Back to Journals » Journal of Pain Research » Volume 18
Factors Associated with Depression, Anxiety, and Sleep Disturbance Among Patients with Moderate-to-Severe Chronic Pain: A Multicenter Cross-Sectional Study
Authors Guo SQ ![]() , Wang LQ, Tu JF
, Wang LQ, Tu JF ![]() , Yang JW
, Yang JW ![]() , Shi GX, Yan SY, Li T, Fu Y, Zhou ZY, Ji CC, Hu H, Han LF, Liu M, Xu SF, Li M, Liu LY, Chen F, Liu CZ
, Shi GX, Yan SY, Li T, Fu Y, Zhou ZY, Ji CC, Hu H, Han LF, Liu M, Xu SF, Li M, Liu LY, Chen F, Liu CZ ![]()
Received 15 August 2025
Accepted for publication 27 November 2025
Published 16 December 2025 Volume 2025:18 Pages 6791—6805
DOI https://doi.org/10.2147/JPR.S561047
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jonathan Greenberg
Shi-Qi Guo,1 Li-Qiong Wang,1 Jian-Feng Tu,1 Jing-Wen Yang,1 Guang-Xia Shi,1 Shi-Yan Yan,1 Tie Li,2 Yong Fu,3 Zhong-Yu Zhou,4 Chang-Chun Ji,5 Hui Hu,6 Long-Fei Han,7 Mi Liu,8 Shi-Fen Xu,9 Meng Li,10 Lan-Ying Liu,11 Feng Chen,12 Cun-Zhi Liu1
1International Acupuncture and Moxibustion Innovation Institute, School of Acupuncture-Moxibustion and Tuina, Beijing University of Chinese Medicine, Beijing, 100029, People’s Republic of China; 2The Third Affiliated Hospital of Changchun University of Chinese Medicine, Changchun, People’s Republic of China; 3The Affiliated Hospital of Jiangxi University of Chinese Medicine, Jiangxi, People’s Republic of China; 4Hubei Province Hospital of Traditional Chinese Medicine, Hubei, People’s Republic of China; 5Shaanxi Province Hospital of Traditional Chinese Medicine, Shaanxi, People’s Republic of China; 6Dongfang Hospital Affiliated to Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 7Shandong University Qilu Hospital High-Tech Zone Hospital, Shandong, People’s Republic of China; 8The First Hospital of Hunan University of Chinese Medicine, Hunan, People’s Republic of China; 9Shanghai Municipal Hospital of Traditional Chinese Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China; 10The Second Affiliated Hospital of Anhui University of Chinese Medicine, Anhui, People’s Republic of China; 11Jiangsu Province Hospital of Chinese Medicine, Jiangsu, People’s Republic of China; 12Wangjing Hospital of China Academy of Chinese Medical Sciences, Beijing, People’s Republic of China
Correspondence: Cun-Zhi Liu, School of Acupuncture and Moxibustion, Beijing University of Chinese Medicine, 11 Bei San Huan Dong Lu, Chaoyang District, Beijing, 100029, People’s Republic of China, Tel +861053912201, Fax +861053912201, Email [email protected]
Objective: This study aimed to investigate the prevalence of depression/anxiety/sleep disturbance (D/A/S), as well as factors associated with these conditions, among patients with moderate-to-severe chronic pain.
Methods: This cross-sectional study was conducted at 13 tertiary hospitals in 10 provinces, enrolling consecutive patients with chronic pain from November 2023 to May 2024. Depression was defined using the Patient Health Questionnaire-9 cutoff of 5 or higher, categories of depression were defined as none (scores: 0– 4); anxiety was defined using the Generalized Anxiety Disorder-7 cutoff of 5 or higher, categories of anxiety were defined as none (scores: 0– 4); sleep disturbance was defined as a total Pittsburgh Sleep Quality Index score of > 5, categories of sleep disturbance were defined as none (scores: 0– 5). Sociodemographic, lifestyle behaviors, and clinical characteristics were collected. Pearson correlation analysis was used to examine correlations among D/A/S. Univariate and multivariate logistic regression analyses were applied to identify factors associated with these conditions.
Results: A total of 1107 patients were analyzed. D/A/S were identified in 36.6%, 19.1%, and 46.3% of the patients with chronic pain, respectively. The co-occurrence of two or three symptoms was 12.8– 26.6%. In the multivariate analysis, patients who reported poor self-rated health (odds ratio [OR] 1.89, 95% confidence interval [CI] 1.33– 2.68) and neuroticism (OR 1.06, 95% CI 1.02– 1.09) were associated with depression. Neck pain (OR 2.60, 95% CI 1.53– 4.42), alcohol consumption (OR 1.83, 95% CI 1.12– 2.99), neuroticism (OR 1.09, 95% CI 1.05– 1.13), and pain interference (OR 1.33, 95% CI 1.17– 1.50) were correlated with anxiety. Alcohol consumption (OR 1.64, 95% CI 1.16– 2.32) and pain interference (OR 1.12, 95% CI 1.03– 1.23) were associated with sleep disturbance.
Conclusion: Among patients with chronic pain, D/A/S are prevalent and linked to distinct factors. Alcohol consumption and pain interference may be associated with both anxiety and sleep disturbance, while neuroticism may be linked to both depression and anxiety. Future systematic management of multifactorial factors may improve their mental health.
Keywords: depression, anxiety, sleep disturbance, human personality, self-rated health, chronic pain
Introduction
Chronic pain is one of the most prevalent chronic conditions globally and can affect all populations.1,2 A systematic review estimated that its prevalence varies from 24% to 60% across different countries.3 Persistent chronic pain increases the risk of a range of mental health problems.4 Depression/anxiety/sleep disturbance (D/A/S) often co-occur in individuals with chronic pain.5,6 These conditions are comorbid and share biological connections, including links to central nervous system sensitization,7 and regions in the brain, such as the prefrontal cortex, anterior cingulate, and thalamus, are associated with both pain and mental health modulations.8 Chronic pain, along with D/A/S, is a risk factor for opioid misuse and dependence, loneliness, and suicide.9,10
According to estimates from the Global Burden of Disease Study 2017, musculoskeletal problems and mental health problems were the two leading causes of years lived with disability (YLDs) in China.11 Co-occurring symptoms may exert a mutually reinforcing effect,12 and resolving depression, anxiety, or sleep disturbance may also alleviate pain.13,14 Pain and depression may influence each other.15 Similarly, anxiety is common in patients with pain, and often enhances the suffering associated with pain.16 Sleep disturbance has been shown to increase pain perception, negatively affect long-term prognosis, and thus act as a significant contributor to pain severity.17
More importantly, compared with chronic pain alone, co-occurrence of these symptoms is associated with impaired function, reduced treatment engagement, and poorer treatment response.18 Pain itself can induce D/A/S.16,19,20 Additionally, several studies have reported more intense pain is linked to greater severity of D/A/S;21,22 other factors may also modulate these symptoms in patients with pain.
Personality characteristics, which have been widely studied in chronic pain and influence the likelihood of persistent pain,23,24 may be linked to D/A/S.25,26 Of the big five personality traits, neuroticism is linked to mental illnesses.27 Neuroticism, indicating susceptibility to psychological distress, characterized by low emotional stability and high susceptibility to negative emotions.28 However, research on personality characteristics among patients with pain who have comorbid D/A/S remains scarce. Self-rated health is an internationally recognized subjective health measurement tool.29 It enables individuals to conduct a comprehensive assessment of their overall health status based on their own physical and psychological experiences.30 Self-rated health may help detect potential depression symptoms,31 and depression symptoms are one of the strongest predictors of poor self-rated health.32 Yet, whether self-rated health is associated with D/A/S in patients with chronic pain remains unclear.
Some studies have reported that pain-related functional interference is strongly associated with mental disorders. However, the relationship between pain interference and depression, anxiety, or sleep disturbance in patients with chronic pain has rarely been investigated. Decreased pain pressure threshold (PPT) is common in chronic pain,33 and mental disorders may increase pain sensitivity.34 Nevertheless, research on PPT differences between patients with pain who have depression, anxiety, or sleep disturbance and those who do not is lacking. Some overlap among D/A/S has been observed, primarily with associations involving female sex, lower education level, smoking, alcohol consumption, lower physical activity, and different pain locations.35–37 However, their specific relationships with respect to D/A/S in patients with chronic pain remain unclear.
