Back to Journals » Patient Preference and Adherence » Volume 18
Shared Decision-Making in the Treatment of Multiple Sclerosis: Results of a Cross-Sectional, Real-World Survey in Europe and the United States
Authors Keenan A, Le HH, Gandhi K, Adedokun L, Jones E, Unsworth M, Pike J, Trenholm E
Received 12 October 2023
Accepted for publication 21 December 2023
Published 16 January 2024 Volume 2024:18 Pages 137—149
DOI https://doi.org/10.2147/PPA.S440410
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Alexander Keenan,1 Hoa H Le,1 Kavita Gandhi,2 Lola Adedokun,3 Eddie Jones,4 Mia Unsworth,4 James Pike,5 Emily Trenholm4
1Scientific Affairs, Janssen Pharmaceuticals Inc., Titusville, NJ, USA; 2Research and Development, Janssen Pharmaceuticals Inc., Titusville, NJ, USA; 3Research and Development, Janssen-Cilag Ltd, High Wycombe, UK; 4Central Nervous System, Adelphi Real World, Bollington, Cheshire, UK; 5Statistics & Data Analytics, Adelphi Real World, Bollington, Cheshire, UK
Correspondence: Mia Unsworth, Adelphi Real World, Adelphi Mill, Grimshaw Lane, Macclesfield, Bollington, Cheshire, SK10 5JB, United Kingdom, Tel +441625578677, Email [email protected]
Introduction: Multiple sclerosis (MS) is a neurodegenerative disease characterized by progressive deterioration of cognitive and physical functioning, reducing activities of daily living and quality of life (QoL). Several treatments are available that modify the course of the disease and reduce the frequency of relapses. Although effective, all treatment options are accompanied by adverse events, and this study aimed to assess the extent to which patients were involved in the choice of treatment.
Methods: Data were drawn from the Adelphi Multiple Sclerosis Disease Specific Program (DSP)™, a cross-sectional survey of healthcare practitioners (HCP) and their patients with MS in real-world clinical settings in Europe and the United States (US) between December 2020 and July 2021. HCPs reported patient demographics, clinical characteristics, current and previous treatment, and treatment outcomes. Patients voluntarily completed questionnaires reporting the physical and psychological impact of their MS and its treatment. Regression analysis with inverse probability of treatment weighting was used to compare treatment outcomes in patients actively involved in their current treatment choice with those who were not.
Results: Of a total of 692 patients, median age 40 years and 64% female, mostly diagnosed with relapsing-remitting MS, those who were involved in shared decision-making tended to choose oral therapies such as dimethyl fumarate more often than HCPs. MS had greater impact on physical and psychological functioning in patients whose HCP made treatment decisions solely. Patients involved in decision-making reported greater satisfaction with their treatment and a better QoL.
Discussion: Because no single optimal therapy exists for patients with MS, treatments should be individualized with consideration of patients’ preferences. Our study shows that shared decision-making is under-utilized in the management of MS and supports the benefits of patient involvement.
Conclusion: Patients who have an active role in treatment decision-making show improved wellbeing and QoL, and overall treatment satisfaction.
Plain Language Summary: Multiple sclerosis (MS) is a disease that affects the brain, causing symptoms such as blurred vision and problems with movements, thoughts, and feelings. MS is a lifelong condition that becomes worse over time and limits the activities that people can do. There are many treatments that can help to reduce relapses (when symptoms become worse), but all have their benefits and drawbacks. It is often the physician who decides which treatment to use, but we wanted to know if patients would feel better if they were involved in the decision.
Using our standardized and validated questionnaires, we surveyed physicians and nurses who treat patients with MS in Europe and the United States of America between December 2020 and July 2021, to assess how they felt about the treatment they chose and its effect on the patient. We also asked the patients themselves how they felt about their illness and treatment, whether they were given the chance to choose which treatment to take, and how their treatment affected their symptoms and overall quality of life.
The information provided by both the physicians and their patients was used to compare how patients responded when they were involved in the treatment decisions. We found that patients who were involved in choosing their treatment were more satisfied with their treatment and responded better than those whose physicians decided alone. Therefore, it is important for physicians treating patients with MS to consider their patients’ preferences when deciding which treatment is best for them.
Keywords: multiple sclerosis, patient preference, decision-making, shared, multinational, survey
Introduction
Multiple sclerosis (MS) is a demyelinating disease of the central nervous system with a variable clinical course characterized by neurological dysfunction and increasing disability over time.1–3 The onset of MS usually occurs in young adults, mainly in the third decade of life, with a mean age at diagnosis of 32 years, and females twice as likely as males to be affected.4 While MS occurs in different forms, the relapsing-remitting form (RRMS) is the most common, affecting about 65% of MS patients.1 Since MS is characterized by a progressive worsening of neurological function, the symptoms and motor deficits can significantly impact patients’ quality of life (QoL) and performance of activities of daily living, resulting in decreased independence and occupational performance, together with an increased utilization of healthcare resources.5
MS is a heterogeneous disease, with symptoms such as relapses, fatigue, cognitive impairment, and brain/spinal cord lesions observed on imaging in some people, but a relatively benign course in others.6 Thus, while neurologists have access to numerous disease-modifying therapies (DMTs) with different modes of action, routes of administration, and safety and efficacy characteristics, treatment often has to be individualized due to the heterogeneity in prognosis, and the time and extent of response to treatment.7
The traditional balance between efficacy and safety is often a primary factor when considering treatment choice.6,8–10 Hence, while high efficacy treatments may be reserved for patients with poor prognostic factors, additional factors such as comorbidities, family planning, risk tolerance, safety, cost, treatment sequencing, and overall patient preferences may be additional considerations for discussion between the treating physicians and their patients.7
As treatment is chronic, both clinical and patient factors need consideration. Shared decision-making between patients and their treating physician is important in ensuring that patients’ treatment matches their personal priorities and preferences in order to achieve optimal compliance and long-term disease outcomes.11 Furthermore, implementing shared decision-making is especially important since patients with MS are faced with a number of treatment options with differing benefits and risks to consider.11 Evidence in multiple disease areas has shown that patient participation in treatment decision-making can result in better treatment compliance and increased patient satisfaction.12
Aim of the Study
The objective of this study was to understand the value of including MS patients in treatment decisions, and its impact on their treatment satisfaction, QoL, and mental and physical wellbeing.
