Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
The Practice of Shared Decision-Making Among Physiotherapists and Patients with Musculoskeletal Conditions
Authors Alotaibi MA ![]() , Alhowimel AS
, Alhowimel AS ![]() , Alodaibi FA
, Alodaibi FA ![]() , Aloraifi M
, Aloraifi M
Received 10 June 2023
Accepted for publication 29 August 2023
Published 8 September 2023 Volume 2023:16 Pages 2655—2665
DOI https://doi.org/10.2147/JMDH.S425315
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mazyad A Alotaibi,1 Ahmed S Alhowimel,1 Faris A Alodaibi,2 Mohammed Aloraifi3
1Department of Health and Rehabilitation Sciences, Prince Sattam Bin Abdulaziz University College of Applied Medical Sciences, Prince Sattam Bin Abdulaziz University, Al-Kharj, Saudi Arabia; 2Department of Rehabilitation Sciences, King Saud University, Riyadh, Saudi Arabia; 3Salamat Medical Hospital, Department of Physiotherapy, Hail, Saudi Arabia
Correspondence: Mazyad A Alotaibi, Department of Health and Rehabilitation Sciences, Prince Sattam Bin Abdulaziz University College of Applied Medical Sciences, Prince Sattam Bin Abdulaziz University, Al-Kharj, 11942, Saudi Arabia, Tel +966115886354, Email [email protected]
Purpose: Shared decision-making (SDM) may be interpreted as a set of core values rather than as a consensus definition. This study aimed to explore how SDM between patients and physiotherapists may lead to patient satisfaction.
Patients and Methods: A cross-sectional study was conducted to examine the relationship between SDM and patient satisfaction. The study targeted physiotherapists and patients with musculoskeletal pain or disorders. A structured questionnaire (the nine-item Shared Decision-Making Questionnaire) was developed to show the extent to which patients felt involved in the process by scoring nine items from 0 to 5 on a six-point scale. t-tests were performed to estimate differences in SDM perceptions between patients and physiotherapists, and regression analyses were performed to estimate the best predictors of SDM.
Results: The questionnaire was completed by a total of 106 patients and nine physiotherapists. The demographic information of the samples was presented with frequency analysis. This study’s findings demonstrate no variations in the final SDM perceptions between patients and physiotherapists, but when SDM was contrasted step-by-step (as items), many variances were discovered. These distinctions reinforce the notion that regardless of the end outcome, the process of reaching a consensus has a distinct profile depending on the type of medical care. Therapists emphasize the first steps, possibly because there is sufficient evidence to make a therapeutic decision. However, patients highlight the final steps, perhaps because the moment for a decision based on the consultation’s nature is approaching.
Conclusion: This study demonstrates that SDM is a complex process that must be examined in multiple stages. However, in physiotherapy contexts, this process exhibits extremely different patterns, reflecting a significantly different perspective of the decision-making process.
Keywords: physical therapy, decision-making, patient preference, musculoskeletal disorders
Introduction
The discipline of physiotherapy derives considerable satisfaction from its recognition as an evidence-based profession.1 Therefore, it is possible to implement study findings via a technique known as shared decision-making (SDM),2 which also makes it easier to provide patient-centered care by encouraging patients to take an active role in the decision-making process.3 SDM is a collaborative process that involves patients, physiotherapists, and clinicians making decisions regarding the patient’s health after discussing the available options; identifying the benefits and demerits of each option; and considering the patient’s values, preferences, and personal circumstances.4 It is also known as patient-centered decision-making or patient-centered SDM.5 SDM enables doctors to utilize evidence-based information while simultaneously positioning the patient (and family members, where applicable) at the center of clinical decision-making. Therefore, a collaborative choice considers the most recent and relevant research information, as well as the physiotherapist’s knowledge, experience, and competence, and the patient’s values and preferences.6 Open communication between the patient and the therapist is essential to the SDM process. The clinician provides evidence-based information about the options and balanced information about each option’s benefits, harms, and uncertainties (including watchful waiting where appropriate).7 Despite the growing importance of SDM in physiotherapy, there remains a need to explore how SDM between patients and physiotherapists influences patient satisfaction and treatment outcomes. Furthermore, many patients do not participate in the decision-making process. This can lead to a number of problems, including patients not being satisfied with their treatment choices, not being aware of the risks and benefits of different treatment options, and not being able to make informed decisions about their care.
Clinicians use their communication skills to actively listen to and engage with patients to elicit their preferences, advise them in accordance with their preferences, and address their concerns. The patients are aware of their disease and how it impacts their daily life, their expectations and anxieties, and their values and preferences for the available alternatives, which may be affected by their prior experiences, those of their friends, or their current circumstances (such as cost and treatment burden).7 Both the physician’s and patient’s perspectives are necessary, and combining them may lead to increased levels of satisfaction with treatment for both the therapist and the patient.8 However, most complaints about healthcare are caused by ineffective communication or by patients obtaining insufficient information to enable them to make decisions based on that knowledge.
Patients’ expectations and ideas regarding interventions, including how they can help and to what extent, may be better managed with the assistance of SDM.9 Additionally, many doctors and patients have ideas about the effectiveness of interventions based on “mechanistic thinking” (that is, how the intervention ought to operate) rather than empirical thinking.10 For instance, many patients’ requests for imaging for back pain are based on the notion that the physician has to “see the issue to know how to treat it”. Although imaging is not frequently advised for lower back pain, many patients still request such procedures. However, via SDM, patients can be provided with more realistic expectations of their alternatives’ advantages and risks.