D/A/S in patients with chronic pain are likely to result from a combination of multiple factors; however, studies comprehensively analyzing these factors remain scarce. Therefore, this multicenter cross-section study aimed to assess which muti-factors are associated with D/A/S in patients with moderate-to-severe chronic pain.
Methods
Study Design and Participants
This multicenter cross-sectional study was conducted from November 2023 to May 2024. Participants were recruited from 13 tertiary hospitals across 10 provinces and municipalities-including Beijing, Hubei, Hunan, Jiangsu, Shanghai, Jilin, Shaanxi, Jiangxi, Anhui, and Shandong- covering the eastern, southern, central, western, and northern regions of China. Eligible patients were aged 18 years or older, had moderate-to-severe chronic musculoskeletal pain (neck pain, low back pain, and knee pain), and were able to speak and read Chinese. Participants were excluded if they had undergone chronic pain-related surgery within the past year. Before participation, all patients provided written informed consent. This study was approved by the Medical Ethical Committee of Beijing University of Chinese Medicine (2023BZYLL0501) and ethics committees of all participating hospitals (Supplementary Table 12). This study was registered with Chinese Clinical Trials.gov (ChiCTR2300076619). The study was conducted in accordance with the Declaration of Helsinki and reported according to the “Strengthening the Reporting of Observational Studies in Epidemiology” (STROBE) guideline.38
Procedures
Clinicians screened all consecutive outpatients with chronic pain in their clinics according to the International Association for the Study of Pain (IASP) classification of chronic pain for International Classification of Diseases (ICD-11). Patients were also asked to complete and enter their data via a touch-screen computer in the waiting area during their first consultation with the clinician, using the Research Electronic Data Capture (REDCap) system as an online questionnaires tool.
The groups were compared for demographics, pain-related characteristics (intensity, interference, location, and PPT), self-rated health, psychological factors (D/A/S, and personality). To further investigate the role of these variables in relation to D/A/S in the whole study.
Measures
The questionnaire was necessarily brief to minimize its impact on clinicians’ and patients’ time (Supplementary Table 1). Chronic pain diagnoses were made, assessed, and recorded by clinicians after examining patients. Participants who had been experiencing continuous or intermittent pain for 3 months or more were classified as having chronic pain.39
Demographics were collected from the pre-appointment questionnaire, as well as lifestyle behaviors, such as smoking status, alcohol intake, sick leave due to pain, and physical activity level. The assessment of self-rated health was derived from a previous study.40 Participants were asked: “In general, would you say your health is: excellent, very good, good, fair or poor?” Self-rated health was treated as a dichotomous indicator (poor health: “fair” or “poor”; good health: “excellent” or “very good” or “good”).41 Self-rated health is a measure that reflects an individual’s integrated perception of their health.30
Pain intensity was assessed using a Numerical Rating Scale (NRS) (range, 0[no pain]-10[worst pain imaginable]).42 The NRS is a validated, well-established measure and is responsive to changes in pain.43 Pain-related functional interference was assessed using the Pain Interference subscale of the Brief Pain Inventory (BPI) (range, 0–10 outcomes).44 This subscale evaluates how pain interferes with daily functioning, with higher scores indicating greater impairment.45
Depression symptoms were assessed using the Patient Health Questionnaire-9 (PHQ-9) (score range, 0–27).46 The PHQ-9 is a standard outpatient tool for screening and detecting the severity of depression.47 Participants with a score at least 5 points were assigned to the “depression group” (referencing established criteria in relevant study),47,48 and those reporting less than 5 points to the “non-depression group”. Anxiety symptoms were assessed using the Generalized Anxiety Disorder-7 (GAD-7) scale (score range, 0–21), which includes seven items evaluating generalized anxiety symptoms over the 14 days prior to assessment.5 Participants with a score of at least 5 points assigned to the “anxiety group”;48,49 those with a score less than 5 points to the “non-anxiety group”. Sleep disturbance was screened using the Pittsburgh Sleep Quality Index (PSQI), a patient-rated scale with a score range of 0–21, with those reporting > 5 points assigned to the “sleep disturbance group”,50,51 and ≤ 5 points to the “normal sleep group”.
Personality was assessed using the Neuroticism Extraversion Openness Five-Factor Inventory (NEO-FFI, Costa & McCrae, available from www.parinc.com).52 The NEO-FFI is a 60-item scale based on the extensively validated empirically five-factor model of personality, including extraversion, openness, conscientiousness, agreeableness, and neuroticism.
Pressure pain threshold (PPT) was measured using a digital pressure algometer with a 1 cm2 tip (Wagner Force Ten™ FDX50, Wagner Instruments, Greenwich, CT, USA). For this measurement, PPT was assessed three times at the left lateral epicondyle of the humerus, the average value of these three measurements was used for analysis.53
Statistical Analysis
The study presented sociodemographic and clinical characteristics of patients with chronic pain in depression vs non-depression groups, anxiety vs non-anxiety groups, sleep disturbance vs normal sleep groups. The variables described using means are as follows: age, pain duration, pain intensity, PPT, pain interference, BMI, human personality, and scores for D/A/S. Continuous variables were compared using two-sample t-tests, and non-normally distributed continuous data were compared using the Mann–Whitney U-test. Categorical variables were compared using the chi-square test. To investigate the factors (ie independent variable) associated with depression (PHQ-9 scores ≥ 5), anxiety (GAD-7 scores ≥ 5), and sleep disturbance (PSQI scores > 5) in patients with chronic pain, all variables were selected based on literature evidence and the suggestions from clinical experts, including individual’s age, sex, BMI, education level, exercise, smoking status, alcohol consumption, self-rated health, pain location, pain duration, PPT, pain intensity, pain interference, pain medicine use, sick leave due to pain, personality, anxiety, depression, and sleep quality (Supplementary Table 2), were entered into univariable logistic regression models. The univariable association between D/A/S and each factor was examined. Those variables associated at P value < 0.20 in the univariate analysis were candidates for inclusion in multiple logistic regression models.54,55
Furthermore, three secondary models were established in this study (Supplementary Table 3). The secondary model 1 (depression) is a predictive model for analyzing the influencing factors of depression, with the predictor set excluding anxiety or sleep disturbance. The secondary model 2 (anxiety) is a predictive model for analyzing the influencing factors of anxiety, with the predictor set excluding depression or sleep disturbance. The secondary model 3 (sleep disturbance) is a predictive model for analyzing the influencing factors of sleep disturbance, with the predictor set excluding anxiety or depression. These models estimated the odds ratios (ORs) and 95% confidence intervals (CIs) for the effect of each variable on each outcome.
Variance Inflation Factor (VIF) was used for collinearity diagnostics, with a criterion of VIF ≥ 5 indicating potential collinearity (Supplementary Table 4). Confirmatory analyses included the following variables: sex, education, pain duration, pain intensity, alcohol consumption, pain interference, self-rated health, neuroticism, and extraversion. Exploratory analyses, focused on age, BMI, sick leave due to pain, pain medicine use, agreeableness, conscientiousness, and openness. The correlations of D/A/S were examined by Pearson’s correlation analysis.
It has been suggested that the number of events per predictor variable (EPV) exceeds 10 in multivariate logistic regression analyses to ensure model adequacy.56 In our study, considering the number of events (405 with depression; 211 with anxiety; 503 with sleep disturbance), we included the 17 variables as described in the model. In addition, sensitivity analysis was performed in this study for the cut-off criteria of ≥ 10 (for depression, based on PHQ-9) and ≥ 10 (for anxiety, based on GAD-7) (Supplementary Table 5). Multiple imputation was used to handle missing data. Unless otherwise stated, the significance level was set at 0.05. All analyses were performed using R software (version 4.2.0).
