Back to Journals » Infection and Drug Resistance » Volume 17
Five Years’ Experience with Respiratory Syncytial Virus Among Hospitalized Patients: A Retrospective Study from Jazan, Saudi Arabia
Authors Dhayhi NS, Aqeel A, Ghazwani S, Gosadi IM ![]() , AlQassimi HM, Thubab A, Sairam IA, Hakami MA, Sawan FA, Asiry SM, Khalifa M, Daghreeri H, Badawy A, Ghawi AA, Arishi H, Almudeer A, Shrwani KJ, Alhazmi AH
, AlQassimi HM, Thubab A, Sairam IA, Hakami MA, Sawan FA, Asiry SM, Khalifa M, Daghreeri H, Badawy A, Ghawi AA, Arishi H, Almudeer A, Shrwani KJ, Alhazmi AH ![]()
Received 11 July 2024
Accepted for publication 20 November 2024
Published 23 November 2024 Volume 2024:17 Pages 5179—5187
DOI https://doi.org/10.2147/IDR.S475574
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Nabil S Dhayhi,1,* Ali Aqeel,2,* Salman Ghazwani,3 Ibrahim M Gosadi,4 Haleemah Mohammed AlQassimi,5 Abdullah Thubab,6 Ibrahim Abdullah Sairam,6 Majed Ahmed Hakami,6 Fahd Ahmed Sawan,6 Sabreen Mohammed Asiry,7 Mawahib Khalifa,7 Hadi Daghreeri,8 Ahmed Badawy,2 Afrah Abdulrahman Ghawi,9 Haidar Arishi,1 Ali Almudeer,2 Khalid J Shrwani,10 Abdulaziz H Alhazmi11,12
1Department of Pediatric Infectious Diseases, King Fahd Central Hospital, Jazan, 45142, Saudi Arabia; 2Department of Neonatology, King Fahd Central Hospital, Jazan, 45142, Saudi Arabia; 3Department of Pediatric Surgery, King Fahd Central Hospital, Jazan, 45142, Saudi Arabia; 4Department of Family and Community Medicine, Faculty of Medicine, Jazan University, Jazan, 45142, Saudi Arabia; 5Department of Pediatric Intensive Care, King Fahd Central Hospital, Jazan, 45142, Saudi Arabia; 6Department of Public Health, King Fahd Central Hospital, Jazan, 45142, Saudi Arabia; 7Department of Pediatric, King Fahd Central Hospital, Jazan, 45142, Saudi Arabia; 8Department of Family Medicine, Directorate General of Health Affairs, Jazan, 45142, Saudi Arabia; 9Department of Pulmonology, King Fahd Central Hospital, Jazan, 45142, Saudi Arabia; 10Public Health Authority, Jazan, 45142, Saudi Arabia; 11Department of Basic Medical Sciences, Faculty of Medicine, Jazan University, Jazan, 45142, Saudi Arabia; 12Health Sciences Research Center, Jazan University, Jazan, 45142, Saudi Arabia
*These authors contributed equally to this work
Correspondence: Abdulaziz H Alhazmi, Department of Basic Medical Sciences, Faculty of Medicine, Jazan University, Jazan, 45142, Saudi Arabia, Email [email protected]
Background: RSV is a common seasonal cause of respiratory infections in children and potentially adults and is considered a major cause of mortality and morbidity. While several studies on RSV have been conducted in Saudi Arabia, none have specifically focused on the southwestern region, where distinct climatic and demographic factors may influence RSV pattern. The current study aims to describe five years of experience with RSV cases among hospitalized patients and factors associated with intensive care admission from a tertiary hospital.
Materials and Methods: The study adopts a retrospective observational design, focusing on suspected respiratory infection cases confirmed by rapid RSV antigen tests from 2015 to 2020. Data including age, sex, comorbidities, and outcomes were collected from a tertiary hospital’s medical records and microbiology laboratory files. Data were analyzed using a t-test and chi-square test.
Results: Among 195 participants, primarily pediatric, monthly, and yearly admissions varied. Monthly variations revealed a U-shaped pattern with most cases reported during January, with a decline in 2020. Oxygen support was required for 40% of cases, and comorbidities were observed in 49.23%. Associations between ICU admission and factors like age, gestational age, ventilation, comorbidities, and length of stay were significant.
Conclusion: RSV infection is one of the important causes of morbidity and intensive care admission among infants and young children in Saudi Arabia. As reported by others, the seasonality of RSV is evident. Despite higher prevalence in a younger population, physicians should consider RSV in adults and older patients. Further national studies are required for a better estimation of the RSV burden on the country.
