Back to Journals » Patient Related Outcome Measures » Volume 14
Generating Items for Measuring Needs-Based Quality of Life and Self-Perceived Health Inequity in Patients with Multimorbidity: Development of the MultiMorbidity Questionnaire (MMQ)
Authors Bissenbakker KH ![]() , Møller A, Jønsson ABR, Brodersen JB
, Møller A, Jønsson ABR, Brodersen JB ![]()
Received 22 June 2023
Accepted for publication 30 September 2023
Published 10 October 2023 Volume 2023:14 Pages 269—282
DOI https://doi.org/10.2147/PROM.S427183
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Robert Howland
Kristine Henderson Bissenbakker,1,2 Anne Møller,1,2 Alexandra Brandt Ryborg Jønsson,3 John Brandt Brodersen1,2
1Research Unit for General Practice and Section of General Practice, Department of Public Health, University of Copenhagen, Copenhagen, Denmark; 2The Research Unit for General Practice in Region Zealand, Primary and eHealth Care, Region Zealand, Denmark; 3Department of People and Technology, Roskilde University, Copenhagen, Denmark
Correspondence: Kristine Henderson Bissenbakker, Øster Farimagsgade 5, Building 24, Copenhagen, 1353, Denmark, Tel +45 3532 7171, Email [email protected]
Purpose: To describe the processes of developing domains and items for the MultiMorbidity Questionnaire (MMQ), a multimorbidity-specific PROM for the assessment of Needs-based QoL.
Patients and Methods: We developed items and domains for the MMQ through 17 qualitative content validity questionnaire interviews with adults with multimorbidity by testing items from an item bank (covering items with content inspired by existing Needs-based QoL measures for single diseases). The interviews alternated between an explorative part and more focused cognitive interview techniques.
Results: Testing the 47 items from the first draft of the MMQ items showed that the Needs-based approach as a framework did not cover all the QoL aspects our informants stated as being important. Therefore, the conceptual framework was supplemented by Self-perceived health inequity, and new items were generated. MMQ, measuring Needs-based QoL (MMQ1) and Self-perceived health inequity (MMQ2), was assembled. MMQ1 covers the domains: “Physical ability” (10 items), “Limitations in everyday life” (15 items), “Worries” (11 items), “My social life” (11 items), “Self-image” (12 items), and “Personal finances” (2 items). Self-perceived health inequity proved to be a relevant framework for other aspects of QoL not covered by the Needs-based approach to QoL. MMQ2 covers the domains: “Experiences of being stigmatized” (five items), “Experiences of not being seen and heard” (four items), “Insufficient understanding of the burden of disease” (three items) and “Experiences of feeling powerless” (five items).
Conclusion: We have developed the final MMQ draft, a multimorbidity-specific PROM for the assessment of Needs-based QoL (MMQ1) and Self-perceived health inequity (MMQ2) with high content validity (regarding content relevance and comprehensiveness). The final MMQ draft will be assessed for its psychometric properties using Modern Test Theory.
Keywords: quality of life, multimorbidity, patient-reported outcome measure, item generation, needs-based approach, self-perceived health inequity
Introduction
An increasing number of patients live with multimorbidity, most often described as the co-occurrence of two or more chronic conditions in one individual.1–3 Multimorbidity is a burden both to society and the individual patient.4–6 Patients struggle to handle the complexities of symptoms, diagnoses, and information, which leads to an increase in the burden of disease and treatment as well as to a lower self-reported quality of life (QoL).5–11 Epidemiologically, it is well-known that disease and treatment burden affects different patient groups disproportionally, as there is an inverse relationship between socio-economic status and self-perceived health status as well as mortality from various diseases.12 For the individual, this structural problem can lead to a feeling of subjective health inequity, termed Self-perceived health inequity in the present study. This covers reactions to how you feel you are perceived when in contact with the healthcare system because of social determinants such as educational background and socio-economic status.13 To the best of our knowledge, it has not been explored how Self-perceived health inequity influences the QoL of patients with multimorbidity.
Due to societal and individual problems related to multimorbidity, numerous intervention studies target these patients and aspects of their QoL.14 Surprisingly, in a recent systematic review, we found no patient-reported outcome measure (PROM) for measuring QoL with adequate measurement properties for patients with multimorbidity.15 Consequently, measures employed in intervention studies and the assessed effects of these studies vary, resulting in inconsistent evidence to support outcomes from specific interventions.14,16
Therefore, we plan to develop the Multimorbidity Questionnaire (MMQ), a PROM to measure Needs-based QoL in patients with multimorbidity. The Needs-based approach to QoL presumes that a person’s ability and opportunity to fulfil their individual needs is decisive for their QoL.17,18 We have chosen this framework for measuring QoL as it implies a holistic view and involves the targeted patient group in the development process, thereby securing high content validity (content relevance and coverage) and understandability of the items.19 As a result, existing Needs-based QoL measures for specific single chronic diseases have shown more responsiveness than the most frequently used generic measures.20
The first step in developing a PROM is to describe the theoretical framework to clarify what is intended to be measured.19,21,22 Therefore, the Needs-based approach was conceptualised for our target group in previous work.23 Through qualitative interviews, we found six domains relevant specifically for and defined by patients with multimorbidity regarding their Needs-based QoL: “Physical ability”, “Self-determination”, “Security”, “Partner and social life”, “Self-image”, and “Personal finances.”23 The second step of MMQ’s development process is to generate relevant item content ensuring the content validity.21 Therefore, the aims of this study were twofold: 1. To develop items for a PROM measuring Needs-based QoL in patients with multimorbidity through qualitative interviews in the predefined domains (Box 1). 2. To explore if Self-perceived health inequity influences the QoL of patients with multimorbidity – and if so, to develop domains and items covering this conceptual framework.
 |
Box 1 Predefined Domains |
Materials and Methods
Study Design and Setting
We used COSMINs (COnsensus-based Standards for the selection of health status Measurement INstruments) Risk of Bias Checklist for assessment of PROMs as a framework for the step-by-step procedure of developing content valid items for the MMQ.24 We tested items from our item bank (elaborated below) for their content relevance and content coverage in qualitative interviews with adults living with multimorbidity. Where these informants found a lack of content coverage of the item-bank compared to the six predefined domains (Box 1) they generated new items specifically relevant for them as patients with multimorbidity. In this process, Self-perceived health inequity as a framework was tested by introducing items and domains covering other aspects of QoL when living with multimorbidity than the Needs-based model. Finally, we tested all items for understandability.
We included 11 informants, and 17 qualitative content validity questionnaire interviews were carried out, as four of the informants were interviewed more than once. New items were developed continuously throughout the interview phase, and repeated interviews allowed for testing items that were not included in the initial interviews and for comparison within and between the participants. The interviews were conducted from December 2018 to October 2019, mainly by the first author (medical doctor), but in close collaboration with the co-authors, an anthropologist and two general practitioners (GPs) and researchers. The interviews took place privately in the informants’ homes, apart from one conducted at the informant’s GPs clinic at his request and two by telephone. The telephone interviews were with informants previously interviewed face-to-face. All the interviews lasted about 1 hr, were carried out in Danish, audio-recorded and later transcribed (apart from the telephone interviews). The first author wrote field notes with observations immediately after each interview.
