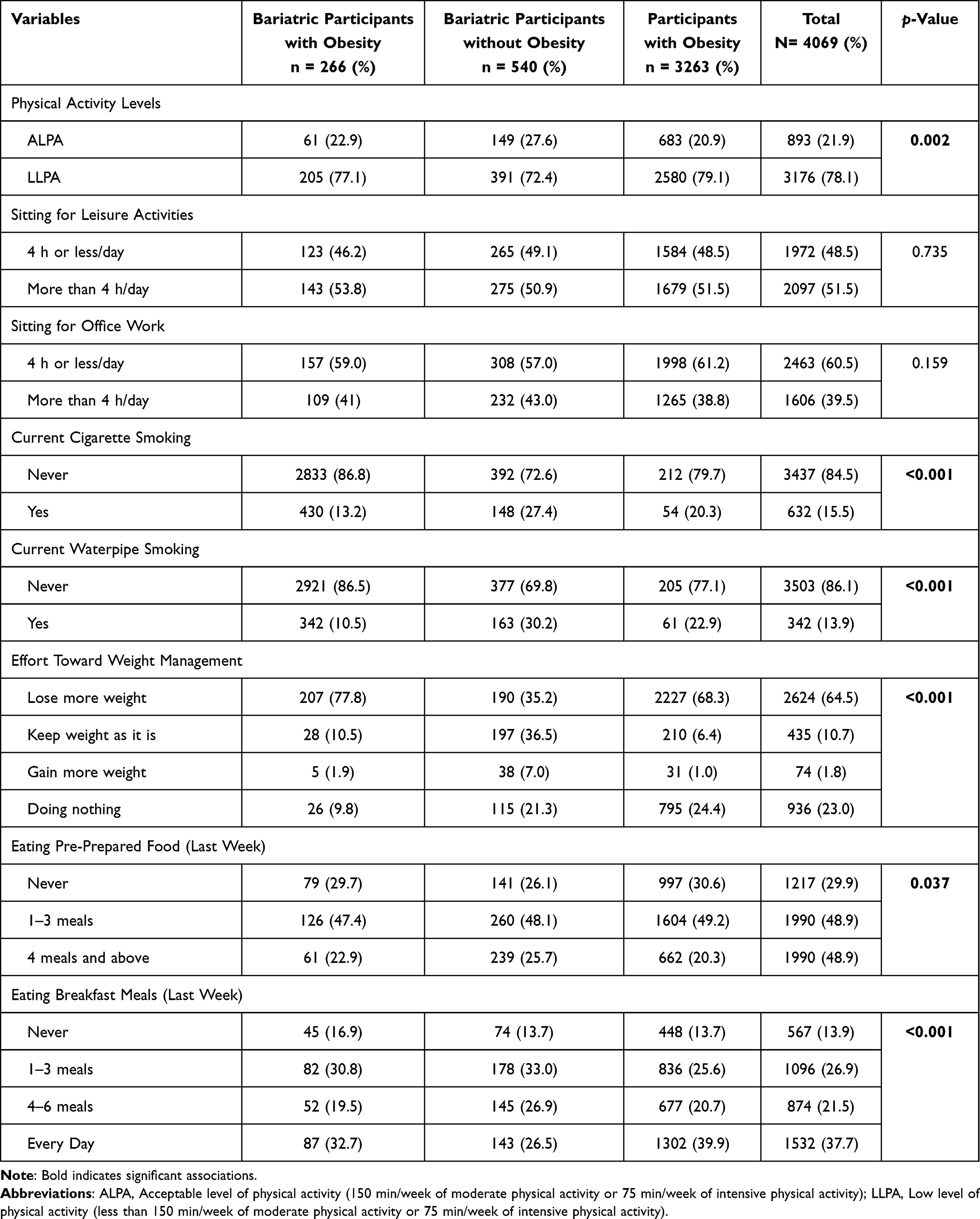 |
Table 2 Participant Lifestyle Characteristics |
Table 3 provides an analysis of attitudes and mental health elements across all three groups. It considers factors like the likelihood of anxiety and depression, overall health self-rated satisfaction, and self-perception of weight. The results indicated that the three obesity status groups significantly differed in terms of their overall health self-satisfaction rating, self-classification of weight, risk of anxiety, risk of depression, and combined risk of anxiety and depression.
