Back to Journals » Journal of Pain Research » Volume 19
Hyperbaric Oxygen Therapy in Managing Chronic Pain Syndromes – A Systematic Review
Authors Leys AM ![]() , Hans GH
, Hans GH ![]() , Saldien V
, Saldien V ![]() , Wildemeersch D
, Wildemeersch D ![]()
Received 19 January 2026
Accepted for publication 11 March 2026
Published 24 March 2026 Volume 2026:19 597243
DOI https://doi.org/10.2147/JPR.S597243
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Anna-Maria Leys,1 Guy Henri Hans,2 Vera Saldien,1 Davina Wildemeersch2
1Department of Anesthesiology, University Hospital Antwerp, Antwerp, Belgium; 2Department of Pain Medicine, University Hospital Antwerp, Antwerp, Belgium
Correspondence: Anna-Maria Leys, University Hospital Antwerp, Drie Eikenstraat 655, Antwerp, 2650, Belgium, Email [email protected]; [email protected]
Background: Chronic pain is a major global health problem for which current treatments often provide insufficient relief. Tissue hypoxia and redox imbalance may contribute to its pathophysiology, prompting interest in hyperbaric oxygen therapy (HBOT) as a potential adjunctive treatment. This review evaluates the therapeutic effects of HBOT in adults with chronic pain syndromes.
Methods: A PRISMA-guided systematic review was conducted (MEDLINE, EMBASE, Cochrane Central Register of Controlled Trials; January 2000 - August 2025). Randomized controlled trials (RCTs) evaluating HBOT in adults with chronic pain were included. Primary outcomes were pain measures (intensity, distribution and sensitivity). Secondary outcomes included multidimensional pain-related outcomes (quality of life, functioning and psychological well-being), analgesic use, neuroimaging findings, and adverse events. Risk of bias was assessed using the Cochrane RoB 2 tool. Due to study heterogeneity, results were synthesized narratively.
Results: Eleven RCTs (480 participants) were included, predominantly involving fibromyalgia (n=8), with additional studies in complex regional pain syndrome (CRPS) (n=1), idiopathic trigeminal neuralgia (n=1) and radiation-induced brachial neuropathy (n=1). Sample sizes ranged from 17 to 71 participants. Most trials showed some concerns or high risk of bias, mainly due to subjective outcomes and lack of blinding. In fibromyalgia, HBOT showed consistent within-group improvements in pain, functioning, and quality of life, with some studies demonstrating between-group benefits. Limited evidence in CRPS and trigeminal neuralgia suggested possible benefit, whereas the trial in radiation-induced brachial plexopathy showed no meaningful improvement. HBOT was generally well tolerated, with mostly mild adverse events.
Conclusion: HBOT shows potential as an adjunctive intervention for selected chronic pain syndromes, particularly fibromyalgia. However, condition-specific effects, inconsistent superiority over controls, methodological limitations, protocol heterogeneity, and limited long-term follow-up constrain the strength of evidence. Larger, standardized trials with extended follow-up are needed before routine clinical implementation can be recommended.
Keywords: HBOT, chronic pain, functional outcomes, fibromyalgia, complex regional pain syndrome, trigeminal neuralgia
Introduction
Chronic pain, commonly defined as pain persisting beyond three months, represents a substantial global health challenge with profound individual, societal, and healthcare implications. According to the International Classification of Diseases (ICD-11) of the World Health Organization it encompasses both chronic primary pain syndromes – such as fibromyalgia and complex regional pain syndrome (CRPS) – and chronic secondary pain conditions, including neuropathic and cancer-related pain1,2 Across these conditions, patients experience substantial suffering, functional impairment, and reduced quality of life. The magnitude of this burden is further highlighted by epidemiological data, with a lifetime prevalence in Europe estimated between 12.7% and 33.7%, underscoring its relevance as a widespread public health concern and highlighting the ongoing need for more effective treatment strategies.3
Management of chronic pain remains particularly challenging, and treatment typically needs to be tailored to the individual patient. Current guidelines emphasize multimodal strategies that integrate pharmacological interventions – such as opioids, nonsteroidal anti-inflammatory drugs, and antidepressants – with non-pharmacological modalities, including exercise, transcutaneous electrical nerve stimulation (TENS), cognitive behavioral therapy, and patient education.4,5
Despite these efforts, outcomes frequently remain unsatisfactory, with treatment often failing to achieve adequate and sustained pain relief. For this reason, the continuous development and evaluation of novel therapeutic approaches aimed at improving long-term outcomes remain imperative.
Role of Hypoxia and Oxidative Stress
Evidence suggests that disturbances in tissue oxygenation and redox balance may contribute to the pathophysiology of chronic pain syndromes. Hypoxia and reactive oxygen species (ROS), which can arise from microvascular dysfunction, (prolonged) inflammation, or reduced perfusion, are thought to contribute to both peripheral and central sensitization.6
At the peripheral level, reduced tissue oxygen may lead to accumulation of hypoxia-inducible factor-1α (HIF-1α), which has been shown to upregulate pro-inflammatory cytokines (eg tumor necrosis factor-α (TNF-α) and interleukin-1β (IL-1β)), potentially enhancing nociceptor excitability.7,8 Hypoxia may also promote a shift toward anaerobic glycolysis, resulting in lactate accumulation and local acidosis, which in turn can activate proton-sensitive channels such as acid-sensing ion channels (ASICs) and transient receptor potential vanilloid 1 (TRPV1), potentially facilitating prolonged nociceptive signaling.9–11 In parallel, excessive ROS production has been observed to cause oxidative modification of ion channels and signaling proteins, lowering nociceptor activation thresholds and promoting ectopic discharges in peripheral fibers.
The resulting amplification of peripheral nociceptive input may alter pain processing within the central nervous system. In the dorsal horn of the spinal cord, sustained afferent signaling has been shown to increase glutamate release and N-methyl-D-aspartate (NMDA) receptor activation, initiating synaptic plasticity that promotes hyperexcitability.12,13 Meanwhile, hypoxia- and ROS-driven signals may also activate microglia and astrocytes, which produce pro-inflammatory mediators (eg IL-1β, TNF-α, IL-6). These glial-derived mediators can amplify excitatory transmission while impairing inhibitory gamma-aminobutyric acid (GABA) pathways, thereby disturbing the balance between excitation and inhibition in pain pathways.14–16 Together with ROS-induced changes in ion-channel expression and function in spinal neurons, these processes are hypothesized to reduce activation thresholds, resulting in prolonged excitatory responses.
Collectively, these hypoxia- and ROS-driven processes, mostly based on preclinical evidence, may establish a condition of sustained neuronal hyperexcitability, affecting both peripheral nociceptors and central pain circuits. This dual sensitization provides a potential neurobiological foundation for clinical manifestations such as hyperalgesia and allodynia, which are cardinal features observed across chronic pain syndromes.17–23
Hyperbaric Oxygen Therapy
Hyperbaric oxygen therapy (HBOT) involves the administration of 100% oxygen at pressures exceeding atmospheric pressure, typically ranging between 1.5 and 3.0 atmospheres absolute (ATA). This significantly increases the amount of oxygen dissolved in plasma, thereby improving tissue oxygenation in ischemic or inflamed areas. The physiological effects are thought to include reversal of hypoxia, suppression of HIF-1α-driven inflammatory pathways, reduction of excessive ROS production, stimulation of angiogenesis, and promotion of tissue repair. Collectively, these mechanisms may contribute to restoration of local homeostasis and may interrupt self-perpetuating cycles of hypoxia, oxidative stress, and inflammation.24,25
Although HBOT has been long established in clinical practice for conditions such as carbon monoxide poisoning, radiation injury, chronic wounds, and refractory infections,24 it has also received attention in the chronic pain field. This interest is driven by mechanistic preclinical evidence that hypoxia, oxidative stress, and inflammation may contribute to peripheral and central sensitization in chronic pain syndromes (as detailed above in the “Role of hypoxia and oxidative stress” subsection). Supporting this rationale, animal models have demonstrated that HBOT can reduce nociceptive hypersensitivity and neuroinflammatory responses, while also exerting direct antinociceptive effects through NO-dependent release of endogenous opioids.26–34 Building on these findings, clinical trials in conditions such as fibromyalgia and CRPS have emerged over the past decades, exploring HBOT as a potential pain management strategy.
