Back to Journals » Cancer Management and Research » Volume 18

Gemcitabine-Based versus Fluoropyrimidine-Based Chemotherapy and Role of Platinum Combination for First-Line Palliative Systemic Treatment in Advanced Ampullary Adenocarcinoma
Authors Wonglhow J ![]() , Wetwittayakhlang P, Sunpaweravong P, Sathitruangsak C, Dechaphunkul A
, Wetwittayakhlang P, Sunpaweravong P, Sathitruangsak C, Dechaphunkul A
Received 10 March 2026
Accepted for publication 27 May 2026
Published 4 June 2026 Volume 2026:18 608153
DOI https://doi.org/10.2147/CMAR.S608153
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Seema Singh
Jirapat Wonglhow,1 Panu Wetwittayakhlang,2 Patrapim Sunpaweravong,1 Chirawadee Sathitruangsak,1 Arunee Dechaphunkul1
1Division of Medical Oncology, Department of Internal Medicine, Faculty of Medicine, Prince of Songkla University, Songkhla, Thailand; 2Division of Gastroenterology and Hepatology, Department of Internal Medicine, Faculty of Medicine, Prince of Songkla University, Songkhla, Thailand
Correspondence: Arunee Dechaphunkul, Division of Medical Oncology, Department of Internal Medicine, Faculty of Medicine, Prince of Songkla University, Songkhla, Thailand, Email [email protected]
Purpose: Ampullary adenocarcinoma is a rare malignancy with limited evidence on the efficacy of systemic chemotherapy for advanced disease. This study aimed to evaluate the treatment outcomes of gemcitabine- and fluoropyrimidine-based regimens and the benefits of platinum combination therapy.
Patients and Methods: This retrospective study reviewed the data of patients with advanced ampullary adenocarcinoma treated at a university hospital in Southern Thailand between 2005 and 2024.
Results: Among the 97 patients, 71 (73.2%) received palliative chemotherapy, including 43 (60.6%) receiving gemcitabine-based regimens and 28 (39.4%) receiving fluoropyrimidine-based regimens. Median overall survival (OS) and progression-free survival (PFS) for gemcitabine-based vs. fluoropyrimidine-based regimens were 14.4 vs. 11.5 months (adjusted hazard ratio [HR] 0.85; 95% CI 0.34– 2.13; P = 0.725) and 8.67 vs. 7.18 months (adjusted HR 0.60; 95% CI 0.26– 1.36; P = 0.219), respectively. No significant difference in OS or PFS was observed between platinum combination and single-agent chemotherapy. The objective response rate (ORR) was 9.3% for gemcitabine-based therapy, 14.3% for fluoropyrimidine-based therapy, and 26.9% for platinum combination therapy, compared to 2.2% for monotherapy.
Conclusion: Gemcitabine- and fluoropyrimidine-based regimens demonstrated comparable survival outcomes. Platinum-combination chemotherapy was associated with a higher ORR, but no significant OS or PFS benefit was observed. Therefore, platinum-combination regimens may be considered in selected patients requiring tumor shrinkage, and these findings should be interpreted as hypothesis-generating real-world evidence.
Keywords: ampullary adenocarcinoma, chemotherapy, survival, fluoropyrimidine, gemcitabine, platinum
Introduction
Ampullary adenocarcinoma is a rare malignancy accounting for less than 1% of all gastrointestinal cancers.1 It arises from the ampulla of Vater, a unique anatomical region in which the common bile duct and pancreatic duct merge before emptying into the duodenum.2 The incidence of this cancer is estimated to be less than one case per 100,000 individuals.1,3,4 Epidemiological studies have suggested variations in prevalence among different ethnic groups, with higher incidence rates observed in the Hispanic and Asian-Pacific Islander populations.3
Although pancreatoduodenectomy remains the standard curative option for localized disease,5,6 nearly half of the patients are ineligible for surgery because of advanced-stage disease or underlying comorbidities.5,7,8 Historically, ampullary adenocarcinoma has been grouped with other periampullary malignancies in clinical trials, leading to a lack of disease-specific data.9–11 To date, no randomized controlled trials have focused exclusively on advanced ampullary cancer.
The ampulla of Vater is composed of distinct epithelial origins, including intestinal, pancreatic, and biliary components, which contribute to the heterogeneity of ampullary adenocarcinomas.5 These tumors are typically classified into intestinal, pancreatobiliary, or mixed histological subtypes.5,9,12,13 Due to this complexity, the optimal systemic chemotherapy regimen for advanced ampullary adenocarcinoma remains uncertain. Most treatment strategies are largely extrapolated from those used for pancreatic, biliary tract, and colorectal cancers.9,12,14 Consequently, systemic chemotherapy selection is often guided by these distinct lineages, with fluoropyrimidine-based regimens typically preferred for the intestinal subtype and gemcitabine-based regimens for the pancreatobiliary subtype. However, no established criteria exist to determine the most effective regimen, and no specific histological subtype has been definitively linked to prognosis or treatment response in a metastatic setting.15–17
Palliative chemotherapy remains the primary treatment approach.18 However, whether fluoropyrimidine- or gemcitabine-based regimens provide superior outcomes remains unclear. Although the ABC-02 trial demonstrated an overall survival benefit of cisplatin plus gemcitabine over gemcitabine alone in advanced biliary tract cancers, this benefit was not evident in a small subgroup of patients with ampullary cancer.10 While platinum-combination regimens are commonly used in pancreaticobiliary and gastrointestinal malignancies to improve tumor response, their role in advanced ampullary adenocarcinoma has not been well established.