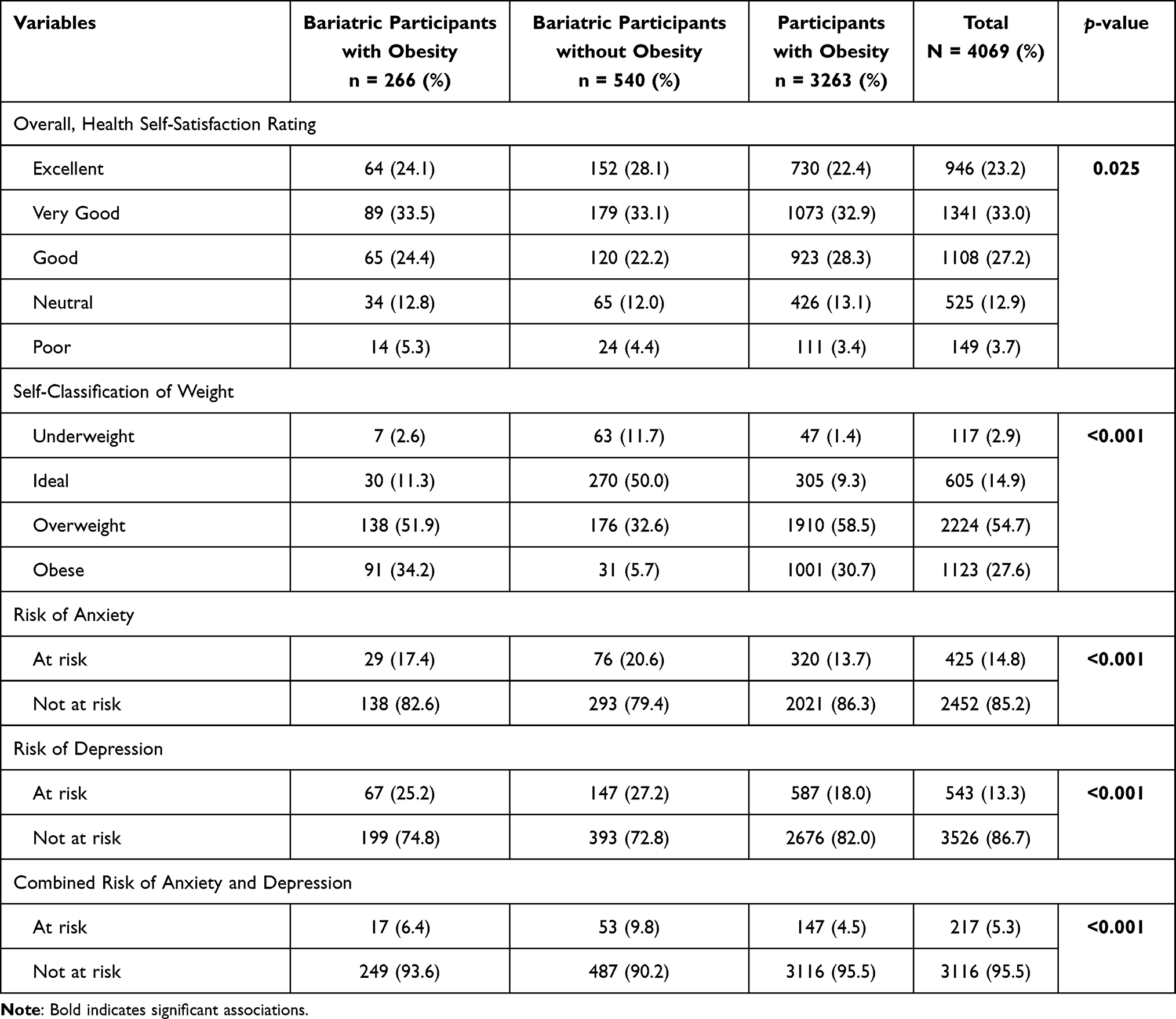 |
Table 3 Perceptions of Health and Mental Health Factors |
Finally, Table 4 offers an examination of the dietary habits of the groups, including the consumption of various food and beverage items such as fruits, vegetables, meats, chicken, seafood, soft drinks, energy drinks, fresh and canned juices. The analysis found that the three obesity status groups were significantly different in their levels of consumption for several items, including fruits, vegetables, chicken, natural juice, canned juice, carbonated drinks, and energy drinks.
