Back to Journals » Patient Preference and Adherence » Volume 19
Factors Influencing Decision-Making and Rehabilitation Among Older Women Who Underwent Total Knee Replacement: A Qualitative Study in Taiwan
Authors Huang CH ![]() , Chen YY
, Chen YY ![]() , Chen SW
, Chen SW ![]() , Wang CT, Lin MH
, Wang CT, Lin MH
Received 21 September 2025
Accepted for publication 26 November 2025
Published 9 December 2025 Volume 2025:19 Pages 3931—3944
DOI https://doi.org/10.2147/PPA.S567269
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ramón Morillo-Verdugo
Ching Han Huang,1 Yun Yee Chen,2 Shu Wen Chen,3 Chen Ti Wang,4 Mei Hsiang Lin3
1Department of Nursing, National Taiwan University Hospital, Taipei, Taiwan; 2Department of Rehabilitation Medicine, Taipei City Hospital, Taipei, Taiwan; 3School of Nursing, National Taipei University of Nursing and Health Sciences, Taipei, Taiwan; 4Department of Orthopedic Surgery, National Taiwan University Hospital, Taipei, Taiwan
Correspondence: Shu Wen Chen, National Taipei University of Nursing and Health Sciences, School of Nursing, No. 365, Ming-Te Road, Peitou District, Taipei, 11219, Taiwan, Email [email protected] Yun Yee Chen, Department of Rehabilitation Medicine, Renai Branch, Taipei City Hospital, No. 10, 4 Section 10, Ren-Ai Road, Daan District, Taipei, 10629, Taiwan, Email [email protected]
Purpose: To explore the factors influencing decision-making and the rehabilitation experiences of older women who underwent total knee replacement (TKR).
Methods: A qualitative descriptive design with purposive sampling was employed. Women aged over 60 who had undergone TKR at a medical center in northern Taiwan were recruited during COVID-19 pandemic. Data were collected through two rounds of face-to-face interviews (3– 5 days and 6– 8 weeks post-surgery) and a follow-up telephone interview conducted 6 months after surgery. Thematic analysis was performed using a constant comparative approach.
Results: Twenty women participated. A central theme—reclaiming independent life through surgical transformation—emerged, encompassing two interrelated themes: (1) Decision-making factors were driven by pain, external concerns (becoming a burden on the family, body image change), dissatisfaction with conservative treatments, and the influence of significant others (physicians, families and friends, peers); (2) Surgical recovery involved striving to achieve the “rehabilitation golden phase” by enduring pain, establishing personal goals, and working toward functional recovery, while managing “challenges in home-based rehabilitation” through coping strategies and social support, and engaging in “post-surgical reflections” to assess pain relief and identify levels of functional recovery.
Conclusion: Older women perceived TKR to regain mobility, autonomy, and reduce dependence on family members. Their decisions reflected the interplay between physical suffering and cultural expectations. Despite rehabilitation challenges, participants demonstrated resilience and strong motivation for recovery. These findings emphasize the importance of gender-sensitive, patient-centered decision-support strategies and family-inclusive, culturally responsive rehabilitation care.
Keywords: total knee replacement, older women, decision-making, patient preference, rehabilitation, qualitative research
Introduction
Osteoarthritis (OA) is the most prevalent joint disorder and a leading cause of pain, disability, and loss of independence among older adults.1 OA is a chronic, progressive condition characterized by degeneration of articular cartilage, remodeling of subchondral bone, osteophyte formation, and varying degrees of synovial inflammation.2–4 These changes result in chronic pain, joint stiffness, and limited mobility, substantially diminishing quality of life.4–6 The knee is the most affected weight-bearing joint, making knee OA particularly disabling.4–6 Epidemiological studies indicate that knee OA contributes significantly to global musculoskeletal disability, often leading to early retirement, increased healthcare utilization, and higher socioeconomic costs.7
Management typically follows a staged approach. Conservative treatments—such as pharmacologic therapy, rehabilitation, and lifestyle modification—aim to relieve pain and preserve mobility.4,5,8 When these measures fail, total knee replacement (TKR) is regarded as the most effective and cost-efficient surgical intervention, providing substantial pain relief and functional restoration for most patients.4–6 Despite its benefits, the decision to undergo TKR is complex, particularly for older adults, as biological, psychological, and social factors intersect.9 Motivation and psychological readiness influence adherence to postoperative rehabilitation and recovery outcomes, including pain reduction, mobility, and daily functioning.9–11 Postoperative satisfaction typically depends on pain relief and functional recovery; however, multiple clinical and psychosocial factors influence these outcomes.12
In Taiwan, TKR is widely performed under the National Health Insurance (NHI) system, which ensures equitable access to surgical care.13–16 The annual number of procedures has tripled over two decades, with women accounting for nearly 70% of all cases.16 While most existing studies emphasize clinical outcomes or rehabilitation effectiveness, limited qualitative research has examined the entire trajectory from surgical decision-making through postoperative recovery.17–21 This study therefore aimed to (1) identify factors influencing older women’s preferences and decisions to undergo TKR, and (2) explore their perceptions and engagement in the rehabilitation process.
Methods
Study Design
A qualitative descriptive design was adopted to explore patient preferences, treatment decisions, and rehabilitation experiences in real-world cultural contexts.22,23 In-depth, semi-structured interviews were used to interpret the subjective meanings participants assigned to their experiences, providing a comprehensive understanding of the phenomenon. Each participant completed two interviews addressing decision-making and post-rehabilitation experiences, with follow-up telephone interviews conducted to clarify individual perspectives on home-based recovery satisfaction. Grounded Theory guided inductive data analysis24 while Symbolic Interactionism informed the interpretation of how women constructed meaning around surgical decisions and rehabilitation.25
Setting and Participants
Participants were recruited purposively from the orthopedic ward of a medical center in northern Taiwan, where 338 patients underwent TKR in 2018 (76% women, 67% aged ≥60 years). Eligible participants were: (1) women aged 60 years or older, (2) who had undergone a primary unilateral TK, and (3) able to communicate in Mandarin Chinese. Exclusion criteria included: (1) a diagnosis of mental illness, (2) dementia, (3) bilateral TKR, or (4) revision TKR.
