Back to Journals » Patient Preference and Adherence » Volume 17
Exploring the Important Determinants Shaping Treatment Preferences: Qualitative Insights into Breast Cancer Patient Experiences and Perspectives in New Zealand
Authors Yeo HY ![]() , Wong JHY, Chan SJ, Latu ATF, Han CH
, Wong JHY, Chan SJ, Latu ATF, Han CH ![]() , Anwar M
, Anwar M ![]() , Marra CA
, Marra CA ![]()
Received 11 October 2023
Accepted for publication 19 December 2023
Published 22 December 2023 Volume 2023:17 Pages 3525—3537
DOI https://doi.org/10.2147/PPA.S443217
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Hui Yee Yeo,1,2 Jacqueline Hui Yi Wong,3 Suz Jack Chan,1 Anna Tiatia Fa’atoese Latu,1 Catherine H Han,4,5 Mudassir Anwar,1 Carlo A Marra1
1School of Pharmacy, University of Otago, Dunedin, New Zealand; 2Clinical Research Center, Hospital Seberang Jaya, Seberang Jaya, Penang, Malaysia; 3Pharmacy Department, Hospital Kuala Lumpur, Kuala Lumpur, Malaysia; 4Auckland Oncology, Auckland, New Zealand; 5Faculty of Medical and Health Sciences, University of Auckland, Auckland, New Zealand
Correspondence: Carlo A Marra, School of Pharmacy, University of Otago, PO Box 56, Dunedin, 9054, New Zealand, Tel +64-34797275, Fax +64-34797034, Email [email protected]
Purpose: Despite the importance of acknowledging patient preferences in treatment decision-making, little is known about the treatment preferences and the factors underlying those preferences of breast cancer patients. This study aims explore patient experience and perspective regarding treatment preferences and identify the important determinants that shape these preferences in the context of New Zealand.
Patients and Methods: Semi-structured online interviews comprised of six focus group discussions and five individual interviews were performed with 26 breast cancer patients. The interviews were recorded, transcribed, and analyzed using the reflexive thematic analysis approach.
Results: Four main themes were derived: (1) positive treatment outcomes; (2) the negative impact of treatment-related side effects on quality of life; (3) treatment accessibility, availability, and timeliness; (4) cost of treatment. Patients revealed a strong preference towards treatments that yield longer survival, achieve remission, and prevent cancer recurrence. Additionally, patients favored treatments with minimal side effects that had minimal impact on their quality of life. There was a notable preference for treatments that were easily accessible and available in a timely manner. However, patients faced challenging decisions in balancing the costs of treatments with their benefits, leading to a consistent preference for treatments supported by government funding or medical insurance to alleviate financial burdens.
Conclusion: Our study reveals that breast cancer patients in New Zealand have different perceptions and preferences regarding cancer treatment. Patients frequently find themselves making trade-offs among various attributes of a treatment, aligning these decisions with their personal values and beliefs. By considering these preferences and trade-offs in future studies that measure patient preferences, healthcare professionals can enhance their support for patients in making informed choices that align with their values and priorities. Additionally, healthcare policymakers can develop patient-centered policies that cater to the unique needs and preferences of breast cancer patients.
Plain Language Summary: Breast cancer is a significant health concern in New Zealand, affecting both the well-being of patients and their families. Despite advancements in treatment, patient preferences regarding treatment risks and benefits are often neglected. This study aims to bridge this knowledge gap by qualitatively exploring the unique experiences and preferences of breast cancer patients in New Zealand, shedding light on the factors influencing their treatment decisions. The study involved a series of interviews with a group of 26 women living with breast cancer. The interview revealed four main themes that shape patients’ preferences for breast cancer treatment:
1. Positive outcomes: Patients revealed a strong preference towards treatments that yield longer survival, achieve remission, and prevent cancer recurrence.
2. Quality of life: Treatment-related side effects negatively impacted patients’ quality of life, affecting them physically, mentally, emotionally, spiritually, and psychosocially. Patients preferred a treatment that entailed few side effects with minimal impact on their quality of life.
3. Treatment accessibility and timeliness: Patients expressed concerns about administrative complexities, long distances to healthcare facilities, timely treatment, and restricted access to treatment options in the country. There was a notable preference for treatments that were easily accessible and available in a timely manner.
4. Cost of treatment: Balancing the cost of treatments with their benefits posed challenging decisions for patients, who consistently voiced a preference for treatments supported by government funding or medical insurance.
The study highlights diverse perspectives and preferences among breast cancer patients in New Zealand about treatment preference. Patients frequently find themselves making trade-offs concerning various attributes of a treatment that align with their individual values and beliefs. Integrating these preferences and trade-offs into future studies and healthcare policies can help healthcare professionals and policymakers better support patients in making informed choices aligned with their values, fostering a more patient-centered healthcare system.
