Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Evolving PCOS Management: From Symptom Control to Phenotype-Targeted Therapy
Authors Wang T, Zhang T, Wang J, Lu T
Received 29 August 2025
Accepted for publication 12 January 2026
Published 4 February 2026 Volume 2026:19 560296
DOI https://doi.org/10.2147/DMSO.S560296
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Melissa Olfert
Tong Wang,1 Tianhong Zhang,2 Jingyuan Wang,1 Tao Lu2
1Department of Reproduction, Qingdao Municipal Hospital, Qingdao, 266071, People’s Republic of China; 2Department of Gynecology, Qingdao Municipal Hospital, Qingdao, 266071, People’s Republic of China
Correspondence: Tao Lu, Email [email protected] Jingyuan Wang, Email [email protected]
Abstract: Polycystic ovary syndrome (PCOS) constitutes a prevalent endocrine and metabolic disorder that substantially compromises reproductive and metabolic health in women of reproductive age. The escalating global prevalence of this multisystem condition underscores the need for innovative, interdisciplinary management strategies. Unlike existing reviews, this paper offers a distinctive synthesis of recent advances in PCOS clinical management, with a novel focus on integrating lifestyle modifications, pharmacological interventions, assisted reproductive techniques, and emerging therapeutic approaches such as digital health tools and personalized medicine. It critically evaluates the mechanisms, efficacy, and limitations of these strategies, while identifying underexplored gaps in current knowledge and practice. Furthermore, the review delineates future research trajectories to bridge these gaps and advance personalized care, ultimately aiming to improve clinical outcomes and patient-centered management.
Keywords: polycystic ovary syndrome, insulin resistance, hyperandrogenism, lifestyle interventions, pharmacological treatment
Introduction
Polycystic ovary syndrome (PCOS) represents a prevalent endocrine disorder affecting reproductive-aged women, with global prevalence exceeding 10%.1 This syndrome manifests through reproductive, metabolic, and psychological disturbances, characterized clinically by hyperandrogenism, ovulatory dysfunction, polycystic ovarian morphology, and metabolic derangements including insulin resistance and obesity. The pathophysiology involves synergistic genetic predispositions, metabolic determinants, and environmental influences. Recent mechanistic insights have revealed novel therapeutic targets, shifting management paradigms from symptom control to pathophysiology-directed approaches. While existing reviews have summarized general interventions, this review distinctively synthesizes the latest advances in mechanism-based and phenotype-specific strategies, offering an integrated perspective that bridges translational research and clinical practice.
PCOS presents substantial clinical heterogeneity that complicates both diagnostic precision and therapeutic management.2 Affected women demonstrate variable phenotypic spectra, ranging from reproductive-dominant manifestations (eg, anovulatory infertility) to metabolic-dominant profiles (eg, insulin resistance with obesity). The Rotterdam diagnostic criteria—requiring ≥2 of: oligo/anovulation, clinical/biochemical hyperandrogenism, or polycystic ovarian morphology—exhibit limitations in identifying normoandrogenic variants, perimenopausal women with metabolic sequelae, and adolescents with evolving presentations. Recognition of PCOS as an independent risk factor for endometrial carcinoma (attributable to chronic anovulation), type 2 diabetes mellitus, and cardiovascular dysfunction underscores the imperative for early intervention to mitigate long-term sequelae. This review critically addresses these diagnostic and phenotypic challenges, proposing a refined framework for subpopulation-specific management that is often overlooked in the current literature.
Insulin resistance represents a central pathophysiological mechanism in PCOS, directly compromising reproductive function while concurrently driving metabolic dysfunction.3,4 Obesity – prevalent in over 50% of cases – significantly exacerbates insulin resistance through adipokine dysregulation.5 This pathophysiological synergy establishes lifestyle interventions (structured dietary modification and evidence-based physical activity) as foundational therapeutic strategies targeting weight reduction and insulin sensitivity restoration. Pharmacotherapy with insulin sensitizers, notably metformin, demonstrates efficacy particularly in insulin-resistant subpopulations. Combined administration of these metabolic regulators with hormonal contraceptives to normalize menstrual cyclicity and counter hyperandrogenism constitutes the contemporary therapeutic paradigm. Unlike previous reviews, we provide a comparative analysis of these conventional approaches with emerging strategies, highlighting context-specific applications based on phenotype and metabolic profile.
Beyond established therapeutics, novel interventions are emerging for PCOS management. Myo-inositol administration demonstrates potential for ameliorating ovarian dysfunction and metabolic irregularities in affected women.6,7 Concurrently, investigational agents including next-generation anti-androgens and insulin-sensitizing compounds undergo evaluation for efficacy across heterogeneous presentations.8 Most significantly, precision medicine approaches incorporating phenotypic stratification and individual patient parameters are increasingly implemented clinically. This evolution toward individualized therapeutic strategies seeks to enhance outcomes through tailored interventions addressing specific pathophysiological profiles. This review uniquely synthesizes these cutting-edge developments, offering critical insights into their mechanistic bases and practical integration into current clinical workflows—a dimension underexplored in earlier comprehensive reviews.
The evolving therapeutic landscape for PCOS reflects progressive mechanistic elucidation of its multifactorial pathophysiology. This review not only synthesizes contemporary advances but also introduces a novel, evidence-based framework for personalizing interventions according to phenotypic and metabolic subtypes.
We underscore the critical importance of phenotype-specific management strategies, critically appraising both established and emerging therapeutics to identify gaps and opportunities in current practice. Continuous expansion of the PCOS evidence base necessitates that clinicians maintain contemporary knowledge of evolving interventions. By providing a forward-looking perspective on translational applications and clinical implementation, this review aims to equip healthcare providers with the tools necessary to enhance patient-centered outcomes while mitigating long-term cardiometabolic and reproductive sequelae.
