Back to Journals » Journal of Pain Research » Volume 19
Efficacy and Safety of Peripheral Nerve Blocks After Arthroscopic Shoulder Surgery: A Systematic Review and Network Meta-Analysis
Authors Gao Y, Huang J, Liu Z, Hu Z, Yan W, Ren D
Received 16 December 2025
Accepted for publication 14 April 2026
Published 21 April 2026 Volume 2026:19 589046
DOI https://doi.org/10.2147/JPR.S589046
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jinlei Li
Yanjun Gao, Jinwen Huang, Zhilong Liu, Zhongyuan Hu, Wenjun Yan, Dongqing Ren
Department of Anesthesiology, Gansu Provincial Hospital, Lanzhou, Gansu, 730000, People’s Republic of China
Correspondence: Dongqing Ren, Email [email protected]
Background: Nerve blocks are commonly used for analgesia following shoulder arthroscopy, but the optimal technique remains uncertain. This network meta-analysis (NMA) evaluates the effect of peripheral nerve blocks in adults undergoing shoulder arthroscopy.
Methods: We searched databases including PubMed, Embase, Web of Science, and the Cochrane Library from their inception to July 2025. Randomized controlled trials (RCTs) to evaluate the effect of peripheral nerve blocks after arthroscopic shoulder surgery were included. The primary outcome was the pain scores at 6 hours postoperatively.
Results: We included 25 RCTs involving 2039 patients and assessed ten techniques. The Visual Analog Scale (VAS) scores at 6 hours were lower with suprascapular and axillary nerve blocks (SANB), followed by coracoid approach brachial plexus (CPB) + suprascapular nerve block (SSB) and supraclavicular brachial plexus block (SCPB). The VAS scores at 12 hours were lower with erector spinae plane block (ESPB), followed by SANB and infraclavicular-suprascapular blocks (ICSB). The VAS scores at 24 hours were lower with SANB, followed by upper trunk block (UTB) and CPB + SSB. The morphine consumption within 24 hours was significantly reduced by UTB, followed by SSB and SCPB. For hemidiaphragmatic paralysis (HDP), ICSB had the lowest incidence (0%), followed by CPB+SSB (21.7%) and SCPB (29.5%). For hoarseness, ICSB and SSB had the lowest incidence (0%), followed by UTB (4.8%). For Horner’s syndrome, ICSB and SSB had the lowest incidence (0%), followed by UTB (5.7%). For motor block, SSB had the lowest incidence (1.2%). For postoperative nausea and vomiting (PONV), ESPB had the lowest incidence (9.4%), followed by SSB (15.4%) and SANB (14.3%).
Limitation: The included studies have differences in local anesthetic agents and postoperative analgesic regimen, which may affect the generalizability of the findings. Our NMA did not include continuous nerve block which have also been shown to provide significant analgesic benefits. There was a lack of data on long-term analgesia and functional outcomes.
Conclusion: The SANB was more likely to improve pain scores within 24 hours and reduce the incidence of PONV, HDP, hoarseness, and Horner’s syndrome. The SSB was proven to have the weakest analgesic effect.
Keywords: arthroscopic, shoulder, analgesia, nerve block, systematic review, network meta-analysis
Introduction
Shoulder pathologies are increasingly prevalent, particularly among the aging population and active individuals, with the incidence of rotator cuff tears, impingement syndrome, and shoulder instability rising steadily.1 These conditions often impair shoulder function and significantly affect quality of life.1 Arthroscopic shoulder surgery has become the mainstay treatment due to its minimally invasive approach, offering effective management of various shoulder disorders.2 However, postoperative pain remains a common and challenging issue, originating primarily from extensive soft tissue manipulation, joint capsule stretching, and nerve irritation during arthroscopy.3 This pain not only hampers early mobilization but also predisposes patients to adverse outcomes such as increased risk of thromboembolic events, prolonged hospitalization, elevated healthcare costs, disrupted sleep, and delayed rehabilitation.3 Consequently, effective perioperative pain management is essential, as it can reduce medical expenses, promote early functional recovery, prevent complications, and facilitate a smoother transition to daily activities.4
Currently, the primary strategies for managing postoperative shoulder pain include systemic intravenous analgesia and regional analgesic techniques. Opioid-based intravenous analgesia continues to be widely employed due to its potent analgesic properties; however, its associated adverse effects—such as respiratory depression, nausea, constipation, sedation, and the risk of dependence—pose significant barriers to rapid recovery.5 Consequently, the Anesthesiologists’ Association advocates for the implementation of multimodal analgesia protocols to address these challenges, with regional nerve blockade techniques serving as the fundamental component of this comprehensive approach.6,7 The interscalene brachial plexus block (ISPB) is often regarded as the gold standard owing to its high analgesic efficacy.8 However, concerns regarding its associated adverse effects—such as hemidiaphragmatic paralysis (HDP),9 Horner’s syndrome,10 and nerve injury11—have prompted interest in alternative techniques such as suprascapular nerve block (SSB),12 axillary nerve block (ANB),13 and others. Among these, SSB and ANB might represent the optimal choice for patients with severe respiratory compromise, given their complete avoidance of HDP. Nevertheless, whether they can serve as effective substitutes for ISPB remains to be conclusively demonstrated, with further high-quality evidence needed to establish their efficacy and safety.
Unlike traditional pairwise meta-analysis, which is confined to direct comparisons between two interventions, network meta-analysis (NMA) enables the simultaneous comparison of multiple interventions by combining direct and indirect evidence within a coherent analytical framework. This approach not only preserves within-trial randomization but also allows for the ranking of interventions based on their efficacy or safety, thereby providing a more comprehensive evidence base for clinical decision-making. The NMA aims to synthesize current evidence from randomized controlled trials (RCTs) to compare the postoperative analgesic efficacy and complication rates associated with various nerve blocks in arthroscopic shoulder procedures. Through this analysis, we seek to identify the most effective and safest nerve block strategies, thereby informing clinical decision-making and improving postoperative outcomes for patients undergoing shoulder arthroscopy.
Methods
The NMA followed the PRISMA guidelines for Network Meta-Analyses.14 The protocol was preregistered and published in the International Prospective Register of Systematic Reviews (CRD420251074318). The NMA began in July 2025.
Eligibility Criteria
The inclusion criteria based on PICOS principles: adult patients undergoing arthroscopic shoulder surgery (P); peripheral nerve blocks included single-injection erector spinae plane block (ESPB), costoclavicular block (CCB), upper trunk block (UTB), coracoid approach brachial plexus (CPB), supraclavicular brachial plexus block (SCPB), intermediate cervical plexus block (ICPB), infraclavicular-suprascapular blocks (ICSB), SANB, ISPB, SSB, and others (I); one of the peripheral nerve blocks, placebo or no block (C); postoperative resting pain scores, morphine consumption within 24 h, HDP, hoarseness, Horner’s syndrome, motor block, postoperative nausea and vomiting (PONV) (O); randomized controlled trials (RCTs) (S).
The exclusion criteria included: (1) the study presented data that was unsuitable for statistical analysis; (2) unpublished studies and crossover randomized trials; (3) studies with duplicate data were identified, and those with incomplete data were excluded.
Study Selection
Databases including PubMed, Embase, Web of Science, and the Cochrane Library were searched from their inception to July 2025, focusing on studies published in English. The search strategy involved combining keywords and MeSH terms such as “arthroscopic”, “arthroscopy”, “shoulder”, “block”, “analgesia”, and “pain” using Boolean operators (AND, OR) to link the terms.
Data Extraction
Two separate reviewers initially evaluated the titles and abstracts of the selected articles. The full texts were then reviewed for inclusion criteria, with any disagreements resolved through discussion with a third reviewer. For data extraction, two independent reviewers collected information from the eligible studies, and a third reviewer verified the accuracy of the extracted data. The data collected included study details, interventions implemented, and outcome measures, all using a predefined standardized form.
