Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Psychological Interventions on Abstinence in Patients with Alcohol Use Disorder: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials
Authors Zhang P ![]() , Zhan J, Wang S
, Zhan J, Wang S ![]() , Tang Y, Chen H
, Tang Y, Chen H ![]() , Wang Y, Wei X, Wen H, Pan T, Chen Z, Tang C
, Wang Y, Wei X, Wen H, Pan T, Chen Z, Tang C ![]() , Xu N, Lu L
, Xu N, Lu L ![]()
Received 30 May 2022
Accepted for publication 8 August 2022
Published 23 August 2022 Volume 2022:18 Pages 1815—1830
DOI https://doi.org/10.2147/NDT.S372300
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Peiming Zhang,1 Jie Zhan,2 Shuting Wang,1 Yuyuan Tang,1 Huishan Chen,1 Yiqiao Wang,1 Xiaojing Wei,1 Hao Wen,3 Ting Pan,4 Ze Chen,1 Chunzhi Tang,1 Nenggui Xu,1 Liming Lu1
1Clinical Research and Big Data Laboratory, South China Research Center for Acupuncture and Moxibustion, Medical College of Acu-Moxi and Rehabilitation, Guangzhou University of Chinese Medicine, Guangzhou City, Guangdong Province, People’s Republic of China; 2Postdoctoral Research Station, Department of Rehabilitation, The Second Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou City, Guangdong Province, People’s Republic of China; 3Department of Neurology, Sun Yat-sen Memorial Hospital of Sun Yat-sen University, Guangzhou City, Guangdong Province, People’s Republic of China; 4TCM Department, Foshan Fosun Chancheng Hospital, Foshan City, Guangdong Province, People’s Republic of China
Correspondence: Liming Lu, Clinical Research and Data Center, South China Research Center for Acupuncture and Moxibustion, Medical College of Acu-Moxi and Rehabilitation, Guangzhou University of Chinese Medicine, No. 232, Waihuan East Road, University Town, Xiaoguwei Street, Panyu District, Guangzhou City, Guangdong Province, People’s Republic of China, Tel +8613751779800, Fax +862039358716, Email [email protected] Chunzhi Tang, Email [email protected]
Purpose: Accumulating research suggests that psychotherapy helps improve abstinence but the difference in the efficacy of multiple psychotherapies in alcohol use disorder (AUD) remains to be explored.
Patients and Methods: A systematic search of databases (Pubmed, Embase, Cochrane Central Register of Controlled Trials (CENTRAL), and EBSCO) for studies (published from inception to April 10th.) of adults diagnosed with AUD accepting psychotherapies was conducted. Studies covering 9 countries and regions. The qualitative analysis pooled 2646 individuals from 34 randomized controlled trials (RCTs) and the networks included 1928 participants (23 RCTs). The outcomes included percentage of days abstinent (PDA), change in drinks per drinking day (change in DDD), and change in craving compared among individuals accepting various psychotherapies. The protocol followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA), and was registered on the International Prospective Register of Systematic Reviews (PROSPERO).
Results: For the network of PDA, motivational enhancement treatment (MET) (35.44, 11.78 to 59.09, high-certainty) and couple therapy (CT) (28.89, 13.42 to 44.36, moderate-certainty) were significantly different from treatment as usual (TAU) with the surface under the cumulative ranking curve (SUCRA) mean rank 1.9 and 1.9 respectively. TAU+supportive psychotherapy (SP) was better than TAU for the change in DDD in the high-quality direct comparison.
Conclusion: The motivational enhancement and the couple therapy show potential amelioration for alcohol abstinence. Additionally, the preferred interventions are different for improving PDA and change in DDD. The evidence network remains to be strengthened.
Keywords: alcohol use disorder, psychotherapy, randomized controlled trial, systematic review, network meta-analysis
Introduction
Alcohol use disorder (AUD) is one of the most common and far-reaching diseases in the current world, increasingly becoming an important public health and social problem. According to the latest global report, alcohol exposure showed an increasing trend in the world. AUD is not only the main cause of the morbidity and mortality burden of various diseases but also the source of intricate effects on mental health.1,2 However, former studies showed that the AUD population has not received sufficient and effective treatment yet,3,4 and it is expected that by 2030, drinking in many regions will continue to increase. Therefore, it is emphasized that cost-effective policies and interventions should be formulated to increase awareness of alcohol risks and reduce consumption.2
AUD usually requires comprehensive intervention to improve both adherence and effectiveness. Control impairment of alcohol use is regarded as an important criterion grouping of pathological models for the diagnosis of substance use disorders: consumption out of control, failed abstinence attempts, craving, and burden derived from seeking.5 When exposed to alcohol-related stimuli, the behavioral effects of brain changes may manifest as repeated relapses and compulsion. Experts6,7 believe that abstinence management involves not only pharmacotherapy but psychotherapy because it is beneficial to help internalize changes in attitudes and behaviors that favor preventing relapse8 with fewer adverse effects and ethical objections but better compliance and affordability than medication treatment.9
Although many clinical studies were on psychotherapy alone or in combination for AUD, most systematic reviews and meta-analyses have only used internal comparisons of cognitive behavioral therapy (CBT),10–12 motivational enhancement treatment (MET),13 couple therapy (CT),14 and mindfulness-oriented therapy (MOT),15 and some conducted a large-scale meta-comparison referred to addiction diseases in general or included mixed study types.16 However, there is no network comparison of randomized controlled trials (RCTs) of multiple types of psychological intervention for AUD and it is unclear which type results in better outcomes. This study conducted a systematic review and network meta-analysis (NMA) of psychotherapies for AUD, which will provide a reference for clinical application and evidence-based research directions of psychotherapy for AUD.
Methods
The meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and we used the PRISMA checklist when reporting (Table S1).17 This protocol has been registered at PROSPERO under registration number CRD42021259428.
Study Inclusion Criteria
All relevant studies were considered eligible if they included the following: randomization; an appropriate comparison group (ie, treatment as usual, usual care, or another active treatment); adult patients (aged 18+) diagnosed with AUD, AD, or alcohol abuse5,18–23 (details found in Table S2); participants receiving a form of psychotherapy (S3), defined by the American Psychiatric Association (APA),24 and classified using the Nottingham Classification of Psychotherapies (Figure S3), as a single or major intervention or as an auxiliary means of integration; assessment of the percentage of days abstinent (PDA), the change in drinks per drinking day (change in DDD) and the change in craving using a validated measure.