Keywords: qualitative research, patient preference, breast cancer, reflexive thematic analysis, treatment preference, treatment decision-making
Introduction
Breast cancer (BC) is the third most common cancer in New Zealand (NZ) with high morbidity and mortality rates.1 Living with both the cancer diagnosis and the accompanying treatment-related side effects exerts tremendous physical and psychological impacts on the lives of patients. Numerous studies have consistently demonstrated that women diagnosed with BC often experience a diminished quality of life (QoL), changes in body image and sexuality, and emotional distress.2–4 Moreover, BC creates a significant emotional burden not only on the patients themselves but also on their families, compounded by the fear of the potential loss of their loved ones.5,6
Advancements in BC treatment have positively impacted patient outcomes. Nevertheless, the decision-making process for BC treatment is largely steered by physicians, and there is limited understanding of patients’ preferences regarding the risks and benefits associated with various treatment options. The preference for specific features among different treatment choices is a subjective matter influenced by a multitude of cultural and personal factors. It is well-established that both patients and healthcare providers exhibit varying preferences when it comes to the treatment of different diseases, including cancer.7 In recent years, there has been increasing recognition of the significance of patient preference in both individual treatment decision-making and the development of public health policies. Patient preferences, which encompass their risk perceptions and overall comfort levels with different treatment approaches, are considered paramount in guiding the selection of treatments.8,9
To the best of our knowledge, there is a lack of qualitative research conducted that explores the unique experiences towards treatment preferences of BC patients, especially in the context of NZ. Existing studies have predominantly focused on aspects such as patients’ experiences with the disease and coping strategies, patient-reported outcome measures, preferences for non-pharmacological treatment, or treatment preferences from the perspective of healthcare providers.10–14 Consequently, there is a significant gap in understanding how concerns about the potential benefits and risks of BC treatment may influence treatment preferences among patients. Addressing this knowledge gap would provide invaluable insights into the decision-making processes of BC patients, ultimately enhancing the delivery of patient-centered care in NZ. Incorporating patient-centered care into the treatment and management of BC not only enhances the effectiveness and adherence to treatment but also enables healthcare providers to make well-informed decisions regarding the most appropriate therapies for individual patients, considering their unique preferences.15 Therefore, this study aims to examine the unique experiences of BC patients regarding their cancer treatment, with a focus on the attributes that contribute to the treatment preferences or decision-making from BC patients’ perspectives.
Materials and Methods
This study utilized a qualitative research approach to gain insight into the treatment experiences and preferences from BC patients’ perspectives. This study adhered to the Consolidated Criteria for Reporting Qualitative Studies (COREQ, Supplementary Table 1).16 The study was approved by the Southern Health and Disability Ethics Committees (Approval number 21/STH/41).
Participants
A purposive sampling strategy was employed to recruit participants from both Auckland Oncology (private clinic) and BC clinics at Middlemore Hospital (public hospital) to include a diverse spectrum of socio-cultural backgrounds and different stages of BC to minimize selection bias. To be eligible for inclusion, individuals had to be diagnosed with a primary BC, 18 years or older, proficient in reading and speaking English, and resided in NZ. Prospective participants who met the inclusion criteria were approached by LB, who served as both an oncology nurse and a research assistant. Those who expressed interest in participating received an email invitation that included an information sheet outlining the study’s objectives, followed by a comprehensive explanation of the nature of participation and the potential risks and benefits involved. Participants were assured that their information would be managed anonymously and treated with strict confidentiality. Initial explanations were conducted over the phone by HYY to establish a relationship, and arrangements were made for a preferred date and time for the interviews. All participants provided informed written consent through email correspondence prior to the commencement of the interviews.
Focus Group Discussion (FGD) and in-Depth Interview (IDI)
To enhance the depth, breadth, and validity of the qualitative research, a combination of two independent data collection methods (FGD and IDI) was employed. Each FGD was moderated by one of three female facilitators: HYY (PhD candidate), AL (senior lecturer), or AR (research assistant). All the IDIs were moderated by HYY. In each FGD or IDI, one of the three facilitators functioned as a co-moderator to facilitate the interview and make field notes regarding nonverbal cues and observed dynamics. Before the data collection, all facilitators participated in a 1-day training session led by HYY. The purpose of this training session was to provide an in-depth understanding of the study’s objectives and familiarize the facilitators with the interview questions. Due to the Covid-19 pandemic restrictions, all the interviews were conducted online over videoconferencing (Zoom Video Communications Inc., 2016), ensuring safety and adherence to health guidelines.
In both FGD and IDI sessions, a semi-structured interview guide, which included pre-planned open questions, prompts, and responsive follow-up questions, was employed (Supplementary Table 2) to facilitate a patient-led discussion whilst ensuring all key areas were covered. The interview guide was developed from a review of the literature and discussion among the experts in oncology and patient preference.17 Throughout the interview process, the guide was modified iteratively based on insights gained from earlier participants to ensure that the additional relevant attributes were adequately addressed in subsequent interviews. A total of six FGDs and five IDIs were conducted. The average durations of FGDs and IDIs were 84 min (range 75–190 minutes) and 56 minutes (range 49–62 minutes), respectively. All interviews were audio-recorded and transcribed verbatim without any identifying information. All transcripts were reviewed for accuracy by the research team. In addition, to ensure accuracy and validity in transcription and interpretation, the transcripts were further subjected to a member check method. This involved providing the interviewees with a transcript of their respective interviews and inviting them to review the content. During this process, the interviewees had the opportunity to verify the accuracy of the transcribed words and expressions, as well as provide feedback on the team’s interpretation of their statements. This member-check method played a crucial role in enhancing the overall validity and reliability of the study’s findings.18 The recruitment and interview were discontinued when sufficient information power was achieved, and no new categories, themes, or explanations appeared in the latter interviews.19,20
Data Analysis
Data were analyzed in NVivo software (v12.6, QRS International) employing reflexive thematic analysis (RTA).19,21 RTA was chosen as this method was not bound by specific theoretical and epistemology boundaries, and it recognizes and acknowledges the influence of the researchers’ subjective interpretation in shaping the final thematic structure. Rigor was upheld through triangulating multiple sources of data, detailed conduct according to the study methodology, immersion in data, reflexive analysis, and application of peer debriefing, review, and feedback between team members.22 The analysis of the data was approached from a realist perspective by assuming participants’ response reflects their communicated experience and intended meaning to determine themes relating to their perspective on BC.23 The analysis process began with repeated listening to the audio files and reading of the transcripts by HYY and HYW, independently, to gain familiarity with the data. Subsequently, HYY generated an initial coding framework based on the key concepts and ideas within the data, which were then reviewed by HYW. This initial coding framework was further developed and grouped into themes and sub-themes using an inductive approach without a pre-existing coding framework. To ensure the accuracy and validity of the final thematic structure deemed representative of the participant’s preference for BC treatment, an iterative process of ongoing discussions and feedback was implemented. In addition to the discussions between HYY and HYW, other members of the research team (SJC, CM, MA, AL, and CH) also provided valuable feedback and input, contributing to the confirmation of the final thematic structure.24
Following the data analysis, the lead researcher HYY proposed that the theme related to the “unmet needs and support mechanism” be analyzed separately due to the immense information power gathered. After extensive discussion, the research team collectively decided to present this theme as a separate study. Therefore, this paper focuses solely on reporting the preference for BC treatment, while the findings pertaining to the unmet needs and support mechanisms experienced by BC patients will be reported in a subsequent article. This approach allows for a more comprehensive and focused analysis of each aspect, providing greater clarity and depth to the findings.