Methods
Study Design
Data were drawn from the Adelphi MS Disease Specific Program (DSP)™, a cross-sectional survey of physicians and their patients with MS, with retrospective data collection, conducted in six moderate-high income regions (France, Germany, Italy, Spain, the United Kingdom [UK], and the United States [US]) between December 2020 and July 2021. The DSP draws data from real-world clinical settings, describing current disease management, the impact of disease burden, and associated treatment effects.13–15
For this survey, neurologists and MS nurses (in the UK only) were recruited through publicly available lists, and the data collection setting was secondary care (public or private hospitals, clinics, or offices). Respondents had to be actively involved in the treatment/management of at least 16 patients with MS per month, and willing to ask patients to participate in the study. Respondents were instructed to complete a record form for up to 16 consecutive patients presenting for routine care. The patient record form contained questions on patient demographic and clinical characteristics including the Extended Disability Status Score [EDSS],16 the Charlson Comorbidity Index,17 and current and previous treatments. The form also captured physician’s attitudes and behaviors regarding the treatment of MS, particularly, how involved their patient was in the decision to prescribe their current MS therapy. Completion of the record form was undertaken through consultation of existing patient clinical records, as well as the judgement and diagnostic skills of the physician, consistent with decisions made in routine clinical practice.
Patients were eligible for inclusion if aged ≥18 years, with a physician-confirmed diagnosis of MS, and were not involved in clinical trials. Each patient with a completed record form was invited to fill out a self-completed questionnaire on a voluntary basis, and after providing informed consent. The questionnaire captured information about the patient’s involvement in deciding their currently prescribed treatment, their perspective on the treatment decision, preferred route of administration, personal experience of MS and its symptoms, and current treatment satisfaction.
Patients’ QoL and wellbeing were also assessed using the patient reported outcome measures, the EuroQoL 5 Dimension, 5 Level instrument (EQ-5D-5L and the Multiple Sclerosis Impact Scale-29 item (MSIS-29). The EQ-5D-5L is a generic multi-attribute health-state classification system by which health-related QoL is assessed in five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression.18 Respondents rate their level of impairment across the five dimensions, each with five response levels, with scores converted into a single index utility weight, from 0 (dead) to 1 (perfect health) using an algorithm based on public (societal) preferences. Respondents also completed a visual analog scale (VAS) to provide a subjective value of their health status from 0 to 100, with higher scores denoting better perceived health.
The Multiple Sclerosis Impact Scale (MSIS-29) is a measure of the physical and psychological impact of MS from the patient’s perspective. The scale is of use in the full range of impairments, disabilities, and handicaps seen in the MS population.19 MSIS-29 Psychological and Physical impact sub-scores can range from 0 to 100, with higher scores indicating worse QoL, and significant worsening defined as an increase by 8 or more points over time.20
Patients completed their questionnaires independently from physicians, returning them in sealed envelopes to ensure confidentiality. Patients were encouraged, but not mandated, to complete all questions; as missing data were not imputed, the base of patients for analysis could vary from variable to variable and is reported separately for each analysis.
Data Analysis
For the analysis of the demographic and clinical characteristics, categorical variables were summarized by frequencies and proportions, and continuous data expressed as means and standard deviations (SD), medians and interquartile ranges (IQR). Continuous variables were compared using t-tests while categorical variables were compared using Fisher’s exact or chi-squared tests.21 Since, in contrast to randomized clinical trials, observational clinical data obtained from a real-world study may not have balanced distributions of characteristics between active and control groups,22 it was therefore considered necessary to account for systematic differences in baseline characteristics between different cohorts when estimating the effect of an intervention on outcomes.
Historically, regression analysis has been employed to account for differences in measured baseline characteristics between treated and untreated subjects. In this study, propensity score methodology was implemented to account for these differences and eliminate the effects of confounding that may be present in the observational data.23 The propensity scores were derived using a logistic regression with covariates for age, sex, Charlson Comorbidity Index, EDSS, and MS diagnosis at current treatment initiation, with a standard mean difference less than 10% considered to indicate a negligible difference in the mean or prevalence of a covariate between the two cohorts.23
Subsequently, inverse probability of treatment weighting (IPTW) was used to compare treatment outcomes and wellbeing in patients who were actively involved in their current treatment decision (patient-led = “treatment” group) and those who were not involved in their current treatment decision (physician-led = “control” group). Following IPTW, regression adjustment was used on the weighted sample using the same covariates, additionally adjusting for time since initiation of current treatment. Linear regression was used to determine differences between decision groups in continuous numeric outcomes, and logistic regression was used to determine differences between decision groups in binary outcomes.
IPTW results in a pseudo-population in which the distribution of patient characteristics used to calculate the propensity score becomes independent of treatment assignment. IPTW provides an estimation of the average treatment effect (ATE), because the study population is re-weighted to assess the effects of shared decision-making in the scenario, were it available to all patients within the population.23–25 The analysis to derive estimates of the ATE after IPTW was also adjusted for the time on current treatment. All other variables used to create the propensity score were derived at the time of the treatment decision.
All analyses were performed using STATA statistical software version 17.0.26 A p-value of less than 0.05 was considered statistically significant.
Ethical Considerations
This study was non-interventional and employed retrospective data collection solely. No tests, treatments, or investigations were performed, and no identifiable protected health information was extracted during the course of the study. Using a check box, patients provided informed consent for use of their anonymized and aggregated data for research and publication in scientific journals. Data were collected in such a way that patients and physicians could not be identified directly; all data were aggregated and de-identified before receipt. The study was performed in full accordance with relevant legislation at the time of data collection, including European Pharmaceutical Marketing Research Association guidelines,27 the US Health Insurance Portability and Accountability Act 1996, and the Health Information Technology for Economic and Clinical Health Act legislation.28
Results
A total of 472 physicians (443 neurologists and 29 MS nurses) provided information on 692 patients who also submitted completed questionnaires (Europe n=471 [68.1%] and US n=221 [31.9%]). Of these patients, 75.9% were diagnosed with RRMS, 10.2% with SPMS and 13.8% with PPMS (Table 1). Patients were stratified into those who reported no involvement in treatment decision making (physician-led, n=488, 70.5%) and those who shared decision making with their physician (patient-led, n=204, 29.5%).
