Back to Journals » Psychology Research and Behavior Management » Volume 16
The Interconnection Between Social Support and Emotional Distress Among Individuals with Chronic Pain: A Narrative Review
Authors Franqueiro AR, Yoon J ![]() , Crago MA, Curiel M, Wilson JM
, Crago MA, Curiel M, Wilson JM
Received 28 July 2023
Accepted for publication 21 October 2023
Published 27 October 2023 Volume 2023:16 Pages 4389—4399
DOI https://doi.org/10.2147/PRBM.S410606
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Angelina R Franqueiro, JiHee Yoon, Madelyn A Crago, Marie Curiel, Jenna M Wilson
Department of Anesthesiology, Perioperative and Pain Medicine, Brigham and Women’s Hospital, Boston, MA, 02115, USA
Correspondence: Jenna M Wilson, Department of Anesthesiology, Perioperative and Pain, Brigham and Women’s Hospital, Boston, MA, 02115, USA, Tel +1 7813673972, Email [email protected]
Abstract: Chronic pain is a public health concern affecting over 100 million U.S. adults. Because chronic pain is multifactorial, it requires a biopsychosocial approach to understand how biological, psychological, and social factors contribute to both the development and maintenance of pain. On average, individuals with chronic pain report higher levels of emotional distress compared to pain-free individuals. Research has demonstrated that social support is associated with better pain outcomes and less emotional distress. It has been proposed that social support may improve pain outcomes by reducing the influence of stressors. However, the majority of research exploring the relationships between social support and pain-related outcomes has focused on the direct relationship between these variables, largely overlooking the process by which social support has a positive influence on pain. This narrative review synthesizes research on how chronic pain, emotional distress, and social support are highly interconnected, yet research investigating chronic pain and emotional distress within a social context is limited. We then highlight disparities in chronic pain, such that the burden of chronic pain is unequal between demographic groups. Next, we discuss existing evidence for the use of group-based interventions to address pain-related outcomes. Lastly, we summarize limitations of prior research studies and highlight gaps in the current literature. Overall, longitudinal research comprehensively investigating the distinct nuances in the measurement of social support and how these nuances relate to emotional distress and pain outcomes is needed and may provide insight into the unique needs of individuals or subgroups. Further, demographically diverse randomized controlled trials are needed to identify the process by which group-based interventions improve pain outcomes and whether these interventions are more effective for particular groups in order to personalize treatment approaches and address inequities in pain care.
Keywords: chronic pain, social support, emotional distress, depression, anxiety, group-based interventions
Introduction
Chronic pain, defined as persistent pain for at least 3 months,1 is a public health concern affecting over 100 million U.S. adults.2–4 Common chronic pain conditions include low back pain, fibromyalgia, migraine, temporomandibular disorders (TMD), and chronic postsurgical pain. Among US adults, new cases of chronic pain are more prevalent than other conditions and diseases, such as diabetes and hypertension.5 Pain is one of the most common causes for seeking medical care,6 resulting in a large burden on the healthcare system. Importantly, chronic pain is a leading cause of physical disability and reduced quality of life.7 Because chronic pain is multifactorial, it requires a biopsychosocial approach to understand how biological, psychological, and social factors contribute to both the development and maintenance of pain.8 Although pain is an experience that often occurs in the presence of others, less research has focused on chronic pain within a social context, particularly investigating the role of social support.9
There is not consensus in the scholarly literature on the definition or conceptualization of the term social support. For example, social support can refer to both received and perceived support from family, friends, or significant others.10 Additionally, support can be measured based on different components, such as the type of support (eg, emotional, tangible, informational) or size of one’s social network (eg, number of close members).10 While some use the terms social support and loneliness interchangeably, social support is distinct from the construct of loneliness, which is an emotional state that often stems from the perception that one’s social needs are not being met by one’s social network.11 For the purpose of this narrative review, and given the limited scholarly literature on the complexities of social support in relation to chronic pain, we use the term social support broadly.
The stress-buffering model suggests that social support positively influences health outcomes by protecting individuals from the harmful effects of stress.12 Several studies have demonstrated that social support is associated with less pain severity and pain-related disability among individuals with chronic pain.13–15 It has been proposed that social support may be associated with less pain by reducing the influence of stressors or modulating an individual’s ability to cope.16 However, the majority of research exploring the relationship between social support and pain-related outcomes among individuals with chronic pain has focused on the direct relationship between these variables, largely overlooking the process by which social support has a positive influence on pain.17
On average, individuals with chronic pain report higher levels of emotional distress, including anxiety and depression, compared to pain-free individuals.18–20 Several review articles have highlighted the increased prevalence of emotional distress among individuals with chronic pain and emphasized how it impacts both the development and maintenance of pain symptoms across a variety of pain conditions (eg, low back pain, multiple sclerosis, TMD).9,15,21,22 While some review articles have also discussed the relations of various social factors (eg, loneliness, dissatisfaction with co-workers, social support) with pain outcomes,15,22 an understanding of how social support exerts its beneficial effects on chronic pain remains understudied. The biopsychosocial model of pain acknowledges how psychological and social factors independently and interactively impact pain outcomes.8 As social support has shown to have a positive impact on emotional distress, it may be particularly important to understand the influence of social support on pain while also considering its impact on emotional distress.
The purpose of this narrative review is to discuss how social support, emotional distress, and pain are highly interconnected, and thus, should be considered in conjunction with one another. A comprehensive approach for understanding emotional distress within a social context may provide further insights into prevention and intervention strategies among individuals with chronic pain. Additionally, we highlight important disparities in chronic pain, such that the burden of chronic pain is unequal between demographic groups, which may be important to consider in relation to emotional distress and social support. We also discuss existing evidence for the use of group-based interventions to address pain-related symptoms. Lastly, we summarize limitations of prior research studies and highlight gaps in the current literature.
Emotional Distress and Social Support Among Individuals with Chronic Pain
A well-studied psychological risk factor for chronic pain is emotional distress, which is often assessed based on an individual’s level of depression or anxiety.15 The severity of depression and anxiety symptoms can range from mild to severe and research has shown a large degree of variability across individuals. Depression often involves feelings of sadness, hopelessness, and helplessness.23 These negative feelings can influence an individual’s thoughts about their chronic pain. For example, an individual with high levels of depression may feel as though there is nothing that they can do to ever make their pain go away. Anxiety often involves feelings of worry or recurring negative thought patterns.24 An individual with high levels of anxiety may ruminate on thoughts related to their pain and worry about whether their pain will ever end. As individuals with chronic pain report higher levels of emotional distress than pain-free individuals, these negative thoughts about their pain and ability to cope with pain may exacerbate their symptoms, putting these individuals at risk of worse outcomes.