Lifestyle Interventions as a Foundational Approach
The Mechanisms of Dietary Adjustments
Low glycemic index diets have emerged as a significant dietary strategy for improving insulin sensitivity, particularly in individuals with PCOS.9,10 These diets focus on consuming carbohydrates that result in a gradual rise in blood glucose levels, thereby minimizing insulin spikes. Evidence consistently demonstrates that Low glycemic index diets enhance metabolic parameters in PCOS, primarily through improved insulin sensitivity. This dietary intervention achieves significant reductions in fasting insulin levels and superior glycemic control by attenuating postprandial glycemia. The physiological mechanism involves modulated insulin kinetics: reduced glucose excursions decrease pancreatic β-cell demand, subsequently improving systemic insulin responsiveness. These metabolic improvements directly ameliorate PCOS symptomatology and support reproductive-metabolic health restoration. Low glycemic index dietary patterns further modulate body composition through favorable weight modulation and adipose tissue reduction, thereby establishing a mechanistic pathway for restoring hypothalamic-pituitary-ovarian axis function and promoting ovulatory cyclicity in polycystic ovary syndrome.11
The Mediterranean dietary pattern – distinguished by high intake of fruits, vegetables, whole grains, legumes, and monounsaturated fatty acids (notably olive oil) – exerts favorable influences on metabolic dysregulation in polycystic ovary syndrome.12 This nutritional paradigm provides substantial antioxidants and anti-inflammatory compounds that mitigate chronic subclinical inflammation inherent to the condition. Evidence establishes that Mediterranean diet adherence correlates with quantifiable improvements in insulin sensitivity, atherogenic dyslipidemia, and mitochondrial function among women with polycystic ovary syndrome. Implementation of this dietary regimen demonstrably reduces insulin resistance parameters while concurrently ameliorating aberrant lipid profiles, collectively enhancing metabolic health indices. The therapeutic effects are primarily mediated through improved endothelial function, attenuated oxidative stress, and optimized hormonal homeostasis, synergistically mitigating adverse reproductive outcomes while reducing the risk of associated comorbidities including type 2 diabetes and cardiovascular disease.
Elevated dietary protein intake facilitates weight modulation and endocrine homeostasis in polycystic ovary syndrome through enhanced satiety signaling, appetite regulation, and thermogenic expenditure. These physiological adaptations subsequently improve characteristic metabolic derangements including fasting insulin elevation and aberrant androgen levels. Dietary interventions emphasizing adequate protein consumption enhance weight management and metabolic outcomes in polycystic ovary syndrome.13 Prioritizing low-saturated-fat protein sources (eg, legumes, fish, lean poultry) mitigates metabolic syndrome sequelae through improved lipid homeostasis and insulin sensitivity.14 Macronutrient distribution favoring protein represents a strategic nutritional approach for comprehensive PCOS management.
Evidence for Exercise Interventions
Exercise interventions, particularly combining aerobic and resistance training, are extensively established to improve key polycystic ovary syndrome parameters. Comparative evidence confirms both modalities significantly enhance insulin sensitivity, optimize body composition, and restore menstrual regularity. Aerobic exercise specifically reduces adiposity markers including body weight and fat mass – critical metabolic mediators for restoring endocrine homeostasis in affected women. Current physiological evidence confirms resistance training increases fat-free mass and elevates basal metabolic rate. This metabolic adaptation enhances insulin sensitivity via upregulated glucose utilization pathways. When integrated with aerobic exercise, the combined regimen demonstrates synergistic efficacy for optimizing both cardiometabolic and reproductive parameters in polycystic ovary syndrome.15–17
High-intensity interval training (HIIT) represents a time-efficient exercise modality for polycystic ovary syndrome management, alternating brief maximal-intensity intervals with active recovery periods. This paradigm enhances cardiovascular adaptation and metabolic biomarkers – including pronounced reductions in adiposity and insulin resistance – more effectively than moderate-intensity protocols. Additionally, HIIT ameliorates psychological comorbidities prevalent in this population.
Exercise frequency and intensity critically modulate clinical outcomes in polycystic ovary syndrome, with evidence demonstrating that moderate-to-vigorous intensity physical activity consistently enhances insulin sensitivity and suppresses androgen levels. Optimized protocols combining ≥150 minutes/week of moderate-intensity exercise with biweekly resistance training elicit significant improvements in cardiometabolic and reproductive parameters. This established dose-response relationship necessitates precision exercise prescriptions individualized to patient capabilities and preferences to maximize adherence and therapeutic efficacy.
Multidimensional Health Outcomes of Behavioral Interventions
Cognitive behavioral therapy (CBT) represents a targeted intervention addressing psychological and behavioral dimensions of polycystic ovary syndrome, enhancing patients’ acquisition of adaptive coping strategies, self-efficacy, and adherence to lifestyle modifications. Through systematic restructuring of maladaptive cognitive patterns underlying stress responses, CBT facilitates sustainable behavioral changes critical for managing core symptoms. Integration with conventional medical management synergistically improves multidimensional outcomes including psychological morbidity metrics and quality-of-life parameters.
Suboptimal sleep parameters constitute a critical modifier of polycystic ovary syndrome pathophysiology, with evidence confirming associations between disrupted sleep architecture and exacerbated insulin resistance coupled with neuroendocrine dysregulation. Targeted interventions improving sleep efficiency mediate metabolic restoration through attenuated hypothalamic-pituitary-adrenal axis activation, thereby enhancing insulin sensitivity and restoring ovarian cyclicity.
Effective stress management constitutes a fundamental component of PCOS care, given chronic stress exacerbates neuroendocrine perturbations and metabolic dysfunction. Evidence confirmed mind-body interventions including mindfulness therapies and yoga downregulate cortisol secretion and restore hypothalamic-pituitary-ovarian axis regulation. This physiological normalization facilitates improved ovarian cyclicity and metabolic parameters, representing an essential adjunct therapeutic modality for comprehensive PCOS management.
Pharmacotherapy Optimization Strategies
Estroprogestin Therapy in PCOS Management
Estroprogestin therapy (EPT), combining estrogen and progestin, remains a cornerstone of pharmacological management for polycystic ovary syndrome (PCOS). Its primary indications include regulating menstrual irregularities, mitigating clinical hyperandrogenism (such as hirsutism and acne), providing contraception, and protecting the endometrium from hyperplasia.18,19
Formulation selection is tailored to individual patient profiles, with newer-generation progestins (eg, drospirenone, desogestrel) offering enhanced anti-androgenic benefits and improved metabolic profiles. Dosing strategies have evolved toward lower estrogen content (eg, 20–30 μg ethinylestradiol) and flexible regimens (eg, 24/4 cycles) to optimize tolerability and efficacy.