Several systematic reviews and meta-analyses have evaluated the efficacy and safety of HBOT. However, these analyses have focused exclusively on fibromyalgia populations and have primarily emphasized quantitative pooling of pain measures.35–37 While statistical synthesis can provide valuable information, the small sample sizes, reliance on subjective outcomes, and heterogeneity in study designs limits the certainty of the available evidence according to established frameworks such as Grading of Recommendations Assessment, Development and Evaluation (GRADE).38
The present review therefore adopts a structured narrative approach to contextualize the available evidence and to identify clinically meaningful patterns that may not be fully captured through statistical aggregation alone. In addition, the scope of this review extends beyond fibromyalgia to systematically identify evidence across chronic pain syndromes and integrates a broader range of multidimensional outcomes.
Accordingly, the objective of this review is to evaluate the therapeutic effects of HBOT in adults with chronic pain syndromes compared with standard care or placebo, focusing primarily on pain intensity, distribution, and sensitivity. Secondary outcomes of interest include multidimensional pain measures – such as quality of life, global functioning, and psychological well-being – as well as analgesic consumption, neuroimaging findings, and adverse events.
Methodology
This systematic review was designed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.39
Data Sources and Search Strategy
A systematic search was performed in the databases MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials. The most recent update of this search was conducted on 22 August 2025. Search terms included “chronic pain”, “persistent pain”, “neuropathic pain”, “complex regional pain syndrome”, “CRPS”, “fibromyalgia”, “hyperbaric oxygen therapy”, “HBOT”, and “oxygen under pressure”. The search was limited to articles published between January 2000 and August 2025, based on a preliminary scoping check which indicated that no relevant randomized controlled trials on HBOT in chronic pain syndromes were published prior to 2000. Complete database-specific search strategies are provided in Supplement 1.
Eligibility Criteria and Study Selection
For this systematic review, we included studies published in English or Dutch that evaluated the use of HBOT in adults (≥18 years) with chronic pain syndromes. Studies involving children, animals, acute pain conditions, or wound healing were excluded. Randomized controlled trials (RCTs) were considered eligible. Narrative or systematic reviews, as well as meta-analyses, were screened for additional relevant studies.
Article selection was conducted by one reviewer (A.M.L)., based on title, abstract, and full-text assessment. The procedure was systematically repeated twice to minimize the risk of omitting relevant studies and to partially offset the absence of a second reviewer. The selection process did not involve the use of any automation tools.
Data Extraction
Data extraction was performed by investigator A.M.L. The following variables were collected: study characteristics (author, year of publication), population details (type of chronic pain, number of participants per group, gender, age, average disease duration), intervention specifics (HBOT protocol - pressure, number of sessions, duration per session, frequency), control conditions (sham HBOT, standard care, no treatment, medication), follow-up intervals, outcome measures (pain intensity, distribution and sensitivity, functional status, quality of life, psychological outcomes, medication use, neuroimaging findings, and adverse events), and results.
Outcomes
Pain measures (intensity, distribution and sensitivity) were considered the primary outcome, while secondary outcomes included multidimensional pain-related outcomes – including quality of life, global functioning and psychological well-being – analgesic use, neuroimaging findings, and adverse events. In recognition of the complex and multifaceted biopsychosocial nature of chronic pain, studies not reporting on pain measures were still included, provided they reported on one or more of the secondary outcomes of interest, allowing for a comprehensive assessment of HBOT’s effects on chronic pain syndromes.
Risk of Bias Appraisal
Risk of bias in the included studies was assessed using the Cochrane Risk of Bias (RoB 2) tool, considering randomization process, deviations from intended interventions, missing outcome data, outcome measurement, and selection bias.40 The assessment was performed by one reviewer (A.M.L)., with uncertainties resolved through consultation with a second reviewer (D.W).