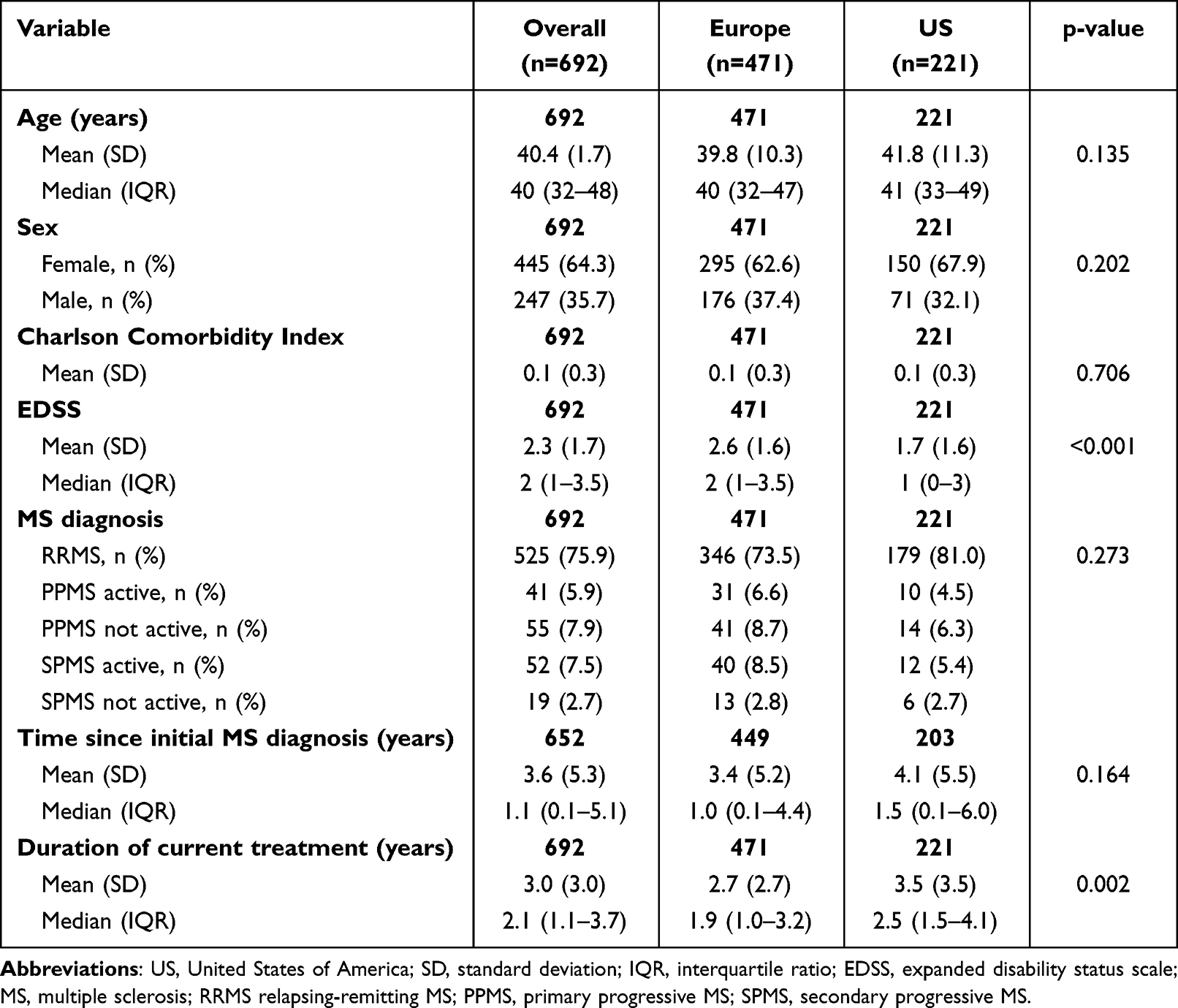 |
Table 1 Patient Demographics and Clinical Characteristics at Initiation of Current Treatment Overall, and by Geographical Location |
Overall, 64% of patients were female, with a median (IQR) age of 40 (32–48) years (Table 1). Patients had been diagnosed with MS for a mean (SD) of 3.6 (5.3) years and had been treated for a mean (SD) of 3.0 (3.0) years. Patients in Europe had more advanced disease compared to those in the US (mean [SD] EDSS 2.6 [1.6] vs 1.7 [1.6], respectively, p<0.001), consistent with the duration of treatment (Table 1). The cohort of patients with physician-led decisions were slightly older (p=0.051), with higher EDSS score (p=0.057) and longer period of treatment p=0.355), but otherwise had similar demographic and clinical characteristics as patients who were involved in treatment decision-making (Table 2).
 |
Table 2 Patient Demographics and Clinical Characteristics at Initiation of Current Treatment in the Overall Sample, and the Physician- or Patient-Led Decision-Making Cohorts |
Current disease modifying treatments (DMT) received by patients in Europe and the US are shown in Table 3. Dimethyl fumarate was the most common DMT overall (19.5% of the sample), and there were differences in the use of oral therapies overall (dimethyl fumarate, fingolimod, teriflunomide, siponimod, cladribine, and ozanimod) between the US and Europe (48.0% and 39.1%, respectively, p=0.032), while glatiramer acetate was prescribed more frequently in the US than in Europe (15.8% vs 6.8%, p<0.001), where more patients received beta-interferon 1a (15.3% vs 7.2%, p=0.003) and 1b (4.5% vs 1.4%, p=0.044) (Table 3). More patients in the US also received monoclonal antibodies such as ocrelizumab, and oral therapies such as fingolimod and teriflunomide, than in Europe, although the differences were not statistically significant (Table 3).