Informants
The informants represent the target group that the PROM is to be used among to ensure content validity.25,26 The informants were above 18, had two or more chronic diagnoses and lived on the island of Zealand (Denmark), and had no connection to the first author. They were recruited via eight GPs, who in initial contact with each of the eligible informants told them briefly about the study and asked permission for the first author to contact them. The informants consisted of a purposive sample, a concept-driven approach of gathering informants most fruitful for the research question.27 This involved specifying inclusion criteria to obtain data from informants affected by the complexities of living with multimorbidity. We constructed the sampling choices based on knowledge of how both socio-economic status and psychiatric diseases are associated with multimorbidity and specific patterns of the effect of multimorbidity on QoL.28–30 Therefore, the inclusion criteria cover specifications such as “age under 65 years and/or one or more psychiatric diagnoses and/or low education” (Supplementary File 1).23,31 Of the 21 eligible patients recruited by the GPs, 11 agreed to participate, 6 was not possible to get in contact with by the first author, and 4 did not find it possible to participate. The sampled informants included common multimorbidity patterns, with diagnoses such as coronary heart disease, diabetes, chronic obstructive pulmonary disease (COPD) and depression.28 To ensure diversity among informants, they varied in age, gender, marital status, diagnoses, and level of education (Table 1). A thorough purposive sampling generated data with high information power that allowed for a relatively small sample size.32 Information power of the data was ensured by holding a constant focus on the aim of the study, specificity of the sample, variation of the gathered data, applied conceptual frameworks, and quality of the dialogue in the interviews throughout all phases.32
 |
Table 1 Characteristics of the Informants |
Data Collection
Item Bank
We assembled an item bank, a pool of possible items for measuring QoL in patients with multimorbidity. As our systematic review yielded no PROMs specifically for patients with multimorbidity regarding their QoL, the item bank consisted of items from existing Needs-based PROMs for patients with the following single diagnosis: depression, pulmonary hypertension, COPD, and asthma.17,33–35 Items were selected by the first author if the content was not condition-specific and possessed face validity. Face validity implies that items are identified as relevant for the subject matter by experts in the field.36,37 Therefore, the selected items were probed for their relevance and comprehensiveness in the author group. Furthermore, content of each item was scrutinised for redundancy and double-barrelled items, or ambiguous items were rephrased. Additionally, themes and quotes from transcribed interviews from a qualitative project concerning patients with multimorbidity and poor self-care were constructed into draft items by the first author and revised by the co-authors.38 Table 2 gives examples of rephrasing/constructing items.
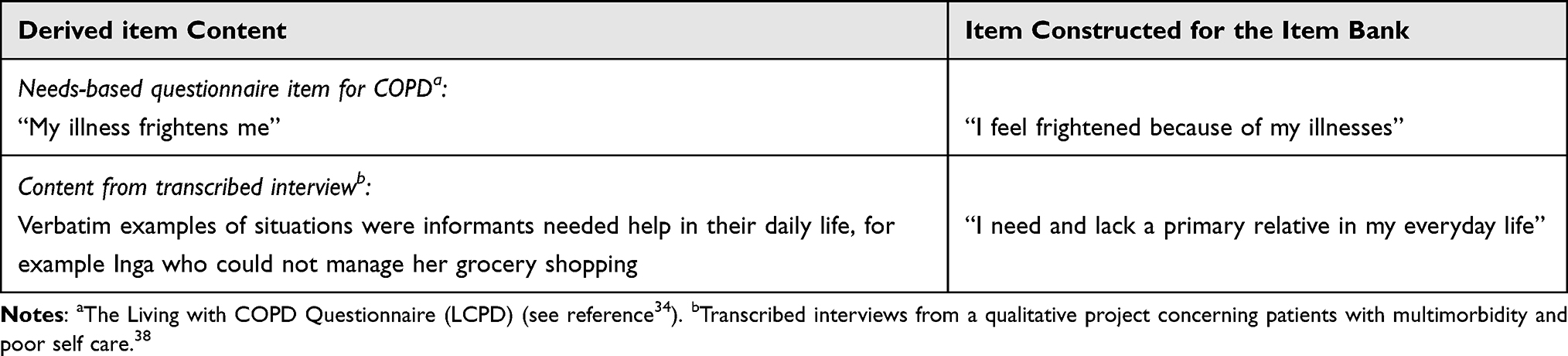 |
Table 2 Rephrasing and Constructing Items for the Item Bank |
The revised item bank consisted of 47 items with unique content and served as the first MMQ draft (Supplementary File 2). Response options were constructed based on experience from previous scale development into the following categories: “No, not at all”, “yes, a little bit”, “yes, quite a lot”, “yes, a lot.” The response option “not applicable” was added to some items, eg, regarding work or a partner. We tested the relevance, comprehensiveness, and ease of completing the response options in all interviews.
Interviews
Each interview alternated between structured cognitive (qualitative) interview techniques focusing on the MMQ draft and an explorative (semi-structured) approach emphasising the informants’ narratives.39–43 Focusing on the MMQ draft as an interview guide, items were endorsed, modified, excluded, or new items were developed. If an item was endorsed, it was grouped in cooperation with the informants into predefined Needs-based QoL domains (Box 1).23
After the first four interviews, we revisited the transcriptions of our previous interviews and discussed our findings within the author group. Consequently, it was decided to test Self-perceived health inequity as a framework covering other aspects of QoL when living with multimorbidity than the Needs-based model. Two preliminary domains were developed by the authors: “feeling of injustice” and “stigmatization.” Moreover, AJ formulated 10 items covering experiences of Self-perceived health inequity in encounters with health-care professionals and local authorities (Supplementary File 3). The preliminary domains and items were based on transcribed interviews, extensive ethnographical fieldwork including notes and transcribed interviews from previous studies regarding subjective health inequity, and theory and frameworks on stigma.44–53 The author group revised the items before they were tested in subsequent interviews along with the items from the item bank.