Metabolically, EPT generally exerts favorable effects on lipid profiles by increasing HDL-C and lowering LDL-C, while its impact on glucose metabolism is modest but warrants monitoring in high-risk individuals. Although there is a slight increase in thrombotic risk, absolute risk remains low for most patients, with contraindications including smoking, obesity, hypertension, and personal history of thrombosis.
Therapeutic decisions should be individualized based on patient symptoms, metabolic risk factors, and preferences, with ongoing evaluation of efficacy and safety. EPT continues to be an effective and versatile option in PCOS management, particularly for those without immediate fertility goals.20
Therapeutic Mechanisms of Insulin Sensitizers
Metformin dose optimization constitutes a cornerstone of PCOS management, directly enhancing insulin sensitivity and normalizing menstrual cyclicity.21–24 Evidence confirms that higher doses significantly improve metabolic parameters and ovulatory function, necessitating evidence-optimized dosing algorithms to balance efficacy against dose-dependent gastrointestinal adverse effects. Thiazolidinediones (TZDs) serve as a validated second-line adjunct therapy for refractory insulin resistance, requiring rigorous patient stratification to mitigate adverse effect profiles including fluid retention and cardiovascular risks.24 Novel applications of sodium-glucose cotransporter-2 (SGLT-2) inhibitors demonstrate preliminary efficacy for metabolic improvement, leveraging pleiotropic benefits of weight reduction and cardioprotection to expand therapeutic paradigms.23
The growing recognition of nutraceuticals in PCOS management has positioned myo-inositol and D-chiro-inositol as promising insulin-sensitizing agents.25,26 These inositol isomers function as intracellular second messengers in insulin signaling pathways, effectively ameliorating insulin resistance—a core pathophysiological feature of PCOS.27 Accumulating evidence from randomized controlled trials demonstrates that myo-inositol supplementation (typically 2–4 g daily) significantly improves insulin sensitivity, restores spontaneous ovulation, and reduces hyperandrogenism markers in PCOS patients.28 Particularly noteworthy is the 40:1 physiological ratio of myo-inositol to D-chiro-inositol, which has shown superior efficacy in restoring ovarian function compared to either isomer alone.29–31 A comprehensive meta-analysis by Unfer et al confirmed that inositol supplementation yields comparable ovulation restoration to metformin, with fewer gastrointestinal adverse effects, positioning it as a viable complementary approach to conventional insulin sensitizers.29 While current evidence predominantly supports its metabolic and reproductive benefits, ongoing investigations are exploring its potential synergistic effects with first-line pharmacological interventions.27
Innovations in Anti-Androgen Therapy
Contemporary anti-androgen therapy for polycystic ovary syndrome requires evidence-based oral contraceptive (OC) formulation selection, prioritizing progestin types aligned with individualized hyperandrogenic manifestations.32 Spironolactone maintains its foundational role, necessitating optimized dosing regimens with potassium monitoring protocols to balance anti-hirsutism efficacy against adverse effects.33 Emerging therapeutic alternatives include novel androgen receptor antagonists demonstrating targeted receptor-specific suppression, warranting rigorous evaluation of long-term safety profiles and comparative effectiveness relative to conventional therapies.
Precision in Ovulation Induction Therapy
Contemporary ovulation induction protocols demonstrate letrozole’s superiority over clomiphene citrate in polycystic ovary syndrome (PCOS) management,34 which reported higher cumulative ovulation rates, improved live birth outcomes, and reduced ovarian hyperstimulation risk. Gonadotropin administration necessitates rigorous risk stratification protocols incorporating antral follicle count and anti-Müllerian hormone assessment to mitigate multifetal gestation complications.35 Predictive modeling of ovarian response enables individualized stimulation dosing, optimizing follicular development while preventing extreme responses through dynamic treatment adjustment algorithms.36
Innovations in Assisted Reproductive Technology
Assisted reproductive technology (ART) has undergone transformative progression through innovations like in vitro fertilization (IVF), now augmented by preimplantation genetic testing (PGT) and artificial intelligence (AI)-enhanced embryo selection. PGT enables comprehensive embryonic genetic screening, increasing IVF efficacy while reducing heritable disorder transmission. Concurrently, AI algorithms integrate multimodal embryological data (morphokinetic, genetic, morphometric) to objectively predict implantation potential, demonstrating superior pregnancy outcome stratification versus conventional morphological assessment.37,38 While innovations like preimplantation genetic testing (PGT) and AI-based embryo selection have broadly advanced assisted reproductive technology (ART), their application must be critically adapted for polycystic ovary syndrome (PCOS) patients. This population faces a heightened risk of ovarian hyperstimulation syndrome (OHSS) following controlled ovarian stimulation. Therefore, PCOS-specific ART protocols emphasize OHSS mitigation strategies—such as GnRH agonist triggers, freeze-all cycles, and gentle stimulation—alongside these technological advances. PGT allows for the detection of genetic anomalies in embryos, which may be particularly relevant given the potential influence of PCOS on oocyte quality. Meanwhile, AI algorithms integrating morphokinetic and metabolic data not only improve embryo selection but may also help predict hyperresponse and OHSS risk, enabling more personalized and safer stimulation strategies for women with PCOS.
