")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Expectations and Experiences of a Group of Patients Enrolled in an Educational Program for Rheumatoid Arthritis at a Specialized Care Center in Colombia
Authors Castiblanco-Montañez RA, Buitrago-Garcia D, Arévalo Velandia A, Garzón-Cepeda JD, Rodríguez-Florido F, Sánchez Vanegas G , Santos-Moreno P
Received 3 July 2022
Accepted for publication 26 October 2022
Published 22 February 2023 Volume 2023:16 Pages 483—492
DOI https://doi.org/10.2147/JMDH.S380001
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Ruth Alexandra Castiblanco-Montañez,1 Diana Buitrago-Garcia,2,3 Adriana Arévalo Velandia,4 Julián David Garzón-Cepeda,4 Fernando Rodríguez-Florido,5 Guillermo Sánchez Vanegas,2,6 Pedro Santos-Moreno5
1Care Perspectives Research Group, Faculty of Nursing, Fundación Universitaria de Ciencias de la Salud – FUCS, Bogotá, Colombia; 2Clinical Epidemiology Graduate Program, Fundación Universitaria de Ciencias de la Salud – FUCS, Bogotá, Colombia; 3Institute of Social and Preventive Medicine (ISPM) and Graduate School for Health Sciences, University of Bern, Bern, Switzerland; 4Faculty of Nursing, Fundación Universitaria de Ciencias de la Salud – FUCS, Bogotá, Colombia; 5BIOMAB IPS -Center for Rheumatoid Arthritis, Bogotá, Colombia; 6Clinical Epídemiology, Hospital Universitario Mayor-Méderi, Universidad del Rosario, Bogotá, Colombia
Correspondence: Pedro Santos-Moreno, BIOMAB IPS -Center for Rheumatoid Arthritis, Calle 48 # 13-86, Bogotá, Colombia, Tel +57 3208094232, Email [email protected]
Introduction: Rheumatoid arthritis is a chronic inflammatory disease diagnosed in a productive stage of life. Patients with RA experience changes in their musculoskeletal system, overall health and quality of life. It has been identified that patients with RA do not have appropriate knowledge about their condition. Educational programs can provide new knowledge, accompaniment, and closer follow-up to improve empowerment and quality of life in patients with RA.
Purpose: To describe rheumatoid arthritis patients’ experiences, perceptions, and expectations when enrolling on a multicomponent educational program in a specialized RA setting.
Patients and Methods: A qualitative study was done. Patients with RA who attended a specialized center and enrolled in an educational program participated in two focus groups. The focus group discussions and the interviews were recorded, transcribed verbatim, analyzed, and emerging themes were constructed.
Results: Thirty-one participants were included in the focus groups. The median age was 60 years IQR (54– 67), 92% were female. Two relevant categories emerged: first, the experience of being diagnosed with RA. Second, the program’s ability to empower participants with knowledge and the possibility of transferring knowledge to other patients with the same condition. In addition, patients gave a high score to the expectations regarding the educational program.
Conclusion: Understanding patients’ expectations when enrolling in an educational program allows educators and clinicians to understand their motivations to create tailored programs that can contribute to acquiring empowerment in the educational process and managing their disease. Stakeholders should consider patients’ expectations when implementing these interventions for patients with RA to adapt the intervention according to the patient’s context and needs, which will directly affect the patient’s adherence and lead to better use and allocation of resources for educational activities.
Keywords: qualitative research, patient preference, patient education
Introduction
Rheumatoid arthritis (RA) is a chronic autoimmune, inflammatory, high-cost disease whose origin involves genetic, environmental, ethnic, and nutritional factors; it affects mainly women in their productive life stage.1 It is characterised by a deterioration of the synovial membranes of the arthrodial joints, which causes pain and inflammation, resulting in severe disability over time. RA results in anatomical changes, affecting the patient physically and psychologically.2 These changes generate difficulty in daily activities, cause pain and disability, and alter the patients’ social, family, and work relationships.3,4 RA affects between 3 and 7% of the population worldwide1, while in low-middle-income countries such as Colombia, the prevalence is 1.49 (95% CI 1.10–1.92).5,6 The aim of the treatment for a patient with RA is to achieve remission or low disease activity, mainly by prescribing a treatment that helps maintain joint function.2 Currently, patients receive synthetic disease-modifying antirheumatic drugs (DMARDs), biologic DMARDs, and targeted synthetic DMARDs7 as pharmacological treatment. In addition, it is recommended that RA patients be managed by a group of specialists such as rheumatologists, psychologists, physiotherapists, occupational therapists, nutritionists, and social workers. It is also recommended to include an educational process to involve the patient in the management process.8
Previous research has identified that patients’ knowledge can improve when they attend one-on-one training sessions where health professionals inform them about their condition and the implications of RA in daily life.9,10 Additionally, implementing educational programs to improve overall patients’ health through accompaniment and empowerment has helped reduce the effects of the disease when used as an additional intervention to conventional health care.10 A study conducted in 2005 with Colombian patients showed how an educational intervention could improve knowledge and physical function in patients with RA.11 The Pan American League of Associations of Rheumatology (PANLAR) recommends the existence of educational programs for people with RA from the initial diagnosis and on an ongoing basis, based on a formal, regular assessment of needs.10 Despite the call for educational intervention for RA patients in countries such as Colombia, there are few programs for patients and caregivers. Regular assessment of needs includes exploring the expectations of patients on RA. The study by Nymberg et al showed that getting to know the expectations of older adults around e-health was relevant to understanding factors related to their adherence and how healthcare personnel interventions should be tailored according to patients’ needs.12 Understanding patients’ expectations when entering an educational program focused on RA can fill the knowledge gap that clinicians can have. It can be helpful to identify their perceptions and ideas, and barriers that deteriorate the educational process. This information can be the base for creating strategies to avoid their dropping out of educational programs.
