Back to Journals » International Journal of Women's Health » Volume 18
Establishment and Validation of a Risk Prediction Model for Cephalic Dystocia in Parturients Under Epidural Labor Analgesia
Authors Han Y, Liu Z, Gan Y, Tan X, Diao Q, Cao Y, Shi Q
Received 13 August 2025
Accepted for publication 3 January 2026
Published 24 January 2026 Volume 2026:18 560398
DOI https://doi.org/10.2147/IJWH.S560398
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Yu Han,* Zengying Liu,* Yanqiong Gan, Xinlin Tan, Qiuyue Diao, Yuting Cao, Qi Shi
Department of Obstetrics, The Affiliated Hospital of North Sichuan Medical College, Nanchong, 637000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qi Shi, Department of Obstetrics, The Affiliated Hospital of North Sichuan Medical College, No. 63, Wenhua Road, Shunqing District, Nanchong, Sichuan, 637000, People’s Republic of China, Tel +86-15983789947, Email [email protected]
Background: While effectively relieving labor pain, epidural analgesia may decrease signs of cephalic dystocia, delaying timely diagnosis and intervention.
Objective: Develop and validate a prediction model for cephalic dystocia risk under epidural analgesia.
Methods: Between January 2021 and October 2024, 855 women who gave birth at the Obstetrics Department of the Affiliated Hospital of North Sichuan Medical College and received epidural analgesia were included in this study. To identify independent risk factors, univariate and multivariate logistic regression analyses were conducted and R software was used to construct a nomogram prediction model. ROC curve analysis, Hosmer-Lemeshow (H-L) tests, calibration plots, and decision curve analysis were used to evaluate the predictive ability of the model. Bootstrap resampling was used for internal validation.
Results: The following factors were found to be independent predictors of cephalic dystocia under epidural analgesia: premature rupture of membranes (OR: 2.73, 95% CI: 1.46– 5.11), prolonged latent phase (OR: 13.82, 95% CI: 7.51– 25.42),fetal abdominal circumference (OR: 5.13, 95% CI: 2.22– 11.81), maternal age (OR:3.87, 95% CI:1.29– 11.59), parity (OR: 16.16, 95% CI: 2.95– 88.55), fetal presentation at the early stage of the active phase (OR: 2.82, 95% CI: 1.63– 4.88), and fetal position at the early stage of the active phase (OR:8.4, 95% CI:4.83– 14.59). The area under the curve (AUC) for this predictive model was 0.910 (95% CI: 0.878– 0.941). The Hosmer-Lemeshow goodness-of-fit test and calibration curve results showed that (P=0.992 > 0.05). Within the clinical decision curve, the net benefit of the nomogram model is higher across the threshold probability range of 0.05 to 0.83.
Conclusion: This risk prediction model can identify high-risk cephalic dystocia post-epidural analgesia during the early active phase of labor, providing an instant assessment tool for timely intervention and better outcomes.
Keywords: cephalic dystocia, epidural labor analgesia, predictive model, nomogram
Introduction
The most prevalent kind of dystocia, cephalic dystocia,1 is characterized by a mismatch between the position of the fetal head and the maternal pelvis. It frequently shows up as poor fetal head rotation, insufficient flexion, and halt of descent, requiring a cesarean section or instrumental vaginal delivery.2 This complication significantly increases the risks of both maternal and fetal challenges, such as postpartum hemorrhage, infection, fetal distress, negative birth experiences, and maternal mortality.3 It is usually identified during the late active phase or second stage of labor.4 The World Health Organization (WHO) report states that the rate of cesarean sections worldwide has risen to 21% and is still rising.5 Dystocia accounts for about 8% of maternal mortality6 and is one of the main criteria for an emergency cesarean section during delivery.2 According to statistics, 10% of full-term cephalic presentations at birth result in challenges, and 20% to 25% of these cases necessitate a cesarean section to end the pregnancy.4
Effectively reducing labor pain is another important goal of intrapartum care, in addition to guaranteeing delivery safety.7 The World Health Organization (WHO) now recommends epidural analgesia as the primary method for labor pain treatment due to its excellent efficacy and safety profile.8 Its use is common around the world; utilization rates in high-income nations vary by location and parity, ranging from 10% to 83%, with primiparas in the US using it at a rate of about 80%.9 The use of epidural analgesia has increased to 50%–80% in certain economically developed areas of China as labor analgesia programs have progressed.10 Since 2021, our institution’s utilization rate has risen from 20% to 40%.
However, epidural analgesia’s increasing prevalence during labor poses additional difficulties for conventional labor management strategies. The impact of epidural analgesia on the progression of labor is still up for debate. According to previous research, it may prolong the first and second stages of labor and raise the risk of maternal fever, operative delivery, and admission to the neonatal intensive care unit.11,12 Although epidural analgesia may be associated with higher chances of instrumental vaginal delivery,13 a 2023 systematic analysis found no significant correlation between epidural analgesia and incidence of cesarean sections or unfavorable infant outcomes.14,15 However, dose-controlled local anesthetics and newer analgesic protocols show promise for reducing these hazards.16
In context of this, our research attempts to address a crucial clinical problem: epidural analgesia during labor may conceal early clinical symptoms of dystocia while relieving pain, which would compromise prompt identification and intervention. This may result in unfavorable outcomes like maternal soft tissue injuries, hemorrhage, infection, fetal distress, neonatal hypoxia, and acidosis in addition to increasing the risk of protracted labor, emergency cesarean sections, and challenging instrumental deliveries.17,18 Predictive models currently in use have significant limitations: First, their limited applicability under epidural analgesia situations stems from the fact that their creation primarily depends on data from non-analgesia populations.19 Second, they lack an early identification method specific to the process of cephalic dystocia and instead concentrate on predicting conversion to cesarean section.7 Furthermore, it is challenging to adequately describe the real advancement of the delivery process because the majority of models do not effectively integrate labor progress indicators.2 In order to close this gap, the goal of this research is to develop and validate a specific early prediction model that incorporates labor indicators for cephalic dystocia under epidural anesthesia. Key risk factors discovered in the literature review,2,20,21 such as maternal age, height, primiparity, obesity, gestational age, macrosomia, nuchal cord, abnormal fetal presentation, premature rupture of membranes, prolonged latent phase, induction of labor, and cervical edema, will be methodically incorporated into the model construction. In the analysis, these factors will be treated simultaneously as predictive variables and confounding factors requiring statistical adjustment to ensure the model’s accuracy after controlling for baseline risks.