Data Collection
Data were collected between September 2020 and May 2021, during the COVID-19 pandemic, through interviews, observations, and field notes. No non-participants were present during the interviews. Each interview was conducted privately with only the participant and the interviewer in the room. This approach minimized external influence on participants’ responses and ensured privacy, comfort, and the authenticity of the data collected. Each participant completed two face-to-face interviews (3–5 days post-surgery; 6–8 weeks post-surgery) and a follow-up telephone interview at 6 months. A semi-structured guide encouraged open discussion (eg, “Can you describe your experience with knee problems before surgery? “How has your condition progressed since returning home?” How would you evaluate satisfaction with the outcome of surgery?) All interviews were audio-recorded, transcribed verbatim, and supplemented by field notes. Recruitment continued until the twentieth participant, at which point thematic saturation was achieved.
Data Analysis
The data were analyzed using the constant comparative method, which involved the sequential processes of open coding, axial coding, and selective coding.24 During analysis, open coding generated initial codes such as “limited mobility,” “concern about burdening family,” “encouragement from others,” and “enduring pain for recovery.” Axial coding then grouped these into broader categories reflecting the themes in Table 1—for example, codes related to mobility restrictions, work limitations, and disrupted sleep were organized under “pain impacts,” while codes describing determination, goal setting, and creative home-based strategies formed “rehabilitation challenges.” Selective coding integrated these categories into the core theme of “reclaiming independent life through surgical transformation.” To ensure consistency, two analysts independently coded transcripts and compared interpretations, resolving differences through discussion and confirmation of category definitions, with peer debriefing used to reach consensus on the final thematic structure.
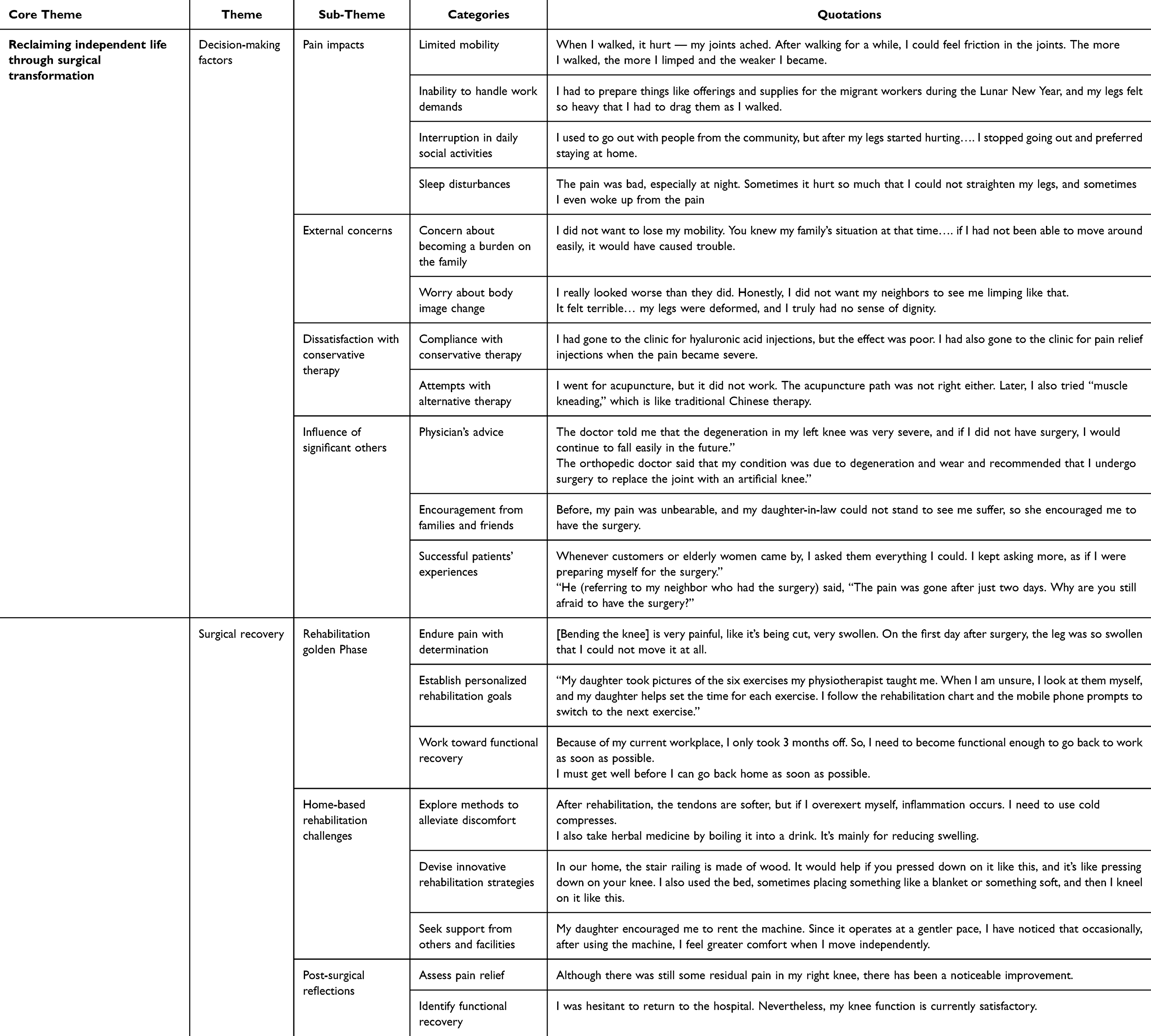 |
Table 1 Core Themes, Themes, Sub-Themes, and Categories Derived from Women’s Experiences of TKR |
Rigor
The study’s rigor was evaluated using Lincoln and Guba’s four criteria for trustworthiness.23 The first female author (CHH), a master ‘s-level nurse with two decades of orthopedic experience and formal qualitative research training, conducted all interviews to ensure depth and consistency. Credibility was established through prolonged engagement (CHH), member checking, and data triangulation across interviews, observations, and field notes. Peer debriefings with experienced qualitative researchers (SWC, and MHL) provided critical reflection on coding, interpretation, and thematic coherence, thereby enhancing analytic transparency. Dependability and confirmability were ensured through systematic documentation, data verification, and an audit trail jointly reviewed by CHH and SWC. Transferability was supported by detailed contextual and methodological descriptions, allowing readers to assess the applicability of findings to comparable clinical and cultural settings.