Quality Assessment
The quality of the included studies was appraised with the Cochrane Collaboration Risk of Bias Tool, examining various domains such as selection bias, performance bias, detection bias, attrition bias, reporting bias, and other potential sources of bias.15 The overall certainty of evidence for each outcome was then graded using the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) system.16
Statistical Analysis
We employed the statistical framework established in our prior work.17 The NMA was performed using STATA 15.1 software, applying a frequentist framework with random effects to account for variability across studies. Risk of bias was evaluated using the Confidence in Network Meta-Analysis (CINeMA) 2.0.0 tool.18 For all relevant comparisons, we calculated relative risks (RR) and mean differences (MD) with 95% confidence intervals (CIs). Pain scores were standardized to a 0–10 visual analogue scale (VAS), and postoperative opioid consumption was converted to intravenous morphine equivalent doses.19 Data reported as medians and interquartile ranges were transformed into means and standard deviations using the validated Luo’s and Wan’s formulas.20,21 Network maps provided visual summaries of the relationships between interventions, while forest plots illustrated study outcomes and global heterogeneity. Netleague tables summarized the relative effectiveness of each intervention. Surface Under the Cumulative Ranking Curve (SUCRA) was used to estimate their ranking probabilities, where a lower value indicated better clinical outcome. Publication bias was examined with funnel plot, and local inconsistency within the network was assessed through the node-splitting method. In cases of heterogeneity, sensitivity and subgroup analyses were conducted to explore potential sources. A p-value of less than 0.05 was considered statistically significant in all analyses.
Results
Study Selection and Characteristics
This NMA included 25 RCTs involving a total of 2,039 patients and covering ten types of nerve blocks.22–46 The study selection process was illustrated in Figure 1. Table 1 summarized the characteristics of all included studies. The primary outcome was reported in 11 RCTs. Among the interventions, ISPB was the most frequently used, followed by SSB and SCPB.
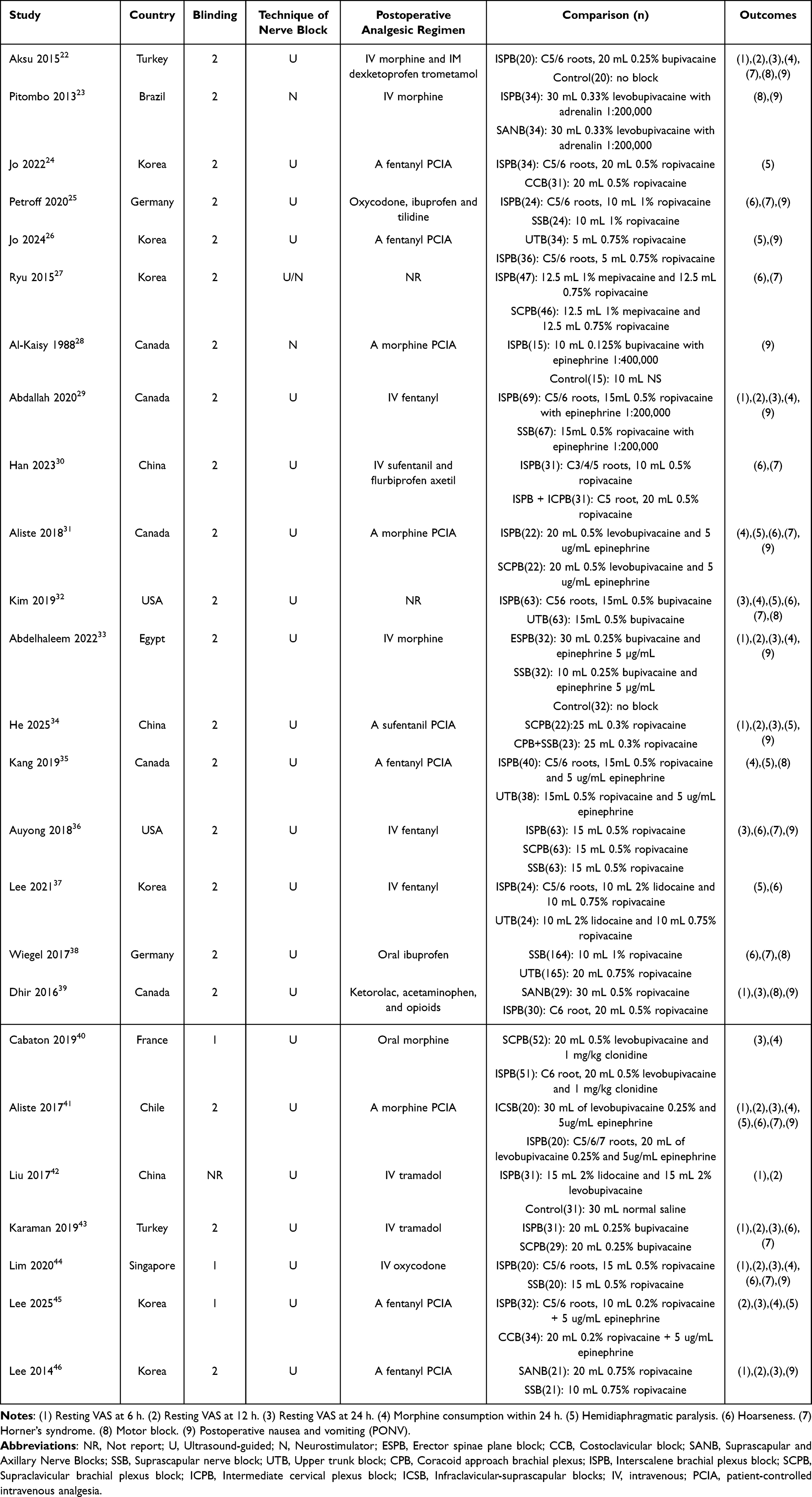 |
Table 1 Study Characteristics of Included Studies |
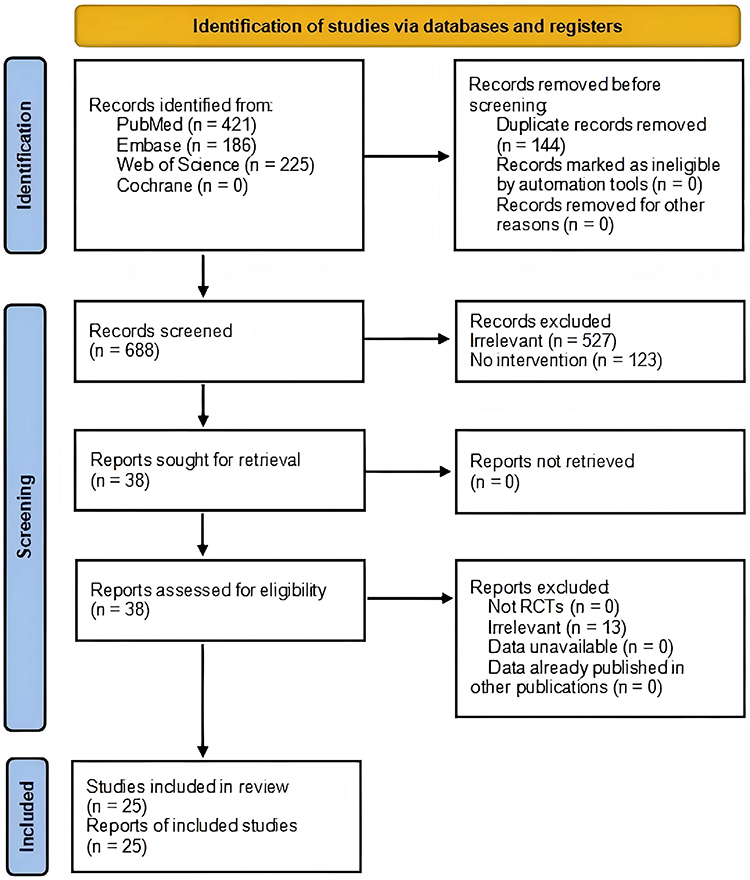 |
Figure 1 PRISMA flow diagram of study selection. |
Resting VAS at 6 h
The analysis included 10 studies with a total of 1,240 patients. Figure 2 illustrated the interventions assessed and their interrelationships. Figure 3 indicated that there was no significant global heterogeneity. Figure 4 showed that there was no evident publication bias. Figure 5 presented the risk of bias assessment. Table 2 highlighted a high risk of inconsistency between ISPB vs. SANB and SANB vs. SSB. Table 3 compared the relative effectiveness of seven different interventions. Figure 6 revealed that SANB had the lowest SUCRA value at 13.6, followed by CPB+SSB (26.4), SCPB (27.8), ICSB (48.7), SSB (56.4), ISPB (61.6), and ESPB (66.2), reflecting their respective rankings.
