")
Back to Journals » International Journal of General Medicine » Volume 16
Overweight and Obesity are Associated with Poorer Survival Among Patients with Advanced Non-Small Cell Lung Cancer Receiving Platinum-Based Chemotherapy
Authors Sutandyo N , Hanafi AR, Jayusman AM, Kurniawati SA, Hanif MA
Received 15 July 2022
Accepted for publication 5 December 2022
Published 6 January 2023 Volume 2023:16 Pages 85—93
DOI https://doi.org/10.2147/IJGM.S382577
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Noorwati Sutandyo,1,2 Arif Riswahyudi Hanafi,3 Achmad Mulawarman Jayusman,3 Sri Agustini Kurniawati,1 Muhamad Alfin Hanif3
1Division of Hematology and Medical Oncology, Department of Internal Medicine, Dharmais National Cancer Hospital, Jakarta, Indonesia; 2Faculty of Medicine, Universitas Indonesia, Jakarta, Indonesia; 3Department of Pulmonology, Dharmais National Cancer Hospital, Jakarta, Indonesia
Correspondence: Noorwati Sutandyo, Email [email protected]
Background and Aim: Most patients with non-small cell lung cancer (NSCLC) are diagnosed in advanced-stage disease and therefore have poor overall survival. It remains unclear whether nutritional status affects response rate and overall survival in NSCLC patients. This study aimed to evaluate the association of nutritional status with treatment response and overall survival in patients with advanced stage of NSCLC.
Methods: Patients aged ≥ 18 years with stage II–IV NSCLC (January–June 2018) in a national cancer center in Indonesia were enrolled in this study. The patients were followed up for 2 years since NSCLC diagnosis was established. Clinical data including age, sex, histology of cancer, disease stage, cachexia, and weight status before chemotherapy were reviewed and analyzed. Logistic regression and Cox regression analyses were performed.
Results: A total of 174 patients (71% males, mean age = 58± 9.4 years) was included. Complete response was found in < 1% patients, partial response 41%, stable disease 33%, and progressive disease 25%. Median survival was 12 months (95% CI: 11– 13 months). Mortality rate was 5.7 per 100 person-months. Poor survival was associated with being males (HR: 1.77, 95% CI: 1.15– 2.72, P = 0.009), and overweight or obesity (HR 1.67, 95% CI: 1.04– 2.69, P = 0.034). These associations were independent of sex, age, staging, histopathology, performance status and D-dimer level at baseline. Cachexia and BMI at baseline were not associated with treatment response.
Conclusion: Males and having overweight or obesity are independently associated with lower survival in patients with advanced stage of NSCLC undergoing platinum-based chemotherapy.
Keywords: body mass index, nutritional status, lung cancer
Introduction
Lung cancer remains one of the most common cancer worldwide and is responsible for almost one-quarter of all cancer death.1 It has been estimated that lung cancer contributes to 1.79 million deaths per year.2 Among lung cancer cases, the predominant type is non-small cell lung cancer (NSCLC) which has an overall 5-year survival of 24%.2 Although various diagnostic tools have been developed to detect NSCLC in early stage, most cases of NSCLC are delayed in diagnosis and/or treatment,1,2 and therefore more than 50% cases are diagnosed in advanced-stage disease.3
Platinum-based therapy has been offered as a first-line treatment in patients with advanced stage of NSCLC and good performance status.3 Nevertheless, the response rate to treatment was estimated only between 20% and 40%, leaving the majority of patients with stable or progressive disease.4 In addition, poor overall survival was reported in most studies.5–7
Nutritional status pre-chemotherapy and weight trajectories during treatment have been suggested to affect response rate and overall survival among patients with advanced stage of NSCLC. However, results from previous studies were conflicting. For instance, some studies found obesity status before treatment was associated with protective effect on mortality,8–10 while other studies indicated that such association was confounded by smoking status.11 Moreover, weight loss or cachexia during treatment has been indicated to be a poor prognostic factor by some studies,12,13 but other studies found no association between weight loss and overall survival in patients with advanced stage of NSCLC.14 Hence, it remains unclear whether nutritional status is a predictor of treatment response and survival in patients with advanced lung cancer, particularly those receiving chemotherapy as standard care. More detailed knowledge in this area would contribute to appropriate clinical decision-making and a more accurate prediction of the outcome. In this study, we, therefore, aimed to evaluate factors associated with treatment response and survival in a cohort of patients with advanced NSCLC receiving platinum-based chemotherapy in a tertiary hospital in Indonesia. The weight status before chemotherapy treatment was the main predictor examined.
