Back to Journals » Journal of Pain Research » Volume 18
Exploring Pain Clinical Specialists’ Perspectives on Opioid Optimization for Chronic Non-Malignant Pain in England
Authors Alenezi A, Paudyal V, Yahyouche A ![]()
Received 15 December 2024
Accepted for publication 29 June 2025
Published 13 August 2025 Volume 2025:18 Pages 4037—4051
DOI https://doi.org/10.2147/JPR.S512418
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Timothy Atkinson
Aziza Alenezi,1 Vibhu Paudyal,2 Asma Yahyouche3
1University Healthcare Center, Northern Border University, Arar, Saudi Arabia; 2Florence Nightingale Faculty of Nursing, Midwifery & Palliative Care, King’s College London, London, UK; 3School of Pharmacy, University of Birmingham, Birmingham, UK
Correspondence: Asma Yahyouche, Email [email protected]
Background: The use of opioids for chronic non-malignant pain (CNMP) offers limited efficacy and carries the potential for addiction. Healthcare professionals in both primary and secondary care settings face challenges when attempting to optimise opioid medications. There are limited studies that investigated the barriers and enablers to opioid reduction, cessation, and optimisation, specifically from a pain clinical specialist perspective.
Objective: This study explores pain clinical specialists’ views on challenges in opioid prescription management—including optimization and tapering—and their interactions with patients and prescribers.
Methods: Participants were recruited through pain clinic, webinars Email outreach, and professional networks. Semi-structured interviews were conducted using a guide based on the Theoretical Domains Framework (TDF) with 11 pain clinical specialists (8 consultants and 3 pharmacists) from NHS England, out of 15 participants who initially expressed interest, recruited via professional networks. Thematic analysis employed Framework Approach with dual coding.
Key Findings: Eleven participants, comprising eight pain doctors and three clinical pharmacists, provided insights. Analysis revealed four key findings: (1) A paradigm shift away from long-term opioid therapy due to concerns about dependency and inadequate pain relief; (2) Strong preference for multidisciplinary, personalized treatment approaches; (3) Significant system-level barriers including care fragmentation and inadequate consultation time; (4) Critical need for enhanced clinician training and patient education programs.
Conclusion: Optimizing opioid use for CNMP requires fundamental changes to current practice, including implementation of integrated care pathways, extended consultation times, and comprehensive education initiatives. These findings provide evidence-based recommendations for improving pain management while reducing inappropriate opioid prescribing.
Keywords: opioid, chronic non-malignant pain (CNMP), theoretical domains framework (TDF)
Background
Chronic non-malignant pain (CNMP) is defined by the International Association for the Study of Pain (IASP) as persistent pain lasting three months or longer, extending beyond the expected tissue healing period. Unlike cancer-related pain, CNMP typically originates from conditions such as fibromyalgia, osteoarthritis, or neuropathic disorders.1,2 In the USA, more than 70,000 deaths linked to opioid overdoses—emphasizing the critical need to better regulate opioid prescribing, especially for chronic pain cases.3 Conversely, evidence also suggests 44.5% of cancer patients still experiencing do not receive sufficient pain management, pointing to a dual challenge of over-prescription and under-treatment.4
In the United Kingdom (UK), over eight million individuals live with CNMP, with half experiencing depression and two-thirds unable to work.5,6 Research utilizing UK primary healthcare data via the Clinical Practice Research Datalink (CPRD) revealed a surge in strong opioid prescriptions for CNMP between 2000 and 2021.7 Tramadol’s reclassification as a Schedule 3 controlled drug in 2014 introduced stricter prescribing rules, which contributed to a noticeable decline in its use and helped curb the overall rise in opioid prescribing in the UK.5,8 For instance, a study by Chen et al reported a notable reduction in tramadol utilization and related mortality following the reclassification.8 Yet, concerns persist over prolonged opioid use, addiction, and related deaths.9 National Health Service (NHS) England reported a substantial drop in opioid prescriptions over four years, albeit with a rise in low-dose prescriptions, signaling ongoing concerns.10
In the context of CNMP, medication optimization is crucial, representing a person-centered approach to safe and effective medication use for optimal patient outcomes.11 Opioid dose optimization aims to achieve the maximum therapeutic benefit with the minimum effective opioid dose while minimizing risks and adverse effects. This involves preventing and mitigating problematic behavior related to opioid use, promoting adherence to prescribed regimens, and addressing issues like dose tapering or complete treatment cessation.12,13 Healthcare professionals are responsible for reassessing medication usage among patients with multi-morbidities, ensuring clinical appropriateness, effectiveness, and safety.11 This can be achieved through the understanding that opioid optimization is not a one-size-fits-all approach involving uniform reduction or cessation.
In the UK, General practitioner (GP)s serve as frontline providers for CNMP, conducting initial assessments and prescribing medications like non-opioids and mild opioids.14,15 When specialized care is needed, referrals to pain clinics staffed with multidisciplinary teams occur. These clinics offer advanced CNMP treatment and personalized plans, complementing primary care provided by GPs.16 Multidisciplinary Team (MDT) proves especially effective in patients using opioids to manage their CNMP, where coordinated care between prescribers, mental health specialists, and other healthcare providers support can safely reduce medication reliance while addressing underlying contributors to dependence.13
The involvement of multidisciplinary teams, including pain specialists, has been shown to be more effective in reducing opioid prescriptions and improving patient outcomes.13,17 Pain specialists play a vital role in addressing patients with multifaceted issues that cannot be managed effectively in primary care settings. Patients referred to pain specialists typically experience more severe pain, which might necessitate higher doses of opioids or present greater difficulty in reducing or stopping opioid use.18 Pain specialists tailor comprehensive treatment plans that address both the physical and psychological aspects of pain and opioid dependence, which are often intertwined in chronic pain patients.19
Exploring the perspectives of pain specialists is crucial because they possess in-depth knowledge and experience in managing complex pain cases. Their insights can inform better treatment protocols and policies aimed at optimizing pain management. Understanding their approaches and challenges can lead to improved patient care strategies and potentially reduce the incidence of opioid dependence and misuse.
Study Aim
This study aims to explore pain specialists’ perspectives on the challenges associated with optimizing, tapering or cessation of prescribed opioids, as well as their experiences in interacting with patients and fellow prescribers on opioid optimization and tapering.
Ethics Approval
Ethical approval for this study was granted by the Ethical Committee (Wales REC 3), with REC reference: 20/WA/0232, Protocol number: RG_19-160 and IRAS project ID: 270017. Written informed consent was obtained from all participants included in the study. Written informed consent was obtained from all participants, including permission to publish anonymized responses and direct quotes.