Given the rarity of ampullary adenocarcinoma, conducting prospective clinical trials remains challenging. Therefore, retrospective studies with larger patient cohorts are important for understanding real-world treatment patterns and generating future research hypotheses. Accordingly, this study aimed to assess the real-world effectiveness of first-line palliative chemotherapy with fluoropyrimidine-based versus gemcitabine-based regimens and to explore the potential role of platinum-combination therapy in patients with advanced ampullary adenocarcinoma.
Materials and Methods
Study Participants
This retrospective study reviewed the medical records of patients diagnosed with advanced-stage ampullary adenocarcinoma between January 2005 and October 2024 at Songklanagarind Hospital. The inclusion criteria were as follows: 1) patients with pathologically confirmed adenocarcinoma of the ampulla of Vater; 2) patients with metastatic disease; 3) patients aged 18 years or older; and 4) patients receiving first-line palliative chemotherapy, including fluoropyrimidine-based or gemcitabine-based regimens or best supportive care (BSC). The exclusion criteria were as follows: 1) concomitant malignancies and 2) patients who received any previous palliative chemotherapy with other regimens.
The baseline clinical characteristics included age, sex, Eastern Cooperative Oncology Group (ECOG) performance status (PS), body mass index (BMI), comorbidities, and baseline laboratory results. They were retrieved from the electronic medical records via the hospital information system at Songklanagarind Hospital. Disease characteristics, including TNM staging as defined by the 8th edition of the American Joint Committee on Cancer, number of organ metastases, tumor differentiation, tumor markers, and treatment information, including chemotherapy regimens and subsequent treatments, were also assessed.
This study was approved by the Ethics Committee of the Research Centre, Faculty of Medicine, Prince of Songkla University (REC.67547141). Due to the study’s retrospective design, the requirement for written informed consent was waived. All identified patient information was removed to maintain confidentiality and ensure patient safety.
Study Procedures
The fluoropyrimidine-based regimens included 5-fluorouracil (5-FU) monotherapy, capecitabine monotherapy, 5-FU plus folinic acid and oxaliplatin (FOLFOX), 5-FU plus cisplatin, and 5-FU plus carboplatin. Gemcitabine-based regimens included gemcitabine monotherapy, gemcitabine plus cisplatin, and gemcitabine plus carboplatin therapy. Each chemotherapy regimen was administered differently: 5-FU monotherapy was repeated every four weeks; capecitabine monotherapy, 5-FU plus cisplatin, and 5-FU plus carboplatin were repeated every three weeks; FOLFOX was repeated every two weeks; gemcitabine monotherapy was repeated every four weeks; and gemcitabine plus cisplatin and gemcitabine plus carboplatin were repeated every three weeks. Chemotherapy was continued for six cycles until disease progression, death, onset of intolerable side effects, or upon the patient’s indication of preference. The primary oncologists adjusted the chemotherapy dose based on the patient’s ECOG PS and baseline laboratory values.
If the first-line chemotherapy regimen was ineffective, subsequent therapeutic treatment was considered. The decision was made based on the patient’s performance status, personal preference, or the feasibility of using alternative agents.
Measurement
The primary objective was to compare the overall survival (OS) and progression-free survival (PFS) between fluoropyrimidine-based chemotherapy and gemcitabine-based chemotherapy. Secondary outcomes were OS and PFS between single-agent chemotherapy and platinum combination chemotherapy. Secondary outcomes included response rate and prognostic factors for OS. OS was defined as the time from the date of diagnosis of advanced-stage ampullary adenocarcinoma to death due to any cause. PFS was defined as the time from the date of diagnosis of advanced-stage ampullary adenocarcinoma until radiological tumor progression according to the Response Evaluation Criteria for Solid Tumors (RECIST) 1.1 criteria or death, whichever occurred first. The response rate was evaluated using RECIST 1.1 criteria. Chest and abdominal computed tomography (CT) was performed every 2–3 months to evaluate treatment responses. The response rates were calculated both in the overall population of patients who initiated first-line chemotherapy and in the subgroup of patients with evaluable radiological response data.
Statistical Analysis
Continuous variables are expressed as medians with interquartile ranges or mean with standard deviations for baseline characteristics, depending on the data distribution. Categorical variables were expressed as frequencies and percentages. Survival curves were generated using the Kaplan–Meier method and compared using the Log rank test. Prognostic factors were identified using univariate and multivariate Cox regression analyses. Variables included in multivariable Cox proportional hazards analyses were selected a priori based on clinical relevance, prior literature, and potential confounding effects on treatment selection and survival outcomes. To minimize model overfitting given the limited sample size, a parsimonious multivariable approach was applied. All statistical analyses were conducted using the R software version 4.3.1 (R Foundation, Vienna, Austria). Two-sided P-values were calculated, and P < 0.05 was considered statistically significant.
Results
Patient Characteristics
A total of 97 patients were included in this study, of whom 71 (73.2%) received first-line palliative chemotherapy and 26 (26.8%) received BSC. Among those who underwent chemotherapy, 28 patients (39.4%) received a fluoropyrimidine-based regimen, and 43 (60.6%) were treated with a gemcitabine-based regimen. The baseline characteristics of patients in the fluoropyrimidine-based, gemcitabine-based, and BSC groups are summarized in Table 1. Overall, the baseline characteristics were well balanced between patients receiving fluoropyrimidine-based and gemcitabine-based chemotherapy, except for BMI. When comparing the chemotherapy and BSC groups, patients in the BSC cohort had a significantly higher proportion of individuals with an ECOG PS of ≥2 and a greater number of patients with low BMI, compared to those receiving chemotherapy. Further details on the baseline characteristics of patients receiving single-agent chemotherapy versus platinum-combined chemotherapy are provided in Table S1, with no statistically significant differences observed between the two groups.