Results
A total of 46 women with BC were invited to participate, of whom 20 declined to participate or did not respond. Among the reasons to decline participation were no access to virtual interviews or work commitments. The study eventually included a total of 26 women, where 21 women who participated in FGDs and 5 women were involved in IDIs. The characteristics of the 26 participants are presented in Table 1. Their mean age was 58 (range 37–76). The participants were a diverse group, consisting of 14 individuals of NZ European descent, 7 of Asian descent, 3 of Māori descent, and 2 of Pacific Islander descent. The predominant diagnosis among the participants was early BC, accounting for 65.4% of the cases.
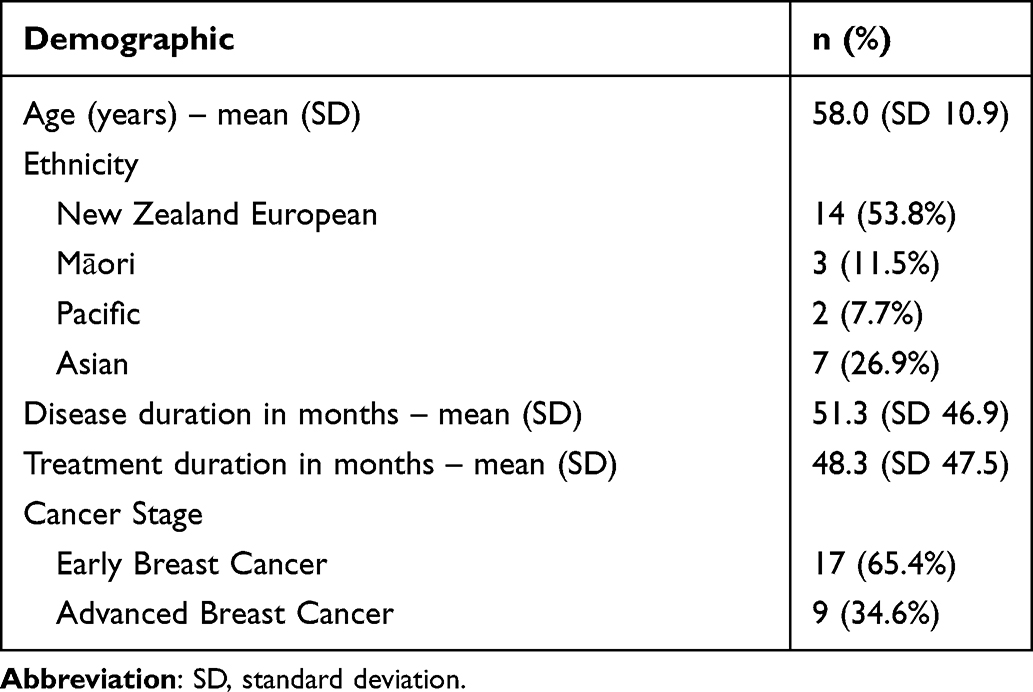 |
Table 1 Characteristics of the FGD and IDI Participants, N=26 |
Thematic Analysis
A total of four distinct but related themes were conceptualized from the RTA, revealing the specific attributes that played a pivotal role in shaping treatment preferences for BC: (1) Positive treatment outcomes, (2) The negative impact of treatment-related side effects on QoL, (3) Accessibility, availability, and timeliness of treatment, and (4) Cost of treatment. The presentation of our results is structured according to these four themes and characterized by fourteen sub-themes.
Theme 1: Positive Treatment Outcomes
The desire for positive treatment outcomes in terms of extended survival, a state of cancer-free, or the prevention of cancer recurrence is a critical aspect of cancer care. While most patients were aware of the potential consequences of BC treatments and expressed a general willingness to endure treatment-related adverse events for the sake of positive treatment outcomes, it is important to note that some patients were not willing to make trade-offs when it came to the potential reduction in QoL associated with the treatment-related side effects.
Survival
Women with BC revealed their varied perspectives on the survival benefits of anticancer treatment. While some patients expressed a willingness to undergo harsh treatments to ensure survival, others focused on their desire to extend their lives as much as possible through treatment.
I don’t mind going through a hard treatment, … it’s more important for me to survive. (Participant K5)
Participant F9 acknowledged the fact that her cancer was incurable but remained optimistic about the treatment benefits. However, participant F12 highlighted the significance of considering the impact on QoL when making treatment decisions, questioning the value of an extended lifespan if it compromises overall well-being.
When I saw the oncologist, she said that this is not curable, but it’s treatable. … so why not? I’ll get the treatment. It doesn’t matter whether it’s for a day or for a year. (Participant F9)
I was given the pills … but the life they were making me lead was not a life. It was anxiousness and depressive and not being able to get out of bed and not feeding myself. Now, if that’s a medication to take to give me an extra year (of life), is it worth it? No! (Participant F12)
Cancer-Free or a State of Remission
Patients with BC expressed the desire to achieve a state of cancer-free or cancer remission. Participant K5 articulated her wish for a magic treatment that guarantees complete healing and prevention of cancer recurrence.
If there’s a magic medicine or treatment, that I go through this treatment and guarantee that my cancer won’t come back, and it’s completely healed, that would be wonderful. (Participant K5)
Disease-free survival is highly valued by patients, and radical interventions such as mastectomy are considered justifiable if they ensure the elimination of all signs of cancer.