 |
Table 2 Exploration of Inconsistency |
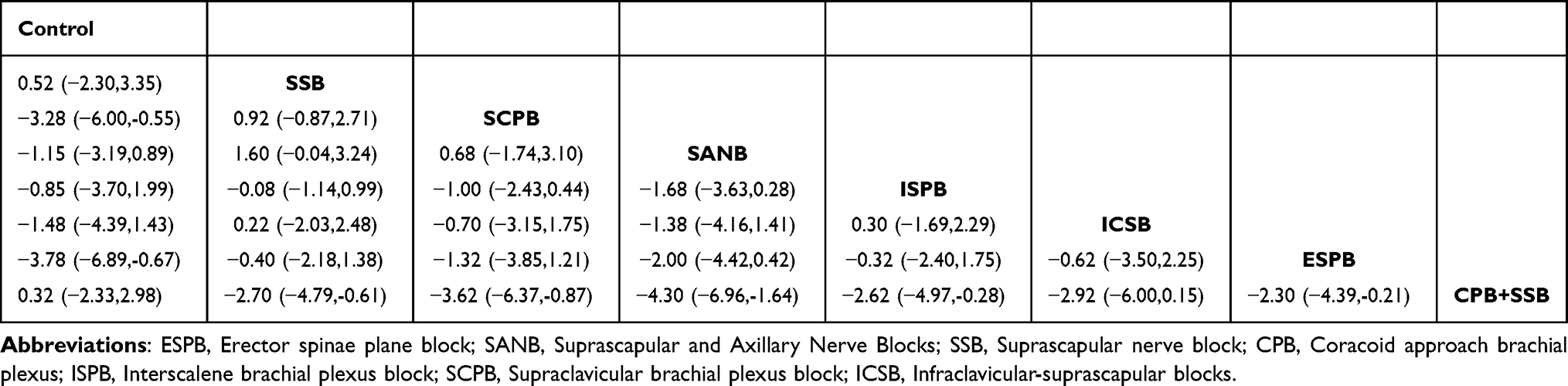 |
Table 3 Netleague Tables of Mixed Estimates |
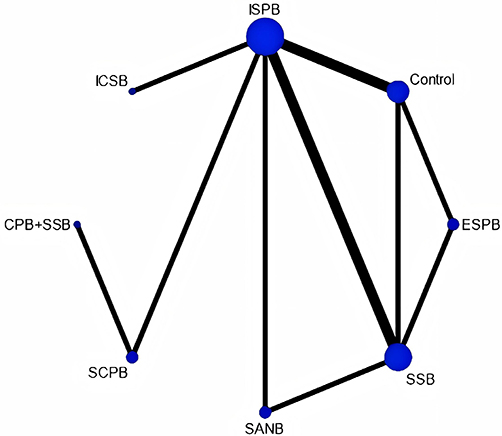 |
Figure 2 Network map of resting VAS at 6 h. ESPB, Erector spinae plane block. SANB, Suprascapular and Axillary Nerve Blocks. SSB, Suprascapular nerve block. CPB, Coracoid approach brachial plexus. ISPB, Interscalene brachial plexus block. SCPB, Supraclavicular brachial plexus block. ICSB, Infraclavicular-suprascapular blocks. |
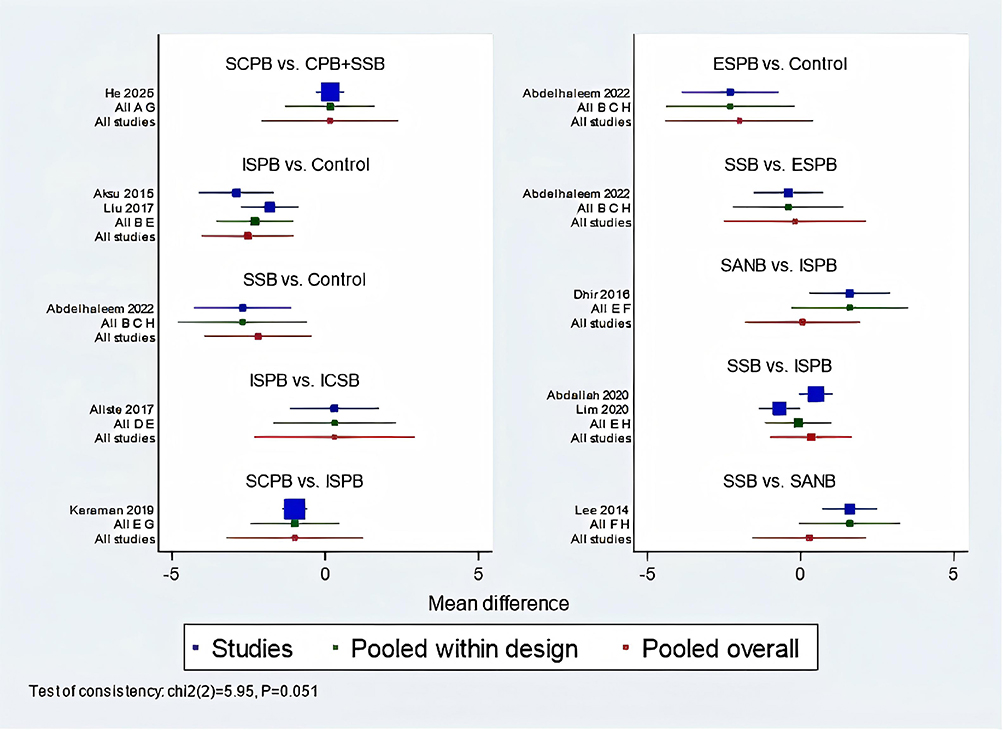 |
Figure 3 Network forest plot of resting VAS at 6 h. |
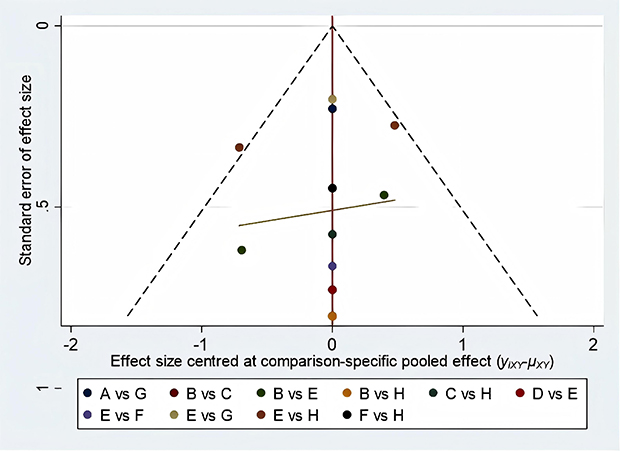 |
Figure 4 Funnel plot of resting VAS at 6 h. |
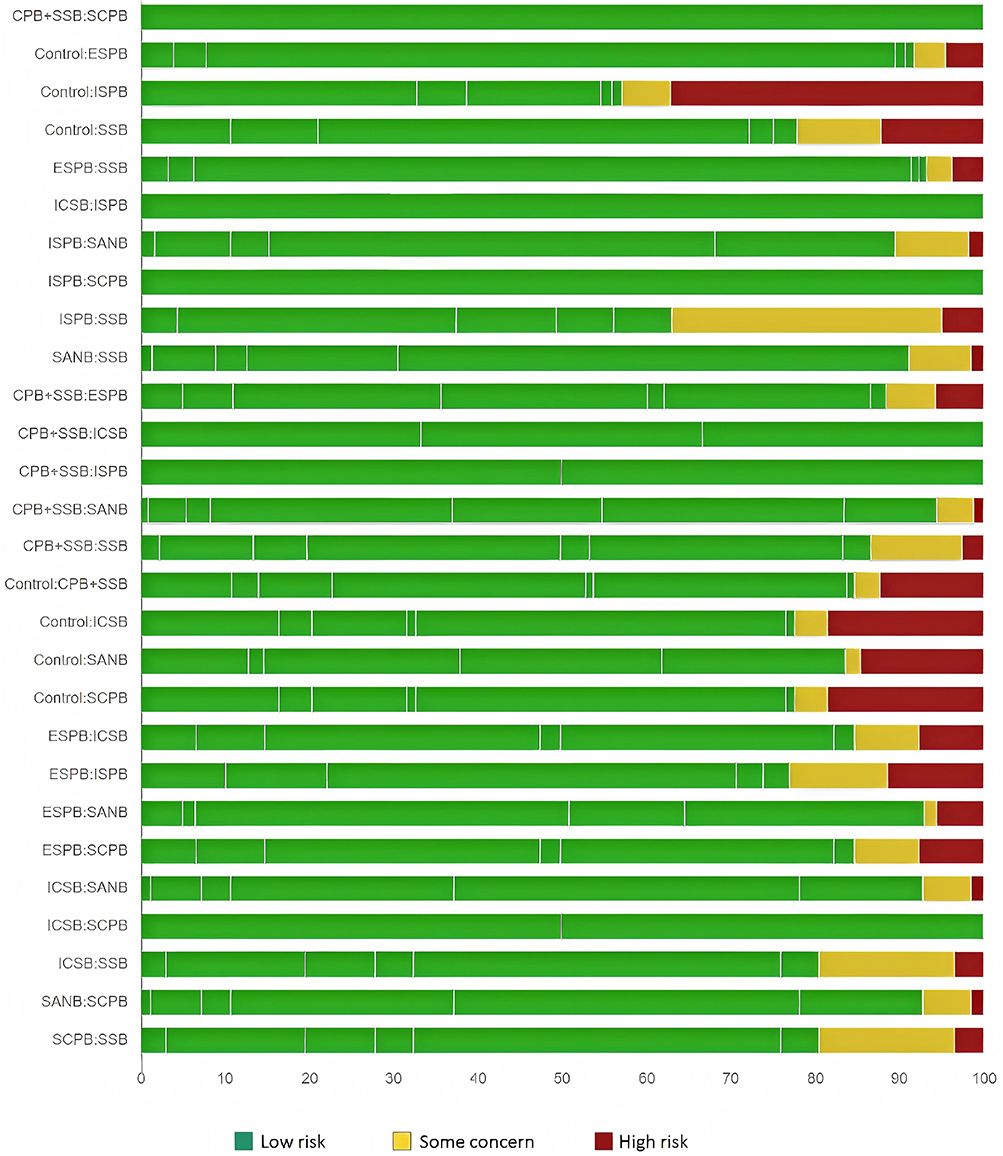 |
Figure 5 Risk of bias of resting VAS at 6 h. |
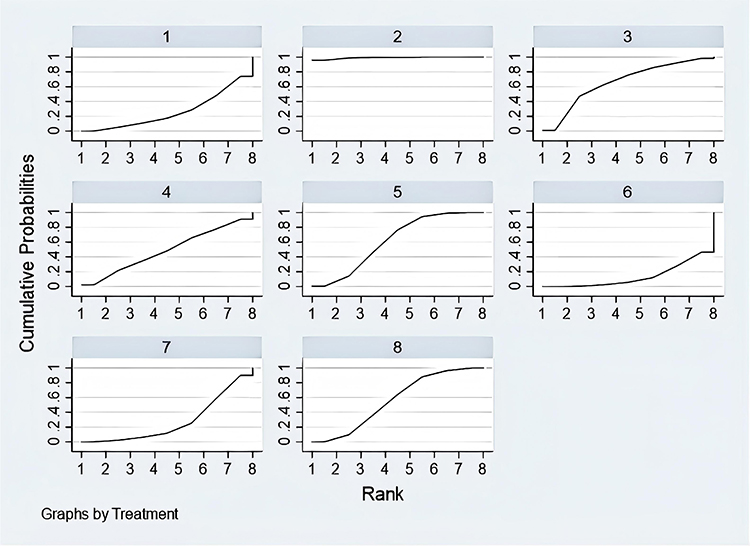 |
Figure 6 SUCRA of resting VAS at 6 h. 1 = CPB+SSB (26.4), 2 = Control (99.2), 3 = ESPB (66.2), 4 = ICSB (48.7), 5 = ISPB (61.6), 6 = SANB (13.6), 7 = SCPB (27.8), 8 = SSB (56.4). ESPB, Erector spinae plane block. SANB, Suprascapular and Axillary Nerve Blocks. SSB, Suprascapular nerve block. CPB, Coracoid approach brachial plexus. ISPB, Interscalene brachial plexus block. SCPB, Supraclavicular brachial plexus block. ICSB, Infraclavicular-suprascapular blocks. |
Resting VAS at 12 h