Data Analysis and Synthesis
Examination of the data presented in Tables 1 and 2 showed substantial clinical and methodological heterogeneity across the included studies. This was reflected in the variability of HBOT protocols, control conditions, and outcome measures, with studies employing diverse assessment instruments. Given this degree of heterogeneity, quantitative synthesis through meta-analysis was considered inappropriate, as statistical pooling could yield misleading results. The findings were synthesized using a narrative approach, focusing on patterns, consistencies, and differences across studies.
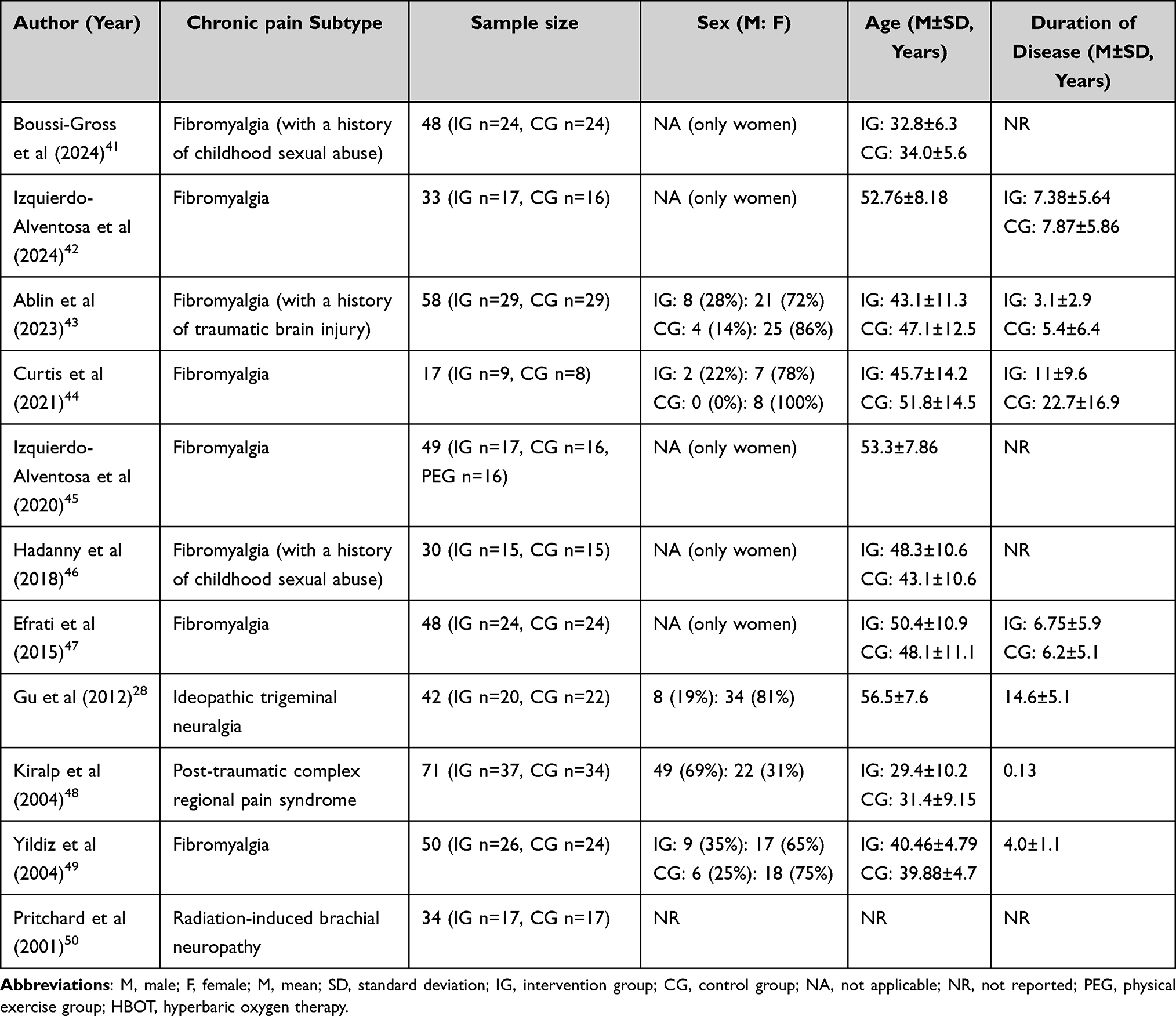 |
Table 1 Demographic Information of Included Studies |
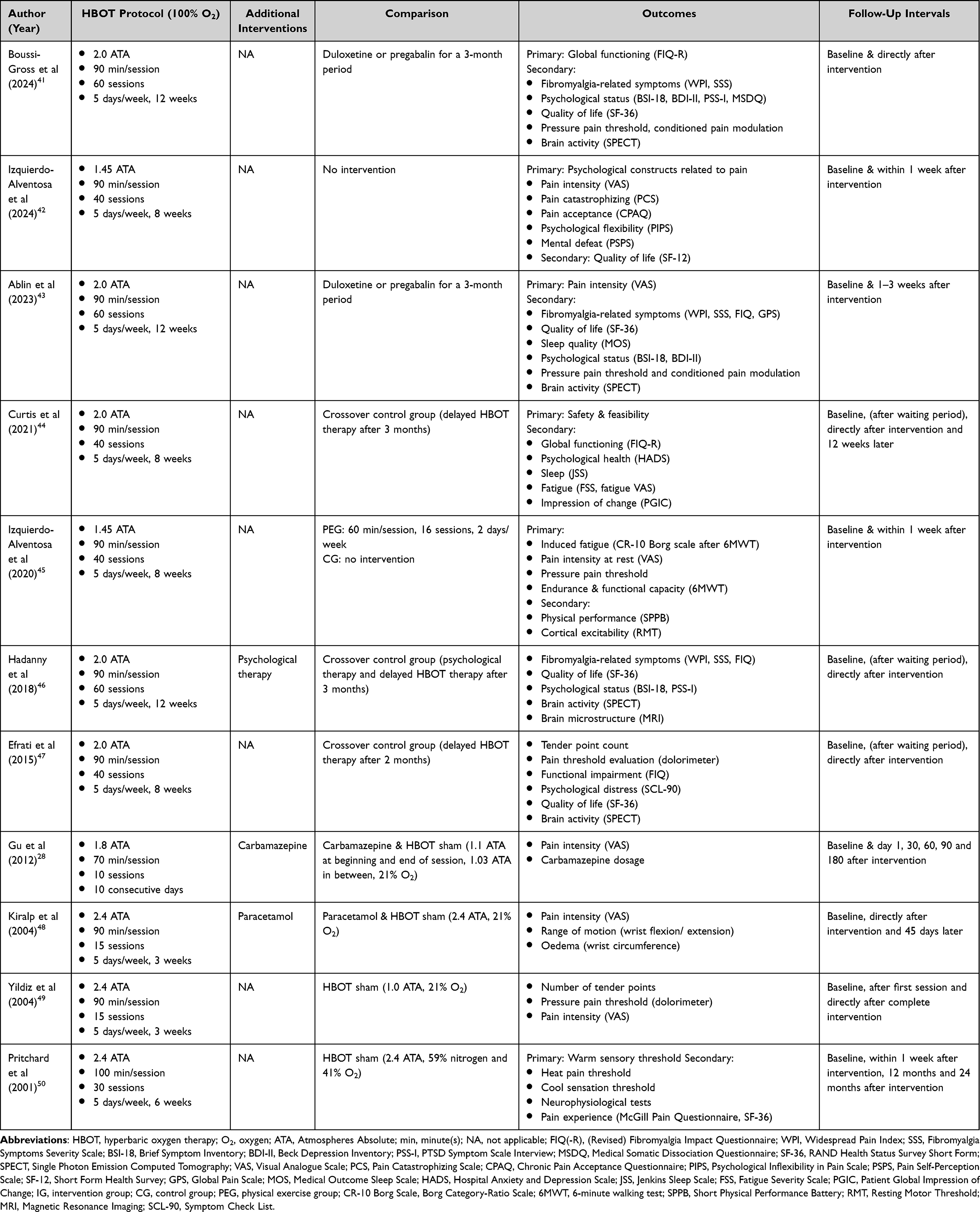 |
Table 2 Summary of Study Characteristics |
Results
Literature Search
A total of 69 results were identified. After removing 32 duplicates, 37 records remained for screening of title and abstract, of which 14 were excluded for not meeting the predefined inclusion and exclusion criteria. Of the 23 remaining results, only 12 articles were available for full text screening. Of these, 11 articles met the predefined inclusion and exclusion criteria and were included in the review,28,41–50 while one was excluded as it was a published study protocol for future studies (see Figure 1).51
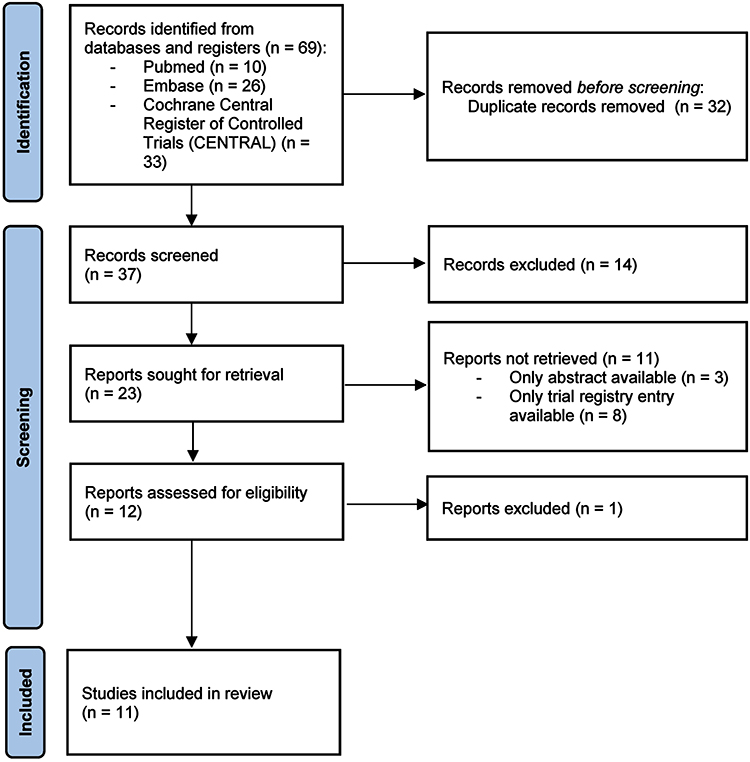 |
Figure 1 Flow diagram of study selection process according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. |
Of the initial 69 results, 10 articles were reviews or meta-analyses that met the inclusion and exclusion criteria.26,35–37,52–57 These publications were screened for potentially missing eligible trials, however, none were identified. The trials cited within these reviews had already been included through our primary search strategy.
Study Characteristics
An overview of study characteristics is presented in Tables 1 and 2. In total, eleven studies published between 2001 and 2024 were analyzed, covering various chronic pain subtypes. Eight out of eleven studies focused on fibromyalgia,41–47,49 including two involving patients with a history of childhood sexual abuse,41,46 and one addressing fibromyalgia after traumatic brain injury.43 The remaining studies included two trials on neuropathic pain – idiopathic trigeminal neuralgia28 and radiation-induced brachial neuropathy50 – and one on post-traumatic CRPS.48 Sample sizes ranged from 17 to 71 participants, resulting in a total of 480 patients across all trials. The study populations consisted mainly of women, reflecting the higher representation of fibromyalgia cases. The only exception was the study by Kiralp et al, in which the CRPS cohort was predominantly male49 The average reported duration of chronic pain varied considerably, from approximately three years in recent-onset cases to more than two decades in long-standing disease.
HBOT protocols also differed substantially across studies, with treatment pressures ranging from 1.45 to 2.4 ATA, a total of 15 to 60 sessions, and individual session duration between 70 and 100 minutes. Most trials employed sham (n=4) or delayed-treatment controls (n=3), whereas others compared HBOT with pharmacological (eg duloxetine, pregabalin, carbamazepine, paracetamol) or psychological therapies, or no new interventions at all In the included trials, sham protocols varied, including normobaric air, mild pressurization, or altered oxygen fractions. These sham procedures are intended to control for expectation and placebo effects. Notably, only the four studies implementing a sham-controlled design were conducted in a double-blind manner.28,48–50 The remaining seven studies compared HBOT with alternative control conditions and were using an open-label design.41–47 Detailed descriptions of the control conditions and sham protocols for each trial are provided in Table 2.
Across studies, participants generally continued their pre-existing treatments during the study period. In three of the eleven studies, an additional intervention (eg physical exercise, carbamazepine, or paracetamol; see Table 2) was initiated alongside HBOT.28,46,48
Outcomes predominantly focused on pain intensity and global functioning, while secondary outcomes assessed quality of life, psychological well-being, and physiological markers such as brain activity. Follow-up intervals varied from immediate post-intervention assessments to long-term evaluations up to 24 months.