Although chronic pain can contribute to emotional distress, several prospective, longitudinal studies have shown that emotional distress may precede and be a risk factor for the development of several common chronic pain conditions, including low back pain, TMD, and chronic postsurgical pain.25–28 For example, among individuals with no history of chronic pain at baseline, depression predicted the development of moderate to severe chronic pain four years later.29 Preoperative (ie, baseline) depression and anxiety have also been shown to predict the development of chronic postsurgical pain after several types of common surgeries.30,31 Additionally, emotional distress has shown to predict the worsening of pain symptoms among individuals already experiencing acute or chronic pain. For example, several studies have shown that both general emotional distress and pain-specific distress (ie, ruminating on and feeling helpless in response to one’s pain) predicted worsened pain severity and pain-related disability over time among individuals with several chronic pain conditions, including fibromyalgia and low back pain.32–34
Within the general population, a large body of literature has consistently shown that social support is associated with less depression and anxiety,35 and longitudinally predicts reduced levels of emotional distress.36 Among individuals with chronic pain, several cross-sectional studies have shown that social support is associated with less depression, anxiety, and pain-related distress.14,37–43 Interestingly, one cross-sectional study found that greater social connectedness was related to lower anxiety, and, in turn, less pain.44 Although social support and social connectedness are distinct constructs, such that social connectedness measures an individual’s sense of belonging (eg, comfortability in the presence of strangers; ability to connect with other people),45 it is plausible that social support may be related to less emotional distress, and, in turn, better pain outcomes. However, limited research has investigated the longitudinal relationship between social support and emotional distress among individuals with chronic pain. While there is some evidence that social support may longitudinally predict less depression and anxiety over time among individuals with chronic pain,46,47 establishing a prospective link between social support and emotional distress could offer valuable insights into a process by which social support confers protective benefits in the context of pain. If emotional distress contributes to the relationship between social support and better pain outcomes, then an intervention designed to enhance one’s social support while simultaneously equipping individuals with coping strategies to better manage negative emotions may prove to be particularly beneficial in improving pain.
Demographic Considerations
Although chronic pain affects individuals from all backgrounds, research has shown that the burden of chronic pain is disproportionately experienced by members of vulnerable groups. Therefore, it is important to consider how gender, race/ethnicity, and age relate to chronic pain, emotional distress, and social support.
Gender
The prevalence of common chronic pain conditions is disproportionately higher for women than men, including fibromyalgia, migraine, TMD, and osteoarthritis.48–50 Additionally, women report more frequent daily pain, pain in more body areas (eg, widespread pain), and higher levels of clinical pain intensity than men.51 Given the documented gender differences in the prevalence and experience of chronic pain, it is necessary to consider gender differences in emotional distress and social support that may importantly influence the pain experience.
Women with chronic pain typically report higher levels of depression and anxiety than men.52,53 Additionally, women report greater emotional distress specifically related to the experience of pain, such as pain-related anxiety and negative ruminative and helpless thoughts about pain.51,54,55 On average, women also perceive more social support to be available if needed,56 report more frequent contact with their social connections,57 have larger social networks, and report more satisfaction with their social networks than men.58 However, much of the work on gender differences in social support has been conducted among the general population. While some studies showed that women with chronic pain used social support as a coping strategy more often and perceived more support to be available from friends than men,47,59 less work has explored gender differences in social support specifically among individuals with chronic pain.
Collectively, these considerations highlight the notable gap in the literature investigating gender differences in social support among individuals with chronic pain and suggest that elucidating these differences may help identify individuals most at-risk for poor pain outcomes, thus allowing for the tailoring of interventions. For example, if men with chronic pain typically report less social support than women, then it may be helpful to tailor interventions for men that incorporate building interpersonal relationships while learning skills to manage pain. Future studies should aim to understand how gender differences in emotional distress may affect chronic pain within a social context.
Race/Ethnicity
An accumulating body of research has demonstrated racial/ethnic disparities in chronic pain, such that underrepresented racial/ethnic groups tend to report more severe clinical pain.60–62 For example, a recent study showed that non-Hispanic Black and Hispanic individuals reported higher pain intensity and pain-related disability than White individuals.63 Similarly, a meta-analysis found that, on average, Black individuals with chronic pain reported higher pain intensity compared to White individuals.64 While studies focused on racial/ethnic differences in pain have primarily compared White and Black individuals, recent research suggests that Native Americans may experience a higher prevalence of chronic pain than other racial/ethnic groups in the U.S.,65,66 further highlighting the need for diverse research studies. Notably, several studies have shown that racial/ethnic disparities are present even while accounting for potential confounders, such as demographic factors (socioeconomic status, education, employment) and other health and medical comorbidities.60 Thus, it is important to consider how racial/ethnic differences in pain may be related to emotional distress and social support.
Research suggests that racial/ethnic differences may exist in emotions linked to the pain experience, such as depression and anxiety. For example, Black individuals with chronic pain tend to report higher levels of anxiety,67 depression, and greater helplessness related to their pain compared to White individuals.68–70 Likewise, a recent study showed that Black and Hispanic individuals with chronic pain reported more symptoms of depression and anxiety than White individuals.71 A meta-analysis also showed that Black individuals engaged in more pain-related rumination and helpless thinking compared to White individuals.72 Importantly, less research has focused on potential racial/ethnic differences in social support among individuals with chronic pain. One study found that Black individuals with chronic pain reported less social support than White individuals,73 whereas another study found no evidence of racial differences in social support.74 Given the scarcity of research on racial/ethnic differences in social support among individuals with chronic pain, it is critical that future studies address this gap. More inclusive research that goes beyond comparing just White and Black individuals is also needed and may provide insight into the implementation of personalized intervention strategies.
Age
Chronic pain is highly prevalent among older adults (≥65 years). Approximately 38–50% of community-dwelling older adults report chronic pain,75,76 and research suggests that the prevalence of chronic pain increases with chronological age.77,78 As life expectancy and the population age continue to rise,79 the number of people over the age of 65 living with chronic pain is expected to increase. Therefore, it is important to consider age-related differences in emotional distress and social support that may influence the experience of pain.
According to the socioemotional selectivity theory, there is a systematic shift in time perspective as people age, which results in a change in motivational goals, emotional well-being, and social relationships.80,81 In early adulthood, people perceive the future as expansive, tend to focus on longer-term goals, and are motivated to acquire knowledge and information. Later in life, however, people view the future as more limited due to an awareness of their own mortality and shift their focus towards shorter-term goals. As a result, older adults tend to focus on the present moment and are motivated to maximize positive experiences and avoid negative experiences.
