Back to Journals » Psoriasis: Targets and Therapy » Volume 15
Global Trends and Future Predictions of Psoriasis Burden: Insights from the GBD 2021 Study
Authors Gu X ![]() , Wang X
, Wang X ![]() , Bin Y, Xue R, Zhu G
, Bin Y, Xue R, Zhu G
Received 5 August 2025
Accepted for publication 25 November 2025
Published 24 December 2025 Volume 2025:15 Pages 569—580
DOI https://doi.org/10.2147/PTT.S558419
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Mio Nakamura
Xiaoyu Gu,1,* Xinquan Wang,2,* Yang Bin,1 Ruzeng Xue,1 Guannan Zhu1
1Department of Dermatology, Dermatology Hospital, Southern Medical University, Guangzhou, Guangdong, People’s Republic of China; 2Department of Dermatology, Xiangya Hospital, Central South University, Changsha, 410008, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guannan Zhu, Dermatology Hospital, Southern Medical University, 2 Lujing Road, Guangzhou, Guangdong, 510000, People’s Republic of China, Email [email protected] Ruzeng Xue, Dermatology Hospital, Southern Medical University, 2 Lujing Road, Guangzhou, Guangdong, 510000, People’s Republic of China, Email [email protected]
Background: Psoriasis is a common chronic inflammatory skin disorder, and the global burden of psoriasis has not been fully disclosed.
Methods: We extracted prevalence, incidence and disability-adjusted life years (DALYs) for psoriasis from 1990 to 2021 in Global Burden of Disease (GBD) and predicted trends in the next 15 years though ARIMA model.
Results: Globally, age-standardized incidence rate (ASIR) of psoriasis increased from 57 cases/100,000 people (95% CI: 55.3~58.8) in 1990 to 62 cases/100,000 people (95% CI: 60.1~63.9) in 2021. Age-standardized prevalence rate (ASPR) and age-standardized disability-adjusted life year rate (ASDR) exhibited similar trends of increases. The global ASIR, ASPR, and ASDR for males were significantly higher than females. In 2021, ASIR peaked in the 55– 69 ages, while ASPR and ASDR reached peaks between the ages of 65– 74. Regionally, ASPR, ASIR, and ASDR in 2021 were highest in high Socio-demographic index (SDI) regions. The highest global regions and countries of ASPR, ASIR and ASDR were Western Europe and Germany, respectively. The East Asia region and Republic of Equatorial Guinea showed most significant growth in these psoriasis indicators since 1990. Furthermore, there was a significant increase in ASIR (8.06%), ASPR (8.14%), and ASDR (13.64%) of global psoriasis over the next 15 years.
Conclusions: Global burden of psoriasis is expected to continuously increase, and strengthening risk-factor management and prioritizing high-risk subgroups (males, elderly, high SDI regions and Western Europe, etc) will be essential for region-specific strategies and future healthcare planning.
Keywords: psoriasis, prevalence, incidence, disability-adjusted life years
Introduction
Psoriasis is an immune-mediated, chronic relapsing inflammatory skin disease characterized primarily by scaly red plaques. It can affect the joints and is often associated with other multi-system diseases such as cardiovascular system diseases, digestive system diseases, and metabolic syndrome.1–3 Psoriasis develops at any age and greatly affects the quality of life for patients. In the United States, the direct costs of psoriasis range from $51.7 billion to $63.2 billion, indirect costs from $23.9 billion to $35.4 billion, and comorbidities contribute an estimated $36.4 billion annually, resulting in a total economic burden of between $112 billion and $135 billion.4 This indirectly reflects the significant economic burden that psoriasis poses to countries.
Currently, global epidemiology reports of psoriasis are incomplete, and prevalence or incidence rates vary across regions due to investigation methods.5–17 Early WHO reports and studies indicate psoriasis affects over 60 million adults and children globally.1 The incidence of psoriasis is roughly equal between males and females, with an average age of onset at 33 years and a bimodal distribution primarily occurring between the ages of 16–22 and 55−60.18 Furthermore, high-income countries have more significant incidence rates than others.19–22 Geographically, no significant correlation between latitude and psoriasis prevalence, with consistent prevalence rates across countries globally.23 However, above epidemiological data have not been updated for a long time, so relevant new data are required to guide prevention and treatment of psoriasis.
To promote global understanding of the epidemiology of psoriasis, the Global Burden of Disease (GBD) 2021 provides global public access to indicators related to psoriasis prevalence, incidence, and disability-adjusted life years (DALYs).24 To the best of our knowledge, a comprehensive analysis of the global burden of psoriasis by age group has not been fully conducted. Here, to better understand the dynamic epidemiologic data on psoriasis trends, this study extracted updated data from GBD 2021 and compared with 1990. Our analysis was disaggregated by gender, age, region, and sociodemographic index (SDI) to identify the populations most affected by psoriasis and to guide targeted prevention and treatment strategies.
Method
Data Acquisition and Download
Data for our study were extracted from the GBD 2021 database (https://vizhub.healthdata.org/gbd-results). This database used the latest epidemiological data and well-established standardized method DisMod-MR 2.1 (disease-model-Bayesian meta-regression). The adjustment for missing data and confounding factors aimed to quantify health levels and trends, and to regularly update the accuracy of the data.25
In the GBD 2021, psoriasis was defined as a common, chronic, and recurrent inflammatory skin disease characterized by abnormal epidermal keratinization and hyperproliferation. Psoriasis diagnosis was based on the international Classification of diseases 10 (ICD-10: L40 and L41). The severity of psoriasis was categorized as mild, moderate, and severe (Table S1). Years were extracted spanning 1990 to 2021, and key metrics included age-standardized prevalence rate (ASPR), age-standardized incidence rate (ASIR), age-standardized disability-adjusted life year rate (ASDR), number of prevalent cases, number of incidence cases, and number of DALYs. Population and area information indicators included age groups, genders, countries, regions, and SDI-classified areas, with the analysis covering 204 countries, 21 GBD regions, and five types of SDI-classified areas. Our study was guided by the Guidelines for Accurate and Transparent Reporting of Health Evaluations (GATHER)26(Table S2).
The SDI was a comprehensive indicator developed by GBD researchers in 2015 to assess the relationship between socioeconomic development and population health. It can be used to evaluate the socioeconomic status of a region. A comprehensive estimation was conducted for the original three covariate inputs (fertility rate for the age group 15 to 49, years of education for individuals aged 15 and above, and life expectancy lost per capita). An index value ranging from 0 to 1 was assigned to represent it. For the GBD 2021, the final SDI value was multiplied by 100 for reporting. A value of 0 represented the theoretically lowest level of development related to health, while a value of 100 represented the theoretically highest level. The higher the SDI value, the better the socioeconomic conditions and health status. The SDI is categorized into five levels based on its value: low, low-middle, middle, high-middle, and high. Patient age groups are divided into 20 categories: ages <5, ages 5–9, ages 10–14, ages 15–19, ages 20–24, ages 25–29, ages 30–34, ages 35–39, ages 40–44, ages 45–49, ages 50–54, ages 55–59, ages 60–64, ages 65–69, ages 70–74, ages 75–79, ages 80–84, ages 85–89, ages 90–94, and ages 95+.