Several included studies originated from overlapping research groups. To assess potential duplication of patient populations, recruitment timelines, clinical trial registration numbers, and baseline characteristics were reviewed. Two publications by Izquierdo et al shared identical recruitment periods and trial registration numbers, with highly comparable baseline characteristics, suggesting that they reported on the same underlying study population42,45 These publications were therefore considered as arising from a single cohort. Although these publications presented different primary and secondary outcome domains, pain intensity (VAS) was reported across both papers. For this shared outcome, we treated the data as originating from a single cohort in the narrative synthesis to avoid double-counting. Studies by Efrati et al, Hadanny et al, Boussi-Gross et al, and Ablin et al, although conducted by overlapping research teams, reported distinct recruitment periods and separate trial registration numbers, supporting inclusion as independent cohorts41,43,46,47 Similarly, studies by Kiralp et al and Yildiz et al investigated different patient populations (fibromyalgia versus CRPS), despite partial overlap in research teams.48,49
Risk of Bias Assessment
Risk of bias in the included studies was assessed using the Cochrane Risk of Bias (RoB 2) tool.40 Overall, no study was judged at low risk of bias (see Figure 2). Seven studies were judged as presenting “some concerns”, primarily due to limitations in the domain “measurement of the outcome”, reflecting the lack of participant blinding and the reliance on subjective self-reported questionnaires as primary endpoints.28,41,43,45–47,50 These trials attempted to compensate for this limitation by also including objective secondary outcomes (eg single photon emission computed tomography (SPECT), pressure pain threshold (PPT), or functional assessments), which led these studies to be judged as presenting “some concerns” instead of “high risk”. Four studies were rated as having a high risk of bias. In two studies, a high risk of bias resulted from open-label study designs in combination with exclusive reliance on subjective endpoints.42,44 In the remaining two studies, this judgment was driven by concerns in the domain “randomization process”, due to unclear allocation procedures (alternate allocation).48,49 Randomization procedures were otherwise generally adequate, baseline characteristics were balanced, and drop-out rates were low, with intention-to-treat analyses commonly applied.
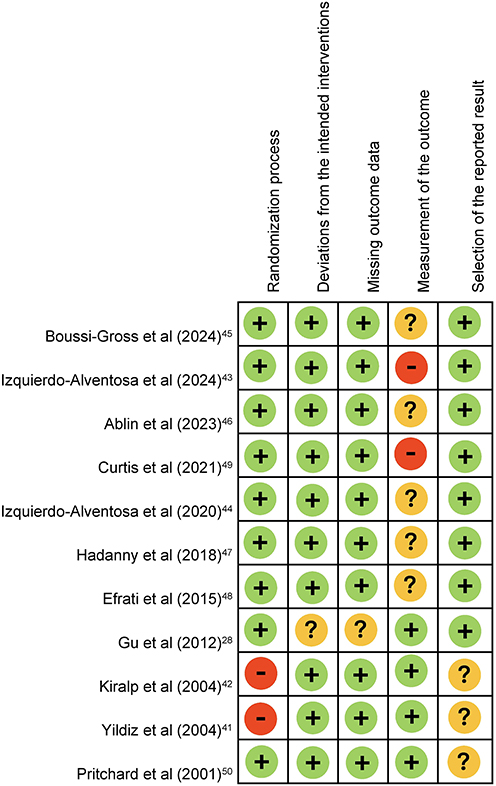 |
Figure 2 Risk of bias summary. Note: Green circle and “+”, low risk of bias; red circle and “-”, high risk of bias; yellow circle and “?”, unclear risk of bias or some concerns. |
Narrative Synthesis of Results
Pain Intensity, Distribution and Sensitivity
Pain Intensity
Nine studies assessed self-reported pain intensity, predominantly using the Visual Analogue Scale (VAS). In fibromyalgia trials, HBOT was associated with reductions in self-reported pain intensity. Yildiz et al reported a mean decrease of 3.31 points on a 11-point scale following 15 sessions of HBOT at 2.4 ATA (p < 0.001), though between-group differences compared to sham control did not reach statistical significance.49 Two complementary studies by Izquierdo-Alventosa et al using lower pressure protocols (1.45 ATA, 40 sessions) both observed reductions in VAS scores of 2.47 points (p < 0.05 and p < 0.001), with large within-group effect sizes (Cohen’s d = 1.06 and 1.24).42,45 However, these studies did not report formal between-group statistical comparisons. In contrast, Ablin et al (2.0 ATA, 60 sessions) demonstrated a statistically significant between-group advantage for HBOT over pharmacological treatment (duloxetine or pregabalin), with a VAS reduction of 2.31 points and a large between-group effect size (Cohen’s d = 0.95, p = 0.001).43
In post-traumatic CRPS, Kiralp et al (2.4 ATA, 15 sessions) reported a 3.1 point reduction in VAS scores in the HBOT group (p < 0.001), an improvement that persisted for 45 days, whereas changes in the sham control group were minimal, resulting in a statistically significant between-group difference (p < 0.001).48 Similarly, in idiopathic trigeminal neuralgia, Gu et al (1.8 ATA, 10 sessions) reported that approximately 60-75% of patients receiving HBOT achieved a VAS reduction of ≥2 points, compared with only 20-30% in the sham control group (p < 0.01), with effects persisting for up to six months.28 However, in contrast to positive findings in other conditions, Pritchard et al (2.4 ATA, 30 sessions) observed no statistically significant reduction in pain scores over 12-month follow-up in patients with radiation-induced brachial plexopathy, as measured by the McGill Pain Questionnaire and SF-36 pain domains, although some participants did report subjective improvements.50
Pain Distribution
Three studies assessed pain distribution in fibromyalgia patients using the self-reported 19-point Widespread Pain Index (WPI), with two trials demonstrating significant within-group improvements after HBOT. Hadanny et al (2.0 ATA, 60 sessions) reported a reduction of 3.7 ± 3.0 points (p = 0.001) with a large within-group effect size (Cohen’s d = 1.03), and similar improvements replicated in the crossover phase.46 In parallel, Boussi-Gross et al (2.0 ATA, 60 sessions), who compared HBOT with pharmacological treatment (duloxetine or pregabalin) rather than using a crossover design, observed an even larger reduction of 4.5 ± 5.9 points (p = 0.001) and likewise reported a large effect size after between-group analyses (Cohen’s d = 0.97).41 The third study, however, by Ablin et al, reported a smaller WPI reduction of 2.4 ± 5.9 points (p = 0.0415), and was not able to demonstrate between-group superiority over pharmacological treatment with duloxetine or pregabalin (p = 0.154).43
Two studies also reported on the number of tender points in fibromyalgia patients. Yildiz et al (2.4 ATA, 15 sessions) observed a significant decrease of 8.9 tender points following HBOT (p < 0.001), however, they were not able to demonstrate a significant between-group differences.49 Meanwhile, Efrati et al (2.0 ATA, 40 sessions) reported reductions in tender point counts of 8.46 points in the primary HBOT group and 11.54 points in the crossover group (on an 18-point tender point assessment). These reductions were accompanied by very large effect sizes (Cohen’s d = 1.5 and 2.24 respectively, p < 0.001) and were supported by significant between-group analyses.47
Pain Sensitivity
Multiple fibromyalgia trials reported increases in pressure pain thresholds (PPT), measured with dolorimetry, following treatment with HBOT.41,43,45,47,49 Effect sizes were generally in the medium range. Ablin et al, also reported a significant correlation between PPT changes and reduction in pain indices.43
Multidimensional Pain Outcomes
Quality of Life
In fibromyalgia trials, HBOT was associated with improvements in quality of life compared with controls, with 29% to 53.3% of HBOT-treated participants no longer meeting diagnostic criteria at post-treatment assessment, versus 0 to 6.7% in control groups.41,43,46 Improvements in SF-36 scores (range 0 to 100) were reported by Boussi-Gross et al, with increases of 24.1 ± 17.9 points in the Physical Component Summary (Cohen’s d = 1.46) and 24.3 ± 20.8 points in the Mental Component Summary (Cohen’s d = 1.03), with significant between-group differences.41 Efrati et al reported smaller but still statistically significant improvements in SF-36 total scores in both the HBOT group (3.3 points, Cohen’s d = 1.0) and the crossover group (2.3 points, Cohen’s d = 0.58), supported by both within- and between-group analyses.47 Other studies focusing on SF-12 and SF-36 subdomains generally found the most pronounced improvements in domains of bodily pain, vitality, and social functioning.42,43,46
In contrast, Pritchard et al observed no overall between-group differences in quality-of-life measures over 12-month follow-up in patients with radiation-induced brachial plexopathy However, participants receiving HBOT did maintain higher scores on the SF-36 physical functioning and emotional role domains at 12 months compared to controls.50
Global Functioning