Refinement of ovarian stimulation protocols has systematically optimized assisted reproductive technology (ART) outcomes. Modern individualized regimens calibrated to patient-specific hormonal dynamics enhance oocyte retrieval efficiency and maturation competence compared to conventional approaches. In vitro oocyte maturation (IVM) techniques now provide viable alternatives for women with polycystic ovary syndrome, enabling competent oocyte acquisition while circumventing gonadotropin-induced hyperstimulation risks.39,40
Cryopreservation constitutes a critical component of assisted reproductive technology (ART), providing long-term storage solutions for gametes and embryos. This capability is particularly vital for fertility preservation prior to gonadotoxic therapies such as chemotherapy or radiation. Vitrification techniques achieve ultrarapid cryoprotectant-free solidification with ice crystal inhibition, significantly improving post-thaw survival rates of oocytes and blastocysts compared to conventional slow-freezing methods.41
The application of engineered biomaterials in assisted reproductive technology (ART) demonstrates enhanced embryo development and implantation outcomes. Specifically, three-dimensional biomimetic scaffolds replicate endometrial microarchitecture, while decellularized extracellular matrices provide critical biochemical signaling, collectively establishing microenvironmental congruence that optimizes blastocyst competence.41
Despite technological progress, persistent inequities in assisted reproductive technology access disproportionately affect socioeconomically disadvantaged populations. Prohibitive out-of-pocket expenditures for advanced techniques necessitate policy-level interventions developing sustainable financing models and scalable service delivery frameworks.42 Telehealth integration with remote monitoring demonstrates efficacy in mitigating geographic barriers to fertility care, enabling comprehensive reproductive endocrinology consultations for underserved populations in rural and low-resource settings.42
In conclusion, assisted reproductive technology advancements progressively enhance therapeutic precision and success metrics through evidence-based protocols. Future innovation requires multidisciplinary collaboration to address cost barriers and optimize resource distribution, ensuring equitable implementation across diverse patient populations. ART’s clinical significance resides in both technological evolution and capacity to mitigate reproductive health disparities through scalable solutions.
Emerging Treatment Strategies Exploration
Regulation of Gut Microbiota
Emerging evidence implicates gut microbiota dysbiosis as a contributory factor in PCOS pathophysiology, with particular relevance to metabolic and reproductive dysfunction. Microbial communities influence core PCOS mechanisms including insulin signaling cascades, systemic inflammation markers, and steroid hormone metabolism. Probiotic administration demonstrates corrective potential for metabolic dysregulation through mechanisms that enhance intestinal barrier integrity and modulate inflammatory pathways. Specific Lactobacillus and Bifidobacterium strains improve insulin receptor sensitivity and lipid homeostasis, with observed reductions in insulin resistance indices and plasma triglyceride concentrations in the PCOS metabolic phenotype. Gut-microbiota-endocrine axis interactions further associate probiotic interventions with normalized gonadotropin secretion patterns and improved ovulatory cyclicity. Optimal therapeutic application requires strain-specific selection, precision dosing, and individual baseline microbiota characterization.43,44
Fecal microbiota transplantation (FMT) represents an investigational therapeutic approach for PCOS and related metabolic disorders. This intervention involves microbiota transfer from healthy donors to recipients with the objective of restoring gut eubiosis. Preliminary evidence demonstrates FMT-mediated gut microbial restructuring correlates with ameliorated hyperandrogenemia, improved insulin sensitivity (reduced HOMA-IR), and attenuated systemic inflammation in PCOS models.45 In PCOS, fecal microbiota transplantation (FMT) corrects gut dysbiosis associated with metabolic and reproductive dysfunction. Rodent studies document FMT-mediated improvements in insulin sensitivity (reduced HOMA-IR) and hyperandrogenemia (25% testosterone reduction). Mechanistically, microbiota-derived metabolites influence hypothalamic-pituitary-ovarian (HPO) axis regulation via vagal afferent signaling, with experimental evidence demonstrating altered gonadotropin-releasing hormone (GnRH) pulsatility following microbiota modulation. However, therapeutic durability beyond 8 weeks remains unestablished, and optimal donor selection criteria require rigorous metabolic health validation.46 Gut-derived metabolites including short-chain fatty acids (SCFAs) modulate neuroinflammatory cascades and endocrine signaling, contributing to ovarian function regulation and metabolic homeostasis in PCOS. Therapeutic strategies enhancing microbial diversity thereby constitute targeted approaches to ameliorate core PCOS pathologies. Future research must delineate precise gut-brain-PCOS axis mechanisms and develop validated microbiota-directed interventions.
Modern Research on Traditional Chinese Medicine
Traditional Chinese Medicine (TCM) herbal formulations demonstrate therapeutic potential in PCOS management through multi-target mechanisms. Clinical evidence confirms that specific herbal preparations modulate reproductive endocrine parameters and metabolic indices. Shouwu Jiangqi Decoction exhibits efficacy in improving menstrual regularity and ovulatory function in PCOS cohorts. This formulation operates via simultaneous modulation of insulin signaling pathways and inflammatory cascades, providing comprehensive symptom management. Integration with acupuncture further enhances therapeutic outcomes, addressing both reproductive dysfunction and metabolic dysregulation characteristic of PCOS pathology.47
Acupuncture demonstrates efficacy in improving insulin sensitivity and ameliorating PCOS manifestations.48 Evidence confirms acupuncture modulates autonomic nervous system activity, enhancing insulin receptor substrate-1 phosphorylation in skeletal muscle. This intervention significantly reduces HOMA-IR indices (mean reduction: 29%) and free androgen index in clinical cohorts. The therapeutic mechanism involves downregulation of sympathetic tone and β-cell function enhancement, with measurable improvements in ovulatory frequency (41% increase versus sham controls). Acupuncture’s safety profile and absence of pharmacological interactions position it as an evidence-based complementary intervention for PCOS management.49,50 While preliminary evidence points to the potential efficacy of acupuncture, the generalizability of these findings remains limited due to considerable heterogeneity across existing studies. To address this issue and definitively establish its therapeutic value, future work must prioritize rigorous randomized controlled trials complemented by systems biology approaches to unravel the precise mechanisms of action.