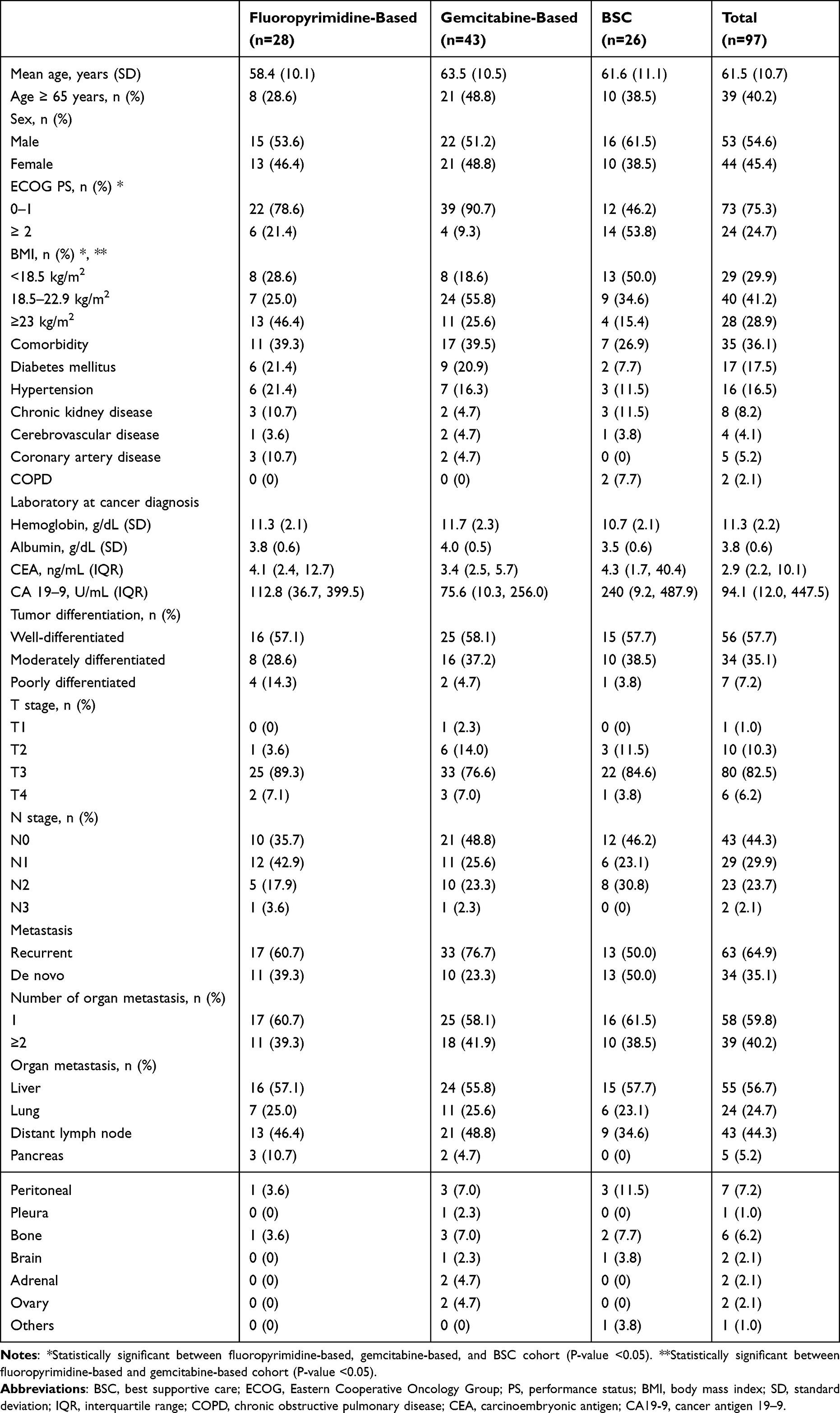 |
Table 1 Baseline Characteristics |
Treatment Information
Among the 28 patients who received a fluoropyrimidine-based regimen, 46.5% received single-agent chemotherapy, and 53.5% received platinum-based combination chemotherapy. In contrast, among those treated with a gemcitabine-based regimen, 74.4% received single-agent chemotherapy, and 25.6% received a platinum-combined regimen. Details of the treatment regimens and related information are provided in Table 2. No statistically significant differences were observed between fluoropyrimidine-based and gemcitabine-based treatments, or between single-agent and platinum-combined chemotherapy. The details of the subsequent treatments are presented in Table S2.
 |
Table 2 Treatment Information |
OS
The median follow-up time for the entire population was 9.79 months (interquartile range [IQR] 6.14–15.44 months). The median OS was 10.10 months (95% confidence interval [CI] 9.30–13.90). Patients who received palliative chemotherapy had significantly improved OS compared to those who received BSC, with a median OS of 13.37 months (95% CI 10.45–15.21) versus 6.37 months (95% CI 4.34–9.66; Hazard ratio [HR] 0.32; 95% CI 0.19–0.53; P < 0.001; Figure 1). Patients who had metastasectomy had a significantly improved median OS compared to those without metastasectomy (34.30 vs. 10.00 months; HR 0.29; 95% CI 0.09–0.96; P = 0.042; Figure S1).
 |
Figure 1 Median OS between patients who received palliative chemotherapy and best supportive care. |
OS Between Fluoropyrimidine- and Gemcitabine-Based Chemotherapy
Patients who received a gemcitabine-based regimen had a median OS of 14.4 months (95% CI 10.0–21.6), compared to 11.5 months (95% CI 8.2–15.0) for those who received a fluoropyrimidine-based regimen (HR 0.52; 95% CI 0.30–0.88; P = 0.015; Figure 2). However, after adjustment for clinically relevant prognostic factors, including ECOG performance status, BMI, CA 19–9 level, and metastatic type, multivariable Cox proportional hazards analysis demonstrated no statistically significant difference in OS between the two groups (adjusted HR 0.62, 95% CI 0.30–1.27; P = 0.191).
