Back to Journals » Journal of Pain Research » Volume 19
Efficacy of Cognitive Behavioral Therapy Combined with Exercise in Patients with Chronic Pain: A Systematic Review and Meta-Analysis
Authors Zhang YZ, Yang B, Jiang CH, Guo YX, Lai XX, Zhang WQ, Zhang H ![]()
Received 30 January 2026
Accepted for publication 14 April 2026
Published 23 April 2026 Volume 2026:19 599315
DOI https://doi.org/10.2147/JPR.S599315
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Rocío de la Vega
Yi-Zhao Zhang,1,2 Biao Yang,1,2 Cheng-Hao Jiang,3 Yu-Xuan Guo,4 Xin-Xin Lai,5 Wei-Qiang Zhang,1 He Zhang1,2
1Department of Physical Education, Central South University, Changsha, Hunan, People’s Republic of China; 2Sports Rehabilitation and Sports Risk Prevention and Control Research Center, Central South University, Changsha, Hunan, People’s Republic of China; 3Department of Sports Science and Physical Education, The Chinese University of Hong Kong, Hong Kong, People’s Republic of China; 4College of Physical Education and Sports, Beijing Normal University, Beijing, People’s Republic of China; 5School of Physical Education, Shandong University, Jinan, Shandong, People’s Republic of China
Correspondence: He Zhang; Wei-Qiang Zhang, Department of Physical Education, Central South University, No. 932 Lushan South Road, Changsha, Hunan, 410083, People’s Republic of China, Email [email protected]; [email protected]
Purpose: To evaluate the effects of cognitive behavioral therapy (CBT) combined with exercise on multidimensional outcomes in adults with chronic pain, and to examine whether these effects were sustained at 3-, 6-, and 12-month follow-up.
Patients and methods: PubMed, Embase, Web of Science, the Cochrane Library, and PsycINFO were searched from inception to December 30, 2025. Randomized controlled trials (RCTs) comparing CBT combined with exercise versus usual care or other control interventions were included.
Results: Thirteen RCTs involving 1679 participants were included. Compared with controls, CBT combined with exercise produced small-to-moderate improvements in pain intensity and functional disability, although heterogeneity was observed across studies. Specifically, significant improvements were observed in pain intensity (SMD = − 0.44, 95% CI: [− 0.72, − 0.16], P = 0.002), functional disability (SMD = − 0.41, 95% CI: [− 0.68, − 0.15], P = 0.002), pain catastrophizing (MD = − 4.35, 95% CI: [− 7.13, − 1.56], P = 0.002), pain self-efficacy (SMD = 0.30, 95% CI: [0.09, 0.51], P = 0.005), fear of movement (MD = − 1.87, 95% CI: [− 3.02, − 0.72], P = 0.001), anxiety (SMD = − 0.29, 95% CI: [− 0.46, − 0.12], P = 0.0007), depression (SMD = − 0.27, 95% CI: [− 0.42, − 0.12], P = 0.0003), and quality of life (PCS: SMD = 0.26, 95% CI: [0.01, 0.50], P = 0.04; MCS: SMD = 0.23, 95% CI: [0.08, 0.38], P = 0.002). No significant improvements were observed in physical performance assessed by the Timed Up and Go Test (TUG) and 6-Minute Walk Test (6MWT). Improvements in pain intensity and functional disability were maintained at 3- and 6-month follow-up, whereas effects on other outcomes were less consistent and were mostly no longer evident at 12 months.
Conclusion: CBT combined with exercise is a feasible multidisciplinary strategy for adults with chronic pain, yielding small-to-moderate improvements in pain intensity and functional disability, with benefits maintained at 3- and 6-month follow-up. Cognitive-behavioral outcomes, mental health, and quality of life also improved, but their long-term maintenance was limited. No significant benefits were observed in physical performance. Future research requires standardized CBT-exercise protocols and broader population representation.
Keywords: chronic pain, cognitive behavioral therapy, exercise, systematic review, meta-analysis
A Letter to the Editor has been published for this article.
A Response to Letter by Mr Hu has been published for this article.
Introduction
Chronic pain is a clinical syndrome characterized by persistent or recurrent pain, commonly defined as pain lasting more than 3 months.1 It is associated with profound effects on physical function, mental health, and social participation.2–4 Epidemiological evidence indicates that chronic pain is a major public health burden worldwide.5 In the United States, 24.3% of adults experienced chronic pain and 8.5% experienced high-impact chronic pain in 2023.6 Its etiology and maintenance involve not only peripheral and central neural alterations but also intricate interactions among emotional, cognitive, and behavioral factors, reflecting its typical biopsychosocial nature.7,8 Traditional biomedical approaches that rely primarily on pharmacological treatments often struggle to provide sustained and comprehensive benefits. Consequently, the clinical management of chronic pain has shifted towards multidisciplinary, integrated intervention strategies aimed at promoting functional recovery and overall health improvement.9
Exercise is recommended as a safe and feasible non-pharmacological component of chronic pain management, with evidence demonstrating its capacity to alleviate pain severity, restore physical function, and enhance quality of life.10,11 However, the efficacy of exercise is frequently compromised by maladaptive psychological factors—such as pain-related fear, catastrophic thinking, and avoidance behaviors.12,13 These factors reduce adherence to exercise regimens, potentially exacerbating physical deconditioning. Cognitive behavioral therapy, grounded in the biopsychosocial framework, effectively targets these maladaptive cognitions, improves coping strategies, and fosters pain self-efficacy.14,15 Yet, while CBT outperforms usual care in reducing disability, evidence suggests its benefits may attenuate over time.16 Thus, as monotherapies, both exercise and CBT exhibit limitations, necessitating a more comprehensive approach.
Recent studies have supported the potential value of multidisciplinary approaches for chronic pain management.9,17 Among these interventions, CBT combined with exercise has received increasing attention. Study reported sustained improvements in functional status in patients with chronic low back pain compared with usual care.18 The combined intervention also demonstrated superior outcomes in pain intensity, pain-related fear, and pain self-efficacy.19 However, existing studies vary in intervention protocols, comparative conditions, and follow-up durations. To date, the previous review has reported high heterogeneity in pooled effect sizes and has failed to demonstrate robust superiority of CBT combined with exercise across certain outcomes.20
Therefore, this systematic review and meta-analysis adopted a clearer definition of CBT based on core cognitive-behavioral elements, and conducted more detailed pre-specified subgroup analyses. It aimed to determine whether CBT combined with exercise is more effective than usual care or other non-pharmacological control interventions for adults with chronic pain, and whether these effects are sustained across different follow-up periods. This more focused synthesis of both efficacy and durability may help inform evidence-based multidisciplinary strategies for chronic pain management.
Methods
Study Design and Protocol Registration
This systematic review and meta-analysis was conducted and reported in accordance with the PRISMA 2020 (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement.21 The study protocol was prospectively registered in PROSPERO (CRD420251266911) to ensure transparency and methodological rigor.
Search Strategy
We systematically searched PubMed, Embase, Web of Science, the Cochrane Library, and PsycINFO from inception to December 30, 2025. The search strategy combined controlled vocabulary terms (eg, MeSH/Emtree) with free-text terms reflecting key concepts, including “chronic pain”, “exercise” or “physical activity”, and “cognitive behavioral therapy”, with database-specific adaptations The primary search terms included chronic pain, musculoskeletal pain, exercise, physical activity, cognitive behavioral therapy, and randomized controlled trial In accordance with the methodological recommendations of Bramer et al,22 we performed supplementary searches in Google Scholar and manually screened the reference lists of included studies and relevant systematic reviews to minimize omissions The complete search strategy is provided in Supplementary Table S1.
Eligibility Criteria
Eligibility criteria were defined according to the PICOS framework. Studies were included if they met all of the following criteria: (1) participants were adults aged ≥ 18 years; (2) participants met the International Association for the Study of Pain (IASP) diagnostic criteria for chronic pain (pain duration ≥ 3 months);1 (3) the study employed a randomized controlled trial design; (4) the intervention group received cognitive behavioral therapy combined with exercise, in which the CBT component was grounded in CBT principles and included one or more core CBT elements (eg, pain education/cognitive understanding, cognitive restructuring, behavioral activation/exposure training, coping skills/problem-solving training, self-efficacy/self-management training, and structured protocol/relapse prevention),23,24 and the exercise followed a defined program; (5) the control group received usual care, wait-list control, or other non-pharmacological interventions (eg, exercise alone or CBT alone); and (6) the study reported at least one continuous outcome suitable for meta-analysis, including pain intensity, functional disability, pain catastrophizing, pain self-efficacy, fear of movement, anxiety, depression, quality of life (physical component summary and mental component summary), or physical performance (Timed Up and Go test or 6-Minute Walk Test).
Studies were excluded if any of the following criteria were met: (1) participants were minors or pregnant women; (2) the type of pain was acute/subacute, or cancer-related pain; (3) participants had experienced relevant surgery within 3 months prior to enrollment, had major physical illnesses, or had severe psychiatric disorders that were explicitly listed as exclusion criteria; (4) the psychological intervention consisted solely of general health education and was not based on CBT principles; (5) the original data required for meta-analysis were unavailable and could not be obtained; or (6) only statistically adjusted results were reported without raw data.
Study Selection and Data Extraction
Study selection and data extraction were independently conducted by two researchers (YXG and CHJ). Initially, titles and abstracts were screened against the inclusion and exclusion criteria, followed by full-text assessment of potentially eligible studies. Disagreements were resolved through discussion, with a third researcher (HZ) consulted when necessary.
A standardized data extraction form was used for all included studies. When reported data were incomplete or unclear, corresponding authors were contacted, or data were extracted from figures using GetData Graph Digitizer. Extracted information included first author, publication year, country, type of pain, sample size, sample age, intervention format, CBT provider, intervention content, intervention frequency, follow-up time, and outcome measurement tools. Assessment time points were extracted and categorized based on the timing reported in the original studies as post-intervention or follow-up. Post-intervention assessments were conducted immediately after the intervention, whereas follow-up assessments were grouped into 3-, 6-, and 12-month categories to distinguish short-, mid-, and long-term maintenance effects and improve comparability across studies. Detailed information on outcomes and measurement tools used in the included studies is provided in Supplementary Table S2.
Statistical Analysis
Statistical analyses were conducted using Review Manager 5.4 and StataMP 16. All outcomes were continuous variables, and changes from baseline to post-intervention or follow-up were analyzed. Effect sizes were expressed as mean differences (MDs) or standardized mean differences (SMDs) with 95% confidence intervals (CIs), depending on whether the same measurement tools were used.
Statistical heterogeneity was assessed using the I2 statistic. A fixed-effects model was applied when I2 ≤ 50%, whereas a random-effects model was used when I2 > 50%. For outcomes exhibiting substantial heterogeneity, pre-specified subgroup analyses were performed to explore potential sources of heterogeneity. Subgroup analyses were stratified by region, intervention delivery format, CBT provider, CBT core elements, and exercise type, which were pre-specified as potential sources of heterogeneity.
For multi-arm trials, shared control groups were split proportionally in accordance with recommendations from the Cochrane Handbook, while retaining the original group means and standard deviations.25 When the sample size of a shared control group was odd, the additional participant was allocated to the control group with the fewest intervention components. All statistical tests were two-sided, and P < 0.05 was considered statistically significant. Leave-one-out sensitivity analyses were conducted to assess the robustness of the pooled results.
