Back to Journals » Journal of Pain Research » Volume 19
Effect of the Evidence-Based and Multidisciplinary Pain Management Program in Patients After Laparoscopic Hepatectomy: A Quasi-Experimental Study
Authors Song X ![]() , Liu Y
, Liu Y ![]() , Zou J, Zhang D
, Zou J, Zhang D ![]() , Bai T, Han Z
, Bai T, Han Z ![]() , Wang Y
, Wang Y ![]()
Received 16 November 2025
Accepted for publication 16 February 2026
Published 24 February 2026 Volume 2026:19 582027
DOI https://doi.org/10.2147/JPR.S582027
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Karina Gritsenko
Xiuxiu Song,1 Yuping Liu,1 Jinnan Zou,2 Dan Zhang,2 Ting Bai,1 Zhengxiang Han,3 Yuqin Wang1
1Nursing Department, Affiliated Hospital of Xuzhou Medical University, XuZhou, JiangSu, People’s Republic of China; 2General Surgery, Affiliated Hospital of Xuzhou Medical University, XuZhou, JiangSu, People’s Republic of China; 3Department of Oncology, Affiliated Hospital of Xuzhou Medical University, XuZhou, JiangSu, People’s Republic of China
Correspondence: Yuqin Wang, Nursing department, The Affiliated Hospital of Xuzhou Medical University, No. 99 Huaihai West Road, Quanshan District, Xuzhou City, Jiangsu Province, People’s Republic of China, Tel +86 13813285927, Email [email protected] Zhengxiang Han, Department of Oncology, The Affiliated Hospital of Xuzhou Medical University, No. 99 Huaihai West Road, Quanshan District, Xuzhou City, Jiangsu Province, People’s Republic of China, Tel +86 13852102216, Email [email protected]
Objective: The study was to explore the clinical effect of the Evidence-Based and Multidisciplinary pain management program for patients after hepatectomy. It examined the program’s impacts on postoperative pain, active pain, quality of life, and satisfaction with pain control.
Methods: A quasi-experimental study was conducted at the Affiliated Hospital of Xuzhou Medical University from May 2024 to April 2025. Fifty-seven patients were enrolled to the experimental (n = 29) and control (n = 28) group. The experimental group was provided evidence-based pain management program by the Acute Pain Service Team. The primary outcome was pain level measured using The Numerical Rating Scale scores. Data were harvested at at the time points of transferring to the ward after surgery, 4 h, 12 h, 24 h, 48 h and 72 h after operation. Secondary outcomes were the Four Grade Functional Activity Score, the Houston Pain Outcome Instrument (HPOI) and quality of life at discharge.
Results: Lower NRS scores were observed in the experimental group compared to the control group at 4 h (t = − 3.979, P < 0.001), 12 h (t = − 2.426, P = 0.019), 24 h (t = − 4.192, P < 0.001), 48 h (t = − 2.924, P = 0.005) and 72 h (t = − 2.797, P = 0.007) after operation. Significant between-group differences were found in the impact of pain on deep breathing at 12 h (z = − 3.472, P = 0.001), 24 h (z = − 2.217, P = 0.027), 48 h (z = − 2.316, P = 0.021), and 72 h (z = − 2.166, P = 0.030), coughing at 24 h (z = − 2.446, P = 0.014), 48 h (z = − 2.803, P = 0.005), and 72 h (z = − 2.580, P = 0.010), turning over at 48 h (z = − 2.639, P = 0.008) and 72 h (z = − 2.493, P = 0.013), and getting out of bed for activities at 48 h (z = − 2.205, P = 0.027) and 72 h (z = − 3.151, P = 0.002) after operation. The experimental group showed significant differences from the control group in all dimensions of HPOI. There were no differences regarding psychological and social functions.
Conclusion: The Evidence-Based and Multidisciplinary pain management program improved postoperative pain, reduced impact of pain on functional activities, and enhanced satisfaction with pain control, but failed to improve psychological and social functions.
