Back to Journals » Nature and Science of Sleep » Volume 17

Effects of Aerobic Exercises at Different Intensities on Sleep Quality in Individuals with Depression: A Systematic Review and Meta-Analysis
Authors Liang J, Pan X, Zhao L, Li Y
Received 2 February 2025
Accepted for publication 9 May 2025
Published 3 September 2025 Volume 2025:17 Pages 2091—2109
DOI https://doi.org/10.2147/NSS.S520079
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
Jiaqi Liang,1 Xuanzhen Pan,1 Li Zhao,1,2 Yan Li1,2
1Department of Exercise Physiology, School of Sport Science, Beijing Sport University, Beijing, People’s Republic of China; 2Beijing Key Laboratory of Sports Performance and Skill Assessment, Beijing Sport University, Beijing, People’s Republic of China
Correspondence: Yan Li, Department of Exercise Physiology, School of Sport Science, Beijing Sport University, No. 48 Xinxi Road, Haidian District, Beijing, 100084, People’s Republic of China, Email [email protected]
Purpose: Depression patients frequently report sleep disorder. Aerobic exercise is believed to improve sleep quality, but its effect on the overall sleep of depressed patients remains uncertain. This study systematically evaluates the effects of aerobic exercises at different intensities on subjective and objective sleep quality in participants diagnosed with depression or at high risk of depression, from studies covering various depression subtypes (including but not limited to geriatric depression, prenatal depression, and poststroke depression), and examines changes in depression, anxiety, and quality of life following aerobic exercise.
Methods: Systematic searches for randomized controlled trials on aerobic exercise, depression, and sleep quality were conducted using PubMed, Web of Science, Embase, and the Cochrane Library up to December 31, 2024. Meta-analysis was performed using Review Manager 5.4.1 and stata 17.0.
Results: In total, 13 trials (n = 994) were included. Aerobic exercise significantly improved subjective sleep quality [SMD = − 0.52, 95% CI = (− 0.66, − 0.38)] but had no significant effect on objectively measured sleep efficiency [SMD = − 0.14, 95% CI = (− 0.46, 0.75)], total sleep time [SMD = 0.30, 95% CI = (− 0.03, 0.62)], or sleep latency [SMD = − 0.11, 95% CI = (− 0.76, 0.54)]. Additionally, aerobic exercise significantly alleviated depression [SMD = − 0.70, 95% CI = (− 0.93, − 0.47)] and anxiety [SMD = − 0.47, 95% CI = (− 0.74, − 0.19)], and enhanced quality of life [SMD = 0.64, 95% CI = (0.36, 0.92)]. Subgroup analyses revealed no significant differences among the different intensities.
Conclusion: Aerobic exercise significantly improves subjective sleep quality, alleviates depressive and anxiety symptoms, and enhances quality of life in depression patients. Light-, moderate-, and vigorous-intensities aerobic exercises have equal positive effects on these indicators. Given the bidirectional relationship between sleep disturbances and depression progression, this study highlights the potential of exercise therapy to disrupt the vicious cycle.
Systematic Review Registration: www.crd.york.ac.uk/PROSPERO/, identifier, CRD42023455212.
Keywords: aerobic exercise, depression, sleep quality, meta-analysis
Introduction
Depression is frequently associated with alterations in sleep neurophysiology, with most patients experiencing either insomnia or excessive sleep episodes.1–5 Sleep electroencephalogram (EEG) studies indicate that patients with depression exhibit typical sleep EEG changes such as disinhibition of rapid eye movement (REM) sleep, impaired sleep continuity, and reduced non-REM sleep.6 These symptoms indicate a lower quality of sleep. Sleep quality is defined as an individual’s self-satisfaction with their sleep experience, commonly assessed through both subjective measures (eg, the Pittsburgh Sleep Quality Index) and objective parameters (eg, polysomnography-derived sleep efficiency).7
In the causal factors that lead to depression, the most well-known hypothesis is the monoamine hypothesis, which posits that alterations in monoamine levels, including the noradrenergic, dopaminergic, and serotonergic systems, are causally linked to depression.8 Among these, serotonin plays an important role in regulating the circadian rhythm of the sleep-wake cycle.9 Consequently, its deficiency is suspected to be one of the underlying mechanisms that may contribute to the reduced sleep quality observed in depressed patients.10 Moreover, a recent study covering 1053 individuals with major depressive disorder demonstrated that insomnia symptoms were associated with reduced cortical surface area.11 Additionally, studies applying magnetic resonance imaging have found volume reductions in the amygdala of patients with depression,12,13 an area that plays a role not only in emotional processing but also in controlling REM sleep.14
However, sleep problems are not merely a byproduct of depression, they can also serve as a causal factor for psychiatric disorders, especially in individuals with chronic poor sleep quality who are more susceptible to developing depression.15,16 Sleep loss generally causes mood problems, subsequently reducing quality of life.17 Sleep loss may increase markers of inflammation, such as interleukin-6 (IL-6) and C-reactive protein (CRP), by activating the sympathetic nervous system and β-adrenergic signaling, leading to increased nuclear factor-kappa B (NF-κB) and the activation of inflammatory gene expression.18 Meanwhile, inflammation may serve as a contributing factor to the development of depression.19 In addition, twin and genome-wide association studies have demonstrated a significant genetic overlap between insomnia and major depression.20–22 These findings indicate a strong and bidirectional association between sleep disorder and depression.23,24 In another word, sleep disorder may trigger the onset of depression, and in turn, depressive symptoms may further worsen sleep quality, creating a vicious cycle that exacerbates the condition.
Pharmacological and psychotherapeutic interventions have made significant advancements in the treatment of depression, yet they are accompanied by a relatively high relapse rate.25,26 Consequently, sleep disorder remains prevalent among individuals recovering from depression.27 Furthermore, anxiety and reduced quality of life are also high-risk factors contributing to the recurrence of depression.28,29 The persistence of residual problems may result in increased subjective distress and an elevated risk of depressive relapse.30 Thus, post-treatment care for patients with depression should encompass a broader range of considerations, extending beyond the mere alleviation of depressive symptoms to focus other critical aspects of psychology and life.
A large number of studies have demonstrated that exercise is effective at reducing depressive symptoms.31–33 Physiologically, exercise is hypothesized to improve depressive symptoms through diverse mechanisms including anti-inflammatory effects,34 reducing oxidative stress,35 and enhancing hippocampal neurogenesis and synaptic plasticity.36 However, there is considerable diversity in the exercise therapy protocols used across studies, and currently, there is no standardization or consistency in the properties of exercise programs, including type, intensity, duration, and frequency.32 Current research indicates that aerobic exercise, resistance training, and mind-body exercises all have the potential to alleviate depressive symptoms and enhance sleep quality.37,38 Considering the feasibility and safety in clinical practice, aerobic exercise and mind-body exercises may be more suitable for patients with depression, with low costs, minimal side effects, and few practical barriers. Thus, aerobic exercise has been the most frequently selected intervention in previous studies.32 Intensity, duration, and frequency are all critical factors in determining treatment efficacy, with intensity often considered to be the most influential.39 Overly intense exercise can cause fatigue and muscle soreness, potentially resulting in sleep problems.40 Exercise intensity refers to the physiological demand of physical activity, typically categorized as light, moderate, or vigorous based on objective measures (eg, heart rate). The latest meta-analysis indicated that physical activity is beneficial for improving the sleep quality of patients with major depressive disorders (MDD).41 However, the authors did not further analyze the impact of different exercise intensities on outcomes, limiting the ability to formulate precise exercise prescriptions for individuals with depression. In addition, few studies have concurrently focused effects of aerobic exercises at different intensities on the other factors that contribute to the recurrence of depression (anxiety and quality of life). Therefore, the present meta-analysis aimed to investigate the effects of aerobic exercises at different intensities on sleep quality, depressive symptoms, anxiety, and quality of life among individuals with depression. In this study, “depression” primarily denotes the core symptoms of MDD as defined by DSM-5 criteria (eg, persistent depressed mood, anhedonia, and sleep disturbances).42 The term “patients with depression” refers to individuals who: (a) meet clinical diagnostic criteria for depression, or (b) are identified as high-risk through validated screening instruments (eg, HDRS17 > 16).43 Notably, some included studies may involve populations with other depression subtypes (eg, prenatal depression) that fulfill these core MDD symptom criteria. To our knowledge, this study is the first to focus on the effects of aerobic exercises at different intensities on sleep-related symptoms and sleep quality in patients with depression.
Method
This systematic review and meta-analysis were based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 2020,44 and the protocol for this systematic review has been prospectively registered in the International Prospective Register of Systematic Reviews database (PROSPERO) on August 27th 2023 (registration number: CRD42023455212).
Search Strategy
We conducted a systematic search of the following 4 databases: PubMed, Web of Science, Embase and the Cochrane Library from the inception of indexing until December 31, 2024 (section 1 of supplementary file 1).
All studies were searched using the following MESH terms and keywords: “depression”, “mood disorder”, “exercise”, “physical activity”, “sport”, “sleep”, “insomnia” et al. Identified records were managed using EndNote 20.5. Two independent authors (JL, XP) assessed all titles, abstracts, and full-text articles to filter and identify relevant studies (section 2 of supplementary file 1). In order to avoid missing related articles as much as possible, we also screened all references from the included studies. Any disagreements during this process were settled by discussion.
Eligibility Criteria
We included trials which met the following criteria: 1) participants were over the age of 18 years old; 2) participants were diagnosed with depression or had a high risk of depression (eg, evaluations above the depression threshold in self-reported depression questionnaires); 3) the trial included at least one experimental group and one control group, and the control group could be a) waitlist controls (no intervention), b) treatment-as-usual controls, or c) active non-exercise controls (eg, relaxation training). The key difference between groups was the addition of aerobic exercise in the experimental group; 4) only trials designed as the randomized controlled trials (RCTs) were searched; 5) the outcomes included the effective indicators reflecting sleep quality, depression, anxiety and quality of life, and reported in the form of means and standard deviations (Mean ± SD) or other forms that could be transformed to Mean ± SD.