Keywords: RSV, respiratory infections, children, Saudi Arabia, Jazan
Introduction
Respiratory Syncytial Virus (RSV) is a predominant cause of lower respiratory tract infections in children and less commonly adults, posing a significant public health burden and exerting a substantial impact both within Saudi Arabia and globally.1–8 By the age of 2 years, a staggering 90% of respiratory infections can be attributed to RSV, with the peak incidence occurring between 6 weeks and 6 months of age.9,10 The seasonality of RSV infections is reported and linked to regional weather patterns, actively spreading during cold months in areas characterized by a temperate climate while persisting throughout the year in regions with tropical climates.2,8,9 In the United States, RSV infection rates were documented at 68.8 per 100 child years in infancy and 82.6 per 100 child years in the second year of life.10
The primary immune response against RSV involves the production of neutralizing antibodies and T-cell-specific immunity.1 However, repeated infections are common across all age groups and do not provide lasting immunity against subsequent infections.2 Globally, approximately 34 million cases of annual acute lower respiratory tract infections are linked to RSV, with 3.4 million cases severe enough to warrant hospitalization.9 Among hospitalized patients, 66,000 deaths have been associated with RSV, particularly affecting children at 2 years of age and those residing in developing countries.9
Various risk factors exacerbate RSV-associated complications and potentially intensive care admission, including congenital heart disease, congenital pulmonary malformations, prematurity, chronic lung disease, and neuromuscular disease.1,5,6,11 Additional risk factors for hospitalization encompass infants below 6 months of age, male gender, children residing in shared households or attending daycare centers, and exposure to tobacco smoke.1,5,6,11 Clinically, RSV presentations include rhinitis, cough, and fever.3 While croup may occur with RSV infection, bronchiolitis, and pneumonia emerge as the predominant manifestations in children.3,5,6 Noteworthy predictors for admission of bronchiolitis cases include prematurity, a history of atopic conditions, chronic lung disease, passive smoking, age less than one year, and lack of exclusive breastfeeding.6
While numerous studies have been conducted in Saudi Arabia to explore the epidemiology of RSV,2–8 none of these studies focused on the southwestern part of the country, where approximately 2 million people reside. This 5-year study aims to fill this gap by investigating RSV epidemiology among hospitalized patients in the southwestern region of Saudi Arabia. The study also aims to identify associated risk factors that could lead to intensive care admission. Providing insights that could inform targeted public health interventions, resource allocation, and clinical management strategies in the region.
Materials and Methods
Study Design and Population
We conducted a retrospective observational study to assess the epidemiology of RSV from January 2015 to December 2020. Our study included hospitalized cases with suspected respiratory infections from all ages, where laboratory results confirmed the presence of RSV using rapid tests. Cases involving other causative agents or repeated RSV-positive tests were excluded.
Data Collection
Data were sourced from the medical records and microbiology laboratory files of a 500-bed tertiary hospital and routinely collected by the infection control team. We extracted all positive RSV results for the BinaxNOW™ RSV Card (Abbott, ME, USA) rapid test, performed on nasopharyngeal swab specimens, a test with a specificity and sensitivity of 93% according to the manufacturer. Comprehensive biographical information, including age and sex, was gathered. Clinical data, such as the timing and month of clinical presentation, delivery details, term of birth (full-term or preterm), comorbidities, a requirement for oxygen support, admission to the intensive care unit (ICU), and outcomes (survival or mortality), were recorded.
Data Analysis
The data underwent cleaning and coding procedures. The study’s findings were summarized using frequencies and proportions. To compare variables associated with ICU admission, T-test and chi-square tests were employed in the data analysis process using SPSS version 23 (IBM Corp., Armonk, NY, USA).
Ethical Considerations
The study received ethical approval from the Health Ethics Committee in Jazan, Saudi Arabia. Confidentiality of collected data was rigorously maintained. This secondary analysis utilized routinely collected anonymized monitoring data in adherence to ethical principles outlined in the Helsinki Declaration and specific guidelines established by the National Committee of Bioethics in Saudi Arabia. Patient charts and laboratory databases provided data as part of routine clinical procedures, with personal and identifiable details systematically excluded. Informed consent was waived due to the retrospective nature of the study.