The analysis included 10 studies with a total of 627 patients. The result was shown in Section 1, Supplementary material. The network map displayed 8 interventions. The network forest plot indicated a high risk of global heterogeneity. The result of node-splitting showed that Control vs. ESPB, Control vs. ISPB, Control vs. SSB, ESPB vs. SSB, and ISPB vs. SSB had a high risk of inconsistency. The ranking showed that ESPB had the lowest SUCRA value (3.4), followed closely by SANB (13.2), ICSB (39.7), SSB (50.6), CPB+SSB (59.8), SCPB (60.2), CCB (62.0), ISPB (62.1).
Resting VAS at 24 h
The analysis included 13 studies with a total of 1042 patients. The result was shown in Section 2, Supplementary material. The network map displayed 9 interventions. The network forest plot did not show any global heterogeneity. The result of node-splitting did not show any significant inconsistency. The ranking showed that SANB had the lowest SUCRA value (2.2), followed closely by UTB (26.6), CPB+SSB (30.7), SCPB (39.0), SSB (41.7), ICSB (46.3), CCB (68.0), ISPB (70.0), ESPB (84.6).
Morphine Consumption Within 24 h
The analysis included 10 studies with a total of 769 patients. The result was shown in Section 3, Supplementary material. The network map displayed 8 interventions. The network forest plot indicated a high risk of global heterogeneity. The result of node-splitting showed that Control vs. ESPB, Control vs. ISPB, Control vs. SSB, ESPB vs. SSB, and ISPB vs. SSB had a high risk of inconsistency. The ranking showed that UTB had the lowest SUCRA value (17.1), followed closely by SSB (20.3), SCPB (28), CCB (39), ISPB (40.7), ICSB (69.4), ESPB (85.5).