… having a mastectomy, to me that was radical treatment, but … took it all out and … there’s no sign of any cancer afterward. (Participant F1)
That was quite an easy decision for me to make, to have the mastectomy. … because that gave me the best chance of surviving without cancer. (Participant F4)
Prevent Cancer Recurrence
BC patients expressed a significant fear of cancer recurrence and highlighted the crucial role of treatment effectiveness in preventing such recurrence. The presentation of the reduced risk of cancer recurrence associated with chemotherapy by oncologists in treatment decision-making played a decisive role in the patient’s choice to proceed with chemotherapy. Some patients emphasized the persistent anxiety related to the possibility of cancer recurrence, which was described as the most challenging aspect of their experience, reflecting the emotional burden and ongoing concern associated with the disease.
I was told (chemotherapy) was an extra 5% of the cancer not returning, then that’s probably why we decided to go with the chemo. (Participant K4)
The anxiety that keeps coming back to me is the fact that you’re going to have the recurrence, especially if you’re high candidate of having a recurrence. That’s the most challenging part for me. (Participant F14)
Theme 2: The Negative Impact of Treatment-Related Side Effects on QoL
At some point in their cancer treatment, patients encountered challenges about recovering from surgery or dealing with side effects from treatments. These difficulties had a profound impact on their overall QoL, affecting their physical, mental, emotional, spiritual, and psychosocial well-being. Women consistently expressed a preference for treatments characterized by minimal side effects, emphasizing the importance of preserving their current QoL.
Physical Wellbeing
Participants expressed that the impact of BC and cancer treatment have affected their daily living activities such as the ability to self-care, ability to work leading to a loss of sense of dignity and self-worth. Women expressed their fear of experiencing physical disability because of BC and its treatment.
The only thing that affected my life is I’m not able to work. I used to work in a printing place, and I’m not allowed to work because it’ll affect my back and arm. (Participant F10)
My husband for a long time was having to take me and shower me and I felt terrible. And he’d take me out of the shower, and I’d have to lie on the floor, and he would say, Get off the floor, it’s dirty. And I just didn’t care. I couldn’t stand. (Participant F12)
The fear of losing mobility and the ability to pursue activities that bring them joy and maintain their physical well-being is evident.
My biggest fear is if I had physical disability. I like to do exercises and so if I can’t do those things, I think my quality of life will be very low. (Participant K2)
Mental and Emotional Wellbeing
The younger patients discussed the emotional impact of losing their eyebrows or hair, or weight gain as the result of treatment-related side effects. They experienced a sense of unattractiveness due to the change in appearance, resulting in a profound impact on their self-esteem and overall emotional well-being. Participant F5 expressed how this distress inflicted upon them that they experienced suicidal ideation.
As soon as you lose your eyebrows, you just look like a ghost… I found them not good for me mentally. (Participant F4)
I feel like I’ve put on weight with the medication and stuff… I’ve never been this big, even when I was pregnant. But my weight is very important to me. (Participant K4)
… it was too awful to continue with. Because I actually felt suicidal. I actually felt like topping myself, it was that bad. (Participant F5)
On the other hand, participant F9 expressed her gratitude for the present treatment, considering it an improvement over previous therapy. She expressed appreciation for the positive experiences and has found joy in various aspects of their lives while maintaining a hopeful mindset.
Maybe the treatment is not as harsh as before … and I’m very thankful that I can eat, sleep pee, and poo normally, which is so good. I can’t complain. And every morning I wake up, I’m very thankful that life is quite long, despite still going on the chemotherapy. (Participant F9)
Spiritual Wellbeing
Māori patients consistently emphasized the importance of spiritual and mental well-being as significant aspects of their overall health. They underscored the necessity for healthcare providers to address their holistic well-being, recognizing that it encompasses more than just physical health.
I have always felt like my people looking after me have cared about me as a whole person, but I’ve never really been asked directly about my wairua (spirit) and hinengāro (mental wellbeing) and stuff, which as a Māori person is important. (Participant K1)
Participant F10 further highlighted the profound impact of spirituality and religious practices in providing emotional support and alleviating pain and anger during challenging times.
I was always angry at being in pain. … when I was able to go to church on Sunday that was my me time. I’d go to the service because I love singing. And I love listening to the choir and singing along and the preachers and it just kind of calmed me down. (Participant F10)
Psychosocial Wellbeing
Participants F11 and F14 expressed the difficulties they face in maintaining family bonds and fulfilling personal responsibility due to cancer and the accompanying treatments. The physical separation from their loved ones has posed a considerable challenge and has resulted in feelings of distress.
That’s the only thing that’s affected having cancer and traveling to visit my children. … and I’m banning most of my family too. So, there’s no physical communication with the family, which I used to have. (Participant F11)
(my children) deserve to have a mother, I want to be there while they are growing. … be able to cook meals for my family is already substantial and I feel like I’m already serving my purpose as a mother, as a wife. (Participant F14)
For those in marital relationships, the cancer treatment has led to substantial changes in the realms of sexuality and social interactions, leading to a profound sense of diminished intimacy.
My libido dropped dramatically. And I craved it, social touch. So that’s been incredibly difficult. It’s a little bit like sexual intimacy. I actually love the social context. (Participant F4)
Theme 3: Accessibility, Availability, and Timeliness of Treatment
Timely and equitable access to BC treatment plays a crucial role in achieving favorable treatment outcomes. Within this context, participants have discussed their diverse experiences and preferences concerning receiving treatment from both public and private healthcare facilities in NZ.
Treatment Accessibility
Participant F4 expressed her frustration with the bureaucratic obstacles and administrative complexities trying to transfer between treatment centers and these have hindered her access to healthcare services.
(transfer between treatment centers) they said it was way too much paperwork and a district nurse couldn’t do it down there because the amount of paperwork wasn’t worth it. And I just found that frustrating. (Participant F4)
Among the challenges encountered by participants during their treatment, the significant distance between their homes and the treatment centers emerged as a prominent issue. This issue was particularly burdensome for patients residing in remote areas of NZ. The participants expressed their desire for a more accessible healthcare system, where shorter and more convenient travel distances to treatment centers should be made available.