This study aims to describe patients’ experiences with RA and their perceptions and expectations when participating in a multicomponent educational program in a specialized center in Bogotá - Colombia.
Materials and Methods
A concurrent mixed design was used with a qualitative approach for this study. RA patients attending a specialized center in Bogotá, Colombia, were invited to participate and enrolled in the “UniversitAR - University of Patients with Rheumatoid Arthritis” education program.
UniversitAR is a multicomponent educational program that seeks to train patients with RA so that over time they become Expert Patients in their health condition, so that they, in turn, become educators for other patients, transferring knowledge about concepts of disease, the importance of adherence to treatment, the relationship between patient and the medical team, and the adoption of healthy lifestyles such as incorporating physical activity or the importance of a balanced diet. The program is based on active participation in treatment, physical activity, healthy nutrition, empowerment, and soft skills development. All patients enrolled had access to the educational program.
All patients who enrolled at the beginning of the educational program were invited to fill out sociodemographic information and the scale of expectations adapted from Borkovec and Nau.12 This tool assesses the patient’s perception of the intervention. The scale has the following five questions:
- How logical is/seems the educational program seem to you?
- How satisfied are you with the educational program?
- How confident would you feel about recommending the educational program?
- How useful do you think the educational program is?
- How dissatisfied are you with the educational program?
The scores ranged from 0 (not at all) to 10 (very much). The patients’ perception was addressed with this scale, and an open question was added for observations.
Statistical analysis was performed using STATA 14®, quantitative variables were reported through measures of central tendency, and qualitative variables were reported as absolute and relative frequencies. A content analysis was used for the open question on program observations, and the relationships between the reported data were described.
Qualitative Component
After the first meeting, participants were invited to a focus group discuss their perceptions and expectations regarding the program through a dynamic process in which the participants exchanged their ideas and opinions.13 A group interview script was used to identify the patients’ experiences with their diagnosis and their expectations regarding the program. Two focus groups were held with an average duration of one hour; the discussion was recorded on audio and transcribed verbatim.
For the analysis, a matrix was built on Microsoft Excel®, following the proposal of Janice M. Morse, where a microanalysis of the stories of each participant was carried out, reviewing and comparing the group discourse to extract the relevant data.14 The data were interpreted and coded into two final categories: Living with rheumatoid arthritis: an unexpected diagnosis that originated radical changes; adherence and expectations of the program to empower patients and increase their knowledge.
Ethical Approval
This project was approved by an ethics Committee, “Comité de Ética en Investigación en Seres Humanos-CEISH”, from the Fundación Universitaria de Ciencias de la Salud-FUCS. Bogotá, Colombia.
Results
In the initial descriptive component, 132 participants provided information about sociodemographic characteristics and filled out the scale of Borkovec and Nau.12 The median age of the participants was 60 years IQR (54–67); 92% were female, 35% were married and, the majority had completed secondary education (Table 1).
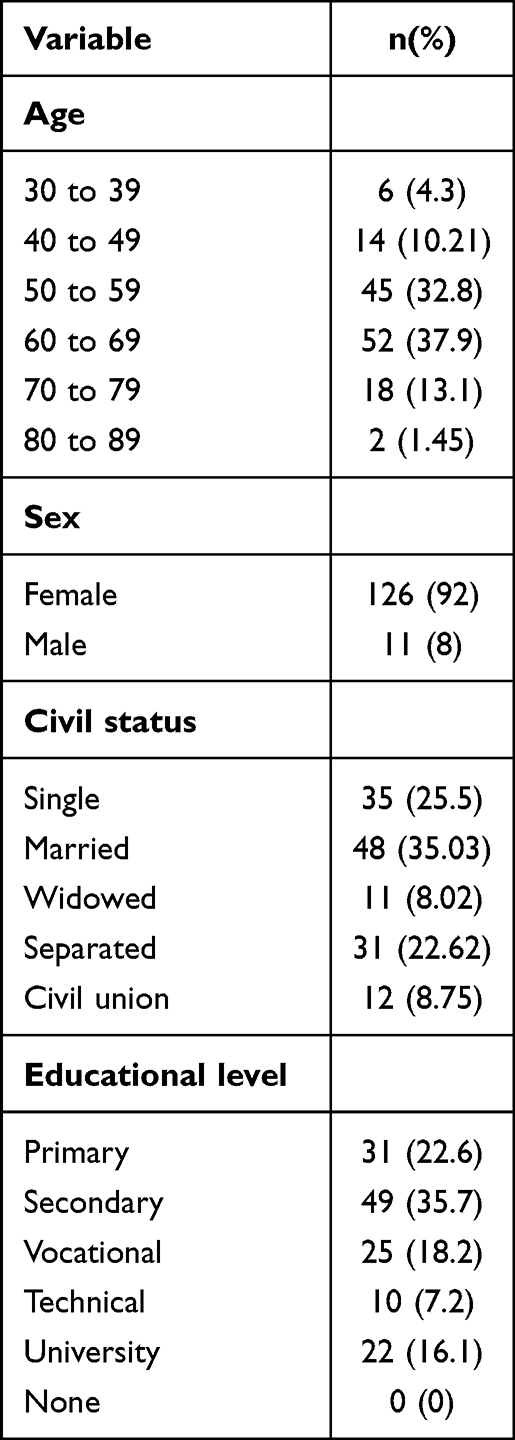 |
Table 1 Sociodemographic Characteristics |
When we evaluated the program expectations through the adapted scale of Borkovec and Nau,12 most participants rated all the questions above seven, and only one rated the logic of the intervention with six points. When asked if the program is logical, it was found that 77.7% of the participants rated it at the level “very much”, 74.4% of the participants rated satisfaction at the “very much” level, and 78.5% would recommend the program within level 10. Likewise, 80.7% of the participants rated the question about intervention usefulness at the highest level of the scale. (Table 2).
 |
Table 2 Scale of Expectations About the Program |
Additionally, in the open question field, participants expressed positive comments such as gratefulness, given that these activities can lead them to a better state of health. The participants also mentioned feeling satisfaction since these activities allow them to expand their knowledge and replicate their learning with their peers with rheumatoid arthritis.
