Back to Journals » International Journal of Women's Health » Volume 17
Efficacy and Safety Comparisons of Lingshu Granule versus Decoction in Polycystic Ovary Syndrome Patients with Insulin Resistance: A Multicenter Randomized Controlled Dose-Finding Trial Protocol
Authors Feng Y, Wen X ![]() , Li X, Luo Y
, Li X, Luo Y
Received 21 July 2025
Accepted for publication 30 October 2025
Published 7 November 2025 Volume 2025:17 Pages 4301—4309
DOI https://doi.org/10.2147/IJWH.S555202
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Yueying Feng,1 Xiaoyu Wen,1 Xiaobin Li,1– 3 Yunyun Luo1– 3
1The Second Clinical College of Guangzhou University of Chinese Medicine, Guangzhou, 510000, People’s Republic of China; 2Department of Gynecology, The Second Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou, 510000, People’s Republic of China; 3Department of Gynecology, Guangdong Provincial Hospital of Chinese Medicine, Guangzhou, 510000, People’s Republic of China
Correspondence: Yunyun Luo, Department of Gynecology, Guangdong Provincial Hospital of Chinese Medicine, 1st Fl. 261 Datong Road, Yuexiu District, Guangzhou, 510000, People’s Republic of China, Tel +8615920124853, Email [email protected]
Introduction: Polycystic ovary syndrome (PCOS) is a common endocrine disorder in women of reproductive age. Although multiple treatment strategies have been proposed, many patients still experience suboptimal outcomes. Our research team has developed the Lingshu formula, which is grounded in traditional Chinese medicine theory, focusing on kidney deficiency and phlegm dampness. Clinical and animal studies have demonstrated its efficacy in improving insulin resistance, regulating hormonal and lipid metabolism, and reducing obesity, which was non-inferior to metformin. However, Lingshu is traditionally prepared in formula decoction, with a complicated and time-consuming process. The granule preparations have offered the advantages of stable drug quality, convenient storage and administration, and high patient compliance. However, the efficacy, safety, and optimal dosage of the Lingshu formula granules compared to its traditional decoction in the treatment of PCOS patients with insulin resistance still require further investigation. Therefore, this study aims to determine whether the Lingshu formula granules are superior to the traditional decoction and to establish their optimal dosage.
Methods: We will conduct a multicenter, randomized, controlled clinical trial targeted to enroll 200 patients. Eligible participants will be randomly assigned, in a 1:1:1:1 ratio, to group A (low-dose Lingshu granules, − 20% from standard dose), group B (medium-dose Lingshu granules, standard dose), group C (high-dose Lingshu granules, +20% from standard dose), or group D (Lingshu decoction). Treatment will last 90 days. The primary outcome is the insulin resistance index, and secondary outcomes include body mass index, waist-to-hip ratio, and laboratory tests, which will be recorded and compared across these four groups. In addition, variations in symptoms related to the Chinese traditional medicine and adverse events will also be documented and compared.
Discussion: The findings are expected to provide a scientific basis for the clinical application of the Lingshu formula granules in PCOS patients with insulin resistance and promote widespread use of traditional Chinese medicine.
Keywords: Lingshu formula, granule, decoction, polycystic ovary syndrome, insulin resistance
Introduction
Polycystic ovary syndrome (PCOS) is an endocrine disorder characterized by irregular menstrual periods, excessive androgen levels, and polycystic ovaries.1 Clinically, affected women often present with obesity, acne, hirsutism, and infertility.2 The global prevalence of PCOS is estimated to be as high as 13%, with particularly high incidence in the Asia–Pacific region.3,4 Approximately 35–80%of PCOS patients have insulin resistance (IR) or hyperinsulinemia.5 Without appropriate management, patients with PCOS and IR can develop various short- and long-term complications—such as dyslipidemia, type 2 diabetes, and cardiovascular disease—that negatively affect psychological well-being and quality of life.6
The exact pathogenesis of PCOS remains unclear, although genetic and lifestyle factors are thought to contribute.7 Current treatments focus on symptom management through lifestyle modification, medications, and hormonal therapy.8 In patients with PCOS and IR, pharmacologic interventions that improve insulin sensitivity are a mainstay of care.7 The most commonly used agent is metformin. Randomized clinical trials have demonstrated its benefits in regulating insulin sensitivity, menstrual cycles, and metabolic parameters; however, its impact on fertility and androgenic symptoms is uncertain.9 Thiazolidinediones constitute another class of insulin-sensitizing agents that enhance insulin action by activating peroxisome proliferator-activated receptor gamma (PPAR-γ) in adipose tissue, muscle, and liver. These drugs can improve insulin sensitivity, reduce androgen levels, restore ovulatory function, and optimize the lipid profile.10 However, previous studies have shown that thiazolidinediones might cause weight gain and increase the risk of cardiovascular events (hazard ratio 2.10, 95% confidence interval 1.35–3.27, p = 0.0010).11–13 Therefore, new treatment strategies with improved efficacy and safety profiles are still needed for patients with PCOS and IR.