Method
Study Design and Conceptual Framework The study utilized the Theoretical Domains Framework (TDF) Version 2 to guide the interviews and analyze data. TDF integrates 128 constructs from 33 behavior and behavioral change theories into 14 distinct domains, providing a robust tool for eliciting a comprehensive set of beliefs and facilitating detailed behavioral analysis 16,19–21 see Table 1. The study design adhered to the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist to ensure comprehensive and transparent reporting.22 See appendix.
 |
Table 1 Mapping of Interview Schedule of TDF Domains |
Inclusion Criteria
Participants were healthcare professionals (doctors, nurses, pharmacists, physiotherapists, psychiatrists) with at least one year of experience in pain management clinics in England, proficient in English, and aged 18 or older. To ensure a diverse sample of pain management professionals and maximize the variety of views and experiences, the study team employed several recruitment strategies targeting these professionals.23,24
Recruitment Methods
Three distinct methods were used to enhance participant numbers and recruit a variety of pain specialists. The first method involved collaboration with a pain clinic in the West Midlands, employing two pain doctors, two nurses, two physiotherapists, and one psychologist. Despite initial interest, participation was hindered by the timing of data collection, coinciding with the onset of lockdown, resulting in lost connections and lack of consent. The second method used a webinar on low back pain hosted by an academic center in the Northwest of England, attended by 93 pain doctors. This approach effectively reached a good number of doctors, reflecting the webinar’s targeted audience. The third recruitment strategy involved sending emails about the study through a major pharmacy chain in the UK, with invitations disseminated to pain pharmacists via research team acquaintances. Efforts to recruit additional healthcare professionals like nurses, physiotherapists, and psychologists were less fruitful, highlighting a gap in available channels for reaching these specialists in pain management. The participants received the study package electronically, which included detailed information about the researcher, her background, and the purpose of the study, allowing them to understand all relevant aspects before participating.
Data Collection
In-depth interviews were conducted to explore pain specialists’ perceptions of opioid optimization for chronic non-malignant pain (CNMP) and solicit suggestions for interventions and strategies to improve opioid use among these patients.25,26 The interview questions were designed based on a comprehensive review of relevant literature,27–29 and insights from the study team’s prior research.13,27 Each question was tailored to address specific TDF domains, with open-ended questions and standardized prompts to ensure thorough exploration. Data collection was conducted from February to August 2021 through semi-structured interviews. Interviews were conducted via telephone from the researcher’s home, adapted to be a quiet environment suitable for high-quality audio recording, in response to the COVID-19 lockdown restrictions. Only the researcher (AA) and the participants were present during the interviews; no one else attended. Each session lasted between 25 and 45 minutes and was audio-recorded for verbatim transcription. No follow-up interviews were conducted due to the attainment of thematic saturation, where no new themes or significant alterations in codes were identified after analyzing the last two interviews.30
Data Analysis
Interviews were recorded on password-protected and encrypted devices to ensure data privacy and security, strictly adhering to the Data Protection Act 2018 (UK Government, 2018).31 The recordings were transcribed verbatim by AA, who removed any identifying information to preserve participant confidentiality. The anonymized transcripts were subsequently imported into a Microsoft Word table for thorough analysis, employing both deductive and inductive methods to deepen the exploration of pain specialists’ perspectives on opioid optimization. Transcripts were not returned to participants for comments or corrections. The thematic analysis commenced with open coding of each transcript line by line, creating code components that were then compared and grouped into categories and themes related to pain specialists’ perceptions of opioid optimization for CNMP patients.32,33 Each code was then classified under TDF domains to understand which themes were predominantly influenced by which domains.34
Research Trustworthiness
AA conducted this study as part of her doctoral research at the University of Birmingham, where she received formal training in qualitative research methodologies, adhering to Lincoln and Guba’s principles of trustworthiness – including credibility, transferability, dependability, and confirmability.35 Credibility was enhanced by employing recognized research methods that have been validated in comparable studies.36 Regular discussions about data analysis and coding in research team meetings further supported the study’s credibility and dependability. Transferability was facilitated by detailed documentation of the findings, supported by direct quotes from interviews, allowing others to evaluate the applicability of the results to other contexts.
Result
Fifteen participants contacted the researcher, but only 11 participants, consisting of 8 pain and anesthesia doctors and 3 clinical pharmacists. See Figure 1.
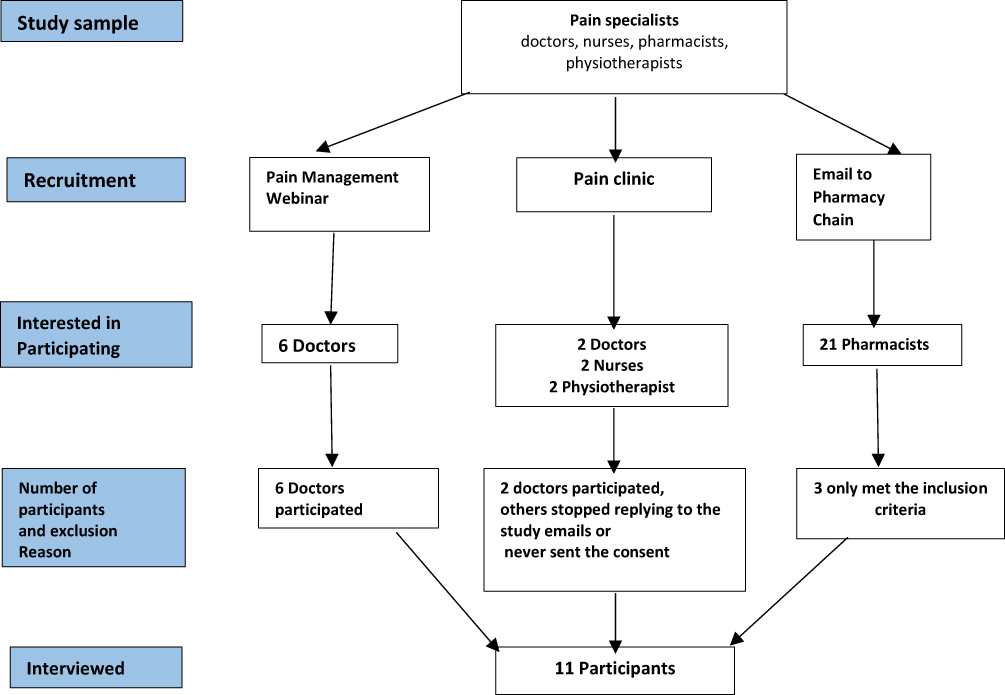 |
Figure 1 Flowchart of the Study Sample Selection Process. |
The study involved 11 participants, consisting of 8 pain and anesthesia doctors and 3 clinical pharmacists. The doctors were distributed across Birmingham (3), Manchester (2), Hull (1), Wakefield (1), and Brierley Hill (1). All 8 doctors were male. In terms of age distribution, 1 doctor was between 25 and 35 years old, 5 were between 36 and 45 years old, and 2 were between 46 and 60 years old. Their experience in chronic pain management varied, with 1 having 1–5 years of experience, 1 having 6–10 years, 4 having 11–15 years, and 2 having over 20 years of experience.
The pharmacists were located in London (1), Coventry (1), and Hull (1). All 3 pharmacists were male. Two pharmacists were aged between 36 and 45 years, and one was aged between 25 and 35 years. In terms of experience in chronic pain management, one pharmacist had 1–5 years of experience, and two had 6–10 years.