Results
Among 1553 participants with RSV tests, the study included a total of 195 participants with RSV-positive cases, with a mean age of 21.28 months (SD = 33.25) (Table 1). Only three adult cases were found to be tested for RSV, and results were negative. Figure 1 represents the distribution of percentages of RSV across the studied years with the highest incidence observed in the year 2019, followed by years 2016 and 2018. In Figure 2, the monthly incidence is depicted in each given year or collectively with a higher incidence between December and January. Figure 3 describes the most common comorbidities associated with RSV infection. The distribution by sex revealed 85 males (43.59%) and 107 females (54.87%). Gestational age analysis indicated 159 participants were born full-term (81.54%), while 33 were preterm (16.92%). Monthly admissions varied, with January having the highest at 43 (22.05%) and September, August, and November having the lowest at 3 each (1.54%). The study lasted multiple years, with the highest representation in 2016 (43 participants, 22.05%) and the lowest in 2017 (18 participants, 9.23%). Ventilation was required for 78 cases (40.00%), and comorbidities were observed in 96 participants (49.23%) [Figure 3]. Outcomes included 175 discharges (89.74%) and 17 deaths (8.72%). Most deaths (14 cases) were among patients with a full-term birth history. Ten out of 17 cases had associated comorbidities, mainly congenital heart diseases (5 cases) followed by cerebral palsy (4 cases). Abnormal liver function tests (LFT) were reported in 30 cases (15.38%). The average length of stay (LOS) was 8.1 days (SD = 12.88), and 62 participants (31.79%) required ICU admission.