In traditional Chinese medicine (TCM), PCOS is viewed as a syndrome of combined deficiency and excess involving multiple organ systems, with kidney deficiency as the root cause and phlegm-dampness and blood stasis as its manifestations.14 Several Chinese herbal formulas have been reported for PCOS treatment, yielding variable outcomes.15,16 Over the past few decades, our research team has developed a novel herbal combination—the Lingshu formula—primarily comprising six ingredients: Epimedium, Curculigo, Atractylodes macrocephala, Angelica sinensis, Pinellia, and Arisaema. Preliminary studies indicate that the Lingshu formula can modulate lipid levels, normalize sex hormones, improve insulin resistance, and reduce body weight.17–21,
The initial preparation of the Lingshu formula involves a decoction, which offers high bioavailability and customizable formulations. However, it is time-consuming to prepare and has an unpleasant taste. The decoction formula also has a short shelf life, making it inconvenient for storage and transportation, which in turn limits its clinical application. Therefore, TCM formula granules of Lingshu have been developed in recent years. TCM formula granules are powdery in texture and are produced and mixed from each component of traditional TCM according to traditional methods, through processes such as extraction and concentration.22 TCM formula granules preserve the strengths and characteristics of traditional Chinese medicine, including treatment based on syndrome differentiation and flexible modification of prescriptions according to symptoms, offering advantages such as convenience in administration, portability, and long shelf life, and simultaneously overcoming the drawbacks associated with traditional decoctions, such as time-consuming preparation and inconvenience in storage and transport. The formula granules can better reflect the modernization and standardization of TCM medication use, leading to improved patient compliance.23–25 Pharmacokinetic studies have shown that TCM formula granules could exhibit improved solubility and bioavailability, allowing them to rapidly enter the systemic circulation and exert therapeutic effects.26 Therefore, we developed Lingshu formula granules from a mixture of each herb granule contained in the Lingshu formula decoctions. However, as a new formula applied in clinical TCM practice, whether Lingshu granules are therapeutically equivalent to traditional decoction remains controversial. Furthermore, some studies have reported that the efficacy of traditional decoctions was only approximately 69% to 84% of that of formula granules.27 It is therefore recommended that the dosage be appropriately reduced when TCM formula granules are administered.
The efficacy comparisons between different Lingshu formulas and the optimal dosage in the treatment of PCOS patients are unknown. Therefore, more studies on the clinical efficacy and safety of the Lingshu granule formula are required before it can be introduced to a wide range of patients with PCOS and IR. We plan to conduct a randomized controlled clinical trial comparing different doses of Lingshu granules with decoction in patients with PCOS and IR, aiming to determine the optimal dose and formula of Lingshu for these patients. This is the first time the granular and decoction forms have been directly compared with each other. Successful completion of this trial may advance the widespread acceptance of TCM.
Materials and Methods
Study Design
This randomized controlled clinical trial plans to use different doses of Lingshu granules and decoction to treat patients with PCOS-IR (Figure 1). We will compare the clinical efficacy and safety of different formulas to determine the optimal therapeutic dose of Lingshu granules and evaluate different Lingshu formulas for the treatment of PCOS-IR patients.
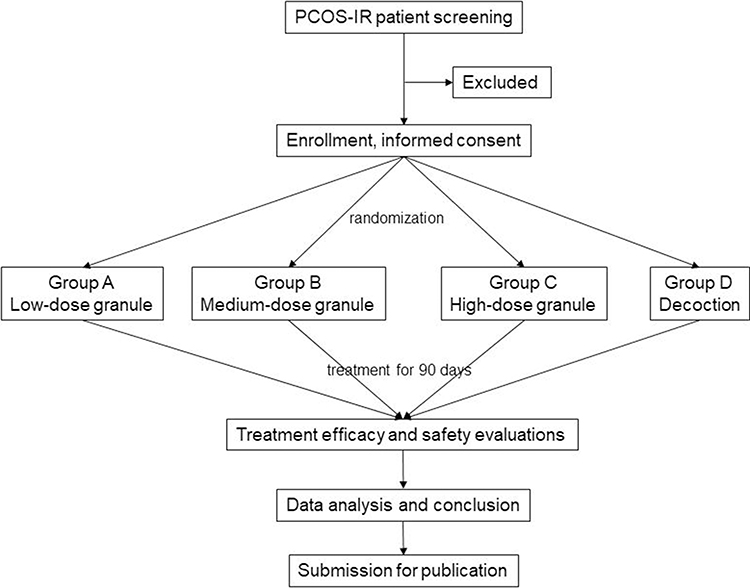 |
Figure 1 Study flow chart. IR, insulin resistance; PCOS, polycystic ovary syndrome. |
Participant Selection
Patients with PCOS and IR who visited the gynecology clinics of Guangdong Provincial Hospital of Traditional Chinese Medicine Dade Road Hospital, Guangdong Provincial Hospital of Traditional Chinese Medicine Ersha Island Hospital, Guangdong Provincial Hospital of Traditional Chinese Medicine Fangcun Hospital, and Guangdong Provincial Hospital of Traditional Chinese Medicine University City Hospital in China will be screened for eligibility.