Risk of Bias Assessment
Risk of bias was independently assessed by two researchers (YXG and CHJ) using the Cochrane Risk of Bias tool, version 2.0 (RoB 2).26 Any disagreements were resolved through discussion, with a third researcher (HZ) consulted for adjudication. The RoB 2 tool evaluates five domains of bias: (1) randomization process; (2) deviations from the intended interventions; (3) missing outcome data; (4) measurement of the outcome; (5) selection of the reported result. Each domain was judged based on signaling questions, and an overall risk of bias assessment of “low risk”, “some concerns”, or “high risk” was assigned.
Certainty of Evidence Assessment
The certainty of evidence for the main post-intervention outcomes, including pain intensity, functional disability, pain catastrophizing, pain self-efficacy, and depression, was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. The assessment was conducted across the GRADE domains of risk of bias, inconsistency, indirectness, imprecision, and publication bias, with other considerations documented when applicable. Each outcome was rated as high, moderate, low, or very low certainty. The evaluation was independently conducted by two researchers (YXG and CHJ), with disagreements resolved through discussion and consultation with a third researcher (HZ) when necessary.
Publication Bias
Potential publication bias was assessed qualitatively using funnel plots. When at least 10 studies were available for an outcome, Egger’s test was performed for quantitative evaluation. A P value > 0.05 was considered to indicate no statistical evidence of significant publication bias.
Results
Study Selection
The study selection process is shown in Figure 1. A total of 6942 records were identified through systematic searches of the predefined databases. After removal of duplicates using EndNote, 5420 records remained. Following title and abstract screening, 49 studies were retrieved for full-text assessment. Of these, several were excluded because of ineligible study design, study population, pain type, or insufficient data for effect size calculation. In addition, screening of reference lists from relevant studies and systematic reviews identified five additional records, all of which were excluded after full-text evaluation. Finally, 13 RCTs were included in the review. Because some studies employed multi-arm designs, a total of 16 independent comparisons were included in the meta-analysis.
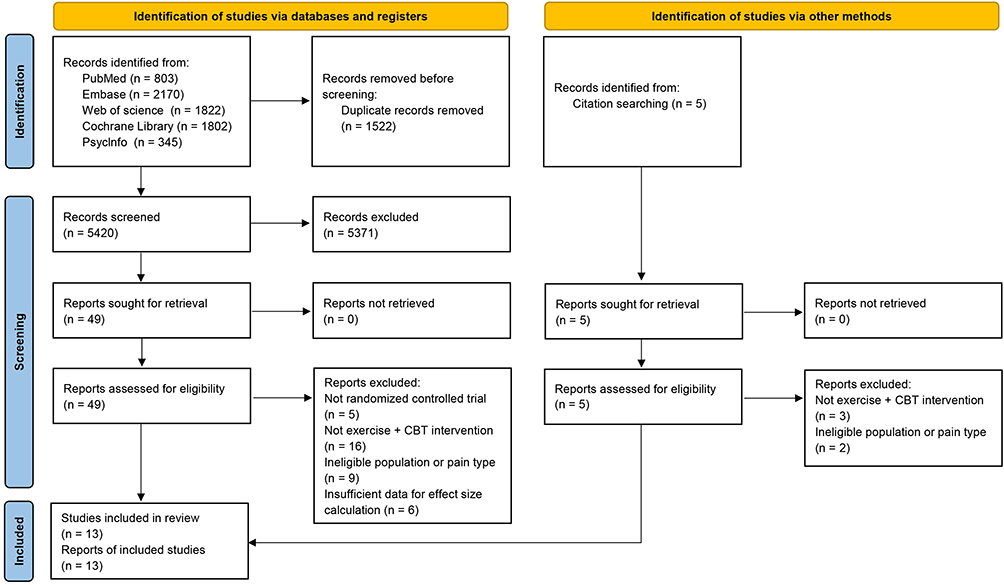 |
Figure 1 PRISMA flow diagram of study selection for the systematic review and meta-analysis. |
Study Characteristics
The main characteristics of the included studies are summarized in Table 1. This systematic review and meta-analysis included 13 randomized controlled trials, yielding 16 independent comparisons and involving a total of 1679 patients with chronic pain. The studies were conducted across diverse regions, including Africa (n = 1), Asia (n = 4), Europe (n = 7), and both Asia and Europe (n = 1). With respect to pain conditions, five studies focused on chronic low back pain, two on fibromyalgia, and one each on chronic whiplash-associated disorders, chronic musculoskeletal pain, and chronic neck pain, while three studies did not specify the pain type. Intervention duration ranged from 4 to 16 weeks. Six studies implemented individual-based interventions, whereas seven employed group-based formats. Regarding CBT providers, five studies were provided by psychologists, while the remaining studies were conducted by physical therapists or researchers. Eight studies included all six CBT core elements, whereas five used partial or CBT-informed approaches. Follow-up assessments were reported at 3 months (n = 5), 6 months (n = 5), and 12 months (n = 3). Further details of the combined interventions, including providers, frequency, and intervention content, are presented in Supplementary Table S3.
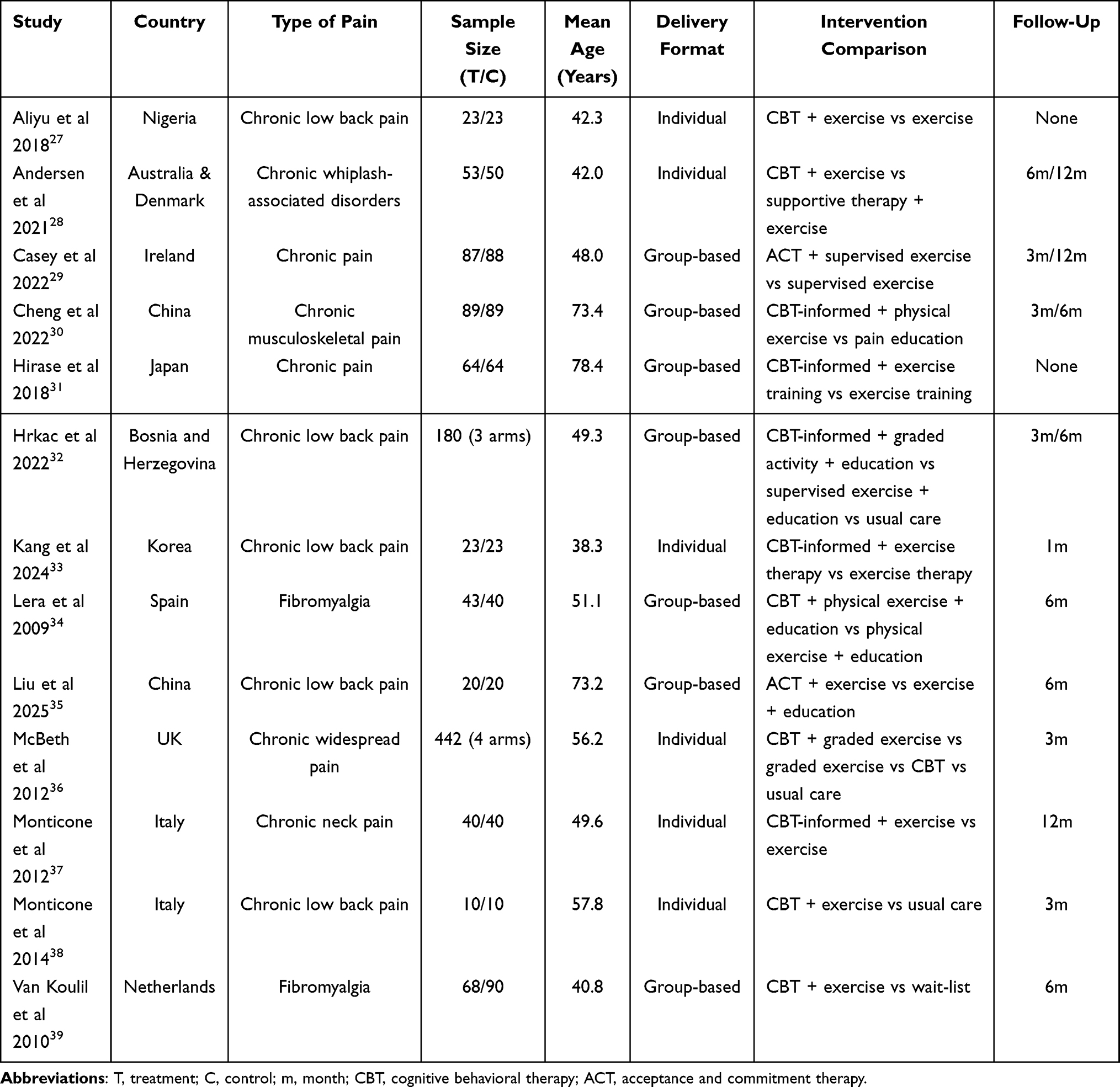 |
Table 1 Characteristics of Included Studies |
Risk of Bias Assessment
Overall, the included studies exhibited low to moderate risk of bias (Figure 2). Among the 13 studies, six were judged to be at low risk, six were rated as having some concerns, and one as high risk. Concerns mainly related to the randomization process and outcome measurement due to insufficient reporting of allocation concealment and unclear blinding of outcome assessors. In addition, several studies showed some concerns regarding deviations from the intended interventions. Only one study was judged to be at high risk overall, primarily because of a high risk of bias in the deviations from intended interventions domain. The remaining studies generally performed well with respect to missing outcome data and selection of the reported results.