PDA was used to measure the self-control and was assessed by Timeline Followback Interviews (TLFBs) or Form-90.25 To some extent, the higher the PDA is, the better the patient’s ability to control drinking is. Change in DDD was assessed by TLFBs or Form-90 to evaluate the change in average drinking on a drinking day, using a “standard drink” as a measure. Change in craving was assessed from the Desire for Alcohol Questionnaire (DAQ), Obsessive-Compulsive Drinking Scale (OCDS), three Likert-type scale items, the Alcohol Craving Questionnaire (ACQ), and the Penn Alcohol Craving Scale (PACS).26 Craving is defined by The Diagnostic and Statistical Manual of Mental Disorders, the 5th version (DSM-V) as an intense desire or urge for the drug, which may occur at any moment, especially when one is exposed to an environment where the alcohol previously was obtained or used;21 higher scores on all scales above indicate a higher level of craving.
Database and Search Strategy
We systematically searched MEDLINE, Embase, Cochrane Central Register of Controlled Trials (CENTRAL), and APA PsycArticles & PsycInfo via EBSCO Databases (published from inception to Apr. 2022). Searches terms about disorders and interventions included alcoholism, alcohol dependence, alcohol addiction, alcohol use disorder, psychotherapy, sensory art therapies, psychological techniques, etc., as either key terms or keywords, with publication types including randomized controlled trial, controlled clinical trial, randomized, etc., published from inception (detailed retrievals are in S4) to April 10th.
Study Screening and Selection
According to the predefined inclusion criteria, two authors (H.C.and S.W.) separately reviewed the list of papers retrieved through preliminarily screening titles and abstracts and full text with Endnote X7 to decide which could be included. Any controversial points were resolved with discussion after an independent review of the list of papers by another author (P.Z.).
Data Extraction and Management
Two authors (Y.W. and X.W.) separately extracted demographic data (country, diagnosis, criterion, comorbidity, outcome, sample size, age, sex, arm, treatment location, level of education, occupational status, marital status, and special or common population), and attempted to obtain the unpublished information necessary for the analysis from the original author by email. If missing information could not be provided, partial publication data were not considered. Studies excluded due to missing data were discussed with regard to their main characteristics to exclude possible biases.
Risk of Bias Assessment
Three authors (T.P. and Z.C. and P. Z.) separately assessed the quality of all reports using the Cochrane risk-of-bias tool for randomized trials (RoB)27 to evaluate study methodological rigor with low, high, or unclear risk of bias (ROB) ratings for each domain. If there were conflicts, a fourth author provided guidance (L.L.) for consensus. To assess small-study effects, funnel plots for meta-analyses including at least 10 trials of varying sizes were planned (when available).
GRADE Quality Assessment of Evidence
The evaluation system GRADE (Grade of Recommendations Assessment, Development and Evaluation) was used to estimate the quality of direct, indirect, and network evidence. The direct evidence effect value and 95% CI are derived from the pairwise comparison results, and the indirect evidence effect value and 95% CI are derived from the node-splitting method. The network evidence comes from the meta-analysis results after fitting the consistency model.
Data Analysis Plan
Measures of Treatment Effect
Three main continuous variables were analyzed, in which PDA used the weighted mean difference (WMD) as the effect size (ES); Cohen’s d method28 was used to eliminate the influence of nonuniform dimensions of DDD and craving change. The closest estimation points to the post-last-treatment were considered. The ES of PDA was computed so that a positive value indicated a favorable outcome (ie, abstinence improvement), while changes in DDD and in craving were computed so that a negative value indicated a favorable outcome (ie, reduction of alcohol consumption and craving). Data based on the intention-to-treat (ITT) sample or modified sample were preferred over data based on completers for all analyses.
Pairwise Meta-Analysis
Direct pairwise meta-analysis (DMA) was conducted by Review Manager Version 5.0. for continuous outcomes. The MD was used to assess the effects on PDA of treatment and standardized mean difference (SMD) was used to assess the effects on DDD and craving change. The percentage of variability across trials was estimated with the I2 statistic if attributable to heterogeneity beyond chance, which was deemed significant when P<0.05 or I2>50%. The random-effects model was also considered, although the data were pooled with the fixed-effects model to ensure model robustness in the case of significant heterogeneity.
Network Meta-Analysis
Frequentist NMA29 was conducted using Stata 14 taking all indirect comparisons into account. The agreement between direct and indirect evidence was assessed using a node-splitting analysis to test consistency.30,31 For any group of interventions included in the closed loop, the results were categorized into direct and indirect comparisons, and the difference was calculated and tested for statistical significance. If P>0.05, they exhibit consistency; otherwise inconsistency. If there was no inconsistency, a consistency model to show which psychotherapy was the most effective was used to produce rank probability plots, data expressed in form of MD or SMD with 95% CI. When there is inconsistency, the source will be discussed. If inconsistency could not be explained, the indirect evidence is unreliable.
Additional Analysis
This study supplemented a network comparison of intervention compliance to assess the patient’s ability to adhere to a specific intervention, using the risk ratio (RR) as the ES. Separate meta-analyses by intervention type (psychotherapies alone or combined) or time point (short-, medium-, and long-term) were planned to assess the robustness of the results; sensitivity analyses were planned that excluded studies with high ROBs; however, these were not completed owing to sparsity of data.
Results
Search results
The search produced 12,937 papers after 3728 duplicates were removed, of which 12,313 were excluded after preliminary screening. After the full-text screening, data were included from 34 independent studies (Table S5) for the qualitative systematic review of the 624 papers in the remaining pool (Figure 1).