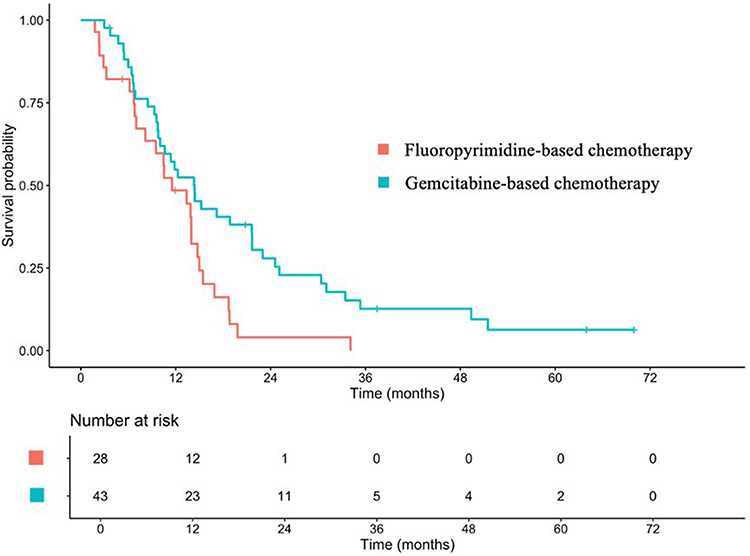 |
Figure 2 Median OS between patients who received fluoropyrimidine- and gemcitabine-based chemotherapy. |
OS Between Monotherapy and Platinum Combined Chemotherapy
Patients who received platinum-based combination chemotherapy had a median OS of 11.90 months (95% CI 10.45–18.70), compared to 14.30 months (95% CI 9.49–18.80) for those who received single-agent chemotherapy (HR 0.86; 95% CI 0.51–1.44; P = 0.562; Figure 3).
 |
Figure 3 Median OS between patients who received monotherapy chemotherapy and platinum combined chemotherapy. |
The median OS for patients who received gemcitabine monotherapy, gemcitabine combined with platinum, fluoropyrimidine monotherapy, and fluoropyrimidine combined with platinum was 13.3 months (95% CI 9.30–21.60), 18.0 months (95% CI 10.61–NA), 14.8 months (95% CI 8.15–NA), and 10.5 months (95% CI 6.80–14.00), respectively. The HR were as follows: gemcitabine combined with platinum vs. gemcitabine monotherapy (HR 0.49; 95% CI 0.19–1.01), fluoropyrimidine combined with platinum vs. fluoropyrimidine monotherapy (HR 1.27; 95% CI 0.58–2.80), gemcitabine monotherapy vs. fluoropyrimidine monotherapy (HR 0.71; 95% CI 0.35–1.46), and gemcitabine combined with platinum vs. fluoropyrimidine combined with platinum (HR 0.25; 95% CI 0.10–0.62).
PFS
PFS Between Fluoropyrimidine- and Gemcitabine-Based Chemotherapy
The median PFS for patients who received gemcitabine-based chemotherapy and fluoropyrimidine-based chemotherapy was 8.67 (95% CI 5.68–13.14) and 7.18 (95% CI 4.20–9.36) months, respectively (HR 0.51; 95% CI 0.30–0.85; P = 0.01; Figure S2). However, after adjustment for clinically relevant prognostic factors, including ECOG performance status, BMI, CA 19–9 level, and metastatic type, multivariable Cox proportional hazards analysis demonstrated no statistically significant difference in PFS between the two groups (adjusted HR 0.63, 95% CI 0.32–1.23; P = 0.175).
PFS Between Single-Agent and Platinum Combination Chemotherapy
Patients who received platinum-based combined chemotherapy had a median PFS of 8.15 months (95% CI 4.27–11.1), compared to 7.95 months (95% CI 5.49–10.3) for those who received only single-agent chemotherapy (HR 0.79; 95% CI 0.47–1.33; P = 0.380; Figure S3).
Response Rates
Among patients who received fluoropyrimidine- and gemcitabine-based regimens, 67.9% and 90.7% of them, respectively, were assessable, showing objective response rates (ORR) of 14.3% and 9.3%, respectively, with no significant difference (P = 0.381). The response rates are presented in Table 3. In contrast, patients who underwent platinum-based combination chemotherapy had an ORR of 26.9%, which was significantly higher than the ORR of patients receiving monotherapy (2.2%; P < 0.05) (Table 4).