Data Analysis
We conducted secondary analysis using relevant data extracted from GBD 2021. We calculated the counts and rates of key indicators such as ASPR, ASIR, and ASDR for psoriasis at the global, regional, and national levels. Among these, DALYs were calculated as the sum of Years Lived with Disability (YLDs) and Years of Life Lost (YLLs). DALYs represented the total number of healthy life years lost from the onset of the disease to death,27 serving as a crucial parameter for assessing the burden of disease.
Based on formula (1), we calculated the age-standardized rate (ASR) of psoriasis per 100,000 people in all age groups, and estimated the ASPR, ASIR, and ASDR:

In the formula (1), ASR was an indicator to compare the frequency of a disease across different populations or time points. By eliminating the influence of differences in population age structure, it would make the results more comparable. Age-specific rates (ai) referred to the frequency of the disease within a particular age group. The population size (or weight) (wi) reflected the representativeness or importance of that age group in the reference standard population. By weightily summing these values and dividing by the total population of the standard population, a standardized rate was obtained for assessing the prevalence of psoriasis.28 ASIR represents the incidence rate adjusted to the GBD standard population, allowing comparison across populations with different age structures, and ASPR and ASDR are derived using the same direct age-standardisation approach.
Additionally, we employed Jointpoint regression analysis to estimate the trends in ASIR, ASPR, and ASDR over time. Monte Carlo permutation tests were used to calculate the Average Annual Percent Change (AAPC) and 95% Confidence Intervals (CIs). The global average trend in the annual change of ASR over time was assessed using the AAPC, as per formula (2):29,30

Where wi represented the duration of each time period (in years), and bi represented the slope coefficient for each time period. The Autoregressive Integrated Moving Average (ARIMA) model predicted future trends in disease development by analyzing the time series of historical data.31 Based on data from GBD 2021, an ARIMA model was constructed, and the “forecast” R package was utilized to project the ASIR, ASPR and ASDR for the next 15 years.
Our work adhered to the Strengthening the Reporting of Cohort Studies in Surgery (STROCSS) guidelines for cohort studies, cross-sectional studies, and case–control studies. Statistical analyses were conducted using R version 4.2.3 and Joinpoint software, with a statistical significance defined as P<0.05.
Result
Global Trends
In 2021, the global burden of psoriasis remained severe with a total incidence of 5.10 million cases (95% CI: 4.95~5.25 million), representing a 78.76% increase since 1990. Meanwhile, ASIR increased with AAPC of 0.266 (95% CI: 0.251~0.282) from 1990 to 2021 (Table 1). In 2021, the global prevalence number of people with psoriasis reached 42.98 million cases (95% CI: 41.65~44.31 million), representing an increase of approximately 86.4% compared to the number of cases in 1990. Between 1990 and 2021, ASPR of psoriasis increased from 477.7 cases/100,000 people (95% CI: 462.1~492.7) to 516.0 cases/100,000 people (95% CI: 500.2 ~ 531.6), with AAPC of 0.243 (95% CI: 0.227~0.258), indicating an upward trend (Table S3). Additionally, DALYs of psoriasis reached 3.70 million cases (95% CI: 2.68~4.92 million) in 2021, representing an increase of 84.8% compared to 1990, when there were 2.00 million cases (95% CI: 1.44~2.67). ASDR increased from 41.1 (95% CI: 29.8~54.9) /100,000 population in 1990 to 44.4 (95% CI:32.2~59.2) /100,000 population in 2021, and AAPC was 0.242 (95% CI: 0.225~0.260) (Table S4).