Furthermore, the management of SDM is defined by numerous elements, one of which is enhanced patient knowledge, which clarifies patient information and allows participation in decision-making. Second, physiotherapists respect patients’ goals and are eager to include them in treatment. Finally, the patient is motivated to acquire independence and self-reliance.11–13 However, numerous obstacles to participation in decision-making exist.14 Additionally, insufficient access to patients exists for their participation in decision-making.15
Musculoskeletal (MSK) discomfort is regarded as a leading cause of pain and disability.16–18 The physiotherapist and patient discuss the facts, reasons for pain, and treatment decisions.2,7 Nevertheless, some patients are dissatisfied with this method, even if it is beneficial, since they do not participate in the decision-making process.19,20 This results in a lack of trust in the physiotherapists, and patients may not have faith in their possible treatments in the future. Moreover, only a few studies have reported on SDM, where all the stakeholders were onboarded to develop appropriate treatment plans for patients. Therefore, this study aimed to explore how SDM between patients and physiotherapists may lead to patient satisfaction.
Materials and Methods
Study Design
A cross-sectional study was conducted to examine the relationship between SDM and patient satisfaction. The study complies with the Declaration of Helsinki.
Study Area and Population
This study was conducted in the city of Hail, Kingdom of Saudi Arabia, in multiple centers for physiotherapy and targeted convenience sample physiotherapists and patients with MSK pain or disorders.
The sample size determination followed the COSMIN guideline, which specifies that the number of participants should be a minimum of seven times the number of items in the questionnaire.21
Inclusion Criteria
Patients were included in this study if they were adults, had MSK pain, and could read and write.
Exclusion Criteria
Patients with non-MSK injuries and those aged <18 years were excluded.
Outcome Measures and Data Collection
The main outcome measure of SDM is a nine-item Shared Decision-Making Questionnaire designed in German and translated into Arabic.22,23 The questionnaire was developed to show the extent to which patients felt involved in the SDM process during treatment for MSK pain. The questionnaire was scored by summing the nine items from 0 to 5 on a six-point Likert scale; the scale ranged from “completely disagree” (0) to “completely agree” (5). The summation of all items led to a raw total score between 0 and 45. Additionally, the multiplication of the raw score by 20/9 gave a forced (transformed) score ranging from 0 to 100, where 0 and 100 indicated the lowest and highest extent of SDM, respectively. The authors encouraged the use of the transformed score because it was more intuitively interpretable.
A physiotherapist was appointed to diagnose the cases, and after identifying the targeted cases, the therapist mentioned the cases to the designated receptionist. The receptionist completed two anonymous questionnaires with matching codes as follows: one each for the physiotherapist and the patient. Tokens enabled the researchers to match the responses from the same consultation. Immediately after the consultation, the patients and physiotherapists completed their questionnaires separately and returned them to the receptionist. The patients were required to return anonymous surveys to the receptionist either by handing them over or leaving them in a locked box. The receptionist kept the completed forms in closed boxes until the researcher collected them. The confidentiality of the participants was ensured to meet research ethics.
Data were collected by members of the research team who had undergone training on the study protocol, including research ethics. The questionnaire consisted of nine questions that dealt with the necessity of making a decision, the desire to make a decision, and the multiplicity of treatment methods; regarding how to proceed with the case, the answer alternatives were “exactly correct”, “largely correct”, “somewhat correct”, “somewhat incorrect”, “largely incorrect”, and “not quite correct”.
Subsequently, the questionnaire was coded in the SPSS program as numbers where exactly true, to a large extent true, true to some extent, incorrect to some extent, incorrect to a large extent, and not completely correct were equivalent to 1, 2, 3, 4, 5, and 6, respectively. Finally, the ratio was calculated using the program, and the bias factor was 0.5.
Statistical Analysis
The demographic information of the samples was reported using frequency analysis. Additionally, t-tests were performed to estimate differences in SDM perceptions (item-by-item and total score) between patients and physiotherapists. The effect sizes were calculated using Cohen’s statistics. Furthermore, to analyze the orientation of item-by-item scores, direct scores were transformed into two categories as follows: “disagree” (responses from 1 to 3) and “agree” (responses from 4 to 6). t-tests were performed to estimate the differences between the two categories. Finally, regression analyses were performed to estimate the best predictors of SDM, the total score, and item-by-item scores. A step-by-step model was used to identify only those variables that played a relevant role in predicting SDM scores. This model introduced only variables with a significant contribution to the equation.
Results
Samples Characteristics
Table 1 shows the sample distribution by age, sex, job, and diagnosis. Overall, 106 patients participated in this study; 64.2% and 35.8% were males and females, respectively. The patients’ ages ranged from 18 to 77 years, with a mean age of 39.06±13.68. Most patients were students (17%), followed by the unemployed (16%) and housewives (14.2%). The diagnoses varied between low back pain (26.4%), neck pain (10.4%), knee osteoarthritis (10.4%), shoulder pain (9.4%), ankle sprain (7.5%), and multiple MSK conditions (35.9%).