HDP
The analysis included 9 studies with a total of 582 patients. The result was shown in Section 4, Supplementary material. The network map displayed 6 interventions. The network forest plot did not show any global heterogeneity. The result of node-splitting did not show any significant inconsistency. The ranking showed that ICSB had the lowest SUCRA value (22.6), followed closely by CPB+SSB (28.1), SCPB (41.7), CCB (48.2), UTB (64.8), ISPB (94.6).
Hoarseness
The analysis included 11 studies with a total of 1079 patients. The result was shown in Section 5, Supplementary material. The network map displayed 6 interventions. The network forest plot did not show any global heterogeneity. The result of node-splitting did not show any significant inconsistency. The ranking showed that ICSB had the lowest SUCRA value (30.2), followed closely by SSB (32.5), UTB (34.0), SCPB (44.9), ISPB (63.7), ISPB+ICPB (94.8).
Horner’s Syndrome
The analysis included 11 studies with a total of 1071 patients. The result was shown in Section 6, Supplementary material. The network map displayed 6 interventions. The network forest plot indicated a high risk of global heterogeneity. The result of node-splitting showed that ISPB vs. SSB and SSB vs. UTB had a high risk of inconsistency. The ranking showed that UTB had the lowest SUCRA value (16.7), followed closely by ICSB (30.3), SSB (46.4), SCPB (49.6), ISPB+ICPB (66.9), ISPB (93.1).
Motor Block
The analysis included 6 studies with a total of 700 patients. The result was shown in Section 7, Supplementary material. The network map displayed 5 interventions. The network forest plot did not show any global heterogeneity. The result of node-splitting did not show any significant inconsistency. The ranking showed that SSB had the lowest SUCRA value (4.5), followed closely by UTB (61.0), SANB (64.8), ISPB (93.1).
PONV
The analysis included 14 studies with a total of 947 patients. The result was shown in Section 8, Supplementary material. The network map displayed 8 interventions. The network forest plot did not show any global heterogeneity. The result of node-splitting showed that ISPB vs. SCPB had a high risk of inconsistency. The ranking showed that ESPB had the lowest SUCRA value (21.7), followed closely by SSB (27.7), SANB (32.2), ISPB (44.2), CPB+SSB (51.1), SCPB (54.0), ICSB (75.6), UTB (77.1).
Summary of Evidences
Table 4 provided a summary of the evidence, including GRADE classifications for each outcome. No single intervention was identified as superior to others regarding analgesia or complication rates. Due to the presence of heterogeneity and inconsistency in the analysis results, we downgraded the quality of evidence for the relevant outcomes. Furthermore, the included studies employed inconsistent definitions for respiratory depression and motor block, which warranted an additional downgrade in the evidence level. Lastly, considerable variations in postoperative pain management protocols prompted a further reduction in the confidence level regarding morphine consumption.
 |
Table 4 Summary of Evidences |
Discussion
In our NMA involving 25 RCTs and 2,039 patients, we evaluated the efficacy of ten types of nerve blocks following shoulder arthroscopy. Our results indicated that SANB, CPB+SSB, and SCPB were more likely to decrease the VAS at 6 h. ESPB, SANB, and ICSB were more likely to decrease the resting VAS at 12 h. SANB, UTB, and CPB+SSB were more likely to decrease the resting VAS at 24 h. UTB, SSB, and SCPB were more likely to decrease morphine consumption within 24 h. The techniques with relatively low incidence of HDP include ICSB (0%), CPB+SSB (21.7%), SCPB (29.5%). The techniques with relatively low incidence of hoarseness include ICSB (0%), SSB (0%), and UTB (4.8%). The techniques with relatively low incidence of Horner’s syndrome include ICSB (0%), SSB (0%), and UTB (5.7%). SSB had the lowest incidence of motor block (1.2%). The techniques with relatively low incidence of PONV include ESPB (9.4%), SSB (15.4%), and SANB (14.3%). From the above data, there is no single technique that simultaneously balances analgesic efficacy and adverse-event incidence. However, SANB was superior to others in reducing pain scores within 24 hours and in lowering the incidence of PONV. ICSB appears to be superior to others in reducing the incidence of HDP, hoarseness, and Horner’s syndrome, but SANB has prevented these complications from occurring via its mechanism of action. Although SSB was superior to others in reducing motor block, it did not demonstrate a primary effect on pain improvement. Additionally, due to inconsistencies in postoperative analgesia regimens and heterogeneity of analysis results, we do not make consistent conclusions regarding morphine consumption.
Currently, many meta-analyses have compared these analgesia strategies for shoulder arthroscopy, reflecting clinicians’ attention to this issue and, at the same time, indicating a lack of more robust evidence to guide clinical practice. We present a comparative analysis between previous researches and our study as follows. Zhang’s study showed that ISPB significantly improved pain on the day of and 1 day after the operation.47 Kalthoff’s study confirmed the analgesic effectiveness of ISPB, SSB, and SANB when compared with control group but did not further compare the relative efficacy strengths and complication profiles among these three techniques.48 White found that SSB did not significantly reduce postoperative pain scores or opioid consumption when compared with ISPB, and the benefits of SSB were limited to Horner’s syndrome, hoarseness, and impaired respiratory function.49 Zhao found that SANB offered greater pain relief than SSB, while there was no difference between ISPB and SANB.50 Sun found that ISPB provided superior analgesia only within the first 6 hours postoperatively compared with SANB, while SANB was associated with lower incidences of numbness/tingling, weakness, Horner’s syndrome, and subjective dyspnea.51 Zhang found that ISPB and CCB provided comparable analgesia and have a similar incidence of PONV.52 These conclusions were similar to ours but still slightly different. Firstly, we both confirm the analgesic effectiveness ISPB, SSB, CCB, and SANB following shoulder arthroscopy. Secondly, ISPB has greater analgesic advantage than SSB, while SSB has greater safety advantage than ISPB. Thirdly, the superior analgesic effect of SANB over SSB can be attributed to its additional blockade of the axillary nerve. While SSB solely targets the suprascapular nerve—which innervates the posterior and superior aspects of the shoulder capsule—SANB also anesthetizes the axillary nerve, which supplies the anterior and inferior portions, resulting in more complete capsular denervation. Fourthly, there is controversy regarding the conclusions about SANB and SIPB. Our results shows that they have a similar VAS at 6 h (MD = −1.68; 95% CI = −3.63 to 0.28), but SANB has a lower VAS at 12 h (MD = −1.49; 95% CI = −2.76 to −0.23) and 24 h (MD = −2.50; 95% CI = −3.73 to −1.27). Finally, only two RCTs report on CCB, but our results support Zhang’s conclusion.