Results
The study includes 20 older women aged 60–84 years (mean = 70.1), all recruited from a single medical center in northern Taiwan. Most participants were married or widowed (90%) and identify with Taoism or Buddhism (100%). The majority had primary or secondary education (80%) and were retired or engaged in domestic work (70%) (Table 2). Analysis of their narratives revealed a core themes: reclaiming independent life through surgical transformation. The core theme reflected how physical, psychosocial, and cultural factors shaped women’s decision-making and recovery experiences following TKR (Table 1).
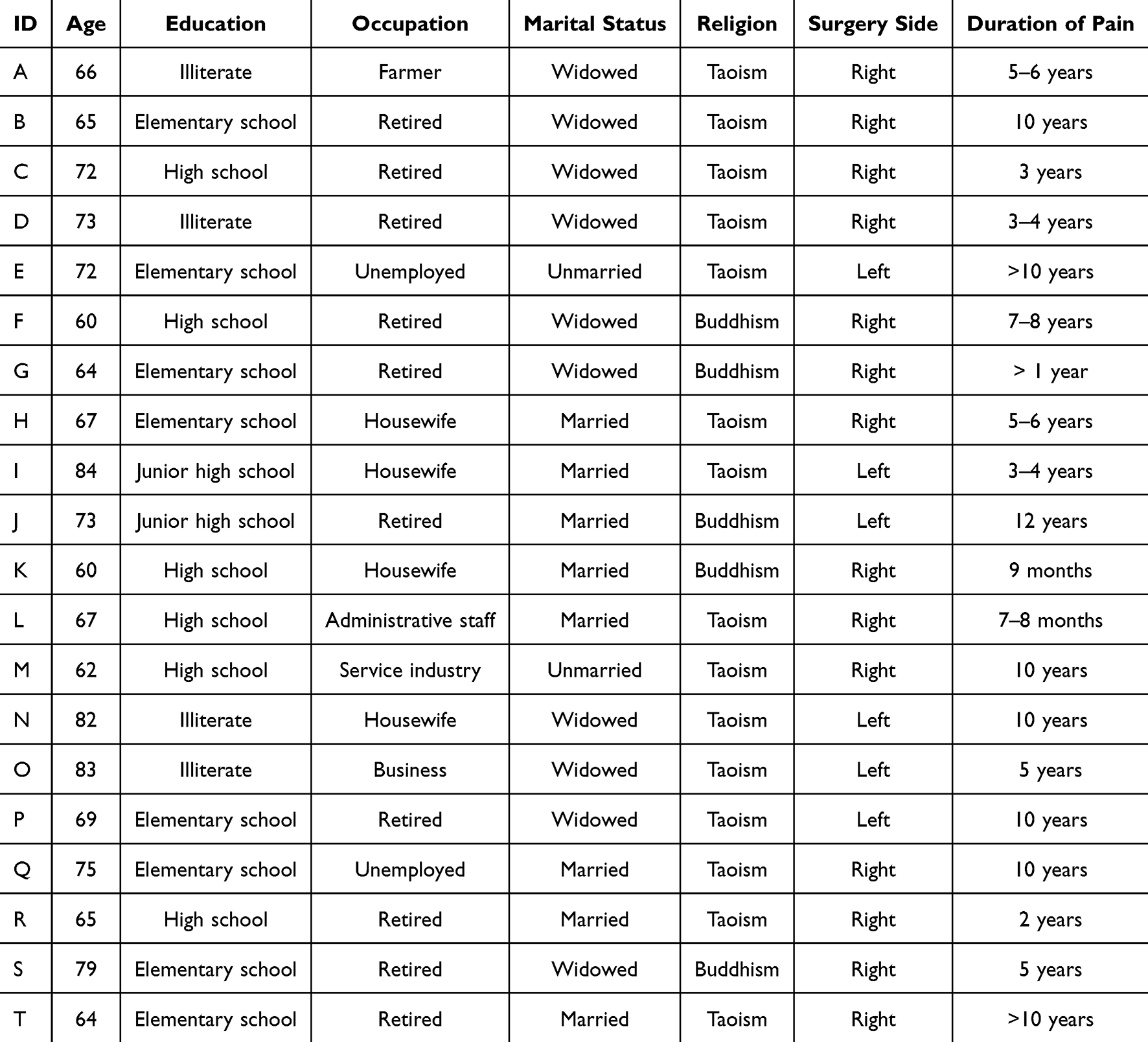 |
Table 2 Demographic Characteristics of Older Women (N = 20) |
Theme 1: Decision-Making Factors
After receiving a diagnosis of OA, the participating women experienced prolonged struggles before deciding to undergo TKR, with the duration ranging from seven months to twelve years. During this period, they lived with persistent pain and sought various nonsurgical treatments to alleviate their discomfort and delay surgery.