The study systematically organizes its findings into themes, each aligned with the Theoretical Domains Framework (TDF), to explore the complexities of opioid management. The theme “Self-Perception and Evolving Trends in Opioid Optimization” is illuminated through quotes under the TDF domains of Knowledge, Professional Role and Identity, and Belief about Consequences, highlighting shifts in self-perception and professional practice. The “Embracing Advanced Approaches in CNMP Management” theme is tied to the TDF domains of Knowledge and Professional Role and Identity, advocating for personalized treatment strategies. The “Opioid Suboptimal Use and Optimization Complexity” theme, linked to the Environmental Context and Resources domain, emphasizes the need for enhanced resources. Lastly, the “Recommended Strategies for Opioid Optimization” theme is associated with the Behavioral Regulation and Environmental Context and Resources domains, underscoring strategies to improve opioid management practices. See Table 2
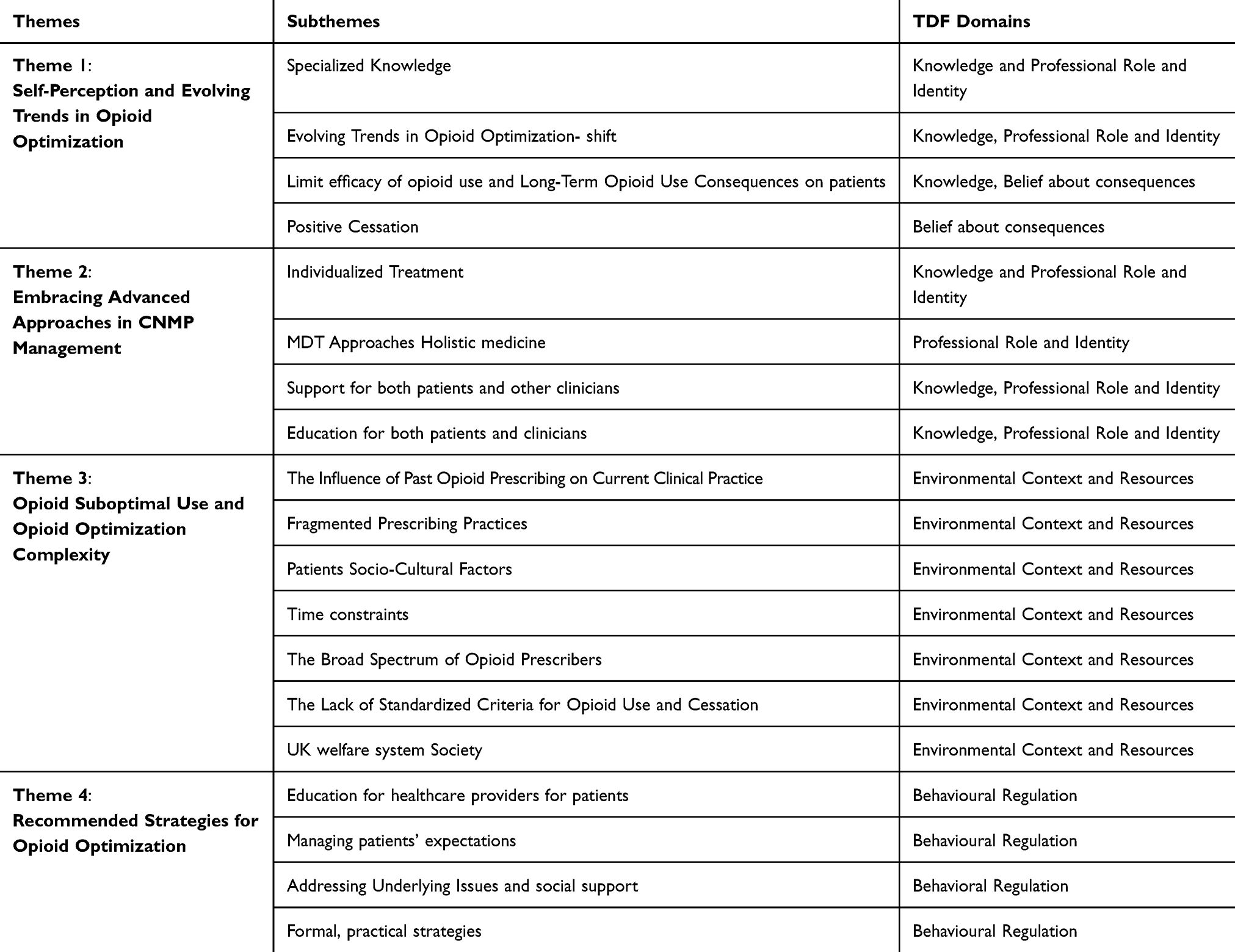 |
Table 2 The Themes Map |
Theme 1: Self-Perception and Evolving Trends in Opioid Optimization
The first theme, Self-Perception and Evolving Trends in Opioid Optimization, examines how pain specialists perceive their roles and the knowledge they apply to opioid management, highlighting a shift in opioid optimization perspectives and practices. Subthemes include Specialized Knowledge, Evolving Trends in Opioid Optimization, Limited Efficacy of Opioid Use, and Long-Term Consequences of Opioid Use on patients, all emphasizing the need for a deep understanding of both professional roles and the outcomes of opioid use. (See Table 3).
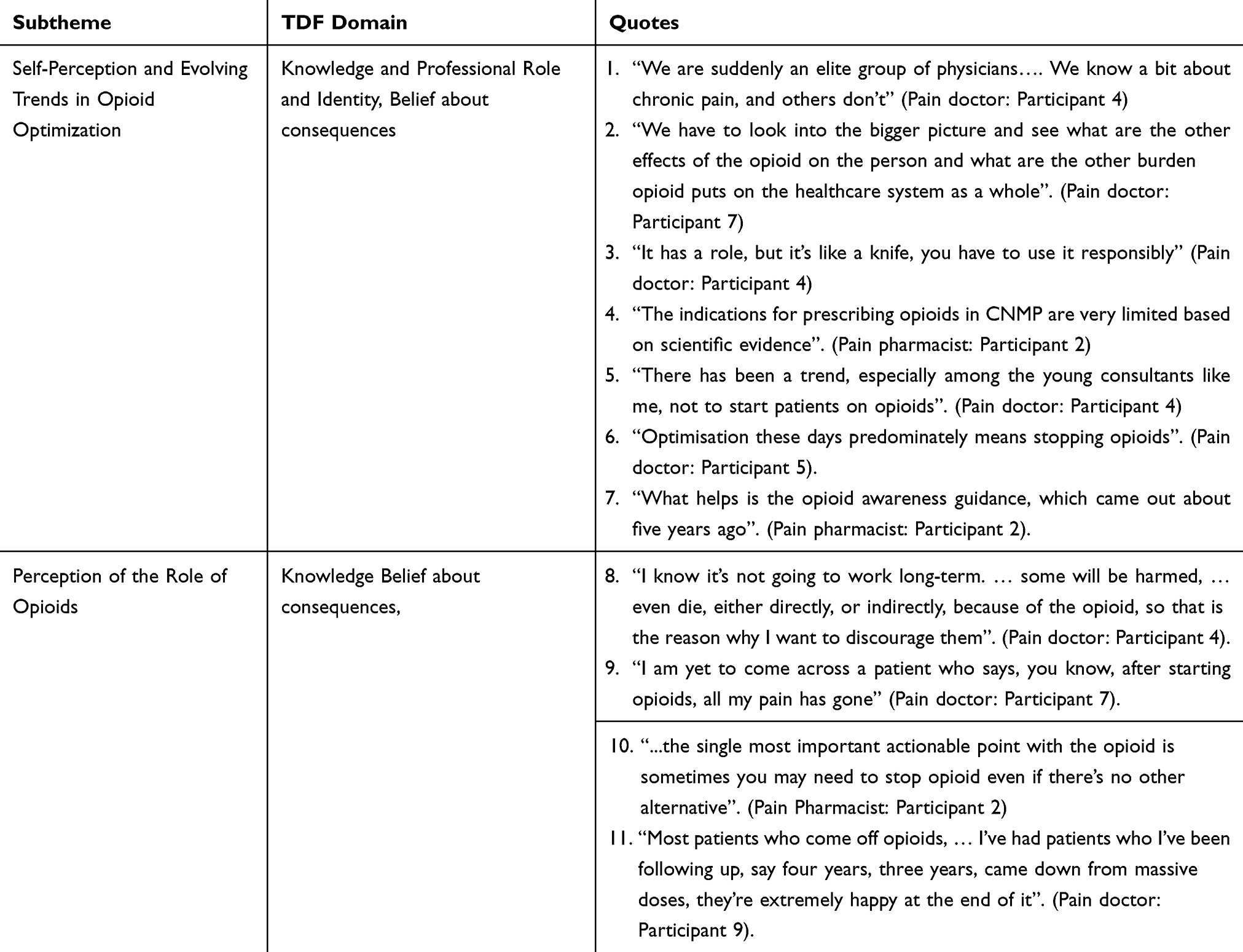 |
Table 3 Self-Perception and Evolving Trends in Opioid Optimization |
Specialized Knowledge and Evolving Trends in Opioid Optimization
Pain specialists consider themselves uniquely equipped to manage chronic pain complexities, setting their expertise apart from other providers. This self-perception is rooted in their extensive and up-to-date specialized knowledge and experience. They view themselves as an elite group of physicians with a deeper understanding of chronic pain (Table 3, Quote 1).
