Back to Journals » Infection and Drug Resistance » Volume 19
Epidemiological Analysis of Tuberculosis in Nakfa District, Eritrea: A 14 Year Spatiotemporal Study and Implications for TB Control
Authors Mengistu ST ![]() , Kesete Y
, Kesete Y ![]() , Tesfay M, Ghebremeskel GG
, Tesfay M, Ghebremeskel GG ![]() , Abraham S, Hamida ME
, Abraham S, Hamida ME ![]() , Achila OO
, Achila OO ![]()
Received 17 September 2025
Accepted for publication 26 February 2026
Published 12 March 2026 Volume 2026:19 568404
DOI https://doi.org/10.2147/IDR.S568404
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hemant Joshi
Samuel Tekle Mengistu,1 Yafet Kesete,2 Meron Tesfay,2 Ghirmay Ghebrekidan Ghebremeskel,1 Saron Abraham,2 Mohammed Elfatih Hamida,3 Oliver Okoth Achila4
1Clinical Medicine, Nakfa Hospital, Nakfa, Eritrea; 2Clinical Laboratory, Nakfa Hospital, Nakfa, Eritrea; 3Unit of Microbiology, Orotta College of Medicine and Health sciences, Asmara, Eritrea; 4Unit of Clinical Laboratory Sciences, Orotta College of Medicine and Health Sciences, Asmara, Eritrea
Correspondence: Ghirmay Ghebrekidan Ghebremeskel, Email [email protected]
Background: Tuberculosis (TB) remains a major global health challenge, with an estimated 10 million new cases and 1.4 million deaths in 2019. Despite this high burden, TB management, control, and overall funding continue to be suboptimal in many parts of the world. In this study, we aimed to provide information on the frequency and spatiotemporal distribution of TB in Nakfa, one of the most remote regions of Eritrea.
Methods: We analyzed 2,155 TB cases recorded from 2007 to 2021. Data were collected from paper-based hospital and registry records at Nakfa Hospital. Demographic information was analyzed using relevant descriptive statistics, including mean ± SD and frequencies. Additional analyses included crude and adjusted incidence rates, annual percentage change (APC), and spatiotemporal distribution of cases. All analyses were conducted using SPSS version 26 for Windows (SPSS Inc. Chicago, Illinois, USA), Joinpoint Regression Program version 4.9.0, and ArcGIS (ArcMap v 10.7.1; Esri, Redlands, CA, USA).
Results: A total of 2,155 suspected TB cases were reported during the study period. Of these, 1,839 (85.3%) were negative, 165 (7.7%) were smear-negative, 47 (2.2%) were smear-positive, and 104 (4.8%) were extrapulmonary TB cases. The mean age ± SD was 35.18 ± 17.74 years. Regarding sex, the female-to-male distribution was 1,213 (56.3%) and 942 (43.7%), respectively. The average annual incidence rate of TB during the study period (2007– 2021) was 55.64 cases per 100,000 inhabitants. Over this period, the crude and age-adjusted incidence rates (aAR) increased from 2009 (aAR = 57.96) to 2018 (aAR = 91.67). In terms of sex, the incidence of TB was disproportionately higher in females (124.87 per 100,000 vs. 65.13 per 100,000 in males in 2017). Spatiotemporal analysis revealed that TB was concentrated in areas near Nakfa Hospital.
Conclusion: Our findings suggest that TB incidence in Nakfa district is relatively stable, but the distribution of the disease is uneven and may be associated with a lack of TB care services in some subzones. We recommend greater decentralization of TB care services and increased case-finding activities to improve the detection and treatment of TB in Nakfa and other remote areas.
Keywords: tuberculosis, prevalence, spatiotemporal, epidemiology, incidence, COVID-19
Introduction
Tuberculosis (TB), a disease caused by the Mycobacterium tuberculosis complex, has been described as a global emergency. In 2019, TB was associated with approximately 1.4 million deaths (range: 1.1–1.3 million) among the HIV-negative population and 251,000 deaths (range: 223,000–281,000) among the HIV-positive population.1 Furthermore, in the same year, an estimated 10.0 million people (range: 9.0–11.1 million) developed TB, including 1 million children. The observed mortality, data further demonstrate, varies significantly across the disparate World Health Organization (WHO) regions. For example, the WHO African region reported a quarter (25%, 2,460,000) of new TB cases in 2019. The region also reported the highest incidence of HIV-associated TB cases and the highest case-fatality ratios globally, making it the most burdened region per capita.2
To mitigate these effects, the United Nations (UN) held its first high-level meeting on TB, titled “United to End TB: An Urgent Global Response to a Global Epidemic”.3 This call to action highlighted the need for actionable strategies designed to accelerate progress toward ending the TB epidemic by 2030.4 The strategy calls for an 80% reduction in TB incidence (to less than 10 annual notified cases per 100,000 population), a 90% reduction in mortality (to less than 10 per 100,000 persons), and zero TB-affected households experiencing catastrophic costs due to TB.5 Efforts to achieve these targets and milestones will require scale-ups in systematic screening of populations using improved diagnostic tests (GeneXpert MTB/RIF, the Genotype MTBDR plus assay, among others). In addition, more effective treatment for active TB and innovative case detection and prevention strategies will be required.6 To actualize these goals, experts have noted that multisectoral efforts targeting the main drivers of TB infection—such as undernutrition, poor housing, poverty, HIV/AIDS, diabetes mellitus (DM), and smoking—should be prioritized.7 Ultimately, these interventions will require increased research and innovation aimed at accelerating the development, discovery, and prompt application of new interventions, policies, and tools.7
Although TB research in Sub-Saharan Africa (SSA) has expanded, there are multiple data deserts. Where data exist, they are often dated, skewed, or narrow in scope. Furthermore, limited attention has been paid to geospatial analysis of TB distribution within communities. For example, Eritrea, a country with a TB prevalence of 67 cases per 100,000 population per year,8 faces significant challenges due to underreporting and limited resources in remote areas. In practice, variations in TB control program performance have been reported across disparate geographical, socioeconomic, and temporal contexts within the country.8 These disparities have important implications for optimizing resource use and overall program efficiency in resource-poor settings.