Materials and Methods
Study Population
A cohort study was conducted in a national cancer center in Indonesia. The population was patients with a histological diagnosis of NSCLC receiving chemotherapy. The patients were enrolled in the study between January and June 2018 and were followed for 2 years after diagnosis. NSCLC diagnosis and its staging were confirmed through histopathological and immunohistochemistry evaluations, pleural fluid cytology, and imaging. All eligible patients received packed red cell transfusion before chemotherapy initiation if the hemoglobin level was below 10 mg/dl and platinum-based chemotherapy according to the current guideline,15 whereby the combination of platinum (cisplatin/carboplatin) and pemetrexed was used as the first-line treatment in patients with adenocarcinoma, whereas the combination of platinum and gemcitabine was used the first-line treatment in patients with squamous cell carcinoma. The second-line treatment for both adenocarcinoma and squamous cell carcinoma was the combination of platinum and taxane.
The inclusion criteria were as follows: (1) patients having a histologically or cytologically confirmed NSCLC with a diagnosis of stage II–IV disease according to the American Joint Committee on Cancer (AJCC) staging manual16; (2) the first diagnosis of NSCLC was at ≥18 years of age; (3) ECOG performance status score was between 0 and 217; (4) normal kidney function assessed by glomerular filtration rate according to Cockroft–Gault formula; (5) normal liver enzymes, where liver enzymes were less or equal to two times of the upper limit normal; and (6) never received cancer treatment before. Patients with EGFR mutations, acute kidney injury, chronic kidney disease, liver dysfunction, or other primary cancer than lung cancer, patients refusing treatment, or patients who died before completing treatment were excluded.
Informed consent was obtained from all patients included in the study and the procedure was conducted according to the Declaration of Helsinki. This study was approved by the ethical committee of Dharmais National Cancer Center, Indonesia (no. 014/KEPK/I/2018).
Baseline Evaluation and Follow-Up
Baseline Data
Patients’ demographics, tumor characteristics, disease history (including body mass index before NSCLC diagnosis), body weight and height, body mass index (BMI), ECOG performance status score, and D-dimer before chemotherapy were collected at enrollment. D-dimer was included into one of the exposure variables as it has been suggested has a predictor of lung cancer prognosis.18 Presence of cachexia, defined as weight loss >5% during the past 6 months or any degree of weight loss >2% in patients with body mass index <20 kg/m2, was also assessed at baseline.19
Treatment Response
Treatment response was assessed 3 weeks after completion of chemotherapy. Evaluation of treatment response was performed according to Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1.20 Treatment response was classified as complete response, partial response, progressive disease, and stable disease. Overall response rate was defined as the proportion of patients achieving complete response and partial response.
Survival Status
Survival was ascertained from follow-up visits in the hospital. If necessary, a phone call with the patients or their family was made. Survival times were calculated in months from the date of NSCLC diagnosis until death due to NSCLC (event) or until the end of follow-up (ie, 2 years after NSCLC diagnosis).
Sampling
Consecutive sampling was used for patients’ recruitment. To achieve at least 80% of power and 5% of significance level, 174 patients were recruited.
Statistical Analysis
Categorical variables were presented as proportions, whereas continuous variables were presented as mean and standard deviation since the continuous data were normally distributed according to the histogram examinations. Chi-square test was used to compare proportions between categorical variables and the treatment response, while an independent t-test was used to assess the mean difference between the continuous variables.