Keywords: a quasi-experimental study, hepatectomy, laparoscopy, liver cancer, pain, pain management
Introduction
Liver cancer is one of the malignant tumors with high mortality worldwide, and surgical resection is the main treatment.1 With the development of minimally invasive techniques, laparoscopic hepatectomy (LH) has gradually been widely used in clinical practice due to its advantages such as less trauma, quick recovery, and fewer postoperative complications. However, even though LH is a minimally invasive surgery, patients still experience postoperative pain. This is mainly related to the following factors: the extensive surgical scope, deep tissue damage (such as diaphragm traction, intercostal nerve stimulation), the diaphragmatic reflex caused by intraoperative carbon dioxide pneumoperitoneum, and the retention of postoperative drainage tubes. In a study2 comparing the analgesic effect of intrathecal morphine, the incidence of moderate to severe pain within 24 hours after surgery in the LH group was 16.1%, significantly lower than 64.3% in the open surgery group. Although the overall pain level of patients undergoing LH is relatively mild, standardized pain management is still needed.
Postoperative pain can trigger multiple system adverse reactions, including physiological, psychological and behavioral reactions.3,4 It increases the risk of cardiovascular disease, inhibiting respiratory and immune function, and may also lead to anxiety, depression and other psychological problems, and even develop into chronic pain, which seriously affects early rehabilitation and quality of life.5,6 Therefore, effective pain management is particularly important and a key to the success of an enhanced recovery after surgery (ERAS) program.7
However, the current clinical practice of pain management after hepatectomy still faces many challenges. On the one hand, pain management programs often have some problems such as insufficient standardization, significant individual differences, and inconsistent compliance in execution.8 Different medical institutions and even different doctors adopt significantly different choices of analgesic drugs, dosages, administration routes, and combination strategies for multimodal analgesia. There is a lack of unified, efficient, and evidence-based best practice guidelines based on high-quality research.9–11 On the other hand, there may also be deficiencies in the attention given by medical staff to pain assessment, as well as in their understanding and application of new pain relief techniques and concepts.12 This could lead to an increase in the incidence of insufficient pain relief for some patients or adverse reactions related to pain medication (such as nausea, vomiting, intestinal paralysis, excessive sedation, and respiratory depression).
In this context, evidence-based practice provides a scientific approach to addressing these issues. Previously, we have developed a perioperative pain management strategy after hepatectomy based on evidence-based evidence and the delphi method.13 This study aims to verify the clinical effectiveness of this strategy in patients undergoing laparoscopic hepatectomy by a quasi-experimental design, focusing on postoperative pain, including pain level, pain impact on functional activities, and satisfaction with pain control, and to provide a basis for further promoting a standardized and individualized pain management pathway.
Methods
Study Design
A quasi-experimental and non-synchronized design was used. This study was approved by the medical ethics committee of the Affiliated Hospital of Xuzhou Medical University (decision number: XYFY2024-KL111-01) and registered in the China clinical trial registry (trial number: ChiCTR2400087506). This study complies with the Declaration of Helsinki.
The study was conducted in the department of general surgery of the Affiliated Hospital of Xuzhou Medical University, which mainly treated patients with liver, gallbladder and thyroid diseases. After admission to the ward, participants were screened by the research assistant, and the patients who met the criteria for scheduling were further recruited. Voluntary participation, anonymity, and confidentiality were ensured throughout the study. All eligible participants were informed that personal data will not be disclosed, and they signed informed consent. During the study, any participant had the right to choose to withdraw from the study.
Study Participants
To prevent diffusion of the treatment, data from the experimental group were collected after those of the control group. This study used convenience sampling. Study participants were enrolled from May 14, 2024, to April 10, 2025. The subjects enrolled in the first stage (May 14, 2024, to October 31, 2024) were assigned to the control group and those from the second stage (November 1, 2024, to April 10, 2025) to the experimental group.
The inclusion criteria in the study were as follows: (1) aged ≥18 years old; (2) primary liver cancer diagnosed by pathological examination; (3) patients who underwent laparoscopic hepatectomy for liver cancer; (4) patients who were conscious and able to communicate. Patients with any of the following conditions were excluded: (1) patients with cancer metastasis to other parts; (2) patients who recently used antidepressant medications; (3) patients with liver abscess or cardiopulmonary dysfunction; (4) pain caused by other diseases. Patients would be withdrawn if they met any of the following criteria: (1) having postoperative complications, such as infection, bleeding, liver failure, etc, which led patients unable to continue to participate in the study; (2) having strict requirements, such as frequent assessment and questionnaire survey, which made patients feel inconvenient and chose to quit; (3) quitting voluntarily.