Pain Impacts
Persistent pain and stiffness interfered with their ability to fulfill work responsibilities, engage in social activities, and maintain regular sleep patterns.
E: When I walked, it hurt — my joints ached. After walking for a while, I could feel friction in the joints. The more I walked, the more I limped and the weaker I became. (limited mobility)
L: I had to prepare things like offerings and supplies for the migrant workers during the Lunar New Year, and my legs felt so heavy that I had to drag them as I walked. (inability to handle work demands)
L: I used to go out with people from the community, but after my legs started hurting…. I stopped going out and preferred staying at home. (interruption in daily social activities)
G: The pain was bad, especially at night. Sometimes it hurt so much that I couldn’t straighten my legs, and sometimes I even woke up from the pain. (sleep disturbances)
External Concerns
Beyond the physical challenges of knee OA, the women also experienced external concerns that influenced their decision-making regarding surgery.
Concern About Becoming a Burden on the Family
As knee OA progressed, many women struggled to maintain their caregiving roles at home. Worsening pain and reduced mobility heightened their fear of burdening family members. Valuing self-reliance, they chose TKR to regain independence and ease their families’ caregiving responsibilities.
B: I hoped my leg would recover so that I could walk around freely without restrictions. I wanted to get better quickly and not become a burden to my children.
M: I didn’t want to lose my mobility. You knew my family’s situation at that time…. if I hadn’t been able to move around easily, it would have caused trouble.
Worry About Body Image Change
Women were distressed by the visible deformity and limping caused by knee OA, which undermined their confidence and sense of normalcy. They viewed TKR to correct alignment, restore appearance, and regain functional mobility.
K: I really looked worse than they did. Honestly, I did not want my neighbors to see me limping like that.
R: It felt terrible… my legs were deformed, and I truly had no sense of dignity.
Dissatisfaction with Conservative Therapy
Despite trying various nonsurgical and alternative treatments to relieve pain and maintain daily function, most women experienced only temporary relief. Their growing dissatisfaction with conservative care strengthened their resolve to pursue surgery as a definitive solution.
Compliance with Conservative Therapy
Many women actively sought medical care across clinics and hospitals, adhering to professional recommendations and undergoing multiple conservative treatments, including medications, physical therapy, and injections such as steroids, hyaluronic acid, or platelet-rich plasma (PRP).
F: I had gone to the clinic for hyaluronic acid injections, but the effect was poor. I had also gone to the clinic for pain relief injections when the pain became severe.
H: I spent about fifty thousand dollars on PRP injections, but they were ineffective. I still felt very uncomfortable.
Attempts with Alternative Therapy
Before deciding on surgery, most women sought relief through alternative therapies, including traditional Chinese medicine, massage, acupuncture, and health supplements. Although these methods occasionally provided temporary comfort, the improvements were short-lived and insufficient to restore normal function.
F: I had first tried acupuncture and visited a traditional Chinese medicine doctor. Each course of treatment lasted quite a long time because I thought I needed to keep it up to get better. The longest one lasted for more than three years before I eventually had the surgery.
L: I went for acupuncture, but it didn’t work. The acupuncture path wasn’t right either. Later, I also tried ‘muscle kneading,’ which is like traditional Chinese therapy. It’s like when a certain area hurts or is injured, they press it hard—it hurt so much, as if my flesh was being pinched.
Influence of Significant Others
The women’s decisions to undergo TKR were shaped by the influence of significant others, including physicians, family members, friends, and other patients who had previously undergone the procedure.
Physician’s Advice
Physicians played a critical role in shaping women’s surgical decisions. Their clear explanations and professional reassurance reduced fear and uncertainty, strengthening women’s confidence in choosing surgery.
G: The doctor told me that the degeneration in my left knee was very severe, and if I didn’t have surgery, I would continue to fall easily in the future.
I: The orthopedic doctor examined me and said that my condition was due to degeneration and wear and recommended that I undergo surgery to replace the joint with an artificial knee.
Encouragement from Families and Friends
Encouragement from family and friends played a vital role in women’s decisions to undergo TKR. Family members offered emotional reassurance and practical support, while peers who had successfully recovered from surgery shared positive experiences that reduced fear and strengthened confidence.
B: My daughter told me that the hospital had good infection control, so she told me not to worry. I thought since I had already decided to have the surgery, I should just do it soon and recover quickly.
C: Before, my pain was unbearable, and my daughter-in-law couldn’t stand to see me suffer, so she encouraged me to have the surgery.
Successful Patients’ Experiences
Women gained reassurance about TKR’s effectiveness by observing other patients who successfully managed pain, completed rehabilitation, and regained mobility in daily life.
F: Whenever customers or elderly women came by, I asked them everything I could. I kept asking more, as if I were preparing myself for the surgery.
O: He (referring to my neighbor who had the surgery) said, ‘The pain was gone after just two days. Why are you still afraid to have the surgery?’ His surgery went well. Now he can walk without using an umbrella for support.
In contrast, observing those who faced complications or slower recovery prompted more cautious consideration. Overall, learning from other patients’ outcomes provided realistic expectations and strongly influenced the women’s decision to proceed with TKR.
A: There was an elderly woman in my village who went back to work in the fields right after her surgery. As a result, she couldn’t walk afterward. I didn’t know whether it was because she didn’t do rehabilitation.
C: When I went to the family medicine clinic, I saw an elderly woman, probably in her eighties. Her mind was very clear, but she couldn’t walk. It took her more than five minutes to walk a very short distance.
Theme 2: Surgical Recovery
Women demonstrate strong determination to restore mobility and independence following TKR.
Rehabilitation Golden Phase
Following TKR, the women actively monitored their postoperative recovery and strived to maximize outcomes during the critical “golden phase” of rehabilitation.