Several studies have shown that older adults report lower levels of depression and anxiety compared to younger adults,82–84 which is known as the “well-being paradox” of aging. Interestingly, research has also shown that older adults report daily stressful hassles as less unpleasant and report less intrusive thoughts and emotional distress in response to these stressors compared to younger adults.85,86 In addition to age-related changes in emotional well-being, research suggests that social relationships change across adulthood. During early adulthood, people tend to explore new social relationships and have larger social networks, as this is a form of knowledge acquisition. In contrast, as people age, they “prune” unrewarding social relationships and focus on maintaining relationships they perceive as emotionally meaningful, favoring quality over quantity. Indeed, research has found that the number of peripheral social connections decreases across adulthood, resulting in a smaller social network, while the number of close social connections remains stable.87,88 Although having a small network size may be related to loneliness, it is the intimacy and importance of relationships that is most critical in older age.84
Notably, the socioemotional selectivity theory has not yet been applied to individuals living with chronic pain, a subgroup that may face more daily stressors and challenges performing everyday activities. Thus, it remains largely unclear how living with chronic pain may influence time perspective, whether the “well-being paradox” applies to this subgroup of older adults, and what impact the possible shift in social relationships has on their lives. Potentially, older adults living with chronic pain may face unique daily challenges that contribute to high levels of emotional distress and the benefits of a smaller, closer social network may not generalize to this subgroup of adults. Yet, one study on patients with chronic low back pain demonstrated that older age was associated with lower levels of depression and anxiety.89 Future studies should aim to critically examine whether the socioemotional selectivity theory applies to older adults living with chronic pain to understand its potential generalizability and subsequently inform treatment approaches. Investigating whether the socioemotional selectivity theory extends to this subgroup of older adults is an important area for future research as the number of older adults with chronic pain continues to grow.
Clinical Implications
A substantial body of evidence suggests that increased social support can facilitate recovery and adaptation to chronic pain, leading to better outcomes.13 Thus, interventions targeting social support have garnered increased attention. One of the most common ways in which social support is integrated into the treatment of chronic pain is by utilizing a group-based modality. Group-based interventions create a sense of community and belonging among participants by providing a supportive environment where individuals with similar chronic conditions can connect to share their challenges and successes, while also learning from those around them.10 These interventions can help individuals feel as though they are better able to manage their chronic pain, while providing them with the tools to evaluate and cope with stressors more effectively, and thus, engage in more adaptive behaviors.90
In general, studies assessing the efficacy of group-based interventions for chronic pain have shown promising results. For example, a meta-analysis found that group-based cognitive behavioral therapy (CBT) resulted in greater improvements in pain, depression, and physical functioning compared to control groups.91 Another meta-analysis found that psychological interventions that used cognitive behavioral techniques (eg, cognitive restructuring, cognitive coping skills) led to reductions in pain and emotional distress, and that the use of group-based interventions resulted in greater improvements compared to individually delivered approaches.92 Online interventions have also become increasingly popular as they can often address barriers of in-person treatments by offering a relatively accessible and convenient means of accessing tools. However, online interventions are often individualized, and thus, they overlook the importance of addressing pain within a social context. Some research has shown that online group-based CBT and acceptance and commitment therapy improved pain, pain-related disability, anxiety, and pain-specific rumination and helplessness.93,94 Additionally, a recent systematic review found that online group-based teletherapy (eg, CBT, mindfulness) reduced pain, emotional distress, pain-specific negative thoughts, and physical disability among individuals with chronic pain.95 Importantly, this review identified a large gap within the literature, such that there are few rigorous randomized controlled trials (RCTs) investigating the efficacy of group-based online interventions among individuals with chronic pain, which is an important area for future studies.
Researchers have also begun to explore the role of support groups on social media platforms, which are accessible in a variety of formats and allow individuals to connect more flexibly. For example, research has found that both peer-led and professionally-guided Facebook groups for chronic pain effectively reduced pain, pain-related disability, and depression, while also increasing social support.96,97 Notably, these studies provide evidence that support programs that do not involve components from psychological interventions are also effective at positively impacting pain and emotional distress. Interestingly, one study also examined the Facebook posts that participants made within these groups and found that individuals with chronic pain tended to refer to people with chronic pain as “us” and individuals without chronic pain as “them.” For example, participants discussed how they often isolate themselves from family and friends because they feel judged and misunderstood by “them.”96 Receiving validation in these social media groups from others who also suffer from chronic pain may potentially reduce emotional distress,98 resulting in improved pain.
In line with this, one factor that has been shown to impede treatment effectiveness in patients with chronic pain is stigma. Pain is a subjective experience and several chronic pain conditions lack clear medical pathology or are non-specific (eg, fibromyalgia, low back pain).99,100 As such, individuals with chronic pain often report feeling as though their friends, family, or health care providers do not believe them, and sometimes even blame or dismiss them, which can result in feelings of invalidation.101 These feelings of invalidation, stemming from the stigma associated with chronic pain, have been shown to impede help-seeking behavior and diminish the efficacy of treatments.102 Therefore, while group-based interventions and those delivered via online platforms have shown promising results, it is important to assess barriers imposed by stigma associated with chronic pain.
Additionally, chronic pain-related stigma intersects with stigmas related to other individual characteristics, and research has shown that gender- and race-related disparities exist within pain management and treatment. Both gender- and race-related stigmas shape how others perceive individuals with chronic pain and their experiences of pain, subsequently affecting how they are treated in a clinical setting. For example, studies have shown that health care providers tend to provide women with less adequate pain care compared to men.103 Specifically, women are perceived as more pain sensitive than men, with the source of their pain often attributed to psychological rather than somatic factors, and they are prescribed less pain medication on average.104,105 Similarly, research has shown that health care providers tend to underestimate pain in Black patients compared to White patients.106 Further, compared to White patients with chronic pain, racial/ethnic minorities are less likely to be prescribed opioids to help manage pain, with the strongest evidence for Black patients.107 Thus, research suggests that chronic pain may be more stigmatized among women and racial/ethnic minorities,108 underscoring the importance of considering these factors when treating patients with chronic pain.
Considerations for Future Research
Social support is a complex construct and few studies have investigated how nuances in its conceptualization may relate to emotional distress or pain among individuals with chronic pain. One longitudinal study of patients with chronic low back pain examined whether subtypes of support (ie, affectionate, informational, and tangible support; positive social interactions) differentially predicted reductions in depression over time.46 Interestingly, they found that tangible and informational support were more consistently associated with recovery from depression and less depressive symptoms over time compared to affectionate support and positive social interactions. These findings provide initial evidence that different aspects of social support may be important for understanding emotional distress among individuals with chronic pain. Future studies should incorporate multidimensional measures that capture these nuances to better understand the relationship of social support with emotional distress and pain. Investigating distinct aspects of social support across chronic pain conditions (eg, TMD, fibromyalgia) may also provide insight into the unique needs of subgroups of individuals based on their condition-specific symptoms. Identifying which aspects of support are most beneficial, and for whom, will help inform intervention targets.
