")
Back to Journals » Psychology Research and Behavior Management » Volume 15
Quality of Life and the Presence of Depression Among Adults with Hair Loss in the South of Saudi Arabia
Authors Alomaish AR , Gosadi IM , Dallak FH , Darraj AI, Jaafari SM, Alshamakhy AE , Mleeh NT
Received 18 May 2022
Accepted for publication 8 July 2022
Published 4 August 2022 Volume 2022:15 Pages 1989—1996
DOI https://doi.org/10.2147/PRBM.S375247
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Abeer R Alomaish,1 Ibrahim M Gosadi,2 Fatimah H Dallak,1 Atheer I Darraj,1 Shatha M Jaafari,1 Arar E Alshamakhy,3 Nouf T Mleeh4
1Faculty of Medicine, Jazan University, Jazan, Saudi Arabia; 2Department of Family and Community Medicine, Faculty of Medicine, Jazan University, Jazan, Saudi Arabia; 3Department of Dermatology, at Prince Muhammad Bin Nassir Hospital, Jazan, Saudi Arabia; 4Department of Dermatology, Faculty of Medicine, King Abdul-Aziz University, Jeddah, Saudi Arabia
Correspondence: Ibrahim M Gosadi, Faculty of Medicine, Jazan University, P.O. Box 2349, Jazan, 82621, Saudi Arabia, Tel +966562137711, Email [email protected]
Purpose: This study aims to measure quality of life and the presence of depression among adults suffering from perceived hair loss.
Methods: This study used a cross-sectional design that targeted adult subjects with perceived hair loss in the Jazan region of Saudi Arabia. Data were collected during interviews in selected primary healthcare centers. Data pertaining to the demography, quality of life, and presence of depression in participants were collected. Quality of life was assessed via a modified Arabic version of the Dermatology Life Quality Index (DLQI). The presence of depression was assessed via Patient Health Questionnaire-9 (PHQ-9). A chi-squared test was used to detect statistically significant differences between the levels of quality of life and depression and the measured demographic characteristics.
Results: A total of 483 subjects reported having hair loss. The median age of the sample was 30 years. The majority of the respondents were female (74.5%) and had university-level education (71.4%). Only 169 (35%) reported seeking medical advice concerning their hair loss. The effect of hair loss on quality of life score varied between 2 and 29, with a median score of 6. The median depression level was 6, and the level varied between 0 and 27. Gender, education level, seeking medical care due to hair loss, and worsening of hair loss seem to have an impact on quality of life and depression levels (p values < 0.05).
Conclusion: Nearly half of the sample experienced a more than moderate impact on their quality of life induced by their perceived hair loss. Additionally, more than half of the sample exhibited moderate or stronger levels of depression. Encouraging subjects with perceived hair loss to seek medical advice concerning their hair loss may result in early identification, appropriate diagnosis, and the use of curative measures, may consequently improving patients’ quality of life and preventing depression.
Keywords: quality of life, depression, hair loss, Jazan, Saudi Arabia
Introduction
Alopecia (hair loss) is a chronic dermatological condition that can be caused by several factors and can occur in any part of the body.1,2 There are several types of hair loss caused by underlying health conditions, hormonal or pharmacological agents, or nutritional deficiencies.3–6 Hair loss can have a psychological impact and influence the overall quality of life of those who are suffering from the condition.