Finally, we must note that the elimination of TB in remote communities in low- and middle-income countries (LMICs) is intrinsically linked to global elimination and prevention efforts. Therefore, further improvements in TB elimination will require granular data on the incidence and prevalence of TB in hard-to-reach populations. Compared to settled communities, identifying cases in remote, resource-poor, nomadic, and pastoral communities in SSA remains a challenge. In Eritrea, there is a clear lack of geospatial epidemiological data on TB in these communities and limited analysis of local determinants. In this study, we aimed to evaluate the spatiotemporal patterns of TB incidence in a semi-nomadic population in one of the remotest parts of Eritrea.
Methods
Study Design and Setting
This was a retrospective observational cross-sectional study. We captured all incident cases of TB from July 2007 to June 2021 at Nakfa Hospital in Eritrea. The hospital is located in the administrative unit (Figure 1). The altitude of Nakfa district ranges from 1500 to 2000 meters above sea level. The district is sparsely populated, with approximately 60,000 inhabitants. Most residents in this pastoralist community lead a semi-nomadic lifestyle. The Nakfa subzone includes one hospital and nine health stations distributed across nine administrative units. See Figure 1 for details.
 |
Figure 1 Map of Eritrea and Nakfa subzone highlighted in black. This map is credited to wikipedia. |
Data Source
Clinical data: All newly diagnosed TB cases registered in patient medical records during the study period were included. The hospital has the only specialized TB laboratory and X-ray equipment in Nakfa district; therefore, community health facilities refer all patients to this facility for diagnosis. TB diagnosis was based on WHO guidelines.9 To collect relevant data, a standardized data abstraction protocol was developed and implemented by trained study personnel to ensure consistency. Inter-rater reliability was assessed using Cohen’s kappa (κ).
Pulmonary TB (PTB+)
Diagnosis was based on positivity of sputum smear or chest radiographic abnormalities consistent with active pulmonary TB. A sputum smear sample was regarded as positive (+) if it contained at least one acid-fast bacillus (AFB) per 100 immersion fields. Bacilli load quantification was undertaken using the following approach: 0 AFB per 1 length; 1–19 AFB per 1 length; 20–199 AFB per 1 length; 5–50 AFB per 1 field, on average; >50 AFB per 1 field, on average.10 A slide was regarded as negative (-) if AFB were absent in at least 300 immersion fields.
Pulmonary TB Smear-Negative (PTB-)
Diagnosis was established if a patient coughed for more than two weeks and met at least three of the following criteria: chest radiographic abnormalities consistent with active pulmonary TB; history of contact with a patient with PTB (or a chronic cougher); and/or constitutional symptoms such as weight loss, loss of appetite, and low-grade evening fever, after at least three negative initial sputum smear results from direct microscopy using AFB or Ziehl-Neelsen staining. Treatment history with broad-spectrum antibiotic therapy was also taken into account.
Extrapulmonary Tuberculosis (EPTB)
Diagnosis was based on the presence of TB at anatomical sites other than the lungs.
Outside Nakfa
Patients coming from regions located outside Nakfa town were recorded as such.
Geographic and Population Data
District boundary data and latitude and longitude coordinates were obtained from the National Statistical Office and Geography Office in Eritrea. For coordinates that could not be obtained from this office, alternate sources (ArcGIS Online (Esri, Redlands, CA, USA) and Google search) were employed. The population pyramid data used to calculate incidence rates were obtained from the National Statistical Office.
Completeness and Data Quality
Data on TB cases in Nakfa were abstracted from pre-existing institutional records (paper-based hospital medical records at Nakfa Hospital). The information recorded for each case included name, date of birth or age, incident date, basis of diagnosis, area of residence, and type of TB. Age groups were classified as: 0–24, 25–44, 45–64, and ≥65 years. To improve comparability, we adopted the direct standardization method and calculated the age-adjusted rate using the WHO standard population. The 2021 Eritrean population pyramid was used as the population dataset to generate age-standardized rates (ASR) per 100,000 population. To address quality concerns, several quality control measures were employed: identification and removal of duplicate records; and correction of structural errors (eg., standardizing data formats). Missing data points, which are common in retrospective studies, were systematically evaluated. Variables with missing data were primarily managed by exclusion from analysis.
Statistical Analysis
All analyses were conducted using SPSS version 26 for Windows (SPSS Inc., Chicago, Illinois, USA), Joinpoint Regression Program version 4.9.0, and ArcGIS (ArcMap v 10.7.1; Esri, Redlands, CA, USA). The crude incidence rate (CIR) and associated annual percentage changes (APC) were estimated using Joinpoint Regression Program version 4.9.0. To estimate incidence, the program divided the total number of cases by the corresponding population at risk, expressed per 100,000 population per year. Trends, including APC and average annual percentage change (AAPC), were analyzed using joinpoint regression. The AAPC, estimated as a weighted average of the estimated APC in each joinpoint segment, was subsequently used to summarize the trends in each analysis. Ninety-five percent confidence intervals (CI) were obtained with standard errors from the fit of the regression.
Results
Demographic Characteristics of Tuberculosis Cases
A total of 2,155 suspected TB cases were reported during the study period. Of these, 1,839 (85.3%) were negative, 165 (7.7%) were smear-negative, 47 (2.2%) were smear-positive, and 104 (4.8%) were extrapulmonary TB cases, yielding a total of 316 persons with TB (PwTB) (Table 1). The median age (interquartile range) for smear-positive PTB, smear-negative PTB, and extrapulmonary TB was 35 (25–50), 39 (25–60), and 26 (16–50) years, respectively. In terms of sex, the female-to-male distribution was 178 (56.3%) vs. 138 (43.7%). The highest frequencies of smear-positive (65 cases, 39.4%) and smear-negative PTB (24 cases, 51.2%) were observed between 2013 and 2016. Approximately 152 (50.2%) of the patients were from the Nakfa area, while 151 (49.8%) were from regions outside Nakfa. Figure 2 shows the distribution of cases over the study period.