Outcomes were treatment response and overall mortality rate. Treatment response was divided into CR/PR and SD/PD. To association of treatment response with patients’ demographics, histological subtypes, staging, presence of cachexia, and hypercoagulable state, logistic regression analyses were performed. Overall mortality rate was assessed. Survival time after diagnosis was calculated using Kaplan–Meier estimates. Differences in survival distributions for each independent variable were analyzed using the Log rank test. Cox proportional hazard regression analysis was then performed to examine the independent associations of independent variables with survival. Hazard ratio (HR) and its 95% CI were presented. Statistical software Stata (version 16) was used to perform all analyses.
Results
Patients’ Characteristics and Treatment Response
A total of 174 patients were included in the analysis (71% males, mean age of all patients = 58.1 ± 9.4 years). The response rate to chemotherapy was 42% (41% partial response, <1% complete response). Patients having stable disease and progressive disease responses were 33% and 2%, respectively. Smoking history was present in 38.5% of the patients. Other than chemotherapy, 10 patients (5.7%) underwent cryotherapy, and 85 patients (48.9%) underwent palliative radiotherapy. Most patients were in stage IV (78%) and had histopathology of adenocarcinoma (71%). The overall mean BMI was 21.9 ± 3.6 kg/m2, with 15.5% of individuals had underweight and 19% overweight or obesity. (Table 1). The patients’ characteristics did not differ by weight status, except for sex. A higher proportion of females was found in the overweight/obesity group compared to the underweight or normal weight group (Table 2).
 |
Table 1 Treatment Response and Patients’ Characteristics |
 |
Table 2 Patients’ Characteristics According to the Weight Status |