According to contemporary labor theories and our team’s previous research,22 the active phase of labor in Chinese women often begins at 5–6 cm cervical dilatation, with some cases starting at 4 cm. Therefore, the model prediction phase is established at the crucial stage of 4–6 cm cervical dilatation. This study is an extension of our team’s prior model for the non-analgesia population, which aims to achieve early risk prediction.19 By providing clinicians with an earlier window of opportunity to implement targeted interventions like position changes and manual cephalic rotation, this would ultimately improve delivery outcomes, reduce cesarean sections, and enhance maternal and neonatal safety.
Material and Methods
Subjects and Study Design
The purpose of this retrospective cohort study was to develop a predictive model for the risk of cephalic dystocia in women receiving epidural analgesia during labor. It was based on medical records from the Obstetrics Department of the Affiliated Hospital of North Sichuan Medical College between January 2021 and October 2024. Full-term, singleton, cephalic pregnant women who experienced vaginal labor trials following epidural analgesia constructed the study population. For internal validation, the same cohort was subjected to bootstrap resampling. The Affiliated Hospital of North Sichuan Medical College provides critical care for high-risk pregnancies at the provincial level. Vaginal deliveries accounted for nearly 45% of the hospital’s average yearly delivery volume of 2800 cases between 2021 and 2024. The Affiliated Hospital of North Sichuan Medical College’s Medical Ethics Committee examined and authorized this study (2022ER029-1). Inclusion criteria: (1) Singleton pregnancy at 37+0 to 41+6 weeks gestation; (2) Cephalic presentation; (3) Receiving epidural analgesia; (4) No contraindications for vaginal delivery. Exclusion criteria: (1) Maternal psychiatric and cognitive disorders; (2) Cervical dilation >6cm at admission; (3) Intrapartum cesarean delivery on maternal request; (4) Non-reassuring fetal status requiring cesarean delivery; (5) Incomplete medical records.
Based on the 10 events per variable (EPV) rule for logistic regression sample size estimation, the minimum sample size should be at least 10 times the number of independent variables.23 This study ultimately included 7 independent variables, with a cephalic dystocia incidence rate of 12.7%. Therefore, according to the formula N = (7 × 10) / 12.7%, the required minimum sample size satisfies the requirement.
Diagnostic Criteria
Cephalic dystocia:24,25 membrane rupture and uterine orifice dilation ≥ 5 cm, normal contractions: cervical dilation stops for ≥4 hours; poor contractions: cervical dilation stops for ≥6 hours; second stage of labor under spinal analgesia after complete uterine orifice in nulliparas >4 hours; second stage of labor under spinal analgesia after complete uterine orifice in multiparas >3hours,with no progression of labor (including descent of the fetal head and rotation). Normal vaginal delivery: refers to pregnancy for 37+0 to 41+6 weeks, the labor process progresses normally, the fetus is naturally delivered in the head position, and the maternal and infant are in good condition after delivery. The operational definition of “favorable maternal and neonatal outcomes” used in this study is as follows: Favorable maternal outcome: No serious complications, such as severe postpartum hemorrhage (blood loss ≥1000 mL), eclampsia, uterine rupture, severe birth canal injury (Grade III/IV perineal laceration), postpartum infection requiring intervention, or transfer to the intensive care unit, occurred during delivery or within 24 hours after delivery. Favorable neonatal outcome: Apgar scores ≥7 at 1 and 5 minutes after delivery, no need for resuscitative measures (such as positive pressure ventilation, endotracheal intubation, or chest compressions) other than standard suctioning, drying, and warming, and no transfer to the neonatal intensive care unit (NICU) for treatment.25,26
Data Collection
Based on a literature review and expert discussions regarding risk factors for cephalic dystocia,2,19 we retrospectively collected the following maternal data: baseline characteristics (age, height, prenatal weight, parity, gestational age), pre-labor conditions (premature rupture of membranes, induction of labor, nuchal cord, fetal abdominal circumference), and intrapartum factors (prolonged latent phase, cervical edema, fetal presentation and position at the early stage of the active phase). The binary variable “whether or not cephalic dystocia occurred” was defined as the outcome variable (1=Yes, 0 =No). The medical record collection form is provided in Appendix 1.
Definitions of Relevant Variables
1. Fetal abdominal circumference: Measured directly by ultrasound using a transverse abdominal section perpendicular to the fetal spine during the week before delivery at the location where the umbilical vein enters the liver. 2. Cervical edema: During the start of active labor, skilled midwives or obstetricians palpate the cervical texture, thickness, and flexibility. To improve objectivity, ultrasonography measurements of cervical tissue thickness or echogenicity are occasionally augmented.
Statistical Analysis
Statistical analysis was performed using R4.4.3 and SPSS25.0 statistical environment. Measurement data that conformed to normal distribution were described by mean ± standard deviation (Mean±SD), measures that were not normally distributed were described by median (interquartile range, IQR), and counting data were described by percentages. Descriptive analysis was carried out using R (tableone package). Initially, 924 instances were considered. Based on the inclusion and exclusion criteria, 69 cases were excluded, including 37 cases with missing critical information (11 cases for fetal abdominal circumference, 16 cases for maternal height, and 10 cases for prenatal weight). In the end, the research contained 855 cases with complete data and no missing variables. The association between the following variables and cephalic dystocia under epidural analgesia was investigated using univariate analysis and logistic regression models created with R software: parity, maternal age, antepartum BMI, premature rupture of membranes, induction of labor, cervical edema, prolonged latent phase, fetal abdominal circumference, nuchal cord, gestational age, fetal presentation and position at the early stage of the active phase. The data are shown as odds ratios (OR) with 95% confidence intervals (CI). The multicollinearity diagnosis includes 10 variables that had P < 0.1 in the univariate analysis. The variance inflation factor (VIF) and tolerance (TOL) were computed using SPSS 25.0. Variables with VIF > 10 or TOL < 0.1 were removed to ensure model stability. For multivariable analysis, R’s backward stepwise regression was employed. The ten variables that were retained after multicollinearity screening were used to create a multivariable logistic regression model in order to identify independent predictors. Results are reported as OR (95% CI), with P <0.05 indicating statistically significant differences. A predictive nomogram model was developed using R’s rms package. Discriminative ability was evaluated by plotting the receiver operating characteristic (ROC) curve and calculating the area under the curve (AUC) using the pROC package. Calibration was assessed with the calibrate package and the Hosmer–Lemeshow goodness-of-fit test (P >0.05 indicating good calibration). Clinical utility was evaluated using decision curve analysis (DCA) implemented with the rmda package. Internal validation was performed using the bootstrap method with 1000 resamples. The Brier score was used to quantify predictive accuracy; scores nearer 0 indicate better results (0–0.25 is considered acceptable).