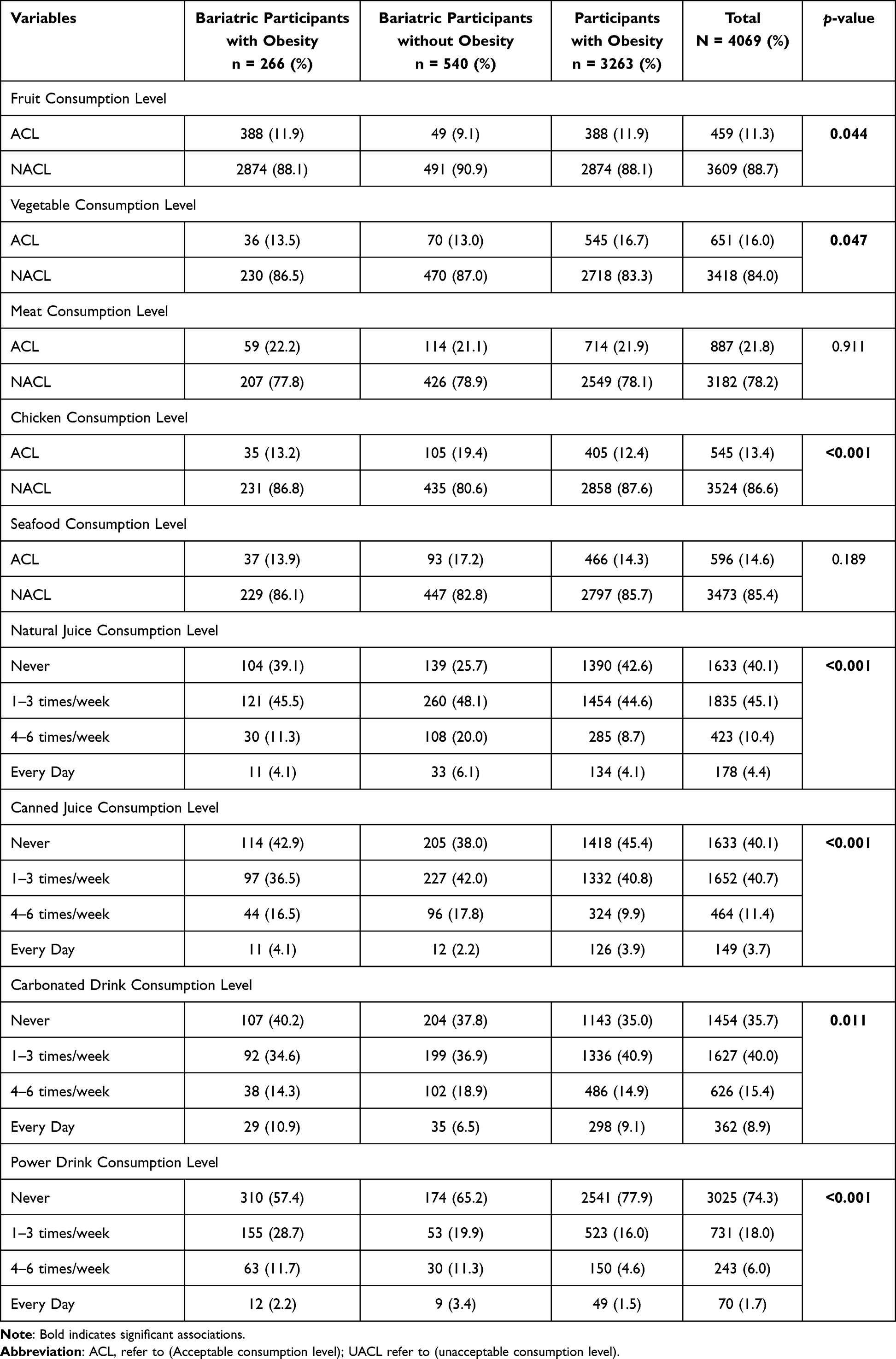 |
Table 4 Dietary Lifestyle and Behaviors |
Two Groups Comparison (Bariatric Surgery and Participants with Obesity and Had Not Had Bariatric Surgery)
In a chi-square analysis we explored the 22 lifestyle and behavior variables including participants who had bariatric surgery and participants with obesity who had not undergone any surgery for weight loss. Eighteen variables were found to have significant differences between these two groups. These variables are: physical activity (χ²(1) = 9.90, p =.002), currently smoking cigarette (χ²(1) = 122.18, p <.001), currently smoking waterpipe (χ²(1) = 206.83, p <.001), effort toward weight management (χ²(3) = 396.70, p <.001), eating pre-prepared food (last week) (χ²(2) = 8.75, p =.013), eating breakfast meals (last week) (χ²(3) = 37.35, p <.001), Overall Health Self-Satisfaction Rating (χ²(4) = 15.56, p =.004), self-classification of weight (χ²(3) = 557.59, p <.001), risk of anxiety (χ²(1) = 12.14, p <.001), risk of depression (χ²(1) =70.21, p <.001), combined risk of anxiety and depression (χ²(1) =22.36, p <.001), fruit consumption level (χ²(1) = 6.14, p =.013), vegetable consumption level (χ²(1) = 6.06, p =.014), chicken consumption level (χ²(1) =13.69, p <.001), natural juice consumption level (χ²(3) =72.45, p <.001), canned juice consumption level (χ²(3) =38.16, p <.001), carbonated drink consumption level (χ²(3) = 9.68, p =.021), power drink consumption level (χ². (3) =118.74, p <.001)
Multivariate Analysis of Factors Linked to Continued Obesity After Bariatric Surgery
Table 5 details a logistic regression analysis aimed at identifying factors linked to continued obesity after bariatric surgery, in contrast to individuals who effectively managed to overcome obesity following surgery. The analysis pinpointed key elements influencing ongoing obesity in the post-surgery phase, such as advanced age, limited educational attainment, female gender, reduced income, waterpipe smoking habits, and the consumption of carbonated drinks.
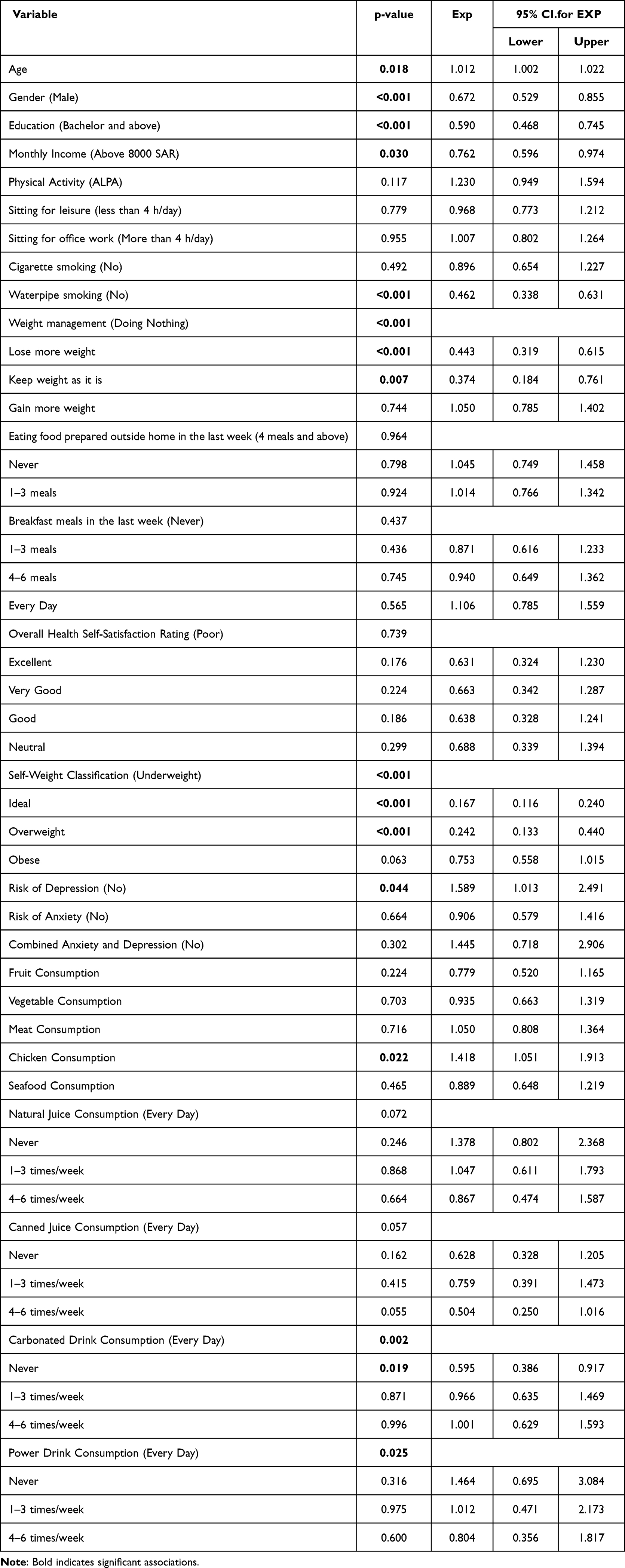 |
Table 5 Logistic Regression Model Results Showing Lifestyle and Behavioral Factors Associated with Obesity in Contrast to Individuals Who Effectively Managed to Overcome Obesity Following Surgery |
Discussion