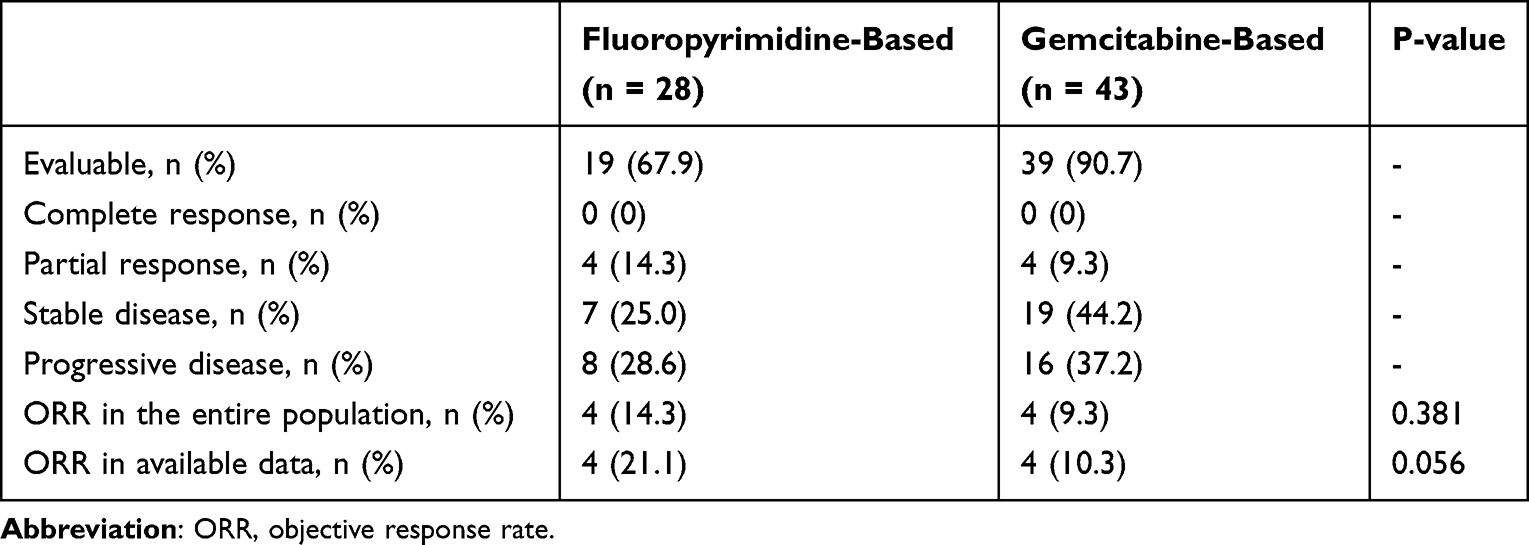 |
Table 3 Response Rates Between Patients Who Received Fluoropyrimidine- and Gemcitabine-Based Regimens |
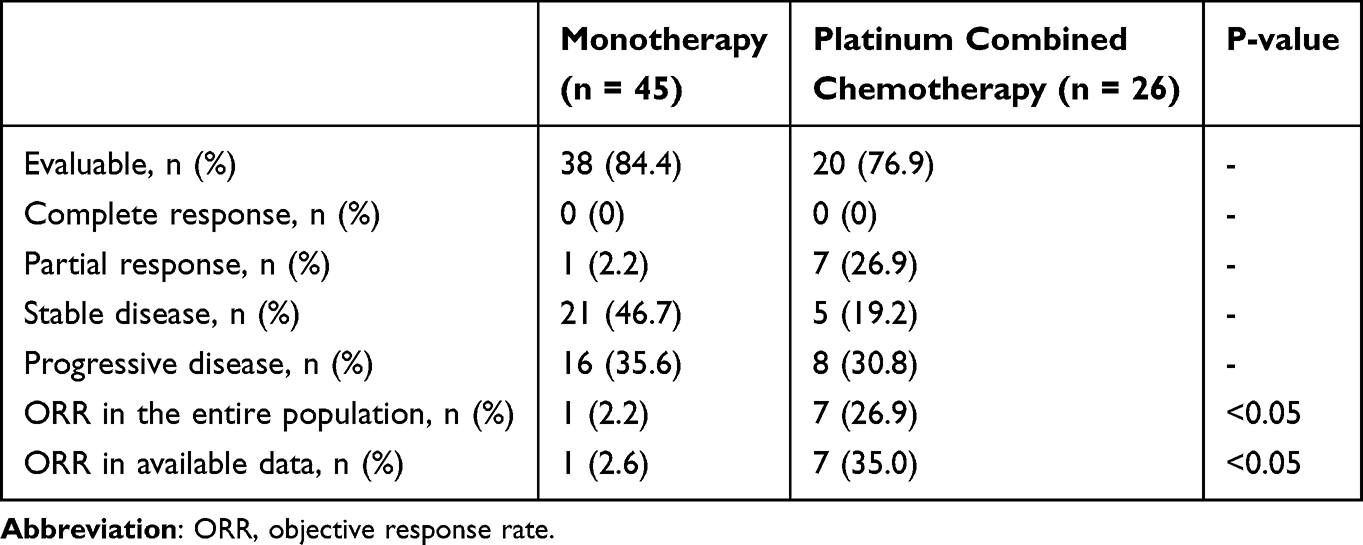 |
Table 4 Response Rates Between Patients Who Received Monotherapy and Platinum Combined Chemotherapy |
Prognostic Factors
Univariate and multivariate Cox proportional hazards models were used to identify the prognostic factors in patients with advanced-stage ampullary adenocarcinoma (Table 5). Multivariable analyses were conducted using complete-case analysis because of missing baseline laboratory data. Among the evaluable patients included in the multivariable overall survival analysis, 49 events were observed. Univariate analysis identified potential prognostic factors, including BMI, ECOG PS, metastatic type, and CA 19–9 level. However, multivariate analysis revealed that only ECOG PS was significantly associated with prognosis.
 |
Table 5 Prognostic Factors |
Discussion
This study compared fluoropyrimidine-based and gemcitabine-based chemotherapy in patients with advanced-stage ampullary adenocarcinoma and further explored the potential role of platinum-combination therapy. Although gemcitabine-based chemotherapy was associated with numerically longer OS in the unadjusted analysis, this difference was attenuated after adjustment for clinically relevant prognostic factors, suggesting broadly comparable effectiveness between gemcitabine- and fluoropyrimidine-based regimens. Similarly, no significant differences in PFS or ORR were observed between the two chemotherapy backbones. Platinum-combination chemotherapy was associated with a higher ORR than single-agent chemotherapy; however, this did not translate into a statistically significant improvement in OS or PFS. Therefore, the potential role of platinum-combination therapy should be interpreted cautiously.