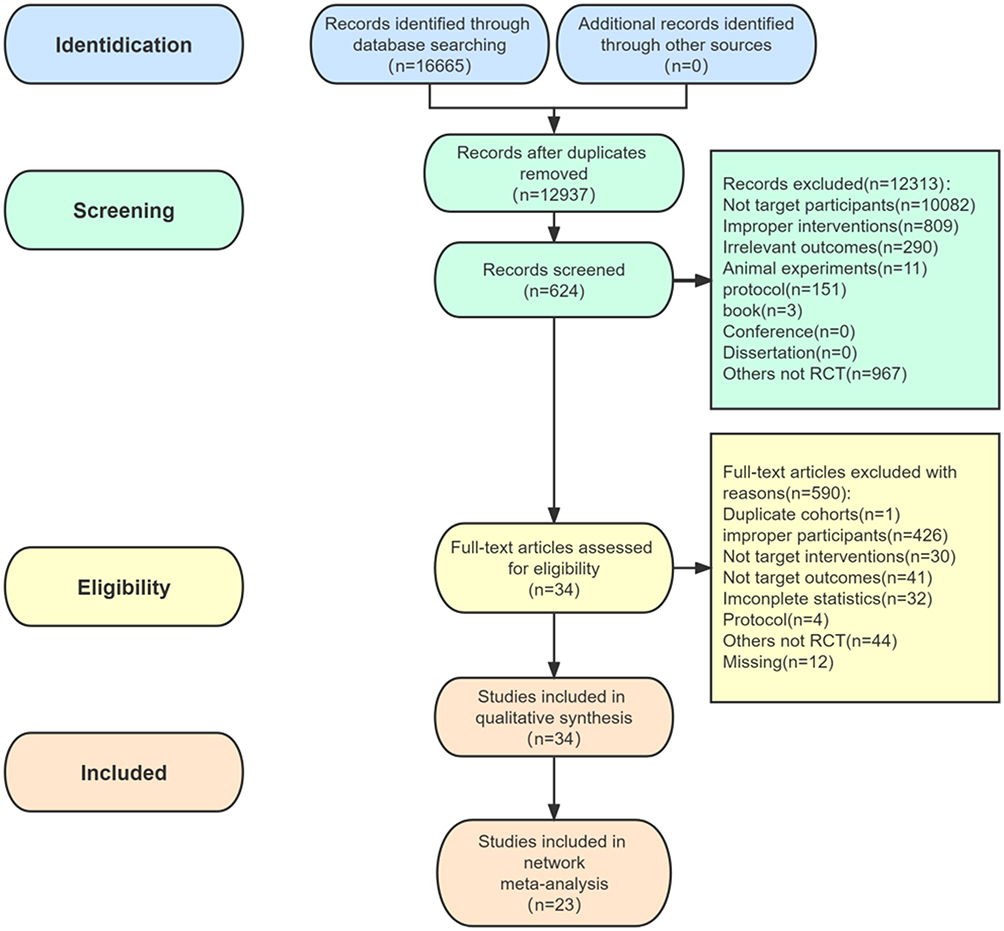 |
Figure 1 Flowchart of study selection. |
Study Characteristics
The data pool for systematic analysis included 2646 individuals (34 RCTs) and for loop included 1928 (23 RCTs), covering: 9 countries and regions; 1981 males, 896 females and 1 transgender; 895 unmarried; 768 unemployed; 1910 outpatients. The mean age was 44.48±11.28 years and the mean education years was 13.61±3.00 years. The psychotherapies (used alone) involved CBT, MT, CT, Supportive psychotherapy (SP), Twelve-step facilitation (TSF), MET, CBM, Affect regulation training (ART), Exposure therapy (ET), Relapse prevention (RP), Mindfulness-oriented therapy (MOT), Relaxation therapy (RT), Brief counseling (BC), and Visual Short-Time Neurofeedback (VSTN), while psychotherapies (combination) involved naltrexone + CBT, naltrexone + MET, naltrexone + BC, fluoxetine + CBT, naltrexone + ET, sertraline + CBT, baclofen + CBT, MET + CT, MT + RP, TSF + CT, CBT + ET, and CBT + SP (details in Figure S5 and Table S5). The common control treatments are Treatment as usual (TAU), placebo (PLC), TAU + PLC, etc. The brief description of the psychotherapies in this study was listed in S3.
Risk of Bias Within Studies
Briefly, as the Supplementary File presents, 14.71% of the included trials were considered low risk, 66.67% were considered unclear risk, and 20.59% were considered high risk (Figure S6A). The unclear ROBs were mainly concentrated in the randomization, allocation concealment, and blinding to therapists and patients, while the high ROBs existed from the implementation to the reporting stage (Figure S6B, details listed in Table S6).
Pairwise Meta-Analysis
Table S7 presents the results of the pairwise meta-analysis and heterogeneity estimates. CBT (MD 30.72, 95% CI 23.63 to 37.81, GRADE high certainty) and MT (8.83, 95% CI 0.30 to 11.36, high certainty) were more efficacious than TAU for PDA but were not pooled because of the single trials. TAU+SP was more efficacious than TAU alone for the change in DDD (pooled SMD −0.57, 95% CI −0.91 to −0.24, I2=0%, high certainty). No difference was found between other direct comparisons.
Network Geometry and Synthesis of Results
The ranking probabilities and surface under the cumulative ranking curve (SUCRA) values are presented in Figure S8A–C and Table S8A–C for the three following outcomes.
The results of PDA were available for 22 arms (780 participants), including all 12 active interventions and TAU (Figure 2). With TAU as reference, the top nine interventions most likely to be accepted were as follows: MET+CT (47.2%), CT (44.8%), CBT (36.6%), RT (25.9%), TSF+CT (24.8%), TAU+CBT (39.4%), MT+RP (43.6%), MT (40.3%), and SP (34%), followed by TAU (50.7%). Among the SUCRA mean rankings, MET, MT, CT, TSF+CT, SP, RT, TAU+CBT, and MT+RP were ranked 1.9, 1.9, 3.0, 4.0, 4.6, 6.8, 7.0, and 7.4, respectively. Among these interventions, MET (MD 35.44, 95% CI 11.78 to 59.09, GRADE high certainty), CT (28.89, 95% CI 13.42 to 44.36, moderate certainty), TSF+CT (25.64, 95% CI 0.44 to 50.83, low certainty), MET+CT (35.24, 95% CI 15.16 to 55.32, very low certainty) and SP (21.79, 95% CI 4.14 to 39.44, very low certainty) were significantly different compared with TAU. Further details were shown in Figure 3 and Table 1–4, and Figure S9Aa–c.