In this study, when the analysis was conducted comparing three obesity status groups - those who had bariatric surgery regardless of their obesity status, and those who were obese but did not choose surgical weight loss options, it was found that out of 26 variables, 21 showed significant differences among the three groups. In addition, twenty-two lifestyle and behavior variables were tested in two groups: participants who had bariatric surgery and participants with obesity who had not undergone any surgery for weight loss. Eighteen variables were found to have significant differences between these two groups. This study primarily investigated lifestyle and behavior changes among participants who have undergone bariatric surgery for obesity, irrespective of surgery type, and compared them with participants with obesity who had not had any type of weight-loss surgery. To our knowledge, this is one of first studies that compared lifestyle factors of those participant who have undergone bariatric surgery and participants with obesity who have not had any surgery.
The present study showed that participants who have undergone bariatric surgery tend to exercise and engage in physical activity more than those who have not had the surgery. At the same time, when asked about their current plan regarding their weight, more participants in the bariatric surgery group answered that they are trying to lose weight or maintain their current weight. A few studies have presented similar findings and we were not able to identify any studies that reported a prevalence of ALPA among people who had bariatric surgery.18 In fact, there is no guideline on the minimum or recommended level of physical activity for those participants who had bariatric surgery, or even for participants with obesity. In addition, sedentary behaviors expressed as leisure sitting hours were not significant in the two groups, which indicated that the majority of participants from both groups kept the same inactivity levels. Sedentary lifestyle and inactive behavior in participants with obesity is well studied in the literature, but only limited studies have been conducted on participants post bariatric surgery.19,20 All of this raises the need for developing specific guidelines on sedentary and physical activity for both groups. In addition, the WHO recommendations for physical activity seem to underestimate the physical activity level needs of overweight and participants with obesity. Their recommendations seem appropriate for people considered normal or underweight. Thus, a need exists to re-evaluate the minimum recommended level of physical activity to prevent overweight and obesity in general.