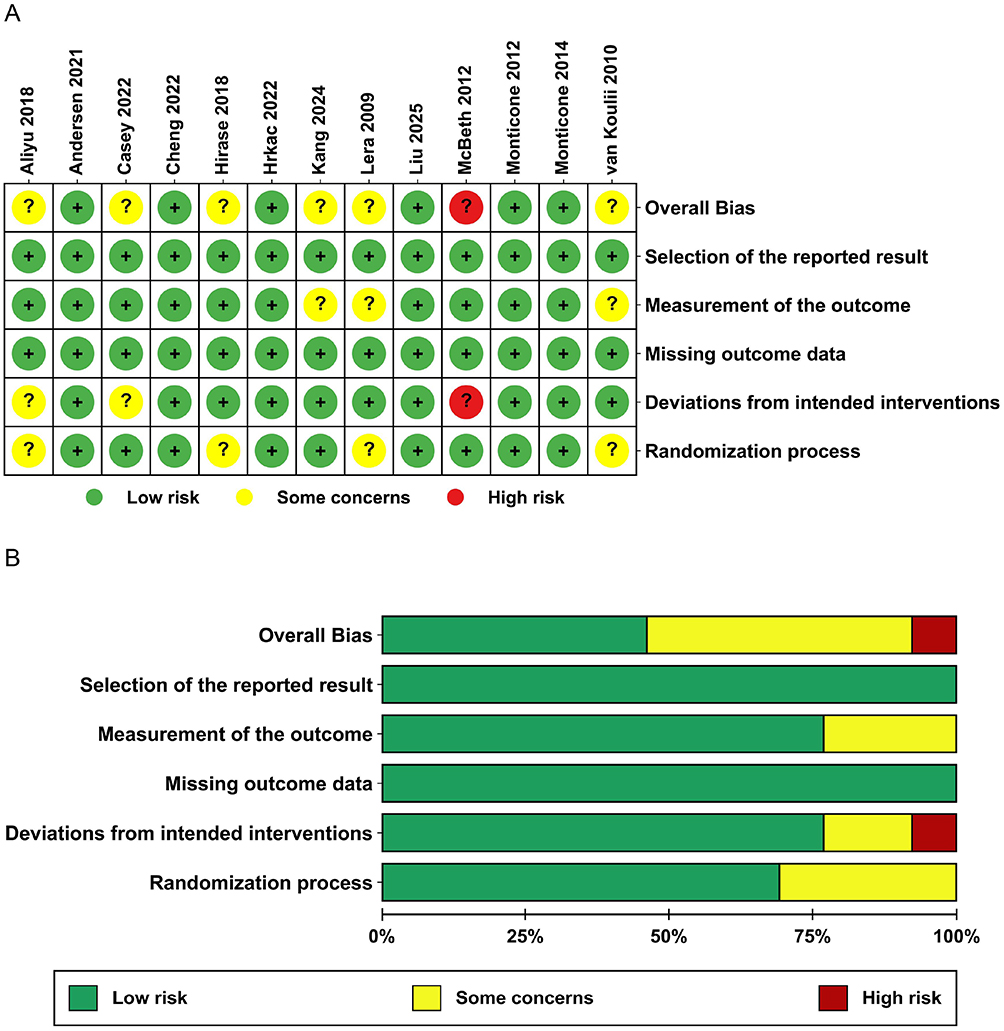 |
Figure 2 Risk of bias assessment of included studies. (A) Risk of bias summary for each study by domain; (B) Risk of bias graph. |
Effects of the Combined Intervention
Pain Intensity
Eleven randomized controlled trials involving 1019 participants reported pain intensity (Figure 3a). Meta-analysis showed that, compared with the control group, cognitive behavioral therapy combined with exercise significantly reduced pain intensity in patients with chronic pain (SMD = −0.44, 95% CI: [−0.72, −0.16], P = 0.002), although substantial heterogeneity was observed (I2 = 77%).
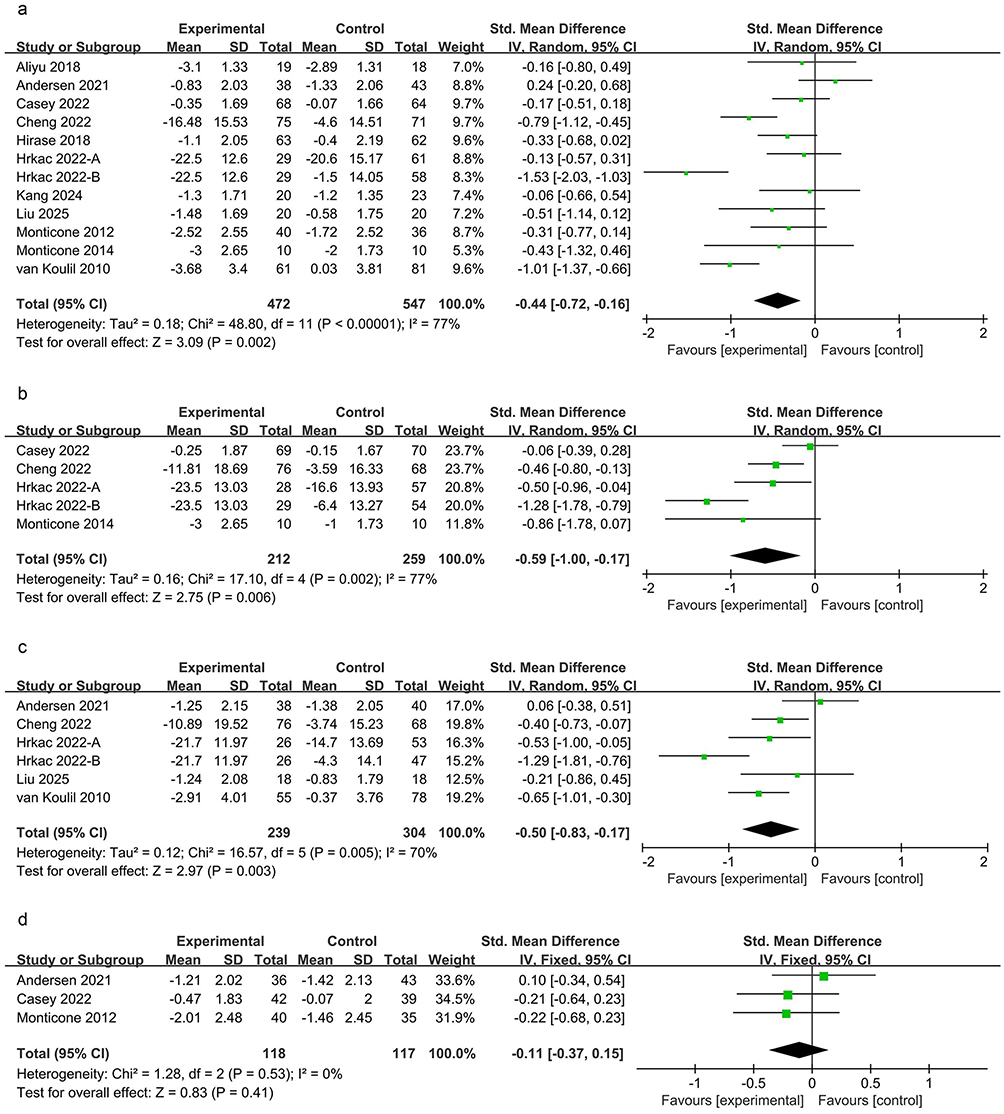 |
Figure 3 Forest plots of pain intensity. (a) Post-intervention; (b) 3-month follow-up; (c) 6-month follow-up; (d) 12-month follow-up. |
Follow-up analyses indicated that the combined intervention maintained statistically significant effects at both short-term and mid-term follow-up. Specifically, pain intensity was significantly reduced at the 3-month follow-up (SMD = −0.59, 95% CI: [−1.00, −0.17], P = 0.006, I2 = 77%; Figure 3b) and at the 6-month follow-up (SMD = −0.50, 95% CI: [−0.83, −0.17], P = 0.003, I2 = 70%; Figure 3c). However, no statistically significant difference in pain intensity was observed at the 12-month follow-up (SMD = −0.11, 95% CI: [−0.37, 0.15], P = 0.41, I2 = 0%; Figure 3d).
Functional Disability
A total of nine RCTs involving 762 patients with chronic pain reported functional disability (Figure 4a). The results showed that, compared with the control group, cognitive behavioral therapy combined with exercise significantly improved functional disability in patients with chronic pain (SMD = −0.41, 95% CI: [−0.68, −0.15], P = 0.002), with substantial heterogeneity among studies (I2 = 66%).
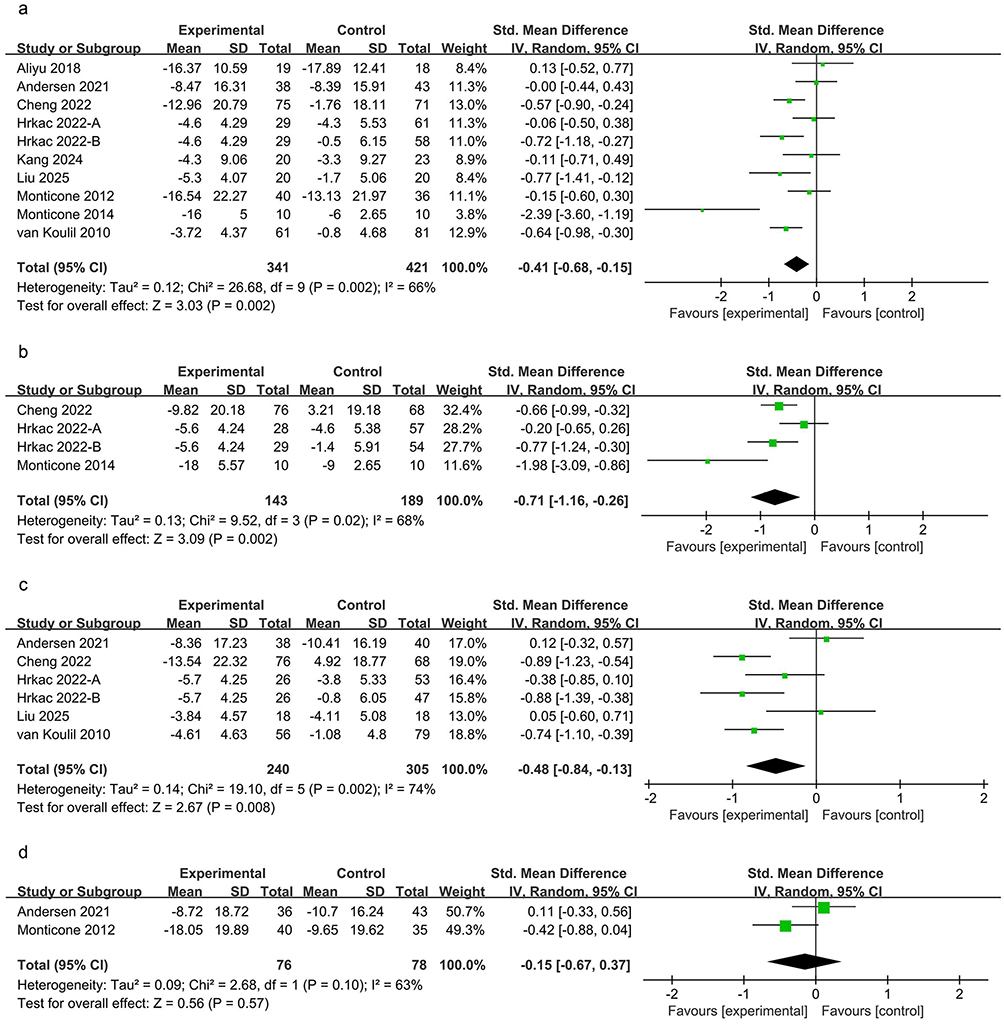 |
Figure 4 Forest plots of functional disability. (a) Post-intervention; (b) 3-month follow-up; (c) 6-month follow-up; (d) 12-month follow-up. |
Follow-up analyses showed that the combined intervention maintained significant improvements in functional disability at both short-term and mid-term follow-up. At the 3-month follow-up, functional disability was significantly reduced (SMD = −0.71, 95% CI: [−1.16, −0.26], P = 0.002, I2 = 68%; Figure 4b), and a significant difference was also observed at the 6-month follow-up (SMD = −0.48, 95% CI: [−0.84, −0.13], P = 0.008, I2 = 74%; Figure 4c). However, no statistically significant difference in functional disability was observed between groups at the 12-month follow-up (SMD = −0.15, 95% CI: [−0.67, 0.37], P = 0.57, I2 = 63%; Figure 4d).
Cognition and Behavior
Six randomized controlled trials involving 537 participants reported pain catastrophizing (Figure 5a). Meta-analysis showed that, compared with the control group, cognitive behavioral therapy combined with exercise significantly decreased catastrophizing in patients with chronic pain (MD = −4.35, 95% CI: [−7.13, −1.56], P = 0.002), although substantial heterogeneity was observed (I2 = 67%). Follow-up analyses indicated that the combined intervention significantly decreased catastrophizing at the 6-month follow-up (MD = −2.44, 95% CI: [−4.57, −0.31], P = 0.02, I2 = 0%; Figure 5c) and the 12-month follow-up (MD = −4.36, 95% CI: [−8.23, −0.49], P = 0.03, I2 = 0%; Figure 5d). No significant effects were observed at the 3-month follow-up (MD = −4.95, 95% CI: [−10.21, 0.31], P = 0.07, I2 = 85%; Figure 5b).