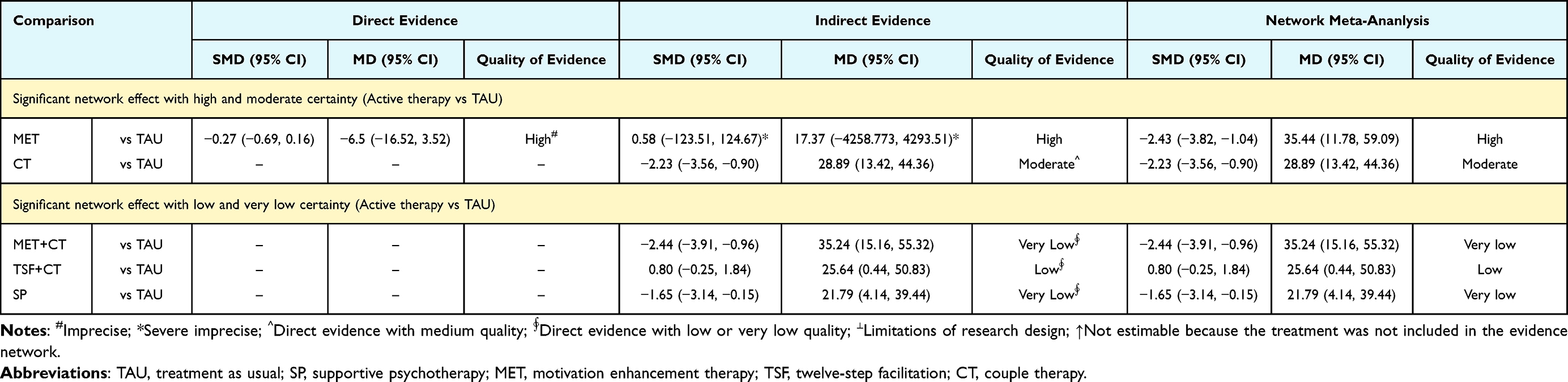 |
Table 1 Estimates of Effect and Quality Ratings for Comparison of Psychotherapies for PDA (Significant Network Effect Between Active Therapy and TAU) |
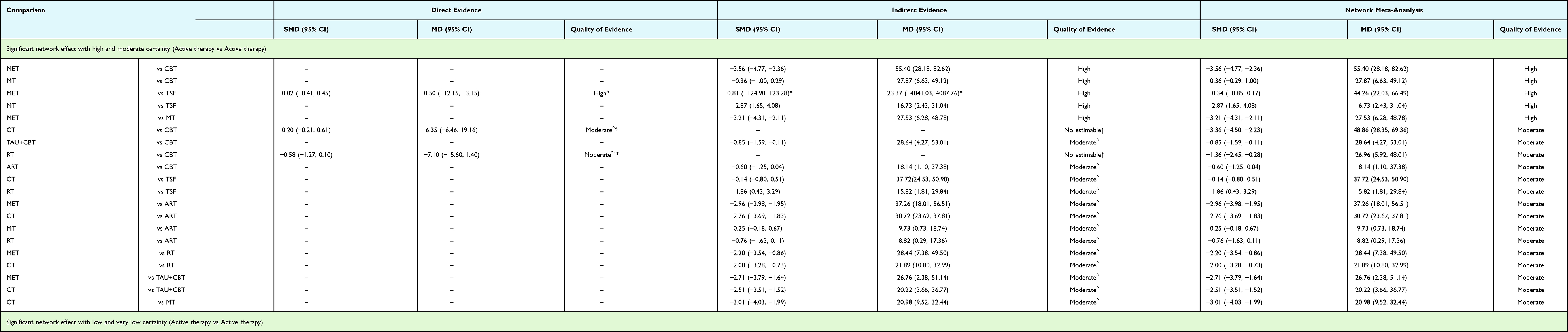 |
Table 2 Estimates of Effect and Quality Ratings for Comparison of Psychotherapies for PDA (Significant Network Effect Between Active Therapy and Active Therapy) |
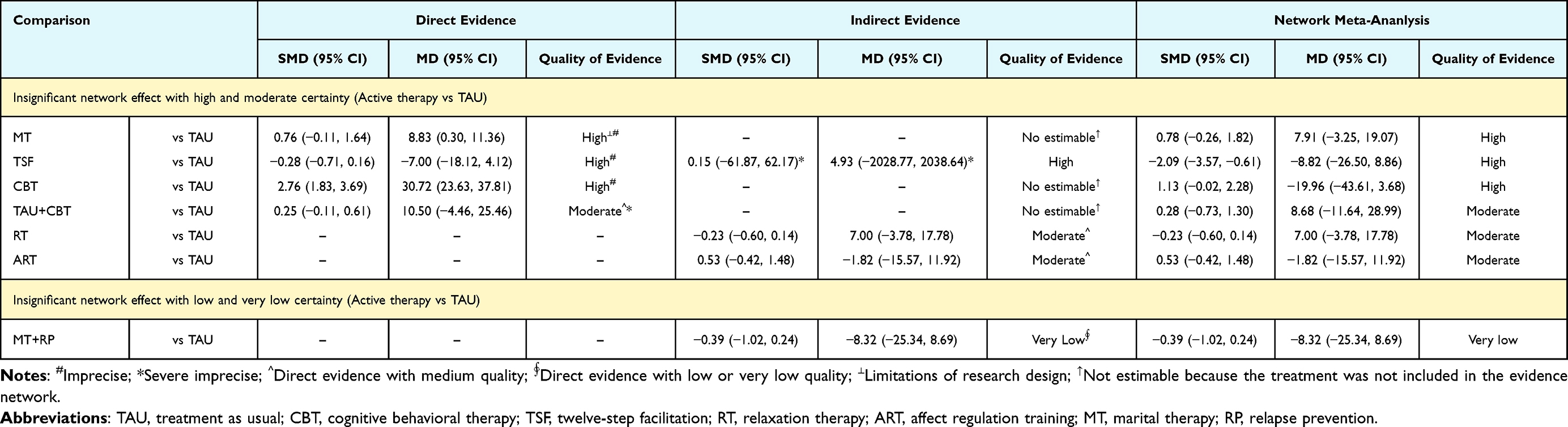 |
Table 3 Estimates of Effect and Quality Ratings for Comparison of Psychotherapies for PDA (Insignificant Network Effect Between Active Therapy and TAU) |
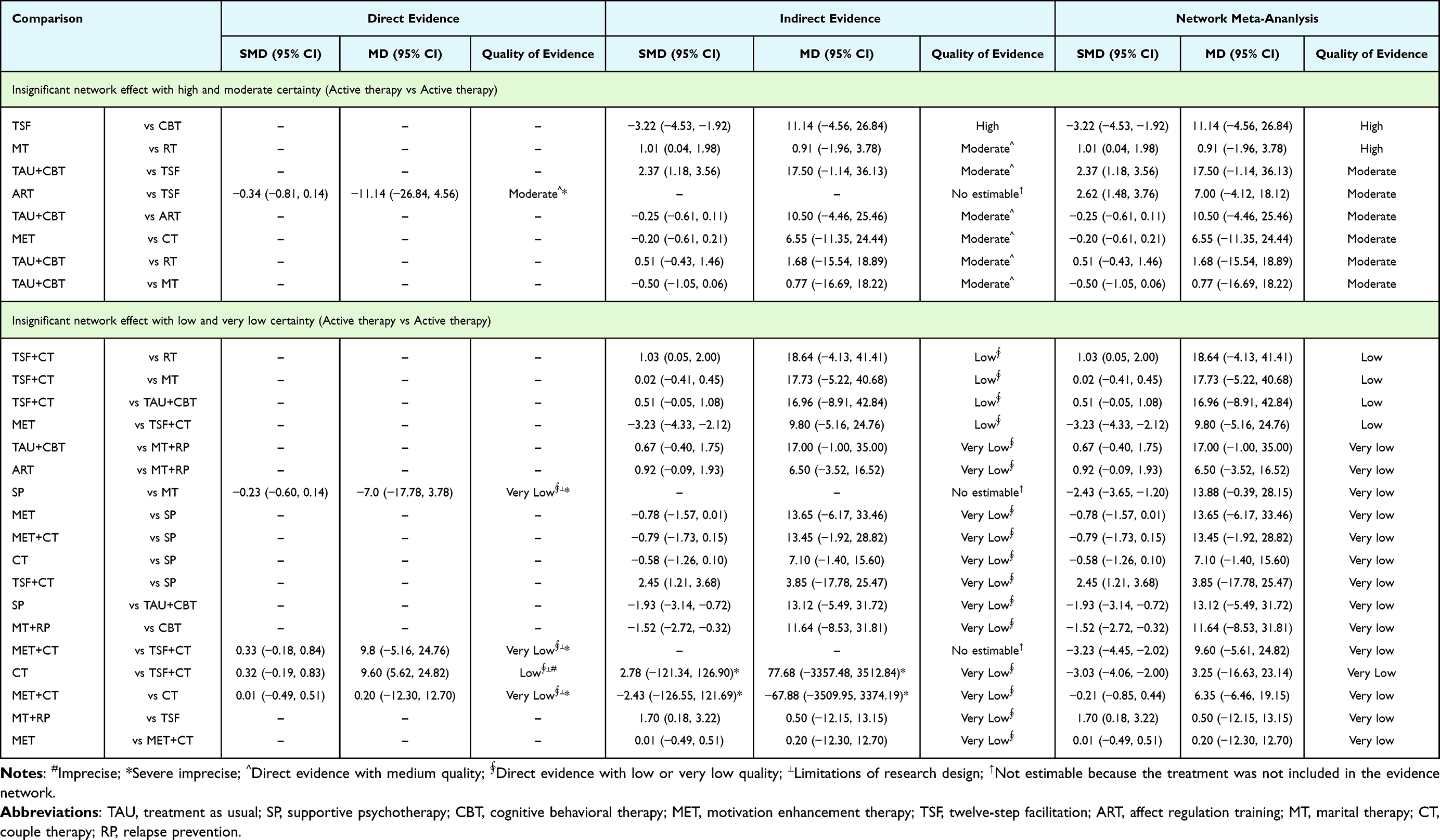 |
Table 4 Estimates of Effect and Quality Ratings for Comparison of Psychotherapies for PDA (Insignificant Network Effect Between Active Therapy and Active Therapy) |
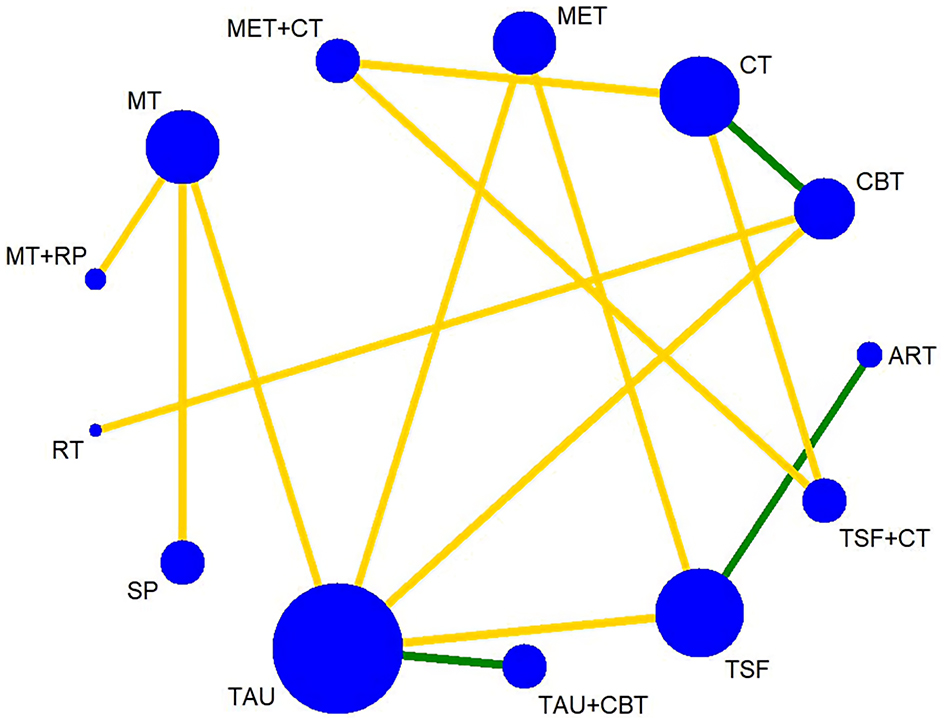 |
Figure 2 Network plot of PDA. Notes: The node size is proportional to the number of participants randomised to each treatment, while the line width is proportional to the number of RCTs comparing each pair of treatments. |
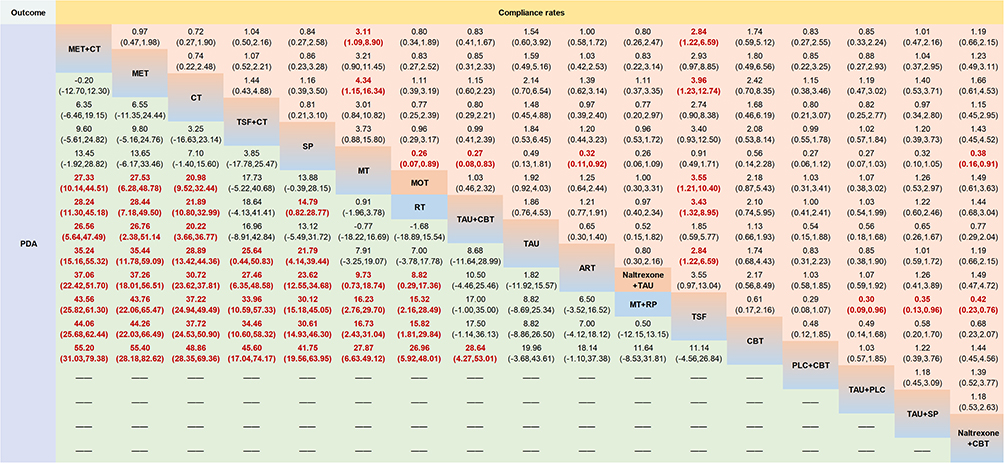 |