The 3-weekly infusions. They limit you too… If I travel down to South Island, I’m going to have to fly back to have the infusions done. They won’t do them anywhere else. So, a little bit limiting. (Participant F19)
Because we’re so far away from treatment centers, 3 hours each way, especially if you’re not feeling particularly well… Being able to stay somewhere safe without having to travel all the time was such an amazing experience of feeling cared for. (Participant F3)
Treatment Availability
Most patients expressed gratitude for the government-funded or insurance-covered treatments they received, considering themselves fortunate in this regard. Nonetheless, limitations persisted for individuals with advanced BC, as well as restricted access to or shortage of certain drugs or treatment options within NZ.
Having triple-negative breast cancer… less options that are available to me, all I can use is surgery, radiation, or chemo. There are no tablets that can help me that I can take for 5, 10 years, or whatever to stay off anything. (Participant F15)
The tricky thing is that we don’t know about half the drugs because they’re not here (in NZ). …I just basically note down every drug that they (BC forum in the US) discuss and look it up to see if we have it here in NZ and half of them, we don’t. (Participant F7)
Timeliness of Treatment
In general, patients were grateful to receive prompt treatment following their diagnosis with minimal delays.
It was a good thing because I didn’t have time to wait around and worry and think, Oh, what’s happening? Is it getting worse? It was really fast and quick and efficient. (Participant F18)
However, it is worth noting that not all patients expressed satisfaction with the timeliness of the treatment provided. Participant F5 highlighted a specific concern regarding inadequate recovery time for the body before initiating the next cycle of treatment.
Because it had gone to the lymph nodes, they wanted to start me on chemo quite quickly. So, I felt I had literally not recovered. And all of a sudden, I was just whammed with these drugs, which I had a lot of side effects to. … and I was sent back in hospital for two weeks. (Participant F5)
Patients who received treatment from public health facilities expressed their concern about the long waiting time between appointments. The prolonged duration between scheduled visits has given rise to anxiety among these individuals, as they create concerns about the potential recurrence of cancer.
Mine is public. I get to see the doctor once a year. For me it’s quite long just to get to see them. You can’t avoid … keep on thinking of possibility that there’s recurrence. (Participant F14)
Theme 4: Cost of Treatment
BC treatment incurs significant direct and indirect costs that can place a substantial financial burden on patients. Participants in this study shared their experience about the financial implications of their BC treatment, focusing on cost and funding.
Public Healthcare System and Funding
Most participants agreed on how the government-funded BC treatment plays a crucial role in alleviating their financial burden. However, there remains a disparity in public medication funding, which can potentially limit individual access to necessary medications due to healthcare budget constraints.
Funding is very critical because how many of us can really afford like the drugs is like $5000 a dose. So, we’re really fortunate it’s funded because otherwise it’s like, oh, you either have to go beg, borrow, and steal or you just have to give up and not have any treatment at all. (Participant F9)
Obviously some medication that they think would be best for you may not be funded. I just can’t believe that us in NZ have got that problem. And I’m just lucky that everything that I had was funded. (Participant F12)
Private Medical Insurance
The availability and coverage of private medical insurance plays a crucial role in managing the cost of BC treatment. Participant F4 shared how she dipped in and out of the public and private healthcare systems to access treatment that was unfunded by the public healthcare system.
I’ve dipped in and out of the private and public sector for my own benefit… I went private so that we could claim back from my insurance the chemo before it was funded. (Participant F4)
One of my treatments is not funded publicly, and I’m just super lucky that I can access that through my insurance. (Participant K1)
However, the extent of coverage and limitations of private medical insurance can vary based on the individual’s insurance plan and policy terms. Participant F15 shared her concerns about reaching the maximum limit of her insurance claimable for chemotherapy expenses.
Chemo now is costing me $5500 a cycle. … my insurance claimable is running out. (Participant F15)
Making Trade-off
Participants highlighted the tough decisions they face when it comes to balancing the cost of treatment and its potential benefits. Patients were forced to make trade-offs between their financial well-being and accessing necessary treatments.
If you had any assets and if you could sell them, then you would start making value judgments about, was it worth it to get five more years of extra life compared to maybe selling your house and then your family not having a house? (Participant K1)
It depends on how serious my condition would be. I guess if my life is at risk, I will probably pay as much as I can. (Participant K5)
Out-of-Pocket Cost
Participant F4 shared her emotional response to the financial burden of drugs that are not funded and subsidized by the government or other assistance programs.
I cried the day I was diagnosed when I was offered the unfunded drug, IBRANCE …was $5850 a month! I expected gold-plated pills when I got them. (Participant F4)
Even with private medical insurance, the monetary impact goes beyond direct medical expenses. Patients often face additional indirect costs, such as administration fees, transportation to and from medical appointments, accommodation during treatment, and the loss of income due to reduced work hours or the inability to work altogether.
Being in the private sector and that everything costs money, even just doing a letter is like $300. (Participant F21)
Discussion
This study is among the first to evaluate the unique experiences and preferences of BC patients regarding BC treatment in the NZ context. Despite the complexity and uniqueness of the experiences and preferences among the study participants, four distinct themes emerged from the interviews. The most prominent aspects of BC treatment, as evidenced by the participants during the interviews, revolve around positive clinical outcomes. A strong desire for extended survival and reduced recurrence rates was frequently expressed by the participants during the interviews. These findings are consistent with that of previous qualitative research in NZ, where individuals undergoing cancer treatment consistently prioritized clinical outcomes as their primary concern.25 In addition, similar observations about the willingness to undergo harsh treatment to gain longer survival were reported in previous qualitative studies.26,27 Nevertheless, the doubts regarding the value of treatment that solely prolongs lifespan while potentially jeopardizing overall well-being and QoL was emphasized. Research has indicated the importance of open discussions between healthcare professionals and patients to establish a treatment plan that is congruent with the individual’s treatment goals and values.28,29
On the other hand, the inevitability of treatment-related toxicity and side effects in cancer treatment was acknowledged. Consistent with earlier studies, participants in this study emphasized the impact of these side effects on various aspects of their QoL. Not only did they affect their physical well-being, but they also had a profound impact on their mental, emotional, spiritual, and psychosocial well-being.2,30–32 An important finding in this study was how living with BC impacted a woman’s self-esteem, body image, sexuality, and personal responsibility as a wife, mother, and employee. Furthermore, similar patterns of suicidal ideation have been observed in other qualitative studies examining the experiences of women with BC.33,34 These findings highlight the significance of integrating comprehensive QoL assessments as one of the crucial components of clinical outcomes in BC treatment. Provision of holistic and culturally competent BC care that considers the mental, emotional, spiritual, and psychosocial well-being, particularly from the perspective of a multicultural country like NZ, is crucial to better capture the potential value of a cancer treatment beyond clinical outcomes.