Both cigarette and waterpipe smoking were significantly higher in bariatric participants. This finding was similar to other studies.21 Although smoking has little to no effect on weight recurrence, many studies have indicated that smoking in relation to bariatric surgery was significantly associated with short- and long-term complications and morbidity.22 A systematic review suggested that smoking 1 year after bariatric surgery is associated with significant postoperative morbidity.23,24 Smoking cessation may minimize the risk of adverse effects after surgery.21 The high prevalence of waterpipe smoking among bariatric participants may also explain the high sitting leisure hours in the same group.
The outcomes of this study corroborate previous research indicating that individuals undergoing bariatric surgery may face an increased risk of psychological conditions, including anxiety and depression, and may exhibit maladaptive eating behaviors. Previous studies have similarly found an increased incidence of mental health conditions in this population.25 For instance, a meta-analysis showed that the prevalence of depression and anxiety in bariatric surgery patients was significantly higher than in the general participants with obesity population.26 This study results further illuminates the complex relationship between mental health risks and dietary lifestyle and behaviors in bariatric surgery patients. The increased psychological distress observed in this study may lead to poor eating behaviors. This resonates with the previous findings reported that emotional distress was linked to uncontrolled and emotional eating in postoperative bariatric patients.27 The physiological basis for these behaviors may lie in the body’s response to stress and how it affects eating habits. When the body is in a state of chronic stress or depression, it releases the hormone cortisol, which can stimulate appetite and promote fat storage.28 This biological reaction, coupled with psychological tendencies to engage in emotional eating or food binges during periods of distress, could explain the maladaptive eating behaviors observed in this study. Understanding these physiological and psychological processes is crucial to optimizing postoperative care for bariatric surgery patients. By identifying the links between anxiety, depression, and poor eating behaviors, healthcare providers can develop targeted interventions to address these issues and improve patient outcomes.