Endure Pain with Determination
During the early postoperative phase, women commonly experienced acute symptoms such as heaviness in the legs, limited knee mobility, and restricted joint extension. Despite these challenging discomforts, the women persevered and endured the pain.
G: It is like you are better off dead, very painful. I pressed that, kept pressing it, and it was still excruciating. You can’t straighten it, can’t lift it high, it just hurts.
L: [Bending the knee] is very painful, like it’s being cut, very swollen. On the first day after surgery, the leg was so swollen that I couldn’t move it at all.
Establish Personalized Rehabilitation Goals
The women diligently adhered to their post-TKR personal rehabilitation plans, performing various exercises such as soon as it was tolerable. Whether independently or with assistance, they followed a structured approach to maximize the effectiveness of their rehabilitation.
C: My daughter took pictures of the six exercises my physiotherapist taught me. When I’m unsure, I look at them myself, and my daughter helps set the time for each exercise. I follow the rehabilitation chart and the mobile phone prompts to switch to the next exercise.
J: “Whatever my daughter asks me to do; I just do it. She even showed me information on how to rehabilitate, and she guides me while I’m doing it.
Work Toward Functional Recovery
After undergoing TKR, the women were motivated to regain knee function and resume their normal daily activities or work responsibilities. They demonstrated strong determination to restore joint mobility and strength, viewing functional recovery as both a personal goal and an indicator of surgical success.
M: Because of my current workplace, I only took 3 months off. So, I need to become functional enough to go back to work as soon as possible.
N: I must get well before I can go back home as soon as possible. It doesn’t matter if I don’t (bend my knees) 90°. I’m 84 years old. What am I afraid of? I can walk, I can sit, I can. (Benchmark: Sit and walk)
Home-Based Rehabilitation Challenges
After home, women faced added challenges to home-based rehabilitation, including limited outpatient access, fear of infection, and lack of supervision. Persistent pain, stiffness, and uncertainty about proper exercise techniques caused stress, yet they remained adaptable—developing self-care strategies, modifying routines, and seeking family or professional support when possible.
Explore Methods to Alleviate Discomfort
At home, women independently managed knee pain, swelling, and stiffness by using hot or cold compresses, adjusting posture, and modifying their diet. Some also turned to traditional or folk remedies, such as herbal drinks or talisman-infused water, to relieve discomfort.
A: After rehabilitation, the tendons are softer, but if I overexert myself, inflammation occurs. I need to use cold compresses.
P: I use aloe vera—the inner layer, not the outer layer. I use the inner layer for compresses. I also take herbal medicine by boiling it into a drink. It’s mainly for reducing swelling.
Devise Innovative Rehabilitation Strategies
Some women adapted their home environments to facilitate knee rehabilitation, seamlessly integrating these changes into their daily routines.
H: In our home, the stair railing is made of wood. It would help if you pressed down on it like this, and it’s like pressing down on your knee. I also used the bed, sometimes placing something like a blanket or something soft, and then I kneel on it like this.
Seek Support from Others and Facilities
Among the women in this study, eight managed their care, four received support from their husbands, their children assisted seven, and one participant received support from her brother. Some women embraced suggestions from family and enlisted the help of loved ones to identify the most effective rehabilitation methods.
M: My daughter encouraged me to rent the machine. Since it operates at a gentler pace, I’ve noticed that occasionally, after using the machine, I feel greater comfort when I move independently.
B: I started practicing by holding onto the doorknob and doing squats, although I still needed to be able to squat.
In the absence of family support, one participant opted to utilize a caregiver through Long-Term Care Service 2.0 to aid her in her daily activities and facilitate her rehabilitation.
D: I’ve applied for a three-hour caregiver [referring to the Long-Term Care Service 2.0 program] who comes once a week. She assists me with bathing and lifting my legs like this.
Some participants incorporated home-based rehabilitation practices alongside regular visits to local healthcare facilities for additional support.
A: I can bend it like this [approximately 90 degrees]. So, I started rehabilitation. My granddaughter drove me to the rehabilitation department of the hospital. The therapist teacher helps me bend it.
E: I go to the rehabilitation clinic daily, and my younger brother helped me bend my leg thrice daily. Six weeks post-surgery, I felt that my rehabilitation was progressing well on my own, so I stopped going to the clinic for rehabilitation.
Post-Surgical Reflections Outcomes
Six months after TKR, about two-thirds of participants reflected improved rehabilitation outcomes, ranging from “extremely satisfied” to “satisfied,” while the remainder felt neutral. Pain relief and functional recovery were the primary indicators used to evaluate rehabilitation effectiveness.
Assess Pain Relief
One woman underwent surgery on her left knee five years before and subsequently required TKR revision on the same knee.
H: Although there is still some residual pain in my right knee, there has been a noticeable improvement.
Another woman had prior surgery on her left knee and, after two years, opted for surgery on her right knee.
T: Approximately a year after the operation, the intensity of the pain lessened.
Identify Functional Recovery
One woman underwent surgery on her right knee, followed by surgery on her left knee two years later. She noted a significant improvement in the outcome after the more recent surgery on her left knee.
H: Despite some lingering numbness in my knee, it has considerably improved compared to the intense pain I endured while walking. I had a realistic understanding of the condition of my knee joint prior to the surgery, and I am content with the results.
Another woman underwent TKR on her left knee and, six months later, had surgery for colorectal cancer. She prioritized addressing the colorectal cancer first and deferred the operation on her right knee. She mentioned that her left knee exhibited good mobility and functionality.
P: Given the worsening state of the epidemic, I am hesitant to return to the hospital. Nevertheless, my knee function is currently satisfactory.
Discussion
This qualitative study explored how older Taiwanese women decided to undergo TKR and engaged in rehabilitation. Findings have revealed that surgical decisions are shaped by the interplay of physical suffering, cultural expectations, and family dynamics, while recovery experiences reflect resilience and a desire to regain independence. Interpreted through the Theory of Planned Behavior (TPB),26 women’s attitudes, subjective norms, and perceived behavioral control (PBC) collectively influenced their choices and behaviors.