When comparing the patients’ characteristics by sex, we found a higher proportion of age ≥60 years in males than females (53% in males vs 20% in females). Adenocarcinoma was less common in males than females (67% in males vs 80% in females), and stage IV disease was less prevalent in males than females (75% in males vs 84% in females).
Patients’ Characteristics Were Not Associated with Treatment Response
Treatment response was not associated with any patients’ characteristics, such as sex, age, smoking history, histopathology, staging, ECOG performance status, BMI, cachexia, or D-dimer level according to the crude and adjusted analysis (Table 3).
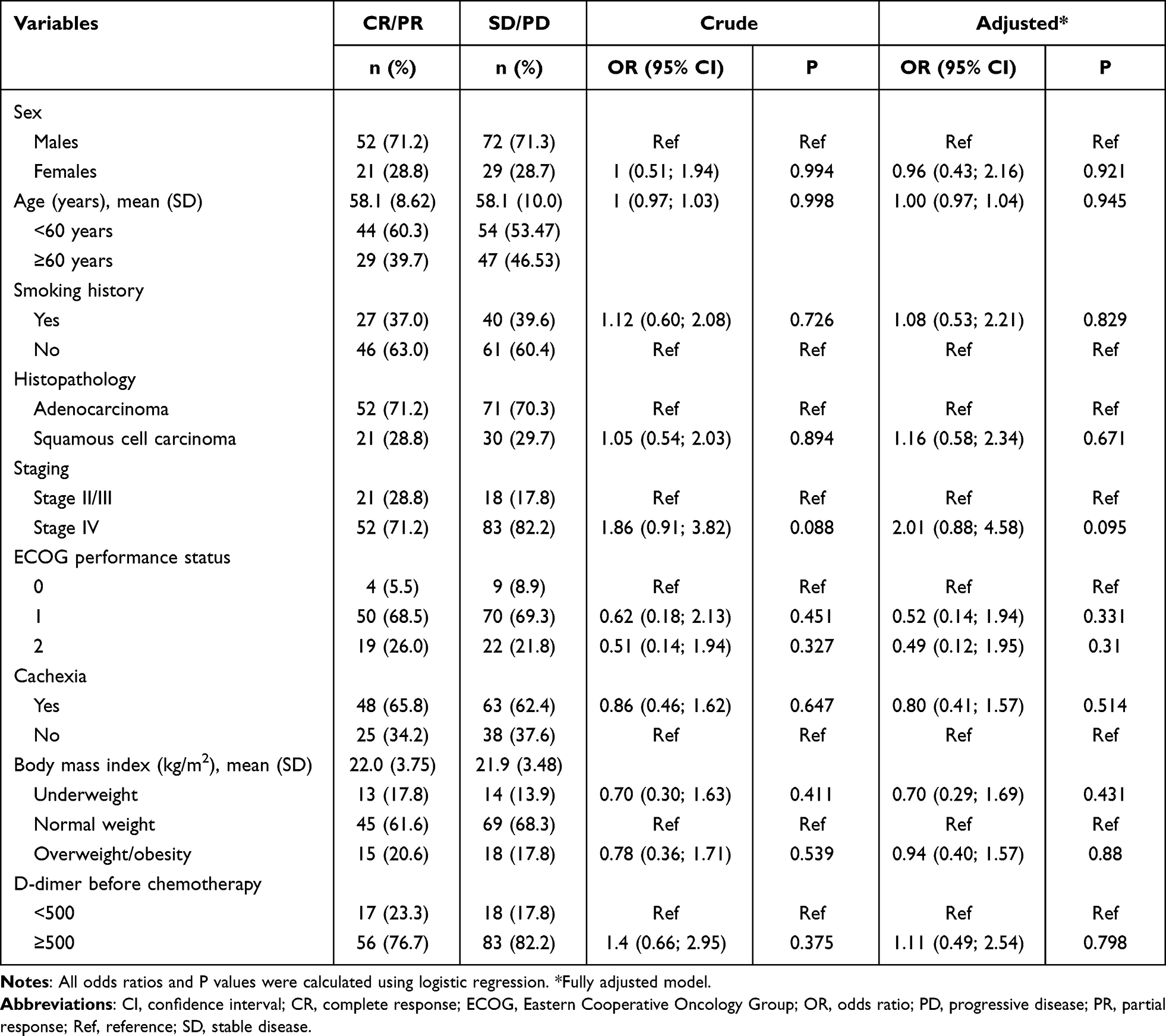 |
Table 3 Association Between Clinical Characteristics and Treatment Response |
Sex and Weight Status Were Associated with Lung Cancer Mortality
During 2 years of follow-up, 134 patients died. Median survival was 12 months (95% CI: 11–13 months). Overall mortality risk was 6.1% (95% CI: 5.1–7.3%), and the mortality rate was 5.7 per 100 person-months. Overall mortality rate significantly was higher among males (6.3 per 100) than females (4.5 per 100), and slightly higher among patients in stage IV (6.1 per 100) than stage III (4.4 per 100). Mortality rate was increasing with increased of BMI, with mortality rate among patients with underweight (4.5 per 100), normal weight (5.8 per 100), and overweight/obesity (6.5 per 100). Based on the Kaplan–Meier graphs, survival function was higher in females than males over time (P = 0.046) and higher in individuals with performance status grade 0 (fully active) than in those with performance status grade 1 or 2 (P = 0.046). On the other hand, no difference in survival function by age, staging, histopathology, cachexia, weight status, or D-dimer. At the first year of follow-up, patients with complete or partial response seemed to have slightly higher survival over time compared to the others. However, after a year of follow-up the survival was similar between patients with complete or partial response vs patients with stable or progressive disease (Figure 1E). Kaplan–Meier graphs stratified by patients’ characteristics are shown in Figure 1A–I.