Although there is growing evidence for the efficacy of group-based interventions for chronic pain, the majority of these studies have been demographically skewed. Most of these studies have largely focused on women and White patients. One major limitation across these studies is that many do not report the racial/ethnic breakdown of their entire sample, but rather only report on the percentage that was White, with some studies not reporting any racial/ethnic information on their sample. Thus, it remains largely unknown what racial/ethnic groups have been included in these studies. As a result, it is unclear how the efficacy of these interventions may generalize to other groups of individuals, or whether these interventions are more effective for particular groups. Because evidence from RCTs is often used to inform clinical practice procedures and policies, it is critical to include diverse participants in research to expand on the generalizability of findings, increase real-world applications, and address inequities in pain care.109
Additionally, while research has shown that several forms of group-based interventions are effective at improving pain outcomes among individuals with chronic pain, the process by which these interventions improve pain remains largely understudied. As many of these interventions have also shown to effectively reduce depression, anxiety, and pain-specific negative thoughts, it is plausible that reductions in emotional distress contribute to improvements in pain. It is critical that future RCTs investigate and identify the causal process that explains the efficacy of these interventions. This information can be used to further inform the development and refinement of intervention strategies. In addition to investigating the means by which group-based interventions effectively reduce pain, it is important to identify for whom these interventions may work best to avoid employing interventions that are not suitable for a subgroup of individuals. Personalized treatment approaches, whereby prevention and intervention strategies are tailored based on the individual/population of interest, are necessary to improve chronic pain disparities.
Conclusion
Psychological and social factors contribute to the development and maintenance of chronic pain, yet research investigating chronic pain and emotional distress within a social context is limited. This narrative review synthesized research on the interconnections between social support, emotional distress, and chronic pain (see Box 1), and demonstrated that more research in this area is needed to fully elucidate these relationships. For example, while there is likely a bidirectional relationship between support, emotional distress, and pain, prospective, longitudinal studies are necessary to determine potential temporal precedence and causation. Additionally, it is important that future studies investigate the distinct nuances in the measurement of social support to identify which aspects of support may be most beneficial, and for whom, to inform intervention targets.
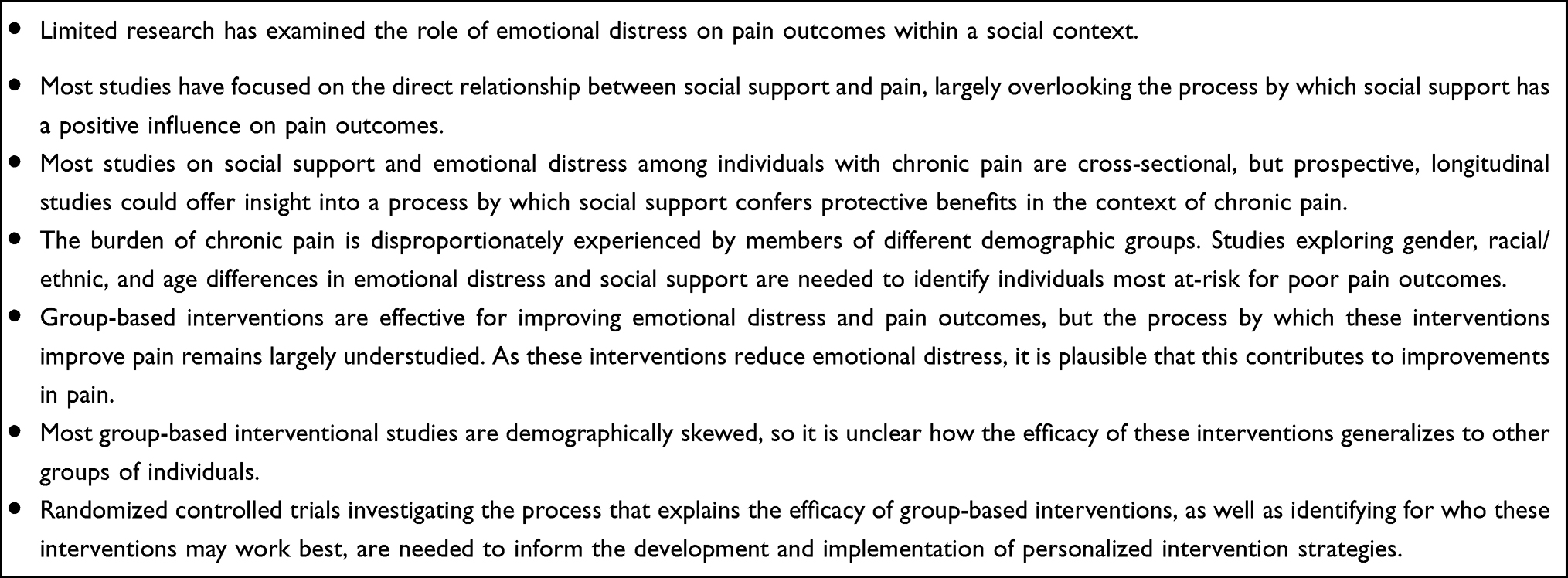 |
Box 1 Key Findings |
While studies have demonstrated that the burden of chronic pain is disproportionately experienced by women, racial/ethnic minorities, and older adults, limited work has focused on how these groups may differentially experience emotional distress within a social context, which may subsequently influence their experience of pain. Although evidence for the use of group-based interventions suggests significant improvements in pain and emotional distress, the process underlying the efficacy of these interventions remains largely unknown. Future RCTs should aim to elucidate the process by which these interventions lead to improvements in pain to inform potential refinements of strategies. Further, it is critical that future RCTs include demographically diverse samples to better understand who may benefit most and to tailor strategies appropriately for the population of interest. Lastly, it is important to note that this was a narrative review of the scholarly literature, and systematic or meta-analytic reviews might reveal additional insights not discussed in this review.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kennedy R, Abd-Elsayed A. The international association for the study of pain (IASP) classification of chronic pain syndromes. Pain. 2019:1101–1103. doi:10.1007/978-3-319-99124-5_234
2. Simon LS. Relieving pain in America: a blueprint for transforming prevention, care, education, and research. J Pain Palliat Care Pharmacother. 2012;26(2):197–198. doi:10.3109/15360288.2012.678473
3. Treede R-D, Rief W, Barke A, et al. A classification of chronic pain for ICD-11. Pain. 2015;156(6):1003. doi:10.1097/j.pain.0000000000000160
4. Yong RJ, Mullins PM, Bhattacharyya N. Prevalence of chronic pain among adults in the United States. Pain. 2022;163(2):e328–e332. doi:10.1097/j.pain.0000000000002291
5. Nahin RL, Feinberg T, Kapos FP, Terman GW. Estimated rates of incident and persistent chronic pain among US adults, 2019–2020. JAMA Netw Open. 2023;6(5):e2313563–e2313563. doi:10.1001/jamanetworkopen.2023.13563
6. Mäntyselkä P, Kumpusalo E, Ahonen R, et al. Pain as a reason to visit the doctor: a study in Finnish primary health care. Pain. 2001;89(2–3):175–180. doi:10.1016/S0304-3959(00)00361-4
7. Goldberg DS, McGee SJ. Pain as a global public health priority. BMC Public Health. 2011;11(1):1–5. doi:10.1186/1471-2458-11-770
8. Gatchel RJ, Peng YB, Peters ML, Fuchs PN, Turk DC. The biopsychosocial approach to chronic pain: scientific advances and future directions. Psychol Bull. 2007;133(4):581. doi:10.1037/0033-2909.133.4.581
9. Meints S, Edwards R. Evaluating psychosocial contributions to chronic pain outcomes. Prog Neuropsychopharmacol Biol Psychiatry. 2018;87:168–182. doi:10.1016/j.pnpbp.2018.01.017
10. Uchino BN. Social Support and Physical Health: Understanding the Health Consequences of Relationships. Yale university press; 2004.