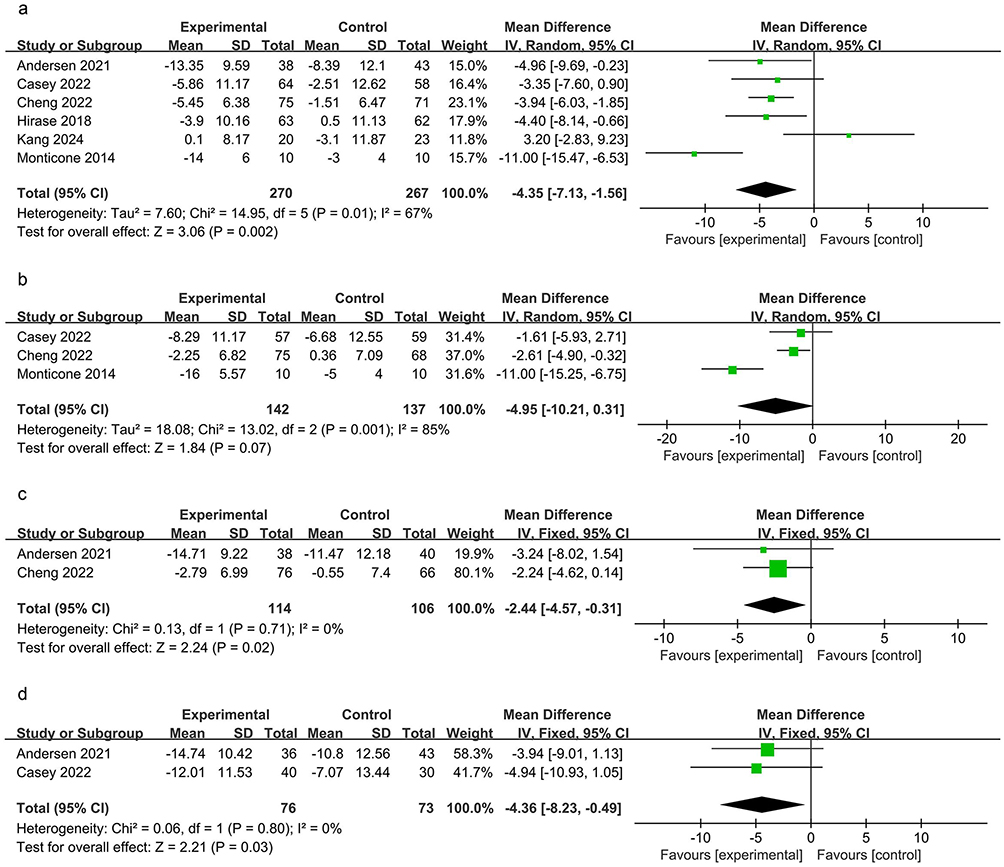 |
Figure 5 Forest plots of pain catastrophizing. (a) Post-intervention; (b) 3-month follow-up; (c) 6-month follow-up; (d) 12-month follow-up. |
Pain self-efficacy was reported in three studies involving 357 patients (Figure 6a). The pooled results indicated that the combined intervention significantly improved pain self-efficacy (SMD = 0.30, 95% CI: [0.09, 0.51], P = 0.005), with no evidence of heterogeneity among studies (I2 = 0%). Follow-up analyses showed that a statistically significant improvement in pain self-efficacy was observed only at the 3-month follow-up (SMD = 0.34, 95% CI: [0.10, 0.58], P = 0.005, I2 = 0%; Figure 6b). No significant differences were observed at the 6-month (SMD = 0.30, 95% CI: [−0.42, 1.03], P = 0.41, I2 = 85%; Figure 6c) or 12-month follow-up (SMD = 0.19, 95% CI: [−0.12, 0.51], P = 0.23, I2 = 0%; Figure 6d).
 |
Figure 6 Forest plots of pain self-efficacy. (a) Post-intervention; (b) 3-month follow-up; (c) 6-month follow-up; (d) 12-month follow-up. |
Four studies involving 576 participants reported fear of movement (Figure 7a). The pooled analysis showed that, compared with the control group, the combined intervention significantly reduced fear of movement in patients with chronic pain (MD = −1.87, 95% CI: [−3.02, −0.72], P = 0.001), with low heterogeneity among studies (I2 = 36%). Follow-up analyses indicated that the combined intervention remained effective at the 3-month follow-up (MD = −3.92, 95% CI: [−7.07, −0.78], P = 0.01, I2 = 84%; Figure 7b) and the 12-month follow-up (MD = −3.12, 95% CI: [−5.95, −0.29], P = 0.03, I2 = 0%; Figure 7c).
 |
Figure 7 Forest plots of fear of movement. (a) Post-intervention; (b) 3-month follow-up; (c) 12-month follow-up. |
Mental Health
Anxiety was reported in five studies involving 570 participants (Figure 8a). Meta-analysis showed that, compared with the control group, the combined intervention significantly alleviated anxiety in patients with chronic pain (SMD = −0.29, 95% CI: [−0.46, −0.12], P = 0.0007), with no evidence of heterogeneity (I2 = 0%). Follow-up analyses indicated that a statistically significant reduction in anxiety was observed only at the 6-month follow-up (SMD = −0.40, 95% CI: [−0.60, −0.19], P = 0.0001, I2 = 50%; Figure 8c). No statistically significant differences were observed at the 3-month follow-up (SMD = −0.13, 95% CI: [−0.36, 0.10], P = 0.27, I2 = 49%; Figure 8b) or the 12-month follow-up (SMD = −0.03, 95% CI: [−0.34, 0.28], P = 0.85, I2 = 0%; Figure 8d).
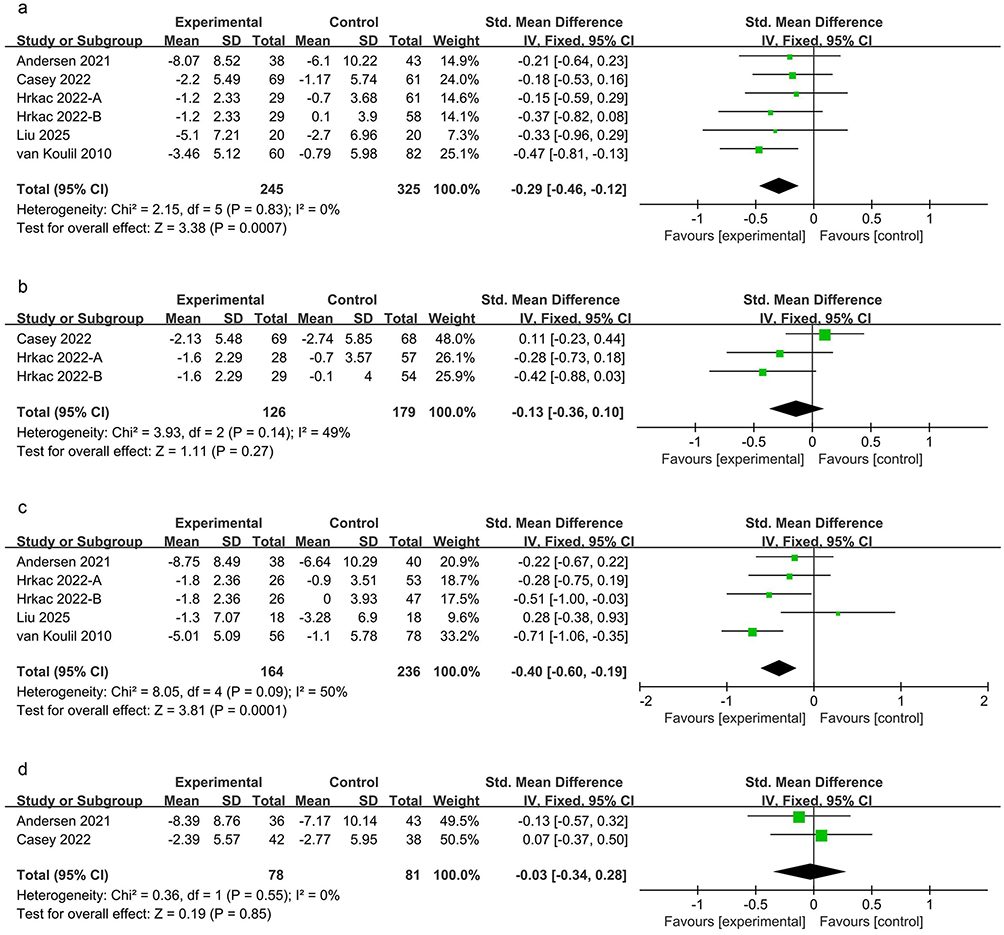 |
Figure 8 Forest plots of anxiety. (a) Post-intervention; (b) 3-month follow-up; (c) 6-month follow-up; (d) 12-month follow-up. |
Seven studies involving 743 patients reported depression (Figure 9a). The results showed that the combined intervention was associated with a significant reduction in depressive symptoms (SMD = −0.27, 95% CI: [−0.42, −0.12], P = 0.0003), with no observed heterogeneity (I2 = 0%). Follow-up analyses indicated that the beneficial effect of the combined intervention reached statistical significance only at the 3-month follow-up (SMD = −0.19, 95% CI: [−0.38, 0.00], P = 0.05, I2 = 0%; Figure 9b). No significant differences were observed at the 6-month (SMD = −0.17, 95% CI: [−0.37, 0.02], P = 0.08, I2 = 0%; Figure 9c) or 12-month follow-up (SMD = −0.10, 95% CI: [−0.42, 0.21], P = 0.52, I2 = 0%; Figure 9d).