Studies that met any of the following criteria were excluded: 1) participants suffered from a significant somatic disorder or other mental disorders (eg, paralysis or schizophrenia); 2) animal studies; 3) case reports, conference abstracts, review articles, or non-English language articles; 4) without available data.
Data Extraction
From each included study, two reviewers (JL, XP) independently extracted the following relevant information: author(s), location, participant characteristics (eg, age and gender), sample size, details of interventions (eg, type, frequency, and duration), and reported outcomes. When continuous variables in the study were reported as median with range or interquartile range, we calculated the Mean ± SD through the validated mathematical method.45,46 We contacted the authors when required data were not reported (section 3 of supplementary file 1).
Quality Assessment
Two authors (JL, XP) independently rated the risk of bias of the RCTs using the revised Cochrane risk of bias, version 2.0 (RoB 2.0) tool.47 All included studies were assessed as “low”, “some concerns”, or “high” on the following domains: 1) randomization process; 2) deviations from the intended interventions; 3) missing outcome data; 4) measurement of the outcome; and 5) selection of the reported result. Disagreements were resolved by consensus.
Statistical Analysis
The meta-analysis was carried out using the Review Manager 5.4.1 version (Cochrane Collaboration, Oxford, UK). If the reported outcomes were measured by different methods, the effect size would be synthesized using the standardized mean difference (SMD). If the outcomes were measured by the same methods, the effect size would be integrated using the weight mean difference (WMD). All metrics were reported with 95% confidential intervals (CI).
The heterogeneity across the studies was evaluated using the I2 index. An I2 value >50% represented substantial heterogeneity for outcomes.48 A random-effect model would be used to aggregate the outcomes for studies with high heterogeneity (I2 > 50%). Otherwise, a fixed-effect model would be chosen (I2 < 50%). Given the inherent differences between the included studies, we conducted an additional analysis using a random-effects model for the outcomes analyzed with a fixed-effect model. In addition, we performed sensitivity analyses to validate the stability of the combined outcomes, assessing the influence of each study on the composite results by removing the individual study one by one. Publication bias was evaluated visually by creating funnel plot via Review Manager 5.4.1 version, as well as by conducting Egger’s regression tests using Stata 17.0 version (Stata Corp, College station, TX, USA) for outcomes.49 Publication bias was considered statistically significant at p value <0.05.
For the subgroup analysis, all included studies were divided into three subgroups based on aerobic exercise intensity: light-, moderate-, and vigorous-intensities. Aerobic exercise intensity was classified according to the definition of Norton et al, 2010.50 ‘Light-intensity’ includes the following: 1.6 < 3 metabolic equivalents (METs), 40 < 55% of maximal heart rate (HRmax), 20 < 40% of heart rate reserve (HRR), or Borg’s rating of perceived exertion (RPE) 8–10; ‘Moderate-intensity’ includes the following: 3 < 6 METs, 55 < 70% of HRmax, 40 < 60% of HRR, or RPE 11–13; ‘Vigorous-intensity’ includes the following: 6 < 9 METs, 70 > 90% of HRmax, 60 < 85% of HRR, or RPE 14–16. If the intensity of the aerobic intervention is not explicitly stated within the trial, a determination will be made by analyzing the specific description of the intervention within the original article, in conjunction with the author’s personal experience. For instance, a study that utilized tai chi as an intervention described this as ‘repetitious, nonstrenuous, slow-paced movement’,51 so we classified it as a light-intensity aerobic exercise.
Results
Study Selection
The search process is shown in Figure 1. We initially searched four electronic databases and found a total of 12819 records (PubMed, n = 1960; Wed of Science, n = 4489; EMBASE, n=2173; Cochrane Library, n = 4197). In addition, we reviewed 593 records that were outside the scope of the search by previewing the references of relevant studies. After deleting duplicates, 8823 records remained. Subsequently, 8756 irrelevant studies were removed by examining article titles and abstracts. The remaining 67 articles were read and evaluated in full-text by each of two independent authors. Finally, 13 eligible studies were included in this systematic review and meta-analysis.43,51–62