Additionally, they perceive themselves as guardians of patient safety and society, influencing their prescribing practices. Pain specialists emphasize the need to evaluate the broader effects of opioid therapy on both patients and the healthcare system (Table 3, Quote 2). While acknowledging that opioids have a role in pain management, they stress the importance of using them responsibly to ensure that the benefits outweigh potential harms (Table 3, Quote 3).
Perceived Role of Opioids in Chronic Non-Malignant Pain (CNMP)
Pain specialists perceive that opioids have a limited role in CNMP. They generally approach opioid use with caution and skepticism, rooted in awareness of the risks associated with prolonged use. Consequently, they minimize opioid prescriptions, particularly for non-cancer patients, and express hesitation in endorsing their long-term use (Table 3, Quote 4).
Many specialists, particularly younger consultants, are moving away from initiating long-term opioid therapy for CNMP due to recognized risks and limited efficacy (Table 3, Quotes 5–6). This shift is supported by updated opioid awareness guidelines and national directives, which promote safer prescribing practices. The focus is now on optimizing pain management through alternative methods, emphasizing evidence-based and patient-centered care to reduce dependency (Table 3, Quote 7).
Participants highlight risks associated with long-term opioid therapy, including immune system impairment, sexual dysfunction, and problematic behaviors (Table 3, Quote 8). They also note that opioids frequently fail to provide complete pain relief (Table 3, Quote 9). Many advocates for tapering and cessation, observing that patients who discontinue opioid therapy often experience improved quality of life and greater satisfaction with their pain management. (Table 3, Quotes 10–11).
Theme 2: Embracing Advanced Approaches in CNMP Management
The second theme, Embracing Advanced Approaches in CNMP Management, focuses on personalized and multidisciplinary strategies to enhance support and education for patients and clinicians. Subthemes include Individualized Treatment, MDT Approaches to Holistic Medicine, and Education for Patients and Clinicians, stressing the importance of knowledge and professional identity in effective pain management. (See Table 4).
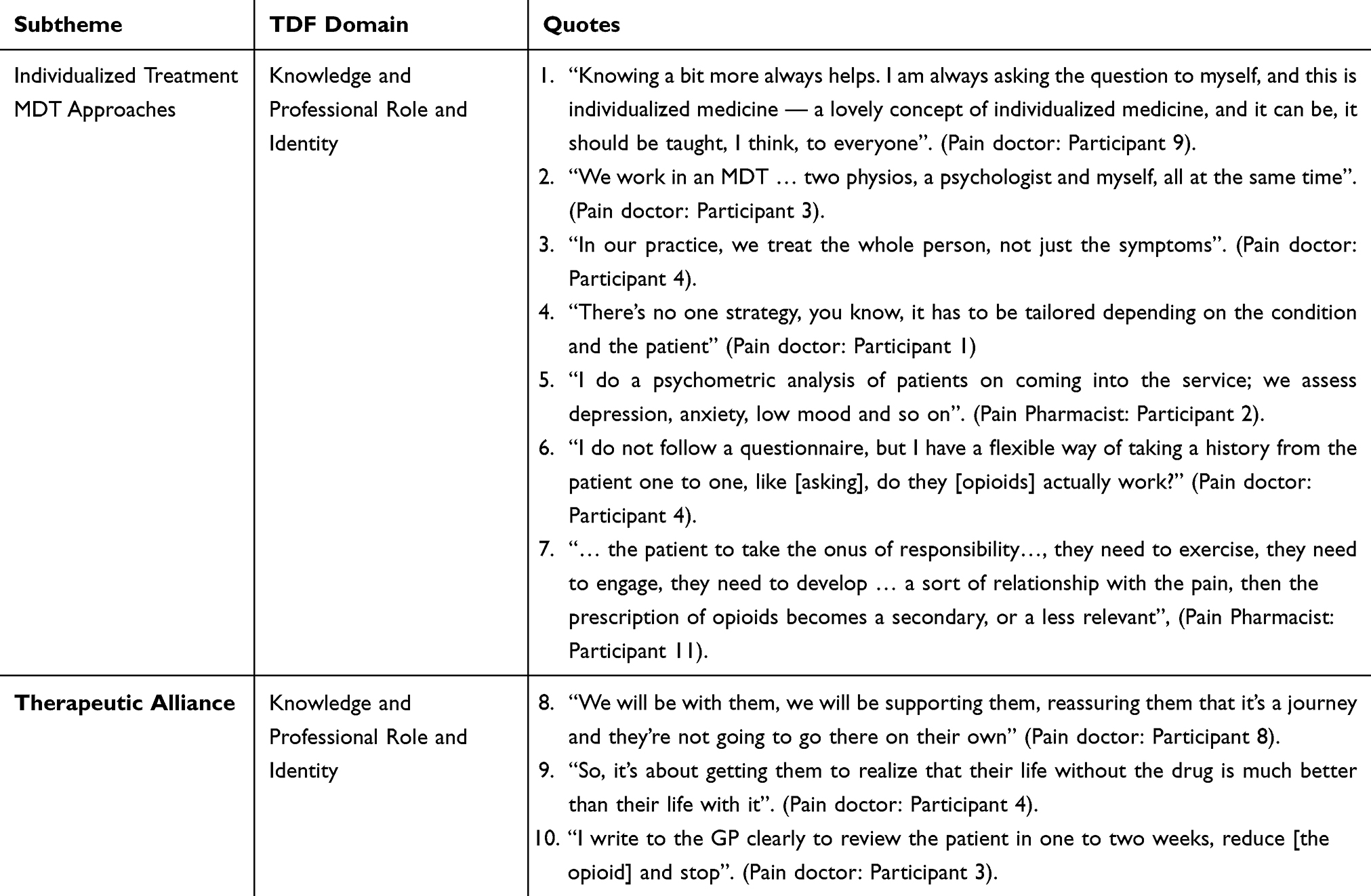 |
Table 4 Embracing Advanced Approaches in CNMP Management |
Individualized Treatment and MDT Approaches
Pain specialists adopt advanced multimodal approaches based on personalized medicine, incorporating non-pharmacological methods aligned with National Institute for Health and Care Excellence (NICE) guidelines (Table 4, Quotes 1–2). They emphasize tailoring interventions to patients’ unique medical histories and continuously assessing responses (Table 4, Quote 3).