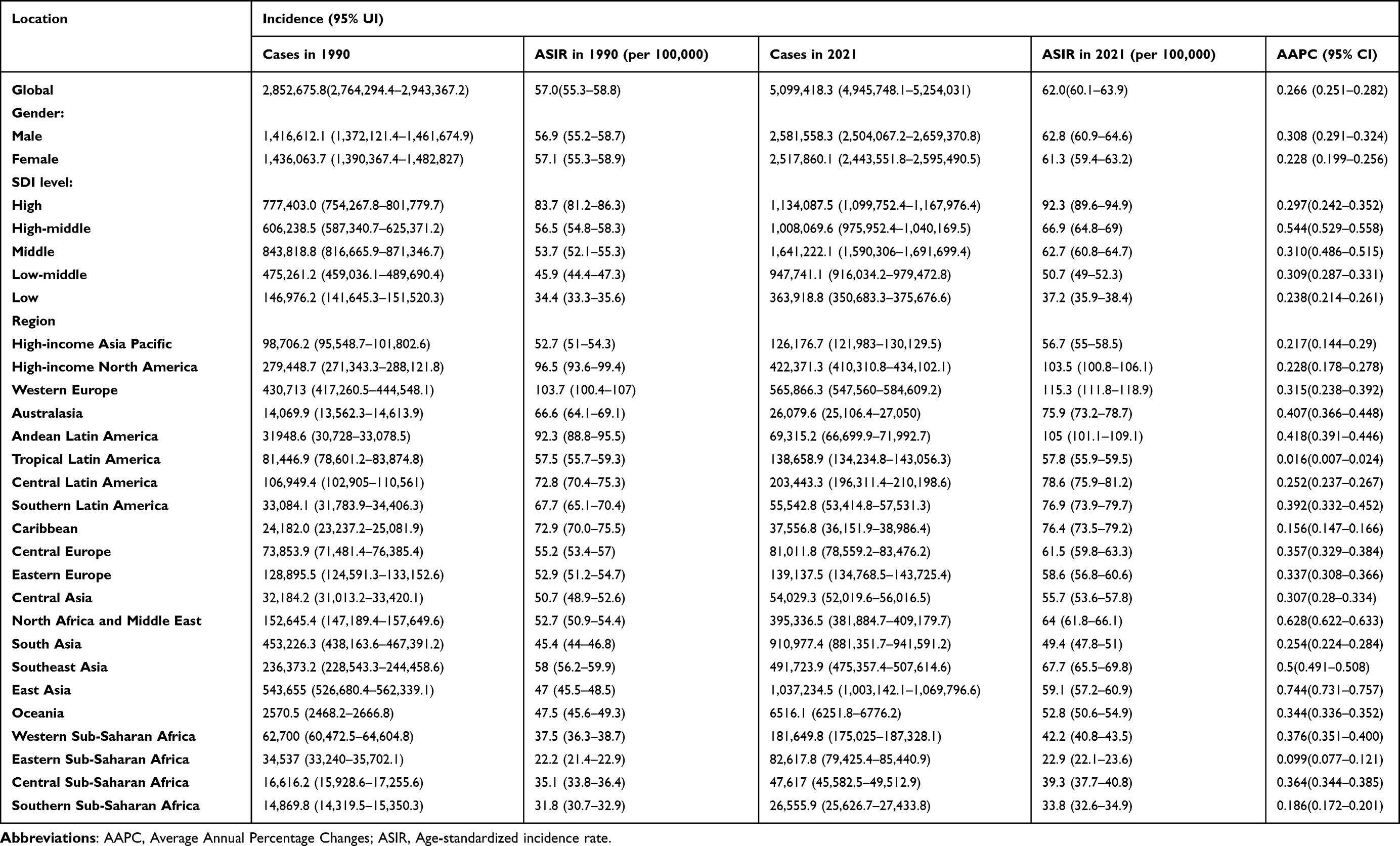 |
Table 1 ASIR and AAPC of Psoriasis at Global and Regional Level |
Global Trends by Gender
From 1990 to 2021, the global disease burden of psoriasis increased in both men and women. In 2021, the ASPR of psoriasis in male was 524.6 cases/100,000 population (95% CI: 508.4~541.1), 3.1% higher than that of psoriasis in female (508.4 cases/100,000 population [95% CI:492.9~523.7]). In 1990, the ASPR of male psoriasis was 478.9 (95% CI:463.0~494.6) cases/100,000 population, which was significantly higher than that of female psoriasis (476.8 cases /100,000 population [95% CI:461.7~491.8]) by 0.4%. Among them, the AAPC of males patients was 0.290 (95% CI:0.270~0.311) and that of females patients was 0.203 (95% CI: 0.186~0.219), indicating that the increase trend of male ASPR was significantly higher than female patients in the past 30 years.
The ASIR for psoriasis in males in 2021 was 62.8 cases/100,000 people (95% CI:60.9~64.6), which was 2.4% higher than in females (61.3 cases/100,000 people [95% CI:59.4~63.2]). The ASIR for psoriasis in females in 1990 was 57.1 cases/100,000 people (95% CI:55.3~58.9), which is 0.3% significantly higher than the males. The ASIR for psoriasis in females in 1990 was 57.1 (95% CI:55.3~58.9) cases/100,000 people, which was significantly higher than the ASIR for males (56.9[95% CI:55.2~58.7] cases/100,000 people) by 0.3%. The AAPC was 0.308 (95% CI:0.291~0.324) for males and 0.228 (95% CI:0.199~0.256) for females, suggesting that the increase in ASIR was significantly higher in males than in females. In addition, the ASDR of males and females also increased over the last 30+ years, with an AAPC of 0.198 (95% CI: 0.180~0.216) for females and 0.293 (95% CI: 0.274~0.311) for males, suggesting that male ASDR growth was significantly higher than that of females (Table 1 and Table S3 and S4).
Global Trends by Age Groups
Globally, the incidence of psoriasis exhibited a bimodal trend in growth between 1990 and 2021. In 2021, the peak incidence number was observed primarily in the age groups of 5–9 years and 50–54 years, with the latter age group being more prominent. The peak incidence in 1990 was mainly in the 5–9 years and 35–39 years age groups, with the 35–39 years age group being more significant. However, both the prevalence number of psoriasis patients and the DALYs showed a unimodal distribution. In 1990, the global number of psoriasis patients peaked in the 35–39 years age group. Nevertheless, in 2021, the global number of psoriasis patients peaked in the 50–54 years age group (Figure 1A).
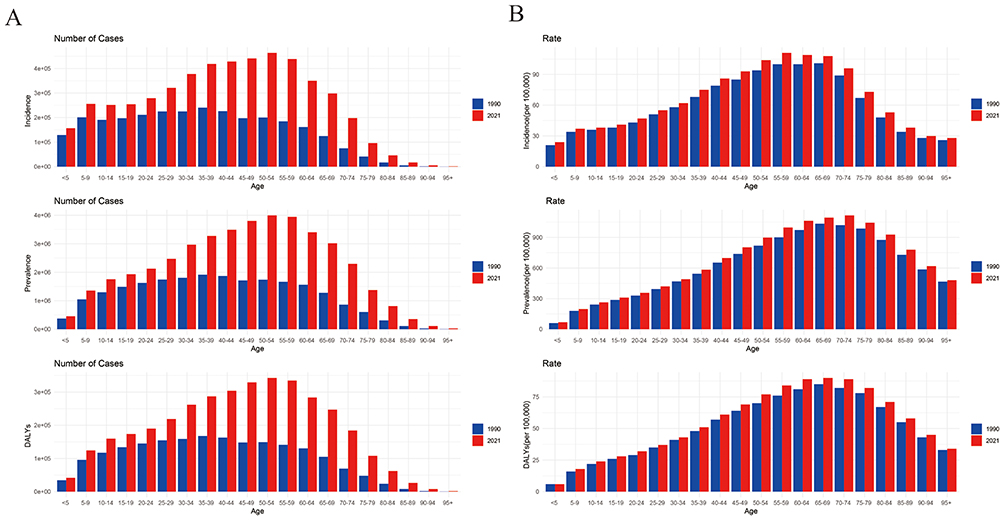 |
Figure 1 The disease burden of psoriasis by age in 1990 and 2021. (A) The cases of incidence, prevalence, and DALYs; (B) ASIR, ASPR and ASDR. Abbreviations: DALYs, Disability-adjusted life-years; ASIR, Age-standardized incidence rate; ASPR, Age-standardized prevalence rate; ASDR, Age-standardized disability-adjusted life-year rate. |
Similarly, globally, psoriasis ASIR by age peaked in 1990 and 2021 in the age group 55–69 years and declined with age. Psoriasis ASPR and ASDR peaked between the ages of 65–74 years (Figure 1B). Globally, ASIR, ASPR and ASDR increased in each age group between 1990 and 2021 (AAPC>0). The most significant increases in psoriasis ASPR (AAPC=0.431, 95% CI: 0.407~0.455), ASIR (AAPC=0.430, 95% CI: 0.397~0.463), and ASDR (AAPC=0.436, 95% CI: 0.407~0.464) were seen in those aged less than 5 years (Table S5).