Results
Patient Characteristics
A total of 1107 patients with chronic pain aged 18 to 85 years (mean ± SD: 41.4 ± 14.6 years) were included, with 700 (63.2%) being women (Table 1). Among them, 612 (55.3%) had a bachelor’s degree, 96 (8.7%) reported smoking, and 307 (27.7%) reported alcohol consumption. Additionally, 653 (59%) self-rated their health as “poor”, 273 (24.7%) had sick leave due to pain; and 496 (44.6%) engaged in ≥ 30 minutes of exercise three times weekly. Neck pain was the most common primary complaint (55.3%, 612), followed by low back pain (52.6%, 582) and knee pain (11.6%, 128). The mean pain duration was 4.03 years, and mean PPT was 26.8 Newtons (N). The sample had a mean NRS score of 6.0 and BPI interference score of 3.1. Regarding psychological measures, the mean PHQ-9 score was 4.3, GAD-7 score was 3.1, and PSQI score was 5.7 (Supplementary Table 6).
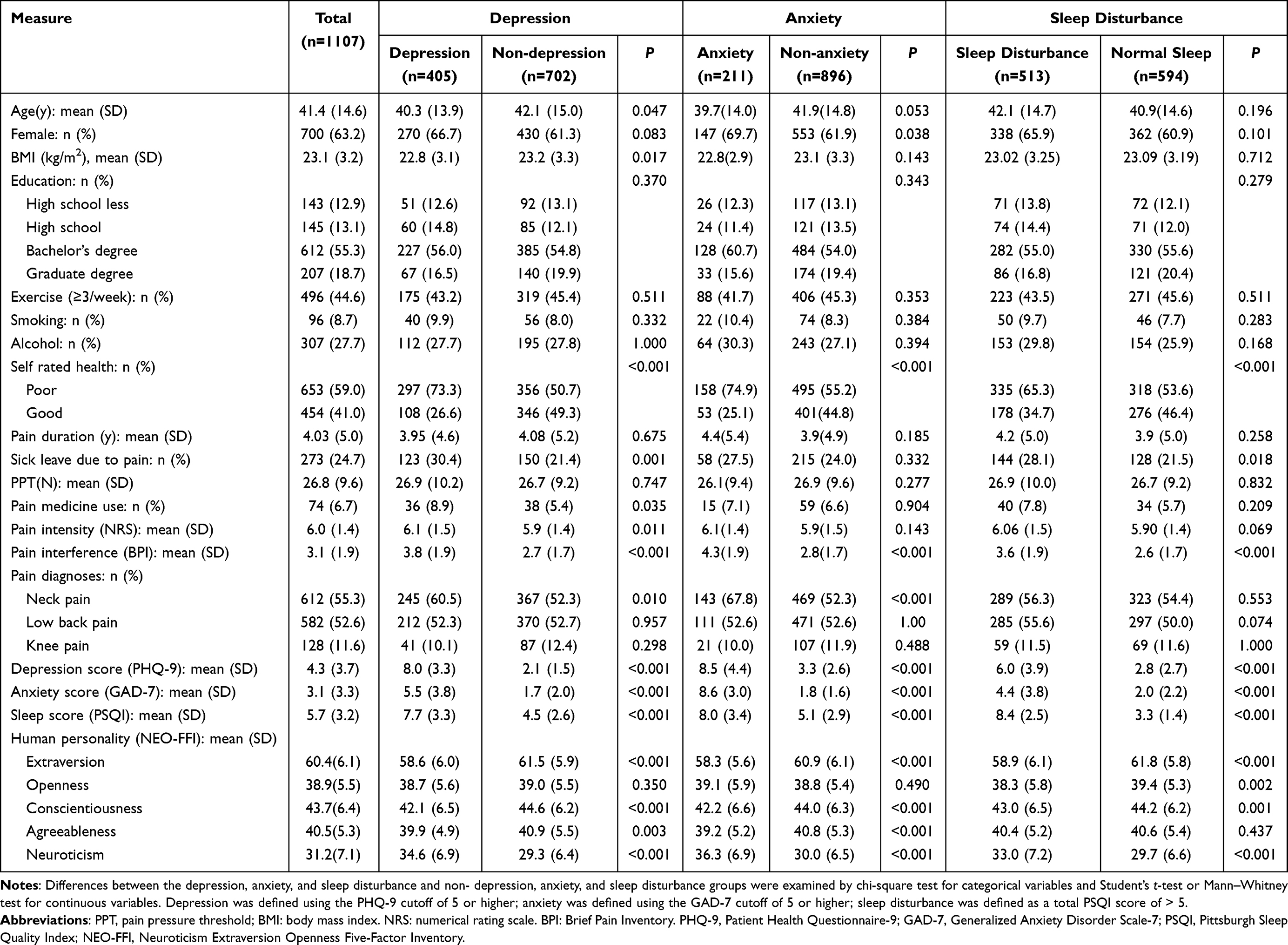 |
Table 1 Characteristics and Self-Reported Outcomes of Patients with Chronic Pain |
Comparison of Demographic and Clinical Characteristics Between Different Groups
There was difference in mean age (40.3 vs 42.1 years) and BMI (22.8 vs 23.2 kg/m2) between depressed and non-depressed patients. The anxiety group had a higher proportion of females than the non-anxiety group (69.7% vs 61.9%) (Table 1). Patients with depression or anxiety more frequently self-rated their health as “poor” (73.3% vs 50.7% and 74.9% vs 55.2%, respectively) and were more likely to have neck pain (60.5% vs 52.3% and 67.8% vs 52.3%, respectively) compared with non-depressed/non-anxiety. Sick leave due to pain was more common in patients with depression (30.4% vs 21.4%) or sleep disturbance (28.1% vs 21.5%) than in those without.
Patients with depression, anxiety, or sleep disturbance had 1.1, 1.5, and 1.0 points higher mean BPI scores, respectively, than non-depression, non-anxiety, or sleep normal groups (Table 1). Patients in depression group also had a 0.2 point higher mean NRS score and more frequent pain medication use (8.9% vs 5.4%) than patients in non-depression group. Additionally, patients with depression had 3.8 points higher mean GAD-7 scores and 3.2 points higher mean PSQI scores than patients without depression; anxiety patients had 5.2 points higher mean PHQ-9 scores and 2.9 points higher mean PSQI scores than non-anxiety patients; and patients with sleep disturbance had 3.2 points higher mean PHQ-9 scores and 2.4 points higher mean GAD-7 scores than those without.
In terms of personality: patients with depression had 5.3points higher neuroticism, 2.9 points lower extraversion, 2.5 points lower conscientiousness, and 1.0 points lower agreeableness than non-depression patients. Anxiety patients had 6.3 points higher neuroticism, 2.6 points lower extraversion, 1.8 points lower conscientiousness, and 1.6 points lower agreeableness than non-anxiety patients. Patients with sleep disturbance had 3.3 points higher neuroticism, 2.9 points lower extraversion, 1.2 points lower conscientiousness, and 1.1 points lower openness than those without sleep disturbance.
Prevalence of D/A/S in Patients with Chronic Pain
Based on the PHQ-9, GAD-7, and PSQI, 405 patients with chronic pain (36.6% of 1107) met the criteria for depression, 211 (19.1%) for anxiety, and 513 (46.3%) for sleep disturbance (Figure 1). Among comorbidities of two symptoms, comorbid depression and sleep disturbance had the highest prevalence (294, 26.6%), followed by comorbid depression and anxiety 175 cases (15.8%), and comorbid anxiety and sleep disturbance 163 (14.7%). The prevalence of all three comorbid symptoms (D/A/S) was 142 (12.8%).