Due to its disfigurement, hair loss can affect an individual’s sense of self, leading to anxiety and depression. Hair loss may cause low self-esteem, affect job performance, and have an adverse effect on a person’s social life.7–9 Furthermore, the limited effectiveness of medications and the failure to find a cure can create further psychological consequences.2
The prevalence of hair loss in a population can be influenced by the demographics and health characteristics of that population. Studies that measure the prevalence of hair loss in Saudi Arabia are mainly limited to an assessment of the prevalence of alopecia areata, an autoimmune-related hair loss. Rates of alopecia areata vary between 6.5%10 and 13.8% [13].11 In a recent cross-sectional investigation conducted in southern Saudi Arabia, the prevalence of all types of hair loss among primary healthcare attendees was 66.3%. The most frequently reported type of alopecia was telogen effluvium, followed by androgenic alopecia.12
Studies that assess the impact of hair loss on quality of life are limited. Two studies have assessed the impact of alopecia areata on quality of life in Saudi Arabia. They reported a statistically significant poorer quality of life among female patients, those with higher incomes, and those with body alopecia areata (p < 0.05).13 Furthermore, in a study by Mubki et al that recruited a sample of 100 patients with alopecia areata from Riyadh, Saudi Arabia, lower quality of life was associated with higher severity of the disease.14 Finally, in a study that involved 207 patients from Riyadh who had been diagnosed with androgenic alopecia, female patients were more likely to suffer reduced quality of life compared with male patients.15
Studies that assess the psychological impact of hair loss in Saudi Arabia are currently lacking. Furthermore, studies that assess quality of life among subjects with hair loss in southern Saudi Arabia are currently lacking. This study aims to measure quality of life and the potential impact of perceived hair loss. Furthermore, this study aims to assess the presence of depression among adults who are suffering from perceived hair loss in southern Saudi Arabia.
Methods
Study Design and Settings
This study used a cross-sectional design that targeted adult subjects with perceived hair loss in the Jazan region of Saudi Arabia. Data were collected in selected primary healthcare centers between August 1st and October 31st, 2020. The study was performed after securing ethical approval from the Jazan Health Ethics Committee (approval number 2018, dated April 2020). Subjects were recruited after securing their informed consent, and the study was performed in accordance with the Declaration of Helsinki.
Data Collection Process
Data were collected via a semi-structured questionnaire that measured variables related to the demography of the participants, their quality of life, and the presence of depression. The demographic section asked participants their age, gender, education level, employment, marital status, height, weight, disease history, and smoking history. Quality of life was assessed via the Arabic version of the Dermatology Life Quality Index (DLQI), which is a validated questionnaire that measures health-related quality of life among patients suffering from dermatological conditions. The questionnaire and its validity are described elsewhere.16 However, due to the nature of our investigation, the wording “skin” originally used in the DLQI was described as “scalp” in questionnaire item number one, and “hair” loss’ in the remaining items to assess the impact of hair loss on quality of life among the recruited participants. The presence of depression was assessed via Patient Health Questionnaire-9 (PHQ-9), which is a validated nine-question survey that is used to assess the level of depression, especially with the presence of symptoms that influence patients’ lives. The questionnaire and its validity are described elsewhere.17 The data collection tool was piloted on a sample of 10 participants to test the clarity of the questions for the studied community and the time needed to complete the recruitment.
Convenient sampling was used to recruit the participants among attendees of 23 randomly selected primary healthcare centers out of the 170 primary healthcare centers in Jazan. A screening question was used to identify individuals with perceived hair loss. The screening question asked the potential participants whether they perceived themselves to have a history of hair loss. Data were collected during interviews with subjects who met the inclusion criteria. Adult subjects who reported having hair loss and agreed to participate were included in the current investigation. Those with no reported history of hair loss or who did not agree to participate in the study were excluded.
Data Analysis
Data analysis was conducted with Statistical Package for the Social Sciences software (version 25). Data were summarized using frequencies and proportions for binary and categorical variables. Scoring of the DLQI was based on a four-point Likert scale, which is described elsewhere.18 Similarly, the PHQ-9 scoring is based on a four-point Likert scale. A description of the scoring and categorization of depression levels can be found elsewhere.17 To enable comparison between study groups, the DLQI was grouped into subjects with little or no effects and those with moderate or high effects. Similarly, subjects with minimal depression levels based on the PHQ-9 scores were compared to those with higher depression levels. A chi-squared test was used to detect statistically significant differences between the levels of quality of life and depression and the measured demographic characteristics.