In addition, we further analyzed the burden of disease for psoriasis by age group and gender. Globally, psoriasis peaked in 1990 at 35–44 years of age for both males and females in terms of prevalence and incidence. The number of DALYs peaked at 25–39 years of age for females in 1990, which is earlier than for males (peak at 40~44 years of age). However, in 2021, psoriasis appeared to peak at 50–55 years for both sexes in terms of the number of people with the disease, the number of morbidities, and the number of DALYs (Figure S1). Similarly, the peaks of ASPR, ASIR and ASDR in 1990 and 2021 in both sexes are mainly concentrated in older age (65–74 years) (Figure S2).
Global Trends by SDI
From 1990 to 2021, psoriasis ASIR was on the rise in all SDI regions (Figure 2). In 2021, psoriasis ASPR (852.3 cases/100,000, 95% CI: 830.1~875.3), ASIR (92.3 cases/100,000, 95% CI: 89.6~94.9) and ASDR (73.3 cases/100,000, 95% CI: 53.2~97.7) were consistently highest in areas with high SDI. Low SDI areas with psoriasis ASPR (268.9 cases/100,000, 95% CI: 260.5~277.4), ASIR (37.2 cases/100,000, 95% CI: 35.9~38.4) and ASDR (23.1 cases/100,000, 95% CI: 16.7~30.9) remained the lowest among all SDI regions. In particular, between 1990 and 2021, it is noteworthy that ASPR, ASIR and ASDR of psoriasis increased in all SDI regions (AAPC>0). In the high-middle SDI region, ASPR (AAPC=0.630, 95% CI: 0.619~0.641), ASIR (AAPC =0.544, 95% CI: 0.529~0.558) and ASDR (AAPC=0.638, 95% CI: 0.618~0.659) increased most significantly (Table 1 and Table S3 and S4).
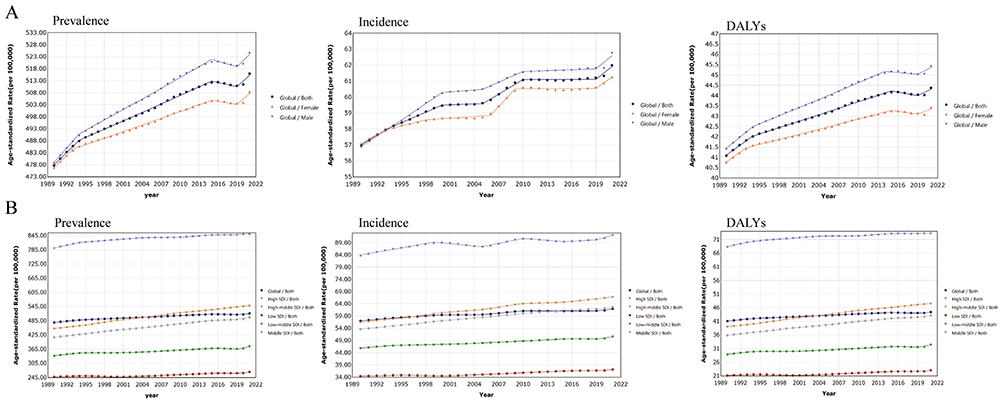 |
Figure 2 Changes in global psoriasis ASIR, ASPR, and ASDR from 1990–2021 (A) Stratified by sex; (B) Stratified by region. Abbreviations: ASIR, Age-standardized incidence rate; ASPR, Age-standardized prevalence rate; ASDR, Age-standardized disability-adjusted life-year rate. |
Regional Trends
The GBD regional classification system covered 204 countries and regions, categorized into 21 regions, which could exhibit significant differences in the ASPR, ASIR and ASDR of psoriasis (Figure 3 and Figure S3 and S4). In 2021, at the regional level, compared to other regions, Western Europe had the highest ASPR for psoriasis (1,155.9 cases/100,000, 95% CI: 1,119.4~1,194.5), ASIR (115.3 cases/100,000, 95% CI: 111.8~118.9), and ASDR (99.8 cases/100,000, 95% CI: 72.2~133.9). However, Eastern Sub-Saharan Africa had the lowest ASPR (150.2 cases/100,000, 95% CI: 145.4~155.1), ASIR (22.9 cases/100,000, 95% CI: 22.1~23.6), and ASDR (13.0 cases/100,000, 95% CI: 9.5~17.3).
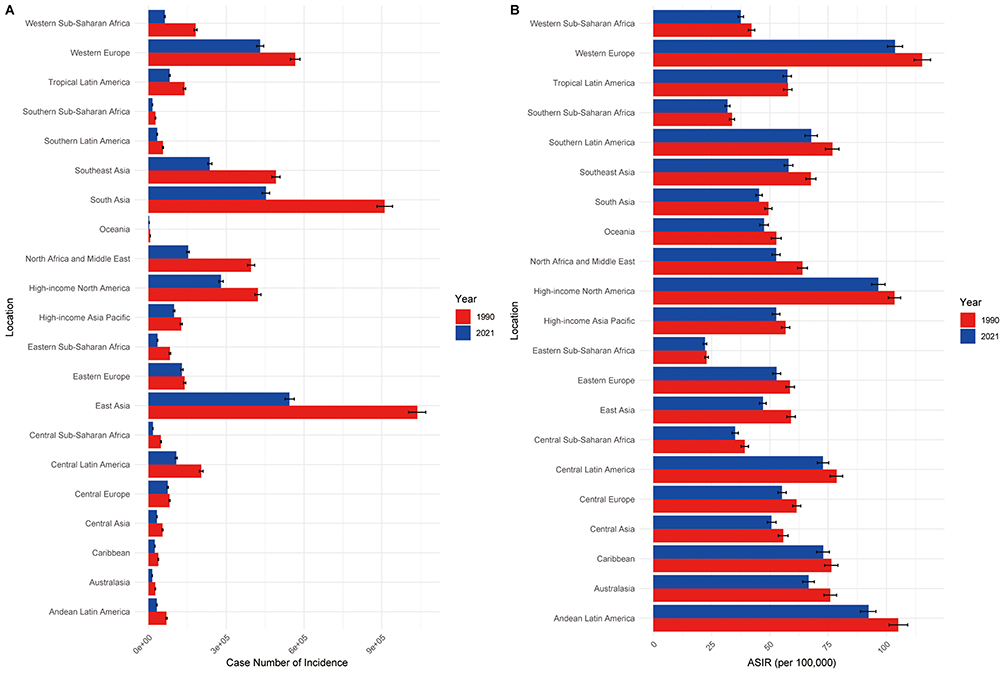 |
Figure 3 Incidence of psoriasis stratified by region in 1990 and 2021. (A) Regional incidence cases (B) Regional incidence rates. Abbreviations: ASIR, Age-standardized incidence rate. |
From 1990 to 2021, psoriasis ASIR, ASPR (except Tropical Latin America), and ASDR (except Tropical Latin America) were all on the rise in GBD. Among them, East Asia psoriasis ASIR (AAPC = 0.744, 95% CI: 0.731~0.757), ASPR (AAPC = 0.874, 95% CI: 0.849~0.899), and ASDR (AAPC = 0.880, 95% CI: 0.855~0.905) were the fastest growing. In addition, we explored the relationship between ASIR, ASPR, and ASDR and SDI in each region after correlating each GBD region with the SDI in each region. It was derived that the three major indicators increased in a wave pattern as the SDI gradually increased (Figure S5–S7).