Statistical Power
Using R’s power.prop.test function, we also performed a post-hoc power analysis for important predictors. For instance, the study’s statistical power to identify the correlation between prolonged latent phase and cephalic dystocia at a two-sided α of 0.05 was 100% based on the observed event rates and the actual sample size. This study found an effect with an OR > 2.61 at the 80% statistical power level.
Epidural Labor Analgesia Protocol
An epidural catheter was inserted at the L2–3 or L3–4 interspace to a depth of 3–5 cm. Following a test dose of 3–5 mL of 1.5% lidocaine, analgesia was maintained with a solution of 0.1% ropivacaine and fentanyl (2μg/mL). This was administered via a continuous background infusion at 6–8 mL/h, with patient-controlled epidural analgesia (PCEA) boluses of 6–8 mL available at a lockout interval of 15–20 minutes. Analgesia was initiated based on maternal request and assessment of labor progress, without a prespecified cervical dilation threshold.
Results
This study included 924 parturients at the Affiliated Hospital of North Sichuan Medical College between January 2021 and October 2024. Every participant was at term, had a single, live, cephalic fetus, and tried vaginal delivery while receiving epidural labor analgesia. As seen in Figure 1, 855 parturients were included in the final modeling analysis following the application of the inclusion and exclusion criteria. Table 1 shows that of these, 109 cases (12.7%) had cephalic dystocia and 746 cases (87.3%) had non-cephalic dystocia.
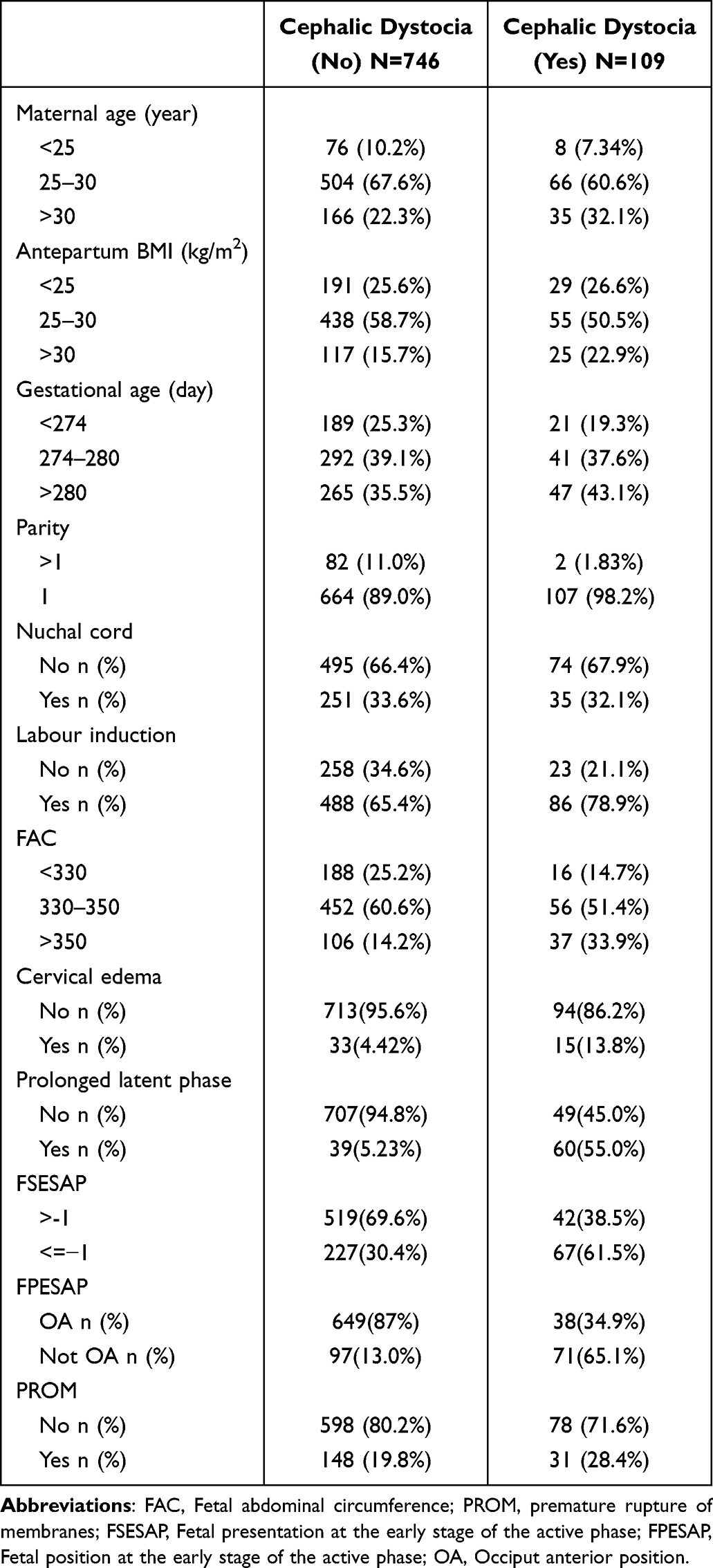 |
Table 1 Baseline Characteristics of Data from the Cephalic Dystocia Group and Non-Cephalic Dystocia Group |
 |
Figure 1 Prediction model flowchart. |
Univariable Analysis
The results of the univariable analysis are presented in Table 2. Maternal age, premature rupture of membranes, labor induction, cervical edema, prolonged latent phase, fetal abdominal circumference, parity, gestational days, fetal presentation and fetal position at the early stage of the active phase (P <0.1).