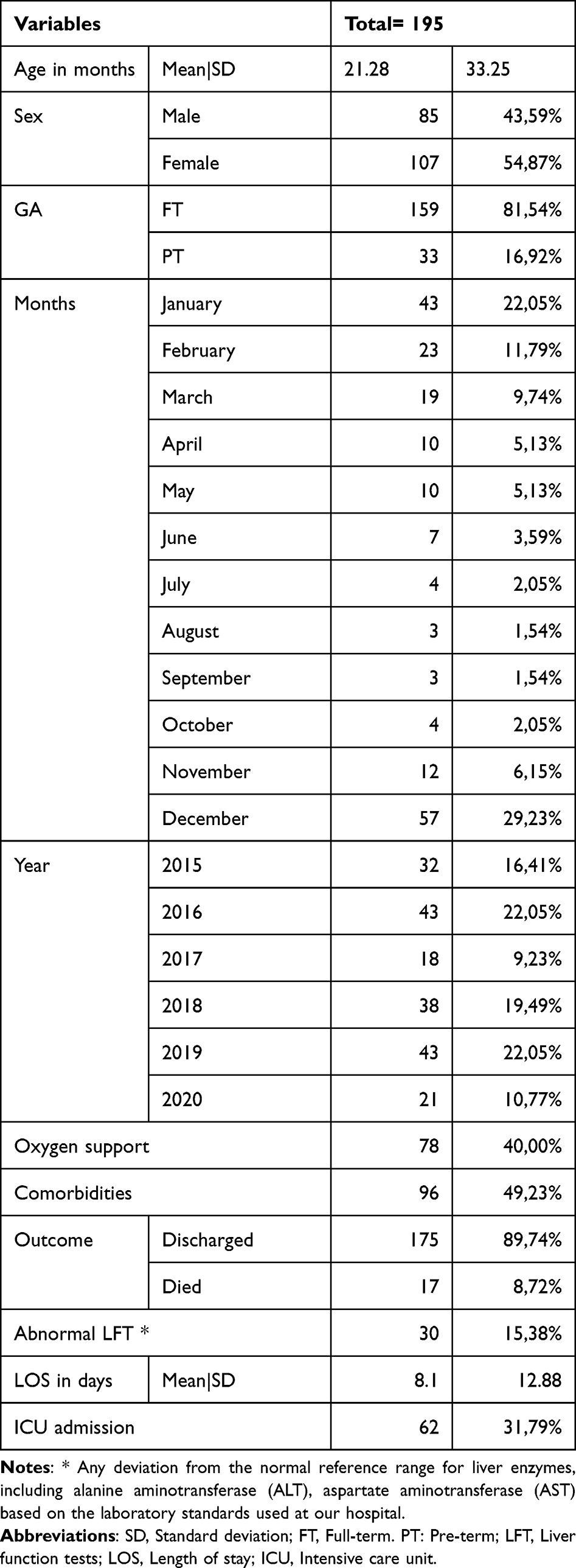 |
Table 1 Characteristics of the Included Population |
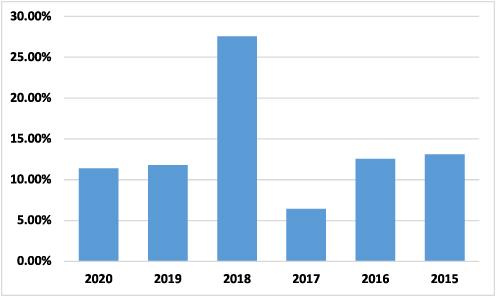 |
Figure 1 Distribution of RSV cases during the studied years. |
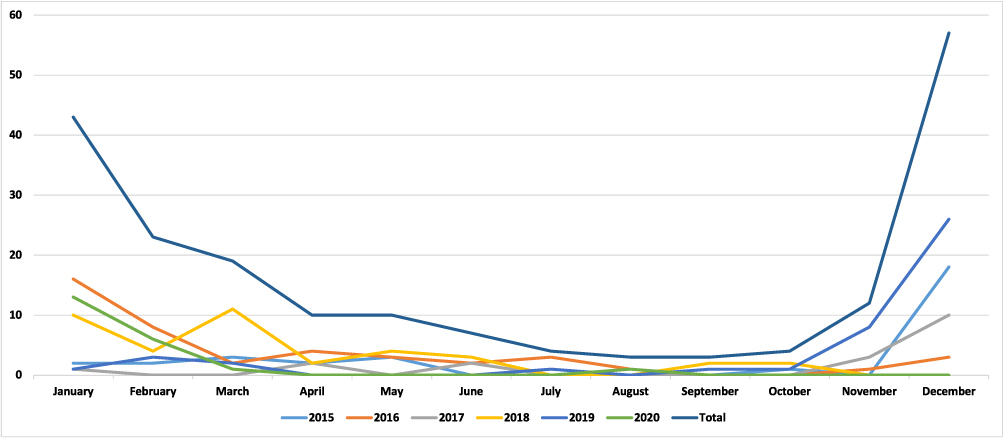 |
Figure 2 Number of RSV cases during the months of the studied period. |
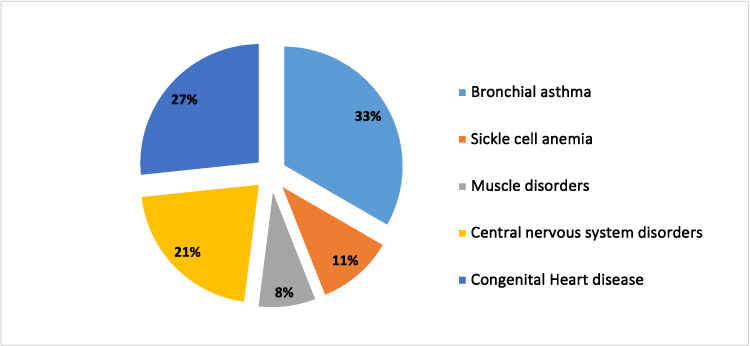 |
Figure 3 Description of the comorbidities associated with RSV cases. |
Among patients categorized based on ICU admission, those admitted had a significantly lower mean age than those not admitted (34.03 vs 41.96, p-value = 0.0001) (Table 2). Gender distribution did not show a significant difference between the two groups (p-value = 0.121). Full-term births were more prevalent among patients not admitted to the ICU (89.31% vs 66.13%, p-value = 0.0001), while preterm births were more common among ICU-admitted patients (9.92% vs 32.26%, p-value = 0.0001). Monthly variations revealed significant differences in several months, such as January (p-value = 0.001), with higher admissions in December for the ICU group. The distribution across years also showed statistically significant differences (p-value = 0.0001), with higher ICU admissions in 2016 and 2018. Ventilation was required more frequently for ICU-admitted patients (90.32% vs 16.79%, p-value = 0.0001). The presence of comorbidities (64.52% vs 16.03%, p-value = 0.005), abnormal liver function tests (35.48% vs 29.77%, p-value = 0.0001), and longer mean length of stay (12.13 vs 11.31 days, p-value = 0.003) were significantly associated with ICU admission. However, sex distribution did not exhibit statistically significant differences between the two groups.