National Trends
In 2021, China, India, USA, Germany, and Indonesia had the highest number of prevalence, incidence, and DALYs. China and India carried the highest burden of psoriasis globally, leading in the number of prevalent cases, incident cases, and DALYs. In addition, Qatar, United Arab Emirates, and Equatorial Guinea ranked highest in all three indicators when comparing the relative change in the number of cases of prevalence, incidence, and DALYs expectancy between 1990 and 2021 (Table S6). Qatar had the highest rate of change in the number of cases of prevalence (886.09%), incidence (813.69%), and DALYs (882.63%) expectancy (Figure S8–S10).
Globally, ASIR, ASPR and ASDR showed significant differences between countries in 2021 (Figure 4 and Figures S11 and S12). Germany, Switzerland, Monaco, Andorra, San Marino and Cyprus had the highest ASIR, ASPR and ASDR. For ASIR, Germany ranked first with 143.6 cases (95% CI: 148.7~139) /100,000 and Switzerland ranked second with 124.8 cases (129.1~120.7) / 100,000. From 1990 to 2021, Republic of Equatorial Guinea had a higher rate of ASPR (AAPC=1.344, 95% CI: 1.311~1.377), ASIR (AAPC=0.969, 95% CI: 0.947~0.991) and ASDR (AAPC=1.347, 95% CI: 1.280~1.413) had the greatest increase, followed by Sultanate of Oman and Republic of Maldives. In contrast, ASPR, ASIR and ASDR decreased significantly (AAPC<0) in the Republic of Burundi, the Republic of South Sudan and the Federal Republic of Somalia (Table S7).
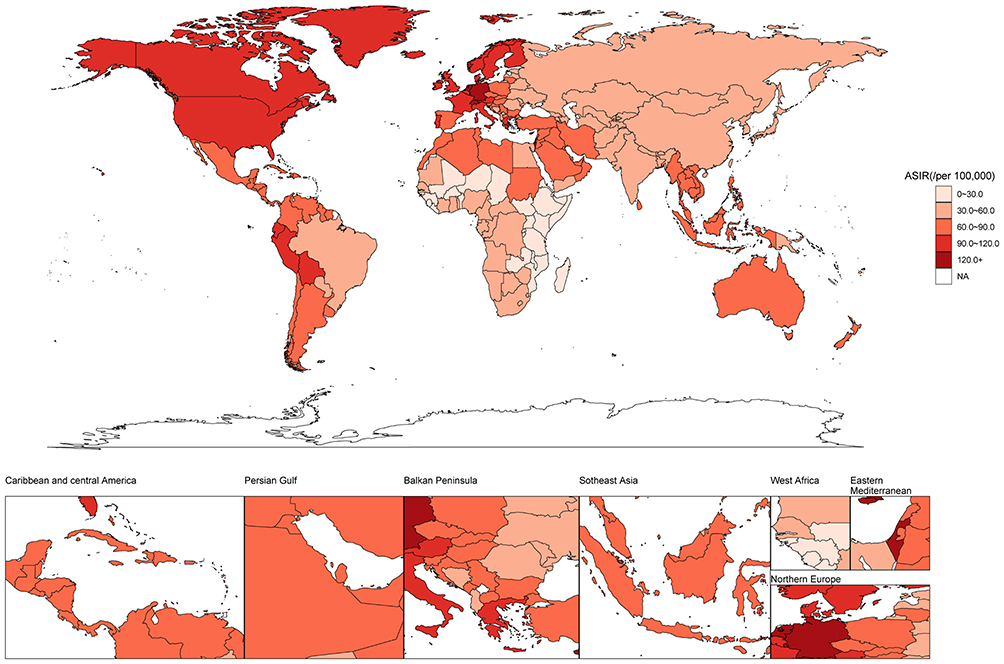 |
Figure 4 Global psoriasis ASIR distribution map. Abbreviations:ASIR, Age-standardized incidence rate. |
Future Forecasts of Global Burden of Psoriasis
The global burden of psoriasis was projected to change significantly between 2021 and 2036, with different measures showing different trends. The global ASIR of psoriasis for both sexes combined was slightly on the rise, with the ASIR projected to increase from approximately 62 cases/100,000 people in 2021 to approximately 67 cases/100,000 people in 2036 (an increased of 8.06%). The ASIR growth was significantly higher in males (6.35%) than in females (4.92%). The ASPR for psoriasis for both sexes combined was projected to rise globally from about 516 cases/100,000 people in 2021 to about 558 cases/100,000 people in 2036, an increase of about 8.14% in 15 years. For males, ASPR was projected to grow rapidly, slightly from about 525 cases/100,000 people in 2021 to 676 cases/100,000 people in 2040, an increase of about 28.76%, which compares favorably to females. In contrast, females were projected to grow slowly, from about 508 cases/100,000 people in 2021 to 544 cases/100,000 people in 2036, an annual growth rate of only 7.09%. The ASDR for both sexes combined was projected to continue to grow slowly, increasing slightly from 44 cases/100,000 people in 2021 to approximately 50 cases/100,000 people in 2036 (an increase of approximately 13.64%), with significantly higher growth in age-standardized ASDR in males (33.33%) than in females (11.63%). In all three metrics, males consistently grew more than females, and males grew significantly more rapidly than females, especially for ASPR and ASDR (Figure 5).