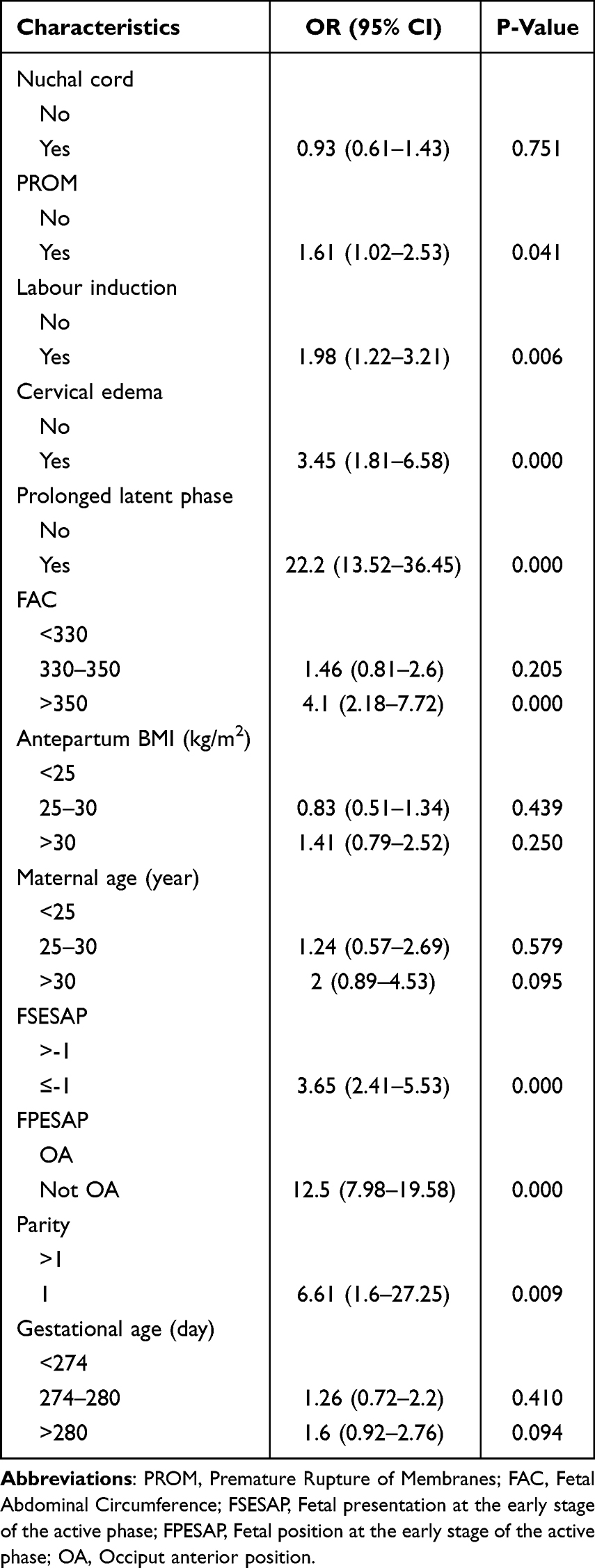 |
Table 2 Univariate Analysis |
Multicollinearity Diagnostics
The ten potential variables were evaluated for multicollinearity (P < 0.1 from univariable analysis). Table 3 presents the detailed data. No substantial multicollinearity was identified among these independent variables (all VIF < 1.3, all TOL > 0.77).
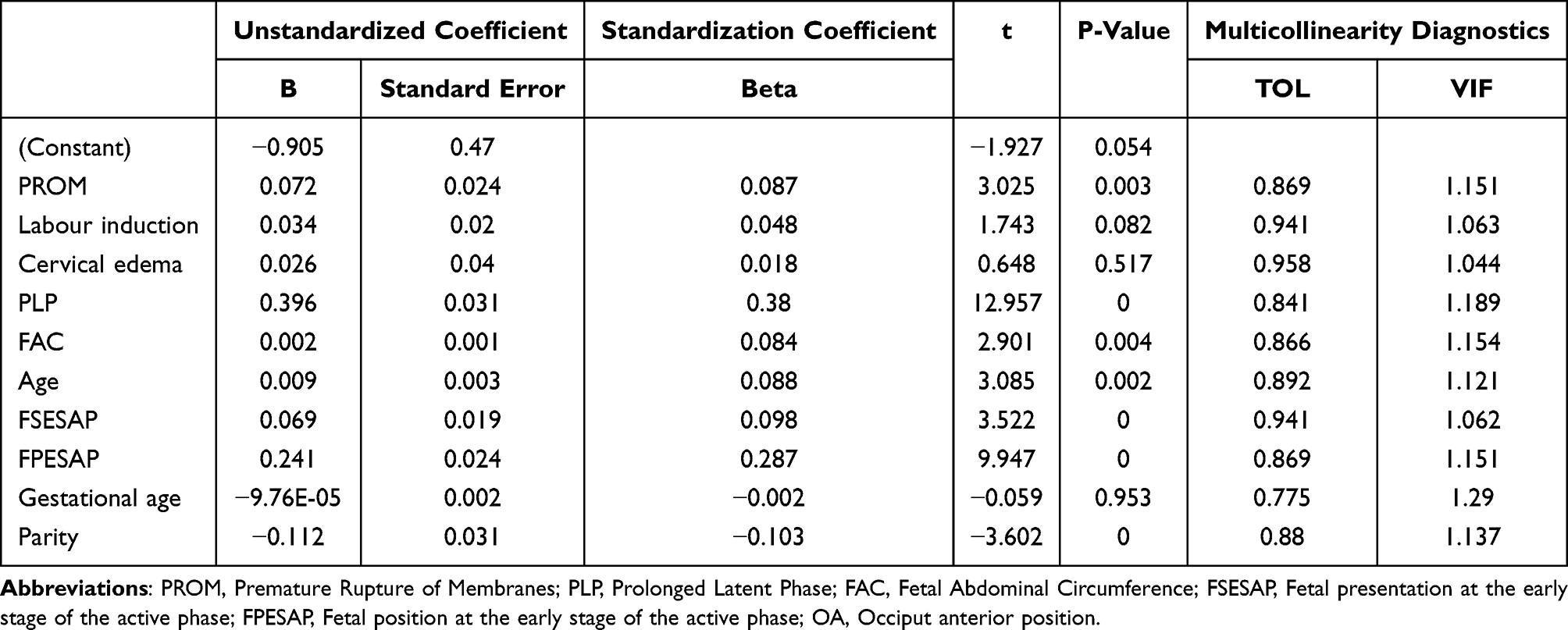 |
Table 3 Multicollinearity Diagnostics |
Multifactorial Logistic Regression Analysis
Seven independent factors were identified using the multivariable logistic regression model (Table 4). These were: premature rupture of membranes (OR 2.73, 95% CI= 1.46–5.11),Prolonged latent phase (OR 13.82, 95% CI= 7.51–25.42),fetal abdominal circumference (OR 5.13, 95% CI= 2.22–11.81), maternal age (OR 3.87,95% CI= 1.29–11.59), parity (OR 16.16, 95% CI= 2.95–88.55), fetal presentation at the early stage of the active phase (OR 2.82, 95% CI= 1.63–4.88), and fetal position at the early stage of the active phase (OR 8.4, 95% CI= 4.83–14.59).