Figure 3 Network meta-ananlysis of PDA. Note: Effect sizes of PDA and compliance rates are represented by summary MDs and RRs respectively, and the 95% CIs of them. For the lower triangle (PDA), values greater than 0 favor the interventions in the corresponding column, whereas values lower than 0 favor the interventions in the corresponding row. For the upper triangle (compliance rates), collected from the included studies with clear information on treatment compliance (a total of 12 articles), values greater than 1 favor the interventions in the corresponding column, whereas values lower than 1 favor the interventions in the corresponding row. |
In terms of changes in DDD, available for 28 treatment arms (1121 participants), all 11 active and 3 control interventions (naltrexone+TAU, TAU, TAU+PLC) were included (Figure S10A). The top four most likely to be accepted were naltrexone+MET (55.4%), naltrexone+CBT (37.8%), PLC+MET (16.5%), and PLC+CBT (18.7%). Among the SUCRA rankings, naltrexone+MET, sertraline+CBT, and naltrexone+CBT were ranked 2.6, 5.1, and 5.2, respectively. The results of the NMA indicate that no treatment showed a significantly better effect than TAU or TAU plus PLC on the change in DDD (Figure S9Ba–c), and (d)). All of the significant evidence from active intervention comparisons were with low certainty (Figure S11B and Table S12A).