Our findings and previous evidences delineated both the analgesic efficacy and safety of each individual nerve block. In parallel, we advanced a deeper understanding of the shoulder neuroanatomy and the mechanisms underlying single-block techniques, which are essential for explaining differences in outcomes and providing more robust evidence to the conclusion. The neural innervation of the shoulder joint is notably complex, involving multiple nerve pathways originating from both the cervical and brachial plexuses.53 The suprascapular nerve, arising from the upper trunk of the brachial plexus (C5-C6), provides a major sensory contribution to the superior and posterior aspects of the shoulder, including parts of the rotator cuff and glenohumeral joint capsule.23 The axillary nerve, also from C5-C6, supplies sensation to the lateral shoulder region and the inferior capsule, playing a crucial role in posterior and lateral shoulder innervation.23 Additional significant contributions come from the lateral pectoral nerve and the upper roots of the brachial plexus, which supply the anterior shoulder and upper arm regions.53 The cervical plexus, formed by anterior rami of C3-C4, supplies cutaneous sensation to the clavicular area and the upper shoulder.30
Shoulder arthroscopy encompasses several common procedures, each targeting specific anatomical structures with distinct sensory innervation patterns crucial for understanding the source of pain. A subacromial decompression addresses the subacromial bursa, coracoacromial ligament, and the acromion’s inferior surface; the bursa and ligament are innervated by the suprascapular and lateral pectoral nerves, while the acromial periosteum is served by the supraclavicular nerves.54 Rotator cuff repair focuses on the tendons of the supraspinatus, infraspinatus, teres minor, and subscapularis, which are innervated by the suprascapular, axillary, and subscapular nerves, respectively.55 For instability, a Bankart repair involves the anteroinferior glenoid labrum and the inferior glenohumeral ligament complex, which receive sensory input primarily from the axillary nerve.56 Similarly, a SLAP lesion repair targets the superior labrum and biceps anchor, a region predominantly innervated by the suprascapular nerve.57 Procedures for pathologies of the long head of the biceps tendon, namely tenotomy or tenodesis, involve a structure innervated at its intra-articular portion by the suprascapular nerve.57 Finally, an acromioclavicular joint resection (Mumford procedure) involves the joint capsule—innervated by the suprascapular, lateral pectoral, and axillary nerves—and the distal clavicle, whose periosteum is supplied by the supraclavicular nerves.58 This intricate and overlapping innervation demands precise and strategic nerve blockade to achieve comprehensive analgesia following shoulder surgery, but the current techniques can only block the main nerves involved in analgesia.
The ISPB engenders extensive blockade of the C5-C7 nerve roots, thereby providing robust anesthesia and analgesia for most upper limb surgeries including those involving the shoulder.22 The SCPB offers a similarly wide coverage, often with technical ease under ultrasound guidance, making it a popular choice.27 The UTB focuses directly on the C5-C6 roots, enables a more selective approach with potentially fewer side effects associated with higher levels of plexus blockade.26 The CPB targets the lateral cord adjacent to the coracoid process, predominantly anesthetizes anterior shoulder structures and the lateral upper limb.34 The ESPB is believed to exert its effect through the spread of local anesthetic to dorsal and ventral rami of thoracic spinal nerves, potentially influencing the posterior and lateral shoulder regions.33 The CCB targets the brachial plexus cords in the infraclavicular area, primarily affects the lateral and medial cords.24 The SSB and SANB are more targeted nerve blocks, focusing primarily on the key sensory pathways supplying the superior and posterior shoulder, offering effective analgesia with relatively low complication rates.23 The ICPB involves infiltration around the C3-C4 nerve roots, predominantly covering the superficial cervical plexus and thereby providing cutaneous anesthesia over the anterior shoulder and clavicular region.30 The ICSB combines approaches to both the suprascapular nerve and the brachial plexus in the infraclavicular region, aims to optimize coverage of both anterior and posterior shoulder structures.41
For high-level plexus blocks such as ISPB, the incidence of HDP remains a significant concern—especially in patients with compromised respiratory function. Horner’s syndrome and nerve injury are other established potential complications. Vascular puncture and pneumothorax are notable risks with SCPB and infraclavicular blocks, emphasizing the importance of ultrasound guidance and meticulous technique. Targeted nerve blocks, such as SSB and SANB, tend to have a safer profile but still carry risks of nerve injury or inadvertent intravascular injection. Cervical plexus blocks can easily cause hoarseness due to recurrent laryngeal nerve involvement, as well as diaphragmatic paralysis if the phrenic nerve is inadvertently affected.
In summary, nerve blockade strategies for shoulder arthroscopy are diverse, with each technique offering distinct advantages and limitations. An in-depth understanding of the underlying anatomy, mechanism of action, and potential risks is essential for optimizing perioperative pain management.
Limitations
Despite the comprehensive overview provided, this review has certain limitations that should be acknowledged. Firstly, our NMA is subject to the inherent limitation common to all meta-analyses. The included studies had differences in study design, sample size, local anesthetic agents, postoperative analgesic regimen, and technique modalities, which may affect the generalizability of the findings. Meanwhile, these inherent limitations contributed to the local inconsistency observed for certain comparisons. Secondly, the interventions included in this paper solely involved single-injection nerve block techniques, with a paucity of compering with local infiltration analgesia59 and continuous nerve block60 which have also been shown to provide significant analgesic benefits. Thirdly, the safety profiles are also often reported in isolated cases or small series, which may underestimate rare but serious adverse events such as pneumothorax, nerve injury, or local anesthetic systemic toxicity. Finally, most of the available data focus on short-term analgesic effects, with a paucity of long-term follow-up information on sustained pain relief, functional recovery, or nerve injury.
Conclusions
Our findings support the use of SANB as a superior analgesic technique following arthroscopic shoulder surgery, improving pain scores within 24 hours and reducing the incidence of PONV, HDP, hoarseness, and Horner’s syndrome. Although SSB more effectively reduces the incidence of motor block, its analgesic efficacy remains comparatively weak. However, it is important to acknowledge that for certain comparisons—specifically, ISPB vs. SANB, and SANB vs. SSB—significant inconsistency was detected between direct and indirect evidence within the NMA. Consequently, clinicians should interpret the results for these comparisons with caution, and further high-quality head-to-head randomized controlled trials are warranted to validate these observations.
Funding
The study is supported by the Hospital Foundation of Gansu Provincial Hospital (21GSSYC-36), the Gansu Provincial Health Industry project (GSWSKY2023-12), the Gansu Provincial Anesthesia and Brain Function Clinical Medical Research Center project (21JR7RA675), and the Gansu Province Key Talent Project: Talent Cultivation in Anesthesiology of Gansu Province Based on a Diversified Innovative Training System (2023RCXM13).
Disclosure
The authors declare that they have no competing interests.