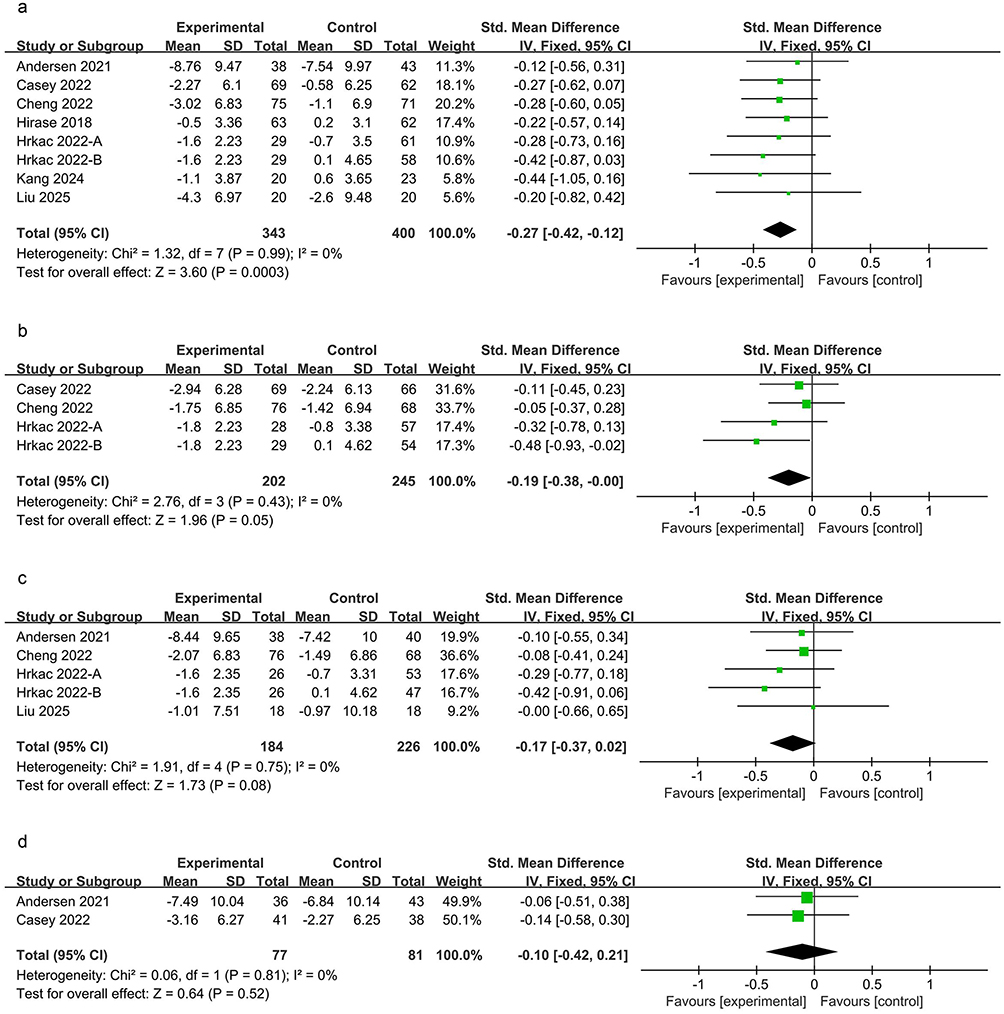 |
Figure 9 Forest plots of depression. (a) Post-intervention; (b) 3-month follow-up; (c) 6-month follow-up; (d) 12-month follow-up. |
Quality of Life
Quality of life outcomes, including the Physical Component Summary (PCS) and Mental Component Summary (MCS), were reported in five studies. For PCS (Figure 10a), cognitive behavioral therapy combined with exercise significantly improved physical health-related quality of life (SMD = 0.26, 95% CI: [0.01, 0.50], P = 0.04), with substantial heterogeneity (I2 = 64%). A significant improvement was also observed at the 3-month follow-up (SMD = 0.37, 95% CI: [0.06, 0.68], P = 0.02, I2 = 72%; Figure 10b). However, no significant improvement was detected at the 6-month follow-up (SMD = 0.39, 95% CI: [−0.18, 0.96], P = 0.18, I2 = 85%; Figure 10c).
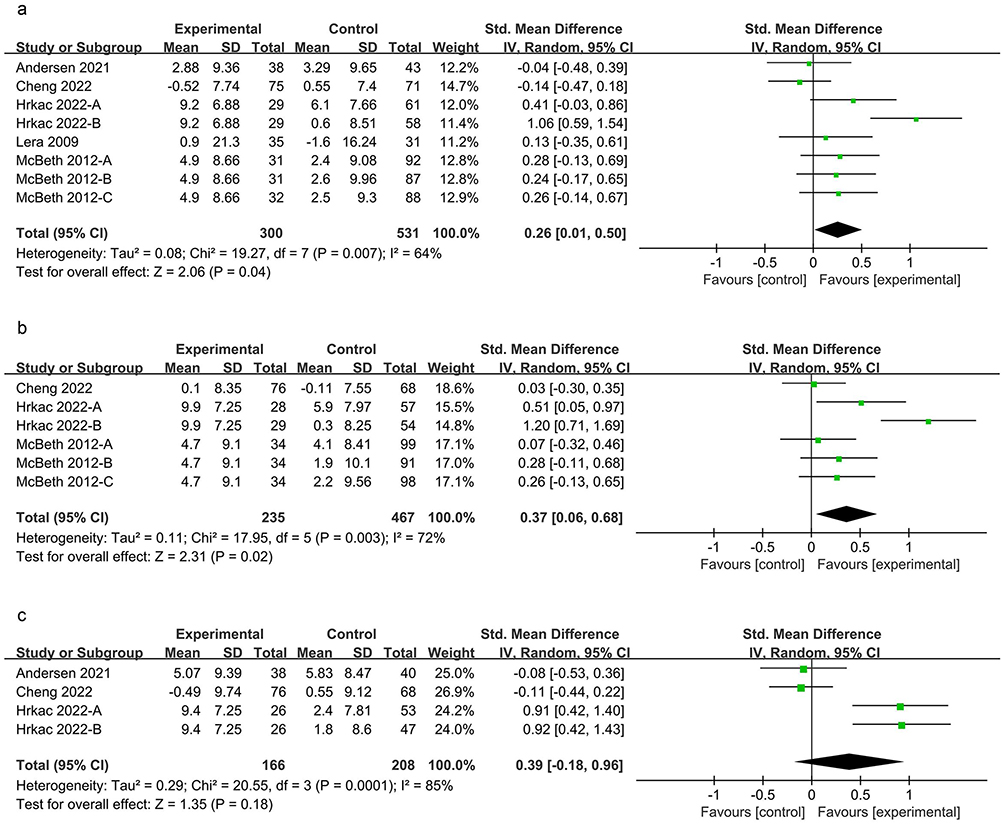 |
Figure 10 Forest plots of physical component summary (PCS) of quality of life. (a) Post-intervention; (b) 3-month follow-up; (c) 6-month follow-up. |
Regarding MCS (Figure 11a), the combined intervention was associated with a significant improvement in mental health-related quality of life (SMD = 0.23, 95% CI: [0.08, 0.38], P = 0.002, I2 = 41%). A significant improvement was also observed at the 6-month follow-up (SMD = 0.36, 95% CI: [0.16, 0.57], P = 0.0006, I2 = 47%; Figure 11c). In contrast, no statistically significant difference between groups was observed at the 3-month follow-up (SMD = 0.13, 95% CI: [−0.03, 0.29], P = 0.11, I2 = 50%; Figure 11b).
 |
Figure 11 Forest plots of mental component summary (MCS) of quality of life. (a) Post-intervention; (b) 3-month follow-up; (c) 6-month follow-up. |
Physical Performance
Among physical performance outcomes, the Timed Up and Go (TUG) test was reported in two studies involving 165 participants (Figure 12a), with no significant difference between groups (MD = −1.01, 95% CI: [−3.34, 1.31], P = 0.39, I2 = 80%). For the 6-Minute Walk Test (6MWT), two studies involving a total of 60 participants were included (Figure 12b). Similarly, the results showed no statistically significant difference (MD = 48.99, 95% CI: [−26.31, 124.29], P = 0.20, I2 = 73%).
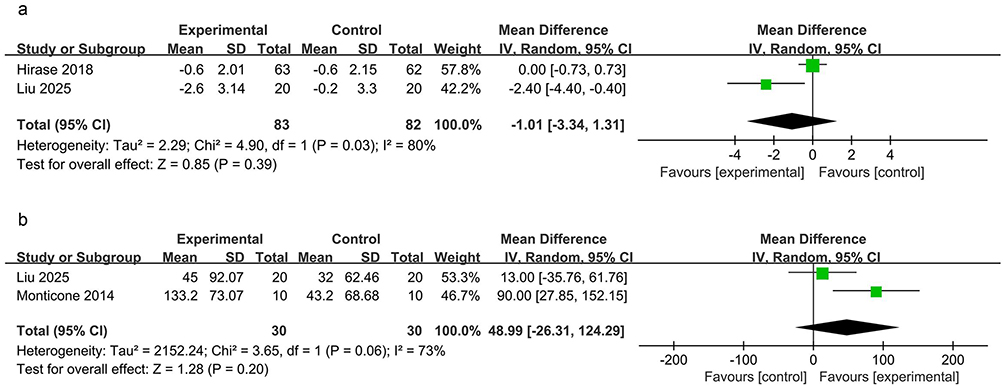 |
Figure 12 Forest plots of physical performance at post-intervention. (a) Timed Up and Go test (TUG); (b) Six-Minute Walk Test (6MWT). |
Subgroup Analyses
All subgroup analyses are presented in Table 2, with detailed forest plots for pain intensity, functional disability, and pain catastrophizing shown in Supplementary Figures S1–S3, respectively. Given the substantial heterogeneity observed for pain intensity, pre-specified subgroup analyses were conducted. The results indicated that: (1) after stratification by study region, the effects were directionally consistent between studies conducted in Asia and Europe, with no statistically significant difference between subgroups (P = 0.63); (2) a significant subgroup difference was observed by intervention delivery format (P = 0.01), with group-based interventions demonstrating larger effects than individual-based interventions; (3) stratification by CBT provider showed no statistically significant difference in pain intensity improvement between interventions delivered by psychologists and non-psychologists (P = 0.07); (4) subgroup analysis based on CBT core elements revealed no significant difference between standard CBT and CBT-informed interventions (P = 0.52); and (5) no significant difference was observed between multimodal exercise and single-mode exercise interventions (P = 0.88).