For changes in craving, available for 12 treatment arms (259 participants), all 4 active interventions and 2 controls (TAU and TAU+PLC)) were included (Figure S10B). TAU+PLC (67.5%) had the highest probability of being best accepted, followed by TAU+SP (44%) and TAU+CBT (40.6%). Among the SUCRA rankings, TAU+PLC, TAU+SP, TAU+CBT, CBT, and TAU+VSTN were ranked 1.4, 2.4, 2.8, 4.0, and 5.1, respectively, and TAU was the lowest (5.3). No treatment showed a significantly better effect than TAU or TAU plus PLC (Figure S11C and Table S12B). Other details were shown in Figure S9Ca–d).
In addition, the compliance of the active interventions also did not show better evidence than TAU in Figure 3 (12 articles included).
Inconsistency
No statistically significant inconsistency were provided by fitting the node-splitting model (P= 0.053 to 0.990) or the global inconsistency model (PDA: P = 0.1688, change of DDD: P = 0.6312, and change of craving: P = 0.0532). Details were listed in S13.
Small-Study Effects
For the publication bias of these three outcome indicators, due to the big number of types of psychological intervention comparisons but the small number of studies in each type, although it can be seen from S14 that both positive and negative reports occurred in the comparison network of PDA, it is still difficult to identify whether there is a small study effect in the comparative study of each pair of psychotherapies (Other details were in S14).
Discussion
Overview of Result
According to this systematic review and NMA, in terms of improving PDA, our findings provided further clarification about the abstinence efficacy of MET and CT protocols, which was significantly better than the efficacy of TAU with relatively higher evidence quality. Among the active interventions for PDA with high or moderate certainty comparisons, the four psychotherapies (MET, CT, MT, and RT) showed better effects than ART, CBT, and TSF, while MET and CT showed better effects than MT and RT, which suggests MET and CT as prior considerations in abstinence improvement. Additionally, TAU+SP was more efficacious than TAU for changing DDD in the high-quality direct comparison, although they had no other connection in the evidence network.
Comparison with Prior Studies
In the past, few systematic reviews have quantitatively presented the abstinence effect of MET on patients with AUD. Previous studies have shown that MET has an insignificant pooled ES in terms of alcohol consumption;13 however, regarding current network analysis, the potential for abstinence improvement of MET was revealed in this study. The latest RCT suggested that MI can reduce alcohol use by enhancing motivation and self-efficacy;32 additionally, helping patients resolve social stress is also one of the possible mechanisms for improving abstinence ability.33
The results of some previous meta-analyses are similar to the network of CT in improving PDA in this study. The use of CT in the acute posttreatment of AD was strongly recommended in some guidelines.34 There is an interaction causing a vicious circle between alcoholism and family relationships.35 Therefore, detecting dysfunctional interaction patterns in family relationships contributes to obtaining alternative relationships. As a previous meta-analysis generally showed, CT is superior to more typical individual-based treatment for married or cohabiting to deal with AD.14
This study provided direct evidence of PDA evaluation for CBT rather than constituting network evidence. For improving PDA, it can be seen from the ranking probability that CBT is better than TAU, but there is no significant difference in the network; this contradiction may be attributable to the non-transferability. The results in this study are similar to those in some recent related systematic reviews,10 which confirmed that CBT did not seem statistically better than other specific evidence-based therapies, revealing a moderate effect declining with time compared with TAU.10,11,36
Moreover, network comparison also provides moderate-quality evidence for the superiority of ART to CBT, but the comparison lacks direct evidence. Highlighting the role of emotion as an important treatment goal of AD,37 one study (study Walitzer 2015) in the loop showed that both ART and TSF significantly reduced alcohol-related consequences and anger-related thoughts as well as increased abstinence and self-confidence, thus their application was urged in AD.38–40
This study also found that TAU+SP showed a significant effect on the change in DDD with high certainty of direct evidence. SP is rarely used independently, and its components are often used as a part of community conventional treatment or other psychological therapies.41 It can be operated face-to-face and can also provide remote support (like studies Agyapong 2012, Lucht 2014, O’Reilly 2019). Additionally, SP previously showed an effect on abstinence improvement in AUD,42 so it also needs to be treated as a kind of active and effective psychological intervention.
Strengths and Limitations of This Review
In terms of the strengths of this review, first, to ensure the designs of evidence-based evidence sources are rigorous and similar enough, this study only included relevant RCTs, focused on the dependent component in AUD, and excluded transient heavy drinking, and hazardous drinking implying risk prediction. Second, this study conducted GRADE evaluations for direct, indirect, and network meta-analyses, which have not been done previously.
Regarding the limitations, the completion and conviction of the conclusion may be weakened by the following aspects. First, some therapies included had few clinical studies and insufficient sample sizes for pooling or looping analyses.43 Second, the small number of included studies and the lack of severity stratification of results in some of the studies did not facilitate the exploration of the association between severity and outcomes. Third, there was a lack of rigorous reports on randomization methods, allocation concealment, and control of implementation bias. Fourth, due to the influence of complex clinical factors and the limitations of the report content, the parameters of psychological intervention are indeed insufficient to support the impact on the outcomes by the duration, which needs to be further explored in clinical practice in the future. Furthermore, this article did not include multiple follow-up time points for analyses due to the limited outcome designs of the eligible studies.
Implications for Clinical Practice and Further Research
The advantages of MET and CT were indicated for abstinence in AUDs in this meta-analysis. They are two alternative psychotherapies on the primary care list of priorities to help persist in abstinence. However, at present, a comparison of rehabilitation strategies through MET for patients in different periods of AUDs remains to be explored. This study also shows some psychotherapies with significant efficacy but low or very low quality, requiring further research and investment. The inevitability that two or more psychotherapies are combined better than a certain therapy alone also needs to be further rigorously proven, and the stability of their long-term effects on AUD remains to be determined further.
Conclusion
This NMA provides evidence of psychotherapies for AUDs drinking control improvement and suggests that MET and CT may be the two preferred psychological options for primary care. Additionally, the preferred interventions for improving PDA and DDD are different. There is still a need for higher-quality RCTs to strengthen the evidence network and confirm the clinical benefits of other psychotherapies.