11. Peplau LA, Perlman D. Loneliness: a sourcebook of current theory, research, and therapy; 1982.
12. Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychol Bull. 1985;98(2):310. doi:10.1037/0033-2909.98.2.310
13. Jensen MP, Moore MR, Bockow TB, Ehde DM, Engel JM. Psychosocial factors and adjustment to chronic pain in persons with physical disabilities: a systematic review. Arch Phys Med Rehabil. 2011;92(1):146–160. doi:10.1016/j.apmr.2010.09.021
14. Wilson JM, Colebaugh CA, Flowers KM, Meints SM, Edwards RR, Schreiber KL. Social support and psychological distress among chronic pain patients: the mediating role of mindfulness. Pers Individ Dif. 2022;190:111551. doi:10.1016/j.paid.2022.111551
15. Edwards RR, Dworkin RH, Sullivan MD, Turk DC, Wasan AD. The role of psychosocial processes in the development and maintenance of chronic pain. J Pain. 2016;17(9):T70–T92. doi:10.1016/j.jpain.2016.01.001
16. Che X, Cash R, Ng SK, Fitzgerald P, Fitzgibbon BM. A systematic review of the processes underlying the main and the buffering effect of social support on the experience of pain. Clin J Pain. 2018;34(11):1061–1076. doi:10.1097/AJP.0000000000000624
17. Bernardes SF, Forgeron P, Fournier K, Reszel J. Beyond solicitousness: a comprehensive review on informal pain-related social support. Pain. 2017;158(11):2066–2076. doi:10.1097/j.pain.0000000000001033
18. Burke AL, Mathias JL, Denson LA. Psychological functioning of people living with chronic pain: a meta‐analytic review. Br J Clin Psychol. 2015;54(3):345–360. doi:10.1111/bjc.12078
19. Howe CQ, Robinson JP, Sullivan MD. Psychiatric and psychological perspectives on chronic pain. Phys Med Rehabil Clin. 2015;26(2):283–300. doi:10.1016/j.pmr.2014.12.003
20. Hoffmann RG, Kotchen JM, Kotchen TA, Cowley T, Dasgupta M, Cowley AW Jr. Temporomandibular disorders and associated clinical comorbidities. Clin J Pain. 2011;27(3):268–274. doi:10.1097/AJP.0b013e31820215f5
21. Turk DC, Fillingim RB, Ohrbach R, Patel KV. Assessment of psychosocial and functional impact of chronic pain. J Pain. 2016;17(9):T21–T49. doi:10.1016/j.jpain.2016.02.006
22. Miaskowski C, Blyth F, Nicosia F, et al. A biopsychosocial model of chronic pain for older adults. Pain Med. 2020;21(9):1793–1805. doi:10.1093/pm/pnz329
23. Abramson LY, Metalsky GI, Alloy LB. Hopelessness depression: a theory-based subtype of depression. Psychol Rev. 1989;96(2):358. doi:10.1037/0033-295X.96.2.358
24. Mathews A. Why worry? The cognitive function of anxiety. Behav Res Ther. 1990;28(6):455–468. doi:10.1016/0005-7967(90)90132-3
25. Fillingim RB, Ohrbach R, Greenspan JD, et al. Psychological factors associated with development of TMD: the OPPERA prospective cohort study. J Pain. 2013;14(12):T75–T90. doi:10.1016/j.jpain.2013.06.009
26. Diatchenko L, Fillingim RB, Smith SB, Maixner W. The phenotypic and genetic signatures of common musculoskeletal pain conditions. Nat Rev Rheumatol. 2013;9(6):340–350. doi:10.1038/nrrheum.2013.43
27. Slade G, Diatchenko L, Bhalang K, et al. Influence of psychological factors on risk of temporomandibular disorders. J Dent Res. 2007;86(11):1120–1125. doi:10.1177/154405910708601119
28. Schreiber KL, Kehlet H, Belfer I, Edwards RR. Predicting, preventing and managing persistent pain after breast cancer surgery: the importance of psychosocial factors. Pain Manag. 2014;4(6):445–459. doi:10.2217/pmt.14.33
29. Landmark T, Dale O, Romundstad P, Woodhouse A, Kaasa S, Borchgrevink PC. Development and course of chronic pain over 4 years in the general population: the HUNT pain study. Eur J Pain. 2018;22(9):1606–1616. doi:10.1002/ejp.1243
30. Theunissen M, Peters ML, Bruce J, Gramke H-F, Marcus MA. Preoperative anxiety and catastrophizing: a systematic review and meta-analysis of the association with chronic postsurgical pain. Clin J Pain. 2012;28(9):819–841. doi:10.1097/AJP.0b013e31824549d6
31. Wilson JM, Colebaugh CA, Flowers KM, et al. Applying the rapid OPPERA algorithm to predict persistent pain outcomes among a cohort of women undergoing breast cancer surgery. J Pain. 2022;23(12):2003–2012. doi:10.1016/j.jpain.2022.07.012
32. Wilson JM, Schreiber KL, Mackey S, et al. Increased pain catastrophizing longitudinally predicts worsened pain severity and interference in patients with chronic pain and cancer: a collaborative health outcomes information registry study (CHOIR). Psycho‐Oncology. 2022;31(10):1753–1761. doi:10.1002/pon.6020
33. Wilson JM, Colebaugh CA, Flowers KM, Edwards RR, Schreiber KL. Profiles of risk and resilience in chronic pain: loneliness, social support, mindfulness, and optimism coming out of the first pandemic year. Pain Med. 2022;23(12):2010–2021. doi:10.1093/pm/pnac079
34. Lerman SF, Rudich Z, Brill S, Shalev H, Shahar G. Longitudinal associations between depression, anxiety, pain, and pain-related disability in chronic pain patients. Psychosom Med. 2015;77(3):333–341. doi:10.1097/PSY.0000000000000158
35. Bjørlykhaug KI, Karlsson B, Hesook SK, Kleppe LC. Social support and recovery from mental health problems: a scoping review. Nordic Social Work Res. 2022;12(5):666–697. doi:10.1080/2156857X.2020.1868553
36. Wang J, Mann F, Lloyd-Evans B, Ma R, Johnson S. Associations between loneliness and perceived social support and outcomes of mental health problems: a systematic review. BMC Psychiatry. 2018;18(1):1–16. doi:10.1186/s12888-018-1736-5