Integrative approaches combining TCM and conventional interventions demonstrate enhanced therapeutic outcomes for PCOS. Clinical evidence confirms that coordinated application of acupuncture and herbal formulations yields synergistic improvements in reproductive-metabolic parameters. Specifically, the integration of acupuncture with Shouwu Jiangqi Decoction significantly improves ovulatory rates and insulin sensitivity beyond single-modality interventions. This combined strategy enables comprehensive management of PCOS heterogeneity, concurrently addressing metabolic dysfunction, hormonal dysregulation, and ovarian dysfunction through complementary biological mechanisms. Standardization of evidence-based TCM-Western medicine integration protocols represents a critical research priority to optimize patient-specific therapeutic regimens.51
Advances in Targeted Therapy Development
Glucagon-like peptide-1 (GLP-1) receptor agonists (GLP-1RAs) are increasingly recognized as a pivotal therapeutic option for metabolic dysfunction in polycystic ovary syndrome (PCOS). Current clinical evidence demonstrates that these agents induce substantial body weight reduction (mean 5.9 kg) and significantly improve insulin sensitivity, with HOMA-IR decreases of ≥31.2%.52–54 Furthermore, emerging data highlight concurrent reproductive benefits, including a 28.4% reduction in free androgen index and the restoration of menstrual cyclicity in 43% of anovulatory patients.55
In contrast, the clinical utility of thiazolidinediones (TZDs) in contemporary polycystic ovary syndrome (PCOS) management is substantially constrained by three interrelated limitations. The most pivotal limitation is drug-induced weight gain,56 which directly opposes fundamental PCOS management objectives centered on obesity control. This drawback is further compounded by the availability of superior therapeutic alternatives, particularly glucagon-like peptide-1 (GLP-1) receptor agonists,53,55,57 which demonstrate dual efficacy in significant weight reduction and glycemic improvement, thereby progressively diminishing the relative value of TZDs. Consequently, these pharmacodynamic and clinical comparative disadvantages have led to the systematic deprioritization of TZDs in current international evidence-based guidelines, which now exclude them from primary treatment recommendations for PCOS.
The established involvement of inflammation in PCOS pathogenesis has stimulated investigation into anti-inflammatory therapeutic strategies. Pharmacological modulation of inflammatory cascades offers potential for ameliorating associated metabolic and reproductive dysfunction. Current pharmacological innovations focus on agents capable of selectively inhibiting pro-inflammatory cytokine networks (eg, TNF-α, IL-6 signaling axes) and normalizing dysregulated immune responses. Experimental evidence from monoclonal antibody therapies indicates biological plausibility for targeting specific inflammatory mediators, suggesting anti-inflammatory approaches may constitute potential therapeutic components within a pathogenesis-targeted PCOS management strategy. Further investigation remains imperative to validate mechanistic pathways, establish long-term safety profiles, and determine clinical integration frameworks for these interventions.58
Epigenetic dysregulation underlies PCOS pathogenesis, characterized by heritable DNA methylation patterns that mediate transgenerational transmission of metabolic-reproductive phenotypes.59 Pharmacolocal DNMT inhibition demonstrates therapeutic efficacy in experimental models, significantly reducing hyperandrogenemia and improving insulin sensitivity.60 Mitochondrial-nuclear epigenetic interactions (mitoepigenetics) further contribute to ovarian dysfunction, establishing these pathways as druggable targets.61 This mechanistic framework supports epigenome-targeting therapeutic strategies to normalize endocrine-metabolic derangements guided by individual methylation signatures.62
Conclusion
Contemporary PCOS management has progressed from symptom control to a precision medicine model targeting multisystem manifestations, integrating three core therapeutic strategies: structured metabolic rehabilitation, hyperandrogenism/insulin resistance pharmacotherapy, and assisted reproductive techniques. To address clinical decision-making efficiency, it is essential to compare the effectiveness of these approaches—for instance, metabolic interventions often yield superior outcomes in obese phenotypes, while reproductive techniques are prioritized for infertility. Moreover, combined strategies, such as integrating pharmacotherapy with lifestyle modifications, demonstrate synergistic benefits in improving metabolic parameters and reproductive success rates. This holistic approach mandates coordinated multidisciplinary care across endocrinology, nutrition, and behavioral health, enabling tailored interventions that enhance patient outcomes. Future advancements should focus on molecular stratification using genomic-epigenetic signatures for precise patient classification, coupled with novel mechanism-based biologics and digital health technologies, to further refine personalized management and optimize therapeutic efficiency (Figure 1).
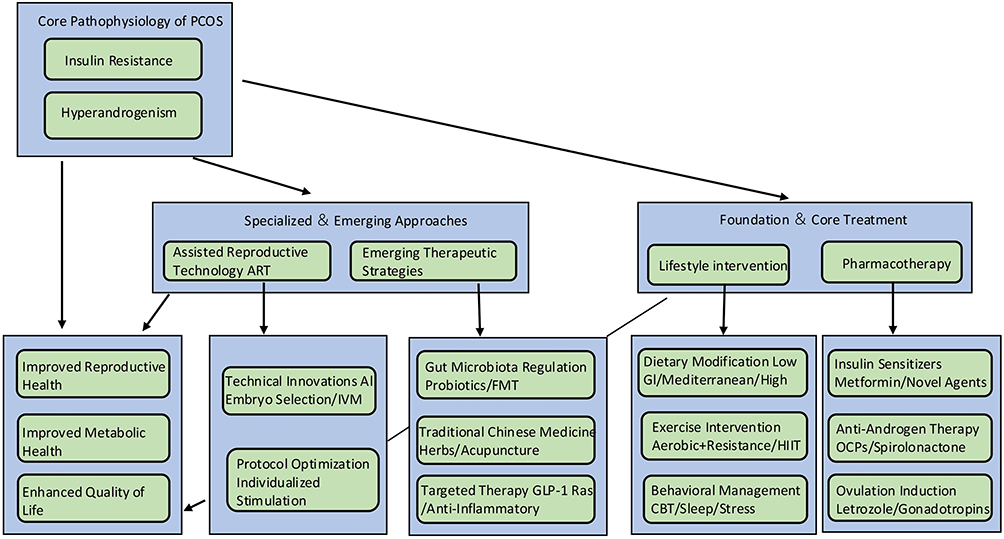 |
Figure 1 The Evolution of PCOS Management: Targeting Phenotypes with Therapeutic Precision. |
Data Sharing Statement
Data sharing is not applicable to this article as no data were created or analyzed in this study.