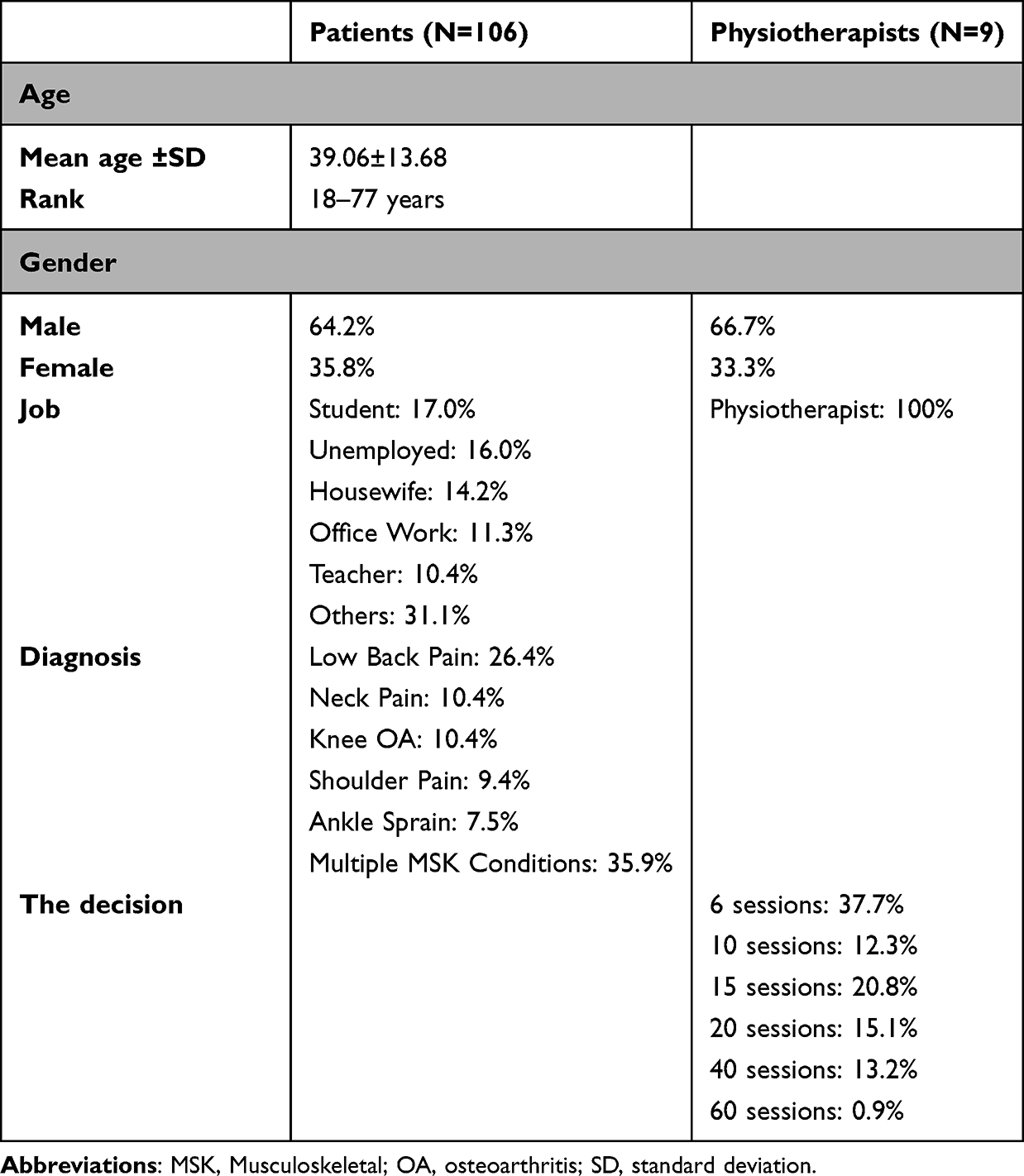 |
Table 1 Sample Characteristics |
According to physiotherapists, 66.7% and 33.3% were males and females, respectively. All patients had specialized physiotherapists. The physiotherapists made different patient treatment decisions, ranging across six and 60 sessions; the most and least frequent treatment decisions involved six (37.7%) and 60 (0.9%) sessions, respectively.
Descriptive Analyses of the Nine-Item Shared Decision-Making Questionnaire (SDM-Q-9) Items
An initial analysis was performed to compare the total SDM-Q-9 scores between patients and physiotherapists. Student’s t-test for the total score (0–100 transformed) showed no statistically significant differences between them (patients: 62.3±20.8; physiotherapists: 63.3±18.6; t [1109] = −0.7). Since no statistically significant differences were found, new t-tests were performed, considering the different items (representing different contents/steps in SDM). Table 2 summarizes the obtained data.
 |
Table 2 Mean Differences Between Patients and Physiotherapists for the Different Steps in the SDM Process, According to the SDM-Q-9 Items |
Although no change was found in the total score, certain categories showed statistically significant differences between the two groups. However, item 8 was the exception, and its lack of variance was consistent with the total score’s lack of differences because the item’s content refers to the final physiotherapists’ shared decision. The observed pattern of differences showed that the physiotherapists’ score was greater in the beginning items (when the professionals notify their patients about the need to make a decision and how patients are ready to participate). Patients scored higher on intermediate elements (options, patient preferences, and bargaining, among others). The physiotherapists scored better on the final item (follow-up).
However, greater impacts were found when physiotherapists scored higher (particularly in the “formulation of equality of partners”), ranging from medium to high effect coefficients. Furthermore, item 5 (patient anticipation) was not statistically significant.
A second analysis was performed to identify the orientation of such differences, which implies the level of agreement between both groups of patients and physiotherapists with the various components of SDM. As previously stated, each item was categorized into two categories as follows: “disagree” (responses ranging from 1 to 3) and “agree” (responses ranging from 1 to 3). (Responses 4 to 6). Data were converted to percentages to facilitate comprehension. Table 3 summarizes the obtained data.