The participants in this study provided insights into their experiences of receiving treatment in both public and private healthcare facilities in NZ. Similar to many other developed countries, NZ has implemented a universal healthcare coverage system that is publicly funded, which is regionally administered, and supplemented by private facility services.35 From the interview, although participants expressed favorable experiences with both public and private facilities, the public facility is often criticized for its bureaucratic obstacles, administrative complexities, and longer waiting time to access treatment or to be seen by physicians. Notwithstanding the above, distance from healthcare facilities has hindered patients’ ability to access the necessary healthcare services. Similar criticism is observed in previous studies, where limited geographical accessibility to treatment and oncologists, instances of misdiagnosis, and prolonged waiting times at health facilities, significantly hindered diagnosis and treatment for BC.28,36 The anticipation and uncertainty surrounding these issues have intensified the feelings of anxiety and stress in coping with the diagnosis and treatment. These findings serve as a crucial wake-up call for healthcare policymakers, urging them to address these issues and work towards establishing a healthcare system that is efficient and effective in meeting the needs of patients. This includes initiatives such as enhancing training for the health workforce, reducing bureaucratic complexities, and expanding the availability of healthcare facilities.
Financial toxicity resulting from cancer treatment can lead to catastrophic healthcare expenditures for patients and their families.37 In addition to the direct medical costs, our study emphasized the impact of indirect medical expenses, such as administration fees, transportation and accommodation during treatment, childcare arrangements, as well as the loss of productivity. For cancer patients, the burden of travel from home to healthcare facilities can be inconvenient and exhausting as this entails additional costs for transportation and accommodation. The unforeseen financial distress resulting from these circumstances may influence patients’ decisions to delay or avoid necessary care, ultimately leading to increased morbidity and mortality rates.38,39 While having adequate medical insurance can alleviate a portion of the financial burden, patients often face challenges in identifying insurance plans that provide coverage for expensive cancer treatments and post-cancer follow-up care.40 Effective communication regarding the cost of cancer treatment between patients and healthcare providers plays a crucial role in optimizing decision-making and reducing the risk of financial toxicities. Therefore, the findings of this study underscore the imperative for a healthcare system that is both comprehensive and accessible, placing a high priority on patient-centered care, affordability, and ensuring equitable access for all patients.
In addition, patients often encounter the need to make nuanced decisions, carefully navigating trade-offs associated with the diverse attributes of a treatment. This decision-making process involves a thoughtful consideration of each treatment aspect, aligning choices with their personal values and beliefs. The complexity of these decisions highlights the importance of tailoring treatment plans to not only address medical considerations but also resonate with the individual patient’s unique perspective, preferences, and ethical considerations.
The strengths of this study reside in the novelty of the research question, specifically tailored to the NZ context. The study effectively identified gaps in the important determinants that BC patients in NZ consider crucial in their cancer treatment. The robust methodology, coupled with the rigorous thematic analysis, enhances the likelihood that the participants have provided a comprehensive picture of the attributes that influenced their treatment preferences and decision-making. We recognize the limitations inherent in this study, primarily stemming from sample selection bias. First is the small sample size of 26 participants with a majority of patients with early BC, hence the results may not be generalizable to the broader BC patient population. Nevertheless, established guidelines suggest that the sample size is considered sufficient to ensure a necessary diversity of opinions and experiences, as well as to validate collective views.41 Second, our sample consists of fewer Māori and Pacific participants than we anticipated. We acknowledge that it may not capture the heterogeneity of the Māori and Pacific populations as a whole. Future studies would benefit from the inclusion of more perspectives from Māori and Pacific participants. Last, due to the COVID-19 pandemic restrictions, all the FGDs and IDIs were conducted via Zoom videoconferencing, which we initially thought might compromise the depth and breadth of the findings. However, to our pleasant surprise, most study participants expressed a positive sentiment towards engaging in online discussions in the comfort of their own homes. Compared to face-to-face FGD or IDI, they felt a sense of ease and safety while being able to “hide” behind the veil of the computer screen. Consequently, this anonymity encouraged them to be more open and freely express their thoughts, including sensitive issues regarding their BC treatment. This is consistent with an existing study where Zoom is a viable tool for qualitative data collection within a health research context due to its ease of use, data-management properties, cost-effectiveness, and security features.42
Conclusion
Our findings indicate that, from the patient’s perspective, pivotal determinants of BC treatment revolve around several key attributes. These include strong preference towards treatments that yield positive outcomes (such as prolonged survival, achieving remission, and preventing recurrence), entail fewer side effects with minimal impact on their quality of life. Additionally, there is a notable preference for treatments that are easily accessible, available in a timely manner, and preferably funded by the government or medical insurance to reduce their financial burden. Nevertheless, patients frequently find themselves making trade-offs when considering various attributes of a treatment, aligning their decisions with their personal values and beliefs. The diverse viewpoints highlighted by our study participants underscore the need for individualized and patient-centered care in the context of BC treatment. These findings provide valuable opportunities for healthcare providers to accommodate these preferences from patients’ perspectives when making treatment decisions. By understanding and integrating patients’ perspectives, healthcare professionals can effectively support patients in making informed choices that are congruent with their values and priorities.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are not publicly available due to the interests of confidentiality. However, participants informed consent included publication of anonymized responses.