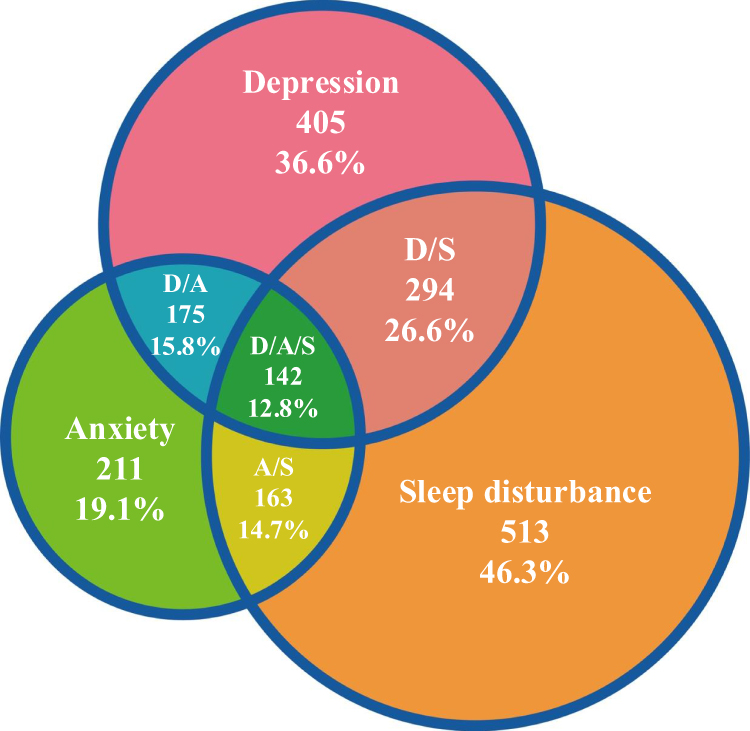 |
Figure 1 Prevalence of D/A/S in patients with chronic pain. Visualizing prevalence of D/A/S, co-occurrence of two symptoms (depression and anxiety, depression and sleep disturbance, anxiety and sleep disturbance), and co-occurrence of three symptoms (D/A/S) in patients with chronic pain in our study. Depression was defined using the PHQ-9 cutoff of 5 or higher; anxiety was defined using the GAD-7 cutoff of 5 or higher; sleep disturbance was defined as a total PSQI score of > 5. Abbreviations: D/A, depression/anxiety; D/S, depression/sleep disturbance; A/S, anxiety/sleep disturbance; D/A/S, depression/anxiety/sleep disturbance. |
Correlations Between D/A/S in Patients with Chronic Pain
Pearson’s correlations between D/A/S are shown in Figure 2. PHQ-9 scores were approximate moderately correlated with GAD-7 scores (Pearson’s correlation coefficient, r = 0.71, 95% CI 0.68–0.73, P < 0.001) and moderately positively correlated with PSQI scores (r = 0.55, 95% CI 0.51–0.59 P < 0.001). GAD-7 scores were moderately positively correlated with PSQI scores (r = 0.47, 95% CI 0.42–0.52, P < 0.001).
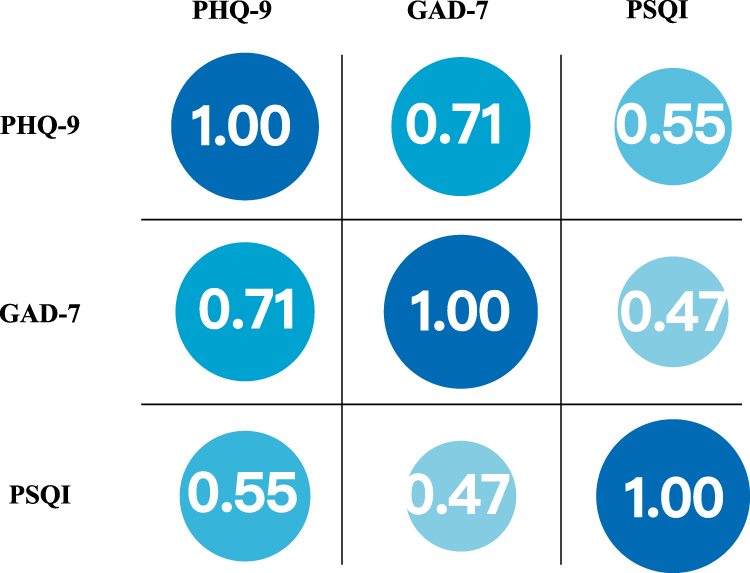 |
Figure 2 Correlations between D/A/S in pain patients. Depression defined using the PHQ-9 cutoff of 5 or higher. Anxiety defined using the GAD-7 cutoff of 5 or higher. Sleep disturbances defined using the PSQI cutoff of 5 or higher. Correlation values < 0.20 were considered as very weak, 0.20 to 0.39 as weak, 0.40 to 0.59 as moderate, and 0.6 and above as strong. Abbreviations: PHQ-9, Patient Health Questionnaire-9; GAD-7, Generalized Anxiety Disorder Scale-7; PSQI, Pittsburgh Sleep Quality Index. |
Different Factors Associated with D/A/S
In the univariable logistic model, variables with a P < 0.20 associated with depression, anxiety, or sleep disturbance included age, sex, BMI, education, pain duration, alcohol consumption, NRS, BPI, self-rated health, sick leave due to pain, PHQ-9, GAD-7, PSQI, personality, neck pain and low back pain. Univariable logistic regression results for all variables are described in Supplementary Table 6. In the multivariable logistic model, poor self-rated health (OR 1.89, 95% CI 1.33–2.68, P < 0.001), lower conscientiousness (OR 0.96, 95% CI 0.93–1.00, P < 0.05) and higher neuroticism (OR 1.06, 95% CI 1.02–1.09, P < 0.001) were associated with depression (Table 2). For anxiety, associated factors included neck pain (OR 2.60, 95% CI 1.53–4.42, P < 0.01), alcohol (OR 1.83, 95% CI 1.12–2.99, P < 0.05), neuroticism (OR 1.09, 95% CI 1.05–1.13, P < 0.001), and pain interference (OR 1.33, 95% CI 1.17–1.50, P < 0.001).Sleep disturbance were associated with alcohol (OR 1.64, 95% CI 1.16–2.32, P < 0.01), pain interference (OR 1.12, 95% CI 1.03–1.23, P < 0.05), and extraversion (OR 0.95, 95% CI 0.93–0.98, P < 0.001) (Figure 3).