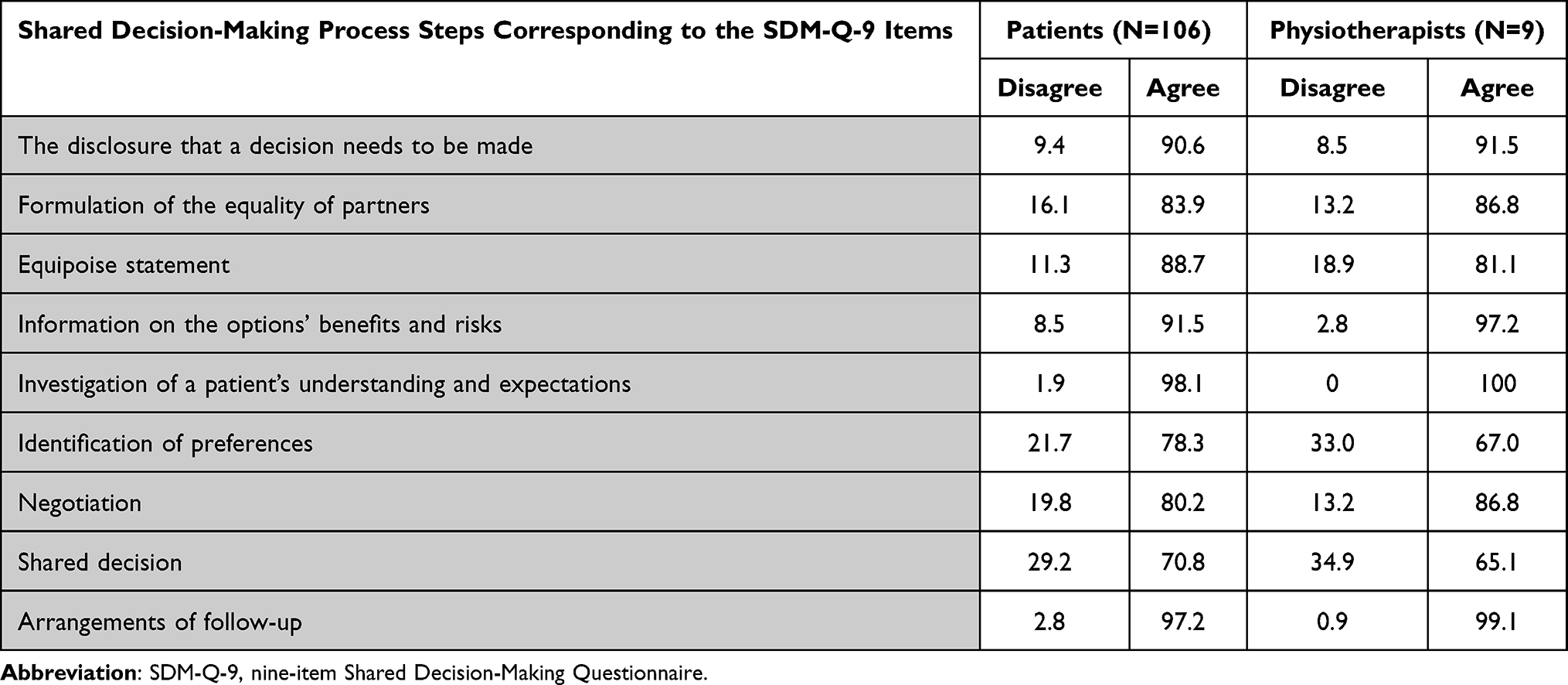 |
Table 3 Percentage Agreement with SDM-Q-9 Contents in Patients and Physiotherapists |
Although the transformed questionnaire scores in both samples were nearly identical (patients: 62.3±20.8; physiotherapists: 63.3±18.6), the results obtained item by item were similar, indicating a similar perspective of the decision-making process in their consultations (Table 3). Most patients agreed with every single item on the questionnaire, and most physiotherapists agreed with five items, although they scored higher. Additionally, most patients agreed with their physiotherapists’ admission that a decision must be made and that their physiotherapists wanted to know how they preferred to engage in making the decision. However, for the most part, they considered that they were educated about the various options available, as well as the benefits and drawbacks of those options.
Considering the various patient and physiotherapist profiles in SDM, the following analysis sought to determine whether contextual clinical variables, such as treatment decisions (number of sessions) and sociodemographic variables (age, gender, and job), played a significant role in predicting those profiles. Several regression analyses were performed on the items as dependent variables. Contextual and sociodemographic variables and sample type (patients and physiotherapists) were introduced as explanatory variables. Table 4 summarizes the obtained coefficients.