Previous studies on these two chemotherapy regimens have been limited by their small sample sizes.14,19–21 Kim et al reported a median OS of 125 months in 29 patients, with no significant difference between gemcitabine- and fluoropyrimidine-based regimens.19 Similarly, Shoji et al, with 26 cases, reported a median OS of 80 and 12.3 months for cisplatin plus 5-FU and cisplatin plus gemcitabine, respectively (P = 0.29).20 In contrast, Jiang et al found a trend toward improved median OS in 64 cases in a fluoropyrimidine group: 191 months versus 12.3 months (P = 0.06).21 However, after adjusting for confounding factors in the multivariate analysis, only a trend favoring fluoropyrimidine-based treatment for OS was observed, without reaching statistical significance (P = 0.07). Our study with 71 patients who received chemotherapy showed that the gemcitabine-based regimen had a median OS of 14.4 months, compared to 11.5 months for the fluoropyrimidine-based regimen, which aligns with previous retrospective studies. Taken together, the findings suggest that the survival of patients with advanced ampullary adenocarcinoma remains poor over time, at approximately 8–19 months. Our study, with the largest sample size reported to date, confirmed that both gemcitabine- and fluoropyrimidine-based regimens have similar efficacies. Factors such as toxicity, treatment details, and patient preferences should also be considered when selecting chemotherapy regimens.
The role of platinum in chemotherapy regimens remains unclear. Our study showed no statistically significant improvement in OS with adding platinum (11.3 vs 14.9 months. Although no strong evidence supports this issue, in biliary tract cancer, the addition of cisplatin to gemcitabine demonstrated an OS benefit over gemcitabine monotherapy (11.7 vs 8.1 months; HR 0.64; 95% CI 0.52–0.80; P < 0.001).10 However, only 20 patients in that study had ampullary cancer, and subgroup analysis showed no significant improvement in OS (HR 0.62, 95% CI 0.21–1.82).10 Our subgroup analysis showed no OS benefit from adding platinum to gemcitabine, consistent with a previous report. Altogether, even with platinum-combined chemotherapy, the OS remained at approximately 12 months, comparable to our study’s OS.
In bowel cancer, a doublet regimen, such as FOLFOX, has demonstrated OS benefits over single-agent 5-FU,22,23 but there is no strong evidence supporting this approach in ampullary cancer. A small Phase 2 single-arm study, which included 23 patients with small bowel adenocarcinoma and 7 patients with ampullary adenocarcinoma, reported a median OS of 12.9 months with capecitabine and oxaliplatin (CAPOX) plus bevacizumab.24 Another study using CAPOX in 18 patients with small bowel adenocarcinoma and 12 patients with ampullary adenocarcinoma reported a median OS of 15.5 months in patients with metastases.25 Upon review, the overall survival reported in these studies was comparable with our findings. No data comparing single-agent 5FU with platinum-based combinations for ampullary adenocarcinoma are available. Our subgroup analysis revealed no difference between 5FU alone and platinum-based combinations. However, a comparison between the platinum plus gemcitabine and platinum plus fluoropyrimidine regimens showed an OS benefit with platinum plus gemcitabine. These data have not been reported in other studies; however, they should be interpreted cautiously because of the small sample sizes. Platinum-combined chemotherapy regimens may not offer an OS benefit compared to single-agent chemotherapy, even with gemcitabine or fluoropyrimidine combinations. However, further research on differential chemotherapeutic benefits based on histological subtypes should be explored. Our study could not draw any conclusions because only six cases (8.5%) reported specific subtypes.
Our study showed an ORR of 11.3% in all patients receiving chemotherapy, with no significant difference between the fluoropyrimidine and gemcitabine regimens (14.3% vs 9.3%). However, the ORR was lower than that reported by Jiang et al (58% for fluoropyrimidine; 21% for gemcitabine)21 In that study, 80% of the patients in the fluoropyrimidine group received platinum doublet therapy compared with 62% in the gemcitabine group. In contrast, only 53.5% of patients in the fluoropyrimidine group and 25.6% in the gemcitabine group received platinum doublet therapy, which may explain the lower ORR observed in our study. Although no significant OS or PFS benefit was observed with platinum-combination chemotherapy, this approach was associated with a higher ORR compared with single-agent chemotherapy. This finding may support consideration of platinum-combination regimens in selected patients who require tumor shrinkage, such as those with high tumor burden or symptomatic disease. However, given the retrospective design, limited subgroup sample size, and potential selection bias, this observation should be interpreted as hypothesis-generating rather than definitive evidence supporting routine use of platinum-combination therapy. Future studies incorporating toxicity and quality-of-life outcomes are needed to better define the clinical utility of platinum-combination therapy.
The key factors influencing survival may not be the chemotherapy regimen itself but maintaining good ECOG PS.26–30 Preserving and improving the ECOG PS is crucial for enhancing survival and increasing the likelihood of receiving subsequent therapy. In our study, most patients who received gemcitabine-based chemotherapy as the first-line treatment subsequently received a fluoropyrimidine-based regimen as the second-line therapy, and vice versa. Based on our findings, approximately 45% of the patients could proceed with second-line therapy. Owing to the anatomical location of the ampulla of Vater, small bowel and biliary obstruction, leading to liver failure and infection, are complications that can result in a decline in the ECOG PS.2,31,32 Early recognition, prevention, and appropriate management of these complications may help maintain a good ECOG PS and allow patients to continue treatment.
This study has some limitations. First, its retrospective, single-center design may have introduced selection bias and residual confounding, particularly in treatment selection between chemotherapy regimens. Treatment decisions may have been influenced by physician preference, patient frailty, comorbidities, and other unmeasured clinical factors not fully captured by ECOG PS. Second, treatment heterogeneity within each chemotherapy backbone, including both monotherapy and platinum-combination regimens, may have influenced the observed outcomes. Third, the relatively small sample size, particularly in subgroup analyses, limited the statistical power to detect modest survival differences. Although a parsimonious multivariable approach was applied to minimize model overfitting, residual model instability cannot be completely excluded. Histological subtype data were available in only 8.5% of cases, limiting our ability to evaluate their prognostic or predictive value. Therefore, we could not evaluate whether outcomes differed between intestinal and pancreatobiliary phenotypes, and the findings should not be interpreted as definitive evidence for selecting chemotherapy according to tumor subtype. Additionally, toxicity and quality-of-life data were not systematically recorded. Despite these limitations, this study represents the largest cohort reported to date and provides hypothesis-generating real-world evidence regarding chemotherapy selection and the potential role of platinum-combination therapy in advanced ampullary adenocarcinoma.