While some specialists use standardized assessments, others prefer flexible, one-on-one discussions to gather necessary information for tailored treatment (Table 4, Quotes 4–5). Participants also stress patient responsibility, encouraging active engagement in therapies such as exercise, psychological support, and physiotherapy (Table 4, Quote 6).
Therapeutic Alliance
Assessment and review form the basis of a therapeutic alliance, where specialists build trust, provide information, and support patients through treatment adjustments. They advocate for reducing medication reliance and reassure patients they are not alone in managing opioid cessation and pain (Table 4, Quotes 7).
Specialists also support other healthcare providers, ensuring clear communication with general practitioners (GPs) on tapering strategies. This collaborative approach extends their advanced management strategies beyond the clinic (Table 4, Quote 9).
Theme 3: Opioid Suboptimal Use and Optimization Complexity
The third theme, Opioid Suboptimal Use and Optimization Complexity, addresses systemic factors influencing opioid prescribing, highlighting the need for improved resources and standardized practices. Subthemes include Influence of Past Prescribing on Current Practice, Fragmented Prescribing Practices, Patients’ Socio-Cultural Factors, Time Constraints, and Broad Spectrum of Opioid Prescribers, categorized under Environmental Context and Resources. (See Table 5).
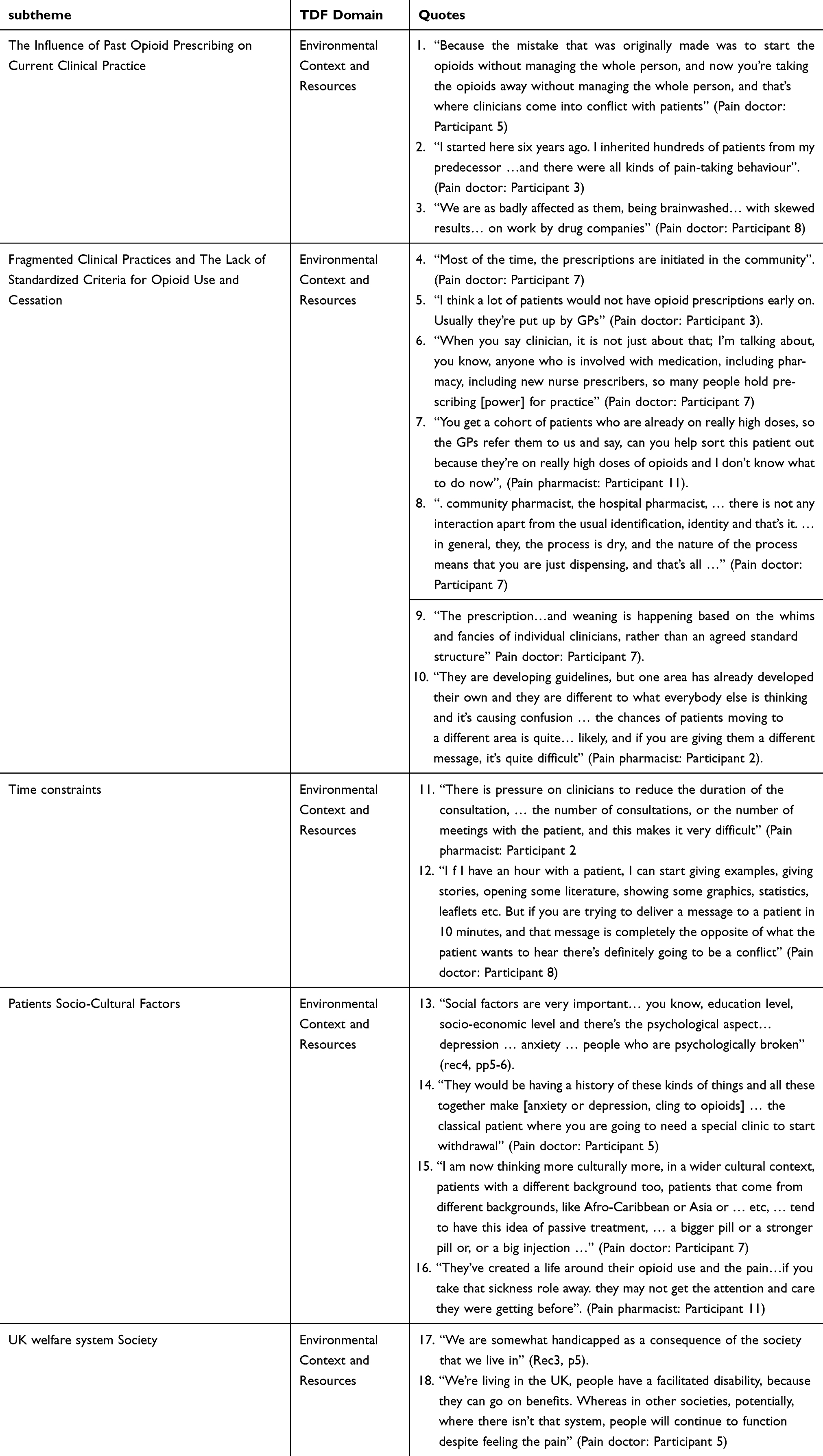 |
Table 5 Opioid Suboptimal Use and Opioid Optimization Complexity |
Influence of Past Opioid Prescribing on Current Practice
Past prescribing practices have led to significant challenges. Specialists note conflicts when opioids are withdrawn without addressing broader patient well-being (Table 5, Quote 1). Many patients were placed on high-dose or long-term opioids by previous clinicians, exacerbating dependency issues (Table 5, Quote 2). Aggressive pharmaceutical marketing further contributed to overprescription, spreading misinformation (Table 5, Quote 3).
Fragmented Clinical Practices and Lack of Standardized Criteria
Efforts to optimize opioid use are hindered by fragmented practices and inconsistent guidelines. Decisions often rely on individual judgment rather than evidence-based protocols, leading to variability in care (Table 5, Quotes 4–5). Poor coordination between GPs, specialists, and pharmacists complicates tapering (Table 5, Quotes 6–7).
The absence of standardized criteria for opioid initiation, tapering, or cessation creates confusion, particularly when patients relocate and encounter differing regional practices (Table 5, Quotes 8–9). Specialists advocate for cohesive, evidence-based guidelines to improve outcomes (Table 5, Quotes 10–11).
Time Pressures
Systemic constraints, particularly limited consultation times (10–15 minutes), hinder thorough patient education and monitoring (Table 5, Quotes 12–13).
Patients’ Socio-Cultural Factors
Socio-cultural factors, such as education level, socio-economic status, and mental health conditions, influence opioid reliance (Table 5, Quotes 14–15). A passive patient mindset, where individuals expect “quick fixes”, complicates optimization (Table 5, Quotes 16–17).
UK Welfare System
Some specialists attribute passive attitudes to the UK welfare system, which medicalizes common issues and facilitates dependency, contrasting with societies lacking such systems (Table 5, Quotes 18–19).
Theme 4: Recommended Strategies for Opioid Optimization
The fourth theme, Recommended Strategies for Opioid Optimization, proposes practical enhancements for opioid management, categorized under Behavioral Regulation. (See Table 6).