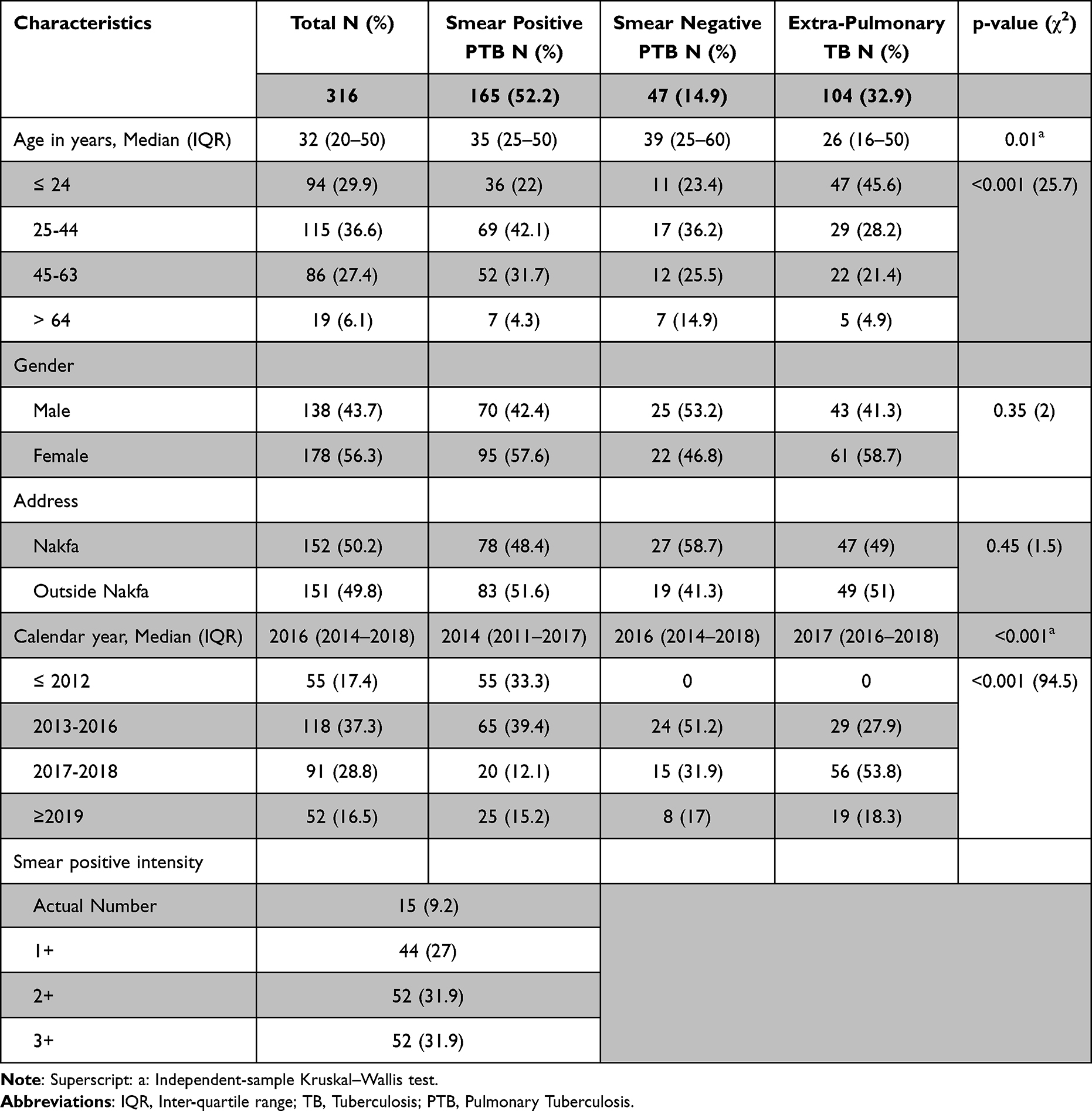 |
Table 1 Sociodemographic Characteristics of Tuberculosis Incidents in Nakfa District, 2007–2021 |
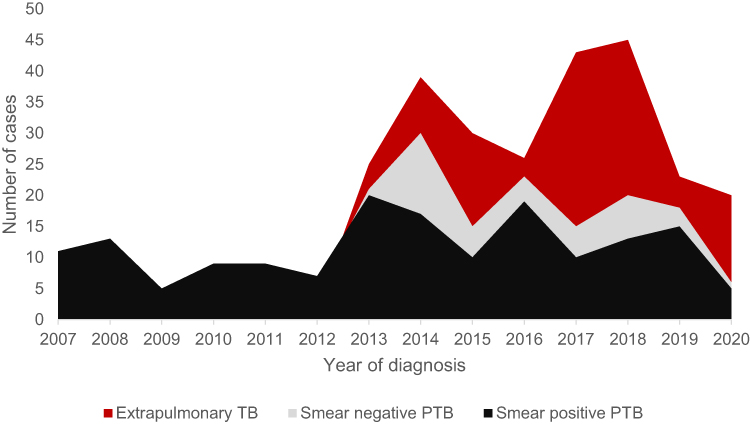 |
Figure 2 Number of cases of extra pulmonary TB, Smear Negative PTB and Smear positive PTB in Nakfa district, Eritrea, 2007–2021. |
General Tuberculosis Incidence Rate Outcomes
According to this study, the average annual incidence rate of TB in Nakfa district during the study period (2007–2021) was 55.64 cases per 100,000 inhabitants. Over this period, the crude and age-adjusted incidence rates (aAR) of TB increased from 2009 (aAR = 57.96) to 2018 (aAR = 91.67). However, a marked decrease in incidence was recorded in subsequent years (aAR = 23.03) (Table 2 and Figure 2). Furthermore, the maximum aAR per 100,000 population was recorded in 2017 among women (aAR = 124.87) compared to men (aAR = 94.06 in 2018). Regarding sex-specific incidence, TB was disproportionately higher in females (124.87 per 100,000 vs. 65.13 per 100,000 in males in 2017). Additionally, males aged 25–44 years had the highest TB incidence, whereas females aged 65 years and older showed an unusual increase in rates after 2017.