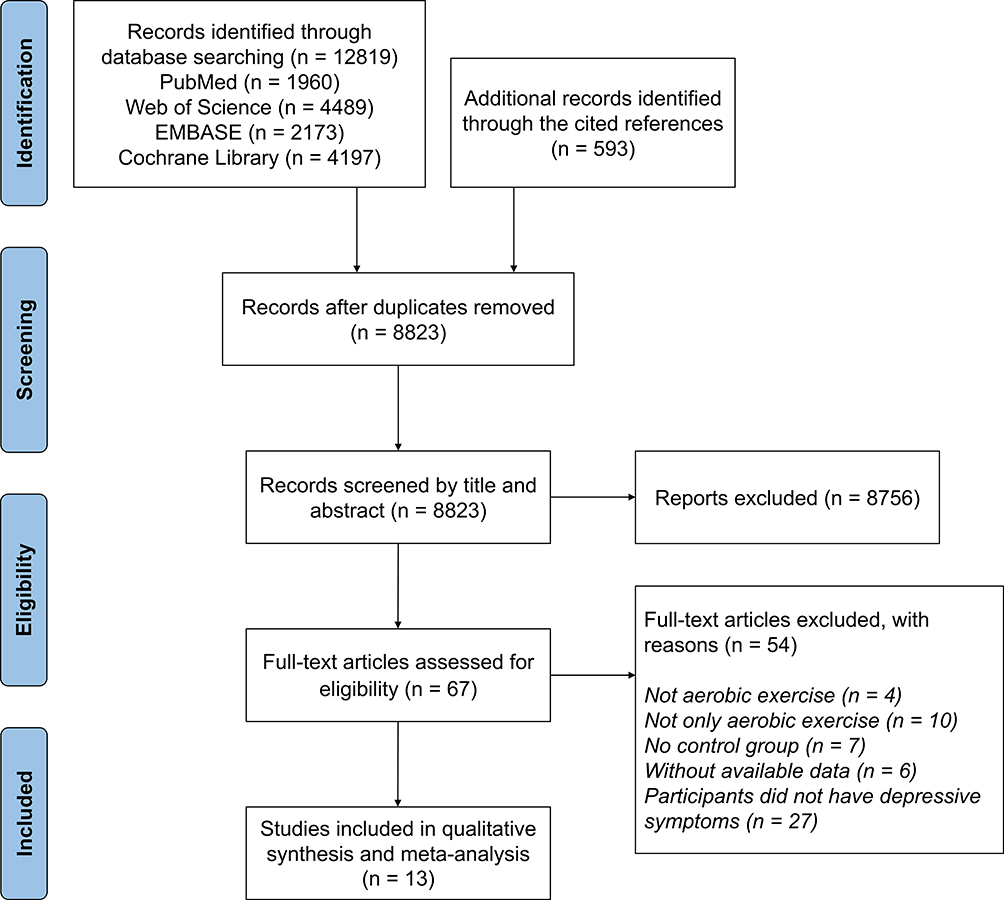 |
Figure 1 Flow diagram of the process of study selection. |
Characteristics of Included Studies
The basic characteristics of the 13 trials included in the analysis are summarized in Table 1. These 13 trials including a total of 994 participants with mild to major depressive disorder as determined by self-report or depression scales. Most of the trials recruited patients of both genders, but two studies were restricted to female,53,55 one of which had pregnant women.53 During data extraction, we noted that a study of Pinniger et al54 had corrected the data from the original article, and the updated data were used in our analysis.63
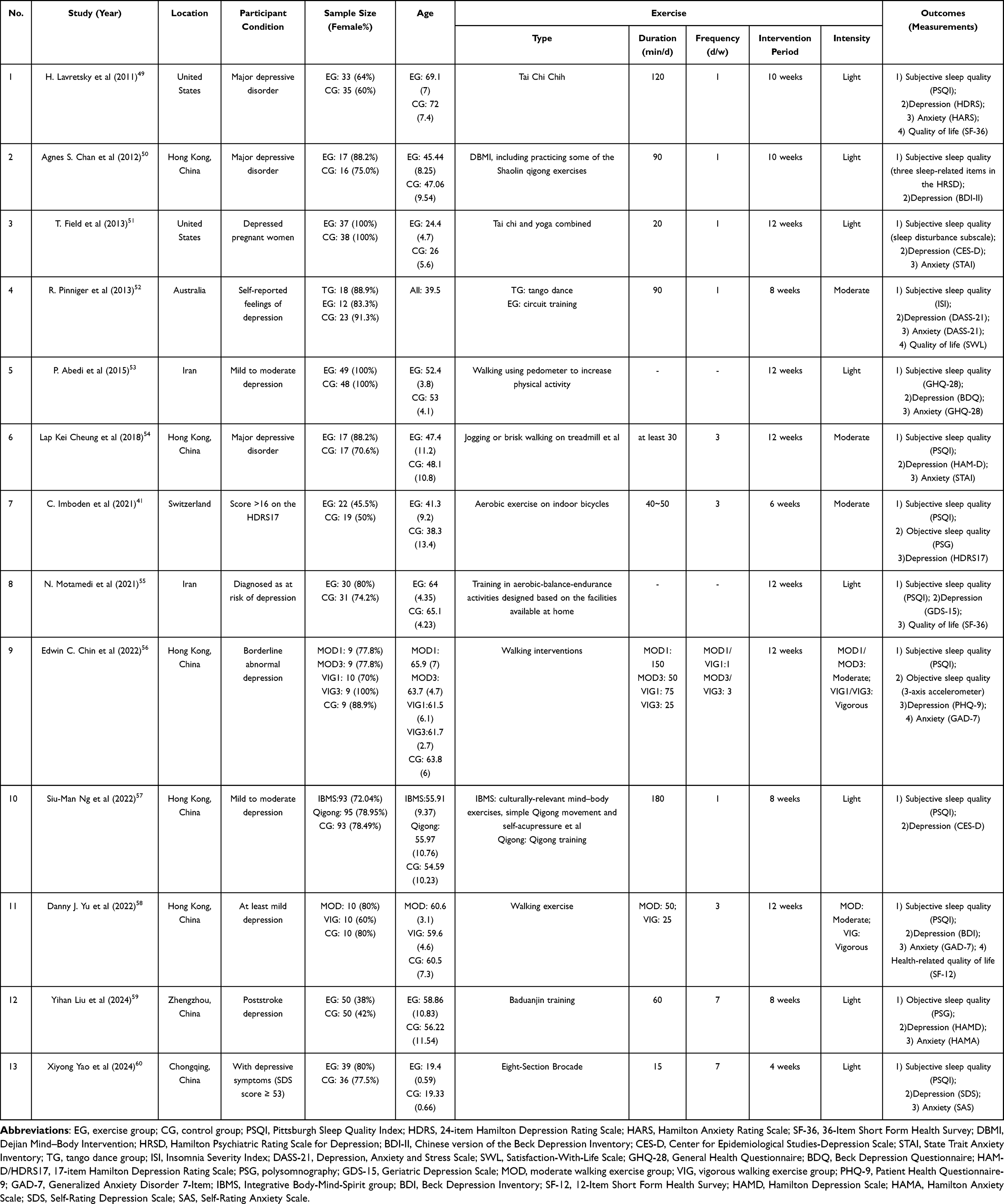 |
Table 1 Basic Characteristics of Included Studies |
All included studies reported aerobic interventions, such as tai chi, qigong, Baduanjin, tango dance, walking, cycling, and other types of aerobic training. Participants in the control group were instructed to maintain a normal daily lifestyle, receive routine care and medication, or perform some light stretching exercises, but not receive any active aerobic intervention. Two multi-arm randomized controlled trials conducted two different forms of aerobic exercise intervention simultaneously,54,59 and one study had an intervention of yoga combined with tai chi.53 The durations of the aerobic interventions were all kept at 4 to 12 weeks, and the frequency of the interventions was mainly 1 or 3 times per week. The aerobic exercise interventions of these trials were defined in terms of intensity based on Norton’s study50 and our subjective judgment. Two trials created multiple intervention groups based on different exercise intensities.58,60 The aerobic exercise interventions in most of the studies were guided and supervised by exercise specialists. Main outcome measures included depressive symptoms, subjective sleep quality, anxiety symptoms, and quality of life, which were detected by self-report questionnaires. There are three studies reporting objective sleep quality; two utilize polysomnography for recording,43,61 while the third employs a 3-axis accelerometer.58
Risk of Bias and Quality Assessment
RoB 2.0 was used to evaluate the methodological quality of the included trials.47 As shown in Figure 2, the assessment results indicated high risk for 1 study,55 some concerns for 2 studies,53,54 and low risk for 10 studies.43,51,52,56–62
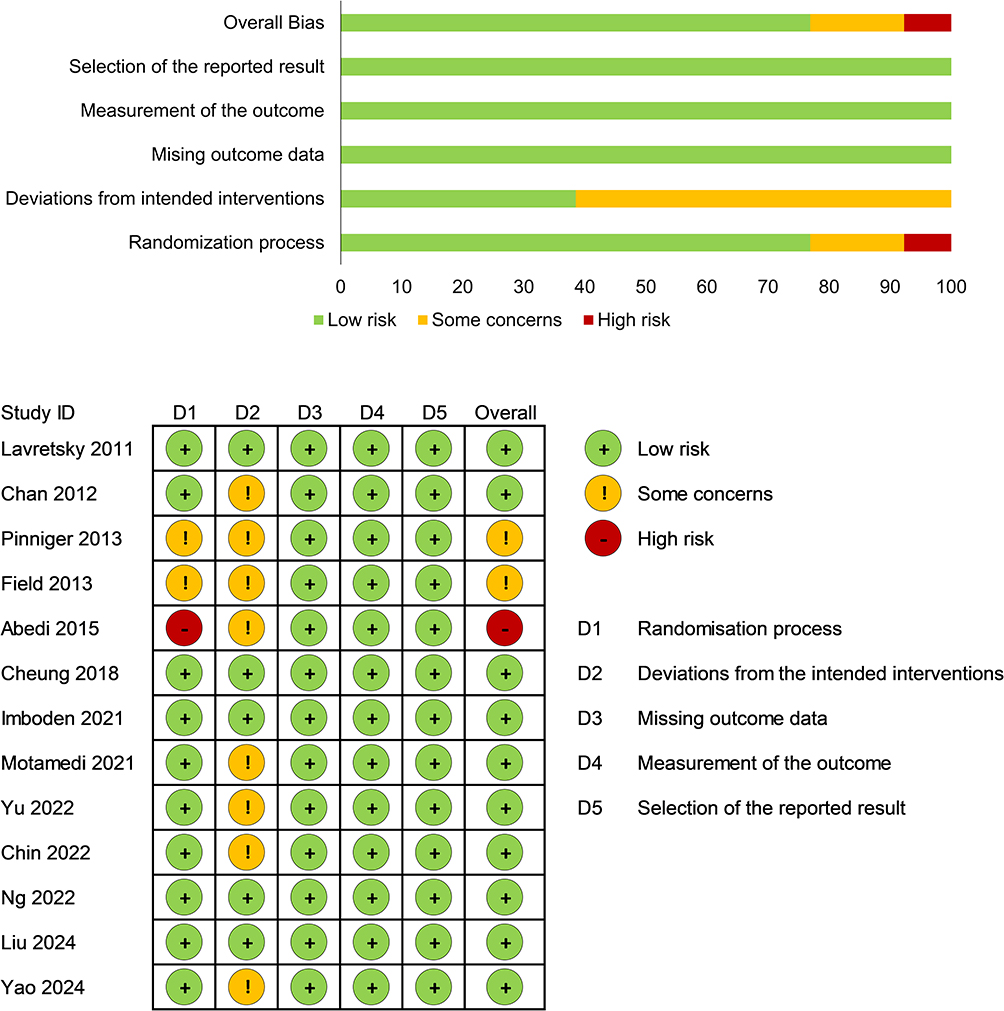 |
Figure 2 Bias of the included studies. |
It is important to note that participants blinding is unfeasible in these non-pharmacological intervention trials. First, members of aerobic exercise group were undoubtedly aware of the interventions they were receiving. Second, the measurements of most outcome were self-completion of scales before and after the interventions. Because of this, we believe that the non-double-blind design might not affect the quality of trials.
Effects of Aerobic Exercises at Different Intensities on Subjective Sleep Quality in Patients with Depression
The combined results for effects of aerobic exercises at different intensities on subjective sleep quality in people with depression are shown in Figure 3. Twelve trials recorded subjective sleep quality by self-reported scales.43,51–60,62 Based on a fixed-effects model, the meta-analysis demonstrated that aerobic exercise significantly improved subjective sleep quality in depressed patients [n = 894; SMD = −0.52, 95% CI = (−0.66, −0.38); p < 0.05]. The result of the random-effects model was consistent with that of the fixed-effects model, underscoring the robustness of the finding (Supplementary Figure S1). These studies exhibited moderate statistical heterogeneity (I2 = 39%).
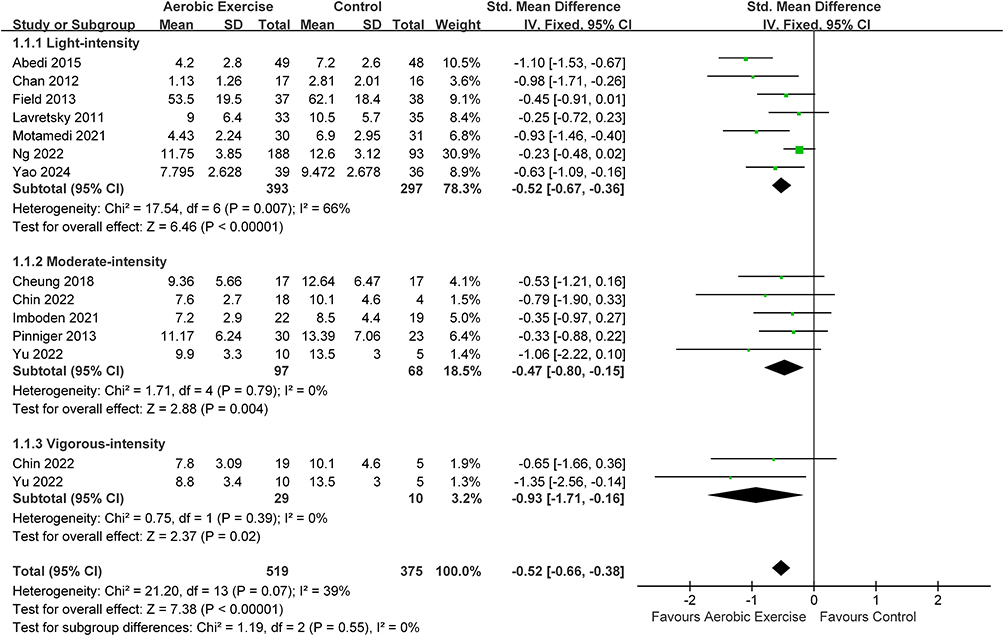 |
Figure 3 Meta-analysis results on the effects of different intensities aerobic exercise interventions on subjective sleep quality in people with depression. Abbreviations: SD, standard deviation; Std, standardized; IV, inverse variance; CI, confidence interval. |
Subgroup analyses showed that there was no significant difference among the three intensities in terms of the effects on subjective sleep quality (p = 0.54, I2 = 0%), suggesting that light [n = 690; SMD = −0.52, 95% CI = (−0.67, −0.36); p < 0.05], moderate [n = 165; SMD = −0.47, 95% CI = (−0.80, −0.15); p < 0.05], and vigorous-intensities [n = 39; SMD = −0.93, 95% CI = (−1.71, −0.16); p < 0.05] aerobic exercise can improve subjective sleep quality in depressed patients. Only the light-intensity group was highly heterogeneous (I2 = 66%).