Results
Among the 744 primary healthcare attendees who were approached, 483 subjects reported having a history of perceived hair loss. Table 1 describes the demographic characteristics of the recruited sample. The majority of the respondents were female (74.5%), had university-level education (71.4%), were not employed (59.6%), and were never smokers (84.9%). The sample was nearly equally distributed with regard to marital status. The median age of the sample was 30 years. Only 27.7% of the sample reported being diagnosed with a chronic disease, while 45.8% of the sample were either overweight or obese. Among this sampling of adults who believed they had hair loss, only 169 (35%) reported seeking medical advice concerning their hair loss. Finally, 36% of the sample reported a progressive worsening of their hair loss since its onset.
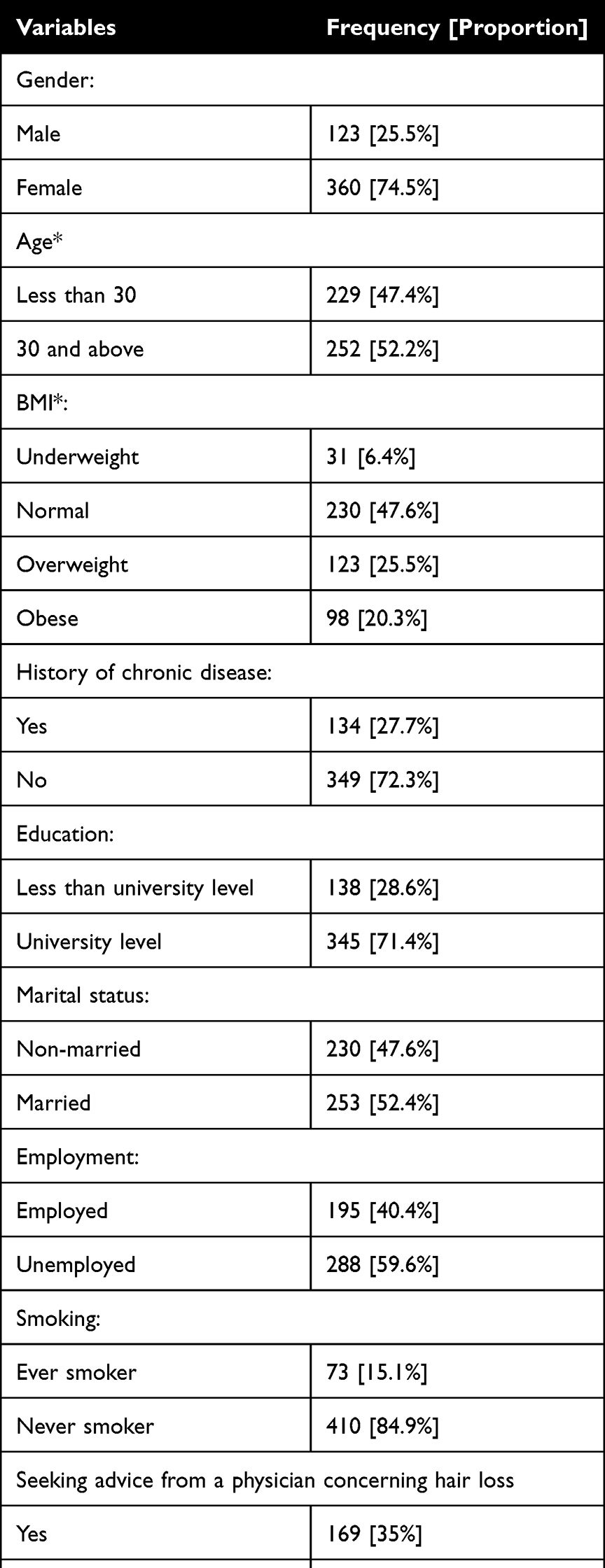 |
Table 1 Demographic Characteristics of 483 Subjects with Perceived Hair Loss from Jazan, Saudi Arabia |
The participants’ responses to the DLQI questionnaire showed that the effect of hair loss on quality of life varied between 2 and 29, with a median score of 6. This shows that hair loss had a moderate or high impact on quality of life among more than half of the sample (55.2%). The proportions of participants who responded with high impact of hair loss on quality of life (by selecting “very much” as a response to the DLQI items) varied between 2.1% and 10.4%.