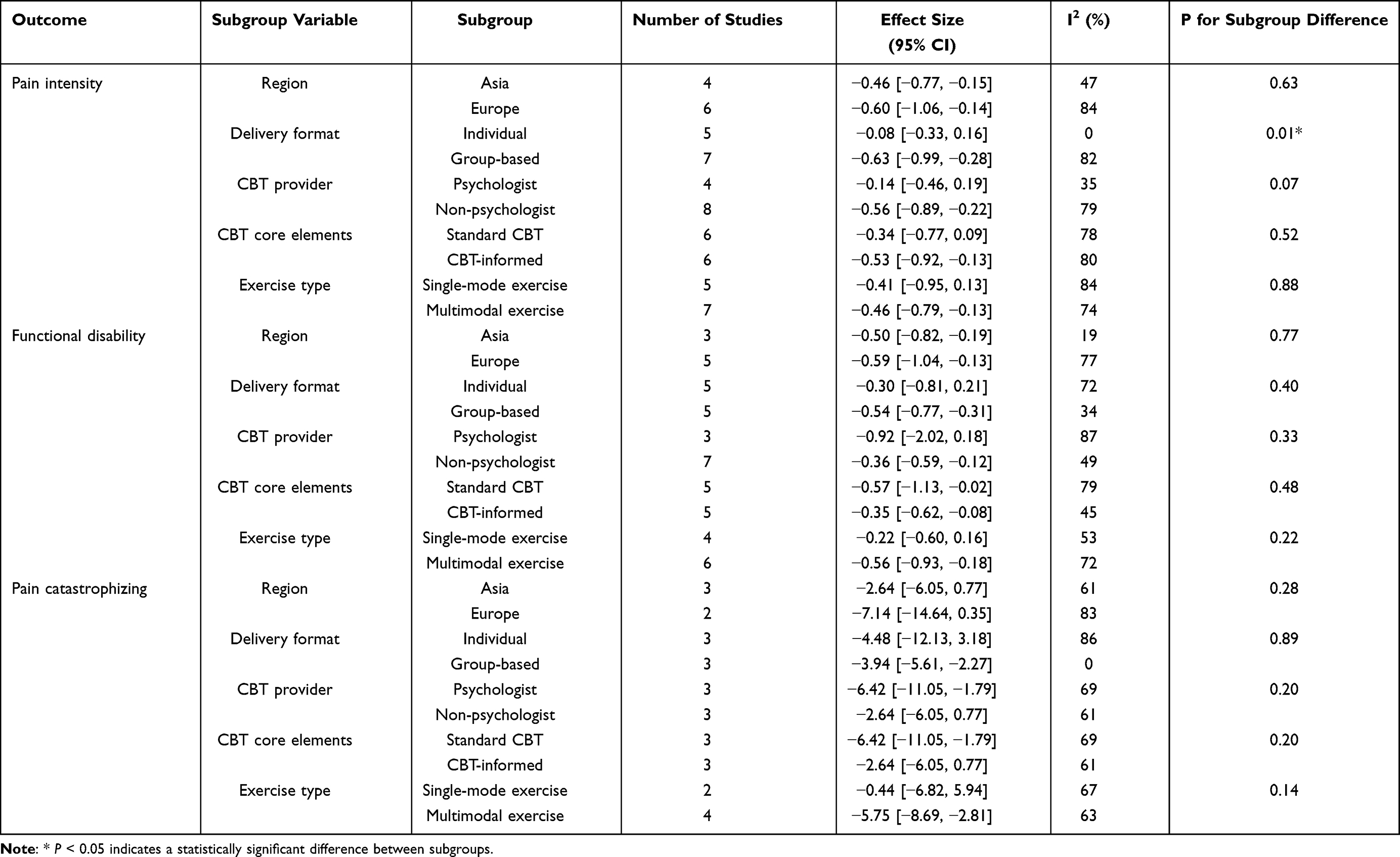 |
Table 2 Results of Subgroup Analysis |
For functional disability, the pooled results also exhibited substantial heterogeneity, prompting further subgroup analyses. These analyses showed that: (1) the effects from Asian and European studies were consistent, with no statistically significant differences between subgroups (P = 0.77); (2) the difference between group-based and individual-based interventions in improving functional disability did not reach statistical significance (P = 0.40); (3) no significant difference was observed between interventions delivered by psychologists and non-psychologists (P = 0.33); (4) no significant difference was detected between standard CBT and CBT-informed interventions (P = 0.48); and (5) differences in pooled effects by exercise type subgroups were not significant (P = 0.22).
Given the substantial heterogeneity observed in catastrophizing, pre-specified subgroup analyses were also performed. No significant differences were identified between subgroups defined by study region, intervention delivery format, CBT provider, CBT core elements, or exercise type.
Sensitivity Analyses
Leave-one-out analyses were performed to evaluate the robustness of the pooled results. The findings showed that the effects for pain intensity, functional disability, catastrophizing, fear of movement, anxiety, depression, and mental health-related quality of life (MCS) did not change substantially after sequentially excluding each study, indicating that the results for these outcomes were generally robust. In contrast, pain self-efficacy and physical health-related quality of life (PCS) were more sensitive to the influence of individual studies. Specifically, exclusion of Casey et al altered both the magnitude and direction of the pooled effects for pain self-efficacy, whereas exclusion of either Hrkac et al or McBeth et al changed the effects for PCS, suggesting that these two outcomes may be influenced by specific studies.
Publication Bias
For outcomes with at least 10 included studies, publication bias was further evaluated. Egger’s test indicated no statistical evidence of significant publication bias for either pain intensity (P = 0.714) or functional disability (P = 0.549). The corresponding funnel plots for publication bias assessment across outcomes are provided in Supplementary Figure S4.
Certainty of Evidence
The certainty of evidence for the five main post-intervention outcomes is summarized in Table 3. Overall, the certainty was moderate for pain intensity, functional disability, pain catastrophizing, and depression, and high for pain self-efficacy. Detailed GRADE assessments for these post-intervention outcomes, as well as the follow-up outcomes for pain intensity and functional disability, are provided in Supplementary Tables S4 and S5, respectively.
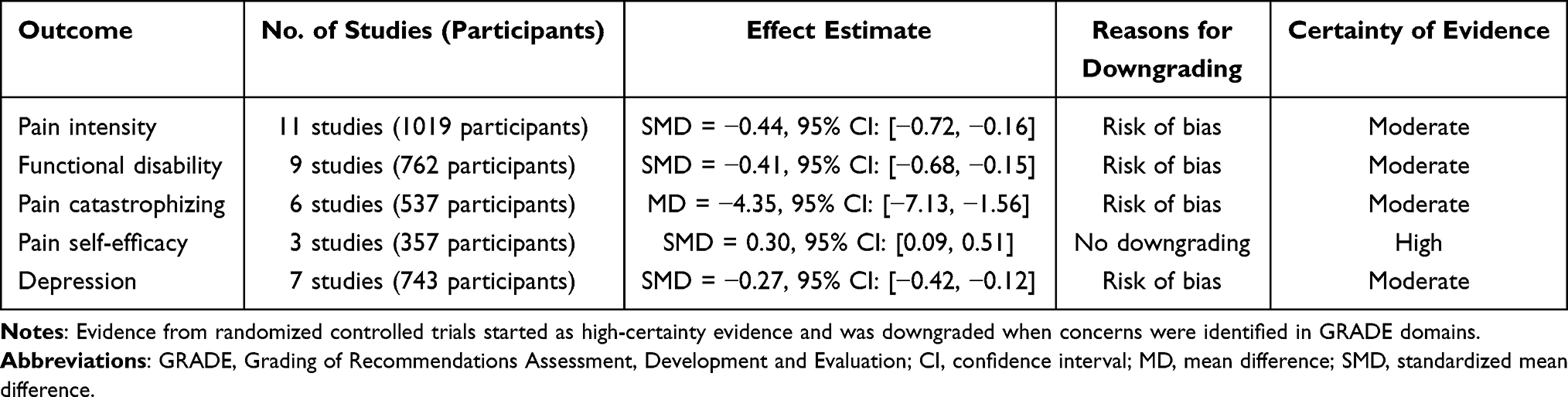 |
Table 3 Summary of GRADE Certainty of Evidence for Post-Intervention Outcomes |
Discussion
Cognitive behavioral therapy combined with exercise is increasingly recognized as a promising multimodal intervention for the clinical management of chronic pain. Our findings demonstrate that this combined approach yields significant improvements in pain intensity, functional disability, cognitive and behavioral outcomes, mental health, and quality of life. However, no significant benefit was observed regarding physical performance. In addition, the combined intervention exhibited sustained benefits in pain intensity, functional disability, and certain cognitive and behavioral outcomes at short- and mid-term follow-ups, whereas the maintenance of effects on mental health and quality of life was relatively limited. Notably, improvements among multiple outcomes tended to attenuate or dissipate during long-term follow-up. Our findings are consistent with previous reviews of multidisciplinary interventions for chronic pain and distinctively focus on the combined application of CBT and exercise. This provides more direct evidence for this multimodal strategy and further elucidates the persistence of its efficacy across different follow-up periods.9,20
This study indicated that the combined intervention showed significant improvements in pain intensity and functional disability among patients with chronic pain. Existing evidence suggests that pain experiences and functional limitations in chronic pain are closely linked to maladaptive cognitive patterns and avoidance behaviors. The combined intervention likely conferred clinical benefits by mitigating these threatening cognitions and avoidance responses.7,40–42 Specifically, CBT modulates pain-related catastrophizing and negative beliefs, thereby optimizing the patient’s cognitive processing of pain.43,44 Concurrently, exercise reduces pain-related avoidance through structured and progressive physical activities, fostering a gradual re-engagement in daily living.45 Thus, by facilitating behavioral changes built upon cognitive restructuring, the combined approach synergistically promotes pain relief and functional recovery. Follow-up analyses further showed that improvements in pain intensity and functional disability were maintained at short- and mid-term follow-up but did not persist at long-term follow-up. These findings suggest that the benefits of the combined intervention may remain stable for a limited period but tend to attenuate over time or fail to persist in the absence of continued intervention or maintenance strategies.
Improvements in cognitive and behavioral outcomes were also observed in this study. Pain catastrophizing is commonly defined as a maladaptive response to pain, characterized by an exaggerated negative appraisal, magnification of pain-related symptoms, persistent pain-related worry, and feelings of helplessness in coping with pain.46 Cognitive-behavioral theory and the fear-avoidance model provide theoretical foundations for understanding its formation and maintenance.47,48 Accordingly, the combined intervention may alter patients’ catastrophic interpretations of pain through cognitive restructuring. When integrated with exercise-based behavioral interventions, these changes can be reinforced through experiential learning, thereby contributing to reductions in catastrophizing.42 Regarding the fear of movement, the observed improvements may be attributed to the reduction of avoidance beliefs via CBT, coupled with the progressive restoration of physical activity engagement facilitated by exercise.49 Furthermore, improvements in pain self-efficacy suggest that the combined intervention may enhance patients’ confidence in pain management and promote engagement in more proactive coping strategies.
The combined intervention also demonstrated improvements in mental health and quality of life. However, the sustainability of these effects appeared limited. Previous studies suggest that cognitive behavioral therapy combined with exercise can alleviate symptoms of anxiety and depression in patients with chronic pain. The effects of combined interventions on anxiety and depression may not be entirely direct, but rather mediated through indirect pathways, such as pain relief, functional improvement, or modifications in maladaptive cognitions.50–52 Evidence suggests that elevated anxiety and depression in chronic pain populations are significantly associated with frequent pain exacerbations, greater functional limitations, and poorer quality of life.53,54 Moreover, catastrophizing, as a key cognitive factor, is closely correlated not only with pain intensity and disability but also with emotional distress and quality of life impairment.55,56 Follow-up analyses revealed limited maintenance of benefits for mental health and quality of life. This may be attributed to the inherent cyclical variability of these outcomes. Additionally, as a highly multidimensional outcome including pain experience, physical function, psychological status, and social participation, quality of life is susceptible to influence from various external factors.57 Overall, while CBT combined with exercise confers positive post-treatment effects for mental health and quality of life, its long-term stability warrants further investigation in future high-quality studies.