Throughout the interview phase, the MMQ draft was continuously adjusted in an iterative process to explore whether the PROM implies content relevance, coverage, and understandability.39,40 The analysis of the content validity and the understandability were conducted with informants by testing items using cognitive interviewing; qualitative techniques rooted in cognitive psychology were applied to questionnaire development in order to study how respondents mentally process items.41 This involves identifying unobservable measurement problems such as whether the informant understood each question as intended, if the informant could retrieve this information from memory, and other processes that influence the answer they would give.39,40 In practical terms, this was done by think-aloud test and verbal probing. Informants were asked using the think-aloud test to read aloud item by item and encouraged to say what came into their minds. Here, the interviewers tested for understandability and observed whether there were items that provoked or made the informants feel uncomfortable. In this case the item was rephrased or removed. Verbal probing ensures comprehensiveness of the items and the response categories by getting descriptive verbatim responses from the informant.25,40 We did this by asking questions such as: “Can you tell me in your own words how that situation affected you?” Although the MMQ draft and cognitive interview techniques guided the interviews, they were structured to allow the interviews to move to a more explorative approach. This was a deliberate choice as the items in many situations proved to serve as vignettes or cases, opening the interview to sensitive topics, as the focus was on a third person as a starting point.42,43 Iteratively structuring the interviews to let the informants lead the direction in such cases captured their narratives, including their perspectives and priorities regarding their QoL.54 When informants pointed to gaps in predefined domains and items or if they felt that aspects beyond the needs-based QoL framework were missing, they were encouraged to talk freely about these issues in their own words.55 This allowed new themes to emerge, and thereby we continuously formulated new items from the informants’ verbatim comments.19,21,56
New items were integrated with the existing items in the MMQ draft in an iterative process, testing them in the following interview. Each item in the MMQ draft was continuously validated by the informants and revised after each interview, ensuring that as far as possible each item is the informant’s own wording.55
The explorative parts of the interviews contributed to the conceptual phase of developing MMQ.23
When reporting the patients’ experiences, we use the term illness to encompass all health-related terms such as health problems, chronic conditions, diagnosis, illness, disease, or sickness. This term was chosen to emphasise the patient's perspective, not necessarily as an expression of trustworthiness concerning a specific condition or diagnosis.
Data Analysis
Data consisted of MMQ drafts and transcribed interviews. The MMQ drafts were continuously analysed and adjusted with the informants through cognitive interviewing as described in the section “interviews.” The transcribed interviews were thematically analysed using Braun and Clarke’s reflexive approach; first they were read in full text and thereafter systematically coded using NVivo.57,58 This was a circular abductive process contributing to introduction of new theories and revisions of the MMQ drafts. The revisions were then tested and analysed in subsequent interviews with informants.
Results
All 47 items from the first draft of the MMQ stemming from a Needs-based approach were probed in qualitative interviews with informants living with multimorbidity.18,56 Primarily, new items were generated during this phase.
Testing the items showed that the Needs-based approach as a framework did not cover all the QoL aspects our informants stated as being important. In this process, conversations originating from the domain “Self-image”, on how the informants looked at and felt about themselves were given a great deal of attention, and new themes and items were revealed. From the domain emerged the subthemes “status”, on how the informants felt their multimorbidity had affected their status in society and “the expectations of those around them.” This subtheme emerges from conversations on QoL and unfolds as frustration towards those around them as they felt labelled because of their chronic conditions. These issues were raised repeatedly in the first interviews and proved to go beyond the two subthemes. The anthropologist in our author group saw a connection between the informants’ descriptions of feeling labelled, even stigmatised, because of their chronic conditions and her previous studies on Subjective health inequity when living with multimorbidity.49,50,52 The informants recognised, gave examples, and thereby validated but modified the two preliminary domains and 10 items. They did not use the term Self-perceived health inequity but spoke in detail of experiences of feeling that their illnesses negatively influenced how they felt they were perceived by the people around them. Consequently, the MMQ draft was divided into MMQ1 (measuring Needs-based QoL) and MMQ2 (measuring Self-perceived health inequity). The process of modifying and generating items for MMQ1, the domains and 10 items for MMQ2, and generating new items is described in detail below and summed up in Figure 1.
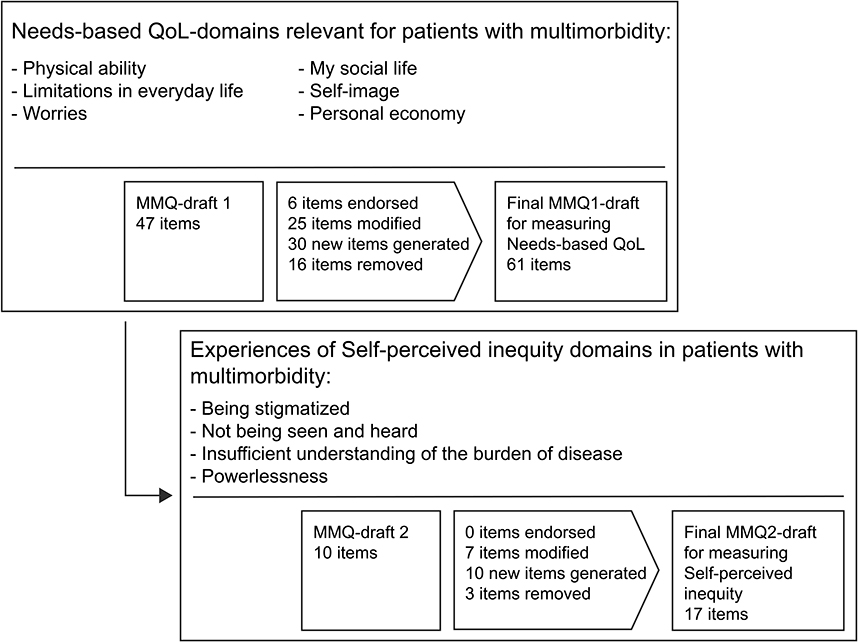 |
Figure 1 The process of generating items for the MultiMorbidity Questionnaire (MMQ1 and MMQ2) through qualitative interviews. |
Domains and Items Related to Needs-Based Quality of Life (MMQ1)
Six items from the first MMQ draft were directly endorsed in the final MMQ draft, 25 items were endorsed after modification, 30 items were developed from the informants’ verbatim comments, and 16 items were found irrelevant and therefore removed (Supplementary File 2). Four of the six existing items that were found relevant and endorsed directly in their original form had content inspired by the Danish version of a pre-existing PROM for measuring QoL in patients with COPD (LCOPD).35 The remaining two directly endorsed were generated from a qualitative project concerning patients with multimorbidity and poor self-care.38 In the 25 modified items, phrases and/or words were changed to improve understandability or relevance for the informants. Table 3 gives an example of how an item was modified through cognitive interviewing in subsequent rounds of interviews.