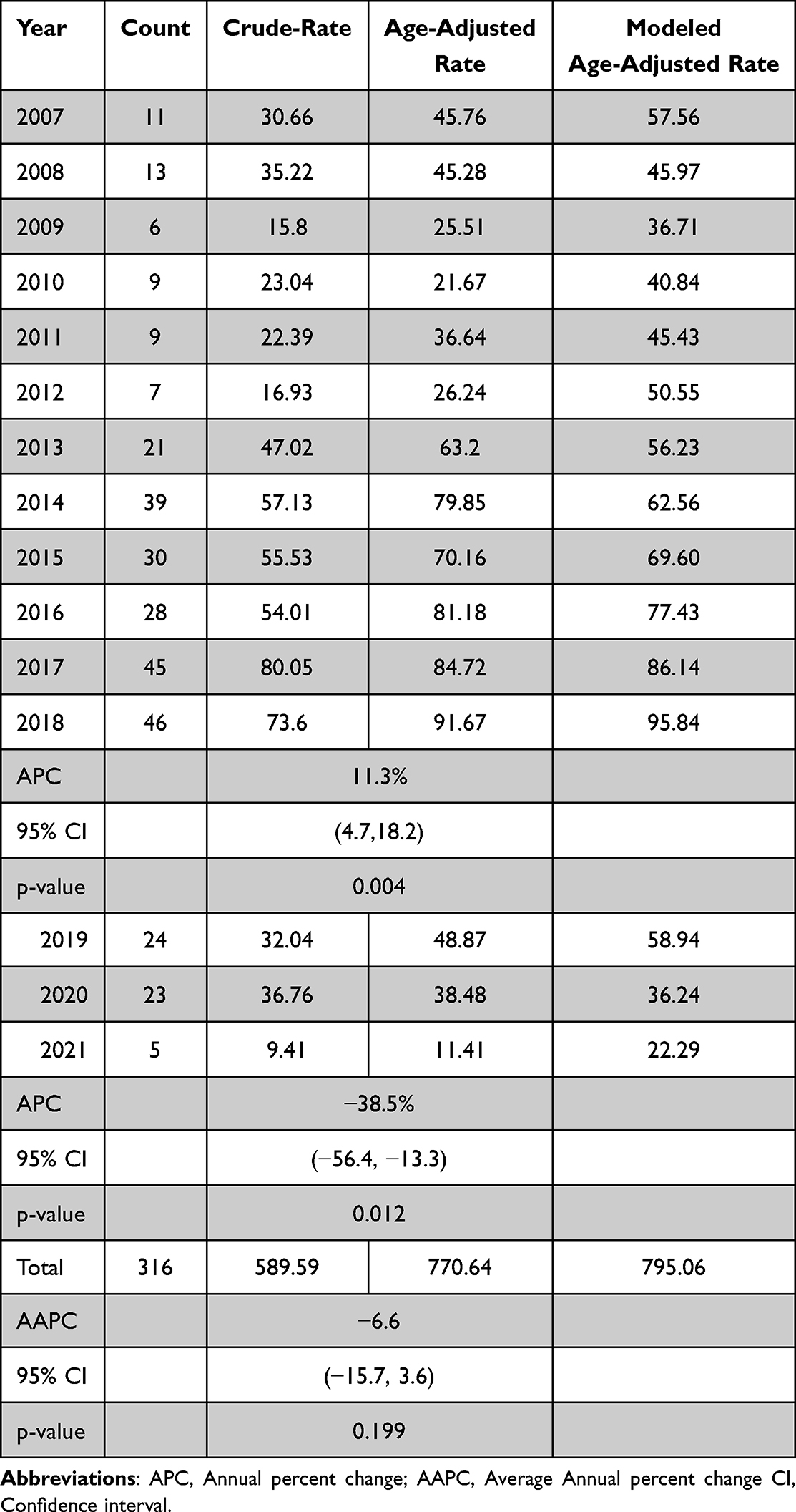 |
Table 2 Crude and Age Standardized Incidence Rate of Tuberculosis year, Nakfa District, 2007–2021 |
Trends in Overall Incidence Rates of Tuberculosis
Joinpoint trend analysis demonstrated that the age-adjusted incidence rate (aAR) of PTB increased linearly from 2007 to 2018 (annual percentage change [APC] = 11.3%, p = 0.004), then decreased from 2019 to 2021 (APC = −38.5%, p = 0.012). The overall average annual percentage change (AAPC) in the incidence rate was −6.6% (95% CI: −15.7 to 3.6) during the entire study period (Table 2).