The proportions of the participants who responded with “very much” when describing the impact of hair loss on quality of life were the highest when the participants described being embarrassed or self-conscious by hair loss (10.4%), followed by impact on clothing options (8.3%) and interference with activities such as shopping or looking after home or garden (7%). Additionally, 6.4% of the participants responded with “very much” when describing suffering scalp itchiness or pain.
Lower impact of hair loss was detected among the other quality of life items. The proportion of participants who responded with “very much” when describing the impact on relationships with partner, friends or relatives was 4.8%. Furthermore, 3.7% of the participants responded with “very much” when describing the impact of hair loss treatments on their homes or taking up time. 3.5% of the sample responded with “very much” when describing the impact of hair loss on social or leisure activities.
The lowest impact of hair loss among the recruited sample was related to sporting activities, work or studying, and on sexual activities. 2.7% and 2.5% of the sample responded with “very much” when describing the impact of hair loss on work or studying and sporting activity respectively. Finally, the smallest impact was identified concerning impact of hair loss on sexual activities, where only 2.1% responded with “very much”.
Responses to the PHQ-9 questionnaire are displayed in Table 2. The median depression level was 6, and the level varied between 0 and 27. Categorization of the sample according to depression level indicated that 61.9% of the sample had a high level of depression that may require treatment. Among the nine items on the PHQ-9 questionnaire, the most frequently reported symptoms were sleep disturbances, fatigue, and loss of appetite.
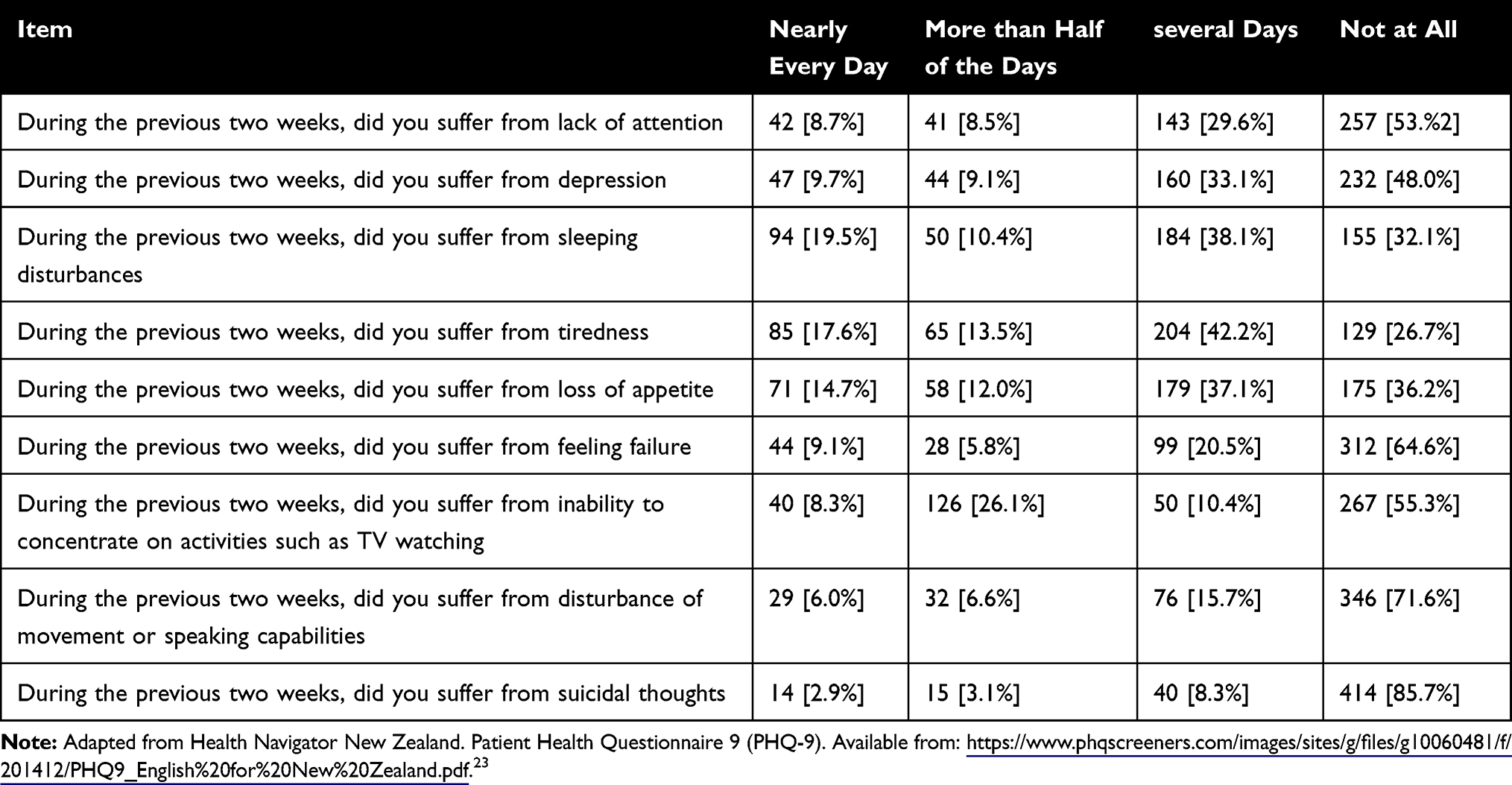 |
Table 2 Responses of 483 Subjects with Perceived Hair Loss from Jazan, Saudi Arabia, to the PHQ-9 Questionnaire |