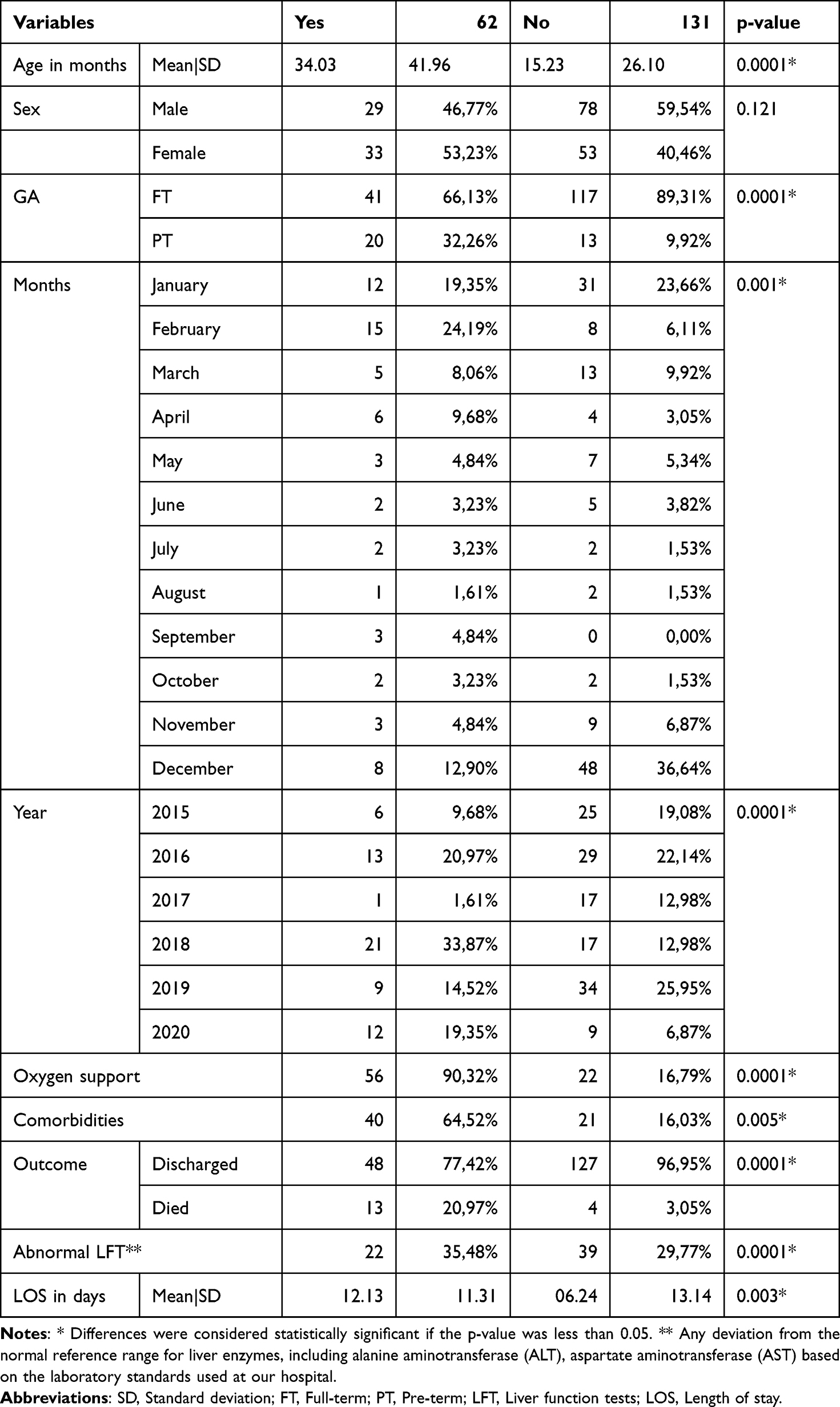 |
Table 2 Patients Categorized Based on ICU Admission |
Discussion
This 5-year study elucidates the epidemiological patterns of RSV among hospitalized patients within the Jazan region of Saudi Arabia from 2015 to 2020. It provides significant insights into the prevalence and characteristics of RSV-positive cases, offering a comprehensive analysis of demographic distribution, comorbidities, outcomes, and seasonal variations in RSV infections.2,8,9 Furthermore, this study will serve as a valuable database for future research, facilitating interventions, exploring alternative diagnostic modalities, and supporting national analyses of respiratory infections caused by RSV.
Among the 195 patients identified as RSV-positive during the study period, a notable overall prevalence of 12.5% was observed, with 54.87% being female and an average age of 21.28 months. Interestingly, 81.54% had no history of prematurity, while 16.92% did. The study delineated specific high-risk cohorts, including preterm infants born before 29 weeks, individuals with chronic lung diseases of prematurity, congenital heart diseases, and those with underlying immune deficiency.1,5,6 The spectrum of comorbidities within the study population was diverse, with 13% exhibiting a suggestive history of bronchial asthma, 10.2% having underlying congenital heart diseases, and smaller proportions manifesting central nervous disorders, sickle cell anemia, and musculoskeletal disorders.