Trends in Tuberculosis Incidence Rates by Sex and Age
The results of the trend analysis by age group are summarized in Table 3. According to these results, incidence rates per 100,000 population decreased from 13.0 to 8.78, 38.04 to 19.26, 84.90 to 19.11, and 67.64 to 45.66 in the 0–24, 25–44, 45–64, and ≥65 years age groups, respectively. In 2017, however, the highest TB incidence was observed in females (aAR = 124.87), particularly among those aged over 65 years. Furthermore, the crude incidence rate (CIR) of TB in individuals aged >65 years increased from 2007 to 2017 (123.8 per 100,000 to 243.5 per 100,000; APC = 16.1%; 95% CI: 8.8–24.0; p < 0.001), then declined in subsequent years from 2018 to 2021 (136.2 per 100,000 to 83.6 per 100,000; APC = −33%; 95% CI: −52.3 to −6.7; p = 0.023). During the same period, males aged <25 years showed a significant increase in APC (9.0%; 95% CI: 3.0–15.3; p = 0.006). In females within the same age group, the APC associated with age-adjusted incidence rates was 14.58% (95% CI: 4.3–25.9) between 2007 and 2018. Furthermore, women aged 65 years and older experienced a steep increase in TB incidence rate from 2012 to 2016 (APC = 57%; 95% CI: 2.5–130.5), followed by a decrease from 2016 to 2021 (APC = −31.8%; 95% CI: −44.3 to −16.5). Among individuals aged 25–44 years, the incidence rate increased from 2007 to 2017 with an APC of 7.56% in both women and men, followed by a decrease in subsequent years (APC = −27.5%). The AAPCs for the entire study period were variable across age categories: 7.8% (95% CI: −1.0 to 17.4) in the 0–24 years group, −3.9% (95% CI: −15.0 to 8.7) in the 25–44 years group, 2.0% (95% CI: −4.6 to 9.0) in the 45–64 years group, and −0.99% (95% CI: −9.7 to 8.9) in the ≥65 years group.
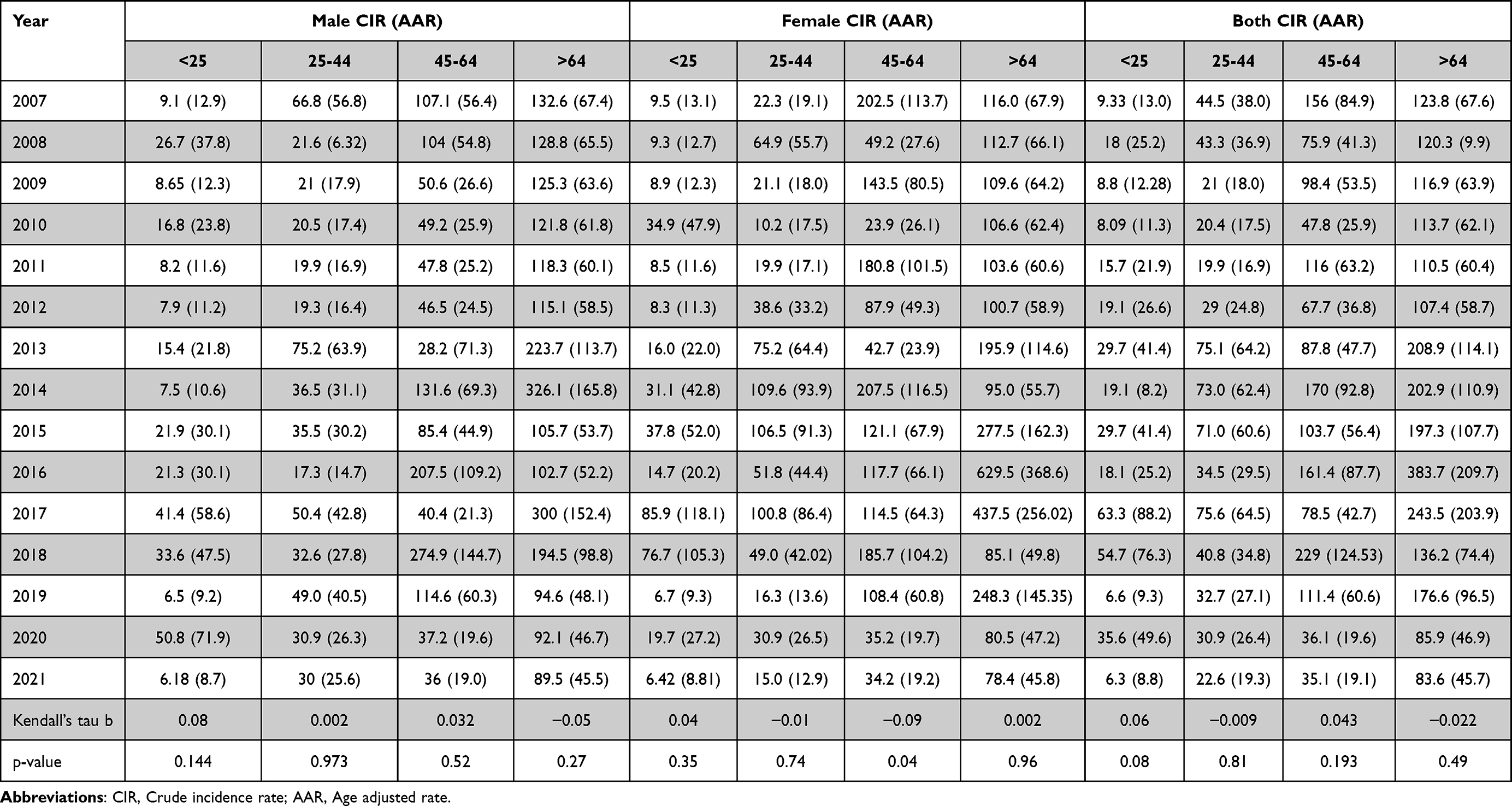 |
Table 3 Yearly CIR and AAR Stratified by Gender and Age-Group; Nakfa District, Eritrea, 2007–2021 |
Mapping and Geospatial Patterns
The residential locations of persons with TB (PwTB) diagnosed at Nakfa Hospital were mapped to identify the geospatial distribution of cases within the region. In this analysis, high-rate clusters were observed in the central region from 2007 to 2014, and in both central and southern prefectures from 2014 to 2021. Nakfa (central region) consistently recorded a relatively higher number of cases, and the number of diagnostic tests performed there was substantially higher than in all other prefectures per study year. Longitudinally, the number of tests across the prefectures did not increase significantly; however, the data reveal higher positivity rates among those prefectures with greater testing volumes compared to those with lower testing volumes. The number of tests decreased in the fiscal years 2019 and 2021, as did the number of confirmed cases.