Decision-Making Factors
Women’s decisions to undergo TKR are primarily motivated by severe pain, restricted mobility, and loss of independence. Their attitudes toward surgery are influenced by expectations of pain relief, restored function, and the ability to continue fulfilling familial and social roles. Consistent with earlier studies, women initially rely on conservative and traditional therapies before considering surgery.27–29 This preference for noninvasive care reflects East Asian health beliefs emphasizing gradual intervention and bodily preservation. Subjective norms are shaped by Chinese sociocultural values grounded in Confucian filial piety and collectivist family orientation,30,31 where maintaining autonomy and avoiding dependence on family are regarded as moral expectations for older adults. Many women concern about burdening their children and view surgery as a way to preserve self-sufficiency and family harmony. External influences—including physician advice, family encouragement, and positive peer experiences—reinforce surgical intentions, whereas negative examples are often dismissed as isolated cases.32–35 PBC is strengthened by women’s confidence in performing TKR through supportive family involvement and by observing successful surgical outcomes of previous patients, which enhance their sense of agency and optimism.
Rehabilitation After TKR
Following surgery, women demonstrate strong determination to engage in rehabilitation, reflecting high self-efficacy and PBC.36 Reclaiming independences through rehabilitation emerges as a central theme, as participants set personalized goals shaped by their social roles and expectations. Caregivers prioritize resuming domestic responsibilities, while working women focus on faster recovery and greater knee flexion, illustrating diverse expressions of self-efficacy. These findings align with prior evidence identifying self-efficacy as a determinant of adherence, physical recovery, and psychological well-being.37–39
In Taiwan, women participate in both home-based rehabilitations, supported by family members and self-directed strategies, and facility-based programs funded by the NHI, which offer structured follow-up and professional guidance.37 This dual rehabilitation system enables women to balance culturally embedded caregiving responsibilities, empowerment, and ongoing medical supervision. International evidence similarly indicates that home-based or tele-rehabilitation after TKR achieves long-term outcomes in pain relief, mobility, and function comparable to those of hospital-based programs, with home-based approaches sometimes promoting faster improvements in range of motion.40,41 Approximately six months after surgery, most women report improved rehabilitation outcomes and satisfaction with recovery.
The cultural dynamics identified in this study have potential transferability to other East Asian societies where Confucian family ethics, collectivist values, and filial responsibility similarly shape health-related decision-making.30,31 In these contexts, older women often perceive surgery and rehabilitation not only as medical acts but as moral responsibilities to remain independent and reduce family burden. Comparable findings have been reported in Asian country of Japan, South Korea, and China, where intergenerational expectations influence treatment choices and recovery engagement.27–29,38,42
Clinical Implications
This study highlights the importance of culturally responsive and patient-centered care throughout the TKR decision-making and rehabilitation process. Guided by the TPB, clinical interventions should enhance PBC through self-management support, strengthen positive attitudes by providing evidence-based education on surgical outcomes, and integrate subjective norms by engaging family members in SDM. Healthcare professionals—particularly nurses, rehabilitation specialists, and case managers—play a pivotal role in implementing these strategies. Interprofessional collaboration ensures continuous guidance and psychosocial support from preoperative counseling through home- and facility-based rehabilitation. Case managers should maintain ongoing follow-up to monitor patients’ progress, reinforce adherence, and address emerging barriers to recovery.
Tailored rehabilitation plans that integrate patients’ cultural beliefs and traditional healing practices can further strengthen motivation and adherence. Taiwan’s NHI supported dual rehabilitation model exemplifies how hospital-based and home-based programs can coexist to promote continuity of care. This approach may serve as a reference for other East Asian healthcare systems seeking to balance accessibility, family participation, and culturally attuned recovery support.
Limitations
This study was conducted at a single medical center and involved only older female participants, which limits the generalizability of the findings. Although data collection extended to six months post-surgery, longer-term outcomes remain unexplored. Future research, including studies involving male participants, diverse settings, and extended follow-up periods, is recommended to capture broader gender and cultural perspectives on decision-making and rehabilitation after TKR.
Conclusions
Older Taiwanese women’s decisions to undergo TKR reflect the interplay of physical pain, loss of mobility, and cultural expectations surrounding autonomy and family roles. Their choices balance enduring discomfort with the desire to maintain independence, shaped by interactions with physicians, family members, and peers. During rehabilitation, women demonstrate resilience and motivation to restore mobility, supported by both family and healthcare professionals. Although some integrate traditional practices, most adhere to structured exercise and medical guidance to regain daily function. These findings underscore that women’s TKR experiences encompass both physical and sociocultural dimensions. Targeted, family-inclusive, and culturally sensitive support—combined with continuous case manager follow-up—can strengthen adherence, promote recovery, and enhance quality of life.
Ethics Approval and Informed Consent
The study was conducted in accordance with the Declaration of Helsinki (as was revised in 2013). Ethical approval was obtained from the Institutional Review Board of National Taiwan University Hospital (Approval No.: 202009031RINA). Participants provided written informed consent, which included permission for the publication of anonymized responses and direct quotations.