PCOS Diagnostic Criteria
PCOS diagnosis is based on the Rotterdam diagnostic criteria recommended by the European Society of Human Reproduction and Embryology (ESHRE) and the American Society for Reproductive Medicine (ASRM) in 2003. POCS is diagnosed based on the presence of any two of the following items.28
1) Abnormal menstruation, such as ovulation or anovulation;
2) Clinical and/or biochemical measurements suggesting hyperandrogenism, and exclude hyperprolactinemia and other endocrine diseases that can produce hyperandrogenism, such as congenital adrenal hyperplasia, ovarian or adrenal tumors, and Cushing’s syndrome;
3) Polycystic ovaries: ultrasound shows that one or both ovaries have≥ 12 follicles with a diameter of 2–9 mm and/or one or both ovarian volumes ≥ 10 mL.
IR Diagnostic Criteria
IR has two diagnostic criteria. The Western medicine diagnostic criteria are based on the Expert Consensus on Methods Assessing and Diagnosing Insulin Resistance, published by the Chinese Diabetes Society in 2018.29 The homeostasis model is applied to assess the IR index (HOMA-IR), HOMA-IR = FPG × FINS/22.5,
FPG, fasting plasma glucose level measured in mmol/L; FINS, fasting insulin level measured in μU/mL.
A HOMA-IR value ≥ 1.66 is diagnosed as IR.30
The Traditional Chinese Medicine (TCM) diagnostic criteria for insulin resistance (IR) are based on the syndrome differentiation of kidney deficiency with phlegm-dampness, as described in the Guiding Principles for Clinical Research of New Traditional Chinese Medicine, issued by the China Ministry of Health in 2002, together with recommendations from relevant TCM gynecological literature.31 The main symptoms include 1) infrequent menstruation or even amenorrhea; 2) waist and knee weakness; 3) chest and abdominal fullness and discomfort. The secondary symptoms (Table 1) include: 1) Pale and thin menstruation; 2) dizziness and tinnitus; 3) fatigue, shortness of breath, and reluctance to speak; 4) overweight or obesity; 5) loose stools; 6) greasy mouth and excessive phlegm.
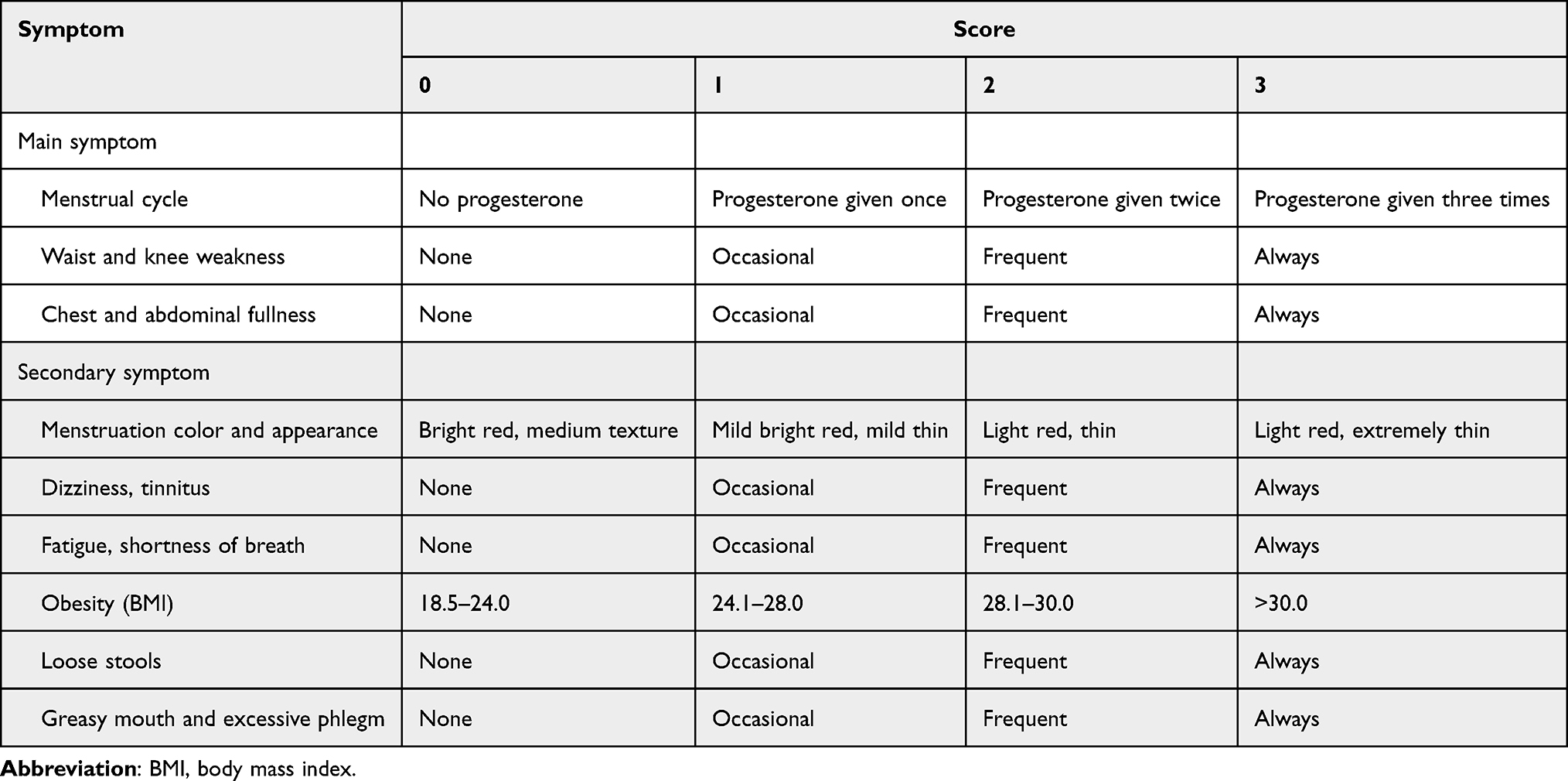 |
Table 1 Traditional Chinese Medicine Symptom Score System |
Tongue: pale and swollen, with a white, greasy, or thick coating.