Contrary to recent reports in various international studies, no positive RSV cases were recorded in hospitalized adult patients, despite the established prevalence of RSV infections in adults.11,12 This observation raises speculation regarding potential factors inherent in the local setting, such as a shortage of tests to be conducted in the emergency rooms, which are mostly initiated based on test requests from treating physicians or non-admitted RSV-positive cases in adults. Thus, clinicians and treating physicians in our region are urged to consider RSV as a potential differential diagnosis in adults and older patients presenting with respiratory infection manifestations. It has been reported that among patients aged over 65 years, RSV positivity could be noted in about 20% of those hospitalized with other risk factors.11,12
Among other factors associated with ICU admission, the U-shape of seasonal variations for RSV infections is well established and observed in the current study in Jazan. Furthermore, following a relatively calm RSV season in 2020 attributed to the SARS-CoV-2 pandemic, outbreaks were observed in subsequent seasons, notably in 2018–2019, as reported by others.13–16 However, this study lacks further serotyping details that could explain this observation. The RSV cases in Jazan witnessed a significant decline after the enforcement of quarantine measures in March 2020. The region’s distinctive climate, characterized by a combination of tropical and temperate weather, likely accounts for the year-round persistence of infections, with peaks occurring during colder months.17 Additionally, the median duration of hospital stay for RSV cases in Jazan was 8 days in the general population and 12 days in patients admitted to the ICU, aligning with other national findings from Riyadh, Saudi Arabia, and several European countries.7,8,18–22 Remarkably, RSV emerged as the most prevalent cause of hospitalization among children in their first year of life,21–23 and among the admitted patients, 31.79% necessitated intensive care, 40% required oxygen support or ventilation, and unfortunately, 8.72% succumbed to death.24,25
Given the retrospective nature of this study and its reliance on rapid RSV antigen tests, it is imperative to recognize the need for future investigations that encompass clinical signs, radiological findings, serotyping, and, most importantly, molecular methods to confirm the diagnosis. It is also essential to consider the impact of preventive measures or vaccination in the Jazan region during the COVID-19 pandemic.26–28 Further, recent global research has shown that the epidemiology of RSV has undergone significant changes, particularly following the COVID-19 pandemic, with altered patterns of seasonality and transmission being reported.29,30 In charting future directions, building upon the foundation laid by this 5-year study on RSV in the Jazan region is crucial. Subsequent investigations should seek the details of clinical signs and radiological findings, utilizing molecular methods and newly emerged syndromic tests to enhance diagnostic accuracy. The absence of positive RSV cases in adults, despite their documented prevalence, highlights the importance of focused research on this demographic, exploring potential factors influencing test requests and guidelines related to admission practices. Additionally, national efforts should be directed toward understanding the impact of preventive measures and vaccinations,18 which are crucial for mitigating the burden of RSV infections. By embracing a holistic approach encompassing both clinical and molecular dimensions, future studies can deepen our understanding of RSV dynamics in our region, offering invaluable insights to inform targeted interventions and contribute to the broader discourse on respiratory health in the region.
Conclusions
In conclusion, this five-year study on RSV among hospitalized individuals in Jazan, Saudi Arabia, from 2015 to 2020 provides valuable insights into demographics and outcomes of the infection. Identifying high-risk groups, with an overall prevalence of 12%, and noting with the absence of adult cases indicates critical considerations. The study serves as a foundational platform for future research, highlighting the importance of heightened clinical awareness, comprehensive diagnostics, and molecular investigations. The observed seasonal patterns and the impact of quarantine measures offer a contextual understanding of the variations in RSV throughout the studied years. Subsequent studies should cover molecular aspects, assess preventive measures, and focus on factors influencing adult cases to further enrich our understanding of RSV dynamics in the region.
Data Sharing Statement
The data presented in this study are available on request from the first author.
Institutional Review Board Statement
The study was approved by the Jazan Health Ethics Committee (REC) at the Ministry of Health.
Author Contributions
Nabil S Dhayhi and Ali Aqeel shared first authorship. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare no conflicts of interest.