Ethics Approval
The study complied with the Declaration of Helsinki and was approved by the Southern Health and Disability Ethics Committees (Approval number 21/STH/41).
Acknowledgments
The authors express their gratitude to the women who willingly took part in this study, sharing their valuable time to discuss their breast cancer treatment experiences and allowing us access to the details of their disease and treatment. Special thanks go to Luisa Bituin for her assistance in patient recruitment and to Afshan Rani for skillfully moderating the interviews.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by the Health Research Council New Zealand Health Delivery Research Activation Grant. The funder did not play a role in study design, data collection, analysis, or interpretation nor were they involved in the preparation and submission of this manuscript. No identifiable information or findings beyond those disclosed in this report have been accessed or made available to the Health Research Council New Zealand.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ministry of Health New Zealand. New cancer registration 2016. Wellington; 2018.
2. Sibeoni J, Picard C, Orri M, et al. Patients’ quality of life during active cancer treatment: a qualitative study. BMC Cancer. 2018;18(1):951. doi:10.1186/s12885-018-4868-6
3. Cebeci F, Yangin HB, Tekeli A. Determination of changes in the sexual lives of young women receiving breast cancer treatment: a qualitative study. Sexual Disabil. 2010;28(4):255–264. doi:10.1007/s11195-010-9169-1
4. Pilevarzadeh M, Amirshahi M, Afsargharehbagh R, Rafiemanesh H, Hashemi S-M, Balouchi A. Global prevalence of depression among breast cancer patients: a systematic review and meta-analysis. Breast Cancer Res Treat. 2019;176(3):519–533. doi:10.1007/s10549-019-05271-3
5. Tavares R, Brandao T, Matos PM. Mothers with breast cancer: a mixed-method systematic review on the impact on the parent-child relationship. Psycho-Oncology. 2018;27(2):367–375. doi:10.1002/pon.4451
6. Hacialioglu N, Ozer N, Yilmaz Karabulutlu E, Erdem N, Erci B. The quality of life of family caregivers of cancer patients in the east of Turkey. Eur J Oncol Nurs. 2010;14(3):211–217. doi:10.1016/j.ejon.2010.01.017
7. Harrison M, Milbers K, Hudson M, Bansback N. Do patients and health care providers have discordant preferences about which aspects of treatments matter most? Evidence from a systematic review of discrete choice experiments. BMJ Open. 2017;7(5):e014719. doi:10.1136/bmjopen-2016-014719
8. Burstein HJ, Curigliano G, Thurlimann B, et al. Customizing local and systemic therapies for women with early breast cancer: the St. Gallen International Consensus Guidelines for treatment of early breast cancer 2021. Ann Oncol. 2021;32(10):1216–1235. doi:10.1016/j.annonc.2021.06.023
9. Cardoso F, Wilking N, Bernardini R, et al. A multi-stakeholder approach in optimising patients’ needs in the benefit assessment process of new metastatic breast cancer treatments. Breast. 2020;52:78–87. doi:10.1016/j.breast.2020.04.011
10. Kane P, Jasperse M, Egan R, et al. Continuity of cancer patient care in New Zealand; the general practitioner perspective. N Z Med J. 2016;129(1440):55–63.
11. Nickel B, McCaffery K, Houssami N, et al. Views of healthcare professionals about the role of active monitoring in the management of ductal carcinoma in situ (DCIS): qualitative interview study. Breast. 2020;54:99–105. doi:10.1016/j.breast.2020.09.002
12. Pilkington S. To What Extent Does the Fear of Recurrence Affect a Woman’s Ability to Move Forward to Survivorship in the First Five Years Post Treatment for Breast Cancer. Auckland: ResearchSpace; 2011.
13. Milne RJ, Heaton-Brown KH, Hansen P, Thomas D, Harvey V, Cubitt A. Quality-of-life valuations of advanced breast cancer by New Zealand women. Pharmacoeconomics. 2006;24(3):281–292. doi:10.2165/00019053-200624030-00007
14. Shaw S, Atkinson K, Jones LM, Judd J. Cancer survivors’ experiences of an exercise program during treatment and while employed: a qualitative pilot study. Health Promot J Austr. 2021;32(S2):378–383. doi:10.1002/hpja.447
15. Shingler SL, Bennett BM, Cramer JA, Towse A, Twelves C, Lloyd AJ. Treatment preference, adherence and outcomes in patients with cancer: literature review and development of a theoretical model. Curr. Med. Res. Opin. 2014;30(11):2329–2341. doi:10.1185/03007995.2014.952715
16. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
17. Yeo HY, Liew AC, Chan SJ, et al. Understanding patient preferences regarding the important determinants of breast cancer treatment: a narrative scoping review manuscript submitted for publication. Patient Preference Adherence. 2023;2023:2679–2706.
18. Creswell JW, Miller DL. Determining validity in qualitative inquiry. Theory into Pract. 2000;39(3):124–130. doi:10.1207/s15430421tip3903_2
19. Braun V, Clarke V. Reflecting on reflexive thematic analysis. Qual Res Sport Exerc Health. 2019;11(4):589–597. doi:10.1080/2159676X.2019.1628806
20. Malterud K, Siersma VD, Guassora AD. Sample size in qualitative interview studies: guided by information power. Qual Health Res. 2016;26(13):1753–1760. doi:10.1177/1049732315617444
21. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
22. Lincoln YS, Guba EG. Naturalistic Inquiry. sage; 1985.
23. Byrne D. A worked example of Braun and Clarke’s approach to reflexive thematic analysis. Qual Quantity. 2021;56(3):1391–1412. doi:10.1007/s11135-021-01182-y
24. Clarke V, Braun V. Successful qualitative research: a practical guide for beginners. Successful Qual Res. 2013;2013:1–400.