References
1. Lowry V, Lavigne P, Zidarov D, et al. A systematic review of clinical practice guidelines on the diagnosis and management of various shoulder disorders. Arch Phys Med Rehabil. 2024;105(2):411–15. doi:10.1016/j.apmr.2023.09.022
2. Huri G, Popescu IA, Rinaldi VG, et al. The evolution of arthroscopic shoulder surgery: current trends and future perspectives. J Clin Med. 2025;14(7):2405. doi:10.3390/jcm14072405
3. Kang RA, Jeong JS, Yoo JC, et al. Improvement in postoperative pain control by combined use of intravenous dexamethasone with intravenous dexmedetomidine after interscalene brachial plexus block for arthroscopic shoulder surgery: a randomised controlled trial. Eur J Anaesthesiol. 2019;36(5):360–368. doi:10.1097/EJA.0000000000000977
4. Aldecoa C, Bettelli G, Bilotta F, et al. Update of the European society of anaesthesiology and intensive care medicine evidence-based and consensus-based guideline on postoperative delirium in adult patients. Eur J Anaesthesiol. 2024;41(2):81–108. doi:10.1097/EJA.0000000000001876
5. Baldo BA. Toxicities of opioid analgesics: respiratory depression, histamine release, hemodynamic changes, hypersensitivity, serotonin toxicity. Arch Toxicol. 2021;95(8):2627–2642. doi:10.1007/s00204-021-03068-2
6. Beverly A, Kaye AD, Ljungqvist O, et al. Essential elements of multimodal analgesia in Enhanced Recovery After Surgery (ERAS) guidelines. Anesthesiol Clin. 2017;35(2):e115–e143. doi:10.1016/j.anclin.2017.01.018
7. Chen YK, Boden KA, Schreiber KL. The role of regional anaesthesia and multimodal analgesia in the prevention of chronic postoperative pain: a narrative review. Anaesthesia. 2021;76(1):8–17. doi:10.1111/anae.15256
8. Kamineni S, Cheppalli NS. Surgeon-administered intraoperative brachial plexus block for open shoulder surgery - a novel and safe technique. Shoulder Elbow. 2023;15(5):571–576. doi:10.1177/17585732221127432
9. Bellew B, Harrop-Griffiths WA, Bedforth N. Interscalene brachial plexus blocks and phrenic nerve palsy. Anesthesiology. 2014;120(4):1056–1057. doi:10.1097/ALN.0000000000000129
10. Alzahrani T, Alnajjar M, Algarni AD, et al. Delayed Horner’s syndrome following ultrasound- guided interscalene brachial plexus block. Saudi J Anaesth. 2014;8(1):121–123. doi:10.4103/1658-354X.125972
11. Shio H, Sakura S, Motooka A, et al. Severe and persistent nerve palsy after ultrasound-guided continuous interscalene brachial plexus block in a teenager undergoing shoulder surgery: a case report. JA Clin Rep. 2020;6(1):15. doi:10.1186/s40981-020-0315-1
12. Chan CW, Peng PW. Suprascapular nerve block: a narrative review. Reg Anesth Pain Med. 2011;36(4):358–373. doi:10.1097/AAP.0b013e3182204ec0
13. Hata A, Sato M, Kunisawa T. Ultrasound-guided proximal-anterior axillary nerve block: a novel technique. Med Ultrason. 2024;26(3):323–324. doi:10.11152/mu-4426
14. Hutton B, Salanti G, Caldwell DM, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. 2015;162(11):777–784. doi:10.7326/M14-2385
15. Higgins JP, Altman DG, Gøtzsche PC, et al. The cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. doi:10.1136/bmj.d5928
16. Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):9246. doi:10.1136/bmj.39489.470347.AD
17. Huang J, Liu X, Wang L, et al. Regional analgesia techniques following nephrectomy: a systematic review and network meta-analysis. Minerva Anestesiol. 2025;91(4):314–324. doi:10.23736/S0375-9393.24.18373-3
18. Noetel M, Sanders T, Gallardo-Gómez D, et al. Effect of exercise for depression: systematic review and network meta-analysis of randomised controlled trials. BMJ. 2024;384:e075847. doi:10.1136/bmj-2023-075847
19. Treillet E, Laurent S, Hadjiat Y. Practical management of opioid rotation and equianalgesia. J Pain Res. 2018;11:2587–2601. doi:10.2147/JPR.S170269
20. Luo D, Wan X, Liu J, et al. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res. 2018;27(6):1785–1805. doi:10.1177/0962280216669183
21. Wan X, Wang W, Liu J, et al. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14:135. doi:10.1186/1471-2288-14-135
22. Aksu R, Biçer C, Ülgey A, et al. Comparison of interscalene brachial plexus block and intra-articular local anesthetic administration on postoperative pain management in arthroscopic shoulder surgery. Braz J Anesthesiol. 2015;65(3):222–229. doi:10.1016/j.bjane.2014.06.005
23. Pitombo PF, Meira Barros R, Matos MA, et al. Selective suprascapular and axillary nerve block provides adequate analgesia and minimal motor block. Comparison with interscalene block. Braz J Anesthesiol. 2013;63(1):45–51. doi:10.1016/S0034-7094(13)70197-1
24. Jo Y, Oh C, Lee WY, et al. Randomised comparison between superior trunk and costoclavicular blocks for arthroscopic shoulder surgery: a noninferiority study. Eur J Anaesthesiol. 2022;39(10):810–817. doi:10.1097/EJA.0000000000001735
25. Petroff D, Wiegel M, Pech V, et al. Differential lung ventilation assessed by electrical impedance tomography in ultrasound-guided anterior suprascapular nerve block vs. interscalene brachial plexus block: a patient and assessor-blind, randomised controlled trial. Eur J Anaesthesiol. 2020;37(12):1105–1114. doi:10.1097/EJA.0000000000001367
26. Jo Y, Oh C, Lee WY, et al. Diaphragm-sparing efficacy of subparaneural upper trunk block for arthroscopic shoulder surgery: a randomised controlled trial. Eur J Anaesthesiol. 2024;41(10):760–768. doi:10.1097/EJA.0000000000002034
27. Ryu T, Kil BT, Kim JH. Comparison between ultrasound-guided supraclavicular and interscalene brachial plexus blocks in patients undergoing arthroscopic shoulder surgery: a prospective, randomized, parallel study. Medicine. 2015;94(40):e1726. doi:10.1097/MD.0000000000001726
28. Al-Kaisy A, McGuire G, Chan VW, et al. Analgesic effect of interscalene block using low-dose bupivacaine for outpatient arthroscopic shoulder surgery. Reg Anesth Pain Med. 1998;23(5):469–473.
29. Abdallah FW, Wijeysundera DN, Laupacis A, et al. Subomohyoid anterior suprascapular block versus interscalene block for arthroscopic shoulder surgery: a multicenter randomized trial. Anesthesiology. 2020;132(4):839–853. doi:10.1097/ALN.0000000000003132
30. Han J, Xu Y, Shan Y, et al. Could C3, 4, and 5 nerve root block be a better alternative to interscalene block plus intermediate cervical plexus block for patients undergoing surgery for midshaft and medial clavicle fractures? A randomized controlled trial. Clin Orthop Relat Res. 2023;481(4):798–807. doi:10.1097/CORR.0000000000002479
31. Aliste J, Bravo D, Fernández D, et al. A randomized comparison between interscalene and small-volume supraclavicular blocks for arthroscopic shoulder surgery. Reg Anesth Pain Med. 2018;43(6):590–595. doi:10.1097/AAP.0000000000000767
32. Kim DH, Lin Y, Beathe JC, et al. Superior trunk block: a phrenic-sparing alternative to the interscalene block: a randomized controlled trial. Anesthesiology. 2019;131(3):521–533. doi:10.1097/ALN.0000000000002841
33. Abdelhaleem NF, Abdelatiff SE, Abdel Naby SM. Comparison of erector spinae plane block at the level of the second thoracic vertebra with suprascapular nerve block for postoperative analgesia in arthroscopic shoulder surgery. Pain Physician. 2022;25(8):577–585.
34. He W, Wu Z, Su S, et al. Coracoid approach brachial plexus block combined with posterior suprascapular nerve block provides analgesia for shoulder arthroscopy: a randomized controlled trial. Sci Rep. 2025;15(1):9555. doi:10.1038/s41598-025-93881-x
35. Kang R, Jeong JS, Chin KJ, et al. Superior trunk block provides noninferior analgesia compared with interscalene brachial plexus block in arthroscopic shoulder surgery. Anesthesiology. 2019;131(6):1316–1326. doi:10.1097/ALN.0000000000002919
36. Auyong DB, Hanson NA, Joseph RS, et al. Comparison of anterior suprascapular, supraclavicular, and interscalene nerve block approaches for major outpatient arthroscopic shoulder surgery: a randomized, double-blind, noninferiority trial. Anesthesiology. 2018;129(1):47–57. doi:10.1097/ALN.0000000000002208
37. Lee MG, Shin YJ, You HS, et al. A comparison of anesthetic quality between interscalene block and superior trunk block for arthroscopic shoulder surgery: a randomized controlled trial. Pain Physician. 2021;24(3):235–242.