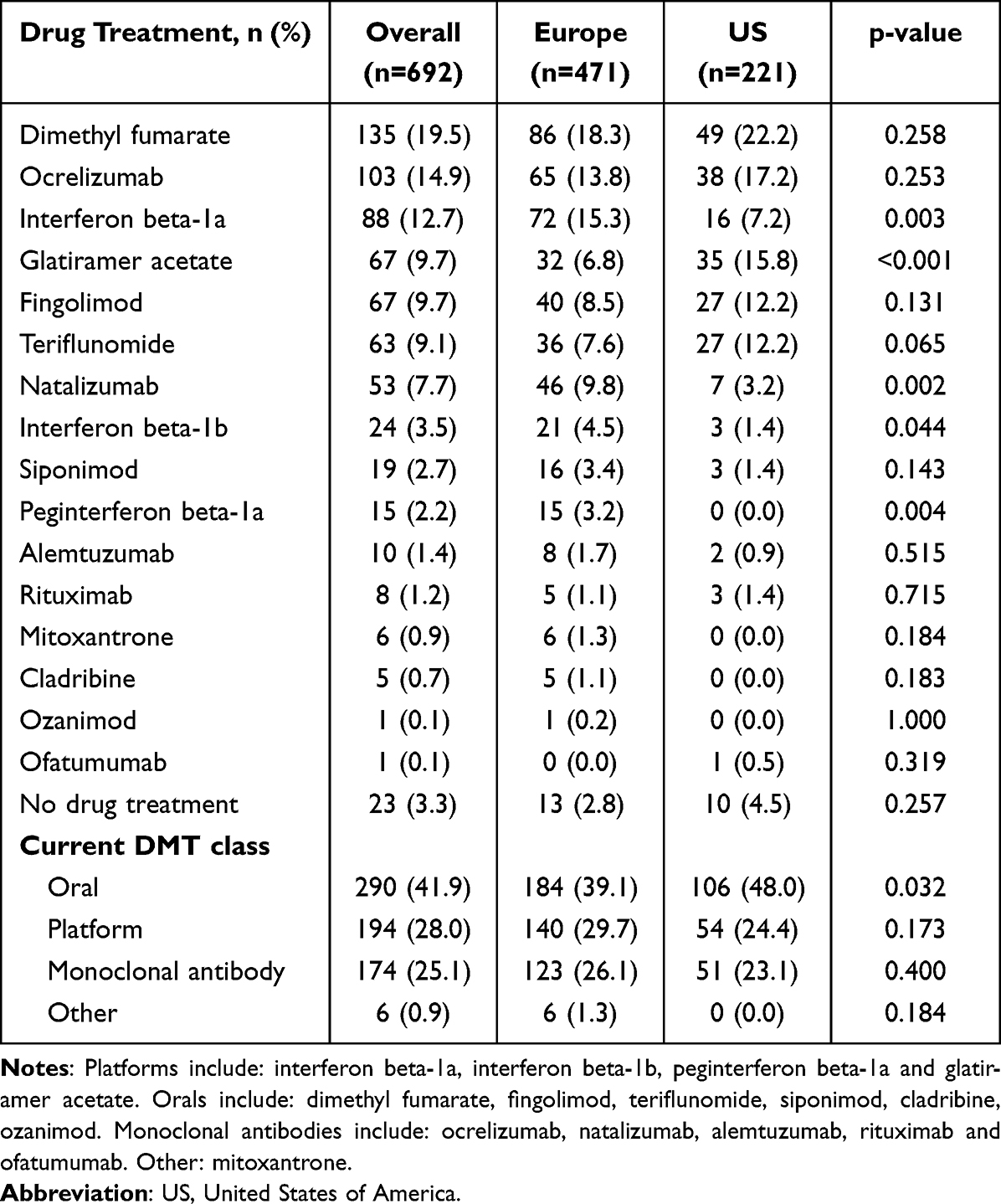 |
Table 3 Current Disease-Modifying Treatments Overall, and by Geographical Location |
When stratified into the decision-making cohorts, a greater proportion of physicians chose platform therapies than the patient-led cohort (31.8% versus 19.1% respectively, p<0.001; Table 4), while 55.9% of patients who were involved in treatment decision-making chose oral therapies such as dimethyl fumarate or teriflunomide compared with 36.1% in the physician-led cohort (p<0.001; Table 4). This pattern was also mirrored at all stages of disease severity, with monoclonal antibodies being the most common treatments chosen by patients with moderate-severe disease in both cohorts (Table 4).
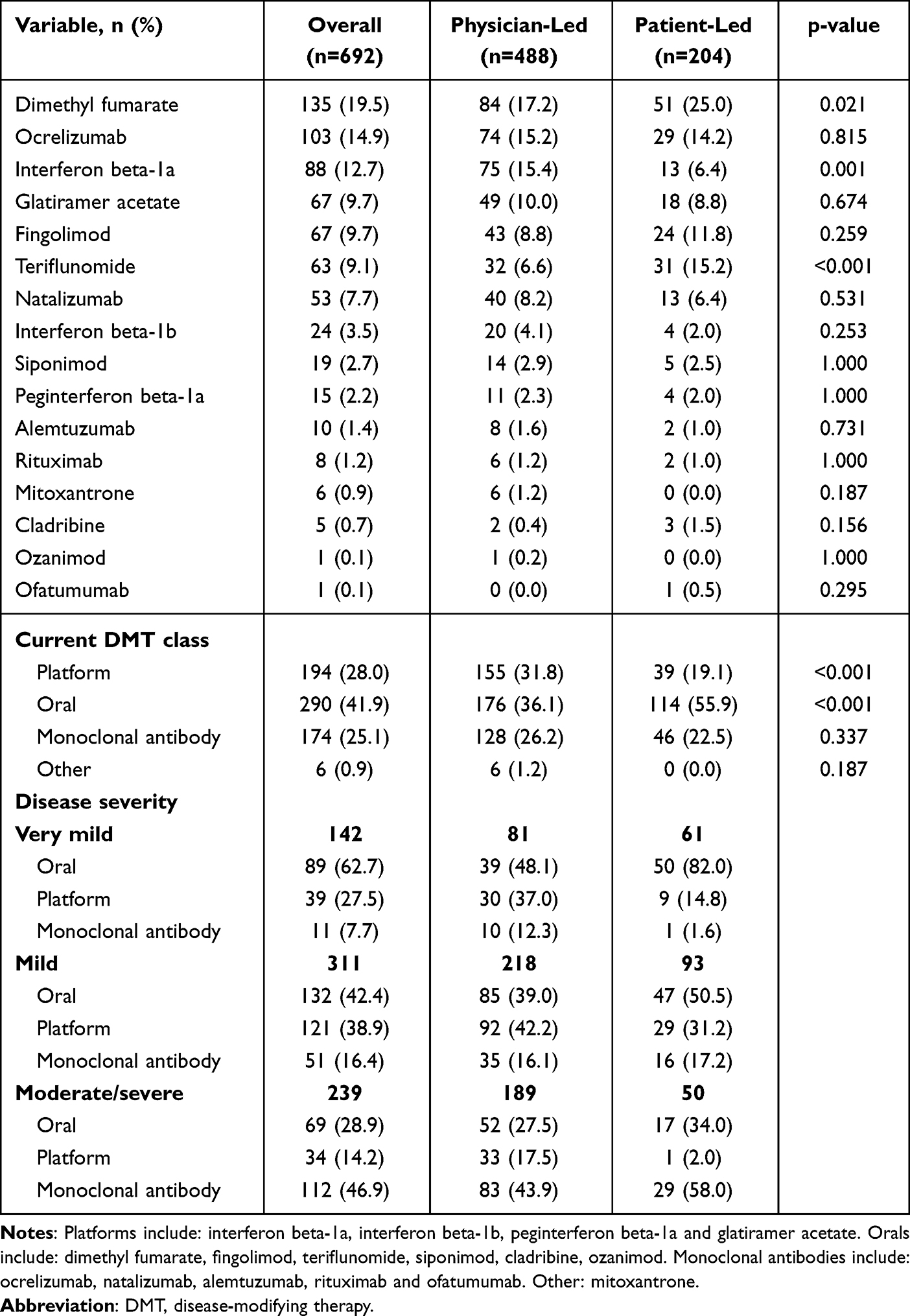 |
Table 4 Current Disease-Modifying Treatments Overall, and in the Physician- or Patient-Led Decision-Making Cohorts |
Following IPTW, there was a general trend to a positive average treatment effect in patient’s assessment of their MS status in those who were involved in their treatment decisions (Table 5). There were significant benefits in perceptions of disease severity (p=0.001), improved mental fatigue (p=0.048), particularly concentration (p=0.034), as well as confidence to proactively discuss switching treatment with their physician (p=0.028). Patients for whom physicians chose their treatment, reported greater physical and psychological impact of their MS on the MSIS-29 (p=0.017 and p<0.001, respectively; Table 5).