Discussion
The average annual incidence rate of TB cases per 100,000 persons is one of the parameters recommended by the WHO to guide TB control efforts globally.4,11 In this study, the incidence rate was relatively stable, with disparate burdens and trends reported for males and females—the highest incidence rates per 100,000 population were recorded in 2017 in females and in 2018 in males. The estimates uncovered in this study corroborate earlier reports that documented relatively low TB rates for Eritrea. For example, a previous population-based study conducted in individuals aged <15 years in 2005 reported a crude incidence rate (CIR) of 83 per 100,000 (95% CI: 41–124 per 100,000) and an age- and sex-adjusted prevalence rate of 50 per 100,000.12 The incidence rate of 55.64 cases per 100,000 inhabitants found in our study is significantly lower than those reported in Ethiopia (age-adjusted rate [AAR] = 108),13 Burundi (AAR = 27–456),14 Mozambique (AAR = 527.8),15 and Morocco (AAR = 188).16 However, the incidence rates were higher than those reported in high-income or middle-income countries such as Japan (AAR = 13.9) and Iran (AAR = 10.88).17
Furthermore, our analysis shows that the incidence rate of TB in the Nakfa region increased from 2007 to 2018 and decreased in subsequent years (2019–2021). However, the average annual percentage change (APC) in the incidence of TB was −6.6% throughout the study period, indicating that the APC in TB incidence is comparatively stable A similar finding has been reported in some African countries in the region. In Burundi, the annual change rates of the incidence of pulmonary TB (PTB) ranged from −32.9% to 5.22% across all clinical types of PTB and from approximately −12.2% to 1.1% for TB overall. Reports further suggest that since 2010, reductions in TB incidence of at least 4% per year have been observed in Kenya, Zambia, Ethiopia, Lesotho, Namibia, Tanzania, and Zimbabwe.6
Undoubtedly, the observed increase in APC of TB from 2009 to 2018 should raise concern. However, it is difficult to disentangle the extent to which this increase in TB burden was associated with enhanced transmission rates versus active case finding. This determination is informed by several considerations. First, Eritrea implemented the Directly Observed Treatment Short-Course (DOTS) as the standard care strategy for TB. In subsequent years, Eritrea implemented and subsequently met all WHO Millennium Development Goals (MDG) TB specifications during this period. This included achieving the benchmarks for microscopy laboratory coverage of one per 100,000 persons, one drug susceptibility testing (DST) laboratory, and one culture laboratory per five million persons, as well as extensive training of laboratory technicians on sputum microscopy and sample collection. During the same timeframe, physicians and laboratory scientists with degree-level training were posted to the medical facility. Globally, an annual decrease in TB incidence was reported,18 with some reports attributing these otherwise marginal declines to modest or minimal decreases in TB incidence in intermediate- and high-burden countries.5,11 Reconciling these developments with a rise in TB transmission in Nakfa district is challenging unless the increase in incidence is attributed to improvements in case detection rates (CDR). In Eritrea, previous reports suggested that CDR was below 70% and that improvements should be within the 1.6- to 5-fold range.12 Therefore, the achievement of MDG TB specifications in Eritrea should correspond to improvements in CDR and a consequent increase in detected TB incidence.
The possibility that improvements in CDR may be the principal factor behind the perceived increase in TB is supported by data on the number of samples collected, timing, and geospatial distribution or trends. For example, the increase in incidence from 2013 to 2019 can partly be attributed to a convergence of programmatic interventions. The significant increase in the number of extrapulmonary TB cases from 2013 is probably linked to the posting of physicians to this facility. Previously, patients were attended to by trained non-physician clinicians (midwives and nurses). The 2016–2018 peak in smear-positive and smear-negative samples coincides with the introduction of the more sensitive fluorescent microscopy (direct Auramine–Rhodamine [AO] stained smears) and non-routine active case-finding activities involving mobile sputum sample collection from community hospitals, health centers, and local health stations in the district. By comparison, the decrease in cases from 2019 to 2020 likely reflects the termination of sputum pooling efforts and the impact of COVID-19 restrictions. The drop in CDR due to COVID-19 has been reported elsewhere. In China, comparisons of national TB CDR in February 2020 and February 2019 reported a 20% drop. In India, a 75% reduction (mean of 11,367 weekly cases) was reported in the three weeks after March 22.19
In terms of case distribution, 2017 and 2018 had the highest spread of cases. Importantly, cases in the pre-2018 era were clustered in areas close to Nakfa Hospital. Previous studies have described the clustering of TB cases in regions in closer proximity to major hospitals.20 Therefore, the geographically distant low-rate clusters observed in this study likely reflect suboptimal CDR arising from access challenges or other factors. Highlighting this problem, the UNICEF Annual Office Country Report 2020 noted that the rugged topography of Eritrea and the long distances between health facilities and communities may restrict service delivery. This problem is compounded by the seasonal migration of nomadic communities between the lowlands and the highlands. Collectively, these findings indicate that TB is largely underdiagnosed in remote or difficult-to-reach locations within the Nakfa region.