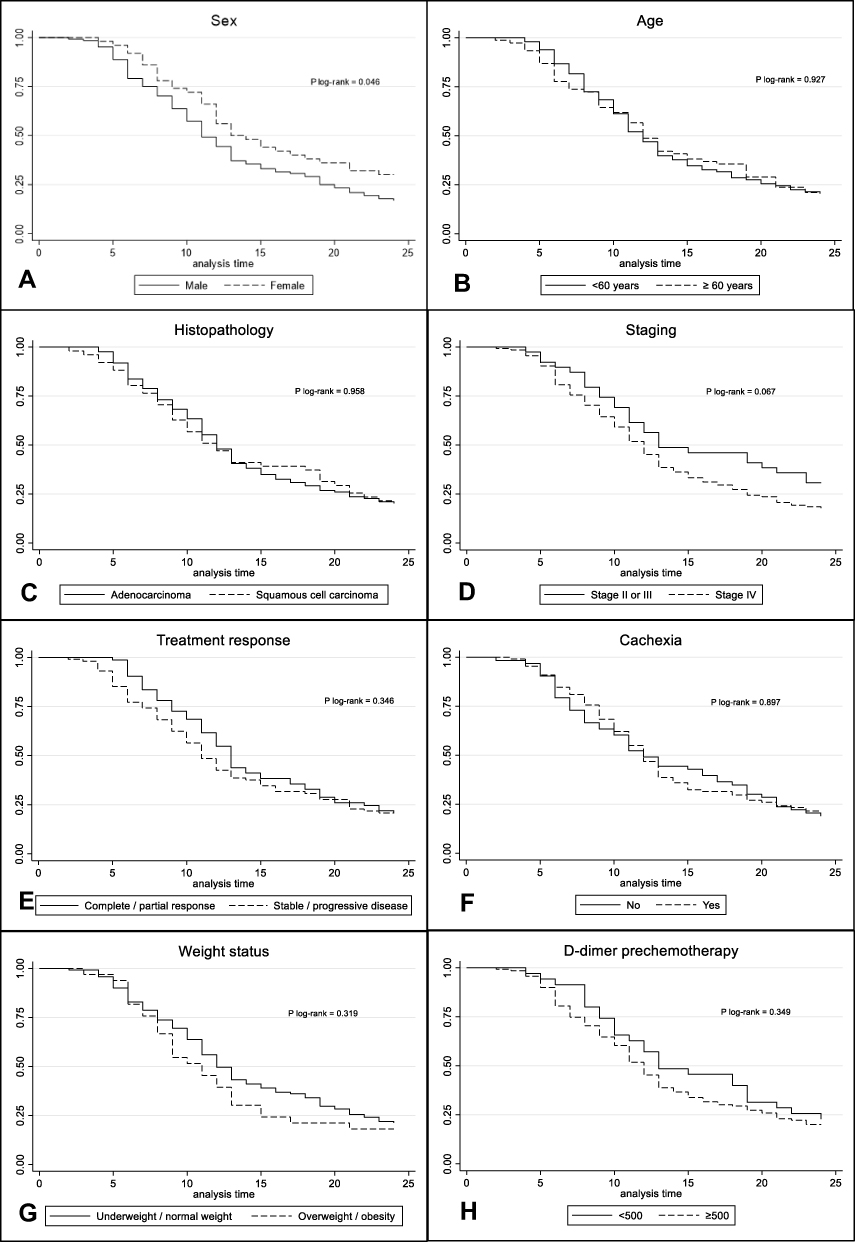 |
Figure 1 Kaplan–Meier graph of survival functions by (A) sex, (B) age, (C) histopathology, (D) staging, (E) treatment response, (F) the presence of cachexia, (G) weight status, (H) weight D-dimer levels at baseline, (I) performance status. |
Crude regression showed no association between 2-year mortality and sex, age, staging, BMI status, histopathology, performance status, and D-dimer. After adjustment for the other factors, males had higher mortality compared to males (HR: 1.77, 95% CI: 1.15–2.72, P = 0.009), whereas individuals with overweight or obesity had higher mortality rate compared to those underweight or normal weight (HR 1.67, 95% CI: 1.04–2.69, P = 0.034). The crude and adjusted HRs are presented in Table 4.
 |
Table 4 Sex and Weight Status Were Associated with 2-Year Mortality Rate |
Discussion
In this hospital-based cohort study, we found that the median survival of the patients with advanced stage of NSCLC undergoing platinum-based chemotherapy was 12 months, with 42% patients had complete or partial response. Neither sex, age, staging, histopathology, cachexia, weight status nor D-dimer was associated with treatment response in advanced stage of NSCLC. Meanwhile, this study demonstrated that males and overweight/obesity were associated with higher 2-year overall mortality rate among patients with NSCLC.