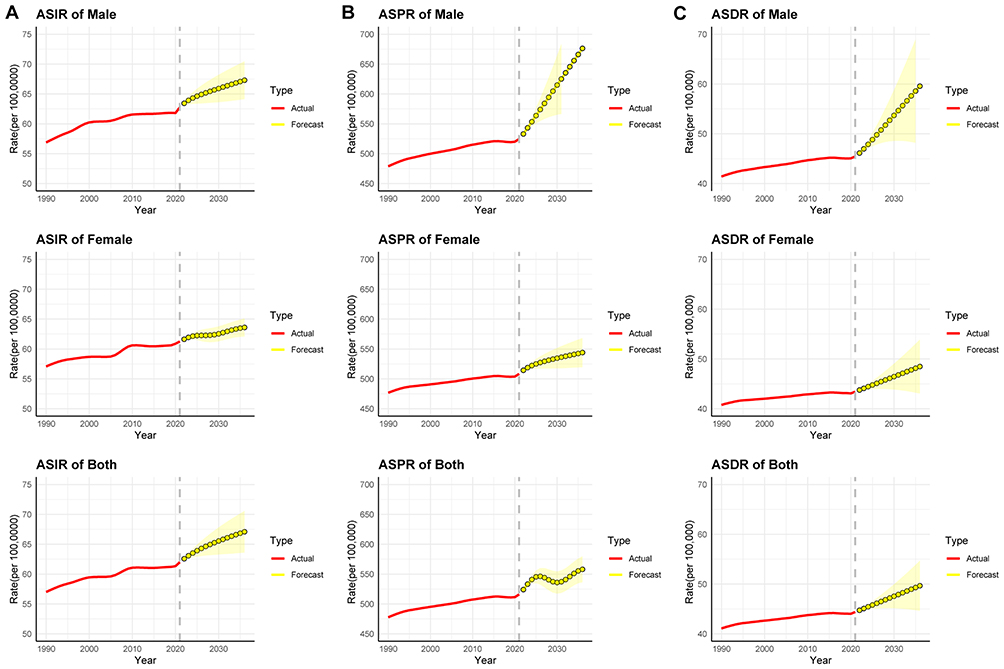 |
Figure 5 ARIMA predictive model stratified by sex to predict psoriasis disease burden over the next 15 years. (A)ASIR; (B) ASPR; (C) ASDR. Abbreviations: ASIR, Age-standardized incidence rate; ASPR, Age-standardized prevalence rate; ASDR, Age-standardized disability-adjusted life-year rate; ASIR, Age-standardized incidence rate; ASPR, Age-standardized prevalence rate; ASDR, Age-standardized disability-adjusted life-year rate. |
The number of incidences, prevalence and DALYs will also increase significantly globally in the future. Globally, there was a significant increase in the global incidence of psoriasis in both sexes combined. It was projected to increase from about 5.10 million cases in 2021 to 8.25 million cases in 2036, an increase of about 61.74%, indicating that the number of people with psoriasis has increased by at least twofold in the last 15 years. The increase in the number of cases in females (25.67%) was slightly higher than the number of cases in males (21.84%). The global prevalence will increase from about 42.98 million cases in 2021 to about 60.33 million cases in 2036, an increase of 40.36%. Among them, the increase in the number of prevalent cases was significantly higher in males (47.29%) than in females (34.11%). The number of psoriasis DALYs for both sexes combined is projected to continue its slow growth, with an overall increase of approximately 32.09% between 2021 and 2036 (Figure S13).
Discussion
In this study, we have provided the most up-to-date and comprehensive assessment of the ASPR, ASIR and ASDR of psoriasis at global, regional and national levels between 1990 and 2021, based on the GBD 2021 study. The results have showed complex variations and trends across regions and sociodemographic indicators, emphasizing the urgent need for more effective and targeted interventions.
Globally, global psoriasis ASIR, ASPR, and ASDR have increased during the last 30+ years, indicating a significant increase in the disease burden of psoriasis, which may be related to environmental changes (eg, environmental pollution and socioeconomics, etc).32 Our stratified analysis of the three major indicators of psoriasis globally shows that psoriasis has increased significantly faster in males than in females over the past 30 years. The ASIR and ASPR of males have gradually surpassed those of females, which is consistent with previous studies.33 Although some studies have also suggested that the incidence of psoriasis is relatively balanced between genders,34,35 a phenomenon that we speculate may be related to the physiological factors, lifestyle (smoking, drinking, exercise, etc), and differences in the expectation of treatment efficacy etc.3,36–38
We also conduct a stratified analysis of psoriasis incidence by age group, which shows a bimodal trend in 1990 and 2021. In 1990, the incidence peaks mainly in childhood and middle-aged, and is more pronounced in the 35–39 ages. However, in 2021, the incidence is mainly concentrated in childhood and middle-aged and older adults, and is more pronounced in the 50–54 ages. The ASIR, ASPR, and ASDR peaks in 1990 and 2021 in middle-aged and older adults (55–75 years) and then declines with age, which is associated with a gradual increase in mortality with age in the elderly and this trend is similar to the findings of previous studies.16,39 To differentiate the burden of disease by gender at different ages, we find that gender does not show differences in age groups. Global numbers of prevalence, incidence, and DALY shift progressively to higher ages in the study years, which may be explained by population aging and increasing population size.
A significant trend of increasing psoriasis ASPR, ASIR and ASDR is observed in all SDI regions from 1990 to 2021. Significant differences in psoriasis disease burden between regions with different levels of socioeconomic development are emphasized, which is attributed to multiple factors. In high SDI areas, which tend to be more industrialized, exposure to chemical compounds is greatly increased. Dietary changes (high-fat and high-sugar diets),40,41 psychosocial factors (stress, anxiety and depression, etc),42 and increased levels of disease awareness43 have led to a significantly higher psoriasis ASIR, and often resulted in a significantly higher burden of disease in these regions. For countries with large population bases (China, India, USA, Germany, India) their numbers of psoriasis incidence, prevalence, and DALYs are the greatest. Regional differences in psoriasis disease are strongly associated with genetic differences, environment exposure, and lifestyle.5,36,44,45 The disparities in these results may be related to differences in regional economic development and the uneven distribution of healthcare resources, particularly in the levels of disease diagnosis and treatment. Our estimates inherently reflect the cumulative impact of past therapeutic advances; therefore, the evolving treatment landscape—particularly biologic therapies—remains a key contextual factor for interpreting long-term trends. Future studies incorporating additional epidemiological, environmental, and behavioral data are needed to clarify the underlying causes of the observed sex-, economic-, regional-, and country-level differences.
Our study is the most up-to-date and comprehensive analysis of the global burden of psoriasis based on the GBD available. However, we should consider several limitations of this study. Firstly, despite the statistically robust methodology used in the GBD, there are marked differences in the quality and availability of disease data across countries and regions, especially in low- and middle-income countries that lack reliable and well-established disease registry systems. The estimates are not derived from real-world studies and are potentially biased, leading to possible underestimation of their true burden of disease or inaccurate data. Secondly, the variability in the levels and standards of psoriasis diagnosis and treatment across different countries worldwide may impact the accuracy of outcome estimations. Thirdly, our future psoriasis incidence patterns and trends are based on current conditions and do not take into account future changes in disease policies, medical technology levels, and other factors. Therefore, they should be predicted at different points in time and update at any time according to the actual situation. Furthermore, the estimates for 2020–2021 should be interpreted with caution, as the COVID-19 pandemic may have led to under-diagnosis and altered healthcare-seeking behaviors for psoriasis, potentially affecting data completeness and accuracy. Finally, the disability weights used in the calculation of DALYs are based on survey data, but the actual experience of people with psoriasis in different cultures is individualized.