References
1. Aikphaibul P, Theerawit T, Sophonphan J, Wacharachaisurapol N, Jitrungruengnij N, Puthanakit T. Risk factors of severe hospitalized respiratory syncytial virus infection in tertiary care center in Thailand. Influenza Other Respir Viruses. 2021;15:64–71. doi:10.1111/irv.12793
2. Alkharsah KR. The scope of respiratory syncytial virus infection in a tertiary hospital in the Eastern Province of Saudi Arabia and the change in seasonal pattern during and after the COVID-19 pandemic. Medicina. 2022;58:1623. doi:10.3390/medicina58111623
3. Alharbi A, Alqwaiee M, Al-Hindi M, et al. Bronchiolitis in children: the Saudi Initiative of Bronchiolitis Diagnosis, Management, and Prevention (SIBRO). Ann Thorac Med. 2018;13:127. doi:10.4103/atm.atm_60_18
4. Ahmed A, Parveen S, Al-Hassinah SM, Al-Amery SF. An overview of respiratory syncytial virus infections in Saudi Arabia. J Infect Dev Ctries. 2018;12:929–936. doi:10.3855/jidc.10736
5. Osman S, Alaa Adeen A, Hetta O, et al. Epidemiology and risk factor analysis of children with bronchiolitis admitted to the intensive care unit at a tertiary care center in Saudi Arabia. Children. 2023;10:646. doi:10.3390/children10040646
6. Al-Shehri MA, Sadeq A, Quli K. Bronchiolitis in Abha, Southwest Saudi Arabia: viral etiology and predictors for hospital admission. West Afr J Med. 2006;24. doi:10.4314/wajm.v24i4.28193
7. Amer HM, Alshaman MS, Farrag MA, Hamad ME, Alsaadi MM, Almajhdi FN. Epidemiology of 11 respiratory RNA viruses in a cohort of hospitalized children in Riyadh, Saudi Arabia. J Med Virol. 2016;88:1086–1091. doi:10.1002/jmv.24435
8. Albogami SS, Alotaibi MR, Alsahli SA, Masuadi E, Alshaalan M. Seasonal variations of respiratory viruses detected from children with respiratory tract infections in Riyadh, Saudi Arabia. J Infect Public Health. 2018;11:183–186. doi:10.1016/j.jiph.2017.06.001
9. Chadha M, Hirve S, Bancej C, et al. Human respiratory syncytial virus and influenza seasonality patterns—early findings from the WHO global respiratory syncytial virus surveillance. Influenza Other Respi Viruses. 2020;14:638–646. doi:10.1111/irv.12726
10. Centers for Disease Control and Prevention. Respiratory Syncytial Virus Infection (RSV). Available from: https://www.cdc.gov/rsv/index.html.
11. Boattini M, Almeida A, Christaki E, et al. Severity of RSV infection in Southern European elderly patients during two consecutive winter seasons (2017–2018). J Med Virol. 2021;93:5152–5157. doi:10.1002/jmv.26938
12. Walsh E, Lee N, Sander I, et al. RSV-associated hospitalization in adults in the USA: a retrospective chart review investigating burden, management strategies, and outcomes. Health Sci Rep. 2022;5:e556. doi:10.1002/hsr2.556
13. Di Mattia G, Nenna R, Mancino E, et al. During the COVID‐19 pandemic where has respiratory syncytial virus gone? Pediatr Pulmonol. 2021;56:3106–3109. doi:10.1002/ppul.25582
14. Vakrilova L, Nikolova SH, Slavov S, Radulova P, Slancheva B. An outbreak of RSV infections in a neonatology clinic during the RSV-season. BMC Pediatr. 2021;21. doi:10.1186/s12887-021-03053-9
15. Eden J-S, Sikazwe C, Xie R, et al. Off-season RSV epidemics in Australia after easing of COVID-19 restrictions. Nat Commun. 2022;13. doi:10.1038/s41467-022-30485-3
16. Ren L, Lin L, Zhang H, et al. Epidemiological and clinical characteristics of respiratory syncytial virus and influenza infections in hospitalized children before and during the COVID‐19 pandemic in Central China. Influenza Other Respir Viruses. 2023;17. doi:10.1111/irv.13103
17. Löwensteyn YN, Zheng Z, Rave N, et al. Year-round respiratory syncytial virus transmission in the Netherlands following the COVID-19 pandemic: a prospective nationwide observational and modeling study. J Infect Dis. 2023;228:1394–1399. doi:10.1093/infdis/jiad282
18. Mulot G, Benchaib M, Plaisant F, et al. Risk factors of very severe RSV infections in a multicenter cohort of very preterm and extreme preterm babies receiving or not palivizumab. Front Pediatr. 2022;10:884120. doi:10.3389/fped.2022.884120
19. Del Riccio M, Spreeuwenberg P, Osei-Yeboah R, et al. Burden of respiratory syncytial virus in the European Union: estimation of RSV-associated hospitalizations in children under 5 years. J Infect Dis. 2023;228:1528–1538. doi:10.1093/infdis/jiad188