Results of the Qualitative Component
In total, 31 participants attended the focus groups. After conducting the interviews, two final categories emerged through the interviews carried out in the focus groups that speak of the participant’s experience with the disease. This experience highlights the disease’s unexpected appearance, the doubts and uncertainties generated from the diagnosis, and the implications that this health condition causes in their daily lives.
First Category: Living with Rheumatoid Arthritis: An Unexpected Diagnosis in Patients’ Lives
Patients find the diagnosis of RA difficult as it is a chronic inflammatory autoimmune disease, diagnosed at the productive age of the person and with whom they have presented difficulties related to access to care.
Healthcare Barriers
Within the process of diagnosis and treatment, the patients described different health care barriers: geographical ones, which referred to the lack of availability, economic restrictions, and difficulties in getting to the health care center since some of the participants do not reside in the city where they receive treatment. Participants reported administrative barriers such as delays in authorizations for appointments with specialists (eg, rheumatologist), delays in providing services such as supplies or deliveries of medications, lack of timely care, and lack of specialists. All of this causes patients to receive varied inadequate treatments without effective results.
Likewise, the participants reported personal barriers where ignorance and the treatment received influenced their emotional and psychological state. The above was evidenced in a lack of response to their needs, disablement, and demotivation, focusing attention on the resolution of physical and clinical aspects, leaving aside the social, spiritual, and psychological dimensions that prevent providing an appropriate diagnosis and adequate treatment (See Box 1).
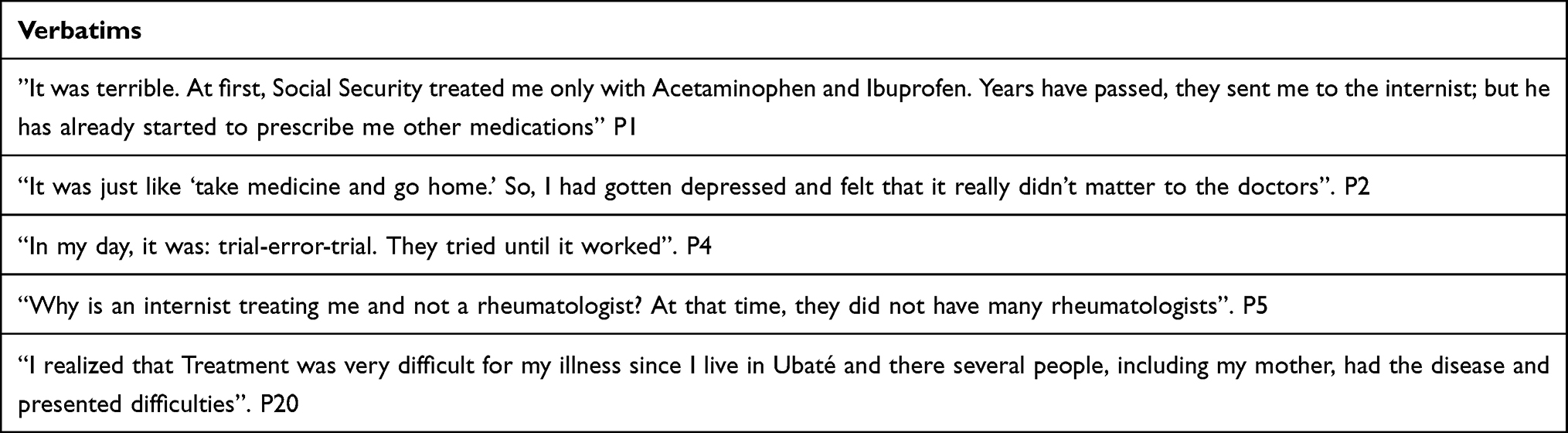 |
Box 1 Live Stories |
Implications of the Disease
We identified that physical effects generate severe and permanent damage to the joints of the hands and feet with significant deformities in the participants, which limited their daily activities such as sitting, tying a shoe, going downstairs, walking, etc.
Some participants received pharmacological therapies to stabilise their condition and improve pain, which led to various adverse effects such as depression, general malaise, and weight gain. Unfortunately, the above occurred without prior dialogue between the patients and the health personnel, leading to discomfort, lack of adherence, and abrupt lifestyle changes.
Regarding the personal and social implications, their work activities changed; in some cases, their state of health did not allow them to carry out the same activity, forcing them to have a job recession, retire, or change jobs due to disability. Consequently, at the family level, some participants reported reduced income, rejection, family intolerance, and overload of their caregivers. On a personal level, they reported emotional instability, substantial lifestyle changes, feelings of worthlessness, incapacity, weakness, and uncertainty facing their new condition (see Box 2).