Given the substantial heterogeneity observed in the pooled outcomes for pain intensity, functional disability, and catastrophizing, subgroup analyses were conducted to investigate potential sources of variation. Generally, intervention effects on pain and disability appeared sensitive to intervention composition. Subgroup analyses revealed that multimodal exercise interventions were associated with numerically larger pooled effect sizes compared with single-mode exercise interventions, although no statistically significant subgroup differences were observed. For pain intensity, group-based interventions demonstrated more favorable effects than individual-based interventions (Group-based: SMD = −0.63 vs Individual-based: SMD = −0.08; P = 0.01), whereas this pattern was not observed for functional disability. These findings suggest that group-based formats may enhance patient engagement and treatment adherence through peer support and social reinforcement, thereby contributing to more favorable outcomes.13,58 Furthermore, multimodal exercise interventions demonstrated consistent improvement trends across multiple subgroups, aligning with previous findings and implying potential advantages of incorporating diverse exercise modalities.59 For catastrophizing, a cognitive processing pattern influenced by both cognitive factors and behavioral engagement, changes may be particularly sensitive to differences in intervention format and composition.60 In this context, group-based interventions and combined interventions incorporating comprehensive exercise modalities tended to yield greater reductions in catastrophizing. No significant subgroup differences were observed between standard CBT and CBT-informed interventions, nor between interventions delivered by psychologists and those delivered by non-psychologists, suggesting that with appropriate training, non-psychologists may be able to effectively implement pain-related cognitive behavioral strategies, potentially improving the accessibility and cost-effectiveness of combined interventions.61,62 Concurrently, CBT-informed approaches incorporating partial cognitive-behavioral elements may yield comparable efficacy to full CBT within combined interventions.63 In this study, ACT was included within a broader CBT framework because it shares common cognitive-behavioral foundations with traditional CBT.64 However, the inclusion of ACT-based or CBT-informed approaches within this broader framework may be one factor contributing to the heterogeneity observed in the pooled results. It is noteworthy that this study did not observe significant improvements in physical performance outcomes (measured by TUG and 6MWT) among patients with chronic pain. This finding is not entirely consistent with previous studies reporting improvements in objective physical performance following CBT-based physical therapy in postoperative chronic pain populations or self-management programs incorporating cognitive-behavioral strategies.42,65 However, these studies primarily targeted specific populations or utilized intervention models with a specific goal of enhancing physical fitness, involving exercise intensities, training durations, and experimental designs that differ from the combined interventions included here. Regarding the lack of significant improvements in physical performance identified in this study, we postulate that the primary objective of the combined intervention was to mitigate pain intensity, reduce functional disability, and decrease pain-related avoidance, rather than to directly enhance physiological conditioning. In addition, only two studies investigating objective physical capacity were included in this analysis. The limited sample size, coupled with relatively conservative exercise intensities and methodological heterogeneity, may have compromised the statistical power to detect true intervention effects. Future research should optimize exercise prescription parameters, specifically intensity and volume, and refine assessment protocols to more accurately elucidate the effects of combined interventions on objective physical capacity in chronic pain populations.
Sensitivity analyses showed that the direction and magnitude of the pooled effects for most outcomes remained stable after sequential exclusion of individual studies, particularly for the primary outcomes of pain intensity and functional disability, supporting the robustness of the main results. In contrast, pain self-efficacy and physical health-related quality of life (PCS) were more sensitive to the influence of individual studies. This sensitivity may be attributable to the limited number of available studies and methodological heterogeneity; therefore, these results should be interpreted with caution. For outcomes with a sufficient number of included studies, Egger’s test did not provide evidence of statistically significant publication bias. Taken together, the results of the sensitivity analyses and publication bias assessments support the overall reliability of the primary findings of this study.
In addition, in this study, more than half of the included studies were judged as having some concerns or high risk of bias, suggesting that the pooled estimates may have been influenced to some extent by methodological limitations. Nevertheless, the GRADE assessment showed that the certainty of evidence for the main post-intervention outcomes ranged from moderate to high, which supports a reasonable level of reliability in the primary findings. Overall, the current evidence generally supports the benefits of CBT combined with exercise. Further high-quality studies are still needed to strengthen the certainty of evidence.
Limitations
Several limitations of this study should be acknowledged. First, although the overall effects of CBT combined with exercise were systematically evaluated, the included studies varied in intervention composition and in the implementation of cognitive behavioral components. In particular, some studies employed CBT-informed interventions without fully reporting their core elements, which limited more detailed analyses of specific intervention components and their contributions to treatment effects. Second, the included studies covered a range of chronic pain conditions, and such clinical heterogeneity may have influenced the pooled estimates. In addition, pain-specific subgroup analyses were not feasible because of the limited number of studies within each condition. Finally, the limited number of studies included for certain outcomes may have compromised the statistical power and robustness of the pooled results.
Conclusion
This systematic review and meta-analysis demonstrates that CBT combined with exercise provides benefits for adults with chronic pain. The combined intervention produced small-to-moderate improvements in pain intensity and functional disability, with effects maintained at short- and mid-term follow-up. Improvements were also observed in cognitive-behavioral outcomes, mental health, and quality of life, but their long-term maintenance was limited. No significant improvements were observed in physical performance. Overall, CBT combined with exercise is a feasible multidisciplinary approach for chronic pain management. Future studies should standardize CBT and exercise protocols and include more diverse populations to better evaluate long-term efficacy.
Data Sharing Statement
The data used and/or analyzed during the current study are available from the corresponding author, He Zhang, upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Research Project of Hunan Provincial Sports Bureau, China (Grant No. 2024KT0168 and 2025KT0214).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Treede RD, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain for the International Classification of Diseases (ICD-11). Pain. 2019;160(1):19–23. doi:10.1097/j.pain.0000000000001384
2. Aaron RV, Ravyts SG, Carnahan ND, et al. Prevalence of depression and anxiety among adults with chronic pain: a systematic review and meta-analysis. JAMA Network Open. 2025;8(3):e250268. doi:10.1001/jamanetworkopen.2025.0268
3. Freynhagen R, Fullen BM, Reneman MF, Treede RD. Functioning in chronic pain: a call for a global definition. Pain. 2024;165(10):2235–2239. doi:10.1097/j.pain.0000000000003307
4. Dueñas M, Ojeda B, Salazar A, Mico JA, Failde I. A review of chronic pain impact on patients, their social environment and the health care system. J Pain Res. 2016;9:457–467. doi:10.2147/JPR.S105892
5. Zhu M, Zhang J, Liang D, et al. Global and regional trends and projections of chronic pain from 1990 to 2035: analyses based on global burden of diseases study 2019. Br J Pain. 2025;19(2):125–137. doi:10.1177/20494637241310697
6. Lucas JW, Sohi I. Chronic pain and high-impact chronic pain in US Adults, 2023. NCHS Data Brief. 2024;(518):CS355235. doi:10.15620/cdc/169630
7. Nicholas MK. The biopsychosocial model of pain 40 years on: time for a reappraisal? Pain. 2022;163(Suppl 1):S3–S14. doi:10.1097/j.pain.0000000000002654
8. Kapos FP, Craig KD, Anderson SR, et al. Social determinants and consequences of pain: toward multilevel, intersectional, and life course perspectives. J Pain. 2024;25(10):104608. doi:10.1016/j.jpain.2024.104608
9. Huttunen MH, Paananen M, Miettunen J, Kalso E, Marttinen MK. Multidisciplinary management of persistent pain in primary care-A systematic review. Eur J Pain. 2024;28(6):886–900. doi:10.1002/ejp.2240
10. Geneen LJ, Moore RA, Clarke C, Martin D, Colvin LA, Smith BH. Physical activity and exercise for chronic pain in adults: an overview of cochrane reviews. Cochrane Database Syst Rev. 2017;4(4):CD011279. doi:10.1002/14651858.CD011279.pub3
11. Silva HJ, Miranda JP, Silva WT, et al. Group-based exercise reduces pain and disability and improves other outcomes in older people with chronic non-specific low back pain: the ESCAPE randomised trial. J Physiother. 2025;71(2):108–116. doi:10.1016/j.jphys.2025.03.003
12. Yihunie M, Abich Y, Demissie SF, Kassa T, Ranganathan P, Janakiraman B. Fear-avoidance beliefs for physical activity among chronic low back pain: a multicenter cross-sectional study. J Pain Res. 2023;16:233–243. doi:10.2147/JPR.S388002
13. Gilanyi YL, Shah B, Cashin AG, et al. Barriers and enablers to exercise adherence in people with nonspecific chronic low back pain: a systematic review of qualitative evidence. Pain. 2024;165(10):2200–2214. doi:10.1097/j.pain.0000000000003234
14. Williams ACC, Fisher E, Hearn L, Eccleston C. Psychological therapies for the management of chronic pain (excluding headache) in adults. Cochrane Database Syst Rev. 2020;8(8):CD007407. doi:10.1002/14651858.CD007407.pub4
15. Sturgeon JA. Psychological therapies for the management of chronic pain. Psychol Res Behav Manag. 2014;7:115–124. doi:10.2147/PRBM.S44762
16. Yang J, Lo WLA, Zheng F, Cheng X, Yu Q, Wang C. Evaluation of cognitive behavioral therapy on improving pain, fear avoidance, and self-efficacy in patients with chronic low back pain: a systematic review and meta-analysis. Pain Res Manag. 2022;2022:4276175. doi:10.1155/2022/4276175
17. Elbers S, Wittink H, Konings S, et al. Longitudinal outcome evaluations of interdisciplinary multimodal pain treatment programmes for patients with chronic primary musculoskeletal pain: a systematic review and meta-analysis. Eur J Pain. 2022;26(2):310–335. doi:10.1002/ejp.1875
18. Lambeek LC, van Mechelen W, Knol DL, Loisel P, Anema JR. Randomised controlled trial of integrated care to reduce disability from chronic low back pain in working and private life. BMJ. 2010;340:c1035. doi:10.1136/bmj.c1035
19. Thompson DP, Oldham JA, Woby SR. Does adding cognitive-behavioural physiotherapy to exercise improve outcome in patients with chronic neck pain? A randomised controlled trial. Physiotherapy. 2016;102(2):170–177. doi:10.1016/j.physio.2015.04.008
20. Cheng JOS, Cheng ST. Effectiveness of physical and cognitive-behavioural intervention programmes for chronic musculoskeletal pain in adults: a systematic review and meta-analysis of randomised controlled trials. PLoS One. 2019;14(10):e0223367. doi:10.1371/journal.pone.0223367
21. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
22. Bramer WM, Rethlefsen ML, Kleijnen J, Franco OH. Optimal database combinations for literature searches in systematic reviews: a prospective exploratory study. Syst Rev. 2017;6(1):245. doi:10.1186/s13643-017-0644-y
23. Beehler GP, Murphy JL, King PR, Dollar KM. Brief Cognitive Behavioral Therapy for Chronic Pain: Therapist Manual. Version 2.0. Washington, DC: US Department of Veterans Affairs; 2021.
24. Rosser BA, Fisher E, Janjua S, Eccleston C, Keogh E, Duggan G. Psychological therapies delivered remotely for the management of chronic pain (excluding headache) in adults. Cochrane Database Syst Rev. 2023;8(8):CD013863. doi:10.1002/14651858.CD013863.pub2
25. Higgins JP, Eldridge S, Li T, et al. Chapter 23: including variants on randomized trials. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, editors. Cochrane Handbook for Systematic Reviews of Interventions. Version 6.5. London: Cochrane; 2024.
26. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. doi:10.1136/bmj.l4898
27. Aliyu FY, Wasiu AA, Bello B. Effects of a combined lumbar stabilization exercise and cognitive behavioral therapy on selected variables of individuals with non-specific low back pain: a randomized clinical trial. Fisioterapia. 2018;40(5):257–264. doi:10.1016/j.ft.2018.07.002
28. Andersen TE, Ravn SL, Armfield N, Maujean A, Requena SS, Sterling M. Trauma-focused cognitive behavioural therapy and exercise for chronic whiplash with comorbid posttraumatic stress disorder: a randomised controlled trial. Pain. 2021;162(4):1221–1232. doi:10.1097/j.pain.0000000000002117
29. Casey MB, Smart KM, Segurado R, et al. Exercise combined with Acceptance and Commitment Therapy compared with a standalone supervised exercise programme for adults with chronic pain: a randomised controlled trial. Pain. 2022;163(6):1158–1171. doi:10.1097/j.pain.0000000000002487
30. Cheng ST, Chen PP, Chow YF, et al. An exercise cum cognitive-behavioral intervention for older adults with chronic pain: a cluster-randomized controlled trial. J Consult Clin Psychol. 2022;90(3):221–233. doi:10.1037/ccp0000698
31. Hirase T, Kataoka H, Nakano J, Inokuchi S, Sakamoto J, Okita M. Effects of a psychosocial intervention programme combined with exercise in community-dwelling older adults with chronic pain: a randomized controlled trial. Eur J Pain. 2018;22(3):592–600. doi:10.1002/ejp.1149
32. Hrkać A, Bilić D, Černy-Obrdalj E, Baketarić I, Puljak L. Comparison of supervised exercise therapy with or without biopsychosocial approach for chronic nonspecific low back pain: a randomized controlled trial. BMC Musculoskelet Disord. 2022;23(1):966. doi:10.1186/s12891-022-05908-3
33. Kang DH, Park JH, Yoon C, et al. Multidisciplinary digital therapeutics for chronic low back pain versus in-person therapeutic exercise with education: a randomized controlled pilot study. J Clin Med. 2024;13(23):7377. doi:10.3390/jcm13237377
34. Lera S, Gelman SM, López MJ, et al. Multidisciplinary treatment of fibromyalgia: does cognitive behavior therapy increase the response to treatment? J Psychosom Res. 2009;67(5):433–441. doi:10.1016/j.jpsychores.2009.01.012
35. Liu JQJ, Mak YW, Tang ALY, et al. Effects of acceptance and commitment therapy plus exercise for older adults with chronic low back pain: a preliminary cluster randomized controlled trial with qualitative interviews. J Pain. 2025;30:105350. doi:10.1016/j.jpain.2025.105350
36. McBeth J, Prescott G, Scotland G, et al. Cognitive behavior therapy, exercise, or both for treating chronic widespread pain. Arch Intern Med. 2012;172(1):48–57. doi:10.1001/archinternmed.2011.555
37. Monticone M, Baiardi P, Vanti C, et al. Chronic neck pain and treatment of cognitive and behavioural factors: results of a randomised controlled clinical trial. Eur Spine J. 2012;21(8):1558–1566. doi:10.1007/s00586-012-2287-y
38. Monticone M, Ambrosini E, Rocca B, Magni S, Brivio F, Ferrante S. A multidisciplinary rehabilitation programme improves disability, kinesiophobia and walking ability in subjects with chronic low back pain: results of a randomised controlled pilot study. Eur Spine J. 2014;23(10):2105–2113. doi:10.1007/s00586-014-3478-5
39. van Koulil S, van Lankveld W, Kraaimaat FW, et al. Tailored cognitive-behavioral therapy and exercise training for high-risk patients with fibromyalgia. Arthritis Care Res. 2010;62(10):1377–1385. doi:10.1002/acr.20268
40. Zale EL, Lange KL, Fields SA, Ditre JW. The relation between pain-related fear and disability: a meta-analysis. J Pain. 2013;14(10):1019–1030. doi:10.1016/j.jpain.2013.05.005
41. Martinez-Calderon J, Jensen MP, Morales-Asencio JM, Luque-Suarez A. Pain catastrophizing and function in individuals with chronic musculoskeletal pain: a systematic review and meta-analysis. Clin J Pain. 2019;35(3):279–293. doi:10.1097/AJP.0000000000000676
42. Archer KR, Devin CJ, Vanston SW, et al. Cognitive-behavioral-based physical therapy for patients with chronic pain undergoing lumbar spine surgery: a randomized controlled trial. J Pain. 2016;17(1):76–89. doi:10.1016/j.jpain.2015.09.013
43. Driscoll MA, Edwards RR, Becker WC, Kaptchuk TJ, Kerns RD. Psychological interventions for the treatment of chronic pain in adults. Psychol Sci Public Interest. 2021;22(2):52–95. doi:10.1177/15291006211008157
44. Bao S, Qiao M, Lu Y, Jiang Y. Neuroimaging mechanism of cognitive behavioral therapy in pain management. Pain Res Manag. 2022;2022:6266619. doi:10.1155/2022/6266619
45. Almeida de Oliveira L, Gross AR, Carlesso L, et al. Graded activity for chronic low back pain. Cochrane Database Syst Rev. 2025;2(2):CD015507. doi:10.1002/14651858.CD015507
46. Petrini L, Arendt-Nielsen L. Understanding pain catastrophizing: putting pieces together. Front Psychol. 2020;11:603420. doi:10.3389/fpsyg.2020.603420
47. Simic K, Savic B, Knezevic NN. Pain catastrophizing: how far have we come. Neurol Int. 2024;16(3):483–501. doi:10.3390/neurolint16030036
48. Rogers AH, Farris SG. A meta-analysis of the associations of elements of the fear-avoidance model of chronic pain with negative affect, depression, anxiety, pain-related disability and pain intensity. Eur J Pain. 2022;26(8):1611–1635. doi:10.1002/ejp.1994
49. Caneiro JP, Bunzli S, O’Sullivan P. Beliefs about the body and pain: the critical role in musculoskeletal pain management. Braz J Phys Ther. 2021;25(1):17–29. doi:10.1016/j.bjpt.2020.06.003
50. Lutsch AG, Baumeister H, Paganini S, Sander LB, Terhorst Y, Domhardt M. Mechanisms of change in digital cognitive behavioral therapy for depression in patients with chronic back pain: a mediation analysis of a multicenter randomized clinical trial. Behav Res Ther. 2023;168:104369. doi:10.1016/j.brat.2023.104369
51. Craner JR, Schumann ME, Barr A, et al. Mediators of change in depressed mood following pain rehabilitation among participants with mild, moderate, or severe depressive symptoms. J Affect Disord. 2022;307:286–293. doi:10.1016/j.jad.2022.03.060
52. Bisby MA, Chandra SS, Dudeney J, Scott AJ, Titov N, Dear BF. Can internet-delivered pain management programs reduce psychological distress in chronic pain? exploring relationships between anxiety and depression, pain intensity, and disability. Pain Med. 2023;24(5):538–546. doi:10.1093/pm/pnac158
53. Sanabria-Mazo JP, Colomer-Carbonell A, Fernández-Vázquez Ó, et al. A systematic review of cognitive behavioral therapy-based interventions for comorbid chronic pain and clinically relevant psychological distress. Front Psychol. 2023;14:1200685. doi:10.3389/fpsyg.2023.1200685
54. De La Rosa JS, Brady BR, Ibrahim MM, et al. Co-occurrence of chronic pain and anxiety/depression symptoms in US adults: prevalence, functional impacts, and opportunities. Pain. 2024;165(3):666–673. doi:10.1097/j.pain.0000000000003056
55. Shimada S, Doorenbos AZ, Goldstein E, Wi D. A systematic review of pain catastrophizing and chronic musculoskeletal pain. Pain Manag Nurs. 2025;27:e72–e84. doi:10.1016/j.pmn.2025.07.014
56. Dimitrijević I, Hnatešen D, Radoš I, Budrovac D, Raguž M. Relationship between psychological factors and health-related quality of life in patients with chronic low back pain. Healthcare. 2024;12(24):2531. doi:10.3390/healthcare12242531
57. Andersen JR, Breivik K, Engelund IE, et al. Correlated physical and mental health composite scores for the RAND-36 and RAND-12 health surveys: can we keep them simple? Health Qual Life Outcomes. 2022;20(1):89. doi:10.1186/s12955-022-01992-0
58. Roberts KE, Ho E, Gassen-Fritsch C, Halliday M, Mattinty MM, Ferreira P. Perceived social support impacts on exercise adherence in patients with chronic low back pain. J Back Musculoskelet Rehabil. 2024;37(6):1467–1477. doi:10.3233/BMR-230239
59. Fernández-Rodríguez R, Álvarez-Bueno C, Cavero-Redondo I, et al. Best exercise options for reducing pain and disability in adults with chronic low back pain: pilates, strength, core-based, and mind-body. A network meta-analysis. J Orthop Sports Phys Ther. 2022;52(8):505–521. doi:10.2519/jospt.2022.10671
60. Meints SM, Edwards RR. Evaluating psychosocial contributions to chronic pain outcomes. Prog Neuropsychopharmacol Biol Psychiatry. 2018;87(Pt B):168–182. doi:10.1016/j.pnpbp.2018.01.017
61. Bennell KL, Ahamed Y, Jull G, et al. Physical therapist-delivered pain coping skills training and exercise for knee osteoarthritis: randomized controlled trial. Arthritis Care Res. 2016;68(5):590–602. doi:10.1002/acr.22744
62. Rutledge T, Atkinson JH, Holloway R, et al. Randomized controlled trial of nurse-delivered cognitive-behavioral therapy versus supportive psychotherapy telehealth interventions for chronic back pain. J Pain. 2018;19(9):1033–1039. doi:10.1016/j.jpain.2018.03.017
63. O’Keeffe M, Purtill H, Kennedy N, et al. Comparative effectiveness of conservative interventions for nonspecific chronic spinal pain: physical, behavioral/psychologically informed, or combined? a systematic review and meta-analysis. J Pain. 2016;17(7):755–774. doi:10.1016/j.jpain.2016.01.473
64. Feliu-Soler A, Montesinos F, Gutiérrez-Martínez O, Scott W, McCracken LM, Luciano JV. Current status of acceptance and commitment therapy for chronic pain: a narrative review. J Pain Res. 2018;11:2145–2159. doi:10.2147/JPR.S144631
65. Turner BJ, Liang Y, Simmonds MJ, Rodriguez N, Bobadilla R, Yin Z. Randomized trial of chronic pain self-management program in the community or clinic for low-income primary care patients. J Gen Intern Med. 2018;33(5):668–677. doi:10.1007/s11606-017-4244-2
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Efficacy and Safety of Acupuncture for Tinnitus-Associated Insomnia: A Protocol for a Systematic Review and Meta-Analysis
Fan L, Gao Y, Zhou J, Hu H, Gao H
Journal of Pain Research 2022, 15:2957-2965
Published Date: 21 September 2022
A Systematic Review and Meta-Analysis Protocol on How Best to Use Non-Pharmacologic Therapies to Manage Chronic Low Back Pain and Associated Depression
Guo Y, Ma Q, Zhou X, Yang J, He K, Shen L, Zhao C, Chen Z, Tan CIC, Chen J
Journal of Pain Research 2022, 15:3509-3521
Published Date: 4 November 2022
Tezepelumab for Patients with Severe Uncontrolled Asthma: A Systematic Review and Meta-Analysis
Zoumot Z, Al Busaidi N, Tashkandi W, Aljohaney AA, Isse S, Vidyasagar K, Ukwaja KN
Journal of Asthma and Allergy 2022, 15:1665-1679
Published Date: 18 November 2022
Effect of Exercise Interventions on Health-Related Quality of Life in Patients with Fibromyalgia Syndrome: A Systematic Review and Network Meta-Analysis
Zhang KD, Wang LY, Zhang ZH, Zhang DX, Lin XW, Meng T, Qi F
Journal of Pain Research 2022, 15:3639-3656
Published Date: 22 November 2022
The Effectiveness of Cognitive Behavioral Therapy-Based Intervention on Improving Sleep-Related Outcomes for People with Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Wang H, Li R, Ge L, Xu F, Wiley JA, Tang S, Sun M
Psychology Research and Behavior Management 2024, 17:957-972
Published Date: 9 March 2024