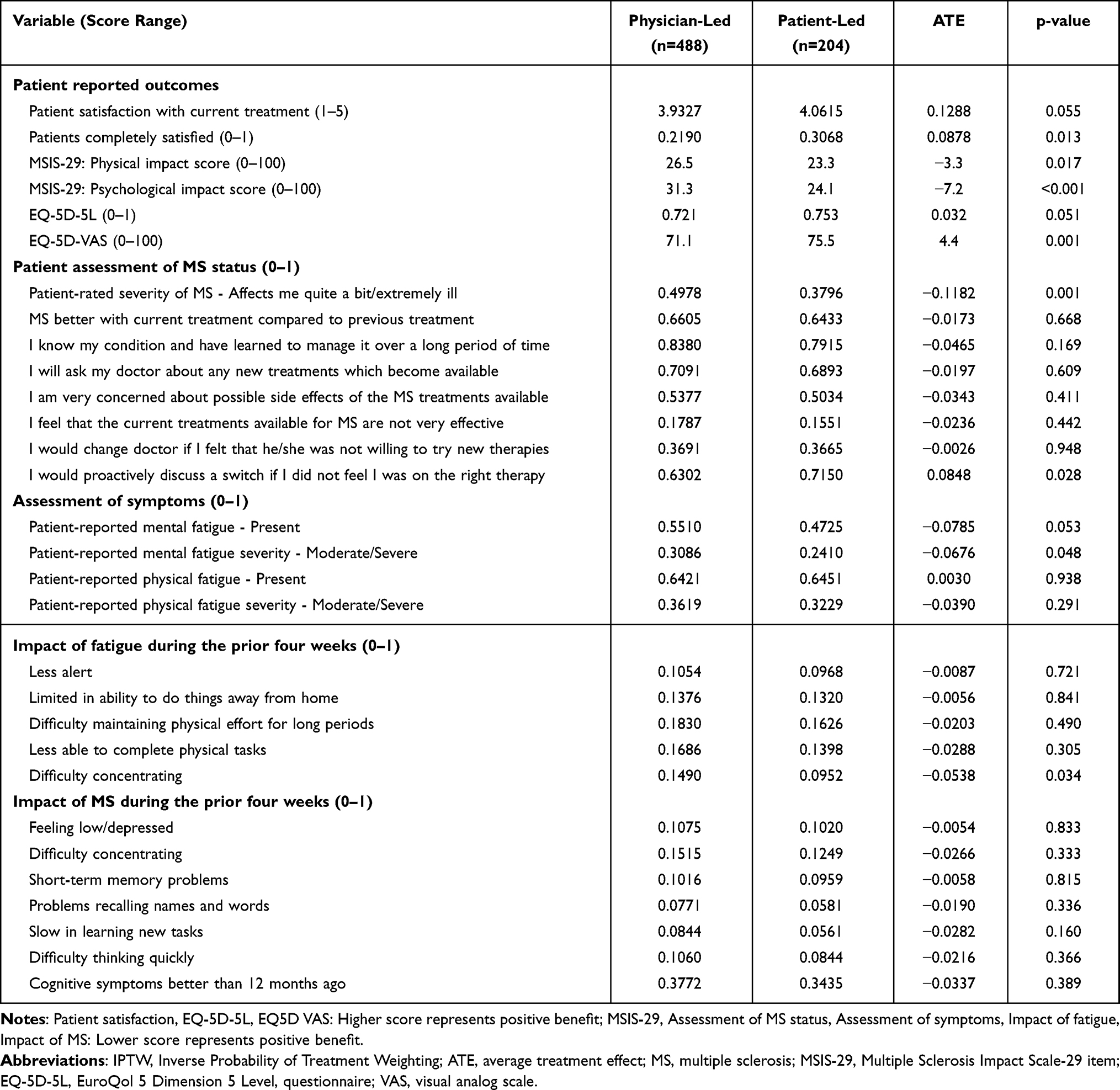 |
Table 5 Impact of Patient Involvement in Treatment Decision Making After IPTW (Total Sample) |
Overall, the benefit of shared decision-making was most apparent on patient reported outcomes, such as patient satisfaction with treatment (p=0.013), and improved wellbeing (EQ-5D-VAS, p=0.001;Table 5). This trend was also reflected in 25.8% of patients who were involved in shared decision-making in Europe (Table 6) and the 38.5% in the US (Table 7), with significantly better scores on the MSIS-29, higher scores on the EQ-5D VAS, and greater satisfaction with their treatment, while patients in the US who were involved in decisions on treatment had significantly less mental fatigue (Table 7).