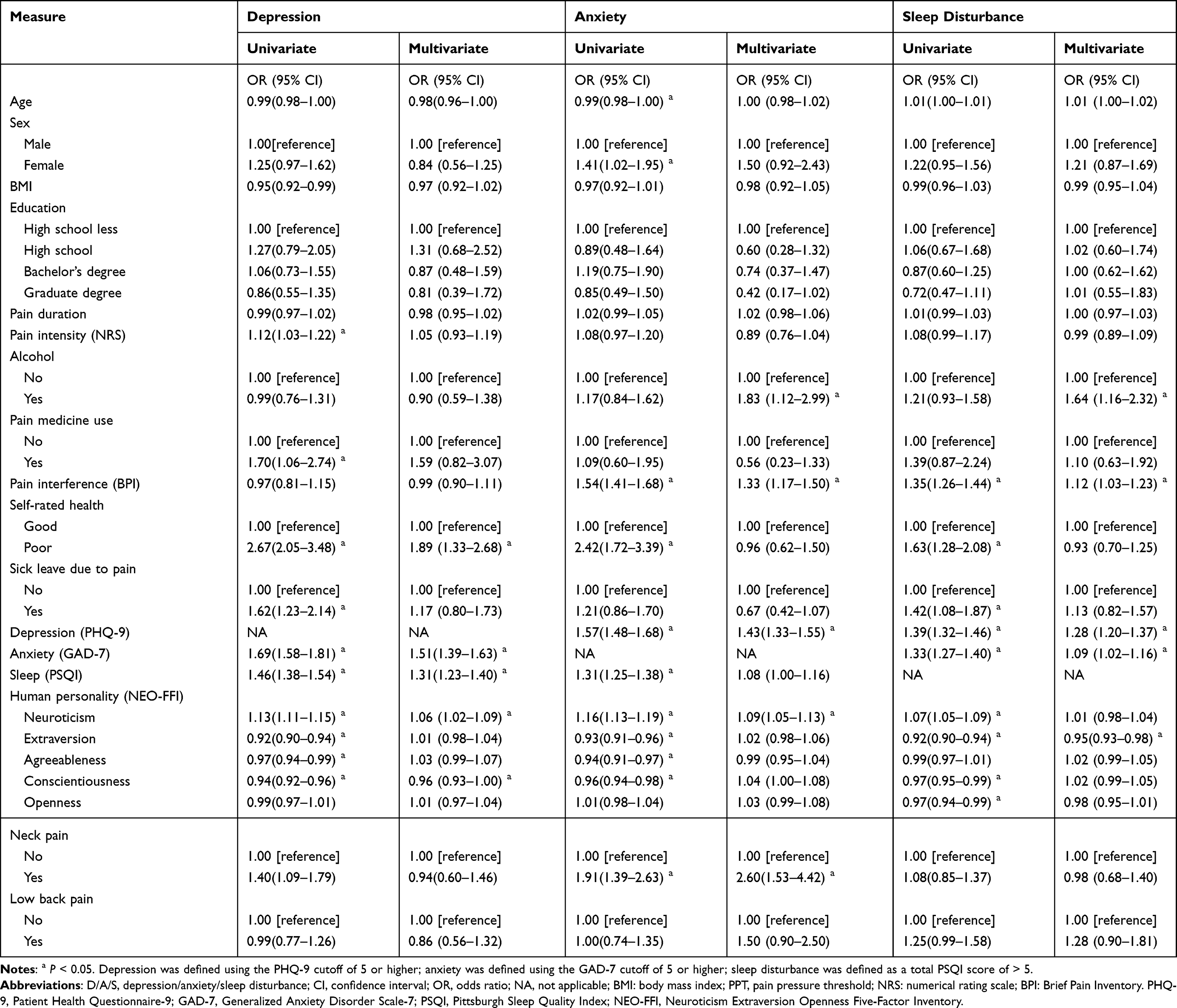 |
Table 2 Logistic Regression Analysis to Identify Factors Associated with D/A/S in Pain Patients |
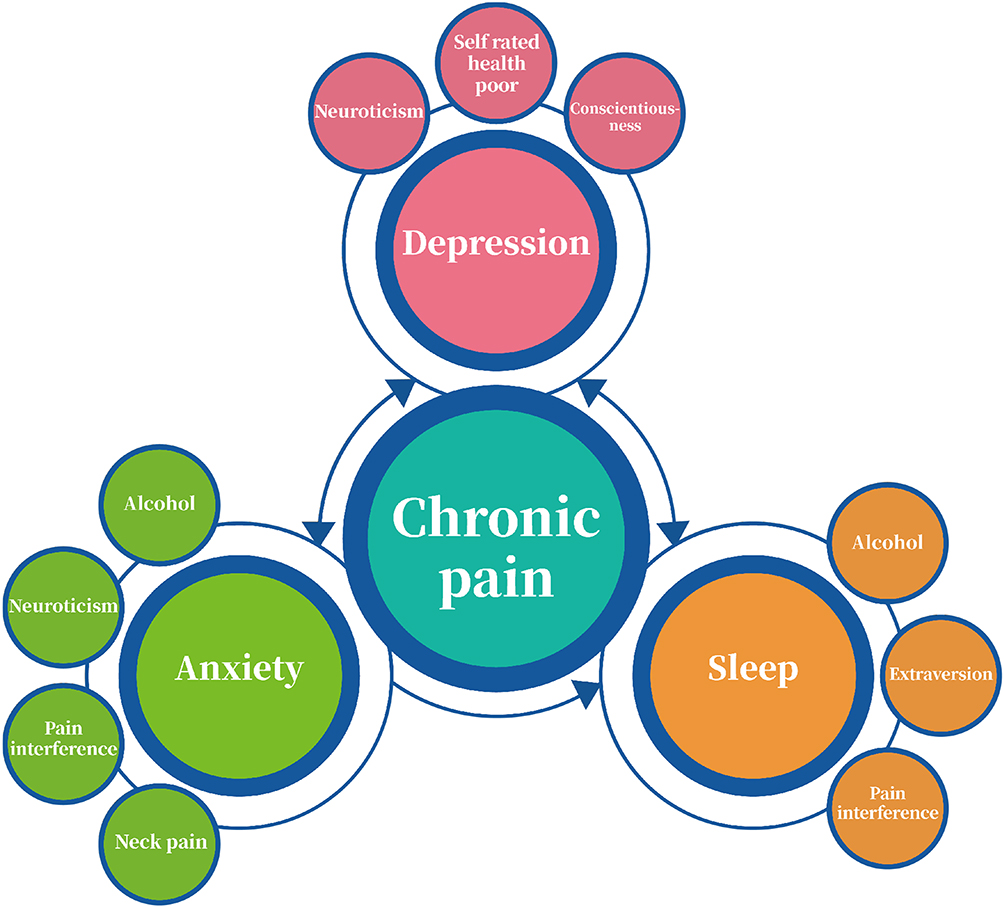 |
Figure 3 A proposed circle of factors in comorbid chronic pain and depression, anxiety, and sleep disturbance. Chronic pain and depression, anxiety, and sleep disturbance were comorbid. In multi-variable logistic regression model, depression and anxiety had associations; sleep disturbance and depression had associations; anxiety is factor for sleep disturbance. Multi-factors may serve as treatment targets. Depression was defined using the PHQ-9 cutoff of 5 or higher; anxiety was defined using the GAD-7 cutoff of 5 or higher; sleep disturbance was defined as a total PSQI score of > 5. |
Discussion
In this muti-center study, the estimated prevalence of one symptom of D/A/S in patients with moderate-to-severe chronic pain occurred in approximately 36.6%, 19.1% and 46.3%, respectively. Meanwhile, the co-occurrence of two or three symptoms ranged from 12.8% to 26.6%. Notably, we found that D/A/S were associated with different factors, though personality (neuroticism) was associated with both depression and anxiety; alcohol and pain interference were associated with both anxiety and sleep disturbance.
Similar to a recent epidemiological study, the prevalence of depression in the patients with chronic pain was 30.2%.6 However, a previous study reported a higher prevalence of probable depression (60.8%) among patients with chronic pain.57 This discrepancy in prevalence may be explained by differences in study populations: the latter study included patients with chronic disabling pain who were unresponsive to medical treatment, and variations in study settings may also have contributed. We also chose to use the IASP definition of chronic pain and PHQ-9 definition of depression, which were consistent with those employed in the two studies.6,57 In this study, 19.1% met criteria for anxiety, which is consistent with a previous finding that the prevalence of generalized anxiety disorder among patients with chronic pain was 18.9%;58 this is also similar to results from a prior study on anxiety and chronic pain in China.59
In this study, sleep disturbance comorbid with chronic pain was prevalent, at 46.3%. This result was consistent with previous studies,60,61 sleep disturbance is a common comorbidity of chronic pain. A systematic review supports the hypothesis that sleep, and pain have a bidirectional and reciprocal relationship.62 Moreover, a previous study supported that sleep disturbance, chronic pain mutually interacts, each increasing the risk of the emergence.63
Several noteworthy findings indicate that patients with D/A/S are not identical. First, the prevalence of depression, anxiety, sleep disturbance, and their comorbid symptoms differed this includes two-symptom combinations (depression with anxiety, depression with sleep disturbance, anxiety with sleep disturbance) and three-symptom comorbidity (D/A/S) in patients with chronic pain. Second, the factors associated with D/A/S were not the same. We identified factors specific to each: poor self-rated health and conscientiousness for depression; neck pain for anxiety; and extraversion for sleep disturbance. Third, we found sleep disturbance was not significantly associated with GAD-7 scores in patients with chronic pain. These differences may explain the distinct profiles of patients with D/A/S observed in our study.
In the present study, neck pain was a factor for anxiety, which was congruent with the findings of a previous pain study.64 However, other studies reported that neck or neck-shoulder pain was associated with depression.65,66 We have considered two reasons for this finding. First, depression was strongly positively correlated with anxiety in our study, and PHQ-9 scores were associated with anxiety. Second, most patients with anxiety had comorbid depression: the prevalence of anxiety was 19.1%, and the comorbidity of depression and anxiety was 15.8%.