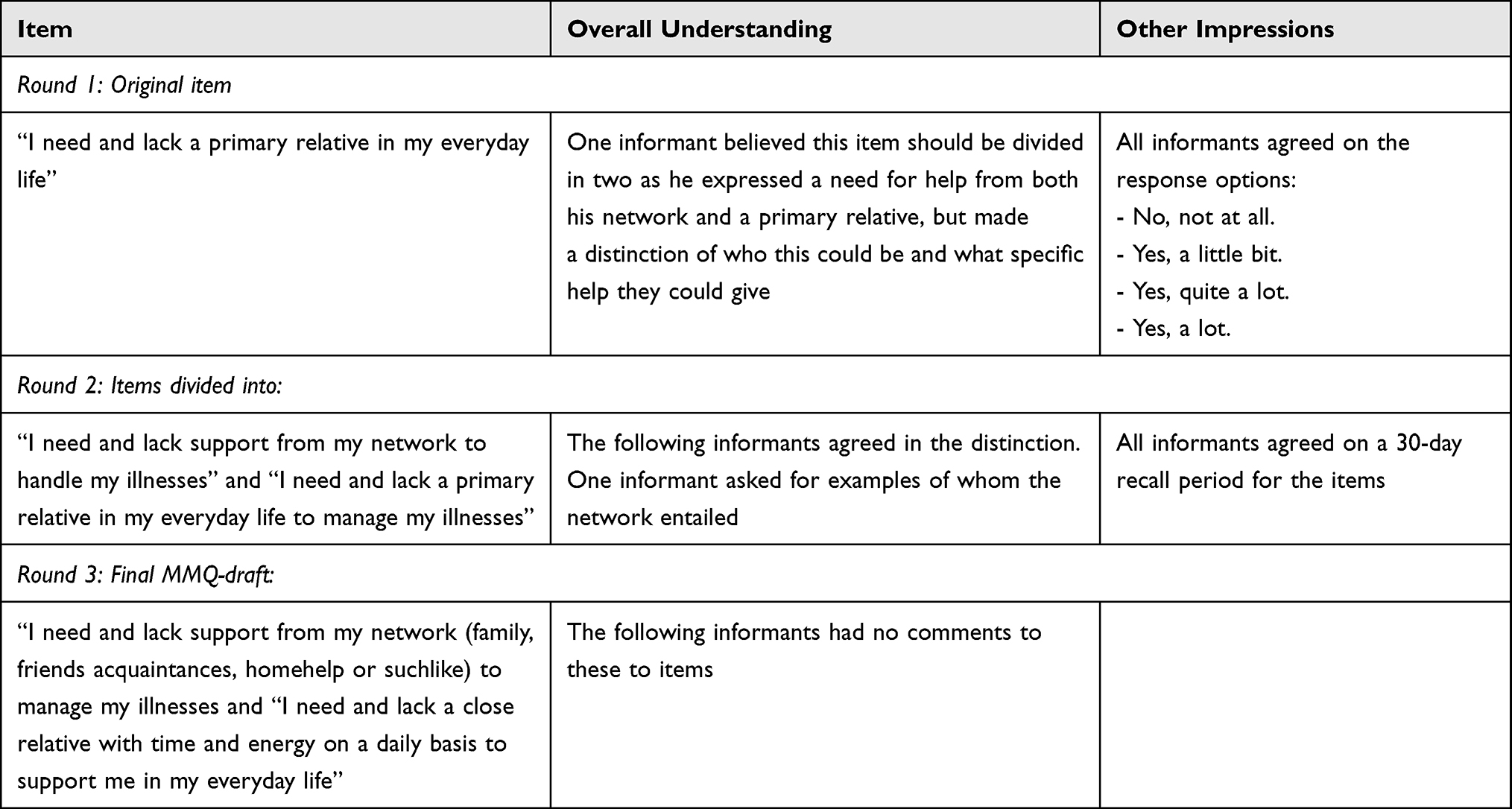 |
Table 3 Example of the Informants’ Modifications Regarding Need-Based QoL |
Through the think-aloud test, the informants stressed that items with content related to mental development (eg, My illnesses hinder me in reaching my full potential) were abstract and irrelevant, and the associated items were therefore removed from the MMQ draft.
In later interviews, the items were tested in reverse, which meant that informants were encouraged to express whether the overall content of items within each domain was relevant and covered a specific domain. During this phase, we found that none of the items in the first MMQ draft covered the predefined domain “Personal finances.” Therefore, four items were generated from the informants’ verbatim comments. Moreover, in this phase, the informants expressed a preference for the wordings of three of the predefined domains being changed to a more negative or neutral expression to cover the actual item content for each domain; “Self-determination” became “Limitations in everyday life”, “Security” became “Worries” and “Partner and social life” became “My social life”.
The final MMQ1 draft for measuring Needs-based QoL in patients with multimorbidity consisted of 61 items related to the domains: “Physical ability” (10 items), “Limitations in everyday life” (15 items), “Worries” (11 items), “My social life” (11 items), “Self-image” (12 items), and “Personal finances” (2 items) (Supplementary File 4 and Table 4).
 |
Table 4 Overall Descriptions of Items Within Each Needs-Based QoL Domain for Patients Living with Multimorbidity* |
Domains and Items Related to Self-Perceived Health Inequity (MMQ2)
The preliminary domains and items regarding Self-perceived health inequity were not only tested in the qualitative interviews but facilitated fruitful conversations concerning the informants’ experiences of this feeling, indicating the relevance of the framework. In particular, numerous stories emerged from testing the constructed items, where the essence was the informants’ perception of not being seen and heard in encounters with health-care professionals and local authorities. This was connected to what some informants described as a feeling of not being understood in their daily struggles related to their illnesses. Others expressed a feeling of powerlessness due to their illnesses; one informant described this as feeling like an “insignificant piece of a jigsaw” when in contact with local authorities. In many cases, especially for patients with a psychiatric disease or conditions generally known to be associated with lifestyle such as COPD or early onset of or ill-regulated diabetes type II, Self-perceived health inequity was unfolded as a feeling of being labelled by people around them because of their illnesses. From the informants’ stories and statements grew new items that were analysed to cover the following domains: “Experiences of being stigmatised”, “Experiences of not being seen and heard”, “Experiences of insufficient understanding of the burden of disease”, and “Experiences of feeling powerless.” Table 5 shows overall description of each domain.
 |
Table 5 Overall Descriptions of Self-Perceived Health Inequity Domains for Patients Living with Multimorbidity |
None of the 10 items generated for testing Self-perceived health inequity as an important aspect of QoL for patients with multimorbidity were endorsed directly in their original form. As a result, seven items were modified and endorsed, and 10 new items were developed. Three items were removed; two because the wording inferior patient was unclear to the informants and one because the term social position was interpreted differently and therefore elaborated in another item concerning the employment situation (Supplementary File 3). Table 6 shows how an item was modified by the informants through cognitive interviewing in three subsequent interviews, to obtain content relevance and understandability.