37. Cano A. Pain catastrophizing and social support in married individuals with chronic pain: the moderating role of pain duration. Pain. 2004;110(3):656–664. doi:10.1016/j.pain.2004.05.004
38. Du S, Hu Y, Bai Y, et al. Emotional distress correlates among patients with chronic nonspecific low back pain: a hierarchical linear regression analysis. Pain Pract. 2019;19(5):510–521. doi:10.1111/papr.12772
39. Nicholas MK, Coulston CM, Asghari A, Malhi GS. Depressive symptoms in patients with chronic pain. Med J Aust. 2009;190(S7):S66–S70. doi:10.5694/j.1326-5377.2009.tb02473.x
40. Zheng X, Wang Y, Jin X, et al. Factors influencing depression in community-dwelling elderly patients with osteoarthritis of the knee in China: a cross-sectional study. BMC Geriatr. 2022;22(1):453. doi:10.1186/s12877-022-03117-0
41. Zyrianova Y, Kelly BD, Gallagher C, et al. Depression and anxiety in rheumatoid arthritis: the role of perceived social support. Ir J Med Sci. 2006;175:32–36. doi:10.1007/BF03167946
42. Matthias MS, Hirsh AT, Ofner S, Daggy J. Exploring the relationships among social support, patient activation, and pain-related outcomes. Pain Med. 2022;23(4):676–685. doi:10.1093/pm/pnab306
43. Cano A, Leong L, Heller JB, Lutz JR. Perceived entitlement to pain-related support and pain catastrophizing: associations with perceived and observed support. PAIN®. 2009;147(1–3):249–254. doi:10.1016/j.pain.2009.09.023
44. Baumgartner JN, Haupt MR, Case LK. Chronic pain patients low in social connectedness report higher pain and need deeper pressure for pain relief. Emotion. 2023. doi:10.1037/emo0001228
45. Lee RM, Robbins SB. The relationship between social connectedness and anxiety, self-esteem, and social identity. J Couns Psychol. 1998;45(3):338–345. doi:10.1109/58.660144
46. McKillop AB, Carroll LJ, Jones CA, Battié MC. The relation of social support and depression in patients with chronic low back pain. Disabil Rehabil. 2017;39(15):1482–1488. doi:10.1080/09638288.2016.1202335
47. Koelmel E, Hughes AJ, Alschuler KN, Ehde DM. Resilience mediates the longitudinal relationships between social support and mental health outcomes in multiple sclerosis. Arch Phys Med Rehabil. 2017;98(6):1139–1148. doi:10.1016/j.apmr.2016.09.127
48. Fillingim RB. Sex, gender, and pain. In: Principles of Gender-Specific Medicine. Elsevier; 2023:769–792.
49. Bartley EJ, Fillingim RB. Sex differences in pain: a brief review of clinical and experimental findings. Br J Anaesth. 2013;111(1):52–58. doi:10.1093/bja/aet127
50. Lai YC, Yap AU, Türp JC. Prevalence of temporomandibular disorders in patients seeking orthodontic treatment: a systematic review. J Oral Rehabil. 2020;47(2):270–280. doi:10.1111/joor.12899
51. Bartley EJ, Palit S. Gender and pain. Curr Anesthesiol Rep. 2016;6:344–353. doi:10.1007/s40140-016-0177-2
52. Castro-Sánchez AM, Matarán-Peñarrocha GA, López-Rodríguez MM, Lara-Palomo IC, Arendt-Nielsen L, Fernández-de-las-Peñas C. Gender differences in pain severity, disability, depression, and widespread pressure pain sensitivity in patients with fibromyalgia syndrome without comorbid conditions. Pain Med. 2012;13(12):1639–1647. doi:10.1111/j.1526-4637.2012.01523.x
53. Serdarevic M, Striley CW, Cottler LB. Gender differences in prescription opioid use. Curr Opin Psychiatry. 2017;30(4):238. doi:10.1097/YCO.0000000000000337
54. Ramírez-Maestre C, Esteve R. The role of sex/gender in the experience of pain: resilience, fear, and acceptance as central variables in the adjustment of men and women with chronic pain. J Pain. 2014;15(6):608–618. e1. doi:10.1016/j.jpain.2014.02.006
55. El-Shormilisy N, Strong J, Meredith PJ. Associations among gender, coping patterns and functioning for individuals with chronic pain: a systematic review. Pain Res Manag. 2015;20:48–55. doi:10.1155/2015/490610
56. Wilson JM, Smith K, Strough J, Delaney R. Knowing you are there makes the difference: perceived social support, preferences for using support, and health. J Women Aging. 2021;33(4):396–410. doi:10.1080/08952841.2020.1860633
57. Fischer CS, Beresford L. Changes in support networks in late middle age: the extension of gender and educational differences. J Gerontol Series B Psychol Sci Soc Sci. 2015;70(1):123–131. doi:10.1093/geronb/gbu057
58. Antonucci T, Akiyama H, Takahashi K. Attachment and close relationships across the life span. Attach Hum Dev. 2004;6(4):353–370. doi:10.1080/1461673042000303136
59. Fillingim RB, King CD, Ribeiro-Dasilva MC, Rahim-Williams B, Riley JL III. Sex, gender, and pain: a review of recent clinical and experimental findings. J Pain. 2009;10(5):447–485. doi:10.1016/j.jpain.2008.12.001
60. Campbell CM, Edwards RR. Ethnic differences in pain and pain management. Pain Manag. 2012;2(3):219–230. doi:10.2217/pmt.12.7
61. Meints SM, Cortes A, Morais CA, Edwards RR. Racial and ethnic differences in the experience and treatment of noncancer pain. Pain Manag. 2019;9(3):317–334. doi:10.2217/pmt-2018-0030
62. Green CR, Anderson KO, Baker TA, et al. The unequal burden of pain: confronting racial and ethnic disparities in pain. Pain Med. 2003;4(3):277–294. doi:10.1046/j.1526-4637.2003.03034.x
63. Yang Y, Reid MC, Grol-Prokopczyk H, Pillemer K. Racial-ethnic disparities in pain intensity and interference among middle-aged and older US adults. J Gerontol Series B. 2022;77(2):e74–e81. doi:10.1093/gerona/glab207
64. Vaughn IA, Terry EL, Bartley EJ, Schaefer N, Fillingim RB. Racial-ethnic differences in osteoarthritis pain and disability: a meta-analysis. J Pain. 2019;20(6):629–644. doi:10.1016/j.jpain.2018.11.012