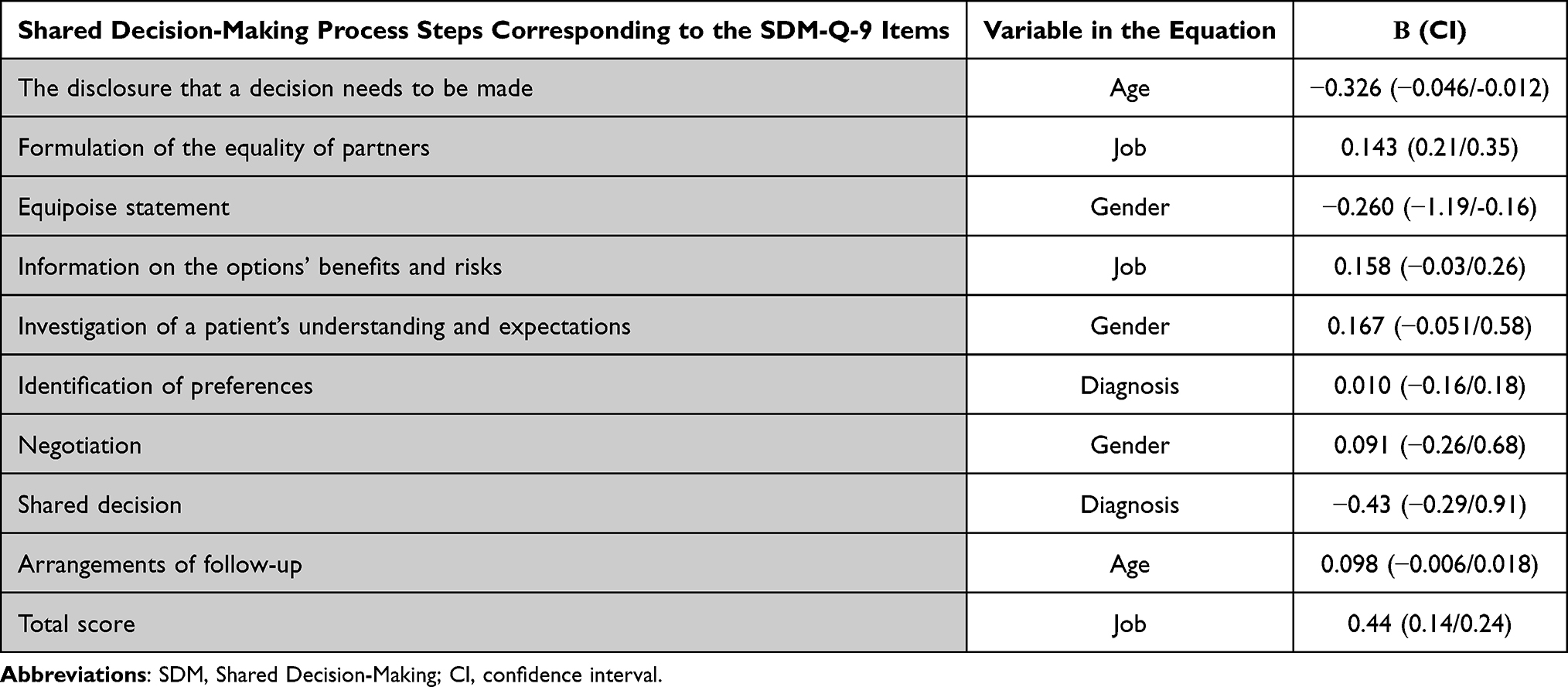 |
Table 4 Regression Analyses (Step-by-Step Model) for Content Considering Age, Job, Diagnosis and Gender as Explanatory Variables |
As can be observed, “Sample type” was present in all equations (and in the first step) except for the total score. Two variables played a significant role depending on the item/content as follows: “diagnosis” contributed positively to the “Identification of preferences” item and “shared decision”. “Gender” only appeared to play a role in predicting the “Equipoise statement” and “Negotiation” items. The “job” variable appears in the first and “follow-up” items. However, the overall score was only predicted (statistically significant) by “job”.
Discussion
This study primarily aimed to investigate whether treatment choices were made jointly or individually by the patients and physiotherapists. The study’s results suggest that the fact that the findings were comparable item-by-item implies that the parties involved in the discussions had a similar viewpoint on the decision-making process. Most patients agreed with each issue on the questionnaire, and most physiotherapists responded affirmatively to five of the questions. Additionally, most patients agreed with their physiotherapists’ admission that a choice must be made. Furthermore, the patients’ physiotherapists wanted to know how the patients wanted to be involved in the decision-making process. In contrast, they believed that they had a good understanding of the myriad possible choices, as well as the advantages and disadvantages of those choices. This was most of their opinion.
Moreover, it can be observed that the term “Sample type” appears in all of the equations, excluding the equation that calculates the overall score. Depending on the item or its content, two major factors exist. One of these factors is known as “diagnosis”, which positively contributes to both the “Identification of preferences” item and the “shared choice” item. However, it appears that “Gender” is only relevant for forecasting the “Equilibrium statement” and the “Negotiation” elements. Both the first and “follow-up” items include the “job” variable in some capacity, and this is the only variable that can accurately predict the total score.
Previous studies in physiotherapy healthcare settings have shown that physiotherapists have a favorable attitude toward involving patients in a procedure of reciprocal communication that considers their choices, values, and expectations, and they are more cautious about sharing decisions.24,25 Our results are consistent with those of many previous studies.
Our results are also compatible with the findings that some participants thought that the physiotherapist had excessive influence over their relationship. This led to a didactic and paternalistic approach, which was poorly accepted and inhibited the involvement of SDM.26,27 This might be because the physician views their job as that of a decision-maker and an advocate for their patients. Another study showed that physiotherapists frequently make incorrect judgments about people’s preferences for involvement in decision-making, which suggests that although therapists frequently have good intentions, they may avoid using SDM on the assumption that patients do not want to participate in the process.28,29 Therefore, to ensure cooperation, there must be a shift in clinicians’ attitudes and behaviors.
Patients who participated in semi-structured interviews and those whose therapists had used the tool described having more in-depth discussions about the benefits and harms of many treatment options, as well as a greater understanding of the structured progression of the treatment options as their condition progressed.30 Additionally, interviews were conducted with physiotherapists before and after using the instrument. During the interviews conducted “before”, therapists voiced their concerns that the tool would increase the time of each session, that patients would be resistant to being involved in decision-making, and that there would be a risk of information overload. In the interviews conducted “after”, the therapists said that the tool had altered their typical mode of communication and that including this tool in clinical practice was usually acceptable and useful.31
In a pilot cluster randomized trial for low back pain involving 19 physiotherapists and 148 participants, patient satisfaction was higher in the control group (67%) than in the intervention group (53%).32 This trend occurred because the patient decision support package consisted of a patient booklet and a 2-hour training for intervention group therapists. However, as part of this pilot study, a process review, which may have explained this result, was not performed. Therefore, it was hypothesized that the decision-support package would lead to patients having less confidence in the efficacy of the many treatment alternatives that were made accessible to them, which would, in turn, lower their expectations of benefit.33
Ethical considerations play a pivotal role in the decision-making process in physiotherapy. The professional code of ethics for physiotherapists mandates them to respect patients’ autonomy, which inherently includes involving patients in decisions about their care. This SDM process is ethically appropriate and aligns with the principles of person-centered care, fostering an environment of mutual respect and cooperation.