In conclusion, despite advances in psoriasis treatment, global ASPR, ASIR, and ASDR have continued to rise, with middle-aged and older adults remaining the most affected populations. In the context of population aging and increasing comorbidities, strengthening risk-factor management and prioritizing high-risk subgroups will be essential for region-specific strategies and future healthcare planning.
Ethics Approval and Consent to Participate
This study used publicly available, aggregated, and de-identified data from the GBD study provided by the Institute for Health Metrics and Evaluation (IHME). The GBD data collection was approved by the Institutional Review Board (IRB) of the University of Washington. As this research involved secondary analysis of anonymized data without personal identifiers, additional ethical approval was not required. In accordance with Items 1 and 2 of Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects (February 18, 2023, China), this study was exempt from further ethical review.
Acknowledgments
We acknowledge the Institute for Health Metrics and Evaluation (IHME) for providing the GBD data, an invaluable resource for advancing public health research and evidence-based policies. We deeply appreciate their contributions.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Griffiths CEM, Armstrong AW, Gudjonsson JE, et al. Psoriasis. Lancet. 2021;397:1301–1315. doi:10.1016/S0140-6736(20)32549-6
2. Korman NJ. Management of psoriasis as a systemic disease: what is the evidence? Br J Dermatol. 2020;182:840–848. doi:10.1111/bjd.18245
3. Comorbidities in people with psoriasis. Br J Dermatol. 2024;190:e31. doi:10.1093/bjd/ljae026
4. Brezinski EA, Dhillon JS, Armstrong AW. Economic burden of psoriasis in the united states: a systematic review. JAMA Dermatol. 2015;151:651–658. doi:10.1001/jamadermatol.2014.3593
5. Chandran V, Raychaudhuri SP. Geoepidemiology and environmental factors of psoriasis and psoriatic arthritis. J Autoimmun. 2010;34:J314–21. doi:10.1016/j.jaut.2009.12.001
6. Danielsen K, Olsen AO, Wilsgaard T, et al. Is the prevalence of psoriasis increasing? A 30-year follow-up of a population-based cohort. Br J Dermatol. 2013;168:1303–1310. doi:10.1111/bjd.12230
7. Egeberg A, Skov L, Gislason GH, et al. Incidence and prevalence of psoriasis in denmark. Acta Derm Venereol. 2017;97:808–812. doi:10.2340/00015555-2672
8. Hernandez-Vasquez A, Molinari L, Larrea N, et al. Psoriasis in Latin America and the Caribbean: a systematic review. J Eur Acad Dermatol Venereol. 2017;31:1991–1998. doi:10.1111/jdv.14393
9. Lee JY, Kang S, Park JS, et al. Prevalence of Psoriasis in Korea: a Population-Based Epidemiological Study Using the Korean National Health Insurance Database. Ann Dermatol. 2017;29:761–767. doi:10.5021/ad.2017.29.6.761
10. Pezzolo E, Cazzaniga S, Colombo P, et al. Psoriasis incidence and lifetime prevalence: suggestion for a higher mortality rate in older age-classes among psoriatic patients compared to the general population in italy. Acta Derm Venereol. 2019;99:400–403. doi:10.2340/00015555-3130
11. Puig L, Ruiz de Morales JG, Dauden E, et al. Prevalence of ten Immune-mediated inflammatory diseases (IMID) in Spain. Rev Esp Salud Publica. 2019;93.
12. Romiti R, Amone M, Menter A, et al. Prevalence of psoriasis in Brazil - a geographical survey. Int J Dermatol. 2017;56:e167–e8. doi:10.1111/ijd.13604
13. Shalom G, Zisman D, Babaev M, et al. Psoriasis in Israel: demographic, epidemiology, and healthcare services utilization. Int J Dermatol. 2018;57:1068–1074. doi:10.1111/ijd.14130
14. Springate DA, Parisi R, Kontopantelis E, et al. Incidence, prevalence and mortality of patients with psoriasis: a U.K. population-based cohort study. Br J Dermatol. 2017;176:650–658. doi:10.1111/bjd.15021
15. Parisi R, Iskandar IYK, Kontopantelis E, et al. National, regional, and worldwide epidemiology of psoriasis: systematic analysis and modelling study. BMJ. 2020;369:m1590. doi:10.1136/bmj.m1590
16. Armstrong AW, Mehta MD, Schupp CW, et al. Psoriasis prevalence in adults in the united states. JAMA Dermatol. 2021;157:940–946. doi:10.1001/jamadermatol.2021.2007
17. Prinz JC, Choon SE, Griffiths CEM, et al. Prevalence, comorbidities and mortality of generalized pustular psoriasis: a literature review. J Eur Acad Dermatol Venereol. 2023;37:256–273. doi:10.1111/jdv.18720
18. Griffiths CE, Barker JN. Pathogenesis and clinical features of psoriasis. Lancet. 2007;370:263–271. doi:10.1016/S0140-6736(07)61128-3
19. Cantarutti A, Dona D, Visentin F, et al. Epidemiology of frequently occurring skin diseases in italian children from 2006 to 2012: a retrospective, population-based study. Pediatr Dermatol. 2015;32:668–678. doi:10.1111/pde.12568
20. Tollefson MM, Crowson CS, McEvoy MT, et al. Incidence of psoriasis in children: a population-based study. J Am Acad Dermatol. 2010;62:979–987. doi:10.1016/j.jaad.2009.07.029
21. Wei JC, Shi LH, Huang JY, et al. Epidemiology and medication pattern change of psoriatic diseases in taiwan from 2000 to 2013: a nationwide, population-based cohort study. J Rheumatol. 2018;45:385–392. doi:10.3899/jrheum.170516
22. Vena GA, Altomare G, Ayala F, et al. Incidence of psoriasis and association with comorbidities in Italy: a 5-year observational study from a national primary care database. Eur J Dermatol. 2010;20:593–598. doi:10.1684/ejd.2010.1017
23. Jacobson CC, Kumar S, Kimball AB. Latitude and psoriasis prevalence. J Am Acad Dermatol. 2011;65:870–873. doi:10.1016/j.jaad.2009.05.047
24. Murray CJL, Collaborators GBD. Findings from the Global Burden of Disease Study 2021. Lancet. 2024;403:2259–2262. doi:10.1016/S0140-6736(24)00769-4