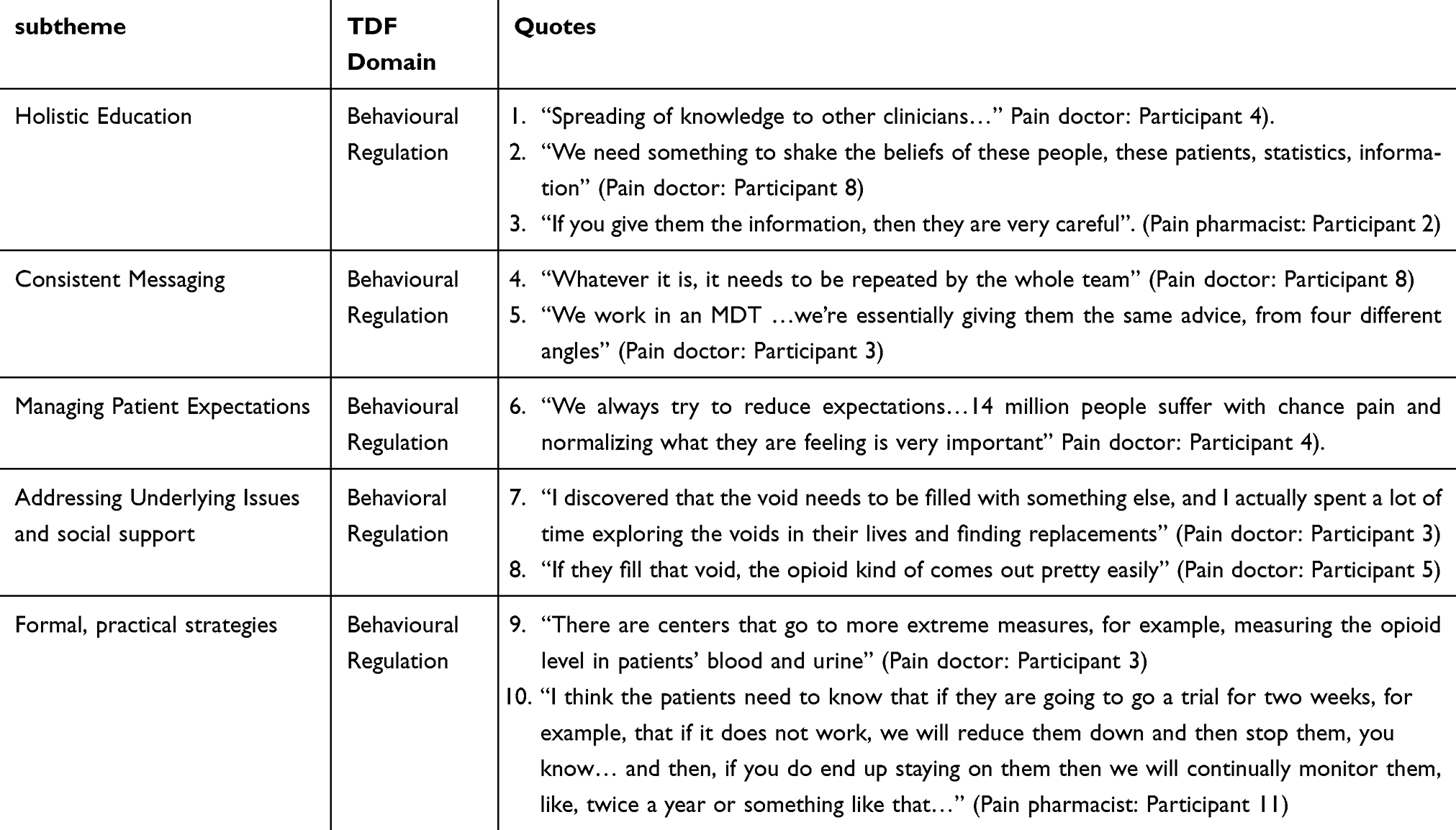 |
Table 6 Recommended Strategies for Opioid Optimization |
Education
Educating patients and clinicians about opioid risks and limited efficacy is critical (Table 6, Quotes 1–3).
Consistent Messaging
Coordinated messaging across multidisciplinary teams (MDTs) improves optimization success (Table 6, Quotes 4–5).
Managing Expectations
Setting realistic expectations about chronic pain and treatment alternatives reduces opioid reliance (Table 6, Quote 6).
Social and Emotional Support
Addressing mental health and social disadvantages helps patients transition from opioid dependence (Table 6, Quotes 7–8).
Formal, Practical Strategies
Suggested measures include national opioid registries, regular drug testing, and patient-prescriber contracts to ensure compliance (Table 6, Quotes 9–10).
Discussion
This study investigates UK pain specialists’ perspectives on opioid optimization for CNMP. The insights gathered highlight the importance of a balanced approach that considers both the therapeutic benefits and potential risks associated with long-term opioid therapy.
A key theme that emerged is self-perception and evolving trends in opioid optimization, where participants expressed confidence and pride in their management of CNMP. They emphasized that their extensive training and clinical experience significantly influence their decisions regarding opioid prescriptions. Pain specialists embraced an advanced approach that focuses on addressing patients’ needs and adjusting opioid prescriptions based on comprehensive assessments of physical, psychological, and emotional factors.37 They advocate for personalized and multidisciplinary approaches to pain management, emphasizing individualized treatment plans that incorporate non-pharmacological methods and adhere to NICE guidelines. This approach is consistent with literature emphasizing the need for ongoing risk-benefit analyses and recognizing the limited efficacy of opioids in managing CNMP.13
Pain specialists viewed the long-term opioid to have little benefit in the treatment of CNMP and are associated with significant side effects and use it only for limited cases after a comprehensive assessment.38 This perspective aligns with the findings many studies, where GPs and pain specialists also considered opioids as a last resort for CNMP management.17,26 Pain specialists’ viewpoints are based on scientific evidence and clinical experience to guide opioid use in CNMP. Studies show limited long-term benefits but significant risks—addiction, overdose, and functional decline.39 A prospective study involving 45 patients undergoing elective detoxification from prescription opioids found that 83.3% of participants reported enhanced overall health status six months post-detoxification. Additionally, 97.7% experienced a significant reduction in pain levels, with an average decrease of 4.51 points on the Visual Analogue Scale (VAS).40
Another theme focused on the impact of past suboptimal opioid prescribing and the complexities of treating CNMP, especially for patients with psychological issues. Challenges such as the involvement of multiple prescribers without cohesive criteria lead to inconsistent patient care. Fragmented prescribing practices, a lack of standardized guidelines, and system fragmentation, as well as inconsistent clinical decisions and poor coordination between general practice, specialist hospitals, and other services, hinder CNMP patient care. These issues, documented in UK healthcare literature, predominantly affect those with complex bio-psychosocial needs.41
One of the challenges highlighted in this study is the knowledge gap among GPs and other healthcare professionals regarding CNMP and opioid optimization in handling complex cases. This finding aligns with studies from the UK and USA, which revealed that GPs and primary care providers often felt helpless and dissatisfied with their ability to manage chronic pain patients.28 This lack of confidence may be due to insufficient CNMP education and training in undergraduate medical school, as highlighted in research from Europe and the USA.28 Meanwhile, pharmacists in this study are viewed as underutilized, with their role often limited to medication dispensing. Community pharmacists in Alenezi et al mentioned that, despite their efforts to communicate prescription concerns to doctors, they rarely receive responses.29
The final theme addressed strategies recommended by participants to optimize opioid use for CNMP patients, advocating for a more nuanced and patient-centered approach. They stressed the importance of providing comprehensive education to healthcare providers, patients, and stakeholders to improve understanding and management of opioid use in CNMP. Enhanced ongoing education for healthcare professionals is crucial to address knowledge gaps in pain management. Also, effective pain education for patients can reduce anxiety, misuse of medications, and enhance patient satisfaction.42,43 Another strategy recommended by the pain specialists are managing patients’ expectations. Studies report that patients often expect complete relief from pain, while in reality, most pain interventions, including opioids, reduce pain by about 30% on average.44,45 Patients often express dissatisfaction when their expectations are unmet, underscoring the importance of managing them. Managing patient expectations and providing social and emotional support are crucial components of effective optimization strategies.44
Limitations
This study had several limitations. The relatively small sample size means the findings might not reflect the full range of experiences or views in the wider population. Future research involving a larger and more varied group would help strengthen and build on these results. Additionally, the study consisted exclusively of men, which may limit the generalizability of the findings.