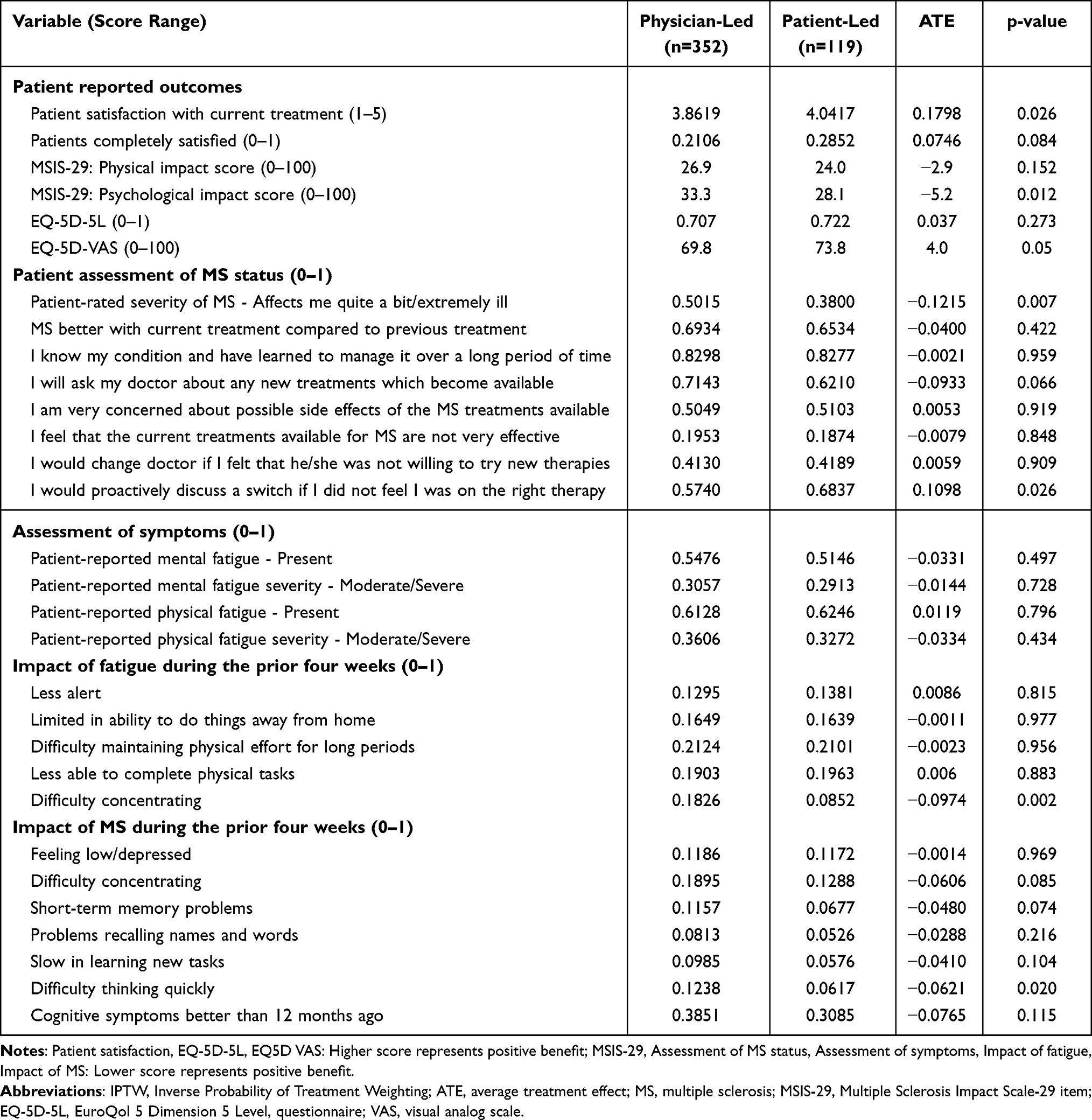 |
Table 6 Impact of Patient Involvement in Treatment Decision Making After IPTW (Europe) |
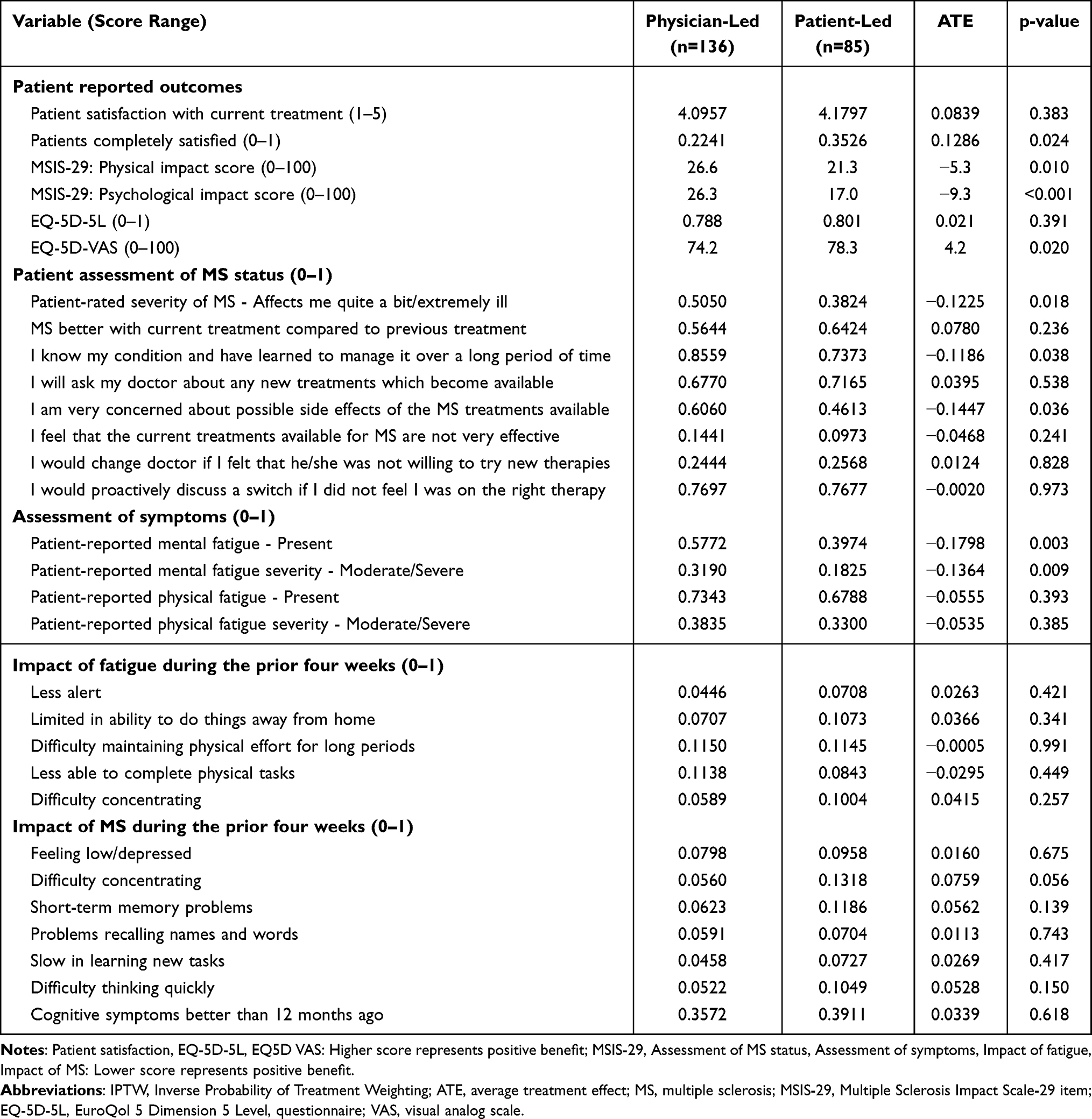 |
Table 7 Impact of Patient Involvement in Treatment Decision Making After IPTW (US) |
Discussion
MS is a life-long, chronic, relapsing and remitting, inflammatory disease with an unpredictable course, characterized by debilitating symptoms and associated with healthcare and emotional burdens that reduce patients’ quality of life and overall productivity. This study of patients with MS in Europe and the US aimed to compare disease status, treatments, and clinical outcomes in patients who were involved in deciding their treatment and those who were not, from a real-world perspective.
Our study showed that less than a third of patients were involved in decisions about their treatment. Patients who were involved in shared decision-making tended to choose an oral treatment, although monoclonal antibodies were more frequently utilized in patients with more advanced disease in both cohorts. We found that patients involved in proactive decision-making reported benefit in several symptoms, including less fatigue and improved cognitive function, as well as better overall QoL.