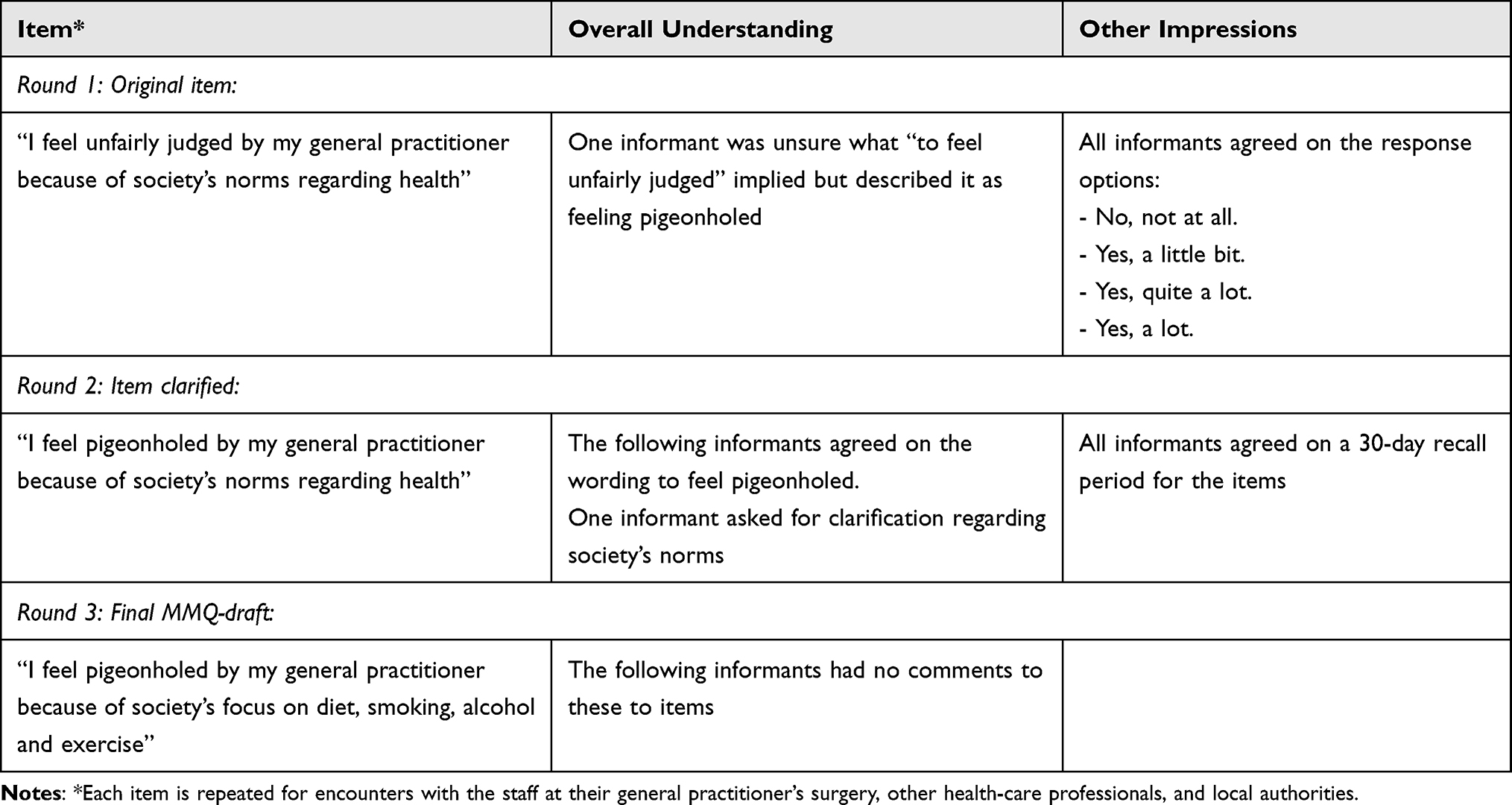 |
Table 6 Example of the Informants’ Item Modification Regarding Self-Perceived Health Inequity |
The process of generating and modifying experiences of Self-perceived health inequity into items showed the content was relevant not only in encounters with health-care professionals but in all the informants’ contacts. Therefore, the items in MMQ2 were repeated for encounters with (i) their general practitioners, (ii) staff at their general practitioner’s surgery, (iii) other health-care professionals, (iv) local authority employees, and (v) family, friends, and others. Not all items were repeated for each encounter as some had specific content that was not relevant, for example, “I feel my general practitioner treats me worse than other patients.” Each item was modified in collaboration with the informants, so content and wording were to the point for a specific encounter.
The final MMQ2 draft for measuring Self-perceived health inequity when living with multimorbidity consisted of a total of 17 items covering the domains “Experiences of being stigmatised” (5 items), “Experiences of not being seen and heard” (4 items), “Insufficient understanding of the burden of disease” (3 items) and “Experiences of feeling powerless” (5 items). These 17 items are relevant for encounters with the general practitioner, other health-care professionals, and local authority employees, whereas 12 are evident for encounters with the staff at their general practitioner’s surgery and seven items in contact with family, friends, and others. In total, this adds up to 70 items in MMQ2 if all professions and relatives are included (Supplementary File 5).
Thus, the final MMQ draft consists of 78 items, divided into MMQ1 for measuring Needs-based QoL (61 items) and MMQ2 for measuring Self-perceived health inequity (17 items).
Discussion
Testing the MMQ draft for its content validity through interviews with patients with multimorbidity elicited that the Needs-based QoL framework had to be supplemented with theory on Self-perceived health inequity to encompass this patient group’s experiences. Confronting the informants with the first MMQ draft consisting of 47 items from our item bank led to an iterative process of endorsing, modifying, removing, and developing new items. Aspects of QoL not covered by the framework of the Needs-based approach emerged, and Self-perceived health inequity was tested as a supplementary framework. This resonated among the informants and thereby led to the generation of new items and resulted in Self-perceived health inequity becoming a coherent but independent part of MMQ; MMQ1 for measuring Needs-based QoL and MMQ2 for measuring Self-perceived health inequity.
The informants’ descriptions of feeling labelled and inferior, especially in encounters with municipalities’ unemployment services in this study, are also seen in Jønsson’s study of patients with multimorbidity where they describe how they often face being subject to discrimination and stigma.49 Frequently this was manifested as self-perceived experiences of being stigmatised and discriminated against due to low socio-economic status, showing how socio-economic determinants are juxtaposed with negative stereotypes and thus may lead to Self-perceived health inequity.49,59 For the individual, this implies reactions to how you feel you are perceived in health-care encounters, which “may lead to a particular agency, which, ironically, may eventually lead to poorer treatment outcomes.”49 Stigma is a well-known barrier to health and is a fundamental cause of health inequality, and it is therefore essential to target in interventions.53,60 Stangl et al have proposed The Health Stigma and Discrimination Framework that describes the stigmatisation process as it unfolds regarding health. The model moves beyond disease silos as Stangl et al believe health interventions should target peoples’ complex realities to positively affect health and well-being.53 The health stigmatisation process is broken down into constituent domains leading to “health and social impacts”; this implies “drivers and facilitators”, “stigma marking”, “stigma experiences and stigma practices”, and “affected populations and institutions.”53 We see from our study how informants feel they are perceived by people around them because of their multimorbidity as examples of stigma experiences. In this context, the GP, staff at the GP’s surgery, other health-care professionals, local authorities, and family, friends, and others play a role as drivers and facilitators of health-related stigma. This becomes apparent through cultural norms or even social judgment, prejudice, and blame, potentially influencing the individual’s QoL, which is very difficult to address in interventions.53 Stangl et al stress the importance of researchers to “test interventions that more appropriately address the lived realities of vulnerable populations accessing healthcare systems.”53 Our future aim is to show that MMQ will contribute to demonstrating the complexities of patients with multimorbidity by making possible the measurement of Needs-based QoL and Self-perceived health inequity required for demonstrating the possible effects of such interventions.