Although bariatric participants are advised to restrict calories by avoiding fatty and unhealthy meals, sweetened drinks, fruit drinks, sodas, and power drinks, the data from this study showed frequent consumption multiple times per week of food prepared outside the home, natural juices, canned juices, and power drinks. In addition, low consumption of both whole fruits and vegetables was shown. In fact, the association between eating prepared food and fast food and the severity of post-bariatric obesity has been investigated in the literature. Many studies have shown that a nutritionally poor diet and consuming high calories meals might reflect later as weight recurrence in postoperative individuals.29–31
Eating changes and behavioral therapy are necessary for all participants with obesity who attempt to lose weight using nonsurgical and surgical interventions. Behavioral and eating changes may have satisfying results. As matter of fact, in a previous study, results were compared to data from a clinical trial of participants with obesity and overweight people who followed nonsurgical intervention or behavioral intervention for six months where they concluded that 60% to 70% of participant who followed behavioral intervention programs lost more than 5% of their weight, while only 50% or less of the participants who had bariatric surgery only lost less than 5% of their weight.31
The logistic regression analysis aimed to explore the factors associated with obesity in the post-operative period following bariatric surgery, in comparison with individuals who successfully achieved weight loss after the procedure. The findings demonstrated that age, lower educational attainment, being female, having a lower income, engaging in waterpipe smoking, and consuming carbonated beverages were significant variables contributing to post-surgical obesity26,32 This aligns with previous research, indicating that sociodemographic factors, behavioral issues, and lifestyle habits can significantly impact weight loss outcomes after bariatric surgery.26 Therefore, it is crucial to consider these factors and provide comprehensive pre-surgical assessments and support to optimize long-term weight management in bariatric surgery patients.33
This study acknowledges certain limitations that should be highlighted. Firstly, the use of secondary data from a cross-sectional study design, while providing a comprehensive analysis, does not establish definitive cause-and-effect relationships between bariatric surgery and the psychological and behavioral outcomes assessed. Being a one-time assessment, it is difficult to determine whether the surgery directly influenced these outcomes or if they were pre-existing conditions. Secondly, this study relies on secondary data analysis, which allows for larger sample sizes and efficiency but limits the exploration of data to the variables and measures already present in the dataset. It is possible that some potentially relevant factors were not included. Moreover, the sample used in this study may not accurately represent the entire population of individuals in Saudi Arabia who have undergone bariatric surgery in terms of generalizability. Furthermore, we acknowledge the importance of BMI as a universally recognized and widely used metric in the categorization of obesity. In our study, BMI was employed as the primary measure for several reasons: 1) standardization and comparability: BMI provides a standardized method for classifying obesity, allowing for comparability across different studies and population; 2) availability and accessibility: In the dataset utilized for our study, BMI was the only available measure for obesity categorization for phone interview and 3) consistency with previous studies employing BMI aligns our methodology with existing literature, enabling us to draw parallels and contribute more effectively to the ongoing discourse in the field of obesity research.
Conclusions
In this secondary analysis research, we compared 22 lifestyle and behavioral variables between two groups: those who underwent bariatric surgery and those with obesity who did not have surgery. Out of these variables, 18 showed a significant disparity between the two groups. The group that underwent bariatric surgery had more challenging issues than the group with obesity in areas such as cigarette and waterpipe smoking, eating food prepared outside the home, missing breakfast, as well as risks of anxiety and depression. Their consumption of fruits and vegetables was also less. The study also identified notable differences among three obesity status groups. These findings highlight the potential for crafting targeted interventions to prevent future health issues like weight regain. By incorporating these insights into post-surgery care, we aim to improve the long-term health outcomes for individuals who have had bariatric surgery. This would ultimately reduce the impact of obesity and enhance the quality of life for these patients.
Informed Consent Statement
All study participants provided their informed consent.