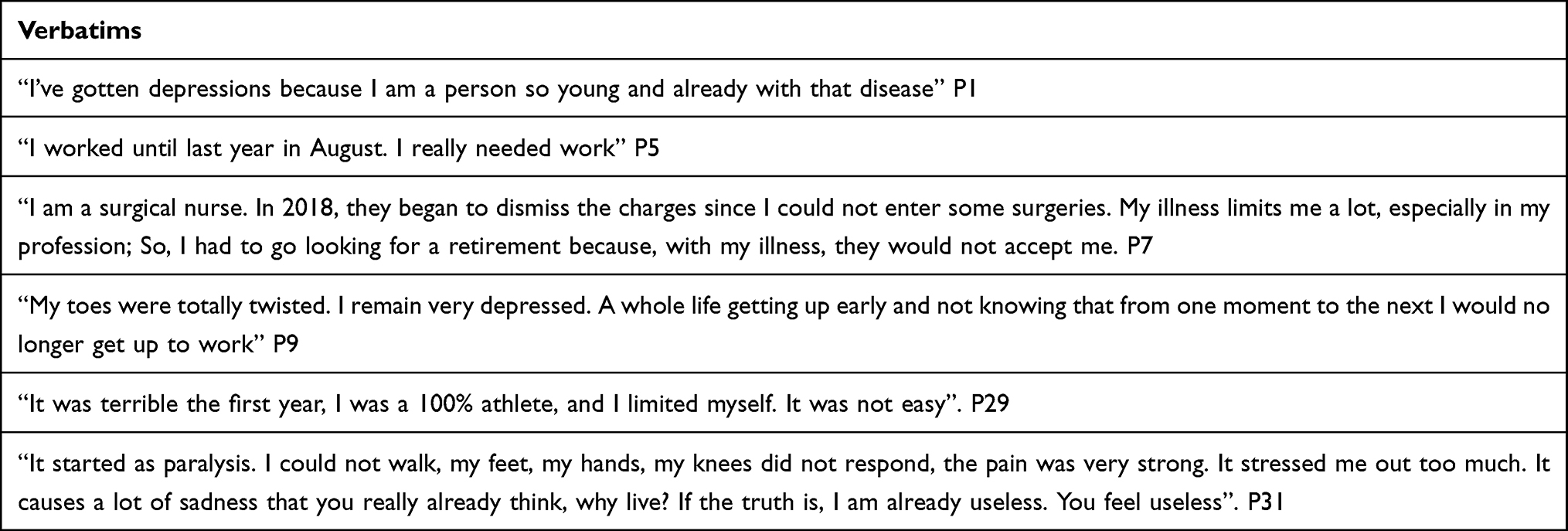 |
Box 2 Disease Implications |
Ignorance and Lack of Interest Regarding the Disease on the Participant’s Part
Some participants were aware of the lack of knowledge about their disease. This lack of knowledge led them to consult information from unreliable sources, making wrong decisions such as self-medication, which prolongs and worsens their diagnosis and decreases their adherence to any treatment. They also mentioned factors such as the lack of time and the importance of undergoing a clinical assessment. Patients did it when the disease began to produce physical conditions such as deformities. At that time, they showed genuine interest in consulting, thus decreasing the disease’s risks (See Box 3).
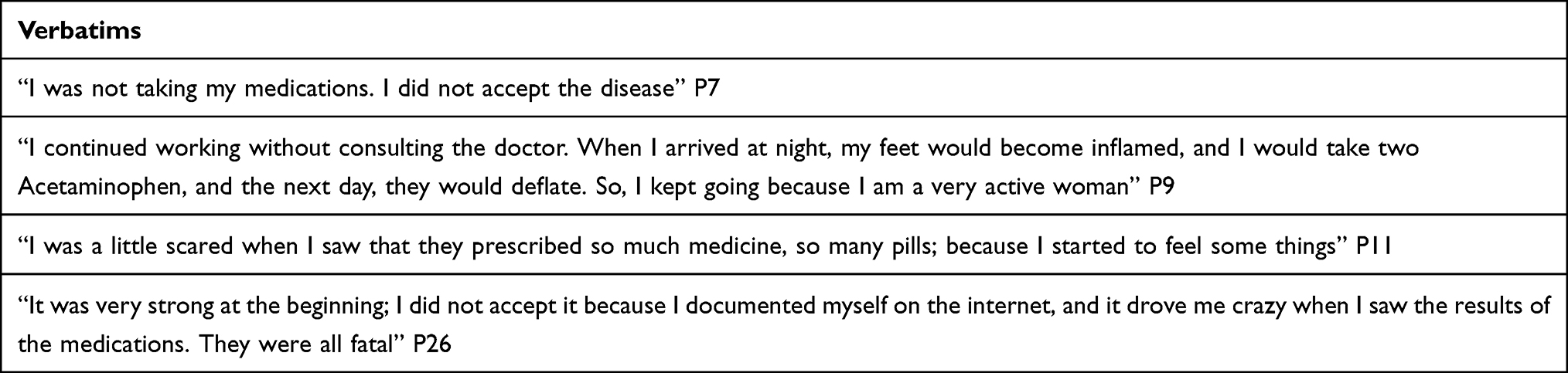 |
Box 3 Attitudes Towards the Disease |
Second Category: Expectations of the Program to Empower Patients and Increase Their Knowledge
The patients who started participating in the educational program raised different expectations regarding the program to empower themselves, improve their quality of life, and become Expert Patients.
Empowerment and Motivations in the Program
The patients stated that their expectations with this program were expanding their knowledge, improving their lifestyles, obtaining accurate information to dispel various myths, and having greater empowerment about their health condition and quality of life. They also spoke about the program motivating them to fight for their rights in the health system and learn to understand and improve their disease and pharmacological treatment. The majority expressed wanting to see the disease as their friend or a life partner. In addition, self-motivation by observing other patients’ psychological and emotional progress with the same condition in the program also expressed the importance of maintaining a positive attitude to improve the attitudes and emotions of the whole family (See Box 4).