Author Contributions
Tong Wang
Conceptualization, Methodology, Formal Analysis, Writing – original draft
Tianhong Zhang
Methodology, Writing – Review & Editing
Jingyuan Wang* (Corresponding Author)
Conceptualization, Supervision, Resources, Writing – Review & Editing
Tao Lu* (Corresponding Author)
Conceptualization, Supervision, Writing – Review & Editing, Validation
All authors gave final approval of the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
No funding was received.
Disclosure
The authors declare no competing financial interest.
References
1. Luo Y, Hong C, Fan H, et al. Trends and distribution of infertility - Asia Pacific Region, 1990-2021. China CDC Wkly. 2024;6(28):689–11. doi:10.46234/ccdcw2024.155
2. Medeiros SF, Barbosa JS, Yamamoto MM. Comparison of steroidogenic pathways among normoandrogenic and hyperandrogenic polycystic ovary syndrome patients and normal cycling women. J Obstet Gynaecol Res. 2015;41(2):254–263. doi:10.1111/jog.12524
3. Liao B, Qiao J, Pang Y. Central regulation of PCOS: abnormal neuronal-reproductive-metabolic circuits in PCOS pathophysiology. Front Endocrinol. 2021;12:667422. doi:10.3389/fendo.2021.667422
4. Siddiqui S, Mateen S, Ahmad R, Moin S. A brief insight into the etiology, genetics, and immunology of polycystic ovarian syndrome (PCOS). J Assist Reprod Genet. 2022;39(11):2439–2473. doi:10.1007/s10815-022-02625-7
5. Li M, Chi X, Wang Y, Setrerrahmane S, Xie W, Xu H. Trends in insulin resistance: insights into mechanisms and therapeutic strategy. Signal Transduct Target Ther. 2022;7(1):216. doi:10.1038/s41392-022-01073-0
6. Unfer V, Nestler JE, Kamenov ZA, Prapas N, Facchinetti F. Effects of Inositol(s) in women with PCOS: a systematic review of randomized controlled trials. Int J Endocrinol. 2016;2016:1849162. doi:10.1155/2016/1849162
7. Katyal G, Kaur G, Ashraf H, et al. Systematic review of the roles of inositol and vitamin D in improving fertility among patients with polycystic ovary syndrome. Clin Exp Reprod Med. 2024;51(3):181–191. doi:10.5653/cerm.2023.06485
8. Capozzi A, Scambia G, Lello S. Polycystic ovary syndrome (PCOS) and adolescence: how can we manage it? Eur J Obstet Gynecol Reprod Biol. 2020;250:235–240. doi:10.1016/j.ejogrb.2020.04.024
9. Barr S, Reeves S, Sharp K, Jeanes YM. An isocaloric low glycemic index diet improves insulin sensitivity in women with polycystic ovary syndrome. J Acad Nutr Diet. 2013;113(11):1523–1531. doi:10.1016/j.jand.2013.06.347
10. Marsh KA, Steinbeck KS, Atkinson FS, Petocz P, Brand-Miller JC. Effect of a low glycemic index compared with a conventional healthy diet on polycystic ovary syndrome. Am J Clin Nutr. 2010;92(1):83–92. doi:10.3945/ajcn.2010.29261
11. Ravat FK, Goswami JR, Nair SM, Thummar KN. A review of metabolic and microbial influences on women with polycystic ovarian syndrome. Steroids. 2024;212:109512. doi:10.1016/j.steroids.2024.109512
12. Barrea L, Arnone A, Annunziata G, et al. Adherence to the mediterranean diet, dietary patterns and body composition in women with Polycystic Ovary Syndrome (PCOS). Nutrients. 2019;11(10):2278. doi:10.3390/nu11102278
13. Chen P, Ni S, Liu QF, Ou-Yang L. Retinol intake and PCOS management: a plasma metabolite and protein analysis via Mendelian randomization and NHANES 2011-2016. Front Nutr. 2024;11:1434648. doi:10.3389/fnut.2024.1434648
14. Wang F, Dou P, Wei W, Liu PJ. Effects of high-protein diets on the cardiometabolic factors and reproductive hormones of women with polycystic ovary syndrome: a systematic review and meta-analysis. Nutr Diabetes. 2024;14(1):6. doi:10.1038/s41387-024-00263-9
15. Ryan AS, Pratley RE, Elahi D, Goldberg AP. Changes in plasma leptin and insulin action with resistive training in postmenopausal women. Int J Obes Relat Metab Disord. 2000;24(1):27–32. doi:10.1038/sj.ijo.0801080
16. Kraemer WJ, Volek JS, Clark KL, et al. Influence of exercise training on physiological and performance changes with weight loss in men. Med Sci Sports Exerc. 1999;31(9):1320–1329. doi:10.1097/00005768-199909000-00014
17. Michou V, Davioti M, Syrakou N, Liakopoulos V, Deligiannis A, Kouidi E. Effects of a combined intradialytic exercise training program on functional capacity and body composition in kidney transplant candidates. J Funct Morphol Kinesiol. 2023;8(1):9.