The final MMQ draft contains domains and items not covered by the most widely used measures in intervention studies for patients with multimorbidity, EQ-5D and SF-36.61–63 This indicates that current measures have low content validity for this specific group of patients and raise questions about the validity of the results in studies including patients with multimorbidity. Comparing the content of EQ-5D and SF-36 with the final MMQ draft (Supplementary File 4), they vary in their focus on physical activity and role functioning. The measurement of Need-based QoL broadens this focus by including aspects such as personal finances and self-image. Furthermore, measuring Self-perceived health inequity includes other aspects of QoL when living with multimorbidity; experiences of feeling stigmatised, powerless, not seen and heard, and an insufficient understanding of the burden of disease, which are not revealed through using EQ-5D and SF-36.
Implications for Research and Policy
The third and final step of the MMQ development is to test the MMQ draft statistically using Modern Test Theory. Hereby we will assess the dimensionality of the domains, test for invariant measurement, and remove items that do not possess adequate psychometric properties. This will ensure a final PROM with adequate measurement properties that can be used for example in prospective longitudinal observation and intervention studies for patients with multimorbidity. The purpose of MMQ is to measure Needs-based QoL and Self-perceived inequity on a population level, enabling adequate assessments of effects of eg, a new intervention. This may potentially have an impact on policy and guidelines for treatment regarding patients living with multimorbidity.
Strengths and Limitations
The primary strength of this study is the thorough item testing and item generation phase using qualitative methods in conversations with informants based on a conceptual model.23 Using the MMQ draft as an interview guide by presenting pre-existing items or items formulated by other informants was a fruitful way of getting the informants to discuss freely personal issues that might not have been touched upon otherwise. For informants, it legitimised touching on topics such as sex, personal finances, and frustrations towards family and friends; topics we have experienced from previous qualitative studies demanded several interviews with the same informant. Yet, alternating between an explorative interview phase with the individual informant as the subject and a cognitive interview phase with the MMQ as the subject deviates from COSMINS Risk of Bias Checklist. Structuring the interviews strictly between the two phases, using different informants might have provided other results.
Another vital strength of this study is the multidisciplinary author group, combining knowledge of the patient group from a clinical perspective and extensive qualitative experience and anthropological fieldwork. A limitation is that we did not test the face validity of the items among experts not part of the research group. Yet, we prioritised content validity through patients with multimorbidity being experts on aspects related to their QoL.
The unavoidable heterogeneity of patients with multimorbidity and relatively small sample size demand a well-considered stratification of informants. Data with high information power was ensured by the process of purposive sampling.27,32 We argue that it is possible to generalise our analyses of our data based on the frameworks of the Needs-based approach and Self-perceived health inequity in other contexts backed up by the transparency/audibility of all phases in the MMQ development.64 Additionally, we have considered the heterogeneity of multimorbidity in our approach to item inclusion, as we were reluctant to remove items at this phase; items were included if relevant right down to one informant, resulting in a large number of items included in the final drafts of the MMQ1 and MMQ2. Furthermore, we continued the modification of the MMQ1 and MMQ2 until no new domains or items emerged.
It can be seen both as a strength and a weakness that the author group are both the developers of the MMQ and the interviewers in the item generation phase. It gave us exhaustive knowledge of every domain and item followed through all processes. Conversely, it could be seen as a potential bias that might have encouraged the patients to be overly positive towards the MMQ draft and introduction of the Self-perceived health inequity items. As interviewers, we were aware of the need to invite patients to be critical. The few items with original content endorsed in the final MMQ draft indicate that the informants shared their possible points of criticism. Furthermore, we believe that the first author being a medical doctor has had an inevitable influence on the data obtained. The informants were assured that the conversation was confidential and that issues brought up in the interview would not be discussed with their GP. At the end of each interview, all the informants were asked whether the interviewer being a medical doctor had an impact on the interview situation. None of them expressed that they would have answered differently to an interviewer with a different profession. Obviously, we cannot say if this would have played out differently, but most of the informants had not realised that the interviewer was a medical doctor and saw her as a representative from the University.
Conclusion
We have developed the MMQ, a multimorbidity-specific questionnaire to measure Needs-based QoL (MMQ1) and Self-perceived health inequity (MMQ2) with high content validity. MMQ1 encompasses the domains: “Physical ability” (10 items), “Limitations in everyday life” (15 items), “Worries” (11 items), “My social life” (11 items), “Self-image” (12 items), and “Personal finances” (2 items). Self-perceived health inequity proved to be a relevant framework for other aspects of QoL not covered by the Needs-based approach to QoL. MMQ2 covers the domains: “Experiences of being stigmatised” (five items), “Experiences of not being seen and heard” (four items), “Insufficient understanding of the burden of disease” (three items), and “Experiences of feeling powerless” (five items).
Abbreviations
COSMIN, COnsensus-based Standards for the selection of health status Measurement INstruments; COPD, Chronic obstructive pulmonary disease; MMQ, Multimorbidity Questionnaire; PROM, patient-reported Outcome Measure; QoL, Quality of Life.
Data Sharing Statement
The dataset, consisting of Danish transcriptions, generated during the current study is not publicly available due to protection of informants’ anonymity and European General Data Protection Regulation (GDPR) law. Data are available in anonymised form upon reasonable request to the first author. All data were analysed using NVivo12.
Ethics Approval and Consent to Participate
Approval of processing of personal data in the study has been given by the University of Copenhagen (Ref.no.: 514-0410/19-3000). This study did not require approval from the Danish Data Protection Agency, Research Ethics Committee, or the National Committee on Health Research. The general rules of research conduct, outlined by the Helsinki Declaration in its latest form, have been followed throughout all processes in this study. All informants were given information about the study before their participation and gave written consent to participate, including informed consent for publication of anonymized responses before the interviews. Informants are anonymised, and all data has been managed according to the European General Data Protection Regulation (GDPR) law.
Consent for Publication
Not applicable. Informants are anonymised, and all data has been managed according to European GDPR law.
Acknowledgments
The authors sincerely thank the participating informants who took part in this study and lead the direction of conducting the MultiMorbidity Questionnaire. We would also like to thank the general practitioners in Region Zealand and The Capital Region who helped to recruit our informants. Lastly, we would also like to thank Susanne Reventlow for inspiration and counselling.
Funding
This study was funded by Region Zealand, Denmark, and Fonden for Almen Praksis (General Practice Foundation, Denmark) (Grant numbers: A1849, A2013, A2662, A3550) and the Novo Nordisk Foundation (Grant number: NNF15OC0019568). Funders have no direct or indirect financial relationship with the authors and no rule or authority in decision about design, collection, management, analysis, interpretation of data, writing of the report or decision about publication.
Disclosure
The authors declare that they have no financial or non-financial competing interests in this work.