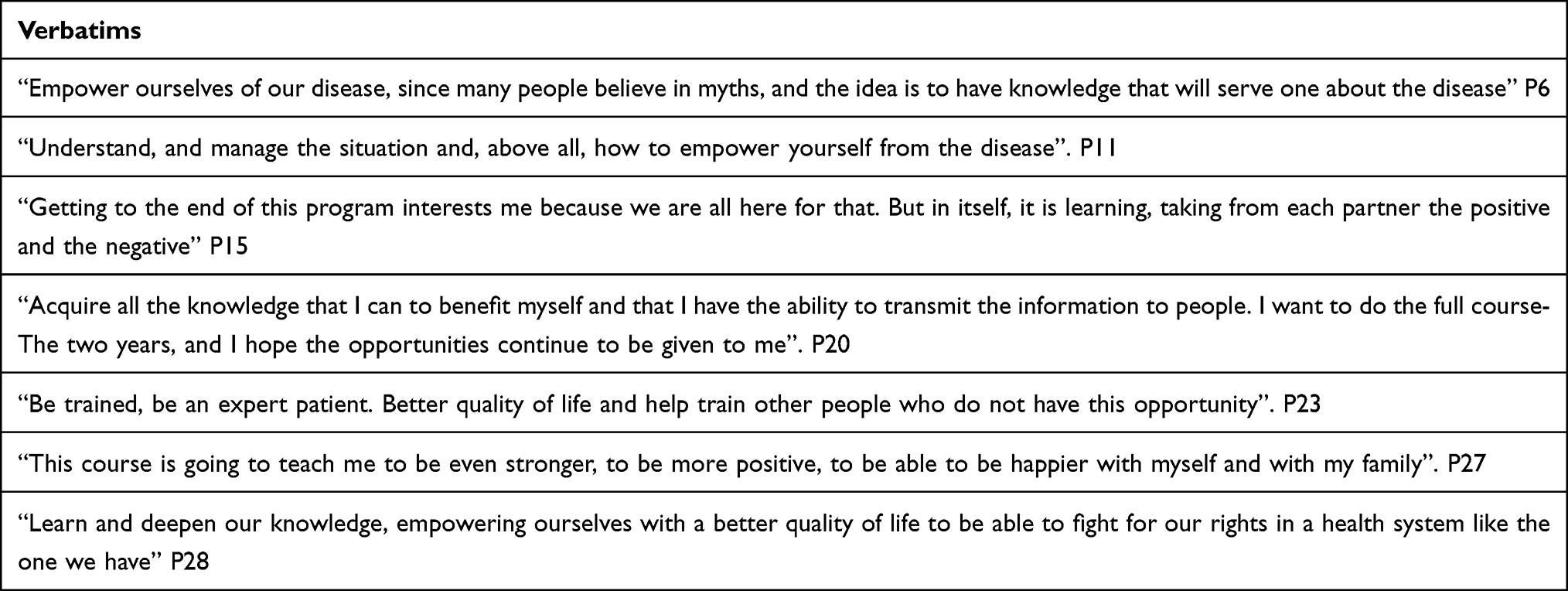 |
Box 4 Patients’ Expectations |
Among the most pressing expectations for patients was being an Expert Patient; this means empowering themselves regarding their disease to provide education and expanding the knowledge of other patients who suffer from the disease and who probably have wrong information or are unaware of many things about the disease. Some participants stated that they wanted to support those who require it, presenting information about the disease in a general way through workshops and conferences and creating spaces where expert patients will listen to the needs of other participants, giving them timely advice. All of this is to help patients with health difficulties (See Box 5).
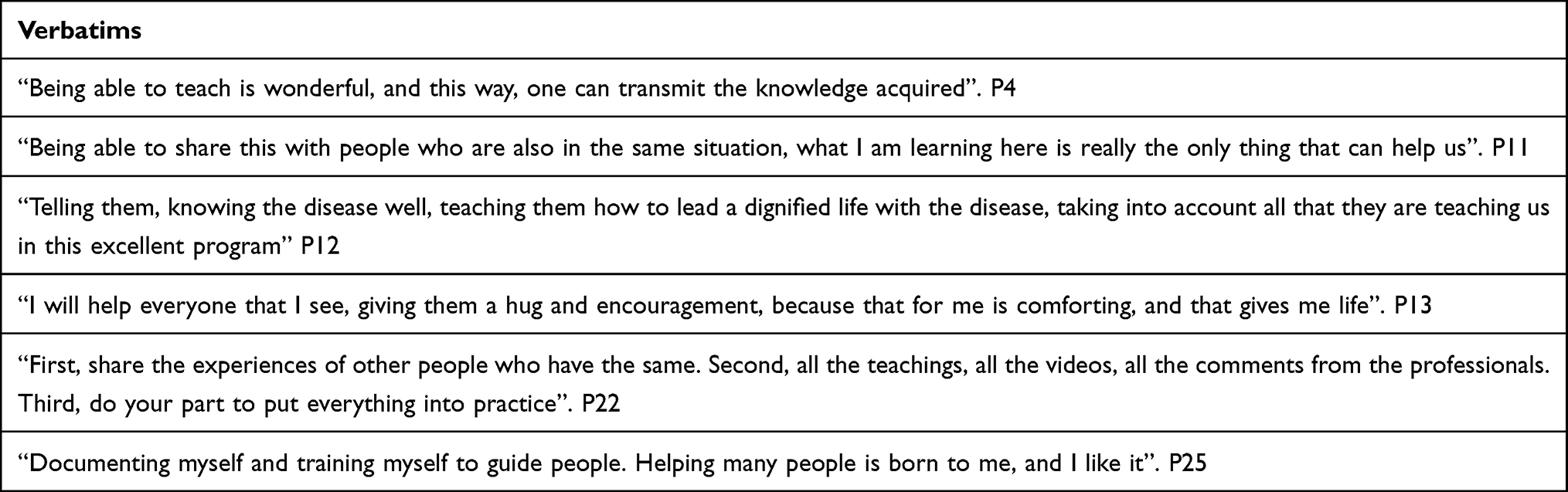 |
Box 5 The Role of the Expert Patient as One Relevant Expectation |
The Educational Program as a Factor to Accept the Disease
Patients describe diverse factors that enhance or improve their experience with the disease, managing to accept it and increasing their treatment adherence. Many patients reiterate that learning about the disease improves their quality of life. It was easier for them to manage their current lifestyle after better understanding RA or having a relative or acquaintance with the disease. In addition, some were driven by additional motivation, such as their family, health personnel, or occupational activities, thus achieving a positive attitude. These patients’ lives have improved by acting positively, and many even try to help others. They manage to feel useful and help prevent, guide, and educate those who are just beginning with their disease and may make mistakes due to their inexperience. All this leads to accepting the disease and improving the lifestyles of patients (See Box 6).