Furthermore, the code of ethics requires physiotherapists to provide accurate and comprehensive information to patients, which is crucial for informed decision-making. It also calls for physiotherapists to respect patients’ values and preferences, which echoes the need for active listening and consideration of patients’ preferences in the SDM process identified in our study. In light of these ethical guidelines, the barriers identified in our study—such as a lack of opportunity, confidence, and capacity on the individual’s side—represent ethical challenges that must be addressed to ensure ethical compliance in physiotherapy practice. Thus, our findings underscore the need for professional development programs for physiotherapists focusing on ethical decision-making, effective patient communication, and strategies for fostering patient participation and empowerment.
To analyze the effects of patient participation in decision-making for maintaining motivation in both clinical practice and patient care, as well as increasing its utilization, routine collection can include proximal, distal, and distant outcomes34,35 included in healthcare system policies, task groups, and government agencies. Both the care pathways of the United Kingdom’s National Health Service and Scotland’s Realistic Medicine policy have been updated to include patient experience and SDM.36
It is necessary to make changes in the activation and preparedness of healthcare providers, patients, and the general public for collaborative decision-making to foster cultural changes at the individual clinician and patient level. Therefore, campaigns that target patients, clinicians, and the public are regarded as a critical component of many implementation methods. These campaigns can increase the acknowledgment of the expertise that both patients and physicians bring to the consultation. The information aimed at patients and the public may focus on ways to empower individuals to take a more active role in managing their medical care.37
The physiotherapist’s desire to make hard decisions was motivated by a wide variety of thinking. The fear of making the “wrong” choice was mentioned, which suggests that individuals are more prone to opt out of high-risk decisions, although other participants were glad to delegate “small” decisions.38 Furthermore, a person’s opinion that they do not have sufficient medical expertise, particularly compared with that of a physician, might also contribute to their fear of making an incorrect choice.39 This is particularly important in the field of MSK physiotherapy, where there are very few treatments that are both 100% successful and free of side effects.
According to a study’s findings, decision preferences may be influenced by cultural, social, and economic variables. This phenomenon has also been observed in other healthcare settings.40 Although these demographics are unchangeable, research has demonstrated that an individual’s behavior may be altered if they are provided with appropriate choice assistance. Therefore, individuals have the capability, regardless of their history, to modify their attitudes and behaviors toward SDM if the necessary help is provided to them at the right time.41
In addition to therapists sharing power, it is necessary to increase people’s capacity and capability to engage in SDM, which is mandatory. However, people in this review could not confront the physiotherapist or assist themselves because they lacked the necessary information and confidence. Consequently, they depended on the physiotherapist and felt powerless. It is important not to misjudge an unwillingness to engage as an incapacity to participate because of a lack of knowledge, confidence, or absence of an atmosphere that supports cooperation.42–44 This may be as easy as granting individuals express permission to participate, or it could be as difficult as questioning attitudes and behaviors at the individual and social levels.45
This study had some strengths and limitations. The study’s findings provide insight into the many factors that impact people’s capability and confidence levels when participating in SDM in MSK physiotherapy. The nature of cross-sectional studies and the use of the Likert scale as a data collection tool are associated with several biases that should be considered.
Future research may consider observing SDM across diagnosis-specific MSK conditions and analyzing the interface of pain or disability with SDM. This can help establish SDM models tailored to particular conditions and aid the efficacy of SDM.
Conclusion
The findings demonstrate that people generally desire to be engaged in decision-making and provide a fresh perspective on their experiences with SDM in MSK physiotherapy. It depicts how people view the main criteria that must be met for SDM to be effective. However, a lack of opportunity, confidence, and capacity on the part of the individual were the primary factors that hindered collaborative decision-making.
Moreover, our study reveals that physiotherapists’ attitudes and behaviors significantly influence patients’ experiences and attitudes toward SDM in MSK physiotherapy. Therefore, for SDM to be effective, physicians should provide decision support via communication that goes in both directions, sharing their knowledge in an easily digestible manner and actively listening to and acting on individuals’ preferences. Building a foundation of trust among participants is also necessary before they feel comfortable enough to participate. Finally, physiotherapists should be aware of the influence they wield in their roles as healthcare professionals and be willing to accept the responsibility of cultivating an atmosphere that actively promotes people’s participation, self-efficacy, and empowerment through a balanced distribution of power.
Data Sharing Statement
All data are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study was approved by The Ethical Committee of Applied Medical Sciences, Prince Sattam Bin Abdulaziz University, Al Kharj, Kingdom of Saudi Arabia (No.: RHPT/021/014). Informed consent was obtained from all participants involved in the study.
Consent for Publication
All participants provided consent for the publication of identifiable details, including photographs and/or videos and/or case history and/or details within the text to be published.
Acknowledgments
We are immensely grateful to the Deanship of Scientific Research at Prince Sattam bin Abdulaziz University, Al-Kharj, Saudi Arabia, for their support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fetters L, Tilson J. Evidence Based Physical Therapy. F A Davis; 2018.