The results of a sensitivity analysis showed that the data reported by Ng et al59 had a large effect on the overall combined effect (Supplementary Figure S2A). However, the original overall effect has not been reversed, so the results can be considered robust. Funnel plots appeared to reveal a slight publication bias (Supplementary Figure S3A), while no statistically significant publication bias was detected through Egger’s test (p = 0.112).
Together, these results suggest that aerobic exercises at different intensities can improve self-reported sleep quality in depressed patients.
Effects of Aerobic Exercises at Different Intensities on Objective Sleep Quality in Patients with Depression
The availability of studies on the effects of aerobic exercises at different intensities on objective sleep quality in people with depression was very sparse. Only three trials (one involving light-intensity,61 two of moderate-intensity,43,58 and one of vigorous intensity)58 were included in the meta-analysis. And, different measurement tools (polysomnography43,61 or accelerometers)58 were used in these trials. Therefore, we analyzed only the overall effect size to determine whether aerobic exercise can improve objective sleep quality.
The pooled results are shown in Figure 4. The combined results of this meta-analysis indicate that there is no evidence to suggest that aerobic exercise has a significant impact on objective sleep quality indicators in depressed patients, including sleep efficiency [n = 168; SMD = 0.14, 95% CI = (−0.46, 0.75); p = 0.64; I2=56%] (Figure 4A), total sleep time [n = 168; SMD = 0.30, 95% CI = (−0.03, 0.62) (Figure 4B); p = 0.07; I2=36%], and sleep onset latency [n = 168; SMD = −0.11, 95% CI = (−0.76, 0.54); p = 0.75; I2=62%] (Figure 4C). Total sleep time was analyzed using a fixed-effect model due to low heterogeneity, and the results were consistent with those from the random-effects model analysis (Supplementary Figure S4).
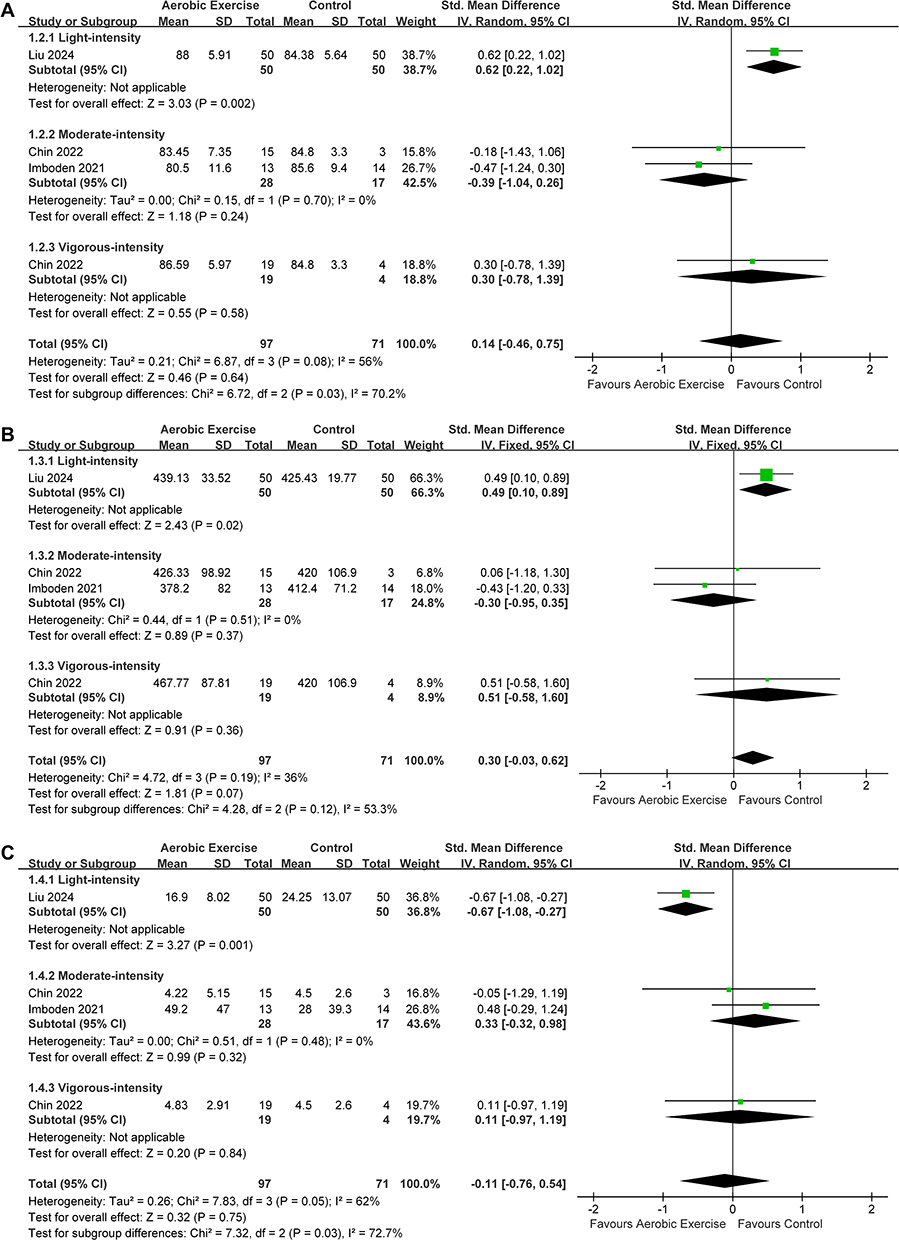 |
Figure 4 Meta-analysis results on the effects of different intensities aerobic exercise interventions on objective sleep quality in people with depression. Forest plots of objective sleep quality: (A) sleep efficiency, (B) total sleep time, (C) sleep onset latency. Abbreviations: SD, standard deviation; Std, standardized; IV, inverse variance; CI, confidence interval. |
Effects of Aerobic Exercises at Different Intensities on Depression Symptoms in Patients with Depression
Summarized results of the effects of aerobic exercises at different intensities on depression symptoms are shown in Figure 5. Thirteen trials included outcome indicators of depression symptoms, eight of which involved light-intensity,51–53,55,57,59,61,62 five of moderate-intensity,43,54,56,58,59 and two of vigorous-intensity.58,60 The meta-analysis showed that aerobic exercise interventions alleviated depression symptoms in depressed patients [n = 994; SMD = −0.70, 95% CI = (−0.93, −0.47); p < 0.05]. These studies showed a high level of heterogeneity (I2 = 60%). Sensitivity analyses revealed that the new combined effect remained constant after exclusion of any individual study for depression symptoms (Supplementary Figure S2B). No statistical (Egger’s test, p = 0.167) or visual (Supplementary Figure S3B) evidence of publication bias was observed.
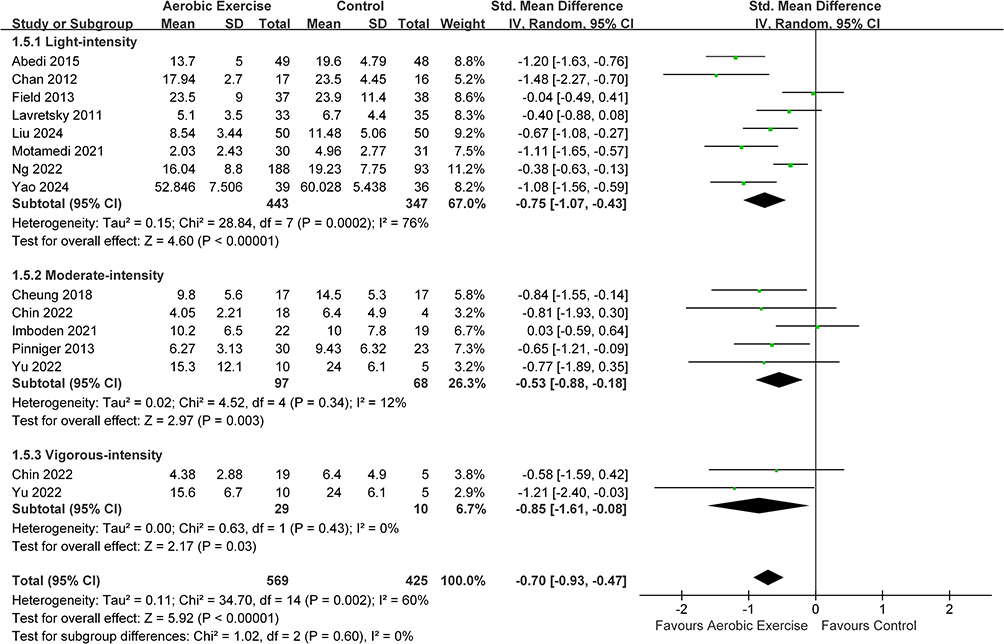 |
Figure 5 Meta-analysis results on the effects of different intensities aerobic exercise interventions on depression symptoms in people with depression. Abbreviations: SD, standard deviation; Std, standardized; IV, inverse variance; CI, confidence interval. |
Subgroup analyses of different exercise intensities showed that light- [n = 790; SMD = −0.75, 95% CI = (−1.07, −0.43); p < 0.05], moderate- [n = 165; SMD = −0.53, 95% CI = (−0.88, −0.18); p < 0.05], and vigorous-intensities [n = 39; SMD = −0.85, 95% CI = (−1.61, −0.08); p < 0.05] aerobic exercises significantly alleviated depression symptoms in depressed patients, and there was no significant difference among the three subgroups in terms of the effects on depression symptoms (p = 0.60, I2 = 0%). Only the light-intensity group had a high level of heterogeneity (I2 = 76%), suggesting that exercise intensity may be the main source of heterogeneity.