Abbreviations
ACQ, Alcohol Craving Questionnaire; ART, Affect regulation training; AUD, Alcohol use disorder; BC, Brief counseling; CBM, Cognitive bias modification; CBT, Cognitive behavioral therapy; CT, Couple therapy; DAQ, Desire for Alcohol Questionnaire; DDD, Drinks per drinking day; DMA, Direct pairwise meta-analysis; DSM-V, Diagnostic and Statistical Manual of Mental Disorders, the 5th version; ES, Effect size; ET, Exposure therapy; GRADE, Grade of Recommendations Assessment, Development and Evaluation; ITT, Intention-to-treat; MOT, Mindfulness-oriented therapy; NMA, Network meta-analysis; OCDS, Obsessive-Compulsive Drinking Scale; PACS, Penn Alcohol Craving Scale; PDA, Percentage of days abstinent; PLC, Placebo; RCT, Randomized controlled trial; ROB, Risk of bias; RP, Relapse prevention; RR, Risk ratio; RT, Relaxation therapy; SMD, Standardized mean difference; SP, Supportive psychotherapy; SUCRA, Surface under the cumulative ranking curve; TAU, Treatment as usual; TLFB, Timeline Followback Interview; TSF, Twelve-step facilitation; VSTN, Visual Short-Time Neurofeedback; WMD, Weighted mean difference.
Funding
This work was funded by:1. National Natural Science Foundation of China (Grant No. 82174527). (Liming Lu) URL: https://www.nsfc.gov.cn/2. The special project of “Lingnan modernization of traditional Chinese medicine” in 2019 Guangdong Provincial R & D Program (NO:2020B1111100008). (Nenggui Xu) URL: https://www.gdzwfw.gov.cn/portal/v2/guide/11440000006939801C2442003003007103. The Chinese Medicine Innovation Team Project of the State Administration of Traditional Chinese Medicine. (Nenggui Xu) URL: http://rjs.satcm.gov.cn/zhengcewenjian/2021-10-26/23006.html4. China Postdoctoral Science Foundation (No.2021M700906). (Jie Zhan) URL: https://jj.chinapostdoctor.org.cn/website/zhengshuchayan.html.The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
Peiming Zhang and Jie Zhan are co-first authors. Professor Liming Lu reports grants from National Natural Science Foundation of China, grants from The special project of “Lingnan modernization of traditional Chinese medicine” in 2019 Guangdong Provincial R & D Program, grants from The Chinese Medicine Innovation Team Project of the State Administration of Traditional Chinese Medicine, during the conduct of the study. The authors declare that they have no other competing interests.
References
1. GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1223–1249. doi:10.1016/S0140-6736(20)30752-2
2. Rumgay H, Shield K, Charvat H, et al. Global burden of cancer in 2020 attributable to alcohol consumption: a population-based study. Lancet Oncol. 2021;22(8):1071–1080. doi:10.1016/S1470-2045(21)00279-5
3. Castillo-Carniglia A, Keyes KM, Hasin DS, Cerdá M. Psychiatric comorbidities in alcohol use disorder. Lancet Psychiatry. 2019;6(12):1068–1080. doi:10.1016/S2215-0366(19)30222-6
4. World Health Organization. Global status report on alcohol and health 2018. World Health Organization; 2018. Available from: https://www.who.int/publications/i/item/9789241565639.
5. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
6. World Health Organization. Clinical Guidelines for Withdrawal Management and Treatment of Drug Dependence in Closed Settings. Geneva: World Health Organization; 2009.
7. Femino J, Freedman K, Goldsmith RJ, et al. The ASAM clinical practice guideline on alcohol withdrawal management: erratum. J Addict Med. 2020;14(5):e280. doi:10.1097/ADM.0000000000000731
8. American Psychiatric Association. Practice Guideline for the Treatment of Patients with Substance Use Disorders.
9. Knox J, Hasin DS, Larson FRR, Kranzler HR. Prevention, screening, and treatment for heavy drinking and alcohol use disorder. Lancet Psychiatry. 2019;6(12):1054–1067. doi:10.1016/S2215-0366(19)30213-5
10. Ray LA, Meredith LR, Kiluk BD, Walthers J, Carroll KM, Magill M. Combined pharmacotherapy and cognitive behavioral therapy for adults with alcohol or substance use disorders: a systematic review and meta-analysis. JAMA Netw Open. 2020;3(6):e208279. doi:10.1001/jamanetworkopen.2020.8279
11. Magill M, Ray L, Kiluk B, et al. A meta-analysis of cognitive-behavioral therapy for alcohol or other drug use disorders: treatment efficacy by contrast condition. J Consult Clin Psychol. 2019;87(12):1093–1105. doi:10.1037/ccp0000447
12. Kiluk BD, Ray LA, Walthers J, Bernstein M, Tonigan JS, Magill M. Technology-delivered cognitive-behavioral interventions for alcohol use: a meta-analysis. Alcohol Clin Exp Res. 2019;43(11):2285–2295. doi:10.1111/acer.14189
13. Riper H, Andersson G, Hunter SB, de Wit J, Berking M, Cuijpers P. Treatment of comorbid alcohol use disorders and depression with cognitive-behavioural therapy and motivational interviewing: a meta-analysis. Addiction. 2014;109(3):394–406. doi:10.1111/add.12441
14. Powers MB, Vedel E, Emmelkamp PM. Behavioral couples therapy (BCT) for alcohol and drug use disorders: a meta-analysis. Clin Psychol Rev. 2008;28(6):952–962. doi:10.1016/j.cpr.2008.02.002
15. Cavicchioli M, Movalli M, Maffei C. The clinical efficacy of mindfulness-based treatments for alcohol and drugs use disorders: a meta-analytic review of randomized and nonrandomized controlled trials. Eur Addict Res. 2018;24(3):137–162. doi:10.1159/000490762
16. Block I, Loeber S. Evidenzbasierte Psychotherapie bei Abhängigkeitserkrankungen [Evidence-based psychotherapy of addictive disorders]. Nervenarzt. 2018;89(3):283–289. doi:10.1007/s00115-018-0483-7
17. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;10:372.
18. Dilling H, Mombour W, Schmidt MH, Schulte-Markwort E. Internationale Klassifikation psychischer Störungen: ICD-10. In: Kapitel V (F) Klinisch-Diagnostische Leitlinien. [The ICD-10 Classification of Mental and Behavioural Disorders].
19. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
20. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
21. Lecrubier Y, Sheehan D, Weiller E, et al. The Mini International Neuropsychiatric Interview (MINI). A short diagnostic structured interview: reliability and validity according to the CIDI. Eur Psychiatry. 1997;12(5):224–231. doi:10.1016/s0924-9338(97)83296-8
22. Selzer ML. The Michigan alcoholism screening test: the quest for a new diagnostic instrument. Am J Psychiatry. 1971;127(12):1653–1658. doi:10.1176/ajp.127.12.1653
23. Saunders JB, Aasland OG, Babor TF, de la Fuente JR, Grant M. Development of the Alcohol Use Disorders Identification Test (AUDIT): who collaborative project on early detection of persons with harmful alcohol consumption–II. Addiction. 1993;88(6):791–804. doi:10.1111/j.1360-0443.1993.tb02093.x
24. Norcross JC. An eclectic definition of psychotherapy. In: Zeig JK, Munion WM, editors. What is Psychotherapy? Contemporary Perspectives. Jossey-Bass; 1990:218–220.