In conclusion, palliative chemotherapy was associated with prolonged survival in patients with advanced-stage ampullary adenocarcinoma, particularly among those with good ECOG performance status. Fluoropyrimidine-based and gemcitabine-based regimens demonstrated broadly comparable effectiveness after adjustment for clinically relevant prognostic factors. Platinum-combination chemotherapy was associated with a higher ORR and may be considered in selected patients requiring tumor shrinkage; however, no significant OS or PFS benefit was observed. These findings should be regarded as hypothesis-generating real-world evidence and warrant validation in larger prospective or multicenter studies incorporating toxicity, quality-of-life, histological subtype, and molecular data.
Abbreviations
OS, overall survival; PFS, progression-free survival; HR, hazard ratio; ORR, objective response rate; ECOG, Eastern Cooperative Oncology Group; PS, performance status; BMI, body mass index; 5-FU, 5-fluorouracil; FOLFOX, 5-FU plus folinic acid and oxaliplatin; RECIST, Response Evaluation Criteria for Solid Tumors; CT, computed tomography; BSC, best supportive care; CI, confidence interval; CAPOX, capecitabine and oxaliplatin.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the Prince of Songkla University (REC.67547141/November 30, 2024). Patient consent was waived because of the retrospective nature of the study. Patient information was anonymized for confidentiality.
Acknowledgments
The authors thank our colleague Jayuphan J for assisting with the statistical analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no specific funding for this article.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Albores-Saavedra J, Schwartz AM, Batich K, Henson DE. Cancers of the ampulla of vater: demographics, morphology, and survival based on 5,625 cases from the SEER program. J Surg Oncol. 2009;100(7):598–13. doi:10.1002/jso.21374
2. Ahn DH, Bekaii-Saab T. Ampullary cancer: an overview. Am Soc Clin Oncol Educ Book. 2014;34(1):112–115. doi:10.14694/EdBook_AM.2014.34.112
3. Goodman MT, Yamamoto J. Descriptive study of gallbladder, extrahepatic bile duct, and ampullary cancers in the United States, 1997-2002. Cancer Causes Control. 2007;18(4):415–422. doi:10.1007/s10552-006-0109-4
4. Heinrich S, Clavien P-A. Ampullary cancer. Curr Opin Gastroenterol. 2010;26(3):280–285. doi:10.1097/MOG.0b013e3283378eb0
5. Rizzo A, Dadduzio V, Lombardi L, Ricci AD, Gadaleta-Caldarola G. Ampullary carcinoma: an overview of a rare entity and discussion of current and future therapeutic challenges. Curr Oncol. 2021;28(5):3393–3402. doi:10.3390/curroncol28050293
6. de Castro SM, van Heek NT, Kuhlmann KF, et al. Surgical management of neoplasms of the ampulla of Vater: local resection or pancreatoduodenectomy and prognostic factors for survival. Surgery. 2004;136(5):994–1002. doi:10.1016/j.surg.2004.03.010
7. Rostain F, Hamza S, Drouillard A, Faivre J, Bouvier A-M, Lepage C. Trends in incidence and management of cancer of the ampulla of Vater. World J Gastroenterol. 2014;20(29):10144–10150. doi:10.3748/wjg.v20.i29.10144
8. Facer BD, Cloyd JM, Manne A, et al. Treatment patterns and outcomes for patients with ampullary carcinoma who do not undergo surgery. Cancers. 2023;15(14):3727. doi:10.3390/cancers15143727
9. Patel M, Uboha NV. Treatment approach to adenocarcinoma of the ampulla of Vater. Curr Treat Options Oncol. 2021;22(11):103. doi:10.1007/s11864-021-00894-5
10. Valle J, Wasan H, Palmer DH, et al. Cisplatin plus gemcitabine versus gemcitabine for biliary tract cancer. N Engl J Med. 2010;362(14):1273–1281. doi:10.1056/NEJMoa0908721
11. Neoptolemos JP, Moore MJ, Cox TF, et al. Effect of adjuvant chemotherapy with fluorouracil plus folinic acid or gemcitabine vs observation on survival in patients with resected periampullary adenocarcinoma: the ESPAC-3 periampullary cancer randomized trial. JAMA. 2012;308(2):147–156. doi:10.1001/jama.2012.7352
12. Chandrasegaram MD, Gill AJ, Samra J, et al. Ampullary cancer of intestinal origin and duodenal cancer—a logical clinical and therapeutic subgroup in periampullary cancer. World J Gastrointest Oncol. 2017;9(10):407–415. doi:10.4251/wjgo.v9.i10.407
13. Pea A, Riva G, Bernasconi R, et al. Ampulla of Vater carcinoma: molecular landscape and clinical implications. World J Gastrointest Oncol. 2018;10(11):370–380. doi:10.4251/wjgo.v10.i11.370
14. Ghosn M, Kourie HR, El Rassy E, et al. Where does chemotherapy stands in the treatment of ampullary carcinoma? A review of literature. World J Gastrointest Oncol. 2016;8(10):745–750. doi:10.4251/wjgo.v8.i10.745
15. Ecker BL, Vollmer CM, Behrman SW, et al. Role of adjuvant multimodality therapy after curative-intent resection of ampullary carcinoma. JAMA Surg. 2019;154(8):706–714. doi:10.1001/jamasurg.2019.1170
16. Moekotte AL, Lof S, Van Roessel S, et al. Histopathologic predictors of survival and recurrence in resected ampullary adenocarcinoma: international multicenter cohort study. Ann Surg. 2020;272(6):1086–1093. doi:10.1097/SLA.0000000000003177
17. Bowitz Lothe IM, Kleive D, Pomianowska E, et al. Clinical relevance of pancreatobiliary and intestinal subtypes of ampullary and duodenal adenocarcinoma: pattern of recurrence, chemotherapy, and survival after pancreatoduodenectomy. Pancreatology. 2019;19(2):316–324. doi:10.1016/j.pan.2019.01.019
18. National Comprehensive Cancer Network. Ampullary adenocarcinoma. version 2. 2025. Available from: https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1511.