Table 3 displays the distribution of the effect of perceived hair loss on quality of life and depression among the 483 subjects with perceived hair loss. The results of the impact of hair loss on quality of life were statistically significant for the education level, history of seeking medical care due to hair loss, and the worsening of hair loss since its commencement (p < 0.05), suggesting that those with higher education levels, those who consulted a physician due to their hair loss, and those who witnessed the worsening of their hair loss were more likely to have their quality of life affected by hair loss. The effect of marital status showed statistically marginal significance (0.06), indicating a higher effect of hair loss on quality of life among married individuals. Distribution according to depression levels indicated that female subjects, those who were unemployed, and those with worsening hair loss had higher levels of depression in comparison to male subjects, those who were employed, and those with no worsening of their hair loss (p < 0.05).
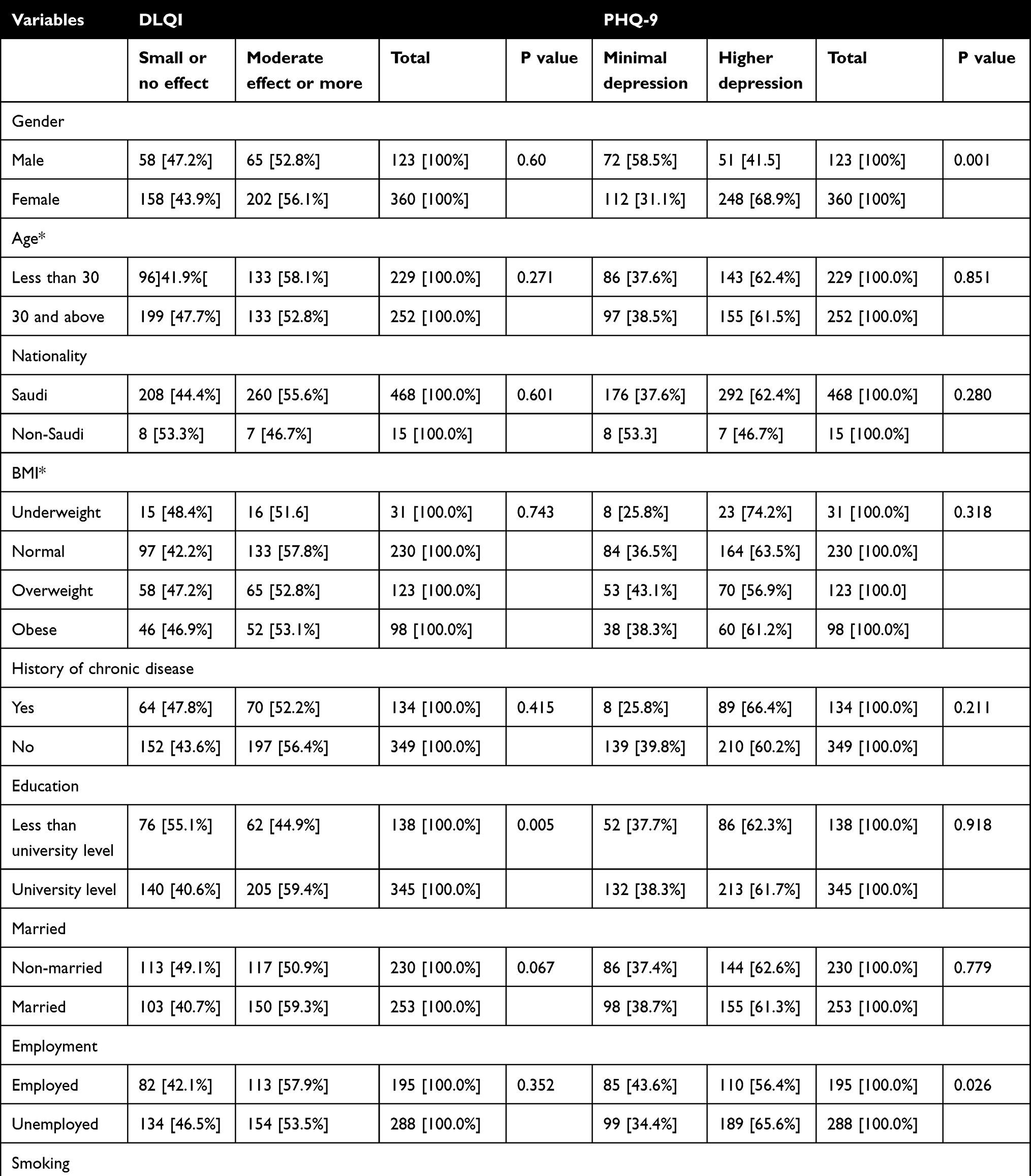 |
Table 3 The Distribution of the Levels of the Effect of Perceived Hair Loss on Quality of Life and Depression According to the Measured Demographics of 483 Subjects in Jazan, Saudi Arabia |
Discussion
This study was a cross-sectional investigation conducted in Jazan in southern Saudi Arabia to measure the impact of perceived hair loss on quality of life and depression. In this sample, perceived hair loss was reported more frequently among female subjects, those with university education, and older subjects. Assessment of the impact of alopecia on quality of life indicated that more than half of the sample suffered a moderate or stronger effect on their quality of life. Furthermore, nearly 62% of the study sample had moderate or stronger levels of depression. The results indicated that those with a higher education level, those with a history of seeking medical advice due to their hair loss, and those who reported a worsening of their hair loss were more likely to have their quality of life affected by alopecia. Female subjects, those who were not employed, and those with a history of worsening hair loss were more likely to have higher levels of depression.