References
1. Willadsen TG, Siersma V, Nicolaisdóttir DR, et al. Multimorbidity and mortality: a 15-year longitudinal registry-based nationwide Danish population study. J Comorbidity. 2018;8(1):2235042X18804063. doi:10.1177/2235042X18804063
2. Uijen AA, van de Lisdonk EH. Multimorbidity in primary care: prevalence and trend over the last 20 years. Eur J Gen Pract. 2008;14:28–32. doi:10.1080/13814780802436093
3. Van Den Akker M, Buntinx F, Knottnerus JA. Comorbidity or multimorbidity. Eur J Gen Pract. 1996;2(2):65–70. doi:10.3109/13814789609162146
4. Glynn LG, Valderas JM, Healy P, et al. The prevalence of multimorbidity in primary care and its effect on health care utilization and cost. Fam Pract. 2011;28(5):516–523. doi:10.1093/fampra/cmr013
5. Fortin M, Bravo G, Hudon C, et al. Relationship Between Multimorbidity and Health-Related Quality of Life of Patients in Primary Care. Qual Life Res. 2006;15(1):83–91. doi:10.1007/s11136-005-8661-z
6. Fortin M, Lapointe L, Hudon C, Vanasse A, Ntetu AL, Maltais D. Multimorbidity and quality of life in primary care: a systematic review. Health Qual Life Outcomes. 2004;2:51. doi:10.1186/1477-7525-2-51
7. Ørtenblad L, Meillier L, Jønsson AR. Multi-morbidity: a patient perspective on navigating the health care system and everyday life. Chronic Illn. 2018;14(4):271–282. doi:10.1177/1742395317731607
8. Tyack Z, Frakes KA, Barnett A, Cornwell P, Kuys S, McPhail S. Predictors of health-related quality of life in people with a complex chronic disease including multimorbidity: a longitudinal cohort study. Qual Life Res. 2016;25(10):2579–2592. doi:10.1007/s11136-016-1282-x
9. Bower P, Harkness E, MacDonald W, Coventry P, Bundy C, Moss-Morris R. Illness representations in patients with multimorbid long-term conditions: qualitative study. Psychol Health. 2012;27:1211–1226. doi:10.1080/08870446.2012.662973
10. Rosbach M, Andersen JS. Patient-experienced burden of treatment in patients with multimorbidity – a systematic review of qualitative data. PLoS One. 2017;12. doi:10.1371/journal.pone.0179916
11. Shippee ND, Shah ND, May CR, Mair FS, Montori VM. Cumulative complexity: a functional, patient-centered model of patient complexity can improve research and practice. J Clin Epidemiol. 2012;65(10):1041–1051. doi:10.1016/j.jclinepi.2012.05.005
12. Marmot MG, Stansfeld S, Patel C, et al. Health inequalities among British civil servants: the Whitehall II study. Lancet. 1991;337(8754):1387–1393. doi:10.1016/0140-6736(91)93068-K
13. Jønsson A, Spaletta O. Tuning the self: revisiting health inequities through the lens of social interaction. Accepted for publication in Ethos; 2023.
14. Smith SM, Wallace E, O’Dowd T, Fortin M. Interventions for improving outcomes in patients with multimorbidity in primary care and community settings. Cochrane Database Syst Rev. 2021;2021(1). doi:10.1002/14651858.CD006560.pub4
15. Møller A, Bissenbakker KH, Arreskov AB, Brodersen J. Specific measures of quality of life in patients with multimorbidity in primary healthcare: a systematic review on patient-reported outcome measures’ adequacy of measurement. Patient Relat Outcome Meas. 2020;11:1–10. doi:10.2147/prom.s226576
16. Smith SM, Soubhi H, Fortin M, Hudon C, O’Dowd T. Managing patients with multimorbidity: systematic review of interventions in primary care and community settings. BMJ. 2012;345(7874):e5205–e5205. doi:10.1136/bmj.e5205
17. Hunt SM, McKenna SP. The QLDS: a scale for the measurement of quality of life in depression. Health Policy. 1992;22(3):307–319. doi:10.1016/0168-8510(92)90004-U
18. McKenna SP, Doward LC. The needs-based approach to quality of life assessment. Value Heal. 2004;7:S1–S3. doi:10.1111/J.1524-4733.2004.7S101.X
19. Brodersen J, Doward LC, Thorsen H, Mckenna SP. Writing Health-Related Items for Rasch Models - Patient-Reported Outcome Scales for Health Sciences: from Medical Paternalism to Patient Autonomy. In: Rasch Models in Health. John Wiley & Sons, Inc.; 2013:281–302. doi:10.1002/9781118574454.ch15
20. Doward LC, McKenna SP, Meads DM. Effectiveness of needs-based quality of life instruments. Value Health. 2004;7(1):S35–8. doi:10.1111/j.1524-4733.2004.7s109.x
21. Comins JD, Brodersen J, Siersma V, Jensen J, Hansen CF, Krogsgaard MR. How to develop a condition-specific PROM. Scand J Med Sci Sports. 2021;31(6):1216–1224. doi:10.1111/SMS.13868
22. Terwee CB, Prinsen CAC, Chiarotto A, et al. COSMIN methodology for evaluating the content validity of patient- reported outcome measures: a Delphi study. Qual Life Res. 2018;1(27):1159–1170. doi:10.1007/s11136-018-1829-0
23. Bissenbakker K, Møller A, Brodersen JB, Jønsson ABR. Conceptualisation of a measurement framework for Needs-based Quality of Life among patients with multimorbidity. J Patient Rep Outcom. 2022;6:83. doi:10.1186/s41687-022-00489-0
24. Prinsen CAC, Mokkink LB, Bouter LM, et al. COSMIN guideline for systematic reviews of patient-reported outcome measures. Qual Life Res. 2018;27(5):1147–1157. doi:10.1007/s11136-018-1798-3
25. Streiner D, Norman G. Health Measurement Scales: A Practical Guide to Their Development and Use. Oxford University Press; 2008.
26. Frost MH, Reeve BB, Liepa AM, Stauffer JW, Hays RD, Sloan JA. What is sufficient evidence for the reliability and validity of patient-reported outcome measures? Value Heal. 2007;10(2). doi:10.1111/J.1524-4733.2007.00272.X
27. Farrugia B. WASP (Write a Scientific Paper): sampling in qualitative research. Early Hum Dev. 2019;133:69–71. doi:10.1016/J.EARLHUMDEV.2019.03.016
28. Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet. 2012;380(9836):37–43. doi:10.1016/S0140-6736(12)60240-2
29. Pathirana TI, Jackson CA. Socioeconomic status and multimorbidity: a systematic review and meta-analysis. Aust N Z J Public Health. 2018;42(2):186–194. doi:10.1111/1753-6405.12762
30. Mujica-Mota RE, Roberts M, Abel G, et al. Common patterns of morbidity and multi-morbidity and their impact on health-related quality of life: evidence from a national survey. Qual Life Res. 2015;24(4):909–918. doi:10.1007/S11136-014-0820-7/FIGURES/4
31. Bissenbakker KH, Jønsson AR, Brodersen J, Møller A. PROMs og livskvalitet. Tidsskr Forsk i Sygd og Samf. 2020;17(32):55–74. doi:10.7146/tfss.v17i32.120975
32. Malterud K, Siersma V, Guassora A. Information power - Sample content and size in qualitative studies. In: Camic P, editor. Qualitative Research in Psychology Expanding Perspectives in Methodology and Design. American Psychological Association; 2021:67–81.