2. Hoffmann TC, Lewis J, Maher CG. Shared decision making should be an integral part of physiotherapy practice. Physiotherapy. 2020;107:43–49. doi:10.1016/j.physio.2019.08.012
3. Grenfell J, Soundy A. People’s experience of shared decision making in musculoskeletal physiotherapy: a systematic review and thematic synthesis. Behav Sci. 2022;12(1). doi:10.3390/bs12010012
4. Topp J, Westenhöfer J, Scholl I, Hahlweg P. Shared decision-making in physical therapy: a cross-sectional study on physiotherapists’ knowledge, attitudes and self-reported use. Patient Educ Couns. 2018;101(2):346–351. doi:10.1016/j.pec.2017.07.031
5. Weiner SJ, Schwartz A, Sharma G, et al. Patient-centered decision making and health care outcomes: an observational study. Ann Intern Med. 2013;158(8):573–579. doi:10.7326/0003-4819-158-8-201304160-00001
6. Moore CL, Kaplan SL. A framework and resources for shared decision making: opportunities for improved physical therapy outcomes. Phys Ther. 2018;98(12):1022–1036. doi:10.1093/ptj/pzy095
7. Hoffmann T, Bakhit M, Michaleff Z. Shared decision making and physical therapy: what, when, how, and why? Braz J Phys Ther. 2022;26(1):100382. doi:10.1016/j.bjpt.2021.100382
8. Joosten EA, DeFuentes-Merillas L, De Weert GH, Sensky T, Van Der Staak CP, de Jong CA. Systematic review of the effects of shared decision-making on patient satisfaction, treatment adherence and health status. Psychother Psychosom. 2008;77(4):219–226. doi:10.1159/000126073
9. Jhy N, Luk BHK. Patient satisfaction: concept analysis in the healthcare context. Patient Educ Couns. 2019;102(4):790–796. doi:10.1016/j.pec.2018.11.013
10. Midgley G, Rajagopalan R. Critical systems thinking, systemic intervention, and beyond. In: Handbook of Systems Sciences. Springer; 2020:1–51.
11. Hofstede SN, van Bodegom-Vos L, Wentink MM, et al. Most important factors for the implementation of shared decision making in sciatica care: ranking among professionals and patients. PLoS One. 2014;9(4):e94176. doi:10.1371/journal.pone.0094176
12. Eliacin J, Salyers MP, Kukla M, Matthias MS. Factors influencing patients’ preferences and perceived involvement in shared decision-making in mental health care. J Ment Health. 2015;24(1):24–28. doi:10.3109/09638237.2014.954695
13. Hughes TM, Merath K, Chen Q, et al. Association of shared decision-making on patient-reported health outcomes and healthcare utilization. Am J Surg. 2018;216(1):7–12. doi:10.1016/j.amjsurg.2018.01.011
14. Légaré F, Witteman HO. Shared decision making: examining key elements and barriers to adoption into routine clinical practice. Health Aff. 2013;32(2):276–284. doi:10.1377/hlthaff.2012.1078
15. Joseph-Williams N, Elwyn G, Edwards A. Knowledge is not power for patients: a systematic review and thematic synthesis of patient-reported barriers and facilitators to shared decision making. Patient Educ Couns. 2014;94(3):291–309. doi:10.1016/j.pec.2013.10.031
16. Crawford JO, Berkovic D, Erwin J, et al. Musculoskeletal health in the workplace. Best Pract Res Clin Rheumatol. 2020;34(5):101558. doi:10.1016/j.berh.2020.101558
17. Li Z, Lin L, Wu H, et al. Global, regional, and national death, and disability-adjusted life-years (DALYs) for cardiovascular disease in 2017 and trends and risk analysis from 1990 to 2017 using the global burden of disease study and implications for prevention. Front Public Health. 2021;9:559751. doi:10.3389/fpubh.2021.559751
18. Kassebaum NJ, Arora M, Barber RM. Global, regional, and national disability-adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE), 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1603–1658. doi:10.1016/S0140-6736(16)31460-X
19. Say RE, Thomson R. The importance of patient preferences in treatment decisions—challenges for doctors. BMJ. 2003;327(7414):542–545. doi:10.1136/bmj.327.7414.542
20. Veenstra CM, Hawley ST. Incorporating patient preferences into cancer care decisions: challenges and opportunities. Cancer. 2020;126(15):3393–3396. doi:10.1002/cncr.32959
21. Prinsen CAC, Mokkink LB, Bouter LM, et al. COSMIN guideline for systematic reviews of patient‐reported outcome measures. Qual Life Res. 2018;27:1147–1157. doi:10.1007/s11136-018-1798-3
22. Goto Y, Miura H, Son D, et al. Psychometric evaluation of the Japanese 9-item shared decision-making questionnaire and its association with decision conflict and patient factors in Japanese primary care. JMA J. 2020;3(3):208–215. doi:10.31662/jmaj.2019-0069
23. Alzubaidi H, Hussein A, Mc Namara K, Scholl I. Psychometric properties of the Arabic version of the 9-item Shared Decision-Making Questionnaire: the entire process from translation to validation. BMJ. 2019;9(4):e026672. doi:10.1136/bmjopen-2018-026672
24. Clayman ML, Bylund CL, Chewning B, Makoul G. The impact of patient participation in health decisions within medical encounters: a systematic review. Med Decis Making. 2016;36(4):427–452. doi:10.1177/0272989X15613530
25. Scalia P, Durand MA, Berkowitz JL, et al. The impact and utility of encounter patient decision aids: systematic review, meta-analysis and narrative synthesis. Patient Educ Couns. 2019;102(5):817–841. doi:10.1016/j.pec.2018.12.020
26. Aasen EM, Kvangarsnes M, Heggen K. Perceptions of patient participation amongst elderly patients with end‐stage renal disease in a dialysis unit. Scand J Caring Sci. 2012;26(1):61–69. doi:10.1111/j.1471-6712.2011.00904.x
27. Martinsson C, Uhlin F, Wenemark M, Eldh AC. Preference‐based patient participation for most, if not all: a cross‐sectional study of patient participation amongst persons with end‐stage kidney disease. Health Expect. 2021;24(5):1833–1841. doi:10.1111/hex.13323
28. Hausheer AC, Suter LC, Kool J. Shared decision-making in physical therapy: a cross-sectional observational study. Eur J Physiother. 2021;23(6):368–376. doi:10.1080/21679169.2020.1772869
29. Joseph-Williams N, Lloyd A, Edwards A, et al. Implementing shared decision making in the NHS: lessons from the MAGIC programme. BMJ. 2017;357:j1744. doi:10.1136/bmj.j1744
30. McIntosh MJ, Morse JM. Situating and constructing diversity in semi-structured interviews. Glob Qual Nurs Res. 2015;2:2333393615597674. doi:10.1177/2333393615597674
31. Lyon MF. A mixed method analysis of the role of balance outcome measures in therapist decision-making and patient outcomes; 2020.