Other factors pointing to underdiagnosis as a problem include the exclusive reliance (up to 2016) on direct microscopy of unconcentrated sputum smears using the Ziehl–Neelsen (ZN) technique. According to some reports, ZN has a highly variable sensitivity (ranging from 20% to 80%) for PTB.21 Moreover, much lower sensitivities have been observed for paucibacillary disease (eg., pediatric and HIV-associated TB).22 Invariably, poor sensitivity can lead to underdiagnosis or delays in diagnosis and progression to advanced TB. The large number of extrapulmonary TB cases observed in this district highlights this possibility. Research shows that most cases of TB are not clinically apparent and that evidence of its presence is difficult to uncover. However, in late chronic TB among individuals of advanced age or with poor immunity (due to HIV/AIDS or malnutrition—whether privational or non-privational), hematogenous dissemination may occur and lead to extrapulmonary disease.22
Programmatic gaps can also lead to failure to detect TB in individuals with limited contact with health facilities or failure to detect the disease because infected individuals do not seek care (patients may resort to options such as spiritual healing, traditional medicines, or face financial and geographical barriers). Confirming some of these concerns, a study based on the GeneXpert MTB/RIF assay conducted in Zambia uncovered a large undiagnosed and subclinical burden of TB cases in adults.23 Furthermore, recent data from several national TB prevalence surveys found patients with relatively advanced disease (based on chest radiographs) who had not sought care.6 At Nakfa Hospital, advanced TB due to late presentation is not uncommon. Overall, we posit that closing the detection (using GeneXpert MTB/RIF assay) and treatment gaps, particularly in remote communities within Eritrea, will have a substantial impact on TB control. To achieve these objectives, local data will be required. Therefore, research on factors associated with underdiagnosis of TB in remote communities in Eritrea and incorporation of these findings into national strategic plans for prevention should be prioritized.
Lastly, our analysis demonstrated that the incidence of TB in the Nakfa region is higher in patients aged >45 years. In this age group, a higher incidence rate per capita was observed in women. This outcome has been reported in studies that have linked TB transmission and burden to age, gender, race, education level, and lifestyle. According to Kawatsu et al, women are at increased risk of TB infection.24 Patients older than 65 years presented a faster increase in incidence rates from 2007 to 2017, with an APC of 16.1%. Furthermore, they had a higher annual prevalence rate per 100,000 during the study years. The connection between age and susceptibility has been attributed to a number of factors, including diabetes mellitus (DM), malignancies, immunosuppression, cardiopulmonary disorders, and malnutrition.25 Furthermore, treatment outcomes in the elderly are often unfavorable due to their vulnerability to intensified and prolonged therapy.26 Additional structural determinants of TB epidemiology include physical challenges, poverty levels, smoking, HIV infection, living conditions, and nutritional status.27 Based on the above observations and similar country reports, the data raise a number of questions pertaining to the health of elderly women—a group often neglected by researchers in Sub-Saharan Africa—in remote regions of Eritrea.
Strengths and Limitations
This study has several important limitations. First, medical records typically suffer from missing data problems (including incomplete patient history and socioeconomic data), and the variables captured can be limited. Ultimately, potential selection bias from using hospital records also exists. Despite this, Nakfa Hospital’s records remain a valuable source of comprehensive TB data in the district. The patient addresses recorded in the medical records corresponded to where the patients lived at the time of diagnosis. However, a significant number of people in this district are semi-nomadic pastoralists. Thus, some residential addresses may not reflect the locations where infection occurred. Technically, the lack of geospatial accuracy due to nomadic migration may limit the generalizability of the results. This notwithstanding, concerns about the potential effects of this phenomenon should not be overemphasized. Last but not least, sputum smear microscopy remains the primary diagnostic tool in this setting. However, research has shown that this technique is associated with underdiagnosis and underestimation of TB burden.
Conclusion
The incidence of TB in Nakfa district is relatively stable A purely spatial analysis identified strong clustering of TB in the areas surrounding Nakfa Hospital. Spatial heterogeneity and variations over time are likely largely explained by underdiagnosis and underreporting arising from access challenges and the routine use of a diagnostic technique with highly variable sensitivity. Consequently, the true burden of TB in this district remains largely unknown. Looking to the future, efforts will be needed to improve access to preventive, diagnostic, and treatment services. Importantly, this study suggests that GeneXpert MTB/RIF testing should be prioritized in mobile health units, and targeted interventions—including contact tracing—are needed in high-risk rural zones.
Data Sharing Statement
The dataset supporting the conclusions of this article is available from the corresponding author on reasonable request.
Ethical Approval and Consent
Ethical clearance was obtained from the Health Research Ethics and Protocol Review Committee of the Ministry of Health, State of Eritrea (Letter of reference: 08/2021). Consent to participate was not obtained from the patients as the nature of study was from retrospective records but review board of Health Research Ethics and Protocol Review Committee of the Ministry of Health has waived the need to obtain informed consent for this study. All ethical and professional considerations were followed during the study to make patients’ identity strictly confidential. All study procedures followed the recommendations of the Declaration of Helsinki Convention.
Acknowledgment
We would like to extend our gratitude to all Nakfa Hospital members for their assistance in data collection and screening. This paper has been uploaded to research square as a pre-print https://www.researchsquare.com/article/rs-2605577/v1.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Organization WH: global tuberculosis report-executive summary. World Health Organization [online] 2019.
2. Asare P, Asante-Poku A, Osei-Wusu S, Otchere ID, Yeboah-Manu D. The relevance of genomic epidemiology for control of tuberculosis in West Africa. Front Public Health. 2021;9:706651.
3. Zumla A, Petersen E. The historic and unprecedented United Nations general assembly high level meeting on tuberculosis (UNGA-HLM-TB)—’United to End TB: an urgent global response to a global epidemic’. Inter J Infect Dis. 2018;75:118–12.
4. Uplekar M, Weil D, Lonnroth K, et al. WHO’s new end TB strategy. Lancet. 2015;385(9979):1799–1801.
5. Organization WH. Implementing the end TB strategy: the essentials. World Health Organization. 2015.
6. Floyd K, Glaziou P, Zumla A, Raviglione M. The global tuberculosis epidemic and progress in care, prevention, and research: an overview in year 3 of the End TB era. Lancet Respir Med. 2018;6(4):299–314.
7. Glaziou P, Floyd K, Raviglione MC. Global epidemiology of tuberculosis. In: Seminars in Respiratory and Critical Care Medicine: 2018. Thieme Medical Publishers; 2018:271–285.
8. Russom M, Woldu HG, Berhane A, Jeannetot DY, Stricker BH, Verhamme K. Effectiveness of a 6-month isoniazid on prevention of incident tuberculosis among people living with HIV in eritrea: a retrospective cohort study. Infect Dis Therapy. 2022;11(1):559–579.