65. Zajacova A, Grol-Prokopczyk H, Fillingim R. Beyond black vs white: racial/ethnic disparities in chronic pain including Hispanic, Asian, Native American, and multiracial US adults. Pain. 2022;163(9):1688–1699. doi:10.1097/j.pain.0000000000002574
66. Ross E, Huber F, Kuhn B, et al. (232) Assessing chronic pain onset in Native Americans: follow-up results from the Oklahoma Study of Native American Pain Risk (OK-SNAP). J Pain. 2019;20(4):S33. doi:10.1016/j.jpain.2019.01.153
67. Riley JL III, Wade JB, Myers CD, Sheffield D, Papas RK, Price DD. Racial/ethnic differences in the experience of chronic pain. Pain. 2002;100(3):291–298. doi:10.1016/S0304-3959(02)00306-8
68. Shavers VL, Bakos A, Sheppard VB. Race, ethnicity, and pain among the US adult population. J Health Care Poor Underserved. 2010;21(1):177–220. doi:10.1353/hpu.0.0255
69. Allen KD, Helmick CG, Schwartz TA, DeVellis RF, Renner JB, Jordan JM. Racial differences in self-reported pain and function among individuals with radiographic hip and knee osteoarthritis: the Johnston County Osteoarthritis Project. Osteoarthritis Cartilage. 2009;17(9):1132–1136. doi:10.1016/j.joca.2009.03.003
70. Aroke EN, Joseph PV, Roy A, et al. Could epigenetics help explain racial disparities in chronic pain? J Pain Res. 2019;Volume 12:701–710. doi:10.2147/JPR.S191848
71. Roseen EJ, Smith CN, Essien UR, et al. Racial and ethnic disparities in the incidence of high-impact chronic pain among primary care patients with acute low back pain: a cohort study. Pain Med. 2023;24(6):633–643. doi:10.1093/pm/pnac193
72. Meints SM, Miller MM, Hirsh AT. Differences in pain coping between black and white Americans: a meta-analysis. J Pain. 2016;17(6):642–653. doi:10.1016/j.jpain.2015.12.017
73. Vina ER, Cloonan YK, Ibrahim SA, Hannon MJ, Boudreau RM, Kwoh CK. Race, sex, and total knee replacement consideration: role of social support. Arthritis Care Res. 2013;65(7):1103–1111. doi:10.1002/acr.21925
74. Mickle AM, Domenico LH, Tanner JJ, et al. Elucidating factors contributing to disparities in pain-related experiences among adults with or at risk for knee osteoarthritis. Front Pain Res. 2023;4:1058476. doi:10.3389/fpain.2023.1058476
75. Patel KV, Guralnik JM, Dansie EJ, Turk DC. Prevalence and impact of pain among older adults in the United States: findings from the 2011 National Health and Aging Trends Study. Pain®. 2013;154(12):2649–2657. doi:10.1016/j.pain.2013.07.029
76. Larsson C, Hansson EE, Sundquist K, Jakobsson U. Chronic pain in older adults: prevalence, incidence, and risk factors. Scand J Rheumatol. 2017;46(4):317–325. doi:10.1080/03009742.2016.1218543
77. Docking RE, Fleming J, Brayne C, Zhao J, Macfarlane GJ, Jones GT. Epidemiology of back pain in older adults: prevalence and risk factors for back pain onset. Rheumatology. 2011;50(9):1645–1653. doi:10.1093/rheumatology/ker175
78. Helme RD, Gibson SJ. The epidemiology of pain in elderly people. Clin Geriatr Med. 2001;17(3):417–431. doi:10.1016/S0749-0690(05)70078-1
79. He W, Goodkind D, Kowal PR. An aging world: 2015. Washington, DC: United States Census Bureau; 2016.
80. Carstensen LL. Selectivity theory: social activity in life-span context. Annu Rev Gerontol Geriatr. 1991;11(1):195–217.
81. Carstensen LL. Evidence for a life-span theory of socioemotional selectivity. Curr Dir Psychol Sci. 1995;4(5):151–156. doi:10.1111/1467-8721.ep11512261
82. Wilson JM, Lee J, Shook NJ. COVID-19 worries and mental health: the moderating effect of age. Aging Ment Health. 2021;25(7):1289–1296. doi:10.1080/13607863.2020.1856778
83. Charles ST, Piazza JR. Age differences in affective well‐being: context matters. Soc Personal Psychol Compass. 2009;3(5):711–724. doi:10.1111/j.1751-9004.2009.00202.x
84. Charles ST, Carstensen LL. Social and emotional aging. Ann Rev Psychol. 2010;61:383–409. doi:10.1146/annurev.psych.093008.100448
85. Neubauer AB, Smyth JM, Sliwinski MJ. Age differences in proactive coping with minor hassles in daily life. J Gerontol Series B. 2019;74(1):7–16. doi:10.1093/geronb/gby061
86. Brose A, Schmiedek F, Lövdén M, Lindenberger U. Normal aging dampens the link between intrusive thoughts and negative affect in reaction to daily stressors. Psychol Aging. 2011;26(2):488. doi:10.1037/a0022287
87. English T, Carstensen LL. Selective narrowing of social networks across adulthood is associated with improved emotional experience in daily life. Int J Behav Dev. 2014;38(2):195–202. doi:10.1177/0165025413515404
88. Bruine de Bruin W, Parker AM, Strough J. Age differences in reported social networks and well-being. Psychol Aging. 2020;35(2):159. doi:10.1037/pag0000415
89. Wettstein M, Eich W, Bieber C, Tesarz J. Pain intensity, disability, and quality of life in patients with chronic low back pain: does age matter? Pain Med. 2019;20(3):464–475. doi:10.1093/pm/pny062
90. Finlay KA, Peacock S, Elander J. Developing successful social support: an interpretative phenomenological analysis of mechanisms and processes in a chronic pain support group. Psychol Health. 2018;33(7):846–871. doi:10.1080/08870446.2017.1421188
91. Khoo E-L, Small R, Cheng W, et al. Comparative evaluation of group-based mindfulness-based stress reduction and cognitive behavioural therapy for the treatment and management of chronic pain: a systematic review and network meta-analysis. BMJ Ment Health. 2019;22(1):26–35.