19. Kim ST, Lee J, Lee KT, et al. The efficacy of frontline platinum-based combination chemotherapy in advanced adenocarcinoma of the ampulla of Vater. Med Oncol. 2010;27(4):1149–1154. doi:10.1007/s12032-009-9351-4
20. Shoji H, Morizane C, Hiraoka N, et al. Twenty-six cases of advanced ampullary adenocarcinoma treated with systemic chemotherapy. Jpn J Clin Oncol. 2014;44(4):324–330. doi:10.1093/jjco/hyt237
21. Jiang ZQ, Varadhachary G, Wang X, et al. A retrospective study of ampullary adenocarcinomas: overall survival and responsiveness to fluoropyrimidine-based chemotherapy. Ann Oncol. 2013;24(9):2349–2353. doi:10.1093/annonc/mdt191
22. Neugut AI, Lin A, Raab GT, et al. FOLFOX and FOLFIRI use in stage IV colon cancer: analysis of SEER-medicare data. Clin Colorectal Cancer. 2019;18(2):133–140. doi:10.1016/j.clcc.2019.01.005
23. Giacchetti S, Perpoint B, Zidani R, et al. Phase III multicenter randomized trial of oxaliplatin added to chronomodulated fluorouracil-leucovorin as first-line treatment of metastatic colorectal cancer. J Clin Oncol. 2000;18(1):136–147. doi:10.1200/JCO.2000.18.1.136
24. Gulhati P, Raghav K, Shroff RT, et al. Bevacizumab combined with capecitabine and oxaliplatin in patients with advanced adenocarcinoma of the small bowel or ampulla of Vater: a single-center, open-label, phase 2 study. Cancer. 2017;123(6):1011–1017. doi:10.1002/cncr.30445
25. Overman MJ, Varadhachary GR, Kopetz S, et al. Phase II study of capecitabine and oxaliplatin for advanced adenocarcinoma of the small bowel and ampulla of vater. J Clin Oncol. 2009;27(16):2598–2603. doi:10.1200/JCO.2008.19.7145
26. Caires-Lima R, Cayres K, Protásio B, et al. Palliative chemotherapy outcomes in patients with ECOG-PS higher than 1. Ecancermedicalscience. 2018;12:831. doi:10.3332/ecancer.2018.831
27. Colloca G. Performance status as prognostic factor in phase III trials of first-line chemotherapy of unresectable or metastatic pancreatic cancer: a trial-level meta-analysis. Asia Pac J Clin Oncol. 2022;18(3):232–239. doi:10.1111/ajco.13598
28. Ekström A, Brun E, Eberhard J, Segerlantz M. Second-line palliative chemotherapy, survival, and prognostic factors in patients with advanced pancreatic cancer. Acta Oncol. 2021;60(12):1580–1588. doi:10.1080/0284186X.2021.1973680
29. Prigerson HG, Bao Y, Shah MA, et al. Chemotherapy use, performance status, and quality of life at the end of life. JAMA Oncol. 2015;1(6):778–784. doi:10.1001/jamaoncol.2015.2378
30. Lamarca A, Palmer DH, Wasan HS, et al. Second-line FOLFOX chemotherapy versus active symptom control for advanced biliary tract cancer (ABC-06): a Phase 3, open-label, randomised, controlled trial. Lancet Oncol. 2021;22(5):690–701. doi:10.1016/S1470-2045(21)00027-9
31. Paluri RK, Kasi A. Periampullary tumors. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2025.
32. Abudalou M, Malkowski M, Huh A, Ricklan D, Stallwood C. Ampullary adenocarcinoma causing small intestinal obstruction. Cureus. 2020;12(11):e11575. doi:10.7759/cureus.11575
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Overweight and Obesity are Associated with Poorer Survival Among Patients with Advanced Non-Small Cell Lung Cancer Receiving Platinum-Based Chemotherapy
Sutandyo N, Hanafi AR, Jayusman AM, Kurniawati SA, Hanif MA
International Journal of General Medicine 2023, 16:85-93
Published Date: 6 January 2023
Survival Outcomes and Efficacy of Platinum in Early Breast Cancer Patients with Germline BRCA1 or BRCA2 Mutation: A Multicenter Retrospective Cohort Study
Chen X, Qian X, Xiao M, Zhang P
Breast Cancer: Targets and Therapy 2023, 15:671-682
Published Date: 4 September 2023
Nab-Paclitaxel Based Chemotherapy in the Treatment of Advanced Epithelioid Hemangioendothelioma: A Single-Institution Experience
Liu X, Yang P, Liu L, Si S, Zhou R, Liu T, Tan H
Cancer Management and Research 2025, 17:373-381
Published Date: 21 February 2025
Prognostic Significance of the CRP-Albumin-Lymphocyte Index (CALLY) in Triple Negative Breast Cancer Patients: A Real-World Retrospective Study
Liu Y, Zhang F, Guo C, Li Q
Breast Cancer: Targets and Therapy 2026, 18:582022
Published Date: 13 March 2026