33. McKenna SP, Doughty N, Meads DM, Doward LC, Pepke-Zaba J. The Cambridge Pulmonary Hypertension Outcome Review (CAMPHOR): a measure of health-related quality of life and quality of life for patients with pulmonary hypertension. Qual Life Res. 2006;15(1):103–115. doi:10.1007/S11136-005-3513-4
34. Meads DM, McKenna SP, Doward LC, et al. Development and validation of the Asthma Life Impact Scale (ALIS). Respir Med. 2010;104(5):633–643. doi:10.1016/J.RMED.2009.11.023
35. McKenna SP, Meads DM, Doward LC, et al. Development and validation of the living with chronic obstructive pulmonary disease questionnaire. Qual Life Res. 2011;20(7):1043–1052. doi:10.1007/S11136-011-9850-6
36. Mosier CI. A critical examination of the concepts of face validity. Educ Psychol Meas. 1947;7(2):191–205. doi:10.1177/001316444700700201
37. Comins JD, Krogsgaard MR, Brodersen J. Ensuring face validity in patient-related outcome scores — a matter of content. Knee. 2013;20:72–78. doi:10.1016/j.knee.2012.10.005
38. Kristensen MAT, Guassora AD, Arreskov AB, Waldorff FB, Hølge-Hazelton B. ‘I’ve put diabetes completely on the shelf till the mental stuff is in place’. How patients with doctor-assessed impaired self-care perceive disease, self-care, and support from general practitioners. A qualitative study. Scand J Prim Health Care. 2018;36(3):342–351. doi:10.1080/02813432.2018.1487436
39. Collins D. Pretesting survey instruments: an overview of cognitive methods. Qual Life Res. 2003;12(3):229–238. doi:10.1023/A:1023254226592
40. Willis G, Reeve BB, Barofsky I. The use of cognitive interviewing techniques in quality-of-life and patient-reported outcomes assessment. In: Outcome Assessment in Cancer: Measures, Methods and Application. Cambridge University Press; 2005:610–623. doi:10.1017/CBO9780511545856.031
41. Willis GB. Cognitive Interviewing: A Tool for Improving Questionnaire Design. Thousand Oaks: Sage Publications; 2005.
42. Finch J. The Vignette Technique in Survey Research. Sociology. 1987;21(1):105–114. doi:10.1177/0038038587021001008
43. Hughes R. Considering the vignette technique and its application to a study of drug injecting and HIV risk and safer behaviour. Sociol Heal Illn. 1998;20(3):381–400. doi:10.1111/1467-9566.00107
44. Goffman E. Stigma: notes on the Management of Spoiled Identity. Jason Aronson. 1974. doi:10.2307/2575995
45. Yates-Doerr E. Reworking the social determinants of health: responding to material-semiotic indeterminacy in public health interventions. Med Anthropol Q. 2020;34(3):378–397. doi:10.1111/MAQ.12586
46. Pedersen A, Haslund-Thomsen H, Curtis T, Grønkjær M. Talk to me, not at me: an ethnographic study on health-related help-seeking behavior among socially marginalized Danish men. Qual Health Res. 2020;30(4):598–609. doi:10.1177/1049732319868966
47. Merrild CH, Vedsted P, Andersen RS. Situating social differences in health and illness practices. Perspect Biol Med. 2017;59(4):547–561. doi:10.1353/PBM.2016.0047
48. Horton S, Barker JC. Stigmatized biologies: examining the cumulative effects of oral health disparities for Mexican American farmworker children. Med Anthropol Q. 2010;24(2):199–219. doi:10.1111/J.1548-1387.2010.01097.X
49. Jønsson ABR. Subjektiv ulighed: oplevelsen af ulighed i sundhed. Tidsskr Forsk i Sygd og Samf. 2021;18(35):95–114. doi:10.7146/tfss.v18i35.129995
50. Steno AM, Jønsson ABR. Spaces out of reach? Service user involvement in residents’ meetings at recovery-oriented social housing facilities for young people with mental health disorders. Heal. 2022;136345932210759. doi:10.1177/13634593221075950
51. Ryborg Jønsson A B, Emilie Christensen I, Reventlow S, Bech Risør M. Responsibilities of risk: living with mental illness during COVID-19. Med Anthropol. 2022;41(3):302–314. doi:10.1080/01459740.2022.2045288
52. Jønsson ABR. Aging with multimorbidity. illness and inequity in everyday live; 2018.
53. Stangl AL, Earnshaw VA, Logie CH, et al. The health stigma and discrimination framework: a global, crosscutting framework to inform research, intervention development, and policy on health-related stigmas. BMC Med. 2019;17(1):1–13. doi:10.1186/S12916-019-1271-3/TABLES/1
54. Ziebland S. Narrative interviewing. Underst Using Heal Exp. 2013;38–48. doi:10.1093/acprof:oso/9780199665372.003.0005
55. Brodersen J, Doward L, Thorsen H, McKenna S. Writing Health-Related Items for Rasch Models - Patient Reported Outcome Scales for Health Sciences. In: Rasch Models in Health. ISTE; 2013:281–302. doi:10.1002/9781118574454.ch15
56. McKenna SP, Doward LC, Niero M, Erdman R. Development of needs-based quality of life instruments. Value Heal. 2004;7(1):17–21. doi:10.1111/j.1524-4733.2004.7s105.x
57. Braun V, Clarke V. Reflecting on reflexive thematic analysis. Qual Res Sport Exerc Heal. 2019;11(4):589–597. doi:10.1080/2159676X.2019.1628806
58. Braun V, Victoria C. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(3):77–101. doi:10.1191/1478088706qp063oa
59. Jønsson AR. DE USUNDE: sundhedsantropologens møde med multisyge ældre på Lolland. Tidsskr Antropol. 2018;2018(77). doi:10.7146/ta.v2018i77.115392
60. Hatzenbuehler ML, Phelan JC, Link BG. Stigma as a fundamental cause of population health inequalities. Am J Public Health. 2013;103(5):813. doi:10.2105/AJPH.2012.301069
61. Makovski TT, Schmitz S, Zeegers MP, Stranges S, van den Akker M. Multimorbidity and quality of life: systematic literature review and meta-analysis. Ageing Res Rev. 2019;53:100903. doi:10.1016/j.arr.2019.04.005
62. EuroQoL. EuroQoL; 1990. Available from: https://euroqol.org/.
63. RAND Health. 36-Item short form survey; 1992. Available from: https://www.rand.org/health/surveys_tools/mos/36-item-short-form.html.
64. Shek DTL, Tang VMY, Han XY. Evaluation of evaluation studies using qualitative research methods in the social work literature (1990–2003): evidence that constitutes a wake-up call. Res Soc Work Pract. 2005;15(3):180–194. doi:10.1177/1049731504271603
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.