Effects of Aerobic Exercises at Different Intensities on Anxiety Symptoms in Patients with Depression
The summary result is shown in Figure 6. A meta-analysis of 9 trials (five involving light-intensity,51,53,55,61,62 four of moderate-intensity,54,56,58,60 and two of vigorous-intensity58,60) showed that aerobic exercise alleviated anxiety symptoms in depressed patients [n = 578; SMD = −0.47, 95% CI = (−0.74, −0.19); p < 0.05]. There was a statistically significant heterogeneity in these studies (I2 = 55%). The sensitivity analyses indicated that this merger effect was stable (Supplementary Figure S2C). Both funnel plot (Supplementary Figure S3C) and Egger’s test (p = 0.776) did not detect publication bias.
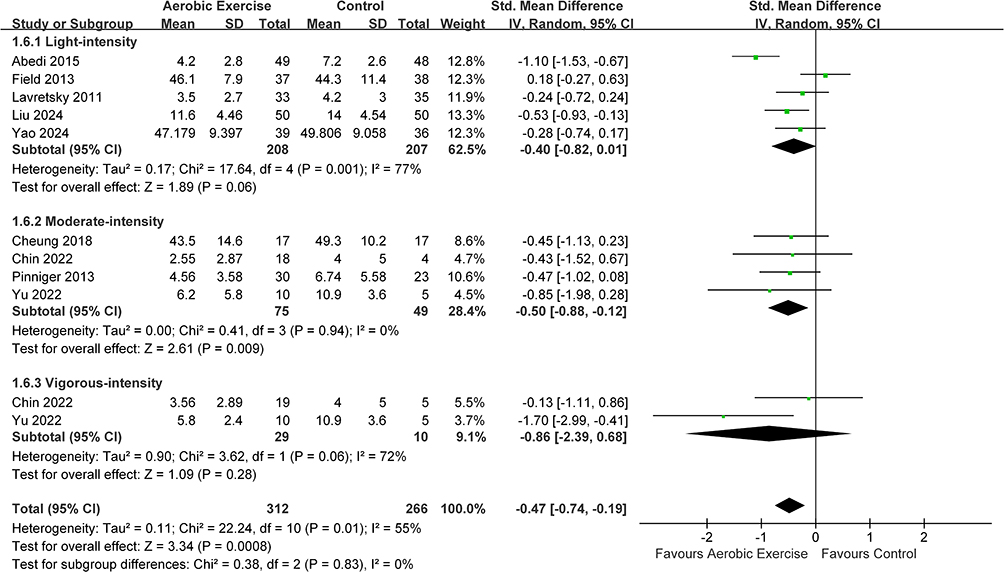 |
Figure 6 Meta-analysis results on the effects of different intensities aerobic exercise interventions on anxiety symptoms in people with depression. Abbreviations: SD, standard deviation; Std, standardized; IV, inverse variance; CI, confidence interval. |
Only moderate-intensity [n = 124; SMD = −0.50, 95% CI = (−0.88, −0.12); p < 0.05] significantly improved anxiety, and within-group heterogeneity was at a low level (I2=0%). In contrast, light [n = 415; SMD = −0.40, 95% CI = (−0.82, 0.01); p = 0.28] and vigorous-intensities [n = 39; SMD = −0.86, 95% CI = (−2.39, 0.68); p = 0.31] did not significantly improved anxiety and both had significant heterogeneity. However, subgroup analyses showed that there was no significant difference among the three intensities in terms of the effects on anxiety symptoms (p = 0.83, I2 = 0%).
Effects of Aerobic Exercises at Different Intensities on Quality of Life in Patients with Depression
There were only four trials with outcomes involving quality of life (two involving light-intensity,51,57 two of moderate-intensity,54,60 and one of vigorous-intensity60). Thus, we analyzed only the overall effect size to determine whether aerobic exercise can enhance quality of life. As shown in Figure 7, the results of the meta-analysis showed that aerobic exercise improved quality of life in depressed patients [n = 212; SMD = 0.64, 95% CI = (0.36, 0.92); p < 0.05]. The level of heterogeneity between these studies was low (I2=0%). The result of the random-effects model was consistent with that of the fixed-effects model (Supplementary Figure S5). The sensitivity analysis suggested that this combined result was robust (Supplementary Figure S2D). No statistical (Egger’s test, p = 0.425) or visual (Supplementary Figure S3D) evidence of publication bias was detected.
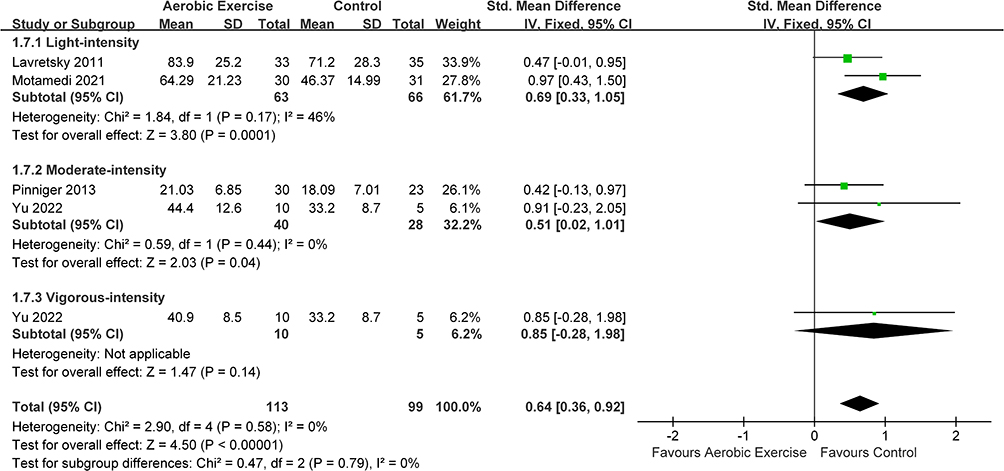 |
Figure 7 Meta-analysis results on the effects of different intensities aerobic exercise interventions on quality of life in people with depression. Abbreviations: SD, standard deviation; Std, standardized; IV, inverse variance; CI, confidence interval. |
Discussion
Principal Findings
Existing research shows that aerobic exercises at different intensities significantly improves subjective sleep quality in individuals with depression. Subgroup analysis further reveals no significant differences between light-, moderate-, and vigorous-intensities aerobic exercises. On the contrary, aerobic exercise had no significant effect on objective sleep quality. However, it is important to note that most studies did not report objective sleep data, leading to a limited sample size in our analysis. Additionally, inherent differences between the two measurement methods must be considered. Previous studies have shown significant discrepancies between subjective and objective sleep quality in patients with major depressive disorder.64,65 Subjective sleep quality is largely influenced by the patient’s feelings and can be affected by factors such as the severity of depression, personality, or age. In contrast, objective sleep quality, measured by external devices, reflects physiological changes during sleep. Most studies have used self-reported scales to assess subjective sleep quality, which is convenient and efficient for clinical screening and large-scale research. In contrast, measuring objective sleep quality requires specialized equipment, which is costly and complex to use, though it offers more accurate quantification. Therefore, the most comprehensive way to assess sleep quality is to integrate both subjective and objective measurements.66 Future research should include more randomized controlled trials that report objective sleep quality to further explore the effects of exercise interventions on both subjective and objective sleep quality in individuals with depression.
Additionally, we found that aerobic exercises at different intensities significantly improved depressive symptoms, anxiety, and quality of life in patients with depression. These findings are consistent with previous studies67–69 and support our hypothesis that sleep quality and emotional state are interrelated in individuals with depression. However, no significant differences were observed among the subgroups at different exercise intensities for these outcomes. This suggests that exercise intensity may not be a critical factor in the benefits of aerobic exercise for sleep quality among patients with depression, and further research incorporating other factors such as frequency and duration of exercise is warranted. Moreover, the fact that light-, moderate-, and vigorous-intensities aerobic exercises have similar effects holds certain significance. First, this is conducive to the promotion of exercise intervention, as low-intensity exercises are characterized by better adherence and are more easily carried out among patients with depression. Second, compared with the physiological responses that occur during moderate- and vigorous-intensities aerobic exercises (bicycling, treadmill exercise, dance, or walking), low-intensity aerobic exercise (tai chi and yoga) focuses more on coordination and cooperation of the body and mind, which results in more improvements in mental health in patients with depression.
Comparison with Other Studies
Numerous studies have shown that exercise improves both subjective and objective sleep quality in the general population.70–74 Emerging evidence suggests that traditional physical exercise (eg, walking, cycling) and mind-body exercise characterized by gentle exercise with coordination of the body (eg, yoga) significantly improved subjective sleep quality in adults compared with control group.72 While these findings provide a mechanistic framework, we caution that direct extrapolation to depressed individuals may be limited due to pathophysiological differences. Therefore, it is crucial to assess the effects of exercise on sleep quality in individuals with depression based on existing research. More specifically, further exploration is needed to identify the most effective forms and intensities of exercise for this population.
Two meta-analyses with similar objectives have been published. A previous network meta-analysis on the effects of exercise on sleep in unipolar depression patients reported that all exercise interventions, except moderate-intensity aerobic exercise (SMD: 0.31; 95% CI: 0.62, 0.00), were more effective than a passive control in improving sleep quality.38 In contrast, our results demonstrate that moderate-intensity aerobic exercise significantly improves subjective sleep quality. Another systematic review and meta-analysis on physical activity and sleep quality in major depressive disorder patients yielded results similar to ours.41 The above meta-analysis has some limitations which should be considered. First, their research samples were limited to MDD and results might not be generalizable to all patients with depression. Second, the exercise modalities included in the above meta-analysis were unrestricted in range. Third, the above meta-analysis did not examine differences at exercise intensity. Fourth, the above meta-analysis did not include objective sleep quality indicators. By comparison, we updated the included studies with all depression patients, included objective sleep quality indicators, and performed subgroup analyses based on exercise intensity.