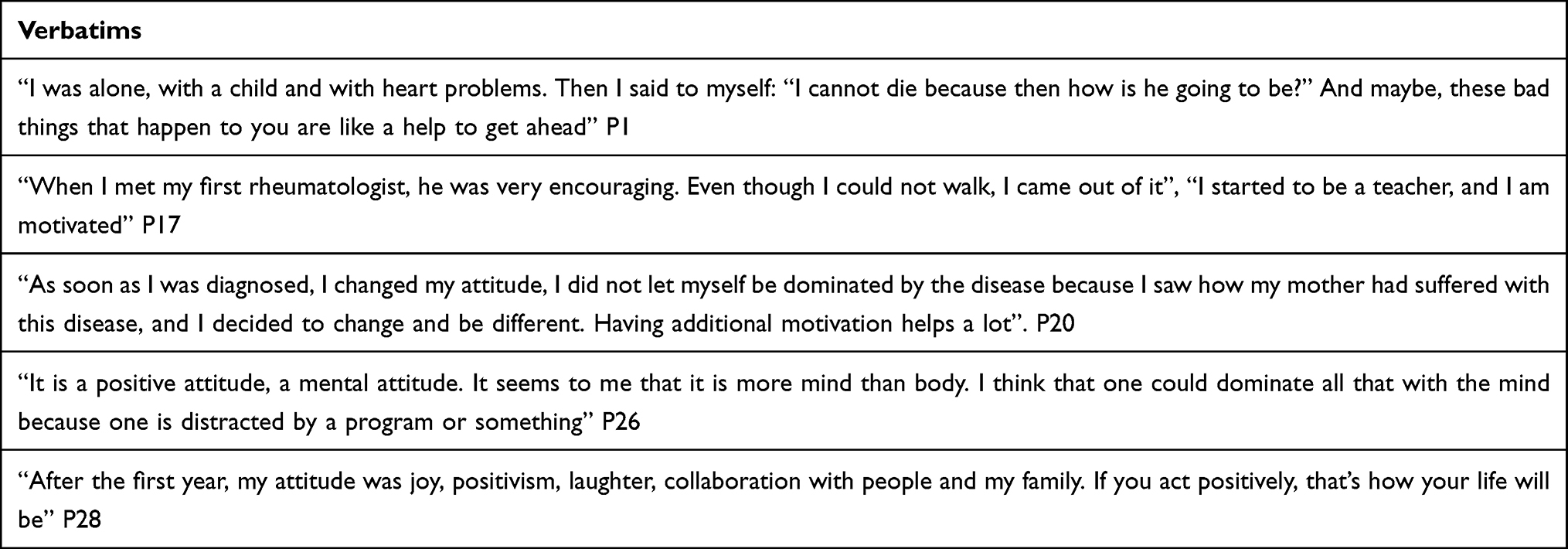 |
Box 6 Factors That Enhance or Improve the Experience of Living with RA |
Adherence and Dropout Factors are Essential in the Development of the Multicomponent Educational Program
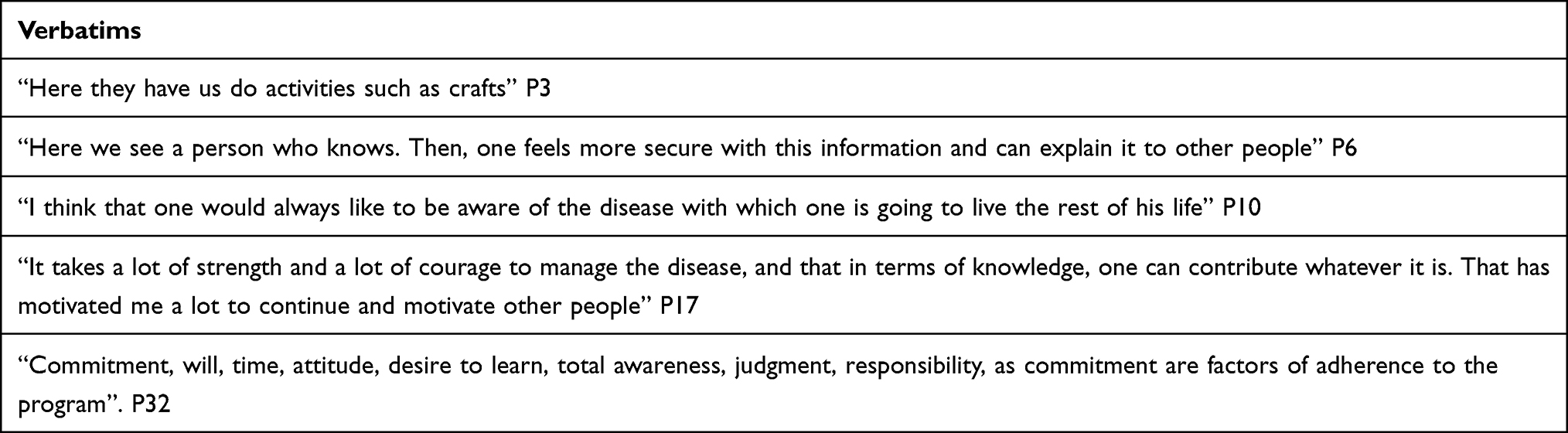
It is essential to consider some factors that favour adherence to the program. Among them are: the opportunity to learn more about the disease, carrying out didactic activities, greater confidence in the staff, and personal aspects such as “Strength, courage, will, experience, knowledge, attitude, and vocation” that increased adherence to the program and therefore their quality of life.