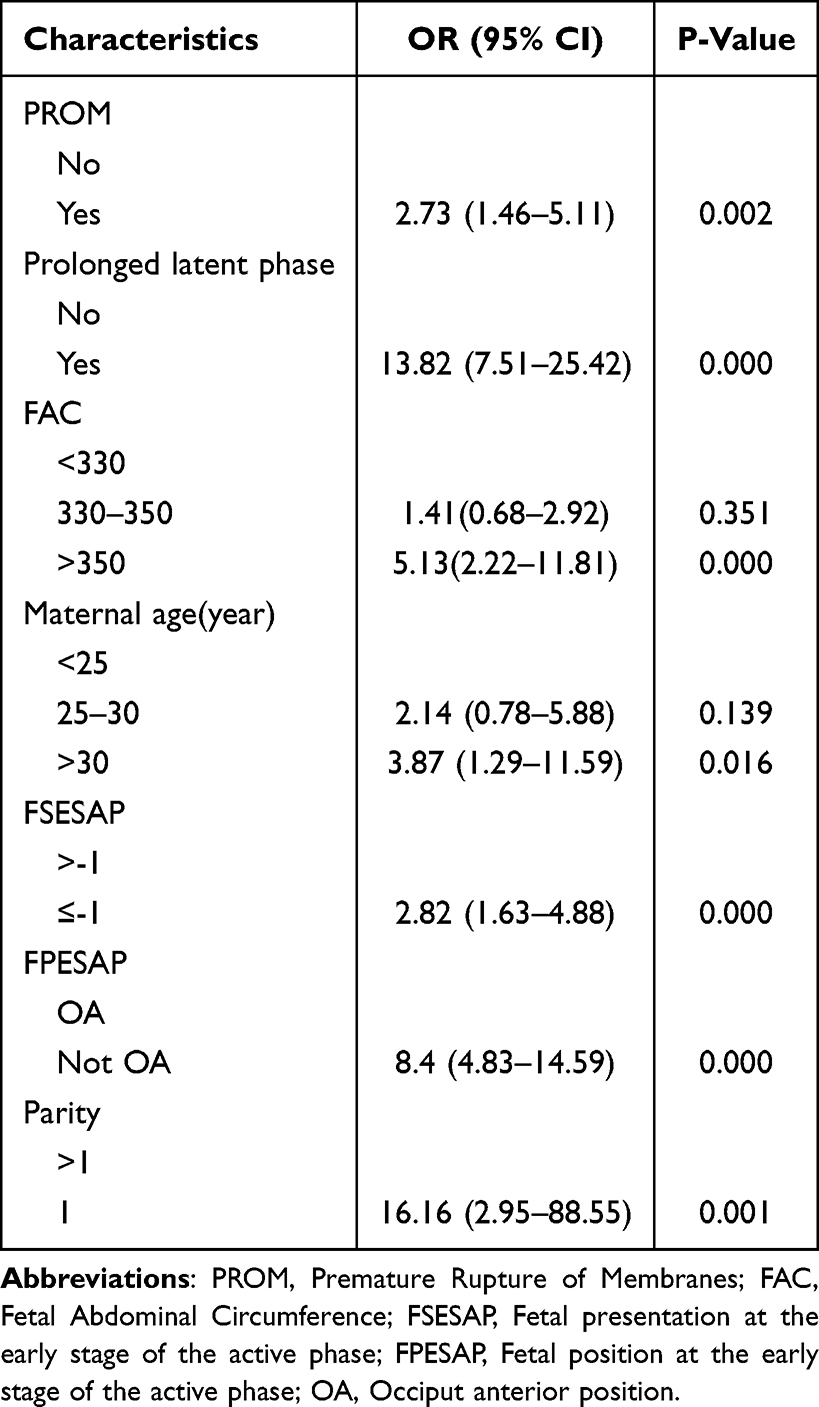 |
Table 4 Multivariate Analysis |
Model Construction
The regression coefficients from the logistic regression analysis were used to establish a multivariable prediction model for the risk of cephalic dystocia under epidural labor analgesia. The following is the model equation: Logit (P) = - 8.079 + 1.004 × premature rupture of membranes (No = 0, Yes = 1) + 2.626 × prolonged latent phase ((No = 0, Yes = 1) + 0.346 × fetal abdominal circumference (<330mm = 0, 330–350 = 1) + 1.634 × fetal abdominal circumference (<330mm = 0, >350 = 1) + 0.762 × maternal age (<25 = 0, 25–30 = 1) + 1.352 ×maternal age (<25 = 0, >30 = 1) + 1.308 × FSESAP (>-1 = 0, ≤-1 = 1) + 2.128 × FPESAP (OA = 0, Not OA = 1) + 2.782 × Parity (≠1 = 0, 1 = 1). The prediction model is shown as a nomogram in Figure 2 to determine every individual’s probability to experience cephalic dystocia while receiving epidural labor analgesia.
 |
Figure 2 Nomogram prediction model. Abbreviations: PROM, Premature Rupture of Membranes; PLP, Prolonged Latent Phase; FAC, Fetal Abdominal Circumference; Age, maternal age; FSESAP, Fetal presentation at the early stage of the active phase; FPESAP, Fetal position at the early stage of the active phase; OA, Occiput anterior position. |
Model Evaluation
The performance of the final prediction model was assessed. The area under the receiver operating characteristic curve (AUC) was 0.910 (95% CI: 0.878–0.941), with a bias-corrected AUC of 0.911 (Figure 3). Internal validation, which comprised calibration curves and the Hosmer-Lemeshow test (P = 0.992; Brier score = 0.063), demonstrated good model calibration (Figure 4). Decision curve analysis (DCA), which showed a net advantage over a threshold probability range of 5% to 83%, was utilized to confirm the model’s clinical utility (Figure 5).
 |
Figure 3 Risk of Cephalic Dystocia ROC Curve. |
 |
Figure 4 Risk of Cephalic Dystocia Calibration Curve. |
 |
Figure 5 Risk of Cephalic Dystocia DCA Curve. |
Discussion
This study successfully developed and validated a nomogram model for predicting the risk of cephalic dystocia in parturients receiving epidural labor analgesia. The model incorporates seven objective clinical variables assessed before and during labor. Parity, prolonged latent phase, and fetal position at the early stage of the active phase were the strongest independent predictors. The clinical signs of cephalic dystocia may be masked by decreased pain perception when using epidural analgesia. The goal of this tool is to give an objective, early warning of this condition.