Pain interference is another important assessment for pain and mental health problems. In this study, pain interference emerged as a factor for anxiety and sleep disturbance, which were consistent with the findings that pain interference was associated anxiety and sleep disturbance.67,68 However, this was not completely in accordance with previous findings that pain interference is a predictor of depression.69 We speculate that this discrepancy may relate to differences in self-report measures: the prior study used the PROMIS Depression scale, which are normalized to a representative sample of the general US population.69 Moreover, most of patients with anxiety had comorbidity depression; thus, the association between pain interference and comorbid depression-anxiety observed here might be acceptable Additionally, alcohol was a factor for depression and sleep disturbance; this was consistent with the previous findings of pain-related anxiety being positively associated with alcohol70 and was similar to another study demonstrating that alcohol disrupts normal sleep architecture.71
A previous study found that neuroticism was considered a risk factor, while conscientiousness and extraversion were protective factors in depression and anxiety.72 Another study indicated that neuroticism seemed to be the most important personality factor associated with more severe anxiety symptoms.73 Our findings were consistent with these studies. Yet, extraversion was a protective factor for sleep disturbance in patients with chronic pain, which was not consistent with a previous study.74 The findings of the current study demonstrated that personality characteristics were an important factor in co-occurrence of chronic pain and D/A/S.
Interestingly, it is likely that many factors may be associated with D/A/S. Figure 3 describes chronic pain, D/A/S and other factors. There may be small improvements in D/A/S when treatment is pain specific. A previous study investigated whether pain-specific and depression-specific acupoints had specific efficacy in patients with comorbid chronic pain and depression.39 Pain-specific acupoints were hypothesized to reduce pain more effectively than depression-specific acupoints; yet the study found no significant difference in pain reduction between the two. Clinicians managing patients with chronic pain may often focus on pain-relieving interventions, with the assessment and treatment of comorbidities being secondary or unaddressed. Paying attention to factors (eg neuroticism, self-rated health, pain interference, and neck pain) may help clinicians early in patients with chronic pain and could prove more effective.
To our knowledge, this is the first nationally representative study to investigate the co-occurrence of chronic pain with D/A/S, and to comprehensively analyze their associated factors among patients with moderate-to-severe chronic pain in China. Including patients with mixed chronic pain reduces the likelihood that findings are limited to a specific pain type. This study assessed a range of variables, including diverse pain assessments (PPT, location, intensity, and interference), multi-dimensional psychological evaluations (D/A/S and personality), and lifestyle behaviors (smoking, alcohol consumption, and exercise), if available, may lead to a conclusion about associated factors and impacts.
Several limitations of this study warrant consideration. First, there is potential for misclassifying symptoms. Although the PHQ-9, GAD-7, and PSQI (self-report screening tools) demonstrate acceptable sensitivity and specificity, they lack the diagnostic validity afforded by clinical evaluation. Second, the study population was recruited from pain clinics, which may limit the generalizability of the findings to the broader chronic pain population. However, the sample was geographically diverse, covering most regions of China, which enhances the representativeness of our findings. Third, the cross-sectional design only identifies associations (not causality), and longitudinal studies are needed to clarify the directionality and causality of these associations. Fourth, while multicollinearity was absent among the variables in the statistical models used (verified via the VIF test), unmeasured confounders could not be fully controlled, which may introduce biases into the results. Fifth, alcohol and smoking were defined as binary variables without collecting precise dose information. Thus, the study compared smoking and alcohol consumption status rather than examining dose-response associations with outcome. Last, model specification issues may compromise the interpretability of the results.
Conclusions
Among patients with chronic pain, D/A/S are highly prevalent and associated with distinct factors. Notably, alcohol consumption and pain interference may be associated with both anxiety and sleep disturbance, while neuroticism may be linked to both depression and anxiety. The identified factors may relate to these mental disorders are noteworthy. Future studies on the systematic management of multifactorial factors may facilitate improvements in the mental health of patients with chronic pain.
Data Sharing Statement
Both the deidentified participant data and program codes used in analysis are available upon reasonable request until 2 years after publication, via the corresponding author [e-mail, [email protected]]. The data can be made available to researchers who provide a methodologically sound proposal in their request. We confirm that the material of this paper has never been published before, are not under consideration for publication elsewhere and have been approved by each author.
Acknowledgments
The authors thank the physicians of the participating pain clinics and are grateful to the participants for contributing to this research.
Funding
The study was supported by the Fundamental Research Funds for the Central Universities (No.2022-JYB-JBZR-035; No.2023-JYB-KYPT-11).The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Murray CJ, Lopez AD. Measuring the global burden of disease. New Engl J Med. 2013;369(5):448–457. doi:10.1056/NEJMra1201534
2. Shi MT, Liu YK, Liang Y, et al. Electroacupuncture participates in pain transition through regulating the KCC2/GABAAR pathway in the spinal dorsal horn of rats. Acupunct Herbal Med. 2025;5(2):217–228. doi:10.1097/HM9.0000000000000000
3. Andrews P, Steultjens M, Riskowski J. Chronic widespread pain prevalence in the general population: a systematic review. Eur J Pain. 2018;22(1):5–18. doi:10.1097/j.pain.0000000000000314
4. Fassberg MM, Cheung G, Canetto SS, et al. A systematic review of physical illness, functional disability, and suicidal behaviour among older adults. Aging Mental Health. 2016;20(2):166–194. doi:10.1186/s12913-016-1423-5
5. McIntosh AM, Hall LS, Zeng Y, et al. Genetic and environmental risk for chronic pain and the contribution of risk variants for major depressive disorder: a family-based mixed-model analysis. PLoS Med. 2016;13(8):e1002090. doi:10.1371/journal.pmed.1002090
6. Rayner L, Hotopf M, Petkova H, Matcham F, Simpson A, McCracken LM. Depression in patients with chronic pain attending a specialised pain treatment centre: prevalence and impact on health care costs. Pain. 2016;157(7):1472–1479. doi:10.1097/j.pain.0000000000000542
7. Satyanarayanan SK, Shih YH, Wen YR, et al. miR-200a-3p modulates gene expression in comorbid pain and depression: molecular implication for central sensitization. Brain Behav Immun. 2019;82:230–238. doi:10.1016/j.bbi.2019.08.190
8. Meerwijk EL, Ford JM, Weiss SJ. Brain regions associated with psychological pain: implications for a neural network and its relationship to physical pain. Brain Imaging Behav. 2013;7(1):1–14. doi:10.1007/s11682-012-9179-y
9. Smit T, Rogers AH, Garey L, Allan NP, Viana AG, Zvolensky MJ. Anxiety sensitivity and pain intensity independently predict opioid misuse and dependence in chronic pain patients. Psychiatry Res. 2020;294:113523. doi:10.1016/j.psychres.2020.113523
10. Smith TO, Dainty JR, Williamson E, Martin KR. Association between musculoskeletal pain with social isolation and loneliness: analysis of the English Longitudinal Study of Ageing. Br J Pain. 2019;13(2):82–90. doi:10.1177/2049463718802868
11. Zhou M, Wang H, Zeng X, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2020;396(10243):26. doi:10.1016/S0140-6736(20)31450-1
12. Alvaro PK, Roberts RM, Harris JK. A systematic review assessing bidirectionality between sleep disturbances, anxiety, and depression. Sleep. 2013;36(7):1059–1068. doi:10.5665/sleep.2810
13. Chou KL, Chi I. Reciprocal relationship between pain and depression in elderly Chinese primary care patients. Int J Geriatr Psychiatry. 2005;20(10):945–952. doi:10.1002/gps.1383
14. Lee MT, Peng WH, Wu CC, et al. Impaired ventrolateral periaqueductal gray-ventral tegmental area pathway contributes to chronic pain-induced depression-like behavior in mice. Mol Neurobiol. 2023;60(10):5708–5724. doi:10.1007/s12035-023-03439-z
15. Han SB, Lee SH, Ha IH, Kim EJ. Association between severity of depressive symptoms and chronic knee pain in Korean adults aged over 50 years: a cross-sectional study using nationally representative data. BMJ Open. 2019;9(12):e032451. doi:10.1136/bmjopen-2019-032451
16. Shen Z, Zhang H, Wu Z, et al. Electroacupuncture alleviates chronic pain-induced anxiety disorders by regulating the rACC-thalamus circuitry. Front Neurosci. 2021;14:615395. doi:10.3389/fnins.2020.615395
17. Chang HA, Fang WH, Liu YP, et al. Sex-specific pathways among tri-allelic serotonin transporter polymorphism, trait neuroticism and generalized anxiety disorder. J Psychiatry Neurosci. 2020;45(6):379–386. doi:10.1503/jpn.190092
18. Ding X, Lin Y, Chen C, et al. DNMT1 mediates chronic pain-related depression by inhibiting GABAergic neuronal activation in the Central Amygdala. Biol Psychiatry. 2023;94(8):672–684. doi:10.1016/j.biopsych.2023.03.015
19. Cleeland CS, Ryan KM. Pain assessment: global use of the brief pain inventory. Ann Acad Med Singapore. 1994;23(2):129–138.