Acknowledgment
The authors thank the 20 women who generously shared their experiences for this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. Lancet. 2019;393(10182):1745–1759. doi:10.1016/S0140-6736(19)30417-9
2. Bannuru RR, Osani MC, Vaysbrot EE, et al. OARSI guidelines for the non-surgical management of knee, Hip, and polyarticular osteoarthritis. Osteoarthritis Cartilage. 2019;27(11):1578–1589. doi:10.1016/j.joca.2019.06.011
3. Katz JN, Arant KR, Loeser RF. Diagnosis and treatment of Hip and knee osteoarthritis: a review. JAMA. 2021;325(6):568–578. doi:10.1001/jama.2020.22171
4. Giorgino R, Albano D, Fusco S, Peretti GM, Mangiavini L, Messina C. Knee osteoarthritis: epidemiology, pathogenesis, and mesenchymal stem cells: what else is new? an update. Int J Mol Sci. 2023;24(7). doi:10.3390/ijms24076405
5. Hawker GA. Osteoarthritis is a serious disease. Clin Exp Rheumatol Sep-Oct. 2019;37(5):3–6.
6. Du X, Liu ZY, Tao XX, et al. Research progress on the pathogenesis of knee osteoarthritis. Orthop Surg. 2023;15(9):2213–2224. doi:10.1111/os.13809
7. Gandhi N, Qadeer AS, Meher A, et al. Costs and models used in the economic analysis of total knee replacement: a systematic review. PLoS One. 2023;18(7):e0280371. doi:10.1371/journal.pone.0280371
8. Geng R, Li J, Yu C, et al. Knee osteoarthritis: current status and research progress in treatment. Exp Ther Med. 2023;26(4):481. doi:10.3892/etm.2023.12180
9. Lim CV, Harithasan D, Ahmad MAB, Mesbah N, Kumar S, Singh DKA. Biopsychosocial determinants for total knee replacement decisions among older adults with chronic knee osteoarthritis: a scoping review. Geriatr. Orthop. Surg. Rehabil. 2025;16:21514593251335882. doi:10.1177/21514593251335882
10. Engström Å, Boström J, Karlsson AC. Women’s experiences of undergoing total knee joint replacement surgery. J Perianesth Nurs. 2017;32(2):86–95. doi:10.1016/j.jopan.2015.11.009
11. Tay Swee Cheng R, Klainin-Yobas P, Holroyd E, Lopez V. A “Journey to regain life” after joint replacement surgery: a qualitative descriptive study. Appl Nurs Res. 2018;41:5–10. doi:10.1016/j.apnr.2018.03.002
12. Nakano N, Shoman H, Olavarria F, Matsumoto T, Kuroda R, Khanduja V. Why are patients dissatisfied following a total knee replacement? a systematic review. Int Orthop. 2020;44(10):1971–2007. doi:10.1007/s00264-020-04607-9
13. Chou TA, Ma HH, Tsai CW, et al. The safety and cost-analysis of simultaneous versus staged bilateral total knee arthroplasty in a Taiwan population. J Chin Med Assoc. 2023;86(5):494–498. doi:10.1097/jcma.0000000000000892
14. Shih JT, Tan TL, Shen PH, et al. Postoperative bisphosphonates use is associated with reduced adverse outcomes after primary total joint arthroplasty of Hip and knee: a atnionwide population-based cohort study. Calcif Tissue Int. 2024;114(5):451–460. doi:10.1007/s00223-024-01192-6
15. Lin FH, Chen HC, Lin C, et al. The increase total knee replacement surgery in Taiwan: a 15-year retrospective study. Medicine. 2018;97(31):e11749. doi:10.1097/MD.0000000000011749
16. Hsu LI, Chen JW, Hou SM. Geographic and hospital variations in the use of red blood cells and tranexamic acid among total Hip and total knee arthroplasty. Formos J Musculoskelet Disord. 2025;16(1):27–33. doi:10.4103/fjmd.FJMD-D-23-00033
17. Al Thaher Y, Alfuqaha OA, Dweidari A. Health‐related quality of life and outcome after total knee replacement: results from a cross‐sectional survey in Jordan. Adv Orthop. 2021;2021(1):5506809. doi:10.1155/2021/5506809
18. Woodland N, Takla A, Estee MM, et al. Patient-reported outcomes following total knee replacement in patients aged 65 years and over—a systematic review. J Clin Med. 2023;12(4):1613. doi:10.3390/jcm9103150
19. Tsang MP, Man GCW, Xin H, et al. The effectiveness of telerehabilitation in patients after total knee replacement: a systematic review and meta-analysis of randomized controlled trials. J Telemed Telecare. 2024;30(5):795–808. doi:10.1177/1357633X221097469
20. Pournajaf S, Goffredo M, Pellicciari L, et al. Effect of balance training using virtual reality-based serious games in individuals with total knee replacement: a randomized controlled trial. Ann Phys Rehabil Med. 2022;65(6):101609. doi:10.1016/j.rehab.2021.101609
21. Jayakumar P, Moore MG, Furlough KA, et al. Comparison of an artificial intelligence–enabled patient decision aid vs educational material on decision quality, shared decision-making, patient experience, and functional outcomes in adults with knee osteoarthritis: a randomized clinical trial. JAMA Network Open. 2021;4(2):e2037107. doi:10.1001/jamanetworkopen.2020.37107
22. Holloway I, Galvin K. Qualitative Research in Nursing and Healthcare.
23. Lincoln YS, Guba EG. Naturalistic Inquiry. Thousand Oaks. SAGE; 1985.
24. Makri C, Neely A. Grounded theory: a guide for exploratory studies in management research. Int J Qual Methods. 2021;20:16094069211013654. doi:10.1177/160940692110136
25. Mukhtar D. The symbolic interactionism theory: a systematic literature review of current research. Int J Mod Trends Soc Sci. 2021;4(17):113–126. doi:10.35631/IJMTSS.417010
26. Ajzen I, Schmidt P. Changing behavior using the theory of planned behavior. In: Hagger MS, Cameron LD, Hamilton K, Hankonen N, Lintunen T, editors. The Handbook of Behavior Change. Cambridge, UK: Cambridge University Press; 2020:17–31.