At least 50% of study population in the present study were alive at 12-months after chemotherapy initiation. This finding was in line with the previous studies both in the western world settings7 and in an Asian country.6 However, the overall response rate to chemotherapy in the present study was higher compared to the other studies in patients with advanced stage NSCLC receiving platinum-based chemotherapy globally21 and in Asia (42% in this study, 20% in a Taiwanese study, 27% in a Japanese study),6,22 despite similar age, sex, and tumor histopathology distribution. This finding suggests that geographical area or ethnicity might to some extent affect the treatment response.
While platinum-based chemotherapy has been one of the main treatment in advanced stage of NSCLC, it was suggested that genetic polymorphism might affect overall response rate.23 A meta-analysis including Asian NSCLC patients receiving platinum-based treatment reported that at least three polymorphisms of the genes were correlated with platinum response.24 Future studies should take genetic polymorphism analysis into account.
Large population-based studies have shown the evidence of gender difference in survival among patients with NSCLC, whereby males have poorer prognosis regardless of stage.5,25 Our finding confirms the evidence from the previous studies. In the present study, females with advanced stage of NSCLC tended to be younger and mostly had adenocarcinoma as the cancer pathology. These favorable characteristics might have contributed to better prognosis in females. However, we also showed that the gender difference in NSCLC survival was independent of age and histopathology. A possible explanation for this finding is the NSCLC tumor biology somewhat differs between females and males.25 In addition, while some other studies reported contradicting finding due to substandard NSCLC treatment in females,26 the better survival in females in this study indicated no gender bias in NSCLC treatment.
Although obesity is known to have negative effect in survival among cancer patients in general,11 obesity paradox in lung cancer has been an interest and indicated by vast literatures. Patients with overweight or obesity have longer survival, whereas underweight worsens the survival.8–10 In contrast, this study found that overweight or obesity before cancer treatment initiation was associated with poorer survival. The beneficial effect of obesity on NSCLC survival has been suggested to be time-limited; obesity was associated with better survival during the first year after NSCLC diagnosis and associated with higher mortality in later years of follow-up.27 This may be a possible reason for rather contradictory finding in our study. Since the setting in the present study is in a tertiary care, there most likely was several weeks or months of waiting time from diagnosis until patients received treatment. A plausible mechanism contributing to the unfavorable effect of obesity in this study is that the increasing insulin-like growth factors (IGF) due to excess adiposity might enhance tumor progression.28 Obesity might also induce chemoresistance to some chemotherapy agents (including platinum-based chemotherapy)29 and seemed to alter the pharmacokinetics of the chemotherapy agents, impair drug delivery, and induce metabolic perturbations such as increased insulin resistance and hyperglycemia.30
Weight loss after NSCLC diagnosis was known to be associated with worse overall survival.12,13 Moreover, cachexia was generally related to toxicity and complications of cancer therapy.31 Interestingly, no association between cachexia and overall survival was observed in the present study. Different study population may be an explanation for this dissimilar finding. Most patients in our study were in end-stage cancer, whereas the previous studies included patients with early and advanced stages. Taken together, the effect of cachexia overall survival might be prominent among patients in earlier stages, but not among patients with advanced stage of NSCLC. Moreover, 22% of the patients with cachexia in the present study had overweight or obesity at baseline and we found an inverse association of overweight or obesity on overall survival. This might overshadow the effect of cachexia on survival. Cachexia in patients with obesity NSCLC has been known to be prevalent.18 Hence, there might be an interaction between cachexia and obesity in predicting overall survival in NSCLC. Future studies investigating whether overall survival in NSCLC in obese patients with cachexia differs from obese patients without cachexia are warranted to understand the interplay between obesity and cachexia in NSCLC.
Some strengths of this study need to be acknowledged. This study was conducted in a national cancer center with patients treated in accordance with international and national guidelines. However, due to the nature of the retrospective study design, prospective studies are needed to confirm the causal association of our findings. Moreover, selection bias might have occurred in the present study since individuals deceased before chemotherapy completion were excluded. In addition, the generalization of the findings in this study might be limited as the study population consisted of patients treated in a referral hospital.