92. Niknejad B, Bolier R, Henderson CR, et al. Association between psychological interventions and chronic pain outcomes in older adults: a systematic review and meta-analysis. JAMA Intern Med. 2018;178(6):830–839. doi:10.1001/jamainternmed.2018.0756
93. Martinson A, Johanson K, Wong S. Examining the efficacy of a Brief Cognitive-Behavioral Therapy for Chronic Pain (Brief CBT-CP) group delivered via VA Video Connect (VVC) among older adult veterans. Clin Gerontol. 2023;1–14. doi:10.1080/07317115.2023.2186303
94. Sanabria-Mazo JP, Colomer-Carbonell A, Borràs X, et al. Efficacy of videoconference group Acceptance and Commitment Therapy (ACT) and Behavioral Activation Therapy for Depression (BATD) for chronic low back pain (CLBP) plus comorbid depressive symptoms: a randomized controlled trial (IMPACT study). J Pain. 2023;24(8):1522–1540. doi:10.1016/j.jpain.2023.04.008
95. Mariano TY, Wan L, Edwards RR, Jamison RN. Online teletherapy for chronic pain: a systematic review. J Telemed Telecare. 2021;27(4):195–208. doi:10.1177/1357633X19871746
96. Tankha H, Pester BD, Brumley KM, et al. A mixed-methods investigation into the us versus them mentality in Facebook groups for chronic pain. Health Psychol. 2023;42(7):460–471. doi:10.1037/hea0001289
97. Pester BD, Tankha H, Caño A, et al. Facing pain together: a randomized controlled trial of the effects of facebook support groups on adults with chronic pain. J Pain. 2022;23(12):2121–2134. doi:10.1016/j.jpain.2022.07.013
98. Edmond SN, Keefe FJ. Validating pain communication: current state of the science. Pain. 2015;156(2):215. doi:10.1097/01.j.pain.0000460301.18207.c2
99. Kool M, Van Middendorp H, Lumley M, et al. Lack of understanding in fibromyalgia and rheumatoid arthritis: the illness invalidation inventory (3* I). Ann Rheum Dis. 2010;69(11):1990–1995. doi:10.1136/ard.2009.123224
100. Koes BW, Van Tulder M, Thomas S. Diagnosis and treatment of low back pain. BMJ. 2006;332(7555):1430–1434. doi:10.1136/bmj.332.7555.1430
101. Holloway I, Sofaer-Bennett B, Walker J. The stigmatisation of people with chronic back pain. Disabil Rehabil. 2007;29(18):1456–1464. doi:10.1080/09638280601107260
102. Slade SC, Molloy E, Keating JL. Stigma experienced by people with nonspecific chronic low back pain: a qualitative study. Pain Med. 2009;10(1):143–154. doi:10.1111/j.1526-4637.2008.00540.x
103. Samulowitz A, Gremyr I, Eriksson E, Hensing G. “Brave men” and “emotional women”: a theory-guided literature review on gender bias in health care and gendered norms towards patients with chronic pain. Pain Res Manag. 2018;2018:1–14. doi:10.1155/2018/6358624
104. Hoffmann DE, Tarzian AJ. The girl who cried pain: a bias against women in the treatment of pain. J Law Med Ethics. 2001;29(1):13–27. doi:10.1111/j.1748-720X.2001.tb00037.x
105. Prego-Jimenez S, Pereda-Pereda E, Perez-Tejada J, Aliri J, Goñi-Balentziaga O, Labaka A. The impact of sexism and gender stereotypes on the legitimization of women’s low back pain. Pain Manag Nurs. 2022;23(5):591–595. doi:10.1016/j.pmn.2022.03.008
106. Hoffman KM, Trawalter S, Axt JR, Oliver MN. Racial bias in pain assessment and treatment recommendations, and false beliefs about biological differences between blacks and whites. Proc Natl Acad Sci. 2016;113(16):4296–4301. doi:10.1073/pnas.1516047113
107. Morales ME, Yong RJ. Racial and ethnic disparities in the treatment of chronic pain. Pain Med. 2021;22(1):75–90. doi:10.1093/pm/pnaa427
108. Perugino F, De Angelis V, Pompili M, Martelletti P. Stigma and chronic pain. Pain Ther. 2022;11(4):1085–1094. doi:10.1007/s40122-022-00418-5
109. Janevic MR, Mathur VA, Booker SQ, et al. Making pain research more inclusive: why and how. J Pain. 2022;23(5):707–728. doi:10.1016/j.jpain.2021.10.004
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Subjective Sleep Disruption and Mood Disorders are Associated with the Risk of Chronic Pain in Patients with Obstructive Sleep Apnea
Liu L, Li X, Xue P, Wu M, Zeng S, Dai Y, Zhou J
Nature and Science of Sleep 2022, 14:2023-2032
Published Date: 7 November 2022
Factors Predicting Mental Health Among Women in Low-Income Communities of a Changing Society: A Mixed-Methods Study
Roberts LR, Sadan V, Siva R, Sathiyaseelan M, Rosalind SE, Suresh P, Montgomery SB
International Journal of Women's Health 2023, 15:381-394
Published Date: 16 March 2023
Research Trends of Acupuncture Therapy for Chronic Pain-Related Depression or Anxiety from 2003 to 2023: A Bibliometric Analysis
Yang P, Wang T, He YJ, Su SY
Journal of Pain Research 2023, 16:4301-4315
Published Date: 15 December 2023
Acceptance and Fear-Avoidance Mediate Outcomes of Interdisciplinary Pain Rehabilitation Programs at 12-Month Follow-Up: A Clinical Registry-Based Longitudinal Cohort Study from the Swedish Quality Registry for Pain Rehabilitation (SQRP)
Gerdle B, Dragioti E, Rivano Fischer M, Ringqvist Å
Journal of Pain Research 2024, 17:83-105
Published Date: 5 January 2024
Suicidal Ideation and Self-Injury in Trigeminal Neuralgia
Fishbein NS, Bakhshaie J, Greenberg J
Journal of Pain Research 2025, 18:2003-2010
Published Date: 12 April 2025