Functional impairment, as measured by the Fibromyalgia Impact Questionnaire (FIQ) and its revised version (FIQR), improved following hyperbaric oxygen therapy across multiple fibromyalgia trials. Curtis et al reported a reduction of 33.8 points in total FIQR scores in the HBOT group (p < 0.001) – significantly greater compared to controls (p = 0.004) – with the control group demonstrating similar improvements after crossover.44 Similar functional gains were reported in three additional studies. Ablin et al observed a reduction of 19.6 ± 17.6 points, accompanied by a large between-group effect size (Cohen’s d = 1.11).43 Hadanny et al reported a reduction of 29.9 ± 27.3 points in the HBOT group, with an even larger reduction of 39.8 ± 21.9 points in the control group following crossover.46 Likewise, Boussi-Gross et al demonstrated a decrease of 24.3 ± 20.9 points, supported by significant between-group analyses and a large effect size (Cohen’s d = 1.27).41 Improvements were also reported at the subdomain level. Efrati et al showed significant gains in the “Function” subscale of the FIQ(R) following HBOT in both the primary HBOT group and crossover group, with medium to large effect sizes (Cohen’s d = 0.64 and 1.29, respectively).47
Objective measures of functional capacity in fibromyalgia patients were reported in one trial. Walking distance in the six-minute walking test (6MWT) increased by 49.5 m following HBOT compared to pre-treatment (Cohen’s d = 1.16), while induced fatigue improved by 1.18 points (Cohen’s d = 0.53). No relevant improvements were seen in control groups. An exercise comparator group demonstrated comparable, though smaller, gains in walking distance (+32 m, Cohen’s d = 0.75). SPPB scores increased significantly following both HBOT (+0.89 points) and physical exercise (+1.4 points), while remaining unchanged in the control group.45
In CRPS, better joint mobility (wrist flexion +19.3°, p < 0.001) and reduced edema (wrist circumference −1.9 cm, p < 0.001) were reported.48
Sleep and Fatigue
Two fibromyalgia trials reported reductions in sleep disturbances, with significant improvements on both the Medical Outcomes Study (MOS) Sleep Problems Index (Cohen’s d = 0.65, p = 0.018) and the Jenkins Sleep Scale (p = 0.04).43,44 Fatigue perception decreased in one study (Cohen’s d = 0.53, p < 0.05),45 although no significant changes were observed on the Fatigue Severity Scale or fatigue VAS in another trial.44
Psychological Well-Being
Psychological and psychiatric outcomes were evaluated in six fibromyalgia trials. Boussi-Gross et al reported significant improvements in Post-Traumatic Stress Disorder (PTSD) severity, somatization, depression, and overall psychological distress, supported by between-group analyses. Large effect sizes were observed for PTSD severity (PTSD Symptom Scale (PSS); Cohen’s d = 0.82) and somatization (Medical Somatic Dissociation Questionnaire (MSDQ); Cohen’s d = 1.01), while moderate effect sizes were found for general psychological distress and depressive symptoms, as measured by the Brief Symptoms Inventory (BSI; Cohen’s d = 0.67) and Beck Depression Inventory (BDI; Cohen’s d = 0.74).41 These results align closely with those reported by Ablin et al, who observed comparable reductions in overall psychological distress and somatization (BSI and MSDQ; Cohen’s d = 0.69 and 0.95 respectively), along with improvements in depressive symptoms (BDI; Cohen’s d = 0.80), compared to controls.43
Evidence from additional studies further support these findings. One trial observed reductions exceeding 50% in somatization, anxiety, and depression (p < 0.001), along with a 29% improvement in PTSD symptoms (p = 0.006).46 Another study found significant and sustained decreases in anxiety and depression as measured by the Hospital Anxiety and Depression Scale (HADS), with improvements maintained at 12-week follow-up.44 Similar effects were observed for psychological distress measured by the Symptom Checklist (SCL-90; Cohen’s d = 0.66).47 Across studies, improvements were generally absent in control groups and were replicated in crossover.
Analgesic Use
Two out of eleven articles described the effect of HBOT on analgesia use.28,47 Gu et al reported a 60-70% decrease in daily carbamazepine requirements in the HBOT group, compared with a 15-20% reduction in controls (p < 001). The decrease was evident within one day after treatment and remained significant for up to 60 days, returning to baseline levels after 90 days.
Similarly, Efrati et al reported significant decreases in analgesic intake following HBOT, with some individuals discontinuing pain medication entirely47 These reductions were observed both in the primary HBOT group and in the crossover group once they received HBOT. The specific classes of analgesic medications were not further specified. Antidepressant use remained largely unchanged in the treated group, although the crossover group demonstrated a modest reduction after HBOT.
Neuroimaging
Four fibromyalgia studies reported neuroimaging outcomes following HBOT.41,43,46,47 Collectively, these studies demonstrated that HBOT was associated with both functional and structural changes in brain regions involved in pain processing and modulation Using SPECT, significant increases in brain activity and cerebral perfusion were consistently observed in multiple Brodmann areas (BA) within the prefrontal and temporal cortices, compared with control or medication groups. One study, by Efrati et al, also reported decreased activity in posterior cortical regions, including somatosensory areas.47
Importantly, three studies performed correlation analyses, demonstrating significant associations between changes in brain activity or microstructure and clinical outcomes41,43,46 Ablin et al found that changes in activity across several Brodmann areas (BA9L, BA36R, BA36L, BA38L and BA46L) significantly correlated with clinical measures of pain, somatization, emotional, physical and social functioning, sleep problems, and general health, as assessed by VAS, Global Pain Scale (GPS), BSI, SF-36 and MOS43 Similarly, Hadanny et al reported significant correlations between perfusion changes in multiple Brodmann areas and improvements in general health, WPI, FIQ, BSI, physical function, and symptom severity scores (SSS).46
Adverse Events
Overall, HBOT was well tolerated, with no serious or life-threatening or permanent adverse events reported. Mild middle-ear barotrauma was the most frequently reported adverse event, occurring in 12-40% of participants.41,43,44,46,47 Other reported events included the inability to adjust ear pressure,47 visual disturbances,41,43,44 headaches43,46 and tinnitus,43 which were usually self-limiting. Emotional reactions, such as emotional distress or resurfacing of suppressed memories, were occasionally described in specific populations with a history of psychological trauma.41,46 In contrast, six studies reported no adverse events at all.28,42,45,48–50
Discussion
Chronic pain syndromes are conditions in which disturbances in tissue oxygenation, microvascular dysfunction, and redox imbalance may contribute to both peripheral and central sensitization. HBOT has been proposed to target these mechanisms by enhancing tissue oxygenation, modulating inflammatory pathways, and promoting neuroplasticity. The present review evaluated the current literature on the effects of HBOT in chronic pain syndromes, noting that the evidence base is predominantly composed of fibromyalgia trials, with very limited data available for CRPS, trigeminal neuralgia, and radiation-induced brachial plexopathy.
Across fibromyalgia, CRPS, and trigeminal neuralgia, trials reported statistically significant within-group reductions in self-reported pain intensity, often in the range of 2-3 points on an 11-point VAS scale. Although the absence of a universally accepted minimal clinically important difference (MCID) for chronic pain complicates interpretation, reductions of this magnitude are often regarded as clinically meaningful.58 However, reliance on within-group change must be interpreted cautiously, particularly in small cohorts and in conditions where placebo responses and contextual effects may be substantial. Evidence for superiority over control or sham conditions was heterogeneous. Trials on CRPS and trigeminal neuralgia demonstrated statistically significant between-group benefits, whereas in fibromyalgia substantial within-group improvements were not consistently accompanied by superiority over sham. Importantly, sham conditions in hyperbaric trials vary considerably, ranging from normobaric air exposure to mild pressurization or altered oxygen fractions. Some of these comparator protocols may even exert physiological effects, potentially attenuating detectable between-group contrasts and complicating interpretation of true treatment-specific efficacy.