Implications for Practice
The findings of this study have several implications for clinical practice. Enhancing collaboration among health professionals, including GPs, pain specialists, and clinical pharmacists, is essential for optimizing opioid use. This can be achieved by developing specific guidelines to facilitate effective communication among all professionals involved in the treatment and follow-up of patients.46 Despite the study’s limitations, it underscores the need for ongoing education and training for healthcare professionals, ensuring they are well-informed about the latest guidelines and best practices to enhance the safety and efficacy of opioid use in chronic pain management.
The importance of a multidisciplinary approach to pain management is highlighted. Healthcare providers should collaborate closely within MDTs to deliver consistent messages and comprehensive care plans to patients. This collaborative approach can address fragmented opioid prescribing practices and improve patient outcomes.
Further Research
Future research should include a larger and more diverse sample of healthcare professionals, exploring the perspectives of female pain specialists and pharmacists, as well as other healthcare providers involved in opioid optimization. Further studies should investigate patient-centered care and education for both healthcare providers and patients about prescribed opioids for CNMP. Enhanced collaboration among healthcare professionals in assessing and supporting patients, and developing interventions based on the perspectives of CNMP patients and all involved healthcare providers, is necessary. Understanding patients’ perceptions and preferences regarding advice from different practitioners, such as GPs versus pain specialists, is also essential.
Conclusion
This study provides insights into UK pain specialists’ perspectives on opioid optimization for CNMP. The findings emphasize the importance of personalized and multidisciplinary approaches, specialized knowledge, and a cautious approach to opioid prescribing. Addressing the challenges of fragmented care and ensuring ongoing education and collaboration among healthcare providers can enhance the optimization of opioid use and improve patient outcomes.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Acknowledgments
We would like to acknowledge the University of Birmingham. The funder had no role in the design and conduct of the research and the interpretation of the data generated.
The authors extend their appreciation to the Deanship of Scientific Research at Northern Border University, Arar, KSA.
Funding
This work was funded by the university of Birmingham. AA was sponsored for her PhD by the Royal Embassy of Saudi Arabia, Cultural Bureau in London.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Treede RD. The international association for the study of pain definition of pain: as valid in 2018 as in 1979, but in need of regularly updated footnotes. Pain Rep. 2018;3(2):e643. doi:10.1097/PR9.0000000000000643
2. Nicholas M, Vlaeyen JWS, Rief W, et al. The IASP classification of chronic pain for ICD-11: chronic primary pain. Pain. 2019;160(1):28–37. doi:10.1097/j.pain.0000000000001390
3. Centers for Disease Control and Prevention. U.S. overdose deaths in 2021 increased half as much as in 2020 – but are still up 15% [Internet]. 2022. Available from: https://www.cdc.gov/nchs/pressroom/nchs_press_releases/2022/202205.htm.
4. Snijders RA, Brom L, Theunissen M, van den Beuken-van Everdingen MH. Update on prevalence of pain in patients with cancer 2022: a systematic literature review and meta-analysis. Cancers. 2023;15(3):591. doi:10.3390/cancers15030591
5. British Pain Society. British pain society press release: chronic pain costs the UK £billions but research funding is inadequate. 2021. Available from: https://www.britishpainsociety.org/mediacentre/news/british-pain-society-press-release-chronic-pain-costs-the-uk-billions-but-research-funding-is-inadequate/.
6. National Institute for Health and Care Excellence. Chronic pain: assessment and management. 2018. Available from: https://www.nice.org.uk/guidance/gid-ng10069/documents/final-scope.
7. Zin CS, Chen LC, Knaggs RD. Changes in trends and pattern of strong opioid prescribing in primary care. Eur J Pain. 2014;18(9):1343–1351. doi:10.1002/j.1532-2149.2014.496.x
8. Chen TC, Chen LC, Knaggs RD. A 15-year overview of increasing tramadol utilisation and associated mortality and the impact of tramadol classification in the United Kingdom. Pharmacoepidemiol Drug Saf. 2018;27(5):487–494. doi:10.1002/pds.4320
9. Taylor S, Annand F, Burkinshaw P, et al. Dependence and withdrawal associated with some prescribed medicines: an evidence review. London: Public Health England; 2019.
10. NHS England. Optimising personalised care for adults prescribed medicines associated with dependence or withdrawal symptoms: framework for action for integrated care boards (ICBs) and primary care. 2023. Available from: https://www.england.nhs.uk/long-read/optimising-personalised-care-for-adults-prescribed-medicines-associated-with-dependence-or-withdrawal-symptoms/.
11. National Institute for Health and Care Excellence. Medicines optimisation: the safe and effective use of medicines to enable the best possible outcomes. 2015. Available from: https://www.nice.org.uk/guidance/ng5/resources/medicines-optimisation-the-safe-and-effective-use-of-medicines-to-enable-the-best-possible-outcomes-pdf-51041805253.
12. Timmerman L, Stronks DL, Groeneweg JG, et al. Prevalence and determinants of medication non-adherence in chronic pain patients: a systematic review. Acta Anaesthesiol Scand. 2016;60(4):416–431. doi:10.1111/aas.12697
13. Alenezi A, Yahyouche A, Paudyal V. Interventions to optimise prescribed medicines and reduce their misuse in chronic non-malignant pain: a systematic review. Eur J Clin Pharmacol. 2021;77(4):467–490. doi:10.1007/s00228-020-03026-4
14. The King’s Fund. How is the NHS structured? The NHS: how providers are regulated and commissioned. 2021. Available from: https://www.kingsfund.org.uk/audio-video/how-is-nhs-structured-funding-flow.
15. NHS England. Domain 2: enhancing quality of life for patients with long-term conditions. Resources for CCGs [Internet]. 2021. Available from: https://www.england.nhs.uk/ourwork/clinical-policy/ltc/resources-for-long-term-conditions.
16. Price CM. The development of methods to assess the quality of care in pain clinics in England and Wales [dissertation]. Southampton: University of Southampton; date unknown.