Funding
No external funding was procured for this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. O’Brien PE. Bariatric surgery: mechanisms, indications and outcomes. J Gastroenterol Hepatol. 2010;25(8):1358–1365. doi:10.1111/j.1440-1746.2010.06391.x
2. Althumiri NA, Basyouni MH, AlMousa N, et al. Obesity in Saudi Arabia in 2020: prevalence, distribution, and its current association with various health conditions. In: Healthcare. MDPI; 2021.
3. Okunogbe A, Nugent R, Spencer G, et al. Economic impacts of overweight and obesity: current and future estimates for eight countries. BMJ Global Health. 2021;6(10):e006351. doi:10.1136/bmjgh-2021-006351
4. Castelnuovo G, Pietrabissa G, Manzoni GM, et al. Cognitive behavioral therapy to aid weight loss in obese patients: current perspectives. Psychol Res Behav Manag. 2017;Volume 10:165–173. doi:10.2147/PRBM.S113278
5. saudi GH. Top priorities in KSA’s healthcare sector. global health Saudi; 2023. Available from: https://www.globalhealthsaudi.com/en/overview/saudi-news/Top-priorities-in-KSAs-healthcare-sector.html.
6. Surgery, A.S.M.B. Bariatric Surgery Procedures; 2023. Available from: https://asmbs.org/patients/bariatric-surgery-procedures.
7. Puzziferri N, Roshek TB, Mayo HG, et al. Long-term follow-up after bariatric surgery: a systematic review. JAMA. 2014;312(9):934–942. doi:10.1001/jama.2014.10706
8. al-Mutairi INAA. Cutting the fat: more than 30,000 gastric sleeve surgeries in Saudi Arabia in 2020. In: English alarabiya. Alarabiya: english.alarabiya; 2021.
9. Al-Johani DN, Health insurance coverage for bariatric surgery from Oct. 1, O.S. gazette, editor. okaz/Saudi gazette: okaz/Saudi gazette; 2022.,
10. 7th IFSO global registry report; 2022.
11. England, N.H.S.N.i.. Appendix 8 guidance for clinical commissioning groups (CCGs): clinical guidance: revision surgery for complex obesity. Obes. Sci. Pract. 2016; 9(5):538–47.
12. Althumiri NA, Bindhim NF, Aldabaeab AE, et al. Comparative analysis of lifestyle behaviors and dietary intake among obese and non-obese individuals following bariatric surgery: a secondary data analysis from 2020 to 2022. Front Nutr. 2023;10:1.
13. Studies, S.A.F.R.a. The sharik diet and health national survey 2023; 2023. Available from: https://sharikhealth.com/attachments/article/89/diet-and-health-survey.pdf.
14. Cohen J. Statistical Power Analysis for the Behavioral Sciences. Academic press; 2013.
15. zdatacloud; 2021 Available from: https://zdatacloud.com/.
16. World Health Organization. Physical activity; 2020 Available from: https://www.who.int/news-room/fact-sheets/detail/physical-activity.
17. BinDhim NF, Althumiri NA, Basyouni MH, et al. Saudi Arabia Mental Health Surveillance System (MHSS): mental health trends amid COVID-19 and comparison with pre-COVID-19 trends. Eur J Psychotraumatology. 2021;12(1):1875642. doi:10.1080/20008198.2021.1875642
18. Shah M, Snell PG, Rao S, et al. High‐volume exercise program in obese bariatric surgery patients: a randomized, controlled trial. Obesity. 2011;19(9):1826–1834. doi:10.1038/oby.2011.172
19. Heinonen I, Helajärvi H, Pahkala K, et al. Sedentary behaviours and obesity in adults: the cardiovascular risk in young finns study. BMJ open. 2013;3(6):e002901. doi:10.1136/bmjopen-2013-002901
20. Vioque J, Torres A, Quiles J. Time spent watching television, sleep duration and obesity in adults living in Valencia, Spain. Int J Obesity. 2000;24(12):1683–1688. doi:10.1038/sj.ijo.0801434
21. Mohan S, Samaan JS, Samakar K. Impact of smoking on weight loss outcomes after bariatric surgery: a literature review. Surg Endosc. 2021;35(11):5936–5952. doi:10.1007/s00464-021-08654-0