38. Wiegel M, Moriggl B, Schwarzkopf P, et al. Anterior suprascapular nerve block versus interscalene brachial plexus block for shoulder surgery in the outpatient setting: a randomized controlled patient- and assessor-blinded trial. Reg Anesth Pain Med. 2017;42(3):310–318. doi:10.1097/AAP.0000000000000573
39. Dhir S, Sondekoppam RV, Sharma R, et al. A comparison of combined suprascapular and axillary nerve blocks to interscalene nerve block for analgesia in arthroscopic shoulder surgery: an equivalence study. Reg Anesth Pain Med. 2016;41(5):564–571. doi:10.1097/AAP.0000000000000436
40. Cabaton J, Nové-Josserand L, Mercadal L, et al. Analgesic efficacy of ultrasound-guided interscalene block vs. supraclavicular block for ambulatory arthroscopic rotator cuff repair: a randomised noninferiority study. Eur J Anaesthesiol. 2019;36(10):778–786. doi:10.1097/EJA.0000000000001065
41. Aliste J, Bravo D, Finlayson RJ, et al. A randomized comparison between interscalene and combined infraclavicular-suprascapular blocks for arthroscopic shoulder surgery. Can J Anaesth. 2018;65(3):280–287. doi:10.1007/s12630-017-1048-0
42. Liu XN, Noh YM, Yang CJ, et al. Effects of a single-dose interscalene block on pain and stress biomarkers in patients undergoing arthroscopic rotator cuff repair: a randomized controlled trial. Arthroscopy. 2017;33(5):918–926. doi:10.1016/j.arthro.2016.09.018
43. Karaman T, Karaman S, Aşçı M, et al. Comparison of ultrasound-guided supraclavicular and interscalene brachial plexus blocks in postoperative pain management after arthroscopic shoulder surgery. Pain Pract. 2019;19(2):196–203. doi:10.1111/papr.12733
44. Lim YC, Koo ZK, Ho VW, et al. Randomized, controlled trial comparing respiratory and analgesic effects of interscalene, anterior suprascapular, and posterior suprascapular nerve blocks for arthroscopic shoulder surgery. Korean J Anesthesiol. 2020;73(5):408–416. doi:10.4097/kja.20141
45. Lee Y, Bang S, Chung J, et al. Costoclavicular block as a diaphragm-sparing nerve block for shoulder surgery: a randomized controlled trial. Korean J Anesthesiol. 2025;78(1):30–38. doi:10.4097/kja.24595
46. Lee JJ, Kim DY, Hwang JT, et al. Effect of ultrasonographically guided axillary nerve block combined with suprascapular nerve block in arthroscopic rotator cuff repair: a randomized controlled trial. Arthroscopy. 2014;30(8):906–914. doi:10.1016/j.arthro.2014.03.014
47. Yan S, Zhao Y, Zhang H. Efficacy and safety of interscalene block combined with general anesthesia for arthroscopic shoulder surgery: a meta-analysis. J Clin Anesth. 2018;47:74–79. doi:10.1016/j.jclinane.2018.03.008
48. Kalthoff A, Sanda M, Tate P, et al. Peripheral nerve blocks outperform general anesthesia for pain control in arthroscopic rotator cuff repair: a systematic review and meta-analysis. Arthroscopy. 2022;38(5):1627–1641. doi:10.1016/j.arthro.2021.11.054
49. White L, Reardon D, Davis K, et al. Anterior suprascapular nerve block versus interscalene brachial plexus block for arthroscopic shoulder surgery: a systematic review and meta-analysis of randomized controlled trials. J Anesth. 2022;36(1):17–25. doi:10.1007/s00540-021-03000-z
50. Zhao J, Xu N, Li J, et al. Efficacy and safety of suprascapular nerve block combined with axillary nerve block for arthroscopic shoulder surgery: a systematic review and meta-analysis of randomized controlled trials. Int J Surg. 2021;94:106111. doi:10.1016/j.ijsu.2021.106111
51. Sun C, Zhang X, Ji X, et al. Suprascapular nerve block and axillary nerve block versus interscalene nerve block for arthroscopic shoulder surgery: a meta-analysis of randomized controlled trials. Medicine. 2021;100(44):e27661. doi:10.1097/MD.0000000000027661
52. Zhang W, Guo Z, Hou X, et al. Comparison of interscalene block with costoclavicular block for arthroscopic shoulder surgery: a meta-analysis. Medicine. 2025;104(29):e43094. doi:10.1097/MD.0000000000043094
53. Park AJ, Liu J, Sethi P, et al. Identification of the sensory dependent locations of the shoulder joint to optimize surgical approaches and reduce postoperative pain: a systematic review. Surg Technol Int. 2020;37:331–335.
54. Aresti NA, Di Mascio L. Subacromial decompression surgery for shoulder pain. BMJ. 2019;364:l586. doi:10.1136/bmj.l586
55. Uquillas CA, Capogna BM, Rossy WH, et al. Postoperative pain control after arthroscopic rotator cuff repair. J Shoulder Elbow Surg. 2016;25(7):1204–1213. doi:10.1016/j.jse.2016.01.026
56. Rodriguez K, Hurley ET, Park CN, et al. Complications following arthroscopic Bankart repair: a systematic review. J Shoulder Elbow Surg. 2024;33(2):435–440. doi:10.1016/j.jse.2023.08.013
57. Shin MH, Baek S, Kim TM, et al. Biceps tenodesis versus Superior Labral Anterior and Posterior (SLAP) lesion repair for the treatment of SLAP lesion in overhead athletes: a systematic review and meta-analysis. Am J Sports Med. 2022;50(14):3987–3997. doi:10.1177/03635465211039822
58. Hohmann E, Tetsworth K, Glatt V. Open versus arthroscopic acromioclavicular joint resection: a systematic review and meta-analysis. Arch Orthop Trauma Surg. 2019;139(5):685–694. doi:10.1007/s00402-019-03114-w
59. Yung EM, Got TC, Patel N, et al. Intra-articular infiltration analgesia for arthroscopic shoulder surgery: a systematic review and meta-analysis. Anaesthesia. 2021;76(4):549–558. doi:10.1111/anae.15172
60. VVG A, Farey JE, Karunaratne S, et al. Subacromial analgesia via continuous infusion catheter vs. placebo following arthroscopic shoulder surgery: a systematic review and meta-analysis of randomized trials. J Shoulder Elbow Surg. 2020;29(3):471–482. doi:10.1016/j.jse.2019.11.010
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Psychological Interventions on Abstinence in Patients with Alcohol Use Disorder: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials
Zhang P, Zhan J, Wang S, Tang Y, Chen H, Wang Y, Wei X, Wen H, Pan T, Chen Z, Tang C, Xu N, Lu L
Neuropsychiatric Disease and Treatment 2022, 18:1815-1830
Published Date: 23 August 2022
Effect of Exercise Interventions on Health-Related Quality of Life in Patients with Fibromyalgia Syndrome: A Systematic Review and Network Meta-Analysis
Zhang KD, Wang LY, Zhang ZH, Zhang DX, Lin XW, Meng T, Qi F
Journal of Pain Research 2022, 15:3639-3656
Published Date: 22 November 2022
Different Intensities of Evening Exercise on Sleep in Healthy Adults: A Systematic Review and Network Meta-Analysis
Yue T, Liu X, Gao Q, Wang Y
Nature and Science of Sleep 2022, 14:2157-2177
Published Date: 14 December 2022
Nonpharmacological Interventions for Management of the Pain-Fatigue-Sleep Disturbance Symptom Cluster in Breast Cancer Patients: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials
He CC, Lin DM, Liu HZ, Wang FF, Guo XF, Zhang XB, Ai YQ, Meng LM
Journal of Pain Research 2023, 16:2713-2728
Published Date: 7 August 2023
Efficacy of Acupuncture-Related Therapy for Migraine: A Systematic Review and Network Meta-Analysis
Liu Y, Wang Y, Mi C, Wang Z, Han Y, Qi X, Ding X
Journal of Pain Research 2024, 17:1107-1132
Published Date: 15 March 2024