The findings of the current study can be compared to similar national and international investigations. In a study by Mubki et al that recruited a sample of 207 subjects from Riyadh with androgenic alopecia, the mean score reported on the DLQI was 7.8, and the scores ranged from 0 to 29. The results of their study indicated a somewhat higher score than our study, which had a median score of 6 on the DLQI.15 However, Mubki et al found that the quality of life of female participants was more likely to be affected than male subjects, which was not detected in our sample.
In another investigation by Mubki et al that measured the impact of alopecia areata on quality of life among a sample of 100 patients from Riyadh, the mean score reported on the DLQI was 7.2, which is relatively higher than the median score identified in our sample. However, Mubki et al did not detect any association between DLQI scores and measured demographic variables among patients with alopecia areata.14
A study by Alsaiari and Fatani measured quality of life among 34 patients diagnosed with alopecia areata from Makkah, Saudi Arabia, via the Skindex-16 questionnaire.13 Alsaiari and Fatani reported that alopecia areata had an impact on quality of life, especially among single individuals and females (p < 0.05), which is different than the findings of our investigation, in which gender and marital status were not correlated with the impact of alopecia on quality of life. These variations between the findings of our investigation and similar investigations conducted in Saudi Arabia can be explained by the nature of our investigation, which was not restricted to androgenic alopecia or alopecia areata but included all types of hair loss and was mainly based on the perceived presence of hair loss rather than having a history of diagnosed alopecia.