Pulse: deep and slippery, or thin and soft.
A diagnosis of IR (kidney deficiency with phlegm dampness syndrome) can be made when all primary symptoms are present, along with at least one to two secondary symptoms, combined with specific tongue and pulse signs.
Participant Selection Criteria
The inclusion criteria are: 1) age 18–40 years old; 2) meeting all the above diagnostic criteria for PCOS, as well as IR with secondary symptoms; 3) negative blood pregnancy test result and no intention for pregnancy within the next 90 days. The exclusion criteria are, 1) with severe concurrent diseases, such as cardiovascular, cerebrovascular, liver, kidney, and hematopoietic system illnesses or mental disorder; 2) diagnosed as type 1 or 2 diabetes; 3) with malignant tumors, adrenal diseases, or other diseases leading to organ failure; 4) received any hormone drugs or drugs that affect insulin secretion in the past month; 5) abnormal liver and kidney function, with serum creatinine>133 μmol/L, alanine aminotransferase and aspartate aminotransferase more than twice the upper limit of normal range, total bilirubin more than twice the upper limit of normal range; 6) with previous allergic reaction to medications or herbs used in the current study; 7) history of alcohol or drug abuse, or other diseases or conditions that reduce the treatment and follow-up compliance, such as frequent job changes or unstable living environment; 8) participation in other clinical studies in the past month, or those who have been using similar drugs and related treatments in the month before randomization, making it difficult to determine the efficacy of the trial medications.
Sample Size Estimation
The trial will include four groups of patients (low, medium, and high doses of Lingshu granules, Lingshu decoction). Based on a pilot study, HOMA-IR could decline 1.4, with a standard deviation of 0.6, after Lingshu treatment. We expect a decrease in the HOMA-IR value of more than 0.4 in the medium-dose group compared to the decoction group. Therefore, we set the threshold as 0.4. With α = 0.025, β = 0.1, and a statistical power of 90%, we determine a sample size of 45 patients in each of the four groups (PASS version 11). Considering a loss-to-follow-up rate of 10%, we aim to include a total of 200 patients in the current study.
Randomization and Blinding
Enrolled patients will be randomly assigned to four groups at a ratio of 1:1:1:1, including group A (low-dose Lingshu granule), group B (medium-dose Lingshu granule), group C (high-dose Lingshu granule), and group D (Lingshu decoction).
The random numbers will be generated in SPSS (version 20.0, IBM, USA). These random numbers will be placed into light-proof, sealed envelopes and managed by a dedicated person for patient group assignment. Both the patients and the research personnel who recorded patient outcomes will be blinded to the group assignment. The randomization plan preparation, storage, and quality control are carried out by the clinical research service team based on evidence-based medicine.
Intervention
Trial herbs will be started within three days of the onset of spontaneous menses or progesterone-induced withdrawal bleeding and will be taken without interruption, including during menstruation. If menses have not occurred within 45 days, one-time oral dydrogesterone (10 mg, twice a day for 5 days) will be given to induce withdrawal bleeding. Treatment continues for 90 days.
Patients in groups A, B, and C receive different doses of Lingshu granules once a day. Patients in group D received Lingshu decoction, 100 mL, twice a day. The Lingshu decoction primarily contains epimedium 9 g, curculigo 9 g, atractylodes macrocephala 15 g, angelica sinensis 9 g, pinellia 9 g, and arisaema 9 g (other components are undisclosed due to patent restriction). The medium-dose Lingshu granule contains the same dose of herbs as the decoction formula. The low-dose Lingshu granule contains 20% less of each herb. The high-dose Lingshu granule contains 20% more of each herb.
Data Collection and Outcome Measurements
All patients will be followed up once every 30 days after the initiation of herb treatment. Pre- and post-treatment data will be collected and recorded promptly in a case report form by dedicated research personnel. Treatment outcomes and safety will be evaluated 90 days after the initiation of the trial herbs. The entire trial phases are shown in Table 2.