Notably, the single trial investigating radiation-induced brachial plexopathy did not demonstrate meaningful pain intensity reductions, suggesting that HBOT-related analgesic effects may be condition-specific rather than generalizable across chronic pain syndromes.
Beyond pain, quality of life, global functioning, and psychological well-being were assessed in multiple trials, again primarily in fibromyalgia. Patients reported significant improvements in quality of life and global functioning, as reflected by SF-12/SF-36 and FIQ(R) scores, often exceeding established thresholds for clinical relevance, suggesting meaningful gains in physical, mental, and global functioning domains.59,60 These findings were generally supported by large effect sizes and significant between-group analyses. Objective measures of physical performance, though limited to two trials, aligned with these subjective improvements, showing increased walking distance, improved SPPB scores, and reduced fatigue in fibromyalgia patients. Psychological outcomes – including PTSD severity, somatization, depression, anxiety, and overall psychological distress – also showed moderate to large within-group improvements.
In CRPS and trigeminal neuralgia, functional outcomes were assessed less comprehensively, however, CRPS patients did report improved joint mobility and reduced edema after HBOT. In radiation-induced brachial plexopathy, improvements in quality-of-life could not be demonstrated, reinforcing the condition-specific nature of the evidence.
Although data on medication use are limited and derived from a small number of trials, the available evidence suggests that HBOT can potentially reduce reliance on analgesics. In trigeminal neuralgia, patients experienced rapid and substantial reductions in carbamazepine requirements alongside improvements in pain intensity. In fibromyalgia, overall analgesic intake declined, with some participants discontinuing medication entirely. However, the study did not specify the classes of analgesics (eg opioid versus non-opioid), limiting interpretation of clinical relevance and generalizability.
Preliminary neuroimaging findings possibly provide a potential mechanistic context for the observed multidimensional improvements but should be interpreted cautiously. Several fibromyalgia trials have identified both functional and structural changes in prefrontal and temporal cortices following HBOT, with some studies demonstrating correlations between cortical alterations and improvements in pain, functional status, and psychological measures. While these observations are consistent with hypotheses of modulation of central sensitization and neuroplastic processes, they are derived from small cohorts and exploratory analyses. As such, neuroimaging data remain hypothesis-generating rather than confirmatory and require replication before conclusions regarding neuroplastic effects can be drawn.
Several key methodological limitations temper confidence in the current evidence base. In addition to the small sample sizes discussed above, participants were predominantly female – consistent with the higher prevalence of fibromyalgia among women and the predominance of fibromyalgia trials in the current evidence base – which restricts broader generalizability across chronic pain populations and to male patients. Majority of studies raised some concerns regarding risk of bias, primarily due to limitations in outcome measurements with reliance on subjective self-reported outcomes and inherent challenges of maintaining adequate blinding in hyperbaric interventions.
Choosing an optimal comparator remains a key methodological challenge for future research. Trials comparing HBOT to standard care often reported large effect sizes but cannot adequately avoid expectation bias or placebo effects. In contrast, sham-controlled designs provide greater internal validity yet face the difficulty of reproducing HBOT sensations without exerting therapeutic pressurization or oxygen exposure. Sham protocols varied considerably across studies (see Table 2), including exposure to ambient air, mild pressure, or altered oxygen fractions, some of which may exert minor physiological effects. This heterogeneity and the difficulty of designing a sham that is both convincing and physiologically inactive complicates interpretation of treatment-specific effects and may contribute to variability in between-group findings.
Substantial heterogeneity in HBOT protocols further limits comparability across studies and prevents firm clinical recommendations regarding optimal treatment regimens. Studies varied in treatment pressure (1.45 to 2.4 ATA), number of sessions (10 to 60), session durations (60 to 120 minutes), patient populations, outcome measures, and comparator conditions. None of the included trials were designed to directly compare different HBOT protocols, and therefore observed differences in efficacy cannot be attributed to protocol characteristics alone. That said, some tentative patterns can be discerned in fibromyalgia. Protocols using moderate pressure of approximately 2.0 ATA delivered over a higher number of sessions (40 to 60 treatments) were most frequently applied and generally associated with large within-group and between-group improvements in pain intensity, WPI, tender points, and PPT. However, positive within-group effects of roughly similar magnitude were also observed in both lower-pressure, longer-duration protocols (eg 1.45 ATA, 40 sessions) and higher-pressure, shorter regimens (eg 2.4 ATA, 15 sessions). Therefore, exploratory comparison cannot suggest a consistent dose-response relationship at this point and future trials comparing HBOT protocols are required before evidence-based recommendations can be made.
Furthermore, in nearly all trials HBOT was delivered alongside participants’ ongoing chronic pain treatments (eg pharmacological, physiotherapy, psychological support and multimodal rehabilitation). Many studies lacked reporting on these concurrent therapies, as such, the observed improvements cannot be attributed exclusively to HBOT, and potential additive or synergistic effects remain unexplored. Future trials should clearly document or even standardize co-interventions to enhance interpretability. Data on optimal timing for initiating HBOT is also lacking. One might expect that earlier intervention in the disease course could have a greater chance of success, however this remains speculative.
From a safety perspective, HBOT does appear to have a generally favorable safety profile, with only mild and transient side effects being reported. The most often observed adverse event was ear discomfort or mild middle-ear barotrauma, often manageable with simple Valsalva maneuvers. Although rare, more severe complications, such as pulmonary barotrauma (including pneumothorax, pneumomediastinum, or arterial gas embolism) and oxygen toxicity, are however possible and have been described in the literature.61,62 Patients should therefore be informed of these potential risks, and pre-treatment screening for cardiac or pulmonary conditions, typically by electrocardiogram and chest x-ray, is often recommended.
Future Directions
To move the field of HBOT in chronic pain syndromes forward, there is a need for large, well-designed randomized controlled trials that adopt standardized HBOT protocols, clearly defining optimal pressure, session duration, and total number of treatments, to enable meaningful comparison across studies. Future trials should incorporate longer follow-up, advanced sham protocols, and assessment of HBOT as adjunctive and standalone therapy and should explore the influence of disease duration on treatment responsiveness. Incorporating neuroimaging and objective biomarkers may clarify the mechanisms through which HBOT influences chronic pain and may help identify patients most likely to benefit. Future research should also consider how the underlying pathophysiology of different chronic pain conditions may influence treatment outcomes, to guide more targeted and mechanism-informed application of HBOT. Applying the GRADE framework to future studies would allow evaluation of the certainty of evidence and provide clinicians with more evidence-based recommendations,38 while cost-effectiveness analyses are needed given the current reimbursement restrictions to determine HBOT’s feasibility and practical role within chronic pain management.
Conclusion
In summary, the current body of evidence suggests that HBOT may hold potential as a safe and useful addition to current multimodal management strategies for selected chronic pain syndromes; however, the available data remain insufficient to support firm conclusions. The existing literature is predominantly driven by fibromyalgia trials, limiting the generalizability of findings to other chronic pain conditions. Evidence in CRPS and trigeminal neuralgia is more limited but suggests possible benefit, whereas the single study in radiation-induced brachial plexopathy did not demonstrate meaningful clinical improvement. Although some trials report improvements across multidimensional pain-related outcomes – including pain intensity, distribution and sensitivity, as well as quality of life, global functional and psychological well-being – superiority over sham remains inconsistent, and methodological limitations temper confidence in these findings. Robust conclusions therefore require large, well-designed randomized controlled trials with standardized HBOT protocols and clearly defined comparators before HBOT can be integrated in routine chronic pain management.
Funding
No financial support was received for research and publication of this review.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Treede RD, Rief W, Barke A, et al. A classification of chronic pain for ICD-11. Pain. 2015;156(6):1003–16. doi:10.1097/j.pain.0000000000000160
2. Treede RD, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain for the International Classification of Diseases (ICD-11). Pain. 2019;160(1):19–27. doi:10.1097/j.pain.0000000000001384
3. Rometsch C, Martin A, Junne F, Cosci F. Chronic pain in European adult populations: a systematic review of prevalence and associated clinical features. Pain. 2025;166(4):719–731. doi:10.1097/j.pain.0000000000003406
4. Shi Y, Wu W. Multimodal non-invasive non-pharmacological therapies for chronic pain: mechanisms and progress. BMC Med. 2023;21(1):372. doi:10.1186/s12916-023-03076-2
5. Cohen SP, Vase L, Hooten WM. Chronic pain: an update on burden, best practices, and new advances. Lancet. 2021;397(10289):2082–2097. doi:10.1016/S0140-6736(21)00393-7
6. Grace PM, Gaudet AD, Staikopoulos V, et al. Nitroxidative signaling mechanisms in pathological pain. Trends Neurosci. 2016;39(12):862–879. doi:10.1016/j.tins.2016.10.003
7. An S, Shi J, Huang J, Li Z, Feng M, Cao G. HIF-1alpha induced by hypoxia promotes peripheral nerve injury recovery through regulating ferroptosis in DRG Neuron Mol Neurobiol. 2024;61(9):6300–6311. doi:10.1007/s12035-024-03964-5
8. Malkov MI, Lee CT, Taylor CT. Regulation of the Hypoxia-Inducible Factor (HIF) by pro-inflammatory cytokines Cells. 2021;10(9):2340. doi:10.3390/cells10092340
9. Deval E, Lingueglia E. Acid-sensing ion channels and nociception in the peripheral and central nervous systems. Neuropharmacology. 2015;94:49–57. doi:10.1016/j.neuropharm.2015.02.009
10. Brito R, Sheth S, Mukherjea D, Rybak LP, Ramkumar V. TRPV1: a potential drug target for treating various diseases. Cells. 2014;3(2):517–545. doi:10.3390/cells3020517
11. Holzer P. Acid-sensitive ion channels and receptors. Handb Exp Pharmacol. 2009(194):283–332.
12. Larsson M, Broman J. Synaptic plasticity and pain: role of ionotropic glutamate receptors. Neuroscientist. 2011;17(3):256–273. doi:10.1177/1073858409349913
13. Latremoliere A, Woolf CJ. Central sensitization: a generator of pain hypersensitivity by central neural plasticity. J Pain. 2009;10(9):895–926. doi:10.1016/j.jpain.2009.06.012
14. Chen G, Zhang YQ, Qadri YJ, Serhan CN, Ji RR. Microglia in pain: detrimental and protective roles in pathogenesis and resolution of pain. Neuron. 2018;100(6):1292–1311. doi:10.1016/j.neuron.2018.11.009
15. Zhao H, Alam A, Chen Q, et al. The role of microglia in the pathobiology of neuropathic pain development: what do we know? Br J Anaesth. 2017;118(4):504–516. doi:10.1093/bja/aex006
16. Yowtak J, Lee KY, Kim HY, et al. Reactive oxygen species contribute to neuropathic pain by reducing spinal GABA release. Pain. 2011;152(4):844–852. doi:10.1016/j.pain.2010.12.034
17. Carrasco C, Naziroglu M, Rodriguez AB, Pariente JA. Neuropathic pain: delving into the oxidative origin and the possible implication of transient receptor potential channels. Front Physiol. 2018;9:95. doi:10.3389/fphys.2018.00095
18. Mallet ML, Hadjivassiliou M, Sarrigiannis PG, Zis P. The role of oxidative stress in peripheral neuropathy. J Mol Neurosci. 2020;70(7):1009–1017. doi:10.1007/s12031-020-01495-x
19. Devarajan J, Mena S, Cheng J. Mechanisms of complex regional pain syndrome Front Pain Res. 2024;5:1385889. doi:10.3389/fpain.2024.1385889
20. Tan EC, Janssen AJ, Roestenberg P, van den Heuvel LP, Goris RJ, Rodenburg RJ. Mitochondrial dysfunction in muscle tissue of complex regional pain syndrome type I patients. Eur J Pain. 2011;15(7):708–715. doi:10.1016/j.ejpain.2010.12.003
21. Mezhov V, Guymer E, Littlejohn G. Central sensitivity and fibromyalgia. Intern Med J. 2021;51(12):1990–1998. doi:10.1111/imj.15430
22. Assavarittirong C, Samborski W, Grygiel-Gorniak B. Oxidative stress in fibromyalgia: from pathology to treatment. Oxid Med Cell Longev. 2022;2022:1582432. doi:10.1155/2022/1582432
23. Rubio-Zarapuz A, Parraca JA, Tornero-Aguilera JF, Clemente-Suarez VJ. Unveiling the link: exploring muscle oxygen saturation in fibromyalgia and its implications for symptomatology and therapeutic strategies. Med Gas Res. 2025;15(1):58–72. doi:10.4103/mgr.MEDGASRES-D-24-00013
24. Choudhury R. Hypoxia and hyperbaric oxygen therapy: a review. Int J Gen Med. 2018;11:431–442. doi:10.2147/IJGM.S172460
25. Alter IL, Hamiter M, Han J, Leu CS, Usseglio J, Lalwani AK. Hyperbaric oxygen and sudden sensorineural hearing loss: a systematic review and meta-analysis. Laryngoscope. 2025.
26. Sutherland AM, Clarke HA, Katz J, Katznelson R. Hyperbaric oxygen therapy: a new treatment for chronic pain? Pain Pract. 2016;16(5):620–628. doi:10.1111/papr.12312
27. Zhao BS, Meng LX, Ding YY, Cao YY. Hyperbaric oxygen treatment produces an antinociceptive response phase and inhibits astrocyte activation and inflammatory response in a rat model of neuropathic pain. J Mol Neurosci. 2014;53(2):251–261. doi:10.1007/s12031-013-0213-3
28. Gu N, Niu JY, Liu WT, et al. Hyperbaric oxygen therapy attenuates neuropathic hyperalgesia in rats and idiopathic trigeminal neuralgia in patients. Eur J Pain. 2012;16(8):1094–1105. doi:10.1002/j.1532-2149.2012.00113.x
29. Ding Y, Yao P, Hong T, et al. The analgesic effect of early hyperbaric oxygen treatment in chronic constriction injury rats and its influence on nNOS and iNOS expression and inflammatory factor production. Mol Pain. 2018;14:1744806918765837. doi:10.1177/1744806918765837
30. Thompson CD, Uhelski ML, Wilson JR, Fuchs PN. Hyperbaric oxygen treatment decreases pain in two nerve injury models. Neurosci Res. 2010;66(3):279–283. doi:10.1016/j.neures.2009.11.010
31. Heeman JH, Zhang Y, Shirachi DY, Quock RM. Involvement of spinal cord opioid mechanisms in the acute antinociceptive effect of hyperbaric oxygen in mice. Brain Res. 2013;1540:42–47. doi:10.1016/j.brainres.2013.09.050
32. Li F, Fang L, Huang S, et al. Hyperbaric oxygenation therapy alleviates chronic constrictive injury-induced neuropathic pain and reduces tumor necrosis factor-alpha production. Anesth Analg. 2011;113(3):626–633. doi:10.1213/ANE.0b013e31821f9544
33. Zelinski LM, Ohgami Y, Chung E, Shirachi DY, Quock RM. A prolonged nitric oxide-dependent, opioid-mediated antinociceptive effect of hyperbaric oxygen in mice. J Pain. 2009;10(2):167–172. doi:10.1016/j.jpain.2008.08.003
34. Ohgami Y, Zylstra CC, Quock LP, Chung E, Shirachi DY, Quock RM. Nitric oxide in hyperbaric oxygen-induced acute antinociception in mice. Neuroreport. 2009;20(15):1325–1329. doi:10.1097/WNR.0b013e3283305a49
35. Cao C, Li Q, Zhang X, Varrassi G, Wang H. Effectiveness of hyperbaric oxygen for fibromyalgia: a meta-analysis of randomized controlled trials. Clin Pract. 2023;13(3):583–595. doi:10.3390/clinpract13030053
36. Chen X, You J, Ma H, Zhou M, Huang C. Efficacy and safety of hyperbaric oxygen therapy for fibromyalgia: a systematic review and meta-analysis. BMJ Open. 2023;13(1):e062322. doi:10.1136/bmjopen-2022-062322
37. Kulshreshtha P, Neyaz O, Begum S, Yadav RK, Deepak KK. Assessment of the efficacy and safety of hyperbaric oxygen therapy on pain in patients with fibromyalgia: a systematic review and meta-analysis of randomised controlled studies. J Med Evidence. 2024;5(1):40–54.
38. Brozek JL, Canelo-Aybar C, Akl EA, et al. GRADE guidelines 30: the GRADE approach to assessing the certainty of modeled evidence-an overview in the context of health decision-making. J Clin Epidemiol. 2021;129:138–150. doi:10.1016/j.jclinepi.2020.09.018
39. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
40. Higgins JP, Altman DG, Gotzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343(oct18 2):d5928. doi:10.1136/bmj.d5928
41. Boussi-Gross R, Catalogna M, Lang E, et al. Hyperbaric oxygen therapy vs. pharmacological intervention in adults with fibromyalgia related to childhood sexual abuse: prospective, randomized clinical trial. Sci Rep. 2024;14(1):11599. doi:10.1038/s41598-024-62161-5
42. Izquierdo-Alventosa R, Ingles M, Cortes-Amador S, et al. Effects of a low-pressure hyperbaric oxygen therapy on psychological constructs related to pain and quality of life in women with fibromyalgia: a randomized clinical trial. Med Clin. 2024;162(11):516–522. doi:10.1016/j.medcli.2023.12.016
43. Ablin JN, Lang E, Catalogna M, et al. Hyperbaric oxygen therapy compared to pharmacological intervention in fibromyalgia patients following traumatic brain injury: a randomized, controlled trial. PLoS One. 2023;18(3):e0282406. doi:10.1371/journal.pone.0282406
44. Curtis K, Katz J, Djaiani C, et al. Evaluation of a hyperbaric oxygen therapy intervention in individuals with fibromyalgia. Pain Med. 2021;22(6):1324–1332. doi:10.1093/pm/pnaa416
45. Izquierdo-Alventosa R, Ingles M, Cortes-Amador S, et al. Comparative study of the effectiveness of a low-pressure hyperbaric oxygen treatment and physical exercise in women with fibromyalgia: randomized clinical trial. Ther Adv Musculoskelet Dis. 2020;12:1759720X20930493. doi:10.1177/1759720X20930493
46. Hadanny A, Bechor Y, Catalogna M, et al. Hyperbaric oxygen therapy can induce neuroplasticity and significant clinical improvement in patients suffering from fibromyalgia with a history of childhood sexual abuse-randomized controlled trial. Front Psychol. 2018;9:2495. doi:10.3389/fpsyg.2018.02495
47. Efrati S, Golan H, Bechor Y, et al. Hyperbaric oxygen therapy can diminish fibromyalgia syndrome--prospective clinical trial. PLoS One. 2015;10(5):e0127012. doi:10.1371/journal.pone.0127012
48. Kiralp MZ, Yildiz S, Vural D, Keskin I, Ay H, Dursun H. Effectiveness of hyperbaric oxygen therapy in the treatment of complex regional pain syndrome. J Int Med Res. 2004;32(3):258–262. doi:10.1177/147323000403200304
49. Yildiz S, Kiralp MZ, Akin A, et al. A new treatment modality for fibromyalgia syndrome: hyperbaric oxygen therapy. J Int Med Res. 2004;32(3):263–267. doi:10.1177/147323000403200305
50. Pritchard J, Anand P, Broome J, et al. Double-blind randomized Phase II study of hyperbaric oxygen in patients with radiation-induced brachial plexopathy. Radiother Oncol. 2001;58(3):279–286. doi:10.1016/S0167-8140(00)00319-4
51. Mota Neto J, Mendes AF, Martins AFM, et al. Protocol of HOTFy: randomised clinical trial to hyperbaric oxygen therapy in fibromyalgia. BMJ Open. 2023;13(1):e069153. doi:10.1136/bmjopen-2022-069153
52. Garcia-Campayo J, Magdalena J, Magallon R, Fernandez-Garcia E, Salas M, Andres E. A meta-analysis of the efficacy of fibromyalgia treatment according to level of care. Arthritis Res Ther. 2008;10(4):R81. doi:10.1186/ar2455
53. Mascarenhas RO, Souza MB, Oliveira MX, et al. Association of therapies with reduced pain and improved quality of life in patients with fibromyalgia: a systematic review and meta-analysis. JAMA Intern Med. 2021;181(1):104–112. doi:10.1001/jamainternmed.2020.5651
54. Carrasco-Vega E, Guiducci S, Nacci F, et al. Efficacy of physiotherapy treatment in medium and long term in adults with fibromyalgia: an umbrella of systematic reviews. Clin Exp Rheumatol. 2024;42(6):1248–1261. doi:10.55563/clinexprheumatol/ctfuqe
55. Han X, He Y, Yuan X, Sun N, Liu X. Hyperbaric oxygen therapy for patients with fibromyalgia: a systematic review protocol. BMJ Open. 2023;13(6):e071092. doi:10.1136/bmjopen-2022-071092
56. Alciati A, Nucera V, Masala IF, et al. One year in review 2021: fibromyalgia. Clin Exp Rheumatol. 2021;39(Suppl 130):3–12. doi:10.55563/clinexprheumatol/gz4i3i
57. Ramphul A, Hoffman GR, Islam S, McGarvey AC, Powell AD. Complaints of neuropathic pain, noxious cervical plexus neuropathy and neck tightness are reported by patients who undergo neck dissection: an institutional study and narrative review. Br J Oral Maxillofac Surg. 2020;58(9):1172–1179. doi:10.1016/j.bjoms.2020.08.037
58. Olsen MF, Bjerre E, Hansen MD, Tendal B, Hilden J, Hrobjartsson A. Minimum clinically important differences in chronic pain vary considerably by baseline pain and methodological factors: systematic review of empirical studies. J Clin Epidemiol. 2018;101:87–106e102. doi:10.1016/j.jclinepi.2018.05.007
59. Bennett RM, Bushmakin AG, Cappelleri JC, Zlateva G, Sadosky AB. Minimal clinically important difference in the fibromyalgia impact questionnaire. J Rheumatol. 2009;36(6):1304–1311. doi:10.3899/jrheum.081090
60. Gronkvist R, Vixner L, Ang B, Grimby-Ekman A. Measurement error, minimal detectable change, and minimal clinically important difference of the short form-36 health survey, hospital anxiety and depression scale, and pain numeric rating scale in patients with chronic pain. J Pain. 2024;25(9):104559. doi:10.1016/j.jpain.2024.104559
61. Zhang Y, Zhou Y, Jia Y, Wang T, Meng D. Adverse effects of hyperbaric oxygen therapy: a systematic review and meta-analysis. Front Med. 2023;10:1160774. doi:10.3389/fmed.2023.1160774
62. Sadri RA, Cooper JS. Hyperbaric Complications. In: StatPearls. Treasure Island (FL) ineligible companies; 2025.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Fibromyalgia: Associations Between Fat Infiltration, Physical Capacity, and Clinical Variables
Gerdle B, Dahlqvist Leinhard O, Lund E, Bengtsson A, Lundberg P, Ghafouri B, Forsgren MF
Journal of Pain Research 2022, 15:2517-2535
Published Date: 27 August 2022
Effects of Hypnotic Analgesia and Transcranial Direct Current Stimulation on Pain Tolerance and Corticospinal Excitability in Individuals with Fibromyalgia: A Cross-Over Randomized Clinical Trial
Schein B, Beltran G, França BR, Sanches PR, Silva DP Jr, Torres IL, Fegni F, Caumo W
Journal of Pain Research 2023, 16:187-203
Published Date: 24 January 2023
The Safety and Efficacy of Low-Dose Naltrexone in Patients with Fibromyalgia: A Systematic Review
Yang J, Shin KM, Do A, Bierle DM, Abu Dabrh AM, Yin Z, Bauer BA, Mohabbat AB
Journal of Pain Research 2023, 16:1017-1023
Published Date: 21 March 2023
Reduced Visuospatial Attention in Personal Space is Not Limited to the Affected Limb in Complex Regional Pain Syndrome
Halicka M, Cousins OR, Ten Brink AF, Vittersø AD, Proulx MJ, Bultitude JH
Journal of Pain Research 2024, 17:1519-1529
Published Date: 23 April 2024
Intravenous Pamidronate in Persistent Complex Regional Pain Syndrome (CRPS): A Retrospective Observational Study on Effectiveness and Tolerability
van der Spek DPC, Huygen FJPM, Hoeks SE, van Daele PLA, Dirckx M
Journal of Pain Research 2026, 19:573167
Published Date: 18 February 2026