Other international investigations provided similar findings. In a Brazilian study by Schmitt et al that was restricted to 157 women attending a dermatology clinic, it was reported that 54% of the participants reported hair loss and 29% reported symptoms of depression, suggesting that perceived hair loss can be associated with mental health.19 Although their sample was restricted to female subjects attending dermatology clinics, the findings are comparable. Higher depression levels were detected among female subjects in this sample, indicating the potential impact of perceived hair loss on increasing levels of depression, especially among female subjects.
A systematic review and meta-analysis performed by Huang et al assessed the influence of androgenic alopecia on health-related quality of life, depression, and self-esteem. Huang et al examined a total of 41 studies with 7995 patients and reported that higher self-rated hair loss severity was inversely associated with quality of life, which is similar to the findings of our investigation. However, their findings indicated that hair loss reduced the quality of life of those with a higher educational level, which is contradictory to our findings. Furthermore, Huang et al did not detect an association between androgenic alopecia and depression levels based on the pooled depression scores.20 Finally, another systematic review and meta-analysis by Okhovat et al assessed the association between alopecia areata, anxiety, and depression. Okhovat et al included eight studies with a total of 6010 patients and 20,961 controls and found higher odds ratios (OR) of anxiety and depression among those with alopecia areata in comparison to the controls (OR: 2.5, 95% confidence interval (CI): 1.54–4.06, and OR: 2.71, 95% CI: 1.52–4.82, respectively).21
The findings of our investigation and the cumulative evidence of the literature suggest an association between hair loss and quality of life and mental health. This notion can be argued to apply to those with perceived hair loss. Given the higher risk of psychological impact among those with hair loss, it is suggested that individuals suffering from hair loss be referred for consultation with a psychiatrist.22
Strengths and Limitations
Our investigation has several areas of strengths and weaknesses. The main strengths of the current investigation are related to targeting subjects who attend general primary healthcare clinics. This can provide a representative sampling for those who have perceived hair loss, especially those who have not sought medical care for their hair loss. Another strength is related to the use of personal interviews, which can increase the quality of the collected data and reduce selection and measurement bias. However, a weakness is the convenient selection of the interviewees, despite the random selection of the primary healthcare centers.
Conclusion
The majority of the subjects in our sample who believed they had hair loss were females. Nearly half of the sample showed a more than moderate impact on quality of life induced by their perceived hair loss. Additionally, more than half of the sample exhibited moderate or strong levels of depression. Gender, education level, seeking medical care due to hair loss, and worsening of hair loss seem to have an impact on quality of life and depression levels. Encouraging subjects with perceived hair loss to seek medical advice concerning their hair loss may result in the early identification of those with hair loss, the appropriate diagnosis of the conditions associated with hair loss, and the use of curative measures, consequently improving quality of life and reducing levels of depression.
Author Contributions
All authors contributed to analyzing data, drafting, or revising the article, have agreed on the journal to which the article will be submitted, have given final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Al Ahoud Am ZPM. Alopecia. Treasure Island (FL): StatPearls; 2020.
2. Hunt N, McHale S. The psychological impact of alopecia. BMJ. 2005;331(7522):951–953. doi:10.1136/bmj.331.7522.951
3. Lin RL, Garibyan L, Kimball AB, Drake LA. Systemic causes of hair loss. Ann Med. 2016;48(6):393–402. doi:10.1080/07853890.2016.1180426
4. Almohanna HM, Ahmed AA, Tsatalis JP, Tosti A. The role of vitamins and minerals in hair Loss: a review. Dermatol Ther. 2019;9(1):51–70. doi:10.1007/s13555-018-0278-6
5. Guo EL, Katta R. Diet and hair loss: effects of nutrient deficiency and supplement use. Dermatol Pract Conc. 2017;7(1):1–10. doi:10.5826/dpc.0701a01
6. Chang YJ, Lee YH, Leong PY, Wang YH, Wei JCC. Impact of rheumatoid arthritis on alopecia: a nationwide population-based cohort study in Taiwan. Front Med. 2020;7. doi:10.3389/fmed.2020.00150
7. Korta DZ, Christiano AM, Bergfeld W, et al. Alopecia areata is a medical disease. J Am Acad Dermatol. 2018;78(4):832–834. doi:10.1016/j.jaad.2017.09.011
8. Merino De Paz N, Martín-González C, Fumero Arteaga M. Psychological impact of alopecia. In: Alopecia: Risk Factors, Treatment and Impact on Quality of Life. 2020;1–20.