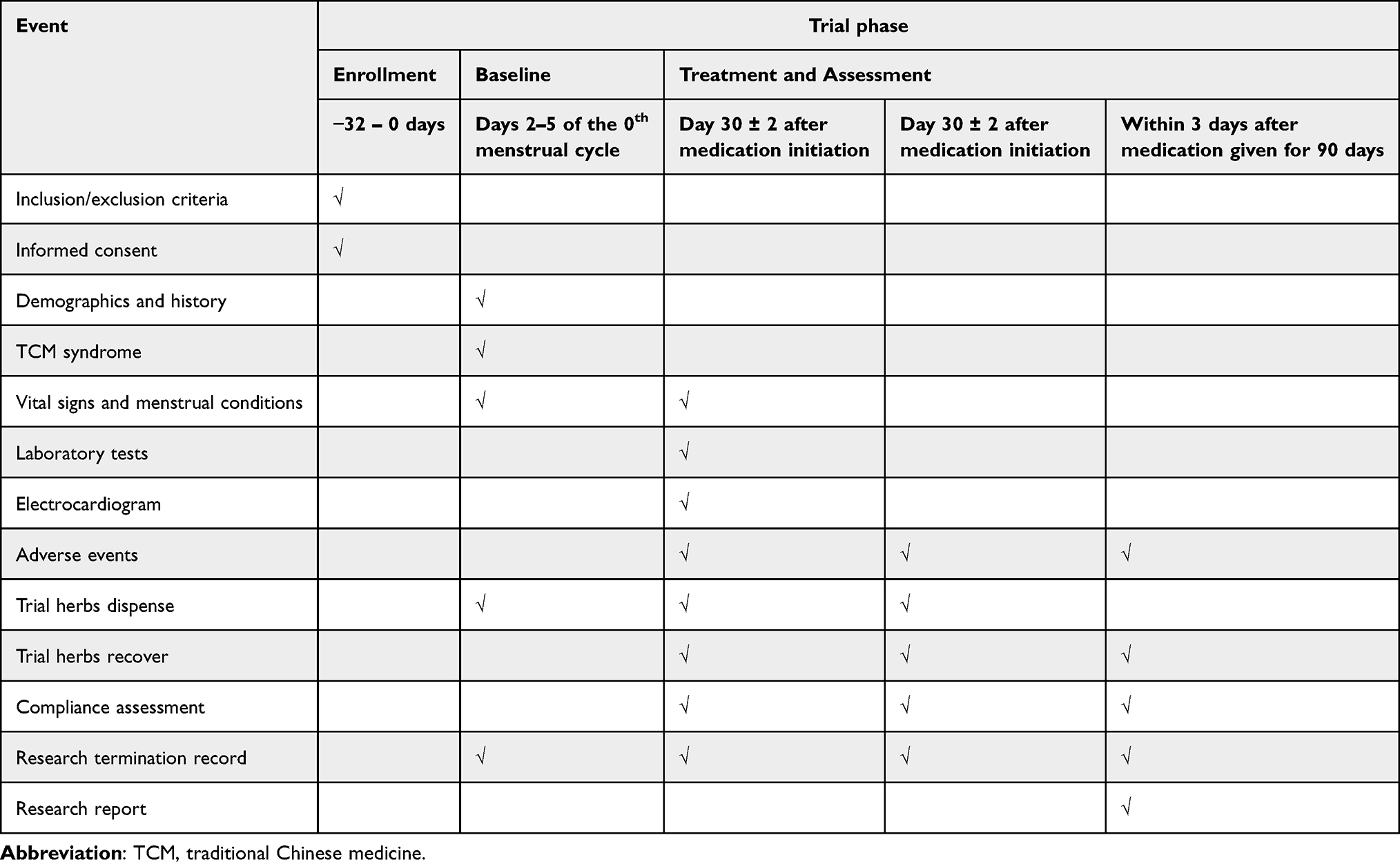 |
Table 2 Flowchart of Trial Phases of Enrollment, Interventions, and Assessment |
Efficacy Evaluation
The primary outcome is the change in HOMA-IR before and after treatment. The secondary outcomes include pre- and post-treatment changes in the body mass index, waist-to-hip ratio, FINS, FPG, serum follicle stimulating hormone (FSH), luteinizing hormone (LH), testosterone, estradiol, prolactin, progesterone, total cholesterol, triglycerides, low-density lipoprotein, high-density lipoprotein, apolipoprotein A, and apolipoprotein B levels, as well as ovarian size measured by the ultrasound. In addition, we developed a TCM symptom-score table with reference to the diagnostic criteria for kidney deficiency and phlegm-dampness in the Guiding Principles for Clinical Research of New Chinese Medicines and the symptom criteria for kidney deficiency and phlegm-dampness in TCM Gynecology (Table 1).31
Safety Evaluation
Safety will be assessed by monitoring vital signs (temperature, heart rate, and blood pressure), laboratory tests—including urinalysis, coagulation profile, and liver and renal function panels—and electrocardiograms, as well as adverse events that occurred during medication administration.
Statistical Analysis
All data will be analyzed in SPSS version 20.0 (IBM, USA) by a dedicated study statistician. Continuous variables will be expressed as mean ± standard deviation or median (interquartile range), depending on the results of normality testing. Categorical variables will be summarized as counts (percentages). Pre- and post-treatment changes among groups will be compared with analysis of variance (ANOVA) for continuous data and the chi-square test or Fisher’s exact test for categorical data, as appropriate. Results with a one-sided P < 0.025 will be considered statistically significant.