25. Diseases GBD, Injuries C. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396:1204–1222.
26. Stevens GA, Alkema L, Black RE, et al. Guidelines for accurate and transparent health estimates reporting: the GATHER statement. Lancet. 2016;388:e19–e23. doi:10.1016/S0140-6736(16)30388-9
27. Collaborators GBDMD. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet Psychiatry. 2022;9:137–150. doi:10.1016/S2215-0366(21)00395-3
28. Lv B, JX L, Si YF, et al. Epidemiological trends of subarachnoid hemorrhage at global, regional, and national level: a trend analysis study from 1990 to 2021. Mil Med Res. 2024;11:46. doi:10.1186/s40779-024-00551-6
29. Yi X, He Y, Zhang Y, et al. Current status, trends, and predictions in the burden of silicosis in 204 countries and territories from 1990 to 2019. Front Public Health. 2023;11:1216924. doi:10.3389/fpubh.2023.1216924
30. Li Z, Zhang X, Sun C, et al. Global, regional, and national burdens of early onset pancreatic cancer in adolescents and adults aged 15-49 years from 1990 to 2019 based on the global burden of disease study 2019: a cross-sectional study. Int J Surg. 2024;110:1929–1940. doi:10.1097/JS9.0000000000001054
31. Vollset SE, Goren E, Yuan CW, et al. Fertility, mortality, migration, and population scenarios for 195 countries and territories from 2017 to 2100: a forecasting analysis for the global burden of disease study. Lancet. 2020;396:1285–1306. doi:10.1016/S0140-6736(20)30677-2
32. Bellinato F, Adami G, Vaienti S, et al. Association between short-term exposure to environmental air pollution and psoriasis flare. JAMA Dermatol. 2022;158:375–381. doi:10.1001/jamadermatol.2021.6019
33. Wang X, Ma R, Shi R, et al. Sex differences in the association between plasma polyunsaturated fatty acids levels and moderate-to-severe plaque psoriasis severity: a cross-sectional and longitudinal study. J Transl Med. 2023;21:834. doi:10.1186/s12967-023-04726-y
34. Nazir Z, Strunk A, Garg A. Age- and sex-adjusted prevalence estimates among adults with psoriasis in the United States. J Am Acad Dermatol. 2022;86:703–705. doi:10.1016/j.jaad.2021.03.020
35. Burshtein J, Strunk A, Garg A. Incidence of psoriasis among adults in the United States: a sex- and age-adjusted population analysis. J Am Acad Dermatol. 2021;84:1023–1029. doi:10.1016/j.jaad.2020.11.039
36. Shen M, Xiao Y, Jing D, et al. Associations of combined lifestyle and genetic risks with incident psoriasis: a prospective cohort study among UK Biobank participants of European ancestry. J Am Acad Dermatol. 2022;87:343–350. doi:10.1016/j.jaad.2022.04.006
37. JT M, AA N, Sommer R, et al. Gender and age significantly determine patient needs and treatment goals in psoriasis - a lesson for practice. J Eur Acad Dermatol Venereol. 2019;33:700–708. doi:10.1111/jdv.15324
38. Napolitano M, Mastroeni S, Fania L, et al. Sex- and gender-associated clinical and psychosocial characteristics of patients with psoriasis. Clin Exp Dermatol. 2020;45:705–711. doi:10.1111/ced.14218
39. Iskandar IYK, Parisi R, Griffiths CEM, et al. Systematic review examining changes over time and variation in the incidence and prevalence of psoriasis by age and gender. Br J Dermatol. 2021;184:243–258. doi:10.1111/bjd.19169
40. Sonomoto K, Song R, Eriksson D, et al. High-fat-diet-associated intestinal microbiota exacerbates psoriasis-like inflammation by enhancing systemic gammadelta T cell IL-17 production. Cell Rep. 2023;42:112713. doi:10.1016/j.celrep.2023.112713
41. Shi Z, Wu X, Santos Rocha C, et al. Short-term western diet intake promotes il-23‒mediated skin and joint inflammation accompanied by changes to the gut microbiota in mice. J Invest Dermatol. 2021;141:1780–1791. doi:10.1016/j.jid.2020.11.032
42. Snast I, Reiter O, Atzmony L, et al. Psychological stress and psoriasis: a systematic review and meta-analysis. Br J Dermatol. 2018;178:1044–1055. doi:10.1111/bjd.16116
43. Ozer I, Yildirim DI. Social awareness about psoriasis: misconceptions, negative prejudices and discriminatory behavior. Dermatol Ther. 2020;33:e14059. doi:10.1111/dth.14059
44. Huang YW, Tsai TF. HLA-Cw1 and Psoriasis. Am J Clin Dermatol. 2021;22:339–347. doi:10.1007/s40257-020-00585-1
45. Gu X, Li Z, Su J. Air pollution and skin diseases: a comprehensive evaluation of the associated mechanism. Ecotoxicol Environ Saf. 2024;278:116429. doi:10.1016/j.ecoenv.2024.116429
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Epidemiological Characteristics of Chronic Viral Hepatitis in Kazakhstan: Data from Unified Nationwide Electronic Healthcare System 2014–2019
Ashimkhanova A, Syssoyev D, Gusmanov A, Yesmembetov K, Yespotayeva A, Abbay A, Nurpeissova A, Sarria-Santamera A, Gaipov A
Infection and Drug Resistance 2022, 15:3333-3346
Published Date: 27 June 2022
Assessment of the Prevalence and Incidence of COVID-19 in Saudi Arabia
Alyahyawi HE, Alharbi RA, Alatawi SK, Ahmed WAM, Almalki SSR
Journal of Multidisciplinary Healthcare 2023, 16:227-236
Published Date: 24 January 2023
Cutaneous Adverse Events After COVID-19 Vaccination
Weschawalit S, Pongcharoen P, Suthiwartnarueput W, Srivilaithon W, Daorattanachai K, Jongrak P, Chakkavittumrong P
Clinical, Cosmetic and Investigational Dermatology 2023, 16:1473-1484
Published Date: 8 June 2023
Disease Burden of Neck Pain in China from 1990 to 2021 and Its Prediction for 2042: The Global Burden of Disease Study 2021
Wei J, Yang K, Xue J, Luo M, Peng W, Yin X, Sun W, Gao C, Teng G, Yin H, Feng M, Li L, Sun K, Zhang W
Journal of Pain Research 2025, 18:1975-1990
Published Date: 11 April 2025
Global, Regional, and National Burden of Alopecia Areata in Children and Adolescents Aged 0-19 years from 1990 to 2021 and Projection to 2040
Lu H, Li J, Ma K, Li L, Wang S, Wang T, Zhang B
Clinical, Cosmetic and Investigational Dermatology 2026, 19:582775
Published Date: 6 February 2026