18. Teede HJ, Tay CT, Laven JJE, et al. Recommendations from the 2023 international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Eur J Endocrinol. 2023;189(2):G43–G64. doi:10.1093/ejendo/lvad096
19. Fraison E, Kostova E, Moran LJ, et al. Metformin versus the combined oral contraceptive pill for hirsutism, acne, and menstrual pattern in polycystic ovary syndrome. Cochrane Database Syst Rev. 2020;8(8):CD005552. doi:10.1002/14651858.CD005552.pub3
20. Mendoza N, Simoncini T, Genazzani AD. Hormonal contraceptive choice for women with PCOS: a systematic review of randomized trials and observational studies. Gynecol Endocrinol. 2014;30(12):850–860. doi:10.3109/09513590.2014.943725
21. Yang X, Qi Y, Hao J, et al. Effects of oral antidiabetic agents on the renin-angiotensin-aldosterone system. Eur J Clin Pharmacol. 2025;81(6):801–813. doi:10.1007/s00228-025-03830-w
22. Pani A, Gironi I, Di Vieste G, Mion E, Bertuzzi F, Pintaudi B. From prediabetes to type 2 diabetes mellitus in women with polycystic ovary syndrome: lifestyle and pharmacological management. Int J Endocrinol. 2020;2020:6276187. doi:10.1155/2020/6276187
23. Szczesnowicz A, Szeliga A, Niwczyk O, Bala G, Meczekalski B. Do GLP-1 analogs have a place in the treatment of PCOS? New insights and promising therapies. J Clin Med. 2023;12(18):5915. doi:10.3390/jcm12185915
24. Yang S, Zhao L, He W, Mi Y. The effect of oral antidiabetic drugs on improving the endocrine and metabolic states in women with polycystic ovary syndrome: a systematic review and network meta-analysis. Drugs. 2022;82(14):1469–1480. doi:10.1007/s40265-022-01779-z
25. Formuso C, Stracquadanio M, Ciotta L. Myo-inositol vs. D-chiro inositol in PCOS treatment. Minerva Ginecologica. 2015;67(4):321–325.
26. Bizzarri M, Logoteta P, Monastra G, Lagana AS. An innovative approach to polycystic ovary syndrome. J Obstet Gynaecol. 2022;42(4):546–556. doi:10.1080/01443615.2021.1920006
27. Kiani AK, Paolacci S, Calogero AE. From Myo-inositol to D-chiro-inositol molecular pathways. Eur Rev Med Pharmacol Sci. 2021;25(5):2390–2402. doi:10.26355/eurrev_202103_25279
28. Vyas L, Raiturker AP, Sud S, et al. Management of polycystic ovary syndrome among Indian women using myo-inositol and D-chiro-inositol. Bioinformation. 2022;18(2):103–110. doi:10.6026/97320630018103
29. Unfer V, Porcaro G. Updates on the myo-inositol plus D-chiro-inositol combined therapy in polycystic ovary syndrome. Exp Rev Clin Pharmacol. 2014;7(5):623–631. doi:10.1586/17512433.2014.925795
30. Gateva A, Unfer V, Kamenov Z. The use of inositol(s) isomers in the management of polycystic ovary syndrome: a comprehensive review. Gynecol Endocrinol. 2018;34(7):545–550. doi:10.1080/09513590.2017.1421632
31. Dinicola S, Chiu TT, Unfer V, Carlomagno G, Bizzarri M. The rationale of the myo-inositol and D-chiro-inositol combined treatment for polycystic ovary syndrome. J Clin Pharmacol. 2014;54(10):1079–1092. doi:10.1002/jcph.362
32. Mercurio MG. Hirsutism: diagnosis and management. J Gend Specif Med. 2001;4(2):29–34,64.
33. Azarchi S, Bienenfeld A, Sicco KL, Marchbein S, Shapiro J, Nagler AR. Androgens in women: hormone-modulating therapies for skin disease. J Am Acad Dermatol. 2019;80(6):1509–1521. doi:10.1016/j.jaad.2018.08.061
34. Legro RS, Brzyski RG, Diamond MP, et al. Letrozole versus clomiphene for infertility in the polycystic ovary syndrome. New Eng J Med. 2014;371(2):119–129. doi:10.1056/NEJMoa1313517
35. Broekmans FJ, Kwee J, Hendriks DJ, Mol BW, Lambalk CB. A systematic review of tests predicting ovarian reserve and IVF outcome. Hum Reprod Update. 2006;12(6):685–718. doi:10.1093/humupd/dml034
36. La marca A, Sighinolfi G, Radi D, et al. Anti-Mullerian hormone (AMH) as a predictive marker in assisted reproductive technology (ART). Hum Reprod Update. 2010;16(2):113–130. doi:10.1093/humupd/dmp036
37. Gudapati S, Chaudhari K, Shrivastava D, Yelne S. Advancements and applications of preimplantation genetic testing in in vitro fertilization: a comprehensive review. Cureus. 2024;16(3):e57357. doi:10.7759/cureus.57357
38. Kakkar P, Gupta S, Paschopoulou KI, et al. The integration of artificial intelligence in assisted reproduction: a comprehensive review. Front Reprod Health. 2025;7:1520919. doi:10.3389/frph.2025.1520919
39. Racca A, Drakopoulos P, Neves AR, Polyzos NP. Current therapeutic options for controlled ovarian stimulation in assisted reproductive technology. Drugs. 2020;80(10):973–994. doi:10.1007/s40265-020-01324-w
40. Coticchio G, Cimadomo D, De Vos M, et al. To rescue or not to rescue immature oocytes: prospects and challenges. Fertil Steril. 2025;123(5):749–758. doi:10.1016/j.fertnstert.2025.02.039
41. Kontogeorgi A, Boutas I, Tsangkalova G, et al. Application of additive manufacturing in assisted reproductive techniques: what is the evidence? A clinical and technical systematic review of the literature. Medicina. 2024;60(11):1889. doi:10.3390/medicina60111889
42. Brodeur TY, Grow D, Esfandiari N. Access to fertility care in geographically underserved populations, a second look. Reprod Sci. 2022;29(7):1983–1987. doi:10.1007/s43032-022-00991-2
43. Fijan S, Smigoc T. Overview of the efficacy of using probiotics for neurosurgical and potential neurosurgical patients. Microorganisms. 2024;12(7):1361. doi:10.3390/microorganisms12071361
44. Rahkola EN, Rautava S, Hiltunen H, Ross C, Lahti L, Isolauri E. The preterm gut microbiota and administration routes of different probiotics: a randomized controlled trial. Pediatr Res. 2023;94(4):1480–1487. doi:10.1038/s41390-023-02560-y
45. Horwat P, Mariowska A, Szymanska A, Dzieciatkowska M, Pierudzka W. Multimodal interventions targeting gut microbiota and microbial metabolites in cognitive impairment. Cureus. 2025;17(6):e85688. doi:10.7759/cureus.85688
46. Wu Q, Gao G, Kwok LY, Lv H, Sun Z. Insomnia: the gut microbiome connection, prospects for probiotic and postbiotic therapies, and future directions. J Adv Res. 2025.