Discussion
PCOS is the most common endocrine-metabolic disorder among women of reproductive age.1 IR is a key contributor to the pathogenesis of PCOS. Evidence shows that IR can increase androgen levels, disrupt follicle development, impair ovarian function, and reduce oocyte quality. IR can also worsen glucose and lipid metabolism and raise the risk of metabolic syndrome. The incidence of Hashimoto’s thyroiditis was also related to IR and relatively low thyroid function and high left ovarian volume in PCOS patients.6,32,33 Although multiple pharmacologic treatments have been used for PCOS-associated IR, their efficacy remains controversial.34 Growing research on TCM suggests that Chinese herbs may offer a meaningful therapeutic option for patients with PCOS and IR.35
Based on TCM principles, we have developed the Lingshu formula, which primarily contains six herbs: Epimedium, Curculigo, Atractylodes macrocephala, Angelica sinensis, Pinellia, and Arisaema (other components are undisclosed due to patent restrictions). Epimedium tonifies the kidney, strengthens bone and muscle, dispels dampness, and enhances libido and fertility.36 Curculigo warms the spleen and strengthens the kidneys and is commonly prescribed for impotence and infertility.37 Atractylodes macrocephala fortifies the spleen, dries dampness, and promotes water metabolism; it is used for fatigue and digestive complaints.38 Angelica sinensis nourishes and invigorates the blood, regulates menstruation, and alleviates pain, thereby improving female reproductive health and correcting blood deficiency.39 Pinellia dries dampness and resolves phlegm and is indicated for cough, excessive phlegm, and indigestion.40 Arisaema transforms phlegm-heat, calms convulsions, and relieves spasms; it is frequently employed for wind-phlegm conditions, stroke, and seizures.41,42
Clinical and animal studies have demonstrated that Lingshu decoction could effectively reduce the HOMA-IR index, body mass index, testosterone, and LH/FSH ratio of PCOS-IR patients and improve the blood lipid profile.17–20 However, traditional preparations, such as Lingshu decoction, have several limitations, including time-consuming preparation, unpalatable taste, short shelf life, and challenges in storage and transportation. In contrast, the formula granules can overcome these drawbacks while preserving the advantages and characteristics of TCM. The granules are easy to take, which can improve patient compliance. Patients may prefer to take granules over decoction formulas. However, whether the pharmacological effects of formula granules are equivalent to those of traditional decoctions remains controversial.43 To date, no studies have directly compared Lingshu formula granules with decoctions in patients with PCOS and IR, which will be the focus of our study. In addition, our clinical trial will also identify the optimal granule dose and clarify the relative effectiveness of the granule and decoction preparations. These results will not only support the clinical use of the Lingshu formula in PCOS-IR but also guide future research. Moreover, successful completion of this trial may advance the widespread acceptance of TCM.
Limitations
We acknowledge several limitations. First, although the trial will be conducted across multiple research centers, all participants will be recruited from the local region, which may limit the generalizability of our findings. Second, the relatively long study duration could affect participant compliance. Finally, only three doses of the Lingshu formula will be evaluated, which may not capture the optimal efficacy dose; additional dose-response studies are therefore warranted.
Ethics and Clinical Registration
The study received approval from the Ethics Committee of Guangdong Provincial Hospital of Chinese Medicine on August 1, 2024 (approval No. BF2024-199-01) and will adhere strictly to the Declaration of Helsinki. The trial was registered with the International Traditional Medicine Clinical Trial Registry Platform (ITMCTR2024000837) on December 17, 2024. All participants will provide written informed consent before enrollment. The study’s purpose, procedures, privacy safeguards, benefits, potential risks, and the voluntary nature of participation will be thoroughly explained to each participant. All data will be securely stored to protect participant confidentiality, and the ethics committee will oversee study conduct.
Study results will be submitted for peer review and publication and will be presented at national and international conferences. After study completion, all data will be stored in a secure cabinet under the custody of the corresponding authors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This work was supported by “Basic and Applied Basic Research Foundation of Guangdong Province (2023A1515220224)”, “Guangdong Provincial Administration of Traditional Chinese Medicine (20232047)”, and “Special Project for Scientific Research in Traditional Chinese Medicine at Guangdong Provincial Hospital of Traditional Chinese Medicine (YN2024GZRPY006)”.
Disclosure
The authors declare that they have no conflict of interest.
References
1. Dong J, Rees DA. Polycystic ovary syndrome: pathophysiology and therapeutic opportunities. BMJ Med. 2023;2(1):e000548. doi:10.1136/bmjmed-2023-000548
2. Lentscher JA, Decherney AH. Clinical presentation and diagnosis of polycystic ovarian syndrome. Clin Obstet Gynecol. 2021;64(1):3–11. doi:10.1097/GRF.0000000000000563
3. Organization WH. Polycystic ovary syndrome. World Health Organization; 2025 [cited 2025 July 2nd]. Available from: https://www.who.int/news-room/fact-sheets/detail/polycystic-ovary-syndrome.