20. Davies KA, Macfarlane GJ, Nicholl BI, et al. Restorative sleep predicts the resolution of chronic widespread pain: results from the EPIFUND study. Rheumatology. 2008;47(12):1809–1813. doi:10.1093/rheumatology/ken389
21. Stein MD, Herman DS, Bailey GL, et al. Chronic pain and depression among primary care patients treated with buprenorphine. J Gen Intern Med. 2015;30(7):935–941. doi:10.1007/s11606-015-3212-y
22. Zhuo M. Neural mechanisms underlying anxiety-chronic pain interactions. Trends Neurosci. 2016;39(3):136–145. doi:10.1016/j.tins.2016.01.006
23. Seto A, Han X, Price LL, Harvey WF, Bannuru RR, Wang C. The role of personality in patients with fibromyalgia. Clin Rheumato. 2019;38(1):149–157. doi:10.1007/s10067-018-4316-7
24. Elgaeva EE, Williams FMK, Zaytseva OO, et al. Bidirectional Mendelian randomization study of personality traits reveals a positive feedback loop between neuroticism and back pain. J Pain. 2023;24(10):1875–1885. doi:10.1016/j.jpain.2023.05.012
25. Hovens JG, Giltay EJ, van Hemert AM, Penninx BW. Childhood maltreatment and the course of depressive and anxiety disorders: the contribution of personality characteristics. Depress Anxiety. 2016;33(1):27–34. doi:10.1002/da.22429
26. Wang Z, Zeng Z. Association between personality characteristics and sleep quality among Chinese middle-aged and older adults: evidence from China family panel studies. BMC Public Health. 2023;23(1):2427. doi:10.1186/s12889-023-17352-6
27. Gupta P, Galimberti M, Liu Y, et al. A genome-wide investigation into the underlying genetic architecture of personality traits and overlap with psychopathology. Nat Hum Behav. 2024;8(11):2235–2249. doi:10.1038/s41562-024-01951-3
28. Huang S, Zhang Y, Ma L, et al. Neuroticism is associated with future disease and mortality risks. Chin Med J. 2025;138(11):1355–1366. doi:10.1097/CM9.0000000000003503
29. Fukui Y, Nagata T, Odagami K, Mori K; W2S-Ohpm study. The relationship between self-rated health and occupational accidents: a nationwide prospective cohort study. J Occup Health. 2025;67(1):uiaf054. doi:10.1093/joccuh/uiaf054
30. Mou Y, Tan Z, Nie H. Retirement and grandchild care in China: mental health consequences and policy implications. BMC Public Health. 2025;25(1):3389. doi:10.1186/s12889-025-24774-x
31. Rantanen AT, Korkeila JJA, Kautiainen H, Korhonen PE. Poor or fair self-rated health is associated with depressive symptoms and impaired perceived physical health: a cross-sectional study in a primary care population at risk for type 2 diabetes and cardiovascular disease. Eur J Gen Pract. 2019;25(3):143–148. doi:10.1080/13814788.2019.1635114
32. Todorova IL, Tucker KL, Jimenez MP, Lincoln AK, Arevalo S, Falcón LM. Determinants of self-rated health and the role of acculturation: implications for health inequalities. Ethn Health. 2013;18(6):563–585. doi:10.1080/13557858.2013.771147
33. Lalouni M, Fust J, Vadenmark-Lundqvist V, Ehrsson HH, Kilteni K, Birgitta Jensen K. Predicting pain: differential pain thresholds during self-induced, externally induced, and imagined self-induced pressure pain. Pain. 2021;162(5):1539–1544. doi:10.1097/j.pain.0000000000002151
34. Bagnato G, De Andres I, Sorbara S, et al. Pain threshold and intensity in rheumatic patients: correlations with the Hamilton depression rating scale. Clin Rheumato. 2015;34(3):555–561. doi:10.1007/s10067-013-2477-y
35. Sá KN, Baptista AF, Matos MA, Lessa Í. Chronic pain and gender in Salvador population. Brazil Pain. 2008;139(3):498–506.
36. Trouvin AP, Attal N, Perrot S. Lifestyle and chronic pain: double jeopardy? Br J Anaesth. 2022;129(3):278–281. doi:10.1016/j.bja.2022.06.006
37. Binnewies J, Nawijn L, van Tol MJ, van der Wee NJA, Veltman DJ, Penninx BWJH. Associations between depression, lifestyle and brain structure: a longitudinal MRI study. Neuroimage. 2021;231:117834. doi:10.1016/j.neuroimage.2021.117834
38. Vandenbroucke JP, von Elm E, Altman DG, et al. STROBE Initiative. Strengthening the reporting of observational studies in epidemiology (STROBE): explanation and elaboration. Int J Surg. 2014;12(12):1500–1524. doi:10.1016/j.ijsu.2014.07.014
39. Treede RD, Rief W, Barke A, et al. A classification of chronic pain for ICD-11. Pain. 2019;160(1):19–27. doi:10.1097/j.pain.0000000000001384
40. Eriksen J, Ekholm O, Sjøgren P, Rasmussen NK. Development of and recovery from long-term pain. A 6-year follow-up study of a cross-section of the adult Danish population. Pain. 2004;108(1–2):154–162. doi:10.1016/j.pain.2003.12.018
41. Moradi-Lakeh M, El Bcheraoui C, Tuffaha M, et al. Self-rated health among Saudi adults: findings from a national survey. J Community Health. 2015;40(5):920–926. doi:10.1007/s10900-015-0014-4
42. Farrar JT, Young JP, LaMoreaux L, Werth JL, Poole MR. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001;94(2):149–158. doi:10.1016/S0304-3959(01)00349-9
43. Euasobhon P, Atisook R, Bumrungchatudom K, Zinboonyahgoon N, Saisavoey N, Jensen MP. Reliability and responsivity of pain intensity scales in individuals with chronic pain. Pain. 2022;163(12):e1184–e1191. doi:10.1097/j.pain.0000000000002692
44. Bair MJ, Ang D, Wu J. Evaluation of stepped care for chronic pain (ESCAPE) in veterans of the iraq and afghanistan conflicts: a randomized clinical trial. JAMA Intern Med. 2015;175(5):682–689. doi:10.1001/jamainternmed.2015.97
45. Macedo LB, Josué AM, Maia PH, Câmara AE, Brasileiro JS. Effect of burst TENS and conventional TENS combined with cryotherapy on pressure pain threshold: randomised, controlled, clinical trial. Physiotherapy. 2015;101(2):155–160. doi:10.1016/j.physio.2014.07.004
46. Levis B, Benedetti A, Thombs BD. DEPRESsion Screening Data (DEPRESSD) Collaboration. Accuracy of Patient Health Questionnaire-9 (PHQ-9) forscreening to detect major depression: individual participant data meta-analysis. BMJ. 2019;365:l1476. doi:10.1136/bmj.l1476
47. Ghazisaeedi M, Mahmoodi H, Arpaci I, Mehrdar S, Barzegari S. Validity, Reliability, and optimal cut-off scores of the WHO-5, PHQ-9, and PHQ-2 to screen depression among University students in Iran. Int J Ment Health Addict. 2022;20(3):1824–1833. doi:10.1007/s11469-021-00483-5
48. Jin Y, Sha S, Tian T, et al. Network analysis of comorbid depression and anxiety and their associations with quality of life among clinicians in public hospitals during the late stage of the COVID-19 pandemic in China. J Affect Disord. 2022;314:193–200. doi:10.1016/j.jad.2022.06.051
49. Hao XY, Guo YX, Lou JS, et al. Mental health changes in elderly patients undergoing non-cardiac surgery during the COVID-19 pandemic in China. J Affect Disord. 2023;343:77–85. doi:10.1016/j.jad.2023.09.025
50. Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