9. Organization WH. Tuberculosis prevalence surveys: a handbook. World Health Organization. 2011.
10. Migambi P, Gasana M, Uwizeye CB, et al. Prevalence of tuberculosis in Rwanda: results of the first nationwide survey in 2012 yielded important lessons for TB control. PLoS One. 2020;15(4):e0231372. doi:10.1371/journal.pone.0231372
11. Organization WH. World health statistics 2018: monitoring health for the SDGs, sustainable development goals. In: Possibilities of Addressing Suicide in the Family Health Strategy. Geneva: WHO;2018.
12. Sebhatu M, Kiflom B, Seyoum M, et al. Determining the burden of tuberculosis in Eritrea: a new approach. BulletinWorld Health Organiz. 2007;85(8):593–599.
13. Dangisso MH, Datiko DG, Lindtjørn B. Spatio-temporal analysis of smear-positive tuberculosis in the Sidama Zone, southern Ethiopia. PLoS One. 2015;10(6):e0126369.
14. Masabarakiza P, Hassaan MA. Spatial-temporal analysis of tuberculosis incidence in Burundi using GIS. J Public Health. 2019;5(6):280–286.
15. Titosse AC, Pimenta Rodrigues MV, Marques Ramos AP, et al. Tuberculosis space-temporal distribution from 2011 to 2016 in the municipality of Maputo, Mozambique. Población y Salud En Mesoamérica. 2021;18(2):270–300.
16. Sadeq M, Bourkadi JE. Spatiotemporal distribution and predictors of tuberculosis incidence in Morocco. Infect Diseases Poverty. 2018;7(1):1–13. doi:10.1186/s40249-018-0429-0
17. Kiani B, Raouf Rahmati A, Bergquist R, et al. Spatio-temporal epidemiology of the tuberculosis incidence rate in Iran 2008 to 2018. BMC Public Health. 2021;21(1):1–20. doi:10.1186/s12889-021-11157-1
18. Murray CJ, Ortblad KF, Guinovart C, et al. Global, regional, and national incidence and mortality for HIV, tuberculosis, and malaria during 1990–2013: a systematic analysis for the global burden of disease study 2013. Lancet. 2014;384(9947):1005–1070.
19. Glaziou P. Predicted impact of the COVID-19 pandemic on global tuberculosis deaths in 2020. MedRxiv. 2021;4:2020–04.
20. Diefenbach-Elstob T, Guernier-Cambert V, Gula B, et al. Spatial distribution of tuberculosis in a rural region of Western Province, Papua New Guinea. Western Pacific Surveillance Response J. 2019;10(4):31. doi:10.5365/wpsar.2019.10.2.001
21. Steingart KR, Ng V, Henry M, et al. Sputum processing methods to improve the sensitivity of smear microscopy for tuberculosis: a systematic review. Lancet Infect Dis. 2006;6(10):664–674. doi:10.1016/S1473-3099(06)70602-8
22. Steingart KR, Henry M, Laal S, et al. Commercial serological antibody detection tests for the diagnosis of pulmonary tuberculosis: a systematic review. PLoS Med. 2007;4(6):e202.
23. Bates M, O’Grady J, Maeurer M, et al. Assessment of the Xpert MTB/RIF assay for diagnosis of tuberculosis with gastric lavage aspirates in children in sub-Saharan Africa: a prospective descriptive study. Lancet Infect Dis. 2013;13(1):36–42.
24. Kawatsu L, Uchimura K, Ohkado A, Isaakidis P. Trend and treatment status of latent tuberculosis infection patients in Japan – analysis of Japan TB Surveillance data. PLoS One. 2017;12(11):e0186588. doi:10.1371/journal.pone.0186588
25. Dheda K, Gumbo T, Gandhi NR, et al. Global control of tuberculosis: from extensively drug-resistant to untreatable tuberculosis. Lancet Respir Med. 2014;2(4):321–338.
26. Ahuja SD, Ashkin D, Avendano M, et al. Multidrug resistant pulmonary tuberculosis treatment regimens and patient outcomes: an individual patient data meta-analysis of 9,153 patients. 2012.
27. Bhushan B, Kajal N, Maske A, Singh S. Manifestations of tuberculosis in elderly versus young hospitalised patients in Amritsar, India. Int J Tuberc Lung Dis. 2012;16(9):1210–1213.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Scoping Review on the Status of Female Breast Cancer in Asia with a Special Focus on Nepal
Dhakal R, Noula M, Roupa Z, Yamasaki EN
Breast Cancer: Targets and Therapy 2022, 14:229-246
Published Date: 26 August 2022
Assessment of the Prevalence and Incidence of COVID-19 in Saudi Arabia
Alyahyawi HE, Alharbi RA, Alatawi SK, Ahmed WAM, Almalki SSR
Journal of Multidisciplinary Healthcare 2023, 16:227-236
Published Date: 24 January 2023
Global Burden of Asthma, and Its Impact on Specific Subgroups: Nasal Polyps, Allergic Rhinitis, Severe Asthma, Eosinophilic Asthma
Rabe APJ, Loke WJ, Gurjar K, Brackley A, Lucero-Prisno III DE
Journal of Asthma and Allergy 2023, 16:1097-1113
Published Date: 6 October 2023
Type 2 Diabetes, the Epidemic: Trends in Prevalence and Incidence, 2004-2020
Overbeek JA, Nijpels G, Swart KMA, Blom MT, Elders PJM, Herings RMC
Diabetes, Metabolic Syndrome and Obesity 2024, 17:1503-1509
Published Date: 28 March 2024
From Pain to Progress: Comprehensive Analysis of Musculoskeletal Disorders Worldwide
Zhou J, Xie S, Xu S, Zhang Y, Li Y, Sun Q, Zhang J, Zhao T
Journal of Pain Research 2024, 17:3455-3472
Published Date: 24 October 2024