20. Diggikar S, Paul A, Razak A, Chandrasekaran M, Swamy RS. Respiratory infections in children born preterm in low and middle‐income countries: a systematic review. Pediatr Pulmonol. 2022;57:2903–2914. doi:10.1002/ppul.26128
21. Hartmann K, Liese JG, Kemmling D, et al. Clinical burden of respiratory syncytial virus in hospitalized children aged ≤5 years (INSPIRE study). J Infect Dis. 2022;226:386–395. doi:10.1093/infdis/jiac137
22. Gea-Izquierdo E, Gil-Prieto R, Hernández-Barrera V, Gil-de-Miguel Á. Respiratory syncytial virus-associated hospitalization in children aged <2 years in Spain from 2018 to 2021. Hum Vaccin Immunother. 2023;19. doi:10.1080/21645515.2023.2231818
23. Kaler J, Hussain A, Patel K, Hernandez T, Ray S. Respiratory syncytial virus: a comprehensive review of transmission, pathophysiology, and manifestation. Cureus. 2023. doi:10.7759/cureus.36342
24. Reichert H, Suh M, Jiang X, et al. Mortality associated with respiratory syncytial virus, bronchiolitis, and influenza among infants in the United States: a birth cohort study from 1999 to 2018. J Infect Dis. 2022;226:S246–S254. doi:10.1093/infdis/jiac127
25. Blau DM, Baillie VL, Els T, et al. Deaths attributed to respiratory syncytial virus in young children in high-mortality rate settings: report from Child Health and Mortality Prevention Surveillance (CHAMPS). Clin Infect Dis. 2021;73:S218–S228. doi:10.1093/cid/ciab509
26. Algaissi AA, Alharbi NK, Hassanain M, Hashem AM. Preparedness and Response to COVID-19 in Saudi Arabia: building on MERS Experience. J Infect Public Health. 2020;13:834–838. doi:10.1016/j.jiph.2020.04.016
27. Alhazmi A, Alamer E, Abdelwahab S, et al. Community-Based Seroprevalence of SARS-CoV-2 Antibodies following the First Wave of the COVID-19 pandemic in Jazan Province, Saudi Arabia. Int J Environ Res Public Health. 2021;18:12451. doi:10.3390/ijerph182312451
28. Albeladi FI, Alluli MM, Daghriri KA, et al. Level of adherence to COVID-19 preventive measures among health care workers in Saudi Arabia. Cureus. 2021;13:e15969. doi:10.7759/cureus.15969
29. Milani GP, Ronchi A, Agostoni C, et al. Correction to: long-lasting effects of COVID-19 pandemic on hospitalizations and severity of bronchiolitis. Eur J Pediatr. 2024;183:4589–4591. doi:10.1007/s00431-024-05707-z
30. Presti S, Manti S, Gammeri C, Parisi GF, Papale M, Leonardi S. Epidemiological shifts in bronchiolitis patterns and impact of the COVID-19: a two-season comparative study. Pediatr Pulmonol. 2024;59:1298–1304. doi:10.1002/ppul.26904
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Quality of Life and the Presence of Depression Among Adults with Hair Loss in the South of Saudi Arabia
Alomaish AR, Gosadi IM, Dallak FH, Darraj AI, Jaafari SM, Alshamakhy AE, Mleeh NT
Psychology Research and Behavior Management 2022, 15:1989-1996
Published Date: 4 August 2022
Factors Affecting Awareness of Pregnancy Screening for Group B Streptococcus Infection Among Women of Reproductive Age in Jazan Province, Saudi Arabia
Zoli SI, Baiti MA, Alhazmi AA, Khormi RM, Sayegh MA, Altubayqi T, Darisi AM, Alhasani RA, Alhazmi SH, Gharawi SO, Muhajir AA, Alhazmi AH
Journal of Multidisciplinary Healthcare 2023, 16:2109-2116
Published Date: 26 July 2023
Nutritional Status and Dietary Behaviors of Children with Intellectual or Developmental Disabilities in Saudi Arabia: A Systematic Review
AlFaris NA, Alshwaiyat NM, ALTamimi JZ, Alagal RI, AlSalehi SM, Al Zarah RI, Alfaiz RF, Alhariqi AI, Alshamri DF, AlSouan NA, AlMousa LA
Journal of Multidisciplinary Healthcare 2024, 17:3371-3399
Published Date: 12 July 2024
Oral Cavity Microbiome Impact on Respiratory Infections Among Children
Crestez AM, Nechita A, Daineanu MP, Busila C, Tatu AL, Ionescu MA, Martinez JD, Debita M
Pediatric Health, Medicine and Therapeutics 2024, 15:311-323
Published Date: 9 October 2024
Serum Vitamin D Profiles of Children with Asthma in Southwest Saudi: A Comparative Cross-Sectional Study
Asseri AA
International Journal of General Medicine 2024, 17:6323-6333
Published Date: 17 December 2024