51. Lee SY, Ju YJ, Lee JE, et al. Factors associated with poor sleep quality in the Korean general population: providing information from the Korean version of the Pittsburgh Sleep Quality Index. J Affect Disord. 2020;271:49–58. doi:10.1016/j.jad.2020.03.069
52. Costantini L, Pasquarella C, Odone A. Screening for depression in primary care with Patient Health Questionnaire-9 (PHQ-9): a systematic review. J Affect Disord. 2021;279:473–483. doi:10.1016/j.jad.2020.09.131
53. Wang X, Li JL, Wei XY, et al. Psychological and neurological predictors of acupuncture effect in patients with chronic pain: a randomized controlled neuroimaging trial. Pain. 2023;164(7):1578–1592. doi:10.1097/j.pain.0000000000002859
54. Suenaga H, Schifter M, Chen N, Ali F, Byth K, Peck C. Impact of oral/dental disease burden on postoperative infective complications: a prospective cohort study. Clin Oral Investig. 2023;27(11):6461–6470. doi:10.1007/s00784-023-05251-4
55. Gevelinger MM, Sanderson DJ, Jaworski E, Doyle PJ. Evaluation of sacral nerve stimulation device revision and explantation in a single center, multidisciplinary study. Neuromodulation. 2020;23(8):1201–1206. doi:10.1111/ner.13050
56. Courvoisier DS, Combescure C, Agoritsas T, Gayet-Ageron A, Perneger TV. Performance of logistic regression modeling: beyond the number of events per variable, the role of data structure. J Clin Epidemiol. 2011;64(9):993–1000. doi:10.1016/j.jclinepi.2010.11.012
57. Chen L, Ashton-James CE, Shi B, et al. Variability in the prevalence of depression among adults with chronic pain: UK Biobank analysis through clinical prediction models. BMC Med. 2024;22(1):167. doi:10.1186/s12916-024-03388-x
58. Rahman NA, Ariaratnam S, Hashim NA, Azhar ZI. Prevalence and factors associated with generalized anxiety disorder among patients with chronic pain: a single center cross sectional study in Malaysia. PLoS One. 2024;19(7):e0307992. doi:10.1371/journal.pone.0307992
59. Hu Y, Yang Z, Li Y, Xu Y, Zhou X, Guo N. Anxiety symptoms and associated factors among chronic low back pain patients in China: a cross-sectional study. Front Public Health. 2022;10:878865. doi:10.1371/journal.pone.0307992
60. Wiklund T, Gerdle B, Linton SJ, Dragioti E, Larsson B. Insomnia is a risk factor for spreading of chronic pain: a Swedish longitudinal population study (SwePain). Eur J Pain. 2020;24(7):1348–1356. doi:10.1002/ejp.1582
61. Cheatle MD, Foster S, Pinkett A, Lesneski M, Qu D, Dhingra L. Assessing and managing sleep disturbance in patients with chronic pain. Sleep Med Clin. 2016;11(4):531–541. doi:10.1016/j.jsmc.2016.08.004
62. Finan PH, Smith MT. The comorbidity of insomnia, chronic pain, and depression: dopamine as a putative mechanism. Sleep Med Rev. 2013;17(3):173–183. doi:10.1016/j.smrv.2012.03.003
63. Gerrits MMJG, van Oppen P, van Marwijk HWJ, Penninx BWJH, van der Horst HE. Pain and the onset of depressive and anxiety disorders. Pain. 2014;155(1):53–59. doi:10.1016/j.pain.2013.09.005
64. Xu Y, Wang Y, Chen J, et al. The comorbidity of mental and physical disorders with self-reported chronic back or neck pain: results from the China Mental Health Survey. J Affect Disord. 2020;260:334–341. doi:10.1016/j.jad.2019.08.089
65. Sørensen L, van Dongen JM, van Tulder M, Oestergaard LG. Prognostic factors for high societal costs: a register-based study on 561,665 patients with shoulder disorders. Pain. 2023;164(9):2104–2111. doi:10.1097/j.pain.0000000000002924
66. Dunbar E, Greer PJ, Melhem N, et al. Constant-severe pain in chronic pancreatitis is associated with genetic loci for major depression in the NAPS2 cohort. J Gastroenterol. 2020;55(10):1000–1009. doi:10.1007/s00535-020-01703-w
67. Thimma Ravindranath P, Smith JG, Niloofar RN, Ebelthite C, Renton T. Sleep disturbances are associated with pain intensity and pain-related functional interference in patients experiencing orofacial pain. J Oral Rehabil. 2023;50(10):980–990. doi:10.1111/joor.13521
68. Zhang W, Singh SP, Clement A, Calfee RP, Bijsterbosch JD, Cheng AL. Improvements in physical function and pain interference and changes in mental health among patients seeking musculoskeletal care. JAMA Network Open. 2023;6(6):e2320520. doi:10.1001/jamanetworkopen.2023.20520
69. Carle AC, Bevans KB, Tucker CA, Forrest CB. Using nationally representative percentiles to interpret PROMIS pediatric measures. Qual Life Res. 2021;30(4):997–1004. doi:10.1007/s11136-020-02700-5
70. LaRowe LR, Powers JM, Garey L, et al. Pain-related anxiety, sex, and co-use of alcohol and prescription opioids among adults with chronic low back pain. Drug Alcohol Depend. 2020;214:108171. doi:10.1016/j.drugalcdep.2020.108171
71. Leino P, Magni G. Depressive and distress symptoms as predictors of low back pain, neck-shoulder pain, and other musculoskeletal morbidity: a 10-year follow-up of metal industry employees. Pain. 1993;53(1):89–94. doi:10.1016/0304-3959(93)90060-3
72. McCullar KS, Barker DH, McGeary JE, et al. Altered sleep architecture following consecutive nights of presleep alcohol. Sleep. 2024;47(4):zsae003. doi:10.1093/sleep/zsae003
73. Vinograd M, Williams A, Sun M, et al. Neuroticism and interpretive bias as risk factors for anxiety and depression. Clin Psychol Sci. 2020;8(4):641–656. doi:10.1177/2167702620906145
74. Rojo-Wissar DM, Wanigatunga AA, Simonsick EM, et al. Personality and insomnia symptoms in older adults: the Baltimore Longitudinal Study of Aging. Sleep. 2021;44(9):zsab082. doi:10.1093/sleep/zsab082
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Psychological Disturbances and Their Association with Sleep Disturbance in Patients Admitted for Arrhythmia Diseases
Hu LX, Tang M, Hua W, Ren XQ, Jia YH, Chu JM, Zhang JT, Liu XN
Neuropsychiatric Disease and Treatment 2022, 18:1739-1750
Published Date: 17 August 2022
Therapy for Psychiatric Comorbidities in Patients with Episodic Cluster Headache: A Prospective Multicenter Study
Liu Q, Zhang Y, Hu C, Yuan D, Wang K, Fan W, Pan F, Li Q, Wang Y, Tan G
Journal of Pain Research 2022, 15:3245-3254
Published Date: 18 October 2022
Subjective Sleep Disruption and Mood Disorders are Associated with the Risk of Chronic Pain in Patients with Obstructive Sleep Apnea
Liu L, Li X, Xue P, Wu M, Zeng S, Dai Y, Zhou J
Nature and Science of Sleep 2022, 14:2023-2032
Published Date: 7 November 2022
The Interconnection Between Social Support and Emotional Distress Among Individuals with Chronic Pain: A Narrative Review
Franqueiro AR, Yoon J, Crago MA, Curiel M, Wilson JM
Psychology Research and Behavior Management 2023, 16:4389-4399
Published Date: 27 October 2023
Research Trends of Acupuncture Therapy for Chronic Pain-Related Depression or Anxiety from 2003 to 2023: A Bibliometric Analysis
Yang P, Wang T, He YJ, Su SY
Journal of Pain Research 2023, 16:4301-4315
Published Date: 15 December 2023