Potential Mechanisms Underlying the Results
Raised level of the cytokine interleukin-6 was seen in the population with sleep disorder or depression.75,76 These findings suggested that there was an association between sleep disorder and depression, and this association was mediated by inflammatory factors. Numerous studies have confirmed that sleep disorder is a stressor that can increase levels of pro-inflammatory factors and induce depressive symptoms through a range of processes.77 First, elevated inflammatory signals alter the transport and metabolism of neurotransmitters that synergistically affect mood, including dopamine, glutamate, and serotonin.78 Chronic exposure to serotonin leads to the desensitization of serotonin 1A receptors, which may cause sleep disorder.79 Second, inflammation affects the growth and survival of neurons. Inflammatory factors contribute to oxidative stress, which can impair glial cells in mood-related brain regions.80 Third, inflammatory factors cause the dysregulation of glutamate, which leads to increased excitotoxicity and decreased production of brain-derived neurotrophic factor (BDNF).81 In addition to their effects on neural system, cytokines also facilitate the dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis.82,83 It has been observed that persistent sleep deprivation may lead to a significant reduction in pituitary adrenocorticotropic hormone response in rats exposed to a fearful environment.84 These dysfunctions in neurotransmission, neuron survival and neuroendocrine responsiveness have been implicated as potential neurobiological mechanisms of depression in humans.
It is well established that exercise has a specific regulatory effect on the immune response.85 Acute exercise typically induces a transient inflammatory response. In contrast to pathological inflammation, the upregulation of inflammatory factors produced by exercise is rapidly restored, accompanied by the production of anti-inflammatory substances, which in turn suppresses the inflammatory response. Long-term regular aerobic exercise has been demonstrated to reduce systemic inflammation through homeostatic adaptation.86 Regular aerobic exercise can also suppress neuroinflammation in brain and promote cognitive function.87 In addition, Imboden et al43 demonstrated that 6-week aerobic exercise intervention decreased HPA axis activity in patients with depression. This suggests that aerobic exercise may improve sleep quality and depressive symptoms by modulating HPA axis activity.
BDNF plays a key role in the pathophysiology of stress-related mood disorders.88 Subsequent studies have identified a significant reduction in plasma BDNF levels in both depressed patients and patients with sleep disorder.89,90 Physical exercise is regarded as a valuable method for regulating BDNF homeostasis. A study demonstrated that both endurance training and sprint interval training significantly elevated BDNF levels in the rat brain, accompanied by improvements in depression and anxiety.91 Further evidence indicates that elevated BDNF levels are associated with enhanced subjective sleep quality in patients with major depressive disorder who receive exercise as an adjunctive therapeutic intervention.92 Baduanjin exercise combined with behavioral therapy has also been reported to be effective in improving the mood and sleep status of post-stroke patients with depression, enhancing their ability to perform daily life and improving their quality of life.61 These beneficial effects were associated with increased levels of 5-hydroxytryptamine and BDNF and decreased serum levels of the pro-inflammatory factor IL-6.
Limitations of the Study
Our study has several limitations. First, some of the exercise forms used in the included studies differ from traditional aerobic exercise, such as mind-body practices like Tai Chi, Qigong, and yoga. These exercises emphasize specific postures, breathing techniques, and mind-body coordination, in contrast to aerobic endurance exercises (eg, running or cycling). As such, the differences between mind-body exercises and conventional aerobic exercise may extend beyond intensity alone. This heterogeneity in exercise modalities could influence the generalizability of our findings to standard aerobic exercise interventions. Second, during the screening process, studies involving serious comorbidities (eg, cancer) were excluded, although such patients often experience insomnia and depressive symptoms. While this decision may have minimized internal biases, it also limited the external validity of our findings. Third, in this meta-analysis, we conducted subgroup analyses based solely on exercise intensity and did not further explore other factors such as duration, frequency, and cycle of the intervention.
Conclusion
In conclusion, the findings of this systematic review and meta-analysis suggest that, with the exception of objective sleep quality, aerobic exercises at different intensities significantly improve subjective sleep quality, alleviate depressive and anxiety symptoms, and enhance quality of life in patients with depression. Subgroup analyses based on exercise intensity revealed no significant differences between light-, moderate-, and vigorous-intensities. These results reveal the potential benefits of aerobic exercise for depression, but also highlight the need for further investigation into factors such as exercise duration, frequency, and their impact on both subjective and objective sleep outcomes.
Data Sharing Statement
The data supporting the results are available upon reasonable request by contacting Dr. Li via email: [email protected].
Acknowledgments
We sincerely thank Mr. Hao Li and Dr. Shiyan Zhang for his assistance in the literature selection and data extraction.
Author Contributions
Jiaqi Liang: Conceptualization, Formal analysis, Investigation, Writing-original draft, Visualization.
Xuanzhen Pan: Investigation, Data Curation, Validation, Writing-original draft.
Li Zhao: Conceptualization, Methodology, Writing-Review & Editing, Supervision.
Yan Li: Conceptualization, Methodology, Writing-Review & Editing, Supervision, Project administration.
All authors approved the final version of the manuscript, agreed to submit it to this journal, and take responsibility for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (32000838); and the Chinese Universities Scientific Fund (2024JNPD002, 2023040).
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Tsuno N, Besset A, Ritchie K. Sleep and depression. J Clin Psychiatry. 2005;66(10):1254–1269. doi:10.4088/jcp.v66n1008
2. Paterson LM, Nutt DJ, Wilson SJ. NAPSAQ-1: national patient sleep assessment questionnaire in depression. Int J Psychiatry Clin Pract. 2009;13(1):48–58. doi:10.1080/13651500802450498
3. Park SC, Kim JM, Jun TY, et al. Prevalence and clinical correlates of insomnia in depressive disorders: the CRESCEND study. Psychiatry Invest. 2013;10(4):373–381. doi:10.4306/pi.2013.10.4.373
4. Soehner AM, Kaplan KA, Harvey AG. Prevalence and clinical correlates of co-occurring insomnia and hypersomnia symptoms in depression. J Affect Disord. 2014;167:93–97. doi:10.1016/j.jad.2014.05.060
5. Tavares VDO, de Sousa GM, Schuch FB, et al. Self-reported mood and lifestyle-related physical activity of young adults with major depressive disorder. Percept Mot Skills. 2024;131(2):489–513. doi:10.1177/00315125241226997
6. Steiger A, Pawlowski M. Depression and sleep. Int J Mol Sci. 2019;20(3):607. doi:10.3390/ijms20030607
7. Nelson KL, Davis JE, Corbett CF. Sleep quality: an evolutionary concept analysis. Nurs Forum. 2022;57(1):144–151. doi:10.1111/nuf.12659
8. Perez-Caballero L, Torres-Sanchez S, Romero-López-Alberca C, González-Saiz F, Mico JA, Berrocoso E. Monoaminergic system and depression. Cell Tissue Res. 2019;377(1):107–113. doi:10.1007/s00441-018-2978-8
9. Nakamaru-Ogiso E, Miyamoto H, Hamada K, Tsukada K, Takai K. Novel biochemical manipulation of brain serotonin reveals a role of serotonin in the circadian rhythm of sleep-wake cycles. Eur J Neurosci. 2012;35(11):1762–1770. doi:10.1111/j.1460-9568.2012.08077.x
10. Nechita F, Pîrlog MC, Chirita AL. Circadian malfunctions in depression - neurobiological and psychosocial approaches. Rom J Morphol Embryol. 2015;56(3):949–955.
11. Leerssen J, Blanken TF, Pozzi E, et al. Brain structural correlates of insomnia severity in 1053 individuals with major depressive disorder: results from the ENIGMA MDD Working Group. Transl Psychiatry. 2020;10(1):425. doi:10.1038/s41398-020-01109-5
12. Tahmasian M, Knight DC, Manoliu A, et al. Aberrant intrinsic connectivity of hippocampus and amygdala overlap in the fronto-insular and dorsomedial-prefrontal cortex in major depressive disorder. Front Hum Neurosci. 2013:7639. doi:10.3389/fnhum.2013.00639.