First, we discovered that the most significant predictor of cephalic dystocia was parity (primiparity), which is consistent with earlier research by Zhu BP et al27 showing that labor abnormalities are substantially more common in primiparas than in multiparas.This may be attributable to factors such as inadequate cervical and pelvic soft-tissue dilatation, differences in myometrial function, and the first-time adaptive response of the pelvic floor in primiparas. Although studies have reported a reduction in uterine contraction frequency following the initiation of epidural labor analgesia,28 the present study design cannot establish such a causal relationship. Second, prolonged latent phase also demonstrated substantial predictive value in our model. Although it is not diagnostic of dystocia, prolonged latent phase is widely regarded as an early indicator of labor abnormality.29 Its etiology is complex, with studies suggesting associations with inadequate cervical ripening, uterine hypocontractility, or early malposition of the fetus.30 In the context of widespread epidural analgesia during labor, it is especially crucial to remember that decreased perception of contractions as a result of pain relief may cause one to miss the warning sign of “prolonged latent phase,” delaying the required clinical assessment and intervention. In situations when analgesia may obscure these early aberrant signals, this risk prediction model properly incorporates these factors to improve monitoring of labor progression and risk identification using objective indicators.
The risk of cephalic dystocia is further influenced by fetal features. Our findings clearly show a significant correlation between the subsequent cephalic dystocia and abnormal fetal position at the early stage of the active phase. This suggests that before entering the most crucial acceleration phase of labor, the fetus was unable to spontaneously rotate into the occipitoanterior position, which paved the way for abnormal rotation and eventual cephalic descent limitations. However, the severe and localized labor pains that act as crucial warning signs are successfully relieved under epidural anesthesia, which may obscure this important information. This “alarm-shielding” effect is probably why epidural analgesia was linked to a higher incidence of persistent occipital posterior position in earlier studies by Lieberman E et al.31 Although epidural analgesia may not directly cause malpresentation, it may make it more difficult to identify and address malpresentation problems immediately, which could result in cephalic dystocia. Furthermore, fetal abdominal circumference (FAC) is a reliable ultrasound marker for evaluating fetal size and predicting macrosomia, and is thus crucial for guiding decisions regarding the mode of delivery.32 Previous studies have reported that an FAC >350 mm significantly increases the risk of dystocia due to macrosomia.33–35 This study similarly identified an FAC >350 mm as an independent risk factor for cephalic dystocia under epidural analgesia. Following epidural administration, the intense pain typically associated with dystocia caused by a large fetal abdominal circumference may be attenuated, potentially impairing timely recognition by the birth attendant and delaying necessary intervention. This study’s objective indicators adequately compensate for the clinical manifestations that epidural analgesia may conceal by acting as predictive tools to replace subjective symptoms.
Other important risk factors are also included in this model. Reduced oxytocin receptors and a physiological deterioration in uterine myometrial function are correlated with advanced maternal age,36 which may reduce the effectiveness of uterine contractions and raise the risk of labor abnormalities. A known indicator of abnormal labor progression is a high fetal presenting part position (above the level of the ischial spines) at the early stage of the active phase.37 Its predictive significance under epidural analgesia is also confirmed by this research. In addition to raising the risk of puerperal and amniotic cavity infections,38 premature membrane rupture could change the rhythm of uterine contractions and fetal rotation, which raises the possibility of dystocia.39 This association is supported by the study’s findings. These factors enable a comprehensive risk evaluation of the maternal starting condition, which forms the basis for personalized labor management.
The application stage of the predictive model in this study is chosen at a cervical dilatation of 4–6 cm. The active phase of labor in Chinese women usually starts at 5–6 cm cervical dilatation, with a minority beginning at 4 cm, according to our research team’s previous findings and contemporary labor concepts.22 A highly credible systematic review cited this study and utilized it as evidence.40 The World Health Organization’s (WHO) recommendations for labor care subsequently cited and incorporated this review.41 Ultimately, the Chinese Guidelines for Normal Delivery established a scientific consensus that establishes 5 cm as the beginning point for the active phase by adhering to and incorporating this WHO recommendation during their development.25 This represents a shift in scientific approach from the conventional fixed standard of “3 cm” to a “dynamic assessment.” This study concentrates the model application on the crucial transition phase of 4–6 cm cervical dilation during active labor, acknowledging individual differences in labor acceleration. In order to enable prompt adjustment of modifiable risk factors, the goal is to identify risks early in or close to the commencement of active labor. This embodies a clinical treatment strategy focused on prevention and offers decision assistance for correcting potentially unfavorable birth outcomes.
Strengths and Limitations
In contrast to previous predictive models, this model is developed using objective indicators and examines maternal and fetal characteristics during the prenatal and intrapartum periods. Our nomogram provides outstanding visualization. In addition to serving as a vital resource for women undergoing epidural analgesia who are susceptible to cephalic dystocia, this tool enables medical professionals quickly execute or modify therapies to reduce unfavorable perinatal outcomes. Nevertheless, there are some limitations to this study. Initially, the model was built using data from pregnant women at a certain time and place because it was a single-center retrospective study. Due to the small sample size, selection bias might have been introduced. Overfitting is a possibility with an EPV of 15.6. Second, this study’s labor progression signs were all evaluated by hand using subjective judgment. However, because this facility is a tertiary teaching institution, labor management is carried out jointly by attending physicians and midwives who are evaluated on a regular basis, guaranteeing some uniformity in labor assessment. Furthermore, despite the inclusion of several critical indicators, data availability limitations prevented the analysis of certain potentially significant elements. Fourth, the retrospective design inherently limits the control of unmeasured confounding. Most importantly, this model has not been validated externally, and its predictive accuracy at other healthcare facilities has not yet been established. We intend to conduct a multicenter, prospective study with a larger sample size in the future. We aim to incorporate additional variables, including maternal psychological factors, pelvimetric measurements, specific epidural analgesia parameters, and intrapartum ultrasound assessments of labor progress.
Conclusion
In conclusion, this study effectively created a nomogram model that included seven objective clinical variables to forecast the probability of cephalic dystocia in parturients using epidural analgesia. With parity, prolonged latent phase, and fetal position at the early stage of the active phase appearing as important predictors, the model showed outstanding discriminatory capacity, the model showed outstanding discriminatory capacity. By providing an early and objective risk assessment, this tool is designed to address the clinical challenge that epidural analgesia may attenuate key warning signs of labor abnormality. It thereby supports clinicians in implementing more timely interventions and individualized labor management, with the potential to improve maternal and neonatal outcomes. Future efforts should focus on external validation and prospective, multicenter studies to further verify and refine the model, ultimately aiming to translate it into an intelligent clinical decision-support tool for broader application.