25. Lorgelly P, Pollard J, Cubi-Molla P, Cole A, Sim D, Sussex J. Outcome-based payment schemes: what outcomes do patients with cancer value? Patient. 2020;13(5):599–610. doi:10.1007/s40271-020-00430-x
26. Dicks E, Roome R, Chafe J, et al. Factors influencing surgical treatment decisions for breast cancer: a qualitative exploration of surgeon and patient perspectives. Curr Oncol. 2019;26(2):e216–e225. doi:10.3747/co.26.4305
27. Harder H, Ballinger R, Langridge C, Ring A, Fallowfield LJ. Adjuvant chemotherapy in elderly women with breast cancer: patients’ perspectives on information giving and decision making. Psycho-Oncology. 2013;22(12):2729–2735. doi:10.1002/pon.3338
28. Lewis S, Yee J, Kilbreath S, Willis K. A qualitative study of women’s experiences of healthcare, treatment and support for metastatic breast cancer. Breast. 2015;24(3):242–247. doi:10.1016/j.breast.2015.02.025
29. Rodriguez KL, Gambino FJ, Butow P, Hagerty R, Arnold RM. Pushing up daisies: implicit and explicit language in oncologist–patient communication about death. Support Care Cancer. 2007;15(2):153–161. doi:10.1007/s00520-006-0108-8
30. Ruddy KJ, Greaney ML, Sprunck-Harrild K, Meyer ME, Emmons KM, Partridge AH. Young women with breast cancer: a focus group study of unmet needs. J Adolesc Young Adult Oncol. 2013;2(4):153–160. doi:10.1089/jayao.2013.0014
31. Nies YH, Ali AM, Abdullah N, Islahudin F, Shah NM. A qualitative study among breast cancer patients on chemotherapy: experiences and side-effects. Patient Preference Adherence. 2018;Volume 12:1955–1964. doi:10.2147/PPA.S168638
32. Hauken MA, Grue M, Dyregrov A. “It’s been a life‐changing experience!” A qualitative study of young adult cancer survivors’ experiences of the coexistence of negative and positive outcomes after cancer treatment. Scand J Psychol. 2019;60(6):577–584. doi:10.1111/sjop.12572
33. Teye-Kwadjo E, Goka A-S, Ussher YAA. Unpacking the psychological and physical well-being of Ghanaian patients with breast cancer. Dialog Health. 2022;1:100060. doi:10.1016/j.dialog.2022.100060
34. Bonsu AB, Aziato L, Clegg-Lamptey JNA. Living with advanced breast cancer among Ghanaian women: emotional and psychosocial experiences. Int J Palliat Care. 2014;2014:1–9. doi:10.1155/2014/403473
35. Gauld R. The New Zealand health care system. Int Profiles Health Care Syst. 2020;2020:149–158.
36. Afaya A, Ramazanu S, Bolarinwa OA, et al. Health system barriers influencing timely breast cancer diagnosis and treatment among women in low and middle-income Asian countries: evidence from a mixed-methods systematic review. BMC Health Serv Res. 2022;22(1):1–17. doi:10.1186/s12913-022-08927-x
37. Smith KT, Monti D, Mir N, Peters E, Tipirneni R, Politi MC. Access is necessary but not sufficient: factors influencing delay and avoidance of health care services. MDM Policy Pract. 2018;3(1):2381468318760298. doi:10.1177/2381468318760298
38. Hanna TP, King WD, Thibodeau S, et al. Mortality due to cancer treatment delay: systematic review and meta-analysis. BMJ. 2020;371:m4087. doi:10.1136/bmj.m4087
39. Ambroggi M, Biasini C, Del Giovane C, Fornari F, Cavanna L. Distance as a barrier to cancer diagnosis and treatment: review of the literature. Oncologist. 2015;20(12):1378–1385. doi:10.1634/theoncologist.2015-0110
40. George N, Grant R, James A, Mir N, Politi MC. Burden associated with selecting and using health insurance to manage care costs: results of a qualitative study of nonelderly cancer survivors. Med Care Res Rev. 2021;78(1):48–56. doi:10.1177/1077558718820232
41. Vasileiou K, Barnett J, Thorpe S, Young T. Characterising and justifying sample size sufficiency in interview-based studies: systematic analysis of qualitative health research over a 15-year period. BMC Med Res Methodol. 2018;18(1):148. doi:10.1186/s12874-018-0594-7
42. Archibald MM, Ambagtsheer RC, Casey MG, Lawless M. Using zoom videoconferencing for qualitative data collection: perceptions and experiences of researchers and participants. Int J Qual Methods. 2019;18:1609406919874596. doi:10.1177/1609406919874596
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Development of Schematics to Illustrate Women’s Experiences with Adjuvant Hormone Therapy in the Treatment of Breast Cancer
AlOmeir O, Patel N, Donyai P
Patient Preference and Adherence 2022, 16:2639-2647
Published Date: 23 September 2022
Expectations and Experiences of a Group of Patients Enrolled in an Educational Program for Rheumatoid Arthritis at a Specialized Care Center in Colombia
Castiblanco-Montañez RA, Buitrago-Garcia D, Arévalo Velandia A, Garzón-Cepeda JD, Rodríguez-Florido F, Sánchez Vanegas G, Santos-Moreno P
Journal of Multidisciplinary Healthcare 2023, 16:483-492
Published Date: 22 February 2023
Understanding Patient Preferences Regarding the Important Determinants of Breast Cancer Treatment: A Narrative Scoping Review
Yeo HY, Liew AC, Chan SJ, Anwar M, Han CHW, Marra CA
Patient Preference and Adherence 2023, 17:2679-2706
Published Date: 31 October 2023
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
A Qualitative Study of Fertility Preservation Experience in Women with Breast Cancer
Wang Z, Yang X, Hong X, He Y, Xu A, Jiang X, Wei Q
International Journal of Women's Health 2025, 17:1143-1155
Published Date: 23 April 2025