13. Bora E, Fornito A, Pantelis C, Yücel M. Gray matter abnormalities in major depressive disorder: a meta-analysis of voxel based morphometry studies. J Affect Disord. 2012;138(1–2):9–18. doi:10.1016/j.jad.2011.03.049
14. Xi MC, Fung SJ, Zhang JH, Sampogna S, Chase MH. The amygdala and the pedunculopontine tegmental nucleus: interactions controlling active (rapid eye movement) sleep. Exp Neurol. 2012;238(1):44–51. doi:10.1016/j.expneurol.2012.08.001
15. Dong L, Xie Y, Zou X. Association between sleep duration and depression in US adults: a cross-sectional study. Article J Affect Disord. 2022;296:183–188. doi:10.1016/j.jad.2021.09.075
16. Baglioni C, Battagliese G, Feige B, et al. Insomnia as a predictor of depression: a meta-analytic evaluation of longitudinal epidemiological studies. Rev J Affect Disord. 2011;135(1–3):10–19. doi:10.1016/j.jad.2011.01.011
17. Morita Y, Sasai-Sakuma T. Optimal total sleep duration per day to maintain health-related quality of life in male collegiate athletes: a cross-sectional study. J Sci Sport Exerc. 2023;5(4):360–368. doi:10.1007/s42978-022-00203-y
18. Irwin MR, Cole SW. Reciprocal regulation of the neural and innate immune systems. Nat Rev Immunol. 2011;11(9):625–632. doi:10.1038/nri3042
19. Miller AH, Raison CL. The role of inflammation in depression: from evolutionary imperative to modern treatment target. Nat Rev Immunol. 2016;16(1):22–34. doi:10.1038/nri.2015.5
20. Lind MJ, Hawn SE, Sheerin CM, et al. An examination of the etiologic overlap between the genetic and environmental influences on insomnia and common psychopathology. Depress Anxiety. 2017;34(5):453–462. doi:10.1002/da.22587
21. Hammerschlag AR, Stringer S, de Leeuw CA, et al. Genome-wide association analysis of insomnia complaints identifies risk genes and genetic overlap with psychiatric and metabolic traits. Nat Genet. 2017;49(11):1584–1592. doi:10.1038/ng.3888
22. Stein MB, McCarthy MJ, Chen CY, et al. Genome-wide analysis of insomnia disorder. Mol Psychiatry. 2018;23(11):2238–2250. doi:10.1038/s41380-018-0033-5
23. Fang H, Tu S, Sheng J, Shao A. Depression in sleep disturbance: a review on a bidirectional relationship, mechanisms and treatment. J Cell Mol Med. 2019;23(4):2324–2332. doi:10.1111/jcmm.14170
24. Plante DT. The evolving nexus of sleep and depression. Am J Psychiatry. 2021;178(10):896–902. doi:10.1176/appi.ajp.2021.21080821
25. Williams N, Simpson AN, Simpson K, Nahas Z. Relapse rates with long-term antidepressant drug therapy: a meta-analysis. Hum Psychopharmacol. 2009;24(5):401–408. doi:10.1002/hup.1033
26. Steinert C, Hofmann M, Kruse J, Leichsenring F. Relapse rates after psychotherapy for depression stable long-term effects? A meta-analysis. J Affect Disord. 2014;168:107–118. doi:10.1016/j.jad.2014.06.043
27. Carney CE, Harris AL, Friedman J, Segal ZV. Residual sleep beliefs and sleep disturbance following cognitive behavioral therapy for major depression. Depress Anxiety. 2011;28(6):464–470. doi:10.1002/da.20811
28. Lorenzo-Luaces L, Amsterdam JD, DeRubeis RJ. Residual anxiety may be associated with depressive relapse during continuation therapy of bipolar II depression. J Affect Disord. 2018;227:379–383. doi:10.1016/j.jad.2017.11.028
29. da Silva AHS, de Freitas LA, Shuhama R, et al. Family environment and depressive episode are associated with relapse after first-episode psychosis. J Psychiatr Ment Health Nurs. 2021;28(6):1065–1078. doi:10.1111/jpm.12735
30. Karp JF, Buysse DJ, Houck PR, Cherry C, Kupfer DJ, Frank E. Relationship of variability in residual symptoms with recurrence of major depressive disorder during maintenance treatment. Am J Psychiatry. 2004;161(10):1877–1884. doi:10.1176/appi.ajp.161.10.1877
31. Stanton R, Reaburn P. Exercise and the treatment of depression: a review of the exercise program variables. J Sci Med Sport. 2014;17(2):177–182. doi:10.1016/j.jsams.2013.03.010
32. Xie YM, Wu ZT, Sun LM, et al. The effects and mechanisms of exercise on the treatment of depression. Front Psychiatry. 2021:12705559. doi:10.3389/fpsyt.2021.705559.
33. Farris SG, Abrantes AM, Uebelacker LA, Weinstock LM, Battle CL. Exercise as a nonpharmacological treatment for depression. Psychiatr Ann. 2019;49(1):6–10. doi:10.3928/00485713-20181204-01
34. Euteneuer F, Dannehl K, Del Rey A, Engler H, Schedlowski M, Rief W. Immunological effects of behavioral activation with exercise in major depression: an exploratory randomized controlled trial. Transl Psychiatry. 2017;7(5):e1132. doi:10.1038/tp.2017.76
35. Silva LAD, Tortelli L, Motta J, et al. Effects of aquatic exercise on mental health, functional autonomy and oxidative stress in depressed elderly individuals: a randomized clinical trial. Clinics. 2019;74:e322. doi:10.6061/clinics/2019/e322
36. Micheli L, Ceccarelli M, D’Andrea G, Tirone F. Depression and adult neurogenesis: positive effects of the antidepressant fluoxetine and of physical exercise. Brain Res Bull. 2018;143:181–193. doi:10.1016/j.brainresbull.2018.09.002
37. Miller KJ, Gonçalves-Bradley DC, Areerob P, Hennessy D, Mesagno C, Grace F. Comparative effectiveness of three exercise types to treat clinical depression in older adults: a systematic review and network meta-analysis of randomised controlled trials. Ageing Res Rev. 2020;58100999. doi:10.1016/j.arr.2019.100999
38. Brupbacher G, Gerger H, Zander-Schellenberg T, et al. The effects of exercise on sleep in unipolar depression: a systematic review and network meta-analysis. Sleep Med Rev. 2021;59:101452. doi:10.1016/j.smrv.2021.101452
39. Li H, Su W, Cai J, Zhao L, Li Y. Effects of exercise of different intensities on withdrawal symptoms among people with substance use disorder: a systematic review and meta-analysis. Front Physiol. 2023;14:1126777. doi:10.3389/fphys.2023.1126777
40. Baron P, Hermand É, Elsworth-Edelsten C, et al. Sleep and subjective recovery in amateur trail runners after the ultra-trail du mont blanc® (UTMB®). J Sci Sport Exerc. 2023;5(2):123–129. doi:10.1007/s42978-021-00154-w
41. Khazaie H, Norouzi E, Rezaie L, Safari-Faramani R. Effect of physical activity on sleep quality in patients with major depression disorder: a systematic review and meta-analysis of randomized controlled trials. Curr Psychol. 2023;42(33):28846–28856. doi:10.1007/s12144-022-03810-8
42. Tolentino JC, Schmidt SL. DSM-5 criteria and depression severity: implications for clinical practice. Front Psych. 2018;9450. doi:10.3389/fpsyt.2018.00450
43. Imboden C, Gerber M, Beck J, et al. Aerobic exercise and stretching as add-on to inpatient treatment for depression have no differential effects on stress-axis activity, serum-BDNF, TNF-alpha and objective sleep measures. Brain Sci. 2021;11(4):411
44. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
45. Luo D, Wan X, Liu J, Tong T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res. 2018;27(6):1785–1805. doi:10.1177/0962280216669183
46. Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14:135. doi:10.1186/1471-2288-14-135
47. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. doi:10.1136/bmj.l4898.
48. Huedo-Medina TB, Sánchez-Meca J, Marín-Martínez F, Botella J. Assessing heterogeneity in meta-analysis: q statistic or I2 index? Psychol Methods. 2006;11(2):193–206. doi:10.1037/1082-989x.11.2.193
49. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–634. doi:10.1136/bmj.315.7109.629
50. Norton K, Norton L, Sadgrove D. Position statement on physical activity and exercise intensity terminology. J Sci Med Sport. 2010;13(5):496–502. doi:10.1016/j.jsams.2009.09.008
51. Lavretsky H, Alstein LL, Olmstead RE, et al. Complementary use of tai chi chih augments escitalopram treatment of geriatric depression: a randomized controlled trial. Am J Geriatr Psychiatry. 2011;19(10):839–850. doi:10.1097/JGP.0b013e31820ee9ef
52. Chan AS, Wong QY, Sze SL, Kwong PP, Han YM, Cheung MC. A Chinese Chan-based mind-body intervention for patients with depression. J Affect Disord. 2012;142(1–3):283–289. doi:10.1016/j.jad.2012.05.018
53. Field T, Diego M, Delgado J, Medina L. Tai chi/yoga reduces prenatal depression, anxiety and sleep disturbances. Complement Ther Clin Pract. 2013;19(1):6–10. doi:10.1016/j.ctcp.2012.10.001
54. Pinniger R, Thorsteinsson Einar B, Brown Rhonda F, McKinley P. Tango dance can reduce distress and insomnia in people with self-referred affective symptoms. Am J Dance Ther. 2013;35(1):
55. Abedi P, Nikkhah P, Najar S. Effect of pedometer-based walking on depression, anxiety and insomnia among postmenopausal women. Climacteric. 2015;18(6):841–845. doi:10.3109/13697137.2015.1065246
56. Cheung LK, L S. A randomized controlled trial on an aerobic exercise programme for depression outpatients. Sport Sci Health. 2018;14:173–181. doi:10.1007/s11332-017-0423-0
57. Motamedi N, Mostajabodaavati SR. Investigating the effect of home-based physical activity schedule on the quality of life, sleep quality, and mood of the elderly at risk of depression as compared to the control group. Adv Biomed Res. 2021;10:17. doi:10.4103/abr.abr_180_20
58. Chin EC, Yu AP, Leung CK, et al. Effects of Exercise Frequency and Intensity on Reducing Depressive Symptoms in Older Adults With Insomnia: a Pilot Randomized Controlled Trial. Front Physiol. 2022;13:863457. doi:10.3389/fphys.2022.863457