Abbreviations
BMI, Body Mass Index; WHO, World Health Organization; OA, Occiput anterior position; OP, Occiput posterior position; OT, Occiput transverse position; DCA, Clinical decision curve; ROC, Receiver operating characteristic curve; AUC, Area Under Curve; OR, Adjusted odds ratio.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This research protocol was approved by the Medical Ethics Committee of the Affiliated Hospital of North Sichuan Medical College (2022ER029-1). The study complies with the Declaration of Helsinki. The written informed consent to participate was obtained from all the patients.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the 2023 Sichuan Primary Health Care Development Research Center Key project (SWFZ23-Z-01), the 2022 National Ministry of Industry and Information Technology (MIIT)/National Health Commission of China (NHCC) “Pilot Project on 5G+ Medical and Healthcare Applications” Project Topic (FX5-08): sub-topic of “Special Pilot Program on Health Promotion for Middle-aged and Elderly People”: “5G+ Maternal and Child Health Service and Management” (JKZX2022-5G03) and the 2020 City-University Cooperation Important R&D Platform Project (19SXHZ0435).
Disclosure
Yu Han and Zengying should be regarded as co-first authors for this study. The authors report no conflicts of interest in this work.
References
1. Ressel GW. ACOG releases report on dystocia and augmentation of labor. Am Fam Physician. 2004;69(5):1290.
2. Nahaee J, Abbas-Alizadeh F, Mirghafourvand M, Mohammad-Alizadeh-Charandabi S. Pre- and during- labour predictors of dystocia in active phase of labour: a case-control study. BMC Pregnancy Childbirth. 2020;20(1):425. doi:10.1186/s12884-020-03113-5
3. Selin L, Wallin G, Berg M. Dystocia in labour - risk factors, management and outcome: a retrospective observational study in a Swedish setting. Acta Obstet Gynecol Scand. 2008;87(2):216–14. doi:10.1080/00016340701837744
4. Huang Y, Ran X, Wang X, Wu D, Yao Z, Zhai J. Development and validation of a machine learning model for prediction of cephalic dystocia. BMC Pregnancy Childbirth. 2025;25(1):862. doi:10.1186/s12884-025-07972-8
5. Betran AP, Ye J, Moller AB, Souza JP, Zhang J. Trends and projections of caesarean section rates: global and regional estimates. BMJ Glob Health. 2021;6(6). doi:10.1136/bmjgh-2021-005671
6. Lawrence ER, Klein TJ, Beyuo TK. Maternal Mortality in Low and Middle-Income Countries. Obstet Gynecol Clin North Am. 2022;49(4):713–733. doi:10.1016/j.ogc.2022.07.001
7. Feng Y, Zhao Y, Shao R, Wang Y, Zhang P. Risk factors and predictive model for intrapartum cesarean delivery in women with epidural analgesia: a retrospective cohort study. PeerJ. 2025;13:e20358. doi:10.7717/peerj.20358
8. Zheng H, Zheng BX, Lin XM. The Trend of Labor Analgesia in the World and China: a Bibliometric Analysis of Publications in Recent 30 Years. J Pain Res. 2020;13:517–526. doi:10.2147/JPR.S232132
9. Seijmonsbergen-Schermers AE, van den Akker T, Rydahl E, et al. Variations in use of childbirth interventions in 13 high-income countries: a multinational cross-sectional study. PLoS Med. 2020;17(5):e1003103. doi:10.1371/journal.pmed.1003103
10. Ni YS, Sun L, Zhang J, Zhou L, Yang JX, Chen R. Experiences of decisional conflict related to epidural labour analgesia among women during late pregnancy in a tertiary hospital in China: a mixed methods study. Midwifery. 2023;126:103798. doi:10.1016/j.midw.2023.103798
11. Anim-Somuah M, Smyth RM, Cyna AM, Cuthbert A. Epidural versus non-epidural or no analgesia for pain management in labour. Cochrane Database Syst Rev. 2018;5(5):Cd000331. doi:10.1002/14651858.CD000331.pub4
12. Høtoft D, Maimburg RD. Epidural analgesia during birth and adverse neonatal outcomes: a population-based cohort study. Women Birth. 2021;34(3):e286–e291. doi:10.1016/j.wombi.2020.05.012
13. Callahan EC, Lee W, Aleshi P, George RB. Modern labor epidural analgesia: implications for labor outcomes and maternal-fetal health. Am J Obstet Gynecol. 2023;228(5s):S1260–s1269. doi:10.1016/j.ajog.2022.06.017
14. Lipschuetz M, Nir EA, Cohen SM, et al. Cervical dilation at the time of epidural catheter insertion is not associated with the degree of prolongation of the first or second stages of labor, or the rate of instrumental vaginal delivery. Acta Obstet Gynecol Scand. 2020;99(8):1039–1049. doi:10.1111/aogs.13822
15. Kearns RJ, Shaw M, Gromski PS, Iliodromiti S, Lawlor DA, Nelson SM. Association of Epidural Analgesia in Women in Labor With Neonatal and Childhood Outcomes in a Population Cohort. JAMA Network Open. 2021;4(10):e2131683. doi:10.1001/jamanetworkopen.2021.31683
16. Wang TT, Sun S, Huang SQ. Effects of Epidural Labor Analgesia With Low Concentrations of Local Anesthetics on Obstetric Outcomes: a Systematic Review and Meta-analysis of Randomized Controlled Trials. Anesth Analg. 2017;124(5):1571–1580. doi:10.1213/ANE.0000000000001709
17. Harper LM, Caughey AB, Roehl KA, Odibo AO, Cahill AG. Defining an abnormal first stage of labor based on maternal and neonatal outcomes. Am J Obstet Gynecol. 2014;210(6):536.e531–537. doi:10.1016/j.ajog.2013.12.027
18. Blankenship SA, Raghuraman N, Delhi A, et al. Association of abnormal first stage of labor duration and maternal and neonatal morbidity. Am J Obstet Gynecol. 2020;223(3):445.e441–445.e415. doi:10.1016/j.ajog.2020.06.053
19. Liu Y, Gong Q, Yuan Y, Shi Q. Prediction model for labour dystocia occurring in the active phase. J Obstet Gynaecol. 2023;43(1):2174837. doi:10.1080/01443615.2023.2174837
20. Gardberg M, Leonova Y, Laakkonen E. Malpresentations--impact on mode of delivery. Acta Obstet Gynecol Scand. 2011;90(5):540–542. doi:10.1111/j.1600-0412.2011.01105.x
21. Kjerulff KH, Attanasio LB, Edmonds JK, Kozhimannil KB, Repke JT. Labor induction and cesarean delivery: a prospective cohort study of first births in Pennsylvania, USA. Birth. 2017;44(3):252–261. doi:10.1111/birt.12286
22. Shi Q, Tan XQ, Liu XR, Tian XB, Qi HB. Labour patterns in Chinese women in Chongqing. Bjog. 2016;123(Suppl 3):57–63. doi:10.1111/1471-0528.14019
23. Dai G, Chen MG, Zhu DF, Cai YT, Gao M. Risk factors of positive lymph node metastasis after radical gastrectomy for gastric cancer and construction of prediction models. Am J Cancer Res. 2024;14(11):5216–5229. doi:10.62347/PEDV7297
24. The Obstetric Group of Obstetrics and Gynecology Branch of the Chinese Medical Association. Specialist consensus on new labour standards and treatment. Chin J Obstet Gynecol. 2014;49(07):486.