32. Patel S, Ngunjiri A, Hee SW, et al. Primum non nocere: shared informed decision making in low back pain–a pilot cluster randomized trial. BMC Musculoskelet Disord. 2014;15:282. doi:10.1186/1471-2474-15-282
33. van Dulmen SA, Maas M, Staal JB, et al. Effectiveness of peer assessment for implementing a Dutch physical therapy low back pain guideline: cluster randomized controlled trial. Phys Ther. 2014;94(10):1396–1409. doi:10.2522/ptj.20130286
34. Beneciuk JM, Osborne R, Hagist MB, et al. American Physical Therapy Association Clinical Practice Guideline implementation for neck and low back pain in outpatient physical therapy: a nonrandomized, cross-sectional stepped-wedge pilot study. J Orthop Sports Phys Ther. 2022;52(2):113–123. doi:10.2519/jospt.2022.10545
35. Elwyn G, Edwards A, Wensing M, et al. Shared decision making: developing the OP-TION scale for measuring patient involvement. BMJ Qual Saf. 2003;12:93–99.
36. Légaré F, Ratté S, Gravel K, Graham ID. Barriers and facilitators to implementing shared decision-making in clinical practice: update of a systematic review of health professionals’ perceptions. Patient Educ Couns. 2008;73(3):526–535. doi:10.1016/j.pec.2008.07.018
37. Lamb CC, Wang Y, Lyytinen K. Shared decision making: does a physician’s decision‐making style affect patient participation in treatment choices for primary immunodeficiency? J Eval Clin Pract. 2019;25(6):1102–1110. doi:10.1111/jep.13162
38. Budtz CR, Rønn-Smidt H, Thomsen JNL, Hansen RP, Christiansen DH. Primary care physiotherapists ability to make correct management decisions–is there room for improvement? A mixed method study. BMC Fam Pract. 2021;22(1):196. doi:10.1186/s12875-021-01546-1
39. Shay LA, Lafata JE. Understanding patient perceptions of shared decision making. Patient Educ Couns. 2014;96(3):295–301. doi:10.1016/j.pec.2014.07.017
40. Nicholson E, McDonnell T, De Brún A, et al. Factors that influence family and parental preferences and decision making for unscheduled paediatric healthcare–systematic review. BMC Health Serv Res. 2020;20(1):663. doi:10.1186/s12913-020-05527-5
41. Shahin W, Kennedy GA, Stupans I. The impact of personal and cultural beliefs on medication adherence of patients with chronic illnesses: a systematic review. Patient Prefer Adherence. 2019;13:1019–1035. doi:10.2147/PPA.S212046
42. Stenner R, Palmer S, Hammond R. What matters most to people in musculoskeletal physiotherapy consultations? A qualitative study. Musculoskelet Sci Pract. 2018;35:84–89. doi:10.1016/j.msksp.2018.03.005
43. Poprzeczny AJ, Stocking K, Showell M, Duffy JMN. Patient decision aids to facilitate shared decision making in obstetrics and gynecology: a systematic review and meta-analysis. Obstet Gynecol. 2020;135(2):444–451. doi:10.1097/AOG.0000000000003664
44. Hargraves I, Montori VM. Decision aids, empowerment, and shared decision making. BMJ. 2014;349:g5811. doi:10.1136/bmj.g5811
45. Muscat DM, Shepherd HL, Nutbeam D, Trevena L, McCaffery KJ. Health literacy and shared decision-making: exploring the relationship to enable meaningful patient engagement in healthcare. J Gen Intern Med. 2021;36(2):521–524. doi:10.1007/s11606-020-05912-0
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Shared Decision-Making in the Treatment of Multiple Sclerosis: Results of a Cross-Sectional, Real-World Survey in Europe and the United States
Keenan A, Le HH, Gandhi K, Adedokun L, Jones E, Unsworth M, Pike J, Trenholm E
Patient Preference and Adherence 2024, 18:137-149
Published Date: 16 January 2024
Factors Influencing Decision-Making and Rehabilitation Among Older Women Who Underwent Total Knee Replacement: A Qualitative Study in Taiwan
Huang CH, Chen YY, Chen SW, Wang CT, Lin MH
Patient Preference and Adherence 2025, 19:3931-3944
Published Date: 9 December 2025