4. Jiang B. The global burden of polycystic ovary syndrome in women of reproductive age: findings from the GBD 2019 study. Int J Womens Health. 2025;17:153–165. doi:10.2147/IJWH.S490836
5. Amisi CA. Markers of insulin resistance in Polycystic ovary syndrome women: an update. World J Diabetes. 2022;13(3):129–149. doi:10.4239/wjd.v13.i3.129
6. Purwar A, Nagpure S. Insulin resistance in polycystic ovarian syndrome. Cureus. 2022;14(10):e30351. doi:10.7759/cureus.30351
7. Zhao H, Zhang J, Cheng X, Nie X, He B. Insulin resistance in polycystic ovary syndrome across various tissues: an updated review of pathogenesis, evaluation, and treatment. J Ovarian Res. 2023;16(1):9. doi:10.1186/s13048-022-01091-0
8. Stanczak NA, Grywalska E, Dudzinska E. The latest reports and treatment methods on polycystic ovary syndrome. Ann Med. 2024;56(1):2357737. doi:10.1080/07853890.2024.2357737
9. Saadati S, Mason T, Godini R, Vanky E, Teede H, Mousa A. Metformin use in women with polycystic ovary syndrome (PCOS): opportunities, benefits, and clinical challenges. Diabetes Obes Metab. 2025;27 Suppl 3(Suppl 3):31–47. doi:10.1111/dom.16422
10. Giglio RV, Papanas N, Rizvi AA, et al. An update on the current and emerging use of thiazolidinediones for type 2 diabetes. Medicina. 2022;58(10):1.
11. Susilawati E, Levita J, Susilawati Y, Sumiwi SA. Review of the case reports on metformin, sulfonylurea, and thiazolidinedione therapies in type 2 diabetes mellitus patients. Med Sci. 2023;11(3). doi:10.3390/medsci11030050
12. Boettcher E, Csako G, Pucino F, Wesley R, Loomba R. Meta-analysis: pioglitazone improves liver histology and fibrosis in patients with non-alcoholic steatohepatitis. Aliment Pharmacol Ther. 2012;35(1):66–75. doi:10.1111/j.1365-2036.2011.04912.x
13. Komajda M, McMurray JJ, Beck-Nielsen H, et al. Heart failure events with rosiglitazone in type 2 diabetes: data from the RECORD clinical trial. Eur Heart J. 2010;31(7):824–831. doi:10.1093/eurheartj/ehp604
14. Lim J, Li J, Feng X, et al. Predicting TCM patterns in PCOS patients: an exploration of feature selection methods and multi-label machine learning models. Heliyon. 2024;10(15):e35283. doi:10.1016/j.heliyon.2024.e35283
15. Xu D, Lu M, Liu Y, et al. An analysis of the clinical medication rules of traditional chinese medicine for polycystic ovary syndrome based on data mining. Evid Based Complement Alternat Med. 2023;2023:6198001. doi:10.1155/2023/6198001
16. Chen H, Deng C, Meng Z, Meng S. Effects of TCM on polycystic ovary syndrome and its cellular endocrine mechanism. Front Endocrinol. 2023;14:956772. doi:10.3389/fendo.2023.956772
17. LX ML. Clinical efficacy of Lingshu granules in polycystic ovary syndrome patients with kidney deficiency and phlegm-dampness and insulin resistance. New Chinese Med. 2011;43(11):3.
18. Zhong XC, Zhang J, Chen QX, Li XB, Deng WM. Clinical efficacy of Lingshu granules combined with clomiphene in patients with polycystic ovary syndrome. New Chin Med. 2010;(42):43–45.
19. HX HXD. Clinical efficacy of Lingshu oral preparation combined with Shenqi capsules in 34 patients with polycystic ovary syndrome. J Pract Med. 2007;18(1):2.
20. Li XB, Li LY, Fu F, Hu XD. Clinical efficacy of sequential therapy with Lingshu oral preparation and shenqi capsules in patients with polycystic ovary syndrome. J Tradit Chin Med. 2007;(12):1079–1081.
21. Li XB, Zhai JL, Li LY, Hu XD Effects of Lingshu granules in endocrine function and lipid metabolism in patients with polycystic ovary syndrome. J Tradit Chin. 2011;(52):31–34.
22. Zhang ZW. Discussion on the reform of decoction dosage form. Shanghai J Traditional Chin Med. 1984;1984(8):30–31.
23. Song JH, Song YR. Development and application prospects of traditional Chinese medicine formula granules. Northern Pharm. 2024;21(12):193–196.
24. Xu Q, Sun DY. Discussion on the advantages and disadvantages of bulk decoction pieces, formula granules, and small-packaged decoction pieces of traditional Chinese medicine. J Admin Trad Chin Med. 2024;32(20):67–69.
25. Zhang XQ, Wei XD, Gu ZX, et al. Application of artificial intelligence-assisted Traditional Chinese medicine formula granules in bone and joint degenerative diseases in the field of holistic health. Front Med Lausanne. 2025;12:1630824. doi:10.3389/fmed.2025.1630824
26. Tian MY, Tao XQ, Han ZX. Progress in pharmacological studies of traditional Chinese medicine formula granules and comparative studies with decoction pieces. J Shenyang Pharmaceut Univ. 2024;41(08):978–994.
27. Li ZJ, Liu HB, Zhang Y. A study on the differences between traditional decoction and formula granule decoction of ze xie tang based on chemical characterization. China Hospital Pharm Eval Anal. 2025;25(04):394–398+402.