27. Ko HF, Chen CH, Dong KR, Wu HC. Effects of acupuncture on postoperative pain after total knee replacement: a systematic review and meta-analysis. Pain Med. 2021;22(9):2117–2127. doi:10.1093/pm/pnab201
28. Moghaddamnezhad S, Daneshjoo A, Sadati SKM. Hydrotherapy and massage: effect on dynamic and static balance and quality of life of people with total knee replacement: a randomized controlled trial. Sport Sci Health. 2025;1–10. doi:10.1007/s11332-025-01434-6
29. Lim WB, Al-Dadah O. Conservative treatment of knee osteoarthritis: a review of the literature. World J Orthop. 2022;13(3):212. doi:10.5312/wjo.v13.i3.212
30. Gu C, Li Z. The Confucian ideal of filial piety and its impact on Chinese family governance. J Sociol Ethnol. 2023;5(2):45–52. doi:10.23977/jsoce.2023.050208
31. Bedford O, Yeh KH, Tan CS. Filial piety as a universal construct: from cultural norms to psychological motivations. Front Psychol. 2022;13:980060. doi:10.3389/fpsyg.2022.980060
32. Traumer L, Sørensen EE, Kusk KH, Skou ST. Investigating the motives of patients with knee OA undergoing a TKR: a qualitative interview study. Musculoskeletal Care. 2018;16(3):380–387. doi:10.1002/msc.1244
33. Barlow T, Scott P, Griffin D, Realpe A. How outcome prediction could affect patient decision making in knee replacements: a qualitative study. BMC Musculoskelet Disord. 2016;17:304. doi:10.1186/s12891-016-1165-x
34. Yeh WL, Tsai YF, Hsu KY, Chen DW, Chen CY. Factors related to the indecision of older adults with knee osteoarthritis about receiving physician-recommended total knee arthroplasty. Disabil Rehabil. 2017;39(22):2302–2307. doi:10.1080/09638288.2016.1226407
35. Wang -C-C, Huang K-C, Ku M-C, et al. Factors influencing the decision to receive total knee replacement among patients with severe knee osteoarthritis under universal health insurance coverage. Sci Rep. 2024;14(1):30028. doi:10.1038/s41598-024-81852-7
36. Fuchs S, Schwettmann L, Katzenberger B, et al. Association of self-efficacy, risk attitudes, and time preferences with health-related quality of life and functioning after total Hip or knee replacement – results of the MobilE-TRA 2 cohort. Health Qual Life Outcomes. 2025;23:44. doi:10.1186/s12955-025-02374-y
37. Meng Y, Deng B, Liang X, et al. Effectiveness of self-efficacy-enhancing interventions on rehabilitation following total Hip replacement: a randomized controlled trial with six-month follow-up. J Orthop Surg Res. 2022;17(1):225. doi:10.1186/s13018-022-03116-2
38. Park KH, Kang HY. The effects of a self-efficacy, theory-based exercise program for patients undergoing with total knee arthroplasty. J Korean Acad Nurs. 2024;54(4):547. doi:10.4040/jkan.24027
39. Maliga M, Sjattar EL, Syahrul S. Effectiveness of integrated education in improving patient self-efficacy after total Hip and knee replacement surgeries. Enferm Clin. 2021;31:S682–S687. doi:10.1016/j.enfcli.2021.07.017
40. Oldrini LM, Sangiorgio A, Nutarelli S, et al. Home-based vs conventional rehabilitation following total knee arthroplasty. Prosthesis. 2025;7(2):34. doi:10.3390/prosthesis7020034
41. Zhang H, Wang J, Jiang Z, Deng T, Li K, Nie Y. Home-based tele-rehabilitation versus hospital-based outpatient rehabilitation for pain and function after initial total knee arthroplasty: a systematic review and meta-analysis. Medicine. 2023;102(51):e36764. doi:10.1097/MD.0000000000036764
42. Hara K, Kanda M, Kobayashi Y, Miyamoto T, Inoue T. Factors affecting the length of hospital stay for total knee arthroplasty in Japan: a retrospective study using the diagnosis procedure combination database. Eur J Med Res. 2024;29(1):122. doi:10.1186/s40001-024-01714-w
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Expectations and Experiences of a Group of Patients Enrolled in an Educational Program for Rheumatoid Arthritis at a Specialized Care Center in Colombia
Castiblanco-Montañez RA, Buitrago-Garcia D, Arévalo Velandia A, Garzón-Cepeda JD, Rodríguez-Florido F, Sánchez Vanegas G, Santos-Moreno P
Journal of Multidisciplinary Healthcare 2023, 16:483-492
Published Date: 22 February 2023
The Practice of Shared Decision-Making Among Physiotherapists and Patients with Musculoskeletal Conditions
Alotaibi MA, Alhowimel AS, Alodaibi FA, Aloraifi M
Journal of Multidisciplinary Healthcare 2023, 16:2655-2665
Published Date: 8 September 2023
Exploring the Important Determinants Shaping Treatment Preferences: Qualitative Insights into Breast Cancer Patient Experiences and Perspectives in New Zealand
Yeo HY, Wong JHY, Chan SJ, Latu ATF, Han CH, Anwar M, Marra CA
Patient Preference and Adherence 2023, 17:3525-3537
Published Date: 22 December 2023
Shared Decision-Making in the Treatment of Multiple Sclerosis: Results of a Cross-Sectional, Real-World Survey in Europe and the United States
Keenan A, Le HH, Gandhi K, Adedokun L, Jones E, Unsworth M, Pike J, Trenholm E
Patient Preference and Adherence 2024, 18:137-149
Published Date: 16 January 2024
Multiple Myeloma Experiences and Preferences: A Mixed Methods Study of Patients and Care Partners in the United States
Flora DR, Byrd R, Platt DA, Hlavacek P, Hoag Goldman E, Cappelleri JC, Kennedy CT, LeBlanc TW
Patient Preference and Adherence 2025, 19:963-979
Published Date: 8 April 2025