The NRS scores were the main indicator. According to the results of Ke et al,14 the average score of NRS of the experimental and control group at 24 h after operation was 3.3 ± 0.6 and 2.8 ± 0.4, respectively. With alpha (α) level of 0.05, and a statistical power of 0.80, a minimum of 28 participants (14 participants per group) will be required for the trial. Considering an attrition rate of 20%, at least 41 participants were included. PASS 15 software was used to calculate the sample size.
A total of 62 participants (32 in the experimental group and 30 in the control group) were recruited. During the study, one participant did not accept the intervention allocation, and four participants withdrew from the study due to being admitted to ICU or disease progression or voluntary withdrawal. Thus, the final analysed data were from 57 total participants (Figure 1), 29 in the experimental group, 28 in the control group.
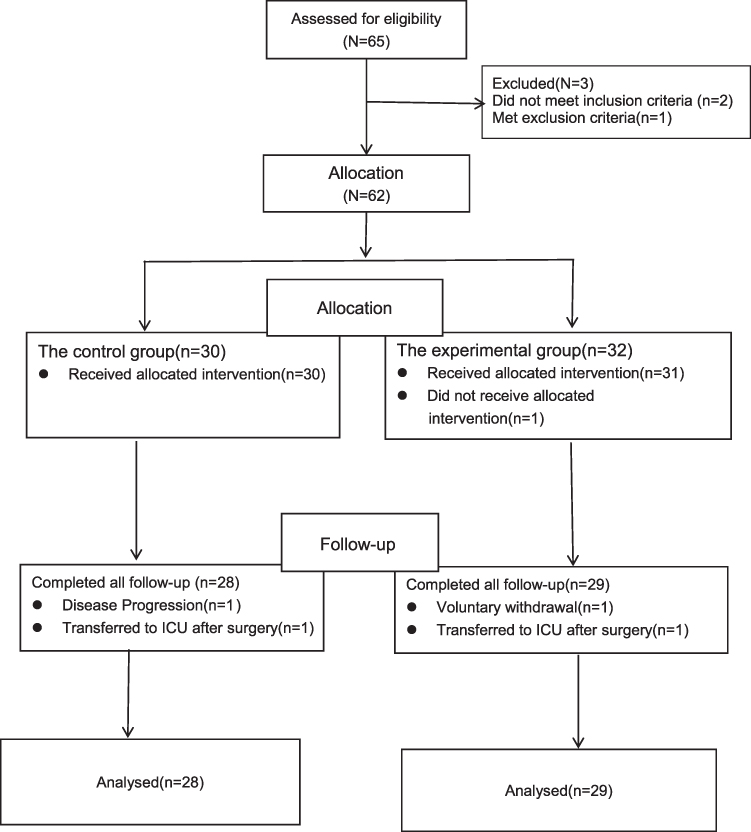 |
Figure 1 Flow diagram of study. |
Intervention
Experimental Group
Establishment and Implementation of the Acute Pain Service Team (APST)
An interdisciplinary Acute Pain Service Team (APST) was formally established and activated exclusively for the experimental group, serving as the core implementer of the intervention.
- Team Composition and Responsibilities: Led by the Director of General Surgery (overall supervision and quality control) and Head Nurse (staffing, training coordination, and workflow management). Core members included pain specialists, attending surgeons, medical oncologists, anesthesiologists, bedside nurses, clinical pharmacists, rehabilitation therapists, and psychologists.
- Standardized Operational Mechanisms: (1) A dedicated WeChat group was used for real-time communication and issue resolution. (2) Biweekly theoretical and skills training sessions were conducted, covering acute pain management guidelines, multimodal analgesia protocols, and psychological intervention techniques. Quarterly competency assessments ensured proficiency among team members. (3) Fidelity Monitoring: The Head Nurse audited 20% of patient records daily to verify adherence to the intervention protocol. Deviations were reviewed and addressed in biweekly team meetings. (4) Standardized checklists were utilized for all procedures to ensure consistency across providers and patients.
Multimodal Perioperative Pain Management Pathway (Admