Back to Journals » Journal of Pain Research » Volume 19
Intravenous Pamidronate in Persistent Complex Regional Pain Syndrome (CRPS): A Retrospective Observational Study on Effectiveness and Tolerability
Authors van der Spek DPC ![]() , Huygen FJPM, Hoeks SE, van Daele PLA, Dirckx M
, Huygen FJPM, Hoeks SE, van Daele PLA, Dirckx M
Received 9 October 2025
Accepted for publication 20 January 2026
Published 18 February 2026 Volume 2026:19 573167
DOI https://doi.org/10.2147/JPR.S573167
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Daniël PC van der Spek,1 Frank JPM Huygen,1 Sanne E Hoeks,1 Paul LA van Daele,2 Maaike Dirckx1
1Department of Anesthesiology, Center for Pain Medicine, Erasmus MC University Medical Center, Rotterdam, the Netherlands; 2Department of Immunology, Erasmus MC University Medical Center, Rotterdam, the Netherlands
Correspondence: Daniël PC van der Spek, Department of Anesthesiology, Center for Pain Medicine, Erasmus MC University Medical Center, Dr. Molewaterplein 40, 3015 GD, Rotterdam, the Netherlands, Email [email protected]
Purpose: Pamidronate is a nitrogen-containing bisphosphonate with immunomodulatory and anti-osteoclastic properties that has shown benefit in early-onset complex regional pain syndrome (CRPS), yet evidence in persistent CRPS remains limited. Given that chronicity may attenuate therapeutic response, this study evaluates the effectiveness and tolerability of intravenous pamidronate in CRPS patients managed in routine clinical practice.
Patients and Methods: We conducted a single-center retrospective observational study, including all adult CRPS patients treated with pamidronate between 2014 and 2024 at our tertiary referral center. Data were collected from medical records at baseline, during treatment and at routine follow-up at approximately 1-, 3-, 6-, and 12-months post-treatment. The primary outcome was the pain trajectory, analyzed using a linear mixed-effects model. Responders were defined by a ≥ 2-point NRS reduction or subjective benefit when NRS data were unavailable.
Results: Of 110 eligible patients, 97 were included with a median age of 45 (IQR 32– 54), and a median disease duration of 31 months (IQR 9– 97). Baseline mean NRS was 7.95 (95% CI: 7.66 to 8.25), declining by 1.10 points (95% CI: − 1.49 to − 0.70; p< 0.001) at 1 month and by 0.66 points (95% CI: − 1.13 to − 0.20; p< 0.01) at 3 months. Responder rates were 34% and 22%, respectively. Treatment-related adverse events occurred in 91% of patients but led to discontinuation in only 6%.
Conclusion: In patients with predominantly persistent CRPS, intravenous pamidronate was well tolerated and associated with a modest, short-term pain relief up to 3 months. No sustained analgesic benefit was evident at later timepoints.
Keywords: complex regional pain syndrome, pamidronate, interventional pain management, chronic pain, treatment outcome, drug-related side effects and adverse reactions
Introduction
Complex regional pain syndrome (CRPS) develops in approximately 6.5% of high-risk individuals, such as post-fracture or post-surgical patients, within 24 months.1 Symptoms often decrease during the first 6 months, yet complete recovery is uncommon.2 In many cases, the condition progresses to a persistent, life-changing disorder with significant physical, psychological, and socioeconomic burdens.2 The syndrome is characterized by prominent, continuous pain that is disproportionate to the inciting event.3,4 Diagnosis follows the Valencia consensus-based adaptation of the diagnostic criteria set forth by the International Association for the study of Pain (IASP).5 Although the underlying mechanisms are complex and not yet fully understood, current evidence suggest that an abnormal, immune-mediated inflammatory response is the initiating trigger.6,7 This inflammation may initiate other peripheral and central mechanisms,7 which may contribute to the persistence and severity of the condition. Early recognition and timely intervention with disease-modifying therapy are therefore crucial to improve long-term outcomes.8
Pamidronate is a nitrogen-containing bisphosphonate administered intravenously and widely used in clinical practice for disorders characterized by bone turnover and inflammatory pain.9,10 Several randomized controlled trials (RCT) have demonstrated that bisphosphonates can provide clinically meaningful pain relief in CRPS, particularly in early disease stages.11 Their analgesic effects are thought to be multifactorial, with inhibition of farnesyl-pyrophosphate synthase (FPPS), a key regulator of osteoclast and immune cell function, representing an important pharmacodynamic mechanism.10 Experimental studies in animal models further suggest that bisphosphonate-induced modulation of inflammatory signaling and nociceptive processing contributes to their analgesic effects, providing a biologically plausible rationale for their use.10,12
Despite these promising mechanisms, evidence for bisphosphonates remains largely limited to studies in acute CRPS, leaving their value in persistent CRPS unclear.13 In routine clinical practice at our tertiary referral center, intravenous pamidronate has been used based on established feasibility, tolerability, and institutional experience. Our clinical observations further indicate substantial heterogeneity in treatment responses. Given the limited evidence for bisphosphonate treatment in persistent CRPS, we aimed to evaluate the effectiveness and tolerability of intravenous pamidronate in patients treated in routine clinical practice at our tertiary referral center. Using real-world data, this study seeks to provide insights into treatment outcomes in more heterogenous, persistent CRPS populations.
Materials and Methods
Study Design and Patient Selection
We conducted a single-center retrospective observational study among all CRPS patients who received intravenous pamidronate as part of routine care at the Erasmus MC University Medical Center between June 2014 and June 2024. Informed consent was waived by the medical ethical review board (MEC-2019-0319). The study complies with the Declaration of Helsinki, the principles of Good Clinical Practice, and the applicable STROBE guidelines.14
To identify eligible patients, we systematically searched the medical database using predefined International Classification of Diseases codes (MG30.04 for ICD-11 and G90.5, G90.6, and G90.7 for ICD-10) in combination with documented pamidronate treatment. Patients were eligible if they met the Valencia consensus-based adaption of the IASP diagnostic criteria5 and were older than 18 years. We excluded patients who were taking immunomodulating medications and those with prior bisphosphonate treatment elsewhere. Only data from the first treatment were included for patients who received repeated treatments.
Outcomes
The primary outcome was the longitudinal change in pain intensity from baseline across multiple timepoints after pamidronate infusion. Secondary outcomes included responder rates, documented subjective benefit and functional improvement, reduction in pain medication, and the incidence and severity of treatment-related adverse events.
Pamidronate Treatment Protocol
The protocol for outpatient treatment with bisphosphonate for CRPS at our institution was developed in collaboration with the Department of Internal Medicine. Laboratory tests, including creatinine and calcium levels, are performed prior to infusion, and consultation with an expert internist is sought if abnormal findings are detected. If there is any doubt regarding dental status, a dentist or oral and maxillofacial surgeon is consulted prior to infusion. Pamidronate is contraindicated only in patients with significant hypersensitivity to bisphosphonates. Patients are monitored with pulse oximeter and non-invasive blood pressure measurements before and after treatment. They receive 60mg of pamidronate diluted in 500mL of 0.9% NaCl. The infusion rate is set at 15mg/h, with a total infusion time of 4 hours. We administer this regimen monthly for a period of 3 months.
Data Collection
Outcomes were retrospectively extracted from medical records at target windows: baseline (pre-infusion), during treatment and approximately 1, 3, 6, and 12 months after the last infusion, selecting the nearest routine-care assessment with a prespecified tolerance (±4 weeks). If none was available, the timepoint was recorded as missing.
Baseline characteristics consisted of patient demographics (age, sex, and body-mass index [BMI]), CRPS characteristics (date of diagnosis, duration of pain, pain intensity, affected limb[s], and signs and symptoms), previous medications and interventions, current medication use, laboratory results (soluble Interleukin-2 receptor [sIL-2R], creatine, estimated CKD-EPI glomerular filtration rate [eGFR], and calcium), and thermography results. Persistent CRPS was defined as a disease that has lasted for more than 12 months.5 Pain intensity was measured using the 11-point numeric pain rating scale (NRS) from 0 to 10, recorded as a point measurement. The CRPS severity score (CSS)15 was calculated post-hoc based on documented signs and symptoms. Patients were also classified post-hoc in the newly proposed CRPS subtypes,16 consisting of the inflammatory, neuropathic/nociplastic, vasomotor, and motor subtype, based on the most prominent signs and symptoms. When available, sIL-2R concentrations (elevated ≥555 U/mL, indicating the inflammatory subtype) and/or thermography findings (warm asymmetry indicating the inflammatory subtype; cold asymmetry indicating the vasomotor subtype) were used to support the classifications. A second investigator (MD) reviewed and validated the subtype classifications.
Pain scores and subjective treatment benefits were collected for each timepoint. Perceived improvement in functionality and tapering of pain medication were collected from the 1-month timepoint onward. Treatment-related adverse events were continuously recorded during each infusion and at the first clinical assessment.
Data collection took place between June 2024 and May 2025 and were stored in a pseudonymized format using Castor® EDC v2024.3.6.0.
Statistical Analysis
Statistical analyses were performed in R (version 4.4.1). As this was a retrospective observational study, the sample size was determined by the available cohort of eligible treated patients. No formal a priori sample size calculation was used to inform study design or inclusion. Data distribution was assessed visually (histograms and residual plots) and with the Shapiro–Wilk test. Variables that met normality assumptions were presented as mean ± standard deviation (SD) and non-normally distributed data as median with interquartile ranges (IQR). Categorical data were reported as counts with percentages. The primary analysis modeled longitudinal NRS pain scores with a linear mixed-effects model (LMM), treating timepoint (eg, baseline, during, 1, 3, 6, and 12 months) as a categorical fixed effect and including a patient-specific random intercept. This approach allows inclusion of all available observations and accommodates unequal numbers of repeated measurements per patient resulting from variable follow-up. Observations were right-censored at the last recorded assessment or at the start of any subsequent CRPS-related intervention (eg, rehabilitation, intravenous ketamine, sympathetic blockade, neurostimulation, or repeat intravenous bisphosphonates) to reduce misattribution of later effects to the index therapy. Concomitant medication was recorded but did not lead to censoring. The model was fit by restricted maximum likelihood using all observed outcomes without imputation. Under a Missing-at-Random (MAR) assumption conditional on the model’s fixed effects and random intercepts, the resulting estimates are unbiased. Responders were defined as individuals who experienced a ≥2-point reduction in NRS score17 or, when no paired NRS data were available, subjective benefit was used. Continuous variables were examined using the unpaired t-test or Mann–Whitney U-test, and categorical variables using the chi-square test or Fisher’s exact test, as appropriate. P-values <0.05 (two-tailed) were considered statistically significant.
Results
Baseline Characteristics
We identified 110 patients, of whom 97 were included in the study (Figure 1). Our cohort consisted predominantly of females (88%) with a median age of 45 (IQR 32–54). CRPS was localized mainly in the lower extremity (77%). The median disease duration was 31 months (IQR 9–97), with 68 (70%) having persistent CRPS. Only 13 patients (13%) had experienced pain for less than 1 year. The median CSS was 12 (IQR 10–13), with the inflammatory subtype being classified in 37 patients (38%) (Table 1). Before receiving pamidronate treatment, almost all patients had undergone conventional therapies or received medication, and 62% had even undergone interventional therapy (Supplementary Table 1).
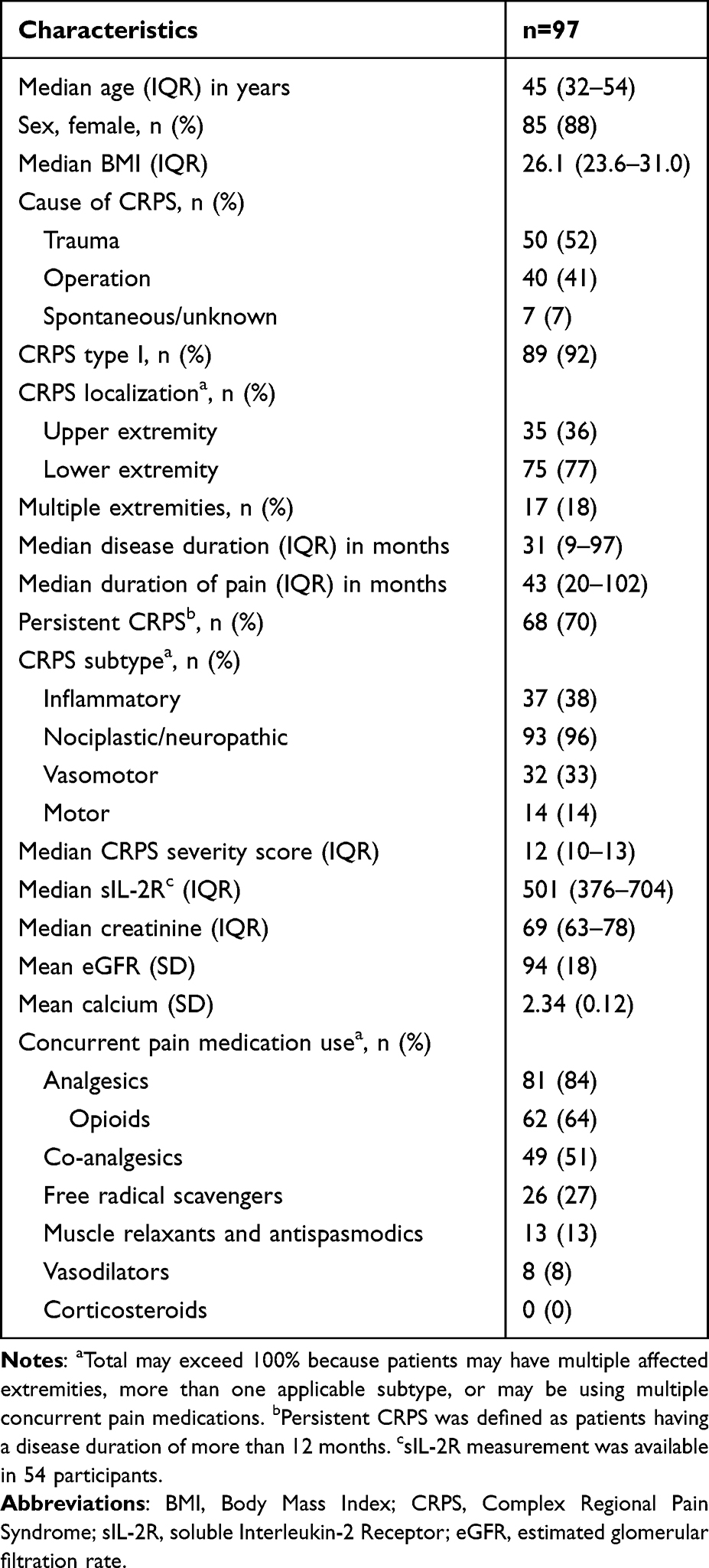 |
Table 1 Baseline Characteristics |
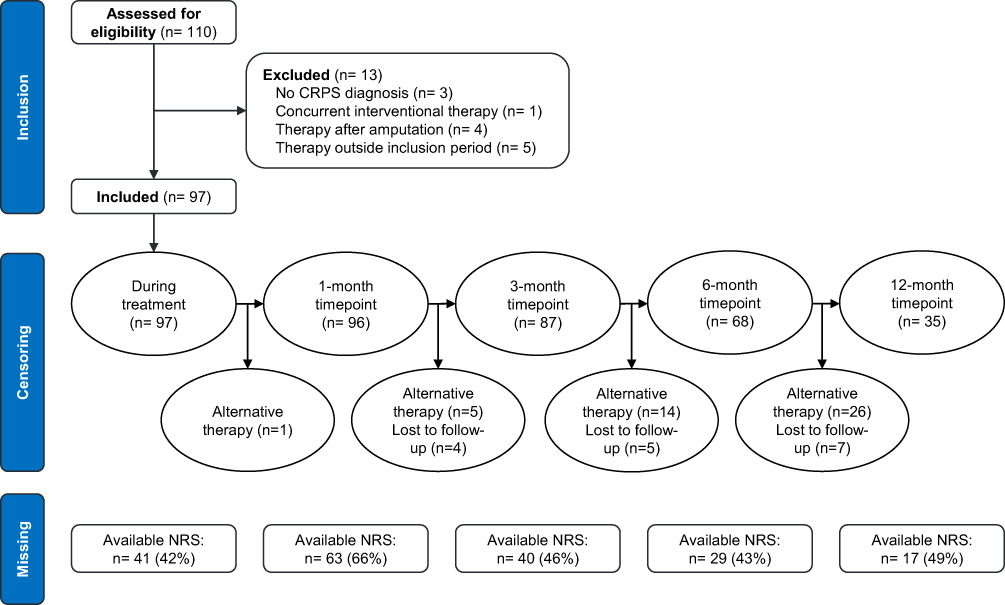 |
Figure 1 Flowchart of patient inclusion, censoring and missing NRS scores. |
Retention and Missing Data
Figure 1 summarizes retention, censoring, and completeness of NRS scores per timepoint. At the during treatment, 1-, 3-, 6-, and 12-month timepoints, the analysis set for the LMM contained 97, 96, 87, 68, and 35 patients. Of the 62 patients censored before 12 months, 46 received alternative therapies and 16 had no further assessments available. NRS scores were available for 96 of 97 at baseline (99%), 41 of 97 during treatment (42%), 63 of 96 at 1 month (66%), 40 of 87 at 3 months (46%), 29 of 68 at 6 months (43%), and 17 of 35 at 12 months (49%).
Effectiveness
Pain trajectories are shown in Figure 2 and Table 2. The estimated mean NRS at baseline was 7.95 (95% CI: 7.66 to 8.25) and declined significantly during the infusion period, with a mean difference of −1.46 (95% CI: −1.92 to −1.00; p<0.001). The mean difference remained significant at 1 month (−1.10; 95% CI: −1.49 to −0.70; p<0.001) and at 3 months (−0.66; 95% CI: −1.13 to −0.20; p<0.01), whereas changes at 6 and 12 months were not. Responder rates were 40% during treatment, 34% at 1 month, and 22% at 3 months (Table 3). Subjective benefit alone was reported by 36% and functional improvement by 29% at 1 month (Table 3). Across follow-up, 11 patients (11%) tapered their pain medications.
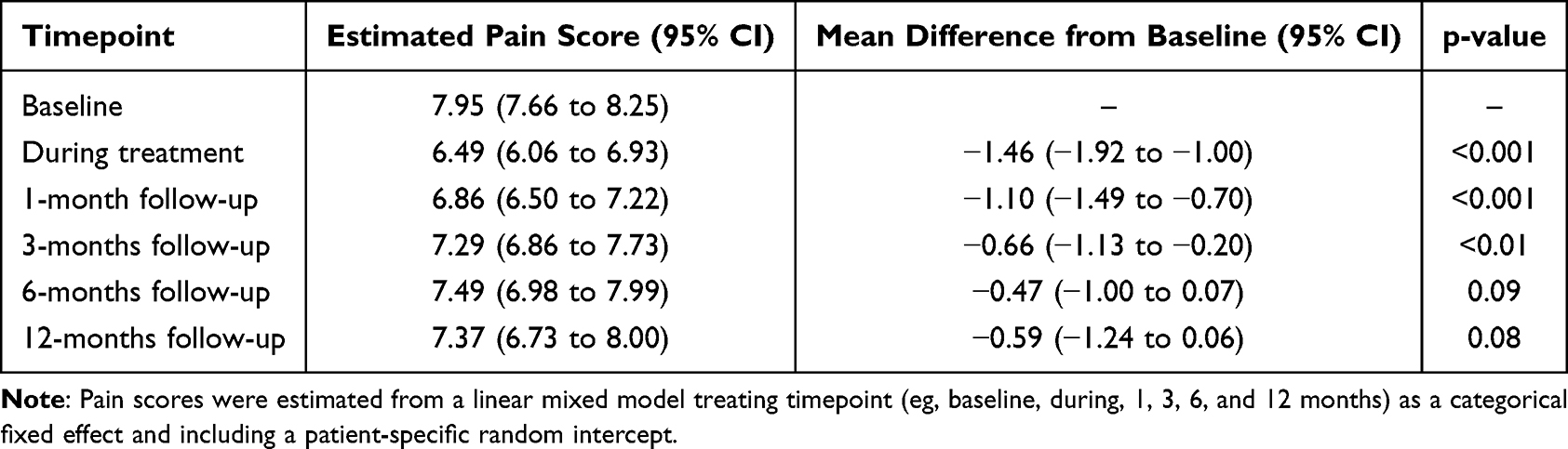 |
Table 2 Linear Mixed Model-Based Pain Score Estimates |
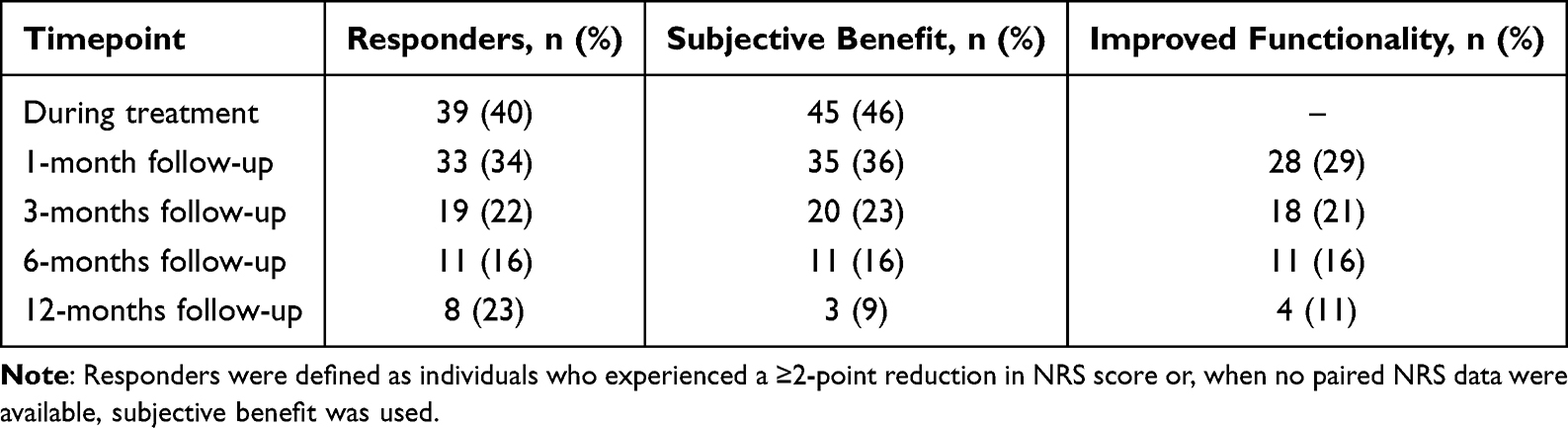 |
Table 3 Proportion of Responders, Patients with Subjective Benefit and Improved Functionality |
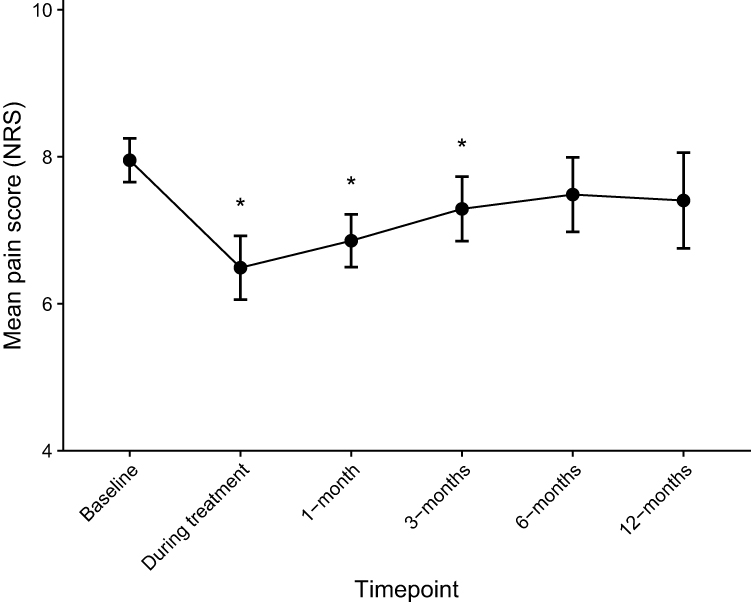 |
Figure 2 Estimated mean NRS by timepoint from the linear-mixed model with a patient-specific random intercept. Observations are right censored at the last assessment or the start of a subsequent CRPS intervention. Data are shown as mean ± 95% confidence interval (error bars), with the asterisk (*) denoting a statistically significant reduction versus baseline (p<0.05). |
Adverse Events
A full cycle of 3 infusions (3 months) was completed by 88 patients (91%), with 6 patients (6%) discontinuing prematurely due to side effects and 3 due to logistical issues. Adverse events occurred in 88 patients (91%) during or shortly after treatment (Table 4). No serious treatment-related adverse events, such as osteonecrosis of the jaw or atypical fractures, occurred, although 25 patients (26%) developed phlebitis. The most common adverse events were the acute phase reaction (63%), followed by pain or a reaction at the infusion site (33%), and myalgia (26%).
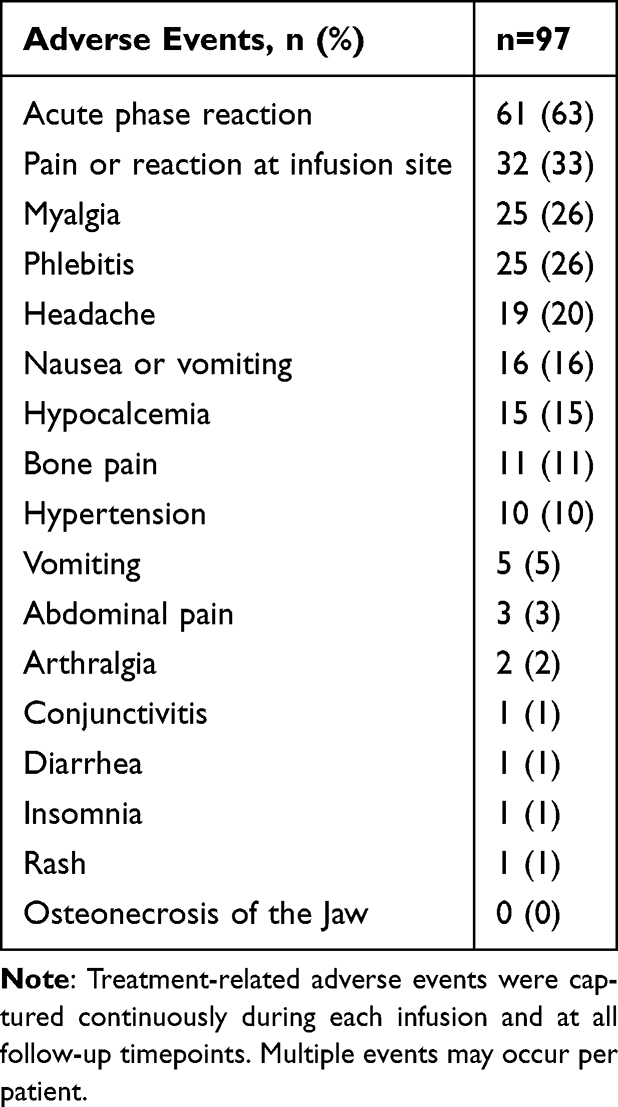 |
Table 4 Adverse Events |
Discussion
In this single-center retrospective observational study of predominantly persistent CRPS patients, pamidronate was associated with a modest short-term reduction in pain lasting up to 3 months. Adverse events were common but generally mild. Overall, these findings suggest limited clinical benefit of intravenous pamidronate in persistent CRPS, with cautious interpretation of longer-term outcomes.
Effectiveness of Bisphosphonates
The quality of evidence for bisphosphonate treatment was recently rated as low to moderate by the Cochrane review and the interventional CRPS guideline, and it was recommended for short-term pain relief with low to moderate certainty.13,16 In placebo-controlled trials, bisphosphonates (irrespective of compound, dosing, or route) reduced pain on the NRS with a standardized mean difference (SMD) of −2.6 (95% CI: −1.8 to −3.4).13 A pooled analysis by Fassio et al which also included post-stroke CRPS and active-controlled studies found a similar benefit, reporting a weighted mean difference (WMD) of −23.8 (95% CI: −28.0 to −19.6) on the VAS/NRS.11 Long-term durability has only been evaluated in the open-label extension of the neridronate RCT, in which almost all participants maintained their improvement at one-year follow-up.18 Several retrospective studies have reported significant long-term effects, with response rates ranging from 56% to 91% at 12 months or beyond. In addition, more than 75% of patients no longer met the CRPS diagnostic criteria or had fewer symptoms.18–21 Specifically for pamidronate, a small RCT demonstrated a significant pain reduction at 3 months after a single 60mg infusion, although no benefit was seen at 1 month.22 A recent retrospective study of 255 patients (mean symptom duration 24 months, variable dosing) found only 14.5% responders at 1 month, rising to 67.1% at 4 months.23 In contrast, our cohort showed a modest reduction in pain during treatment up to 3 months. The estimated MD remained small (MD −1.10 [95% CI: −1.49 to −0.70] at 1 month and −0.66 [95% CI: −1.13 to −0.20] at 3 months) and may therefore have limited clinical value, despite responder rates of 34% and 20%, respectively. Taken together, previous studies and our data confirm a robust early analgesic benefit but differ in terms of the magnitude and durability of the response.
Plausible explanations for the smaller effect size and limited durability in our study include the clearly different case-mix and methodological approach. Nevertheless, the symptom improvement observed in a subset of patients may reflect residual anti-inflammatory and neuromodulatory effects of pamidronate, even in the context of longstanding disease. In the RCTs and other long-term reports, males accounted for 23–55% of participants and the mean age was frequently above 55 years.19–21,23–26 In contrast, our study predominantly consisted of females (88%) with a median age of 45 years. Disease chronicity also differed significantly from previous studies. Bisphosphonate therapy was usually started within 6 months of the disease onset,19,20,24–26 reflecting mainly acute CRPS. This distinguishes our study, as we investigated a mixed population with a median CRPS duration and pain duration exceeding 1 year in most participants (70% and 87%, respectively), representing a cohort with predominantly persistent disease. This distinction is crucial, as several proposed mechanisms of bisphosphonates are time dependent. For example, inhibition of FFPS and the resulting decrease in pro-inflammatory cytokine release are only effective when inflammation is still active. Once residual damage and nociplastic changes have developed, the relevance of this anti-inflammatory mechanism likely diminishes.27 Similarly, bisphosphonate-induced reductions in microglial activation may help to prevent or limit peripheral and central sensitization, processes that otherwise become increasingly pronounced over time. Acute CRPS can also be difficult to distinguish from prolonged healing, disuse, or overuse. Consequently, early interventions may appear highly effective, although their apparent benefit can be confounded by natural recovery. Symptoms often improve within the first 6 months,2 while persistent CRPS is defined by symptoms lasting longer than 12 months.5 Moreover, some studies included concurrent physiotherapy,20,26 further confounding true treatment effects. In addition, our conservative handling of missing data and response rates may have led to lower estimates and responder rates than previously reported. In summary, the specific demographic profile, pathophysiological features of persistent CRPS, and conservative methodological approach are likely to explain the more modest and less durable treatment effects in our cohort. Although prior studies have suggested predictors of response, our data did not allow reliable identification of patient characteristics associated with a meaningful treatment response.
Tolerability of Bisphosphonates
Bisphosphonates are well tolerated in CRPS patients, with no serious adverse events, such as osteonecrosis of the jaw and atypical fractures, reported thus far.11 However, adverse events were more common in patients receiving bisphosphonates than in those receiving placebo (relative risk [RR]: 2.1; 95% CI: 1.3 to 3.5), affecting up to 63% of patients.11,13 We observed an even higher rate of treatment-related adverse events, reported by 88% of patients, with acute phase reactions being the most common (63%). Despite the high incidence of side effects, only 6 patients (6%) discontinued prematurely. Consistent with previous studies, our findings support the overall conclusion that bisphosphonates are well tolerated and safe in the treatment of CRPS.11,13
Strengths and Limitations
Drawing firm conclusions about the effectiveness of bisphosphonate therapy remains challenging given the limitations of the existing evidence. Most previous RCTs did not specify the diagnostic criteria used, enrolled patients with short disease duration, and were geographically concentrated in Italy, limiting generalizability and underrepresenting persistent CRPS. The few RCTs that included persistent CRPS patients were terminated early for futility,13 raising concerns about publication bias. While our findings contribute new data on persistent CRPS, they should be interpreted in light of the limitations posed by the single-arm retrospective observational design.
First, without a comparison group, observed changes cannot be fully separated from natural recovery, regression to the mean, or placebo effects. Although several features of this cohort mitigate these risks, they do not eliminate them. Most patients had persistent CRPS, a stage where spontaneous remission is uncommon.2 Many also had previously failed interventional treatments, a context in which explicit expectations of benefit are often dampened, potentially reducing expectancy-driven placebo responses.28 Even so, non-expectancy placebo mechanisms and unmeasured confounding (eg, psychosocial factors or subtle subtype differences that influence both treatment selection and outcomes) cannot be excluded. Second, the retrospective design resulted in missing or inconsistently reported data. We modeled pain trajectories with an LMM, which uses all available repeated measures. For the 1- and 3-month timepoints, data availability was higher, allowing more reliable estimation of short-term effects. In contrast, at the 6- and 12-month timepoints, more than 75% of patients were censored due to initiation of alternative therapies. As a result, conclusions regarding longer-term effectiveness are uncertain, and these should be interpreted with caution. Nevertheless, the overall pattern of pain trajectories, characterized by improvement during treatment followed by a subsequent decline, supports the conclusion that any analgesic benefit of pamidronate may be short-lasting. Last, our cohort included a higher proportion of persistent CRPS than prior trials, limiting comparability with studies of early disease. At the same time, our heterogeneous, practice-based sample better reflects routine care. Nonetheless, given the possible effect modification by duration, our findings likely generalize best to persistent CRPS rather than uniformly across all durations.
Conclusion
In routine clinical practice, intravenous pamidronate was generally well tolerated and associated with modest, short-term pain relief in patients with predominantly persistent CRPS. Given that this effect was modest and not sustained beyond the initial treatment period, the overall clinical benefit in persistent CRPS appears limited. These findings underscore the need for cautious interpretation and highlight the importance of further prospective studies to better define the role of bisphosphonates across different stages of CRPS.
Institutional Review Board Statement
This study was approved by the medical ethical review board of the Erasmus MC University Medical Center (MEC-2019-0319). The requirement for informed consent was waived by the board due to the retrospective nature of the study and the use of existing medical records. All patient data were handled in accordance with applicable data protection regulations and were pseudonymized prior to analysis to ensure patient confidentiality.
Abbreviations
BMI, Body mass index; CRPS, Complex regional pain syndrome; CSS, CRPS severity score; eGFR, estimated CKD‑EPI glomerular filtration rate; FPPS, farnesyl‑pyrophosphate synthase; IASP, International Association for the Study of Pain; IQR, Interquartile range; LMM, linear mixed-effects model; MAR, Missing‑at‑Random; MD, Mean difference; NRS, Numeric rating scale; OR, Odds ratio; RCT, Randomized controlled trial; RR, relative risk; sIL‑2R, soluble Interleukin‑2 receptor; SD, Standard deviation; SMD, Standardized mean difference; WMD, Weighted mean difference.
Data Sharing Statement
The data that support the findings of this study are available from the Erasmus MC University Medical Center but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are, however, available from the authors upon reasonable request and with permission of the Erasmus MC University Medical Center.
Acknowledgments
The authors gratefully acknowledge the Graduate School of Erasmus MC University Medical Center for their insightful critique and valuable feedback on this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all of these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors have no sources of funding to declare for this article.
Disclosure
Prof. Dr. F Huygen reports personal fees from ABBOTT; grants from Saluda and Boston Scientific, outside the submitted work. The authors declare that they have no other conflict of interest regarding the publication of this article.
References
1. D’Souza RS, Klasova J, Saini C, et al. Global burden of complex regional pain syndrome in at-risk populations: estimates of prevalence from 35 countries between 1993 and 2023. Anesth Analg. 2025. doi:10.1213/ANE.0000000000007421
2. Johnson S, Cowell F, Gillespie S, Goebel A. Complex regional pain syndrome what is the outcome? - a systematic review of the course and impact of CRPS at 12 months from symptom onset and beyond. Eur. J. Pain. 2022;26:1203–10. doi:10.1002/ejp.1953
3. Harden NR, Bruehl S, Perez R, et al. Validation of proposed diagnostic criteria (the “Budapest Criteria”) for complex regional pain syndrome. Pain. 2010;150:268–274. doi:10.1016/j.pain.2010.04.030
4. de Mos M, de Bruijn AG, Huygen FJ, Dieleman JP, Stricker BH, Sturkenboom MC. The incidence of complex regional pain syndrome: a population-based study. Pain. 2007;129:12–20. doi:10.1016/j.pain.2006.09.008
5. Goebel A, Birklein F, Brunner F, et al. The Valencia consensus-based adaptation of the IASP complex regional pain syndrome diagnostic criteria. Pain. 2021;162:2346–2348. doi:10.1097/j.pain.0000000000002245
6. Ferraro MC, O’Connell NE, Sommer C, et al. Complex regional pain syndrome: advances in epidemiology, pathophysiology, diagnosis, and treatment. Lancet Neurol. 2024;23:522–533. doi:10.1016/S1474-4422(24)00076-0
7. Mangnus TJP, Bharwani KD, Dirckx M, Huygen F. From a symptom-based to a mechanism-based pharmacotherapeutic treatment in complex regional pain syndrome. Drugs. 2022;82:511–531. doi:10.1007/s40265-022-01685-4
8. Harnik MA, Kesselring P, Ott A, Urman RD, Luedi MM. Complex regional pain syndrome (crps) and the value of early detection. Curr Pain Headache Rep. 2023;27:417–427. doi:10.1007/s11916-023-01124-3
9. Ballard T, Chargui S. Pamidronate. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025.
10. Tzschentke TM. Pharmacology of bisphosphonates in pain. Br J Pharmacol. 2021;178:1973–1994. doi:10.1111/bph.14799
11. Fassio A, Mantovani A, Gatti D, et al. Pharmacological treatment in adult patients with CRPS-I: a systematic review and meta-analysis of randomized controlled trials. Rheumatology. 2022;61:3534–3546. doi:10.1093/rheumatology/keac060
12. Wang L, Guo TZ, Hou S, et al. Bisphosphonates inhibit pain, bone loss, and inflammation in a rat tibia fracture model of complex regional pain syndrome. Anesth Analg. 2016;123:1033–1045. doi:10.1213/ANE.0000000000001518
13. Ferraro MC, Cashin AG, Wand BM, et al. Interventions for treating pain and disability in adults with complex regional pain syndrome- an overview of systematic reviews. Cochrane Database Syst Rev. 2023;6:CD009416.
14. von Elm E, Altman DG, Egger M, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. 2007;335:806–808. doi:10.1136/bmj.39335.541782.AD
15. Harden RN, Maihofner C, Abousaad E, et al. A prospective, multisite, international validation of the complex regional pain syndrome severity score. Pain. 2017;158:1430–1436. doi:10.1097/j.pain.0000000000000927
16. van der Spek DPC, Dirckx M, Mangnus TJP, Cohen SP, Huygen F. Complex regional pain syndrome. Pain Pract. 2025;25:e13413. doi:10.1111/papr.13413
17. Farrar JT, Young JP Jr, LaMoreaux L, Werth JL, Poole MR. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001;94:149–158. doi:10.1016/S0304-3959(01)00349-9
18. Varenna M, Gatti D, Zucchi F, et al. Long-term efficacy and safety of neridronate treatment in patients with complex regional pain syndrome type 1: a pre-specified, open-label, extension study. Ther Adv Musculoskelet Dis. 2022;14:1759720X221142274. doi:10.1177/1759720X221142274
19. Ciaffi J, Festuccia G, Ripamonti C, et al. Benign Evolution of Complex Regional Pain Syndrome (CRPS) type 1 in patients treated with intravenous neridronate: a single-center real-life experience. Pharmaceuticals. 2024;18:17. doi:10.3390/ph18010017
20. Varenna M, Zucchi F, Orsini F, Crotti C, Calabrese G, Caporali R. Is CRPS-1 a chronic disabling disease? A long-term, real-life study on patients treated with neridronate. Clin Med Insights Arthritis Musculoskelet Disord. 2024;17:11795441241294098. doi:10.1177/11795441241294098
21. Adami G, Fassio A, Rossini M, et al. Long-term effectiveness and predictors of bisphosphonate treatment in type I complex regional pain syndrome. Clin Exp Rheumatol. 2024;42:961–966. doi:10.55563/clinexprheumatol/sdv5qt
22. Robinson JN, Sandom J, Chapman PT. Efficacy of pamidronate in complex regional pain syndrome type I. Pain Med. 2004;5:276–280. doi:10.1111/j.1526-4637.2004.04038.x
23. Doussiere M, Besnier C, Hamidou Y, et al. Evaluation of the efficacy and tolerance of pamidronate in complex regional pain syndrom type 1. Sci Rep. 2025;15:25745. doi:10.1038/s41598-025-11356-5
24. Chevreau M, Romand X, Gaudin P, Juvin R, Baillet A. Bisphosphonates for treatment of complex regional pain syndrome type 1: a systematic literature review and meta-analysis of randomized controlled trials versus placebo. Joint Bone Spine. 2017;84:393–399. doi:10.1016/j.jbspin.2017.03.009
25. Varenna M, Braga V, Gatti D, et al. Intramuscular neridronate for the treatment of complex regional pain syndrome type 1: a randomized, double-blind, placebo-controlled study. Ther Adv Musculoskelet Dis. 2021;13:1759720X211014020. doi:10.1177/1759720X211014020
26. Varenna M, Manara M, Rovelli F, Zucchi F, Sinigaglia L. Predictors of responsiveness to bisphosphonate treatment in patients with complex regional pain syndrome type i: a retrospective chart analysis. Pain Med. 2017;18:1131–1138. doi:10.1093/pm/pnw207
27. Dirckx M, Stronks DL, Groeneweg G, Huygen FJ. Effect of immunomodulating medications in complex regional pain syndrome: a systematic review. Clin J Pain. 2012;28:355–363. doi:10.1097/AJP.0b013e31822efe30
28. Kaptchuk TJ, Hemond CC, Miller FG. Placebos in chronic pain: evidence, theory, ethics, and use in clinical practice. BMJ. 2020;370:m1668.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Reduced Visuospatial Attention in Personal Space is Not Limited to the Affected Limb in Complex Regional Pain Syndrome
Halicka M, Cousins OR, Ten Brink AF, Vittersø AD, Proulx MJ, Bultitude JH
Journal of Pain Research 2024, 17:1519-1529
Published Date: 23 April 2024
Hyperbaric Oxygen Therapy in Managing Chronic Pain Syndromes – A Systematic Review
Leys AM, Hans GH, Saldien V, Wildemeersch D
Journal of Pain Research 2026, 19:597243
Published Date: 24 March 2026