25. Obstetrics and Gynecology Branch of the Chinese Medical Association, Obstetrics and Gynecology Branch of the Chinese Medical Association, Pereinatal Medicine Branch. Guidelines for normal childbirth. Chin J Obstet Gynecol. 2020;55(06):361–370.
26. Lk CFG, Bloom SL, et al. Williams Obstetrics.
27. Zhu BP, Grigorescu V, Le T, et al. Labor dystocia and its association with interpregnancy interval. Am J Obstet Gynecol. 2006;195(1):121–128. doi:10.1016/j.ajog.2005.12.016
28. Frenken MWE, Schyns-van den Berg A, Oei SG, et al. Uterine contraction frequency after initiation of labour epidural analgesia using electrohysterography monitoring: a prospective pilot study. Int J Obstet Anesth. 2025;62:104296. doi:10.1016/j.ijoa.2024.104296
29. Tilden EL, Caughey AB, Ahlberg M, et al. Latent phase duration and associated outcomes: a contemporary, population-based observational study. Am J Obstet Gynecol. 2023;228(5s):S1025–S1036.e1029. doi:10.1016/j.ajog.2022.10.003
30. Cohen WR, Friedman EA. The latent phase of labor. Am J Obstet Gynecol. 2023;228(5s):S1017–s1024. doi:10.1016/j.ajog.2022.04.029
31. Lieberman E, Davidson K, Lee-Parritz A, Shearer E. Changes in fetal position during labor and their association with epidural analgesia. Obstet Gynecol. 2005;105(5 Pt 1):974–982. doi:10.1097/01.AOG.0000158861.43593.49
32. Melamed N, Yogev Y, Meizner I, Mashiach R, Pardo J, Ben-Haroush A. Prediction of fetal macrosomia: effect of sonographic fetal weight-estimation model and threshold used. Ultrasound Obstet Gynecol. 2011;38(1):74–81. doi:10.1002/uog.8930
33. Jazayeri A, Heffron JA, Phillips R, Spellacy WN. Macrosomia prediction using ultrasound fetal abdominal circumference of 35 centimeters or more. Obstet Gynecol. 1999;93(4):523–526. doi:10.1016/s0029-7844(98)00520-1
34. Chaabane K, Trigui K, Louati D, et al. Antenatal macrosomia prediction using sonographic fetal abdominal circumference in South Tunisia. Pan Afr Med J. 2013;14:111. doi:10.11604/pamj.2013.14.111.1979
35. Dadkhah F, Kashanian M, Bonyad Z, Larijani T. Predicting neonatal weight of more than 4000 g using fetal abdominal circumference measurement by ultrasound at 38–40 weeks of pregnancy: a study in Iran. J Obstet Gynaecol Res. 2013;39(1):170–174. doi:10.1111/j.1447-0756.2012.01918.x
36. Nassar AH, Usta IM. Advanced maternal age. Part II: long-term consequences. Am J Perinatol. 2009;26(2):107–112. doi:10.1055/s-0028-1090593
37. Kjaergaard H, Olsen J, Ottesen B, Nyberg P, Dykes AK. Obstetric risk indicators for labour dystocia in nulliparous women: a multi-centre cohort study. BMC Pregnancy Childbirth. 2008;8(1):45. doi:10.1186/1471-2393-8-45
38. Garg A, Jaiswal A. Evaluation and Management of Premature Rupture of Membranes: a Review Article. Cureus. 2023;15(3):e36615. doi:10.7759/cureus.36615
39. Park KH, Hong JS, Ko JK, et al. Comparative study of induction of labor in nulliparous women with premature rupture of membranes at term compared to those with intact membranes: duration of labor and mode of delivery. J Obstet Gynaecol Res. 2006;32(5):482–488. doi:10.1111/j.1447-0756.2006.00443.x
40. Oladapo OT, Diaz V, Bonet M, et al. Cervical dilatation patterns of ‘low-risk’ women with spontaneous labour and normal perinatal outcomes: a systematic review. Bjog. 2018;125(8):944–954. doi:10.1111/1471-0528.14930
41. WHO Guidelines Approved by the Guidelines Review Committee. WHO Recommendations: Intrapartum Care for a Positive Childbirth Experience. Geneva: World Health Organization; 2018.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Predictive Nomogram with Age and Laboratory Findings for Severe COVID-19 in Hunan Province, China
Jiang J, Zhong W, Huang W, Gao Y, He Y, Li X, Liu Z, Zhou H, Fu Y, Liu R, Zhang W
Therapeutics and Clinical Risk Management 2022, 18:579-591
Published Date: 17 May 2022
Establishment and Validation of a Predictive Nomogram for Hallux Valgus with Pain Under the Second Metatarsal
Bai Z, Cao X, Yang Y, Sun X, Dong Y, Wen J, Sun W
Journal of Pain Research 2022, 15:3523-3536
Published Date: 7 November 2022
Establishment and Validation of a Model for Disease-Free Survival Rate Prediction Using the Combination of microRNA-381 and Clinical Indicators in Patients with Breast Cancer
Shen J, Wang M, Li F, Yan H, Wang R, Zhou J
Breast Cancer: Targets and Therapy 2022, 14:375-389
Published Date: 30 November 2022
A Visualized Mortality Prediction Score Model in Hematological Malignancies Patients with Carbapenem-Resistant Organisms Bloodstream Infection
Qian C, Wu Q, Ruan Z, Liu F, Li W, Shi W, Ma L, Peng D, Yin H, Yao L, Li Z, Hong M, Xia L
Infection and Drug Resistance 2023, 16:201-215
Published Date: 7 January 2023
Establishment and Validation of a Predictive Model for Post-Treatment Anxiety Based on Patient Attributes and Pre-Treatment Anxiety Scores
Sun W, Shen J, Sun R, Zhou D, Li H
Psychology Research and Behavior Management 2023, 16:3883-3894
Published Date: 19 September 2023