28. Rotterdam EA-SPcwg. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum Reprod. 2004;19(1):41–47. doi:10.1093/humrep/deh098
29. Association DSot CM. Expert Consensus on Methods for Assessing and Diagnosing Insulin Resistance. Chin J Diabetes Mellitus. 2018;10(6):9.
30. Lin JF, Li X, Zhu MW. Classification of polycystic ovary syndrome. Chin J Obstetrics Gynecol. 2006;41(10):5.
31. XY Z. [Guiding Principles for Clinical Research of New Traditional Chinese Medicine]. Beijing: China Medical Science and Technology Press; 2002.
32. Zhao H, Zhang Y, Ye J, et al. A comparative study on insulin secretion, insulin resistance and thyroid function in patients with polycystic ovary syndrome with and without hashimoto’s thyroiditis. Diabetes Metab Syndr Obes. 2021;14:1817–1821. doi:10.2147/DMSO.S300015
33. Gencer G, Serin AN, Gencer K. Analysis of the effect of hashimoto’s thyroiditis and insulin resistance on ovarian volume in patients with polycystic ovary syndrome. BMC Womens Health. 2023;23(1):86. doi:10.1186/s12905-023-02200-x
34. Waghmare SV, Shanoo A. Polycystic ovary syndrome: a literature review with a focus on diagnosis, pathophysiology, and management. Cureus. 2023;15(10):e47408. doi:10.7759/cureus.47408
35. Sun M, Qiu X, Yuan Z, Xu C, Chen Z. New advances in traditional chinese medicine interventions for epilepsy: where are we and what do we know? Chin Med. 2025;20(1):37. doi:10.1186/s13020-025-01088-z
36. Cui J, Lin L, Hao F, et al. Comprehensive review of the traditional uses and the potential benefits of epimedium folium. Front Pharmacol. 2024;15:1415265. doi:10.3389/fphar.2024.1415265
37. Chen L, Qu B, Wang H, et al. The effect of curculigo orchioides (Xianmao) on kidney energy metabolism and the related mechanism in rats based on metabolomics. Food Sci Nutr. 2021;9(11):6194–6212. doi:10.1002/fsn3.2573
38. Zhu B, Zhang QL, Hua JW, Cheng WL, Qin LP. The traditional uses, phytochemistry, and pharmacology of Atractylodes macrocephala Koidz.: a review. J Ethnopharmacol. 2018;226:143–167. doi:10.1016/j.jep.2018.08.023
39. Ren C, Luo Y, Li X, et al. Pharmacological action of Angelica sinensis polysaccharides: a review. Front Pharmacol. 2024;15:1510976.
40. Zou T, Wang J, Wu X, et al. A review of the research progress on Pinellia ternata (Thunb.) Breit.: botany, traditional uses, phytochemistry, pharmacology, toxicity and quality control. Heliyon. 2023;9(11):e22153. doi:10.1016/j.heliyon.2023.e22153
41. Li J, Bai L, Wei F, et al. Therapeutic mechanisms of herbal medicines against insulin resistance: a review. Front Pharmacol. 2019;10:661. doi:10.3389/fphar.2019.00661
42. Kant K, Lal UR, Rawat R, Kumar A, Ghosh M. Genus arisaema: a review of traditional importance, chemistry and biological activities. Comb Chem High Throughput Screen. 2020;23(7):624–648. doi:10.2174/1386207323666200416150754
43. Qiu R, Zhang X, Zhao C, Li M, Shang H. Comparison of the efficacy of dispensing granules with traditional decoction: a systematic review and meta-analysis. Ann Transl Med. 2018;6(3):38. doi:10.21037/atm.2017.10.22
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Tumor Necrosis Factor Alpha Level in the Uterine Fluid of Patients with Polycystic Ovary Syndrome and Its Correlation with Clinical Parameters
Ha LX, Li WX, Du YD, Yuan YY, Qu XX
Journal of Inflammation Research 2022, 15:6015-6020
Published Date: 29 October 2022
Thyroid Hormones and Cardiometabolic Risk Factors in Saudi Women with Polycystic Ovary Syndrome: A Cross-Sectional Study
Saeed WM, Alsehli F
International Journal of Women's Health 2023, 15:1197-1203
Published Date: 26 July 2023
Correlation Between Hemoglobin Levels and Polycystic Ovary Syndrome Metabolic Disorder
Ha LX, Du YD, Qu XX, Wang JJ
Diabetes, Metabolic Syndrome and Obesity 2023, 16:3019-3027
Published Date: 28 September 2023
Association Between rs2278426 Polymorphism of the ANGPTL8 Gene and Polycystic Ovary Syndrome
Wu H, Wang H, Sun L, Liu M, Wang H, Sun X, Zhang W
Diabetes, Metabolic Syndrome and Obesity 2024, 17:1749-1760
Published Date: 16 April 2024
Glycolytic Dysfunction in Granulosa Cells and Its Contribution to Metabolic Dysfunction in Polycystic Ovary Syndrome
Cao Z, Zhou Q, An J, Guo X, Jia X, Qiu Y
Drug Design, Development and Therapy 2025, 19:5255-5270
Published Date: 18 June 2025