9. Zhang M, Zhang N. Quality of life assessment in patients with alopecia areata and androgenetic alopecia in the People’s Republic of China. Patient Prefer Adherence. 2017;11:151–155. doi:10.2147/PPA.S121218
10. Abd El-Mawla AA, Maghrabi I. Prevalence and treatment of Alopecia areata in Taif area, KSA. Saudi J Med Med Sci. 2015;4(2):125. doi:10.4103/2278-0521.157891
11. Al-ajlan A, Alqahtani ME, Alsuwaidan S, Alsalhi A. Prevalence of Alopecia Areata in Saudi Arabia: cross-sectional descriptive study. Cureus. 2020;12:9.
12. Alomaish AR, Gosadi IM, Dallak FH, et al. Prevalence of alopecia and its contributing factors among primary healthcare attendees in the Jazan region, Saudi Arabia. Fam Med Prim Care Rev. 2021;10(10):3851–3856. doi:10.4103/jfmpc.jfmpc_1070_21
13. Alsaiari S, Fatani M. Demographic and clinical profile of alopecia areata in Makkah, Saudi Arabia and it’s impact on quality of life. Int J Med Health Res. 2018;4(3):7.
14. Mubki T, Altelhab S, Alhargan A, Alnomair N, Alkhalifah A. Quality of life in patients with alopecia areata: a cross-sectional study in Saudi Arabia. Saudi Univ Med J. 2017;4(2):7.
15. Mubki T, Dayel S, AlHargan A, AlGhamdi K, AlKhalifah A. Quality of life and willingness-to-pay in patients with androgenetic alopecia. Egypt J Dermatol Venerol. 2019;39(1):31–36. doi:10.4103/ejdv.ejdv_33_18
16. Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI)–a simple practical measure for routine clinical use. Clin Exp Dermatol. 1994;19(3):210–216. doi:10.1111/j.1365-2230.1994.tb01167.x
17. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
18. Finlay AY, Khan GK. Dermatology Life Quality Index; 2019. Available from: https://www.cardiff.ac.uk/medicine/resources/quality-of-life-questionnaires/dermatology-life-quality-index.
19. Schmitt JV, Ribeiro CF, Souza FH, Siqueira EB, Bebber FR. Hair loss perception and symptoms of depression in female outpatients attending a general dermatology clinic. An Bras Dermatol. 2012;87(3):412–417. doi:10.1590/S0365-05962012000300010
20. Huang CH, Fu Y, Chi CC. Health-related quality of life, depression, and self-esteem in patients with androgenetic alopecia: a systematic review and meta-analysis. JAMA Dermatol. 2021;157(8):963–970. doi:10.1001/jamadermatol.2021.2196
21. Okhovat JP, Marks DH, Manatis-Lornell A, Hagigeorges D, Locascio JJ, Senna MM. Association between Alopecia Areata, Anxiety, and depression: a systematic review and meta-analysis. J Am Acad Dermatol. 2019. doi:10.1016/j.jaad.2019.05.086
22. Marahatta S, Agrawal S, Adhikari BR. Psychological impact of Alopecia Areata. Dermatol Res Pract. 2020;2020:8879343. doi:10.1155/2020/8879343
23. Adapted from Health Navigator New Zealand. PatientHealthQuestionnaire9(PHQ-). Available from: https://www.phqscreeners.com/images/sites/g/files/g10060481/f/201412/PHQ9_English%20for%20New%20Zealand.pdf. Accessed July 30, 2022
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.