59. Ng SM, Yin MXC, Chan JSM, et al. Impact of mind-body intervention on proinflammatory cytokines interleukin 6 and 1β: a three-arm randomized controlled trial for persons with sleep disturbance and depression. Brain Behav Immun. 2022;99:166–176. doi:10.1016/j.bbi.2021.09.022
60. Yu DJ, Yu AP, Leung CK, et al. Comparison of moderate and vigorous walking exercise on reducing depression in middle-aged and older adults: a pilot randomized controlled trial. Eur J Sport Sci. 2022;23(6):1018–1027. doi:10.1080/17461391.2022.2079424
61. Liu Y, Chen C, Du H, Xue M, Zhu N. Impact of Baduanjin exercise combined with rational emotive behavior therapy on sleep and mood in patients with poststroke depression: a randomized controlled trial. Medicine. 2024;103(19):e38180. doi:10.1097/md.0000000000038180
62. Yao X, Xiong L, Ouyang Y, Wang H, Zhu L. Research on the intervention effect of five-element music combined with eight-section brocade on depression among medical students in higher vocational colleges. Front Psychol. 2024;15:1439713. doi:10.3389/fpsyg.2024.1439713
63. Pinniger R, Thorsteinsson EB, Brown RF, McKinley P. Tango dance can reduce distress and insomnia in people with self-referred affective symptoms (vol 35, pg 60, 2013). Correction. Am J Dance Ther. 2020;42(1):143–144. doi:10.1007/s10465-019-09319-1
64. Tsuchiyama K, Nagayama H, Kudo K, Kojima K, Yamada K. Discrepancy between subjective and objective sleep in patients with depression. Psychiatry Clin Neurosci. 2003;57(3):259–264. doi:10.1046/j.1440-1819.2003.01114.x
65. Kung PY, Chou KR, Lin KC, Hsu HW, Chung MH. Sleep disturbances in patients with major depressive disorder: incongruence between sleep log and actigraphy. Arch Psychiatr Nurs. 2015;29(1):39–42. doi:10.1016/j.apnu.2014.09.006
66. Chen Y, Zhou E, Wang Y, Wu Y, Xu G, Chen L. The past, present, and future of sleep quality assessment and monitoring. Brain Res. 2023;1810:148333. doi:10.1016/j.brainres.2023.148333
67. Schuch FB, Vancampfort D, Rosenbaum S, Richards J, Ward PB, Stubbs B. Exercise improves physical and psychological quality of life in people with depression: a meta-analysis including the evaluation of control group response. Psychiatry Res. 2016;241:47–54. doi:10.1016/j.psychres.2016.04.054
68. Morres ID, Hatzigeorgiadis A, Stathi A, et al. Aerobic exercise for adult patients with major depressive disorder in mental health services: a systematic review and meta-analysis. Depress Anxiety. 2019;36(1):39–53. doi:10.1002/da.22842
69. Chen C, Du S, Shao Q, et al. The effects of aerobic exercise for depression: an umbrella review of systematic reviews and meta-analyses. J Bodyw Mov Ther. 2024;40:2161–2172. doi:10.1016/j.jbmt.2024.10.068
70. Kredlow MA, Capozzoli MC, Hearon BA, Calkins AW, Otto MW. The effects of physical activity on sleep: a meta-analytic review. J Behav Med. 2015;38(3):427–449. doi:10.1007/s10865-015-9617-6
71. Lang C, Kalak N, Brand S, Holsboer-Trachsler E, Pühse U, Gerber M. The relationship between physical activity and sleep from mid adolescence to early adulthood. A systematic review of methodological approaches and meta-analysis. Sleep Med Rev. 2016;28:32–45. doi:10.1016/j.smrv.2015.07.004
72. Xie Y, Liu S, Chen X-J, Yu -H-H, Yang Y, Wang W. Effects of exercise on sleep quality and insomnia in adults: a systematic review and meta-analysis of randomized controlled trials. Review Front Psychiatry. 2021;12664499. doi:10.3389/fpsyt.2021.664499
73. Zhou XJ, Kong Y, Yu BB, Shi SN, He H. Effects of exercise on sleep quality in general population: meta-analysis and systematic review. Sleep Med. 2025;125:1–13. doi:10.1016/j.sleep.2024.10.036
74. Collins BEG, Hartmann TE, Marino FE, Skein M. A comparison of acute high- and moderate-intensity exercise on cardio- metabolic function and sleep among shift workers. J Sci Sport Exerc. 2024;6(1):35–43. doi:10.1007/s42978-022-00212-x
75. Słuzewska A, Rybakowski JK, Laciak M, Mackiewicz A, Sobieska M, Wiktorowicz K. Interleukin-6 serum levels in depressed patients before and after treatment with fluoxetine. Ann N Y Acad Sci. 1995;762:474–476. doi:10.1111/j.1749-6632.1995.tb32372.x
76. Vgontzas AN, Zoumakis M, Bixler EO, et al. Impaired nighttime sleep in healthy old versus young adults is associated with elevated plasma interleukin-6 and cortisol levels: physiologic and therapeutic implications. J Clin Endocrinol Metab. 2003;88(5):2087–2095. doi:10.1210/jc.2002-021176
77. Lucassen PJ, Meerlo P, Naylor AS, et al. Regulation of adult neurogenesis by stress, sleep disruption, exercise and inflammation: Implications for depression and antidepressant action. Eur Neuropsychopharmacol. 2010;20(1):1–17. doi:10.1016/j.euroneuro.2009.08.003
78. Capuron L, Miller AH. Immune system to brain signaling: neuropsychopharmacological implications. Pharmacol Ther. 2011;130(2):226–238. doi:10.1016/j.pharmthera.2011.01.014
79. Roman V, Walstra I, Luiten PG, Meerlo P. Too little sleep gradually desensitizes the serotonin 1A receptor system. Sleep. 2005;28(12):1505–1510.
80. Leonard B, Maes M. Mechanistic explanations how cell-mediated immune activation, inflammation and oxidative and nitrosative stress pathways and their sequels and concomitants play a role in the pathophysiology of unipolar depression. Neurosci Biobehav Rev. 2012;36(2):764–785. doi:10.1016/j.neubiorev.2011.12.005
81. Eyre H, Baune BT. Neuroplastic changes in depression: a role for the immune system. Psychoneuroendocrinology. 2012;37(9):1397–1416. doi:10.1016/j.psyneuen.2012.03.019
82. Pace TW, Hu F, Miller AH. Cytokine-effects on glucocorticoid receptor function: relevance to glucocorticoid resistance and the pathophysiology and treatment of major depression. Brain Behav Immun. 2007;21(1):9–19. doi:10.1016/j.bbi.2006.08.009
83. Stetler C, Miller GE. Depression and hypothalamic-pituitary-adrenal activation: a quantitative summary of four decades of research. Psychosom Med. 2011;73(2):114–126. doi:10.1097/PSY.0b013e31820ad12b
84. Novati A, Roman V, Cetin T, et al. Chronically restricted sleep leads to depression-like changes in neurotransmitter receptor sensitivity and neuroendocrine stress reactivity in rats. Sleep. 2008;31(11):1579–1585. doi:10.1093/sleep/31.11.1579
85. Nieman DC, Wentz LM. The compelling link between physical activity and the body’s defense system. J Sport Health Sci. 2019;8(3):201–217. doi:10.1016/j.jshs.2018.09.009
86. de Lemos ET, Pinto R, Oliveira J, et al. Differential effects of acute (extenuating) and chronic (training) exercise on inflammation and oxidative stress status in an animal model of type 2 diabetes mellitus. Mediators Inflamm. 2011;2011:253061. doi:10.1155/2011/253061
87. Guo Y, Yan M, Li L, Zhao L, Li Y. Treadmill exercise prevents cognitive impairments in adolescent intermittent ethanol rats by reducing the excessive activation of microglia cell in the hippocampus. Int J Mol Sci. 2022;23(23). doi:10.3390/ijms232314701
88. Schmitt K, Holsboer-Trachsler E, Eckert A. BDNF in sleep, insomnia, and sleep deprivation. Ann Med. 2016;48(1–2):42–51. doi:10.3109/07853890.2015.1131327
89. Martinowich K, Manji H, Lu B. New insights into BDNF function in depression and anxiety. Nat Neurosci. 2007;10(9):1089–1093. doi:10.1038/nn1971
90. Giese M, Unternährer E, Hüttig H, et al. BDNF: an indicator of insomnia? Mol Psychiatry. 2014;19(2):151–152. doi:10.1038/mp.2013.10
91. TaheriChadorneshin H, Cheragh-Birjandi S, Ramezani S, Abtahi-Eivary SH. Comparing sprint and endurance training on anxiety, depression and its relation with brain-derived neurotrophic factor in rats. Behav Brain Res. 2017;329:1–5. doi:10.1016/j.bbr.2017.04.034
92. Gourgouvelis J, Yielder P, Clarke ST, Behbahani H, Murphy BA. Exercise leads to better clinical outcomes in those receiving medication plus cognitive behavioral therapy for major depressive disorder. Front Psychiatry. 2018;9:37. doi:10.3389/fpsyt.2018.00037
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Efficacy and Safety of Acupuncture for Depression-Related Insomnia: Protocol for a Systematic Review and Meta-Analysis
Hu H, Li Z, Cheng Y, Gao H
Journal of Pain Research 2022, 15:1939-1947
Published Date: 13 July 2022
An Evidence-Based Nursing Intervention Decreases Anxiety, Depression, Sleep Quality and Somatic Symptoms of Patients with Acute Ischemic Stroke
Gao WJ, Bao WJ, Sun SJ
Neuropsychiatric Disease and Treatment 2022, 18:2443-2451
Published Date: 25 October 2022
Relationship Between Physical Exercise and Cognitive Impairment Among Older Adults with Type 2 Diabetes: Chain Mediating Roles of Sleep Quality and Depression
Zhang H, Zhang Y, Sheng S, Xing Y, Mou Z, Zhang Y, Shi Z, Yu Z, Gao Q, Cai W, Jing Q
Psychology Research and Behavior Management 2023, 16:817-828
Published Date: 17 March 2023
Correlation Analysis Between Disease Activity and Anxiety, Depression, Sleep Disturbance, and Quality of Life in Patients with Inflammatory Bowel Disease
Yu R, Liu C, Zhang J, Li J, Tian S, Ding F, Liu Z, Wang T, Liu Z, Jiang C, Shi J, Wu K, Dong W
Nature and Science of Sleep 2023, 15:407-421
Published Date: 26 May 2023
The Correlation Between Night Shift Work Schedules, Sleep Quality, and Depression Symptoms
Alreshidi SM, Rayani AM
Neuropsychiatric Disease and Treatment 2023, 19:1565-1571
Published Date: 7 July 2023