Our findings are consistent with a literature review which also found that patients who were involved in treatment decision-making were more likely to experience better affective-cognitive outcomes and treatment satisfaction.29 The association of shared decision-making with better satisfaction and treatment adherence has also been reported in other studies.30,31 Nevertheless, there is evidence that shared decision-making is underutilized in clinical practice in MS.11,32
MS patients and their treating physicians are a relevant model for shared decision-making owing to the need for treatment individualization and the multitude of interventions available for the physician to prescribe. Since no single optimal treatment currently exists, and treatment often has to be individualized depending on presenting symptoms and prognosis,7 therapy should be tailored to disease progression and severity.33 Optimal individualized treatment requires the treating physician to also consider the patients’ understanding and preference of treatment options.
Our study supports patient involvement in treatment decisions, indicating that physicians should encourage patient participation in the decision-making process, including providing information on treatment options, benefits, and risks, and consider patient preferences. The ultimate aim should be the implementation of an individualized treatment plan that patients are satisfied with and willing to adhere to.2,12 The potential for patients to have increased confidence in the chosen treatment through closer interaction with the physician, leading to improved outcomes, should be investigated in future studies in patients with MS.
Limitations
The survey was not based on a true random sample of physicians or patients and, while minimal inclusion criteria governed the selection of the participating physicians, participation was influenced by willingness to complete the survey. The identification of the target patient group was also based on the judgement of the respondent physician and not a formalized diagnostic checklist but is representative of the individual physician’s real-world classification of the patient. Patients were recruited at various stages of disease but, as most patients had RRMS and more advanced disease, the findings may not be representative of all patients with MS. In the data analysis, it was not feasible to correct for multiple comparisons, so those observations that were observed to be statistically significant should be viewed with caution. Moreover, the cross-sectional design of this study precludes any conclusions about causal relationships, although identification of significant associations is possible.
Conclusions
Our study highlights the importance for patients with MS to be involved in treatment decisions. The survey found that, when patients play an active role in treatment decision making, their involvement leads to improved wellbeing and QoL, and better overall treatment satisfaction. Nevertheless, our study still reported that over two-thirds of physicians lead treatment decisions with little to no shared decision-making. Future studies should continue to address the impact of shared decision-making across a variety of clinical settings, in order to encourage more patient involvement, and improve clinical outcomes.
Abbreviations
ATE, Average Treatment Effect; DMT, Disease Modifying Treatment; DSP, Disease Specific Program; EDSS, Extended Disability Status Score; EQ-5D-5L, EuroQoL 5 Dimension, 5 Level Instrument; HCPs, Healthcare Practitioner; IPTW, inverse probability of treatment weighting; IQR, Interquartile Range; MS, Multiple Sclerosis; MSIS-29, Multiple Sclerosis Impact Scale; PPMS, primary progressive multiple sclerosis; QoL, Quality of Life; RRMS, Relapsing-remitting Multiple Sclerosis; SD, Standard Deviations; UK, United Kingdom; US, United States; EQ-VAS, EuroQoL visual analog scale.
Data Sharing Statement
All data, ie methodology, materials, data and data analysis, that support the findings of this survey are the intellectual property of Adelphi Real World. All requests for access should be addressed directly to Mia Unsworth at [email protected].
Mia Unsworth is an employee of Adelphi Real World.
Ethics Approval and Informed Consent
The study was performed in accordance with relevant guidelines; ethics approval was obtained from Western Institutional Review Board, protocol number: AG8937.
Acknowledgments
Medical writing support under the guidance of the authors was provided by K. Ian Johnson BSc, MBPS, SRPharmS, Harrogate House, Macclesfield, UK on behalf of Adelphi Real World in accordance with Good Publication Practice (GPP) guidelines.34
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Janssen Pharmaceuticals Inc. did not influence the original survey through either contribution to the design of questionnaires or data collection. The analysis described here used data from the Adelphi Real World MS DSP. The DSP is a wholly owned Adelphi Real World product. Janssen Pharmaceuticals Inc. is one of multiple subscribers to the DSP. Publication of survey results was not contingent on the subscriber’s approval or censorship of the manuscript.
Disclosure
AK (Scientific Affairs), HHL (Scientific Affairs), KG (Research Development), and LA are employees of Janssen Pharmaceuticals Inc. EJ, MU, JP, and ET are employees of Adelphi Real World. AK, HHL, KG and LA are employees of Janssen Pharmaceuticals Inc., part of Johnson and Johnson group of companies and holds stock/stock options of Johnson and Johnson. EJ, MU, JP and ET are employees of Adelphi Real World. The authors report no other conflicts of interest in this work.
References
1. Battaglia MA, Bezzini D, Cecchini I, et al. Patients with multiple sclerosis: a burden and cost of illness study. J Neurol. 2022;269(9):5127–5135. doi:10.1007/s00415-022-11169-w
2. Kremer IEH, Jongen PJ, Evers S, Hoogervorst ELJ, Verhagen WIM, Hiligsmann M. Patient decision aid based on multi-criteria decision analysis for disease-modifying drugs for multiple sclerosis: prototype development. BMC Med Inform Decis Mak. 2021;21(1):123. doi:10.1186/s12911-021-01479-w
3. Stenager E. A global perspective on the burden of multiple sclerosis. Lancet Neurol. 2019;18(3):227–228. doi:10.1016/s1474-4422(18)30498-8
4. Walton C, King R, Rechtman L, et al. Rising prevalence of multiple sclerosis worldwide: insights from the Atlas of MS, third edition. Mult Scler. 2020;26(14):1816–1821. doi:10.1177/1352458520970841
5. Pérez de Heredia-Torres M, Huertas-Hoyas E, Sánchez-Camarero C, et al. Occupational performance in multiple sclerosis and its relationship with quality of life and fatigue. Eur J Phys Rehabil Med. 2020;56(2):148–154. doi:10.23736/s1973-9087.20.05914-6