We found that some patients presented difficulties leading to dropping out of the program and decreasing adherence to it. One of these was the patient’s economic situation since the transportation to and from the appointments means additional expenses. It makes adherence difficult since by not attending the program, the continuity of the information received would be lost, hindering the learning process (See Box 7).
 |
Box 7 Experiences Around the Educational Program |
Discussion
We found that patients with RA have high expectations and satisfaction when accessing an educational program to improve their condition. Patients described that receiving the diagnosis of RA was unexpected, and they perceived the effects of their disease at the physical, psychological and social levels, almost always with negative consequences in their lives. Patients reported that attending a structured educational program allowed them to acquire knowledge and avoid consulting unreliable sources that may lead them to self-medication or not adhere to treatment due to the variety of information about RA. Additionally, they recognised that receiving education is an opportunity to empower themselves and it is an opportunity to become active actors in managing their condition and help their peers with RA.
Our findings are similar to those of other published studies, such as the one conducted by Kristiansen et al15 who, through an ethnographic study, identified that patients with RA who participate in an educational program could make a transition between having an RA diagnosis, acquiring concepts, and being a chronic patient with knowledge or a patient who is an expert on their disease. This study also highlighted the importance of receiving education from professional staff who can guide them through their process.
Regarding the evaluation of evidence on the subject from a quantitative perspective, a randomised clinical trial done by Moghadam et al16 that aimed to assess the effect of an educational program on self-confidence in women with RA demonstrated that educational programs could be effective in developing awareness in women with RA and at the same time allowed them to create alternatives to adapt to the changes that the disease brings. The study published by Barlow et al17 found that once they receive structured education about RA, patients can change their behaviour, better adhere to treatment, and improve their quality of life. In the Latin American context, the study by Castellano and collaborators showed that psychological stress might trigger symptoms in RA. Therefore, the more unstable the emotional state of patients with RA, there may be pain increments and other symptoms of the disease, which can generate resistance to their condition, worsening their quality of life, coinciding with what is manifested by the patients who participated in our study.18
Educational programs conducted in patients with other chronic conditions have also shown the significant potential to improve their lives. A study conducted by Almeida et al19 found that participants who received an educational intervention compared to the group that received only conventional care had better self-care outcomes in managing the therapeutic regimen.21 When patients know their perceptions of the disease, it is possible to understand how the condition influenced their life and emotions and how misconceptions can be addressed in tailored educational programs.20 From the decision-making perspective incorporating the patients’ voice from a qualitative approach has shown how it is possible to call attention to the barriers and facilitators to adopting new interventions and technologies into different populations and how tailored interventions are needed.21
One of the strengths of this study is that it is a pioneer in investigating from a qualitative perspective the expectations of patients who decided to participate in an educational program from a qualitative methodology. These findings may lead to new educational interventions directly affecting patients with chronic diseases such as RA. In addition, it provides evidence in the rheumatology specialty as it relates to the values and preferences of patients, a vital component in evidence-based practice.22 We also are aware of the study’s limitations. Due to the nature of the qualitative design23 we included a small and non-random sample of patients, which may lead to selection bias due to the willingness to participate in our study; thus, it is impossible to confirm that our results represent the total population of patients with RA. Additionally, due to the time since the RA diagnosis patients could this study could be at risk of recall bias. Finally, since patients were already enrolled in the educational program and knew that they were being questioned about the program, there may be response bias, resulting in a positive response to the program’s expectations and qualifications.
Conclusion
Knowing the expectations, experiences, and feelings of patients with RA regarding their condition and entering an educational program has allowed us to understand the complexity of RA from another point of view. Additionally, it enables us to know patients’ expectations for a program that responds to the needs of patients. Evidence obtained by applying qualitative research methods is a starting point to highlight the patients’ voices in the policymaking process and for health systems to formally create educational programs for patients with chronic conditions such as RA.
Ethics Approval and Informed Consent
An Ethics Committee approved this project. This study complies with the Declaration of Helsinki.
The study participants previously signed an informed consent form, expressing their total autonomy, willingness, and prior understanding of its scope. Participants consented the publication of anonymised responses.
Funding
This study is part of the project “Impact of the implementation of a multicomponent educational program for patients with rheumatoid arthritis in a specialized center in Bogotá. Colombia” (695180763684), funded by the Ministry of Science, Technology, and Innovation of Colombia (MINCIENCIAS), through call 807 for Science, Technology, and Innovation in Health projects – 2018.
Disclosure
PSM has received financial compensation for conferences, counselling, advisory boards, and travel. It also has received financial support to attend academic events and project funding from AbbVie, Abbott, Biopas-UCB, Bristol, Janssen, Lilly, Pfizer, Roche, and Sanofi. RACM, DBG, AAV, JDG, FRF and GSV have no conflicts of interest in this work.