22. Kowalewski PK, Olszewski R, Walędziak MS, et al. Cigarette smoking and its impact on weight loss after bariatric surgery: a single center, retrospective study. Surg Obesity Related Dis. 2018;14(8):1163–1166. doi:10.1016/j.soard.2018.05.004
23. Yuce TK, Khorfan R, Soper NJ, et al. Post-operative complications and readmissions associated with smoking following bariatric surgery. J Gastrointestinal Surg. 2020;24(3):525–530. doi:10.1007/s11605-019-04488-3
24. Livingston EH, Arterburn D, Schifftner TL, et al. National surgical quality improvement program analysis of bariatric operations: modifiable risk factors contribute to bariatric surgical adverse outcomes. J Am Coll Surg. 2006;203(5):625–633. doi:10.1016/j.jamcollsurg.2006.07.006
25. Dawes AJ, Maggard-Gibbons M, Maher AR, et al. Mental health conditions among patients seeking and undergoing bariatric surgery: a meta-analysis. JAMA. 2016;315(2):150–163. doi:10.1001/jama.2015.18118
26. Marchitelli S, Ricci E, Mazza C, et al. Obesity and psychological factors associated with weight loss after bariatric surgery: a longitudinal study. Nutrients. 2022;14(13):2690. doi:10.3390/nu14132690
27. Meany G, Conceição E, Mitchell JE. Binge eating, binge eating disorder and loss of control eating: effects on weight outcomes after bariatric surgery. Eur Eat Disord Rev. 2014;22(2):87–91. doi:10.1002/erv.2273
28. Adam TC, Epel ES. Stress, eating and the reward system. Physiol Behav. 2007;91(4):449–458. doi:10.1016/j.physbeh.2007.04.011
29. Bastos ECL, Barbosa EMWG, Soriano GMS, et al. Determinants of weight regain after bariatric surgery. Arq Bras Cir Dig. 2013;26:26–32. doi:10.1590/S0102-67202013000600007
30. El Ansari W, Elhag W. Weight regain and insufficient weight loss after bariatric surgery: definitions, prevalence, mechanisms, predictors, prevention and management strategies, and knowledge gaps—a scoping review. Obes Surg. 2021;31(4):1755–1766. doi:10.1007/s11695-020-05160-5
31. King WC, Belle SH, Hinerman AS, et al. Patient behaviors and characteristics related to weight regain following roux-en-Y gastric bypass: a multicenter prospective cohort study. Ann Surg. 2020;272(6):1044. doi:10.1097/SLA.0000000000003281
32. Azhri AS, Almuqati A, Azzeh F, et al. Factors influencing body weight one year after bariatric surgery. Medicine. 2023;102(11):e33111. doi:10.1097/MD.0000000000033111
33. DiGiorgi M. Factors Associated with Long Term Weight Regain After Bariatric Surgery. Columbia University; 2012.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Insight on Semaglutide for Chronic Weight Management in Adults: Patient Selection and Special Considerations
Chao AM, Tronieri JS, Amaro A, Wadden TA
Drug Design, Development and Therapy 2022, 16:4449-4461
Published Date: 29 December 2022
Baseline Serum BCAAs are Related to the Improvement in Insulin Resistance in Obese People After a Weight Loss Intervention
Zhang C, Wang S, Wu Y, Guo Y, Wang X
Diabetes, Metabolic Syndrome and Obesity 2023, 16:179-186
Published Date: 19 January 2023
Effect of Weight Loss on the Apnea Hypopnea Index is Related to Waist Circumference in Chinese Adults with Overweight and Obesity
Ren Y, Cui X, Zhu X, Guo H, Zhou Q, Yuan P, Cheng H, Wu W
Diabetes, Metabolic Syndrome and Obesity 2024, 17:453-463
Published Date: 27 January 2024
Impact of Pathological Grades of Metabolic Dysfunction-Associated Steatotic Liver Disease on Weight Loss Following Laparoscopic Sleeve Gastrectomy
Qu YF, Wang K, Li Y, Cheng YG, Hu SY, Zhong MW
Diabetes, Metabolic Syndrome and Obesity 2025, 18:2547-2560
Published Date: 29 July 2025
Assessing the Impact of Bariatric Surgery on Quality of Life in the Saudi Population: A Systematic Review
Alqhtani H
Diabetes, Metabolic Syndrome and Obesity 2026, 19:572545
Published Date: 13 February 2026