Conclusions
Males and excess adiposity are associated with poorer survival among patients with advanced stage of NSCLC receiving platinum-based chemotherapy.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2021. CA-A CANCER J Clin. 2021;71(1):7–33. doi:10.3322/caac.21654
2. Thai AA, Solomon BJ, Sequist LV, Gainor JF, Heist RS. Lung cancer. Lancet. 2021;398(10299):535–554. doi:10.1016/S0140-6736(21)00312-3
3. Casal-Mouriño A, Ruano-Ravina A, Lorenzo-González M, et al. Epidemiology of stage III lung cancer: frequency, diagnostic characteristics, and survival. Transl Lung Cancer Res. 2021;10(1):506–518. doi:10.21037/tlcr.2020.03.40
4. Sirohi B, Ashley S, Norton A, et al. Early response to platinum-based first-line chemotherapy in non-small cell lung cancer may predict survival. J Thorac Oncol. 2007;2(8):735–740. doi:10.1097/JTO.0b013e31811f3a7d
5. Spini A, Gini R, Rosellini P, et al. First-line pharmacotherapies and survival among patients diagnosed with non-resectable NSCLC: a real-life setting study with gender prospective. Cancers. 2021;13:23. doi:10.3390/cancers13236129
6. Lai C-L, Wei Y-F, Hsia T-C, et al. S-1 plus cisplatin as first-line treatment of patients with advanced non-small cell lung cancer in Taiwan. Asia Pac J Clin Oncol. 2020;16(2):e68–73. doi:10.1111/ajco.13294
7. Daly ME, Singh N, Ismaila N, et al. Management of stage III non–small-cell lung cancer: ASCO guideline. J Clin Oncol. 2021;40(12):1356–1384. doi:10.1200/JCO.21.02528
8. Icard P, Schussler O, Loi M, et al. Pre-disease and pre-surgery BMI, weight loss and sarcopenia impact survival of resected lung cancer independently of tumor stage. Cancers. 2020;12(2):Feb. doi:10.3390/cancers12020266
9. Shepshelovich D, Xu W, Lu L, et al. Body Mass Index (BMI), BMI change, and overall survival in patients with SCLC and NSCLC: a pooled analysis of the international lung cancer consortium. J Thorac Oncol. 2019;14(9):1594–1607. doi:10.1016/j.jtho.2019.05.031
10. Zhang X, Liu Y, Shao H, Zheng X. Obesity paradox in lung cancer prognosis: evolving biological insights and clinical implications. J Thorac Oncol off Publ Int Assoc Study Lung Cancer. 2017;12(10):1478–1488.
11. Petrelli F, Cortellini A, Indini A, et al. Association of obesity with survival outcomes in patients with cancer: a systematic review and meta-analysis. JAMA Netw Open. 2021;4(3):e213520–e213520. doi:10.1001/jamanetworkopen.2021.3520
12. Yuan QY, Du ML, Loehrer E, et al. Postdiagnosis BMI change is associated with non-small cell lung cancer survival. CANCER Epidemiol BIOMARKERS Prev. 2022;31(1):262–268. doi:10.1158/1055-9965.EPI-21-0503
13. You D, Wang D, Wu Y, et al. Associations of genetic risk, BMI trajectories, and the risk of non-small cell lung cancer: a population-based cohort study. BMC Med. 2022;20:1. doi:10.1186/s12916-022-02400-6
14. Simmons CP, Koinis F, Fallon MT, et al. Prognosis in advanced lung cancer – a prospective study examining key clinicopathological factors. Lung Cancer. 2015;88(3):304–309. doi:10.1016/j.lungcan.2015.03.020
15. Ettinger DS, Wood DE, Aisner DL, et al. Non–small cell lung cancer, version 5.2017, NCCN clinical practice guidelines in oncology. J Natl Compr Cancer Netw. 2017;15(4):504–535. doi:10.6004/jnccn.2017.0050
16. Amin MB, Greene FL, Edge SB, et al. The eighth edition AJCC cancer staging manual: continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J Clin. 2017;67:93–99. doi:10.3322/caac.21388
17. Sok M, Zavrl M, Greif B, Srpčič M. Objective assessment of WHO/ECOG performance status. Support Care Cancer off J Multinatl Assoc. 2019;27(10):3793–3798.