References
1. Cross M, Smith E, Hoy D, et al. The global burden of rheumatoid arthritis: estimates from the global burden of disease 2010 study. Ann Rheum Dis. 2014;73(7):1316–1322. doi:10.1136/annrheumdis-2013-204627
2. Lee DM, Weinblatt ME. Rheumatoid arthritis. Lancet. 2001;358(9285):903–911. doi:10.1016/S0140-6736(01)06075-5
3. Franco-Aguirre JQ, Cardona-Tapias AA, Cardona-Arias JA. Health Related Quality of Life in Patients with Rheumatoid Arthritis from Medellín-Colombia, 2014. Rev Colomb Reumatol. 2015;22:153–161. doi:10.1016/j.rcreu.2015.08.001
4. Huyser B, Parker JC. Stress and rheumatoid arthritis: an integrative review. Arthritis Care Res. 1998;11(2):135–145. doi:10.1002/art.1790110209
5. Londoño J, Peláez-Ballestas I, Cuervo F, et al. Prevalence of rheumatic disease in Colombia according to the Colombian Rheumatology Association (COPCORD) strategy. Prevalence study of rheumatic disease in Colombian population older than 18 years. Rev Colomb Reumatol. 2018;25:245–256. doi:10.1016/j.rcreu.2018.08.003
6. Fernández-ávila DG, Rincón-Riaño DN, Bernal-Macías S, Gutiérrez Dávila JM, Rosselli D. Prevalence of rheumatoid arthritis in Colombia according to information from the comprehensive Information System of Social Security. Rev Colomb Reumatol. 2019;26:83–87. doi:10.1016/j.rcreu.2019.01.003
7. Radu AF, Bungau SG. Management of rheumatoid arthritis: an overview. Cells. 2021;10:11. doi:10.3390/cells10112857
8. Santos-Moreno P, Castañeda O, Garro B, Flores D, Sánchez G, Castro C. From the model of integral attention to the creation of centers of excellence in rheumatoid arthritis. Clin Rheumatol. 2015;34(Suppl1):S71–S77. doi:10.1007/s10067-015-3017-8
9. Mäkeläinen P, Vehviläinen-Julkunen K, Pietilä AM. Rheumatoid arthritis patients’ knowledge of the disease and its treatments: a descriptive study. Musculoskelet Care. 2009;7(1):31–44. doi:10.1002/msc.138
10. Khoury V, Kourilovitch M, Massardo L. Education for patients with rheumatoid arthritis in Latin America and the Caribbean. Clin Rheumatol. 2015;34 Suppl 1(Suppl1):S45–49. doi:10.1007/s10067-015-3014-y
11. Escorcia ME, Osorio H, Pérez CA, Thulcán M, Caballero Uribe CV, Borda pérez M. Effectiveness of an Educational Intervention in Patients with Rheumatoid Arthritis. University Hospital North. Barranquilla. April-May, 2005. Rev Colomb Reumatol. 2006;13:11–19.
12. Borkovec TD, Nau SD. Credibility of analogue therapy rationales. J Behav Ther Exp Psychiatry. 1972;3(4):257–260. doi:10.1016/0005-7916(72)90045-6
13. Silveira Donaduzzi D, Colomé BCL, Heck WT, Nunes da Silva Fernandes M, Viero V. Focal group and content analysis in qualitative research. Index Enferm. 2015;24(1–2):71–75. doi:10.4321/S1132-12962015000100016
14. Morse JM, Bottorff J. Critical in qualitative research methods issues. Universidad de Alicante Alicante; 2005.
15. Kristiansen TM, Antoft R. Patient education as a status passage in life - an ethnographic study exploring participation in a Danish group based patient education programme. Soc Sci Med. 2016;158:34–42. doi:10.1016/j.socscimed.2016.04.012
16. Moghadam H, Iran H, Mohammad Ali N. The effect of educational program on self-efficacy of women with rheumatoid arthritis: a randomized controlled clinical trial. Int J Community Based Nurs Midwifery. 2018;6(1):12–20.
17. Barlow JH, Turner AP, Wright CC. A randomized controlled study of the arthritis self-management programme in the UK. Health Educ Res. 2000;15(6):665–680. doi:10.1093/her/15.6.665
18. Castellano G, Alemán A, Irisarri M, Callero W, Siri J. Effects of a Mindfulness-based stress reduction intervention (MBSRP) on clinical parameters in Rheumatoid Arthritis. Rev Urug Med Interna. 2019;4:15–23.
19. Almeida M, Sousa M, Loureiro H. Effectiveness of an empowerment-based educational program in self-efficacy perception in patients with diabetes. Rev Enferm Ref. 2019;IV Série:33–42. doi:10.12707/RIV19037
20. Nasimi M, Abedini R, Daneshpazjooh M, et al. Illness perception of patients with pemphigus vulgaris. Int J Womens Dermatol. 2019;5(2):96–99. doi:10.1016/j.ijwd.2018.08.012
21. Jones IR, Berney L, Kelly M, et al. Is patient involvement possible when decisions involve scarce resources? A qualitative study of decision-making in primary care. Soc Sci Med. 2004;59(1):93–102. doi:10.1016/j.socscimed.2003.10.007
22. Sackett DL, Rosenberg WMC, Gray JAM, Haynes RB, Richardson WS. Evidence based medicine: what it is and what it isn’t. BMJ. 1996;312(7023):71. doi:10.1136/bmj.312.7023.71
23. Pope C, Ziebland S, Mays N. Qualitative research in health care. Analysing qualitative data. BMJ. 2000;320(7227):114–116. doi:10.1136/bmj.320.7227.114
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.