17. Seangrung R, Tempeetikul T, Pannarunothai S, et al. Perspectives of pain specialists, patients, and family members on long-term opioid use for chronic non-cancer pain: a qualitative study. BMC Anesthesiol. 2021;21(1):275. doi:10.1186/s12871-021-01501-8
18. Brinksman S. Opioids and chronic pain in primary care. Br J Gen Pract. 2018;68(669):454. doi:10.3399/bjgp18X698921
19. Cane J, O’Connor D, Michie S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement Sci. 2012;7(1):37. doi:10.1186/1748-5908-7-37
20. Michie S, Johnston M, Abraham C, et al. Making psychological theory useful for implementing evidence-based practice: a consensus approach. BMJ Qual Saf. 2005;14(1):26–33. doi:10.1136/qshc.2004.011155
21. Atkins L, Francis J, Islam R, et al. A guide to using the theoretical domains framework of behaviour change to investigate implementation problems. Implement Sci. 2017;12(1):77. doi:10.1186/s13012-017-0605-9
22. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
23. Robinson OC. Sampling in interview-based qualitative research: a theoretical and practical guide. Qual Res Psychol. 2014;11(1):25–41. doi:10.1080/14780887.2013.801543
24. Boddy CR. Sample size for qualitative research. Qual Market Res. 2016;19(4):426–432. doi:10.1108/QMR-06-2016-0053
25. Kahlke RM. Generic qualitative approaches: pitfalls and benefits of methodological mixology. Int J Qual Methods. 2014;13(1):37–52. doi:10.1177/160940691401300119
26. Kennedy MC, Henman MC, Cousins G. General practitioners and chronic non-malignant pain management in older patients: a qualitative study. Pharmacy. 2016;4(1):15. doi:10.3390/pharmacy4010015
27. Cross AJ, Buchbinder R, Mathieson S, et al. Barriers and enablers to monitoring and deprescribing opioid analgesics for chronic non-cancer pain: a systematic review with qualitative evidence synthesis using the theoretical domains framework. BMJ Qual Saf. 2022;31(5):387–400. doi:10.1136/bmjqs-2021-014186
28. McCrorie C, Closs SJ, House A, et al. Understanding long-term opioid prescribing for non-cancer pain in primary care: a qualitative study. BMC Fam Pract. 2015;16(1):121. doi:10.1186/s12875-015-0335-5
29. Alenezi A, Yahyouche A, Paudyal V. Roles, barriers and behavioral determinants related to community pharmacists’ involvement in optimizing opioid therapy for chronic pain: a qualitative study. Int J Clin Pharm. 2022;44(1):163–179. doi:10.1007/s11096-021-01331-1
30. Saunders B, Sim J, Kingstone T, et al. Saturation in qualitative research: exploring its conceptualization and operationalization. Qual Quantity. 2018;52(4):1893–1907. doi:10.1007/s11135-017-0574-8
31. UK Government. Data protection act 2018. 2018. Available from: https://www.legislation.gov.uk/ukpga/2018/12/contents/enacted.
32. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
33. Thomas DR. A general inductive approach for analyzing qualitative evaluation data. Am J Eval. 2006;27(2):237–246. doi:10.1177/1098214005283748
34. Francis JJ, Stockton C, Eccles MP, et al. Evidence-based selection of theories for designing behaviour change interventions: using methods based on theoretical construct domains to understand clinicians’ blood transfusion behaviour. British J Health Psychol. 2009;14(4):625–646. doi:10.1348/135910709X467666
35. Lincoln YS, Guba EG. But is it rigorous? Trustworthiness and authenticity in naturalistic evaluation. New Directions Program Eval. 1986;1986(30):73–84. doi:10.1002/ev.1427
36. Shenton AK. Strategies for ensuring trustworthiness in qualitative research projects. Educ Inf. 2004;22(2):63–75. doi:10.3233/EFI-2004-22201
37. Gatchel RJ, Peng YB, Peters ML, Fuchs PN, Turk DC. The biopsychosocial approach to chronic pain: scientific advances and future directions. Psychol Bull. 2007;133(4):581–624. doi:10.1037/0033-2909.133.4.581
38. Frieden TR, Houry D. Reducing the risks of relief — the CDC opioid-prescribing guideline. N Engl J Med. 2016;374(16):1501–1504. doi:10.1056/NEJMp1602369
39. Chou R, Turner JA, Devine EB, et al. The effectiveness and risks of long-term opioid therapy for chronic pain: a systematic review for a national institutes of health pathways to prevention workshop. Ann Internal Med. 2015;162(4):276–286. doi:10.7326/M14-2559
40. Laubner Sakalauskienė G, Stražnickaitė I, Miškinytė S, Zdanavičius L, Šipylaitė J, Badaras R. Impact of prescription opioid detoxification on quality of life and pain levels. Clinics Pract. 2024;14(4):1529–1537. doi:10.3390/clinpract14040114
41. Jerjes W. Enhancing medication adherence through interprofessional collaboration: insights from the UK experience. J Gen Intern Med. 2024;40(2):489–490. doi:10.1007/s11606-024-09137-3
42. Moffat AK, Apajee J, Le Blanc VT, et al. Reducing opioid use for chronic non-cancer pain in primary care using an evidence-based, theory-informed, multistrategic, multistakeholder approach: a single-arm time series with segmented regression. BMJ Qual Saf. 2024;32(11):623–633. doi:10.1136/bmjqs-2023-015923
43. Marris D, Theophanous K, Cabezon P, Dunlap Z, Donaldson M. The impact of combining pain education strategies with physical therapy interventions for patients with chronic pain: a systematic review and meta-analysis of randomized controlled trials. Physiother Theory Pract. 2019;37(4):461–472. doi:10.1080/09593985.2019.1633714
44. Alenezi A, Yahyouche A, Paudyal V. Patient perspectives on the appropriate use of prescribed opioids in chronic non-malignant pain: analysis of online forums using theoretical domains framework. J Pain Res. 2022;15:1567–1583. doi:10.2147/JPR.S357354
45. Busse JW, Wang L, Kamaleldin M, et al. Opioids for chronic noncancer pain: a systematic review and meta-analysis. JAMA. 2018;320(23):2448–2460. doi:10.1001/jama.2018.18472
46. Thakur T, Frey M, Chewning B. Communication between patients and health care professionals about opioid medications. Exploratory Res Clin Soc Pharm. 2021;2:100030. doi:10.1016/j.rcsop.2021.100030
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cohort Description: Preventing an Opioid Epidemic in Norway – Focusing on Treatment of Chronic Pain (POINT) – A National Registry-Based Study
Hamina A, Odsbu I, Borchgrevink PC, Chen LC, Clausen T, Espnes KA, Gjesdal K, Handal M, Hartikainen S, Hjellvik V, Holter MTS, Høibø T, Kurita GP, Langaas HC, Lid TG, Nøst TH, Sjøgren P, Skurtveit S
Clinical Epidemiology 2022, 14:1477-1486
Published Date: 8 December 2022
Tapentadol: A Review of Experimental Pharmacology Studies, Clinical Trials, and Recent Findings
Alshehri FS
Drug Design, Development and Therapy 2023, 17:851-861
Published Date: 21 March 2023
A Randomized, Double-Blind, Placebo-Controlled Trial to Evaluate the Therapeutic Effect of Magnesium-L-Threonate Supplementation for Persistent Pain After Breast Cancer Surgery
Ni Y, Deng F, Yu S, Zhang J, Zhang X, Huang D, Zhou H
Breast Cancer: Targets and Therapy 2023, 15:495-504
Published Date: 25 July 2023
Engagement in Integrative and Nonpharmacologic Pain Management Modalities Among Adults with Chronic Pain: Analysis of the 2019 National Health Interview Survey
Rodgers-Melnick SN, Trager RJ, Love TE, Dusek JA
Journal of Pain Research 2024, 17:253-264
Published Date: 16 January 2024
Pharmacological Prescribing and Satisfaction with Pain Treatment Among Non-Hispanic Black Men with Chronic Pain
Oloruntoba O, Bergeron CD, Zhong L, Merianos AL, Sherman LD, Kew CL, Goidel RK, Smith ML
Patient Preference and Adherence 2024, 18:187-195
Published Date: 19 January 2024