6. Van Wijmeersch B, Hartung HP, Vermersch P, et al. Using personalized prognosis in the treatment of relapsing multiple sclerosis: a practical guide. Front Immunol. 2022;13:991291. doi:10.3389/fimmu.2022.991291
7. Rotstein D, Montalban X. Reaching an evidence-based prognosis for personalized treatment of multiple sclerosis. Nat Rev Neurol. 2019;15(5):287–300. doi:10.1038/s41582-019-0170-8
8. Araujo L, Geertsen SS, Amedume A, Higuchi K, van Wingerden J. Persistence; adherence, and switching to higher-cost therapy in patients with multiple sclerosis initiating oral disease-modifying therapies: a retrospective real-world study. Neurol Ther. 2022;11(4):1735–1748. doi:10.1007/s40120-022-00404-1
9. Samjoo IA, Worthington E, Drudge C, et al. Efficacy classification of modern therapies in multiple sclerosis. J Comp Eff Res. 2021;10(6):495–507. doi:10.2217/cer-2020-0267
10. Yang JH, Rempe T, Whitmire N, Dunn-Pirio A, Graves JS. Therapeutic advances in multiple sclerosis. Front Neurol. 2022;13:824926. doi:10.3389/fneur.2022.824926
11. Colligan E, Metzler A, Tiryaki E. Shared decision-making in multiple sclerosis. Mult Scler. 2017;23(2):185–190. doi:10.1177/1352458516671204
12. Cofield SS, Thomas N, Tyry T, Fox RJ, Salter A. Shared decision making and autonomy among US participants with multiple sclerosis in the NARCOMS registry. Int J MS Care. 2017;19(6):303–312. doi:10.7224/1537-2073.2016-091
13. Anderson P, Benford M, Harris N, Karavali M, Piercy J. Real-world physician and patient behaviour across countries: disease-specific programmes - A means to understand. Curr Med Res Opin. 2008;24(11):3063–3072. doi:10.1185/03007990802457040
14. Babineaux SM, Curtis B, Holbrook T, Milligan G, Piercy J. Evidence for validity of a national physician and patient-reported, cross-sectional survey in China and UK: the disease specific programme. BMJ Open. 2016;6(8):e010352. doi:10.1136/bmjopen-2015-010352
15. Higgins V, Piercy J, Roughley A, et al. Trends in medication use in patients with type 2 diabetes mellitus: a long-term view of real-world treatment between 2000 and 2015. Diabetes Metab Syndr Obes. 2016;9:371–380. doi:10.2147/dmso.S120101
16. Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology. 1983;33(11):1444–1452. doi:10.1212/wnl.33.11.1444
17. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
18. Devlin NJ, Brooks R. EQ-5D and the EuroQol Group: past, present and future. Appl Health Econ Health Policy. 2017;15(2):127–137. doi:10.1007/s40258-017-0310-5
19. McGuigan C, Hutchinson M. The multiple sclerosis impact scale (MSIS-29) is a reliable and sensitive measure. J Neurol Neurosurg Psychiatry. 2004;75(2):266–269.
20. Phillips GA, Wyrwich KW, Guo S, et al. Responder definition of the multiple sclerosis impact scale physical impact subscale for patients with physical worsening. Mult Scler. 2014;20(13):1753–1760. doi:10.1177/1352458514530489
21. Armitage P, Berry G, Matthews JNS. Statistical Methods in Medical Research. Blackwell Science Ltd; 2002.
22. Franchetti Y. Use of propensity scoring and its application to real world data: advantages, disadvantages, and methodological objectives explained to researchers without using mathematical equations. J Clin Pharmacol. 2021. doi:10.1002/jcph.1989
23. Austin PC, Stuart EA. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat Med. 2015;34(28):3661–3679. doi:10.1002/sim.6607
24. Allan V, Ramagopalan SV, Mardekian J, et al. Propensity score matching and inverse probability of treatment weighting to address confounding by indication in comparative effectiveness research of oral anticoagulants. J Comp Eff Res. 2020;9(9):603–614. doi:10.2217/cer-2020-0013
25. Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res. 2011;46(3):399–424. doi:10.1080/00273171.2011.568786
26. StataCorp LLC. Stata Statistical Software: Release 17. StataCorp LLC; 2021.
27. EphRMA. European Pharmaceutical Market Research Association (EphMRA) code of conduct 2019; 2019. Available from: http://www.ephmra.org/Code-of-Conduct-Support.
28. Rosenbloom ST, Smith JRL, Bowen R, Burns J, Riplinger L, Payne TH. Updating HIPAA for the electronic medical record era. J Am Med Inform Assoc. 2019;26(10):1115–1119. doi:10.1093/jamia/ocz090
29. Shay LA, Lafata JE. Where is the evidence? A systematic review of shared decision making and patient outcomes. Med Decis Making. 2015;35(1):114–131. doi:10.1177/0272989x14551638
30. Ben-Zacharia A, Adamson M, Boyd A, et al. Impact of shared decision making on disease-modifying drug adherence in multiple sclerosis. Int J MS Care. 2018;20(6):287–297. doi:10.7224/1537-2073.2017-070
31. Koudriavtseva T, Onesti E, Pestalozza IF, Sperduti I, Jandolo B. The importance of physician-patient relationship for improvement of adherence to long-term therapy: data of survey in a cohort of multiple sclerosis patients with mild and moderate disability. Neurol Sci. 2012;33(3):575–584. doi:10.1007/s10072-011-0776-0
32. Hawkes N. Seeing things from the patients’ view: what will it take? BMJ. 2015;
33. Jonker MF, Donkers B, Goossens LMA, et al. Summarizing patient preferences for the competitive landscape of multiple sclerosis treatment options. Med Decis Making. 2020;40(2):198–211. doi:10.1177/0272989x19897944
34. DeTora LM, Toroser D, Sykes A, et al. Good Publication Practice (GPP) guidelines for company-sponsored biomedical research: 2022 update. Ann Intern Med. 2022;175(9):1298–1304. doi:10.7326/m22-1460
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Practice of Shared Decision-Making Among Physiotherapists and Patients with Musculoskeletal Conditions
Alotaibi MA, Alhowimel AS, Alodaibi FA, Aloraifi M
Journal of Multidisciplinary Healthcare 2023, 16:2655-2665
Published Date: 8 September 2023
Preferences, Adherence, and Satisfaction: Three Years of Treatment Experiences of People with Multiple Sclerosis
Hoffmann O, Paul F, Haase R, Kern R, Ziemssen T
Patient Preference and Adherence 2024, 18:455-466
Published Date: 22 February 2024
Patient Experiences with the Impacts of Multiple Sclerosis & Disease-Modifying Therapies
Talente B, Finseth LT, Blake N, Costello K, Schmidt H, Vandigo J, Oehrlein EM
ClinicoEconomics and Outcomes Research 2025, 17:199-215
Published Date: 15 March 2025
Neurologists’ Openness to Evidence-Based Innovation in Multiple Sclerosis Care: Individual and Structural Determinants
Monreal E, Gómez-Ballesteros R, Meca-Lallana V, Caminero AB, Meca-Lallana JE, Martínez-Yélamos S, Landete L, García-Domínguez JM, Agüera E, García-Arcelay E, Medrano N, Villar LM, Maurino J
Neuropsychiatric Disease and Treatment 2025, 21:1523-1531
Published Date: 29 July 2025
Factors Influencing Decision-Making and Rehabilitation Among Older Women Who Underwent Total Knee Replacement: A Qualitative Study in Taiwan
Huang CH, Chen YY, Chen SW, Wang CT, Lin MH
Patient Preference and Adherence 2025, 19:3931-3944
Published Date: 9 December 2025