18. Ma M, Cao R, Wang W, et al. The D-dimer level predicts the prognosis in patients with lung cancer: a systematic review and meta-analysis. J Cardiothorac Surg. 2021;16(1):243. doi:10.1186/s13019-021-01618-4
19. Fearon K, Strasser F, Anker SD, et al. Definition and classification of cancer cachexia: an international consensus. Lancet Oncol. 2011;12(5):489–495. doi:10.1016/S1470-2045(10)70218-7
20. Schwartz LH, Litière S, de Vries E, et al. RECIST 1.1-Update and clarification: from the RECIST committee. Eur J Cancer. 2016;62:132–137. doi:10.1016/j.ejca.2016.03.081
21. Bareschino MA, Schettino C, Rossi A, et al. Treatment of advanced non small cell lung cancer. J Thorac Dis. 2011;(2):122–133. doi:10.3978/j.issn.2072-1439.2010.12.08
22. Kubota K, Sakai H, Katakami N, et al. A randomized Phase III trial of oral S-1 plus cisplatin versus docetaxel plus cisplatin in Japanese patients with advanced non-small-cell lung cancer: TCOG0701 CATS trial. Ann Oncol off J Eur Soc Med Oncol. 2015;26(7):1401–1408. doi:10.1093/annonc/mdv190
23. Hildebrandt MAT, Gu J, Wu X. Pharmacogenomics of platinum-based chemotherapy in NSCLC. Expert Opin Drug Metab Toxicol. 2009;5(7):745–755. doi:10.1517/17425250902973711
24. Yin J-Y, Huang Q, Zhao Y-C, Zhou -H-H, Liu Z-Q. Meta-analysis on pharmacogenetics of platinum-based chemotherapy in non small cell lung cancer (NSCLC) patients. PLoS One. 2012;7(6):e38150. doi:10.1371/journal.pone.0038150
25. Radkiewicz C, Dickman PW, Johansson ALV, Wagenius G, Edgren G, Lambe M. Sex and survival in non-small cell lung cancer: a nationwide cohort study. PLoS One. 2019;14(6):e0219206. doi:10.1371/journal.pone.0219206
26. Caldarella A, Crocetti E, Comin CE, Janni A, Pegna AL, Paci E. Gender differences in non-small cell lung cancer: a population-based study. Eur J Surg Oncol. 2007;33(6):763–768. doi:10.1016/j.ejso.2007.01.001
27. Dahlberg SE, Schiller JH, Bonomi PB, et al.Body mass index and its association with clinical outcomes for advanced non-small-cell lung cancer patients enrolled on eastern cooperative oncology group clinical trials. J Thorac Oncol. 2013;(9):1121–1127. doi:10.1097/JTO.0b013e31829cf942
28. Hua H, Kong Q, Yin J, Zhang J, Jiang Y. Insulin-like growth factor receptor signaling in tumorigenesis and drug resistance: a challenge for cancer therapy. J Hematol Oncol. 2020;13(1):64. doi:10.1186/s13045-020-00904-3
29. Hall RG, Jean GW, Sigler M, Shah S. Dosing considerations for obese patients receiving cancer chemotherapeutic agents. Ann Pharmacother. 2013;47(12):1666–1674. doi:10.1177/1060028013509789
30. Lashinger L, Rossi E, Hursting S. Obesity and resistance to cancer chemotherapy: interacting roles of inflammation and metabolic dysregulation. Clin Pharmacol Ther. 2014;96:458–463. doi:10.1038/clpt.2014.136
31. Baracos VE, Martin L, Korc M, Guttridge DC, Fearon KCH. Cancer-associated cachexia. Nat Rev Dis Prim. 2018;4:17105. doi:10.1038/nrdp.2017.105
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.