47. Yang L, Liu T, Liao Y, et al. Potential therapeutic application and mechanism of gut microbiota-derived extracellular vesicles in polycystic ovary syndrome. Biomed Pharmacother. 2024;180:117504. doi:10.1016/j.biopha.2024.117504
48. Ye Y, Zhou CC, Hu HQ, Fukuzawa I, Zhang HL. Underlying mechanisms of acupuncture therapy on polycystic ovary syndrome: evidences from animal and clinical studies. Front Endocrinol. 2022;13:1035929. doi:10.3389/fendo.2022.1035929
49. Chen H, Deng C, Meng Z, Meng S. Effects of TCM on polycystic ovary syndrome and its cellular endocrine mechanism. Front Endocrinol. 2023;14:956772. doi:10.3389/fendo.2023.956772
50. Li J, Wu W, Stener-Victorin E, et al. A prospective pilot study of the effect of acupuncture on insulin sensitivity in women with polycystic ovary syndrome and insulin resistance. Acupunct Med. 2020;38(5):310–318. doi:10.1177/0964528420902144
51. Luo J, Hu F, Jia Z, et al. Research progress of traditional chinese medicine in adjuvant treatment of type 1 diabetes. Phytother Res. 2025;39(12):5567–5603. doi:10.1002/ptr.8514
52. Elkind-Hirsch KE, Chappell N, Shaler D, Storment J, Bellanger D. Liraglutide 3 mg on weight, body composition, and hormonal and metabolic parameters in women with obesity and polycystic ovary syndrome: a randomized placebo-controlled-phase 3 study. Fertil Steril. 2022;118(2):371–381. doi:10.1016/j.fertnstert.2022.04.027
53. Austregésilo de Athayde De Hollanda Morais B, Martins Prizão V, de Moura de Souza M. The efficacy and safety of GLP-1 agonists in PCOS women living with obesity in promoting weight loss and hormonal regulation: a meta-analysis of randomized controlled trials. J Diabetes Complications. 2024;38(10):108834. doi:10.1016/j.jdiacomp.2024.108834
54. Ge JJ, Wang DJ, Song W, Shen SM, Ge WH. The effectiveness and safety of liraglutide in treating overweight/obese patients with polycystic ovary syndrome: a meta-analysis. J Endocrinol Invest. 2022;45(2):261–273. doi:10.1007/s40618-021-01666-6
55. Han Y, Li Y, He B. GLP-1 receptor agonists versus metformin in PCOS: a systematic review and meta-analysis. Reprod Biomed Online. 2019;39(2):332–342. doi:10.1016/j.rbmo.2019.04.017
56. Diamanti-Kandarakis E, Dunaif A. Insulin resistance and the polycystic ovary syndrome revisited: an update on mechanisms and implications. Endocr Rev. 2012;33(6):981–1030. doi:10.1210/er.2011-1034
57. Zhou L, Qu H, Yang L, Shou L. Effects of GLP1RAs on pregnancy rate and menstrual cyclicity in women with polycystic ovary syndrome: a meta-analysis and systematic review. BMC Endocrine Disorders. 2023;23(1):245. doi:10.1186/s12902-023-01500-5
58. Rakocevic J, Dobric M, Borovic ML, Milutinovic K, Milenkovic S, Tomasevic M. Anti-inflammatory therapy in coronary artery disease: where do we stand? Rev Cardiovasc Med. 2023;24(1):10. doi:10.31083/j.rcm2401010
59. Boedt T, Matthys C, Fong SL, et al. Systematic development of a mobile preconception lifestyle programme for couples undergoing IVF: the PreLiFe-programme. Hum Reprod. 2021;36(9):2493–2505. doi:10.1093/humrep/deab166
60. Choudhari R, Tayade S, Tiwari A, Satone P. Diagnosis, management, and associated comorbidities of polycystic ovary syndrome: a narrative review. Cureus. 2024;16(4):e58733. doi:10.7759/cureus.58733
61. Shukla P, Melkani GC. Mitochondrial epigenetic modifications and nuclear-mitochondrial communication: a new dimension towards understanding and attenuating the pathogenesis in women with PCOS. Rev Endocr Metab Disord. 2023;24(2):317–326. doi:10.1007/s11154-023-09789-2
62. Frampton R, Hocking S, Snaith JR, Greenfield JR. Targeting cardiometabolic risk in type 1 diabetes through incretin physiology. Trends Endocrinol Metab. 2025. doi:10.1016/j.tem.2025.06.004
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Tumor Necrosis Factor Alpha Level in the Uterine Fluid of Patients with Polycystic Ovary Syndrome and Its Correlation with Clinical Parameters
Ha LX, Li WX, Du YD, Yuan YY, Qu XX
Journal of Inflammation Research 2022, 15:6015-6020
Published Date: 29 October 2022
Thyroid Hormones and Cardiometabolic Risk Factors in Saudi Women with Polycystic Ovary Syndrome: A Cross-Sectional Study
Saeed WM, Alsehli F
International Journal of Women's Health 2023, 15:1197-1203
Published Date: 26 July 2023
Correlation Between Hemoglobin Levels and Polycystic Ovary Syndrome Metabolic Disorder
Ha LX, Du YD, Qu XX, Wang JJ
Diabetes, Metabolic Syndrome and Obesity 2023, 16:3019-3027
Published Date: 28 September 2023
Association Between rs2278426 Polymorphism of the ANGPTL8 Gene and Polycystic Ovary Syndrome
Wu H, Wang H, Sun L, Liu M, Wang H, Sun X, Zhang W
Diabetes, Metabolic Syndrome and Obesity 2024, 17:1749-1760
Published Date: 16 April 2024
Glycolytic Dysfunction in Granulosa Cells and Its Contribution to Metabolic Dysfunction in Polycystic Ovary Syndrome
Cao Z, Zhou Q, An J, Guo X, Jia X, Qiu Y
Drug Design, Development and Therapy 2025, 19:5255-5270
Published Date: 18 June 2025