25. Merrill JE, Fan P, Wray TB, Miranda R. Assessment of alcohol use and consequences: comparison of data collected via timeline followback interview and daily reports. J Stud Alcohol Drugs. 2020;81(2):212–219. doi:10.15288/jsad.2020.81.212
26. Singleton EG, Henningfield JE, Tiffany S. Alcohol craving questionnaire: ACQ-Now: background and administration manual. NIDA Addiction Research Centre; 1994.
27. Higgins JP, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. doi:10.1136/bmj.d5928
28. Cohen J. Statistical power analysis for the behavioral sciences–second edition. Hillsdale New Jersey: 12 Lawrence Erlbaum Associates Inc; 1988:77–83.
29. Carlin BP, Hong H, Shamliyan TA, Sainfort F, Kane RL. Case Study Comparing Bayesian and Frequentist Approaches for Multiple Treatment Comparisons. Rockville (MD): Agency for Healthcare Research and Quality (US); 2013.
30. Dias S, Welton NJ, Caldwell DM, Ades AE. Checking consistency in mixed treatment comparison meta-analysis. Stat Med. 2010;29(7–8):932–944. doi:10.1002/sim.3767
31. Puhan MA, Schünemann HJ, Murad MH, et al. A GRADE Working Group approach for rating the quality of treatment effect estimates from network meta-analysis. BMJ. 2015;349:g5630. doi:10.1136/bmj.g5630
32. Feldstein Ewing S, Bryan AD, Dash GF, Lovejoy TI, Borsari B, Schmiege SJ. Randomized controlled trial of motivational interviewing for alcohol and cannabis use within a predominantly Hispanic adolescent sample. Exp Clin Psychopharmacol. 2021. doi:10.1037/pha0000445.
33. Santa Ana EJ, LaRowe SD, Gebregziabher M, et al. Randomized controlled trial of group motivational interviewing for veterans with substance use disorders. Drug Alcohol Depend. 2021;223:108716. doi:10.1016/j.drugalcdep.2021.108716
34. (DG-SUCHT). S3 guideline “Screening, diagnosis and treatment of alcohol-related disorders”. German Society for Psychiatry and Psychotherapy, Psychosomatics and Neurology (DGPPN) German Society for Addiction Research and Addiction Therapy e.V. AWMF; 2020. Available from: https://www.awmf.org/uploads/tx_szleitlinien/076-001l_S3-Screening-Diagnose-Behandlung-alkoholbezogene-Stoerungen_2021-02.pdf.
35. Loeber S, Mann K. Entwicklung einer evidenzbasierten Psychotherapie bei Alkoholismus. Eine Ubersicht [The development of evidence-based psychotherapy for use in alcoholism. A review]. Nervenarzt. 2006;77(5):558–566. doi:10.1007/s00115-005-2000-z
36. Magill M, Ray LA. Cognitive-behavioral treatment with adult alcohol and illicit drug users: a meta-analysis of randomized controlled trials. J Stud Alcohol Drugs. 2009;70(4):516–527. doi:10.15288/jsad.2009.70.516
37. Chermack ST, Grogan-Kaylor A, Perron BE, Murray RL, De Chavez P, Walton MA. Violence among men and women in substance use disorder treatment: a multi-level event-based analysis. Drug Alcohol Depend. 2010;112(3):194–200. doi:10.1016/j.drugalcdep.2010.06.005
38. Chermack ST, Murray RL, Walton MA, Booth BA, Wryobeck J, Blow FC. Partner aggression among men and women in substance use disorder treatment: correlates of psychological and physical aggression and injury. Drug Alcohol Depend. 2008;98(1–2):35–44. doi:10.1016/j.drugalcdep.2008.04.010
39. Rothman EF, Cheng DM, Pedley A, et al. Interpersonal violence exposure and alcohol treatment utilization among medical inpatients with alcohol dependence. J Subst Abuse Treat. 2008;34(4):464–470. doi:10.1016/j.jsat.2007.07.006
40. Easton CJ, Mandel DL, Hunkele KA, Nich C, Rounsaville BJ, Carroll KM. A cognitive behavioral therapy for alcohol-dependent domestic violence offenders: an integrated substance abuse-domestic violence treatment approach (SADV). Am J Addict. 2007;16(1):24–31. doi:10.1080/10550490601077809
41. Sannibale C, Teesson M, Creamer M, et al. Randomized controlled trial of cognitive behaviour therapy for comorbid post-traumatic stress disorder and alcohol use disorders. Addiction. 2013;108(8):1397–1410. doi:10.1111/add.12167
42. O’Malley SS, Jaffe AJ, Chang G, Schottenfeld RS, Meyer RE, Rounsaville B. Naltrexone and coping skills therapy for alcohol dependence. A controlled study. Arch Gen Psychiatry. 1992;49(11):881–887. doi:10.1001/archpsyc.1992.01820110045007
43. Mellentin AI, Skøt L, Nielsen B, et al. Cue exposure therapy for the treatment of alcohol use disorders: a meta-analytic review. Clin Psychol Rev. 2017;57:195–207. doi:10.1016/j.cpr.2017.07.006
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Exercise Interventions on Health-Related Quality of Life in Patients with Fibromyalgia Syndrome: A Systematic Review and Network Meta-Analysis
Zhang KD, Wang LY, Zhang ZH, Zhang DX, Lin XW, Meng T, Qi F
Journal of Pain Research 2022, 15:3639-3656
Published Date: 22 November 2022
Different Intensities of Evening Exercise on Sleep in Healthy Adults: A Systematic Review and Network Meta-Analysis
Yue T, Liu X, Gao Q, Wang Y
Nature and Science of Sleep 2022, 14:2157-2177
Published Date: 14 December 2022
Systematic Review of Safety of RTS,S with AS01 and AS02 Adjuvant Systems Using Data from Randomized Controlled Trials in Infants, Children, and Adults
Yihunie W, Kebede B, Tegegne BA, Getachew M, Abebe D, Aschale Y, Belew H, Bahiru B
Clinical Pharmacology: Advances and Applications 2023, 15:21-32
Published Date: 14 March 2023
Oxytocin and Women Postpartum Depression: A Systematic Review of Randomized Controlled Trials

Zhu J, Jin J, Tang J
Neuropsychiatric Disease and Treatment 2023, 19:939-947
Published Date: 18 April 2023
Efficacy of Acupuncture-Related Therapy for Migraine: A Systematic Review and Network Meta-Analysis
Liu Y, Wang Y, Mi C, Wang Z, Han Y, Qi X, Ding X
Journal of Pain Research 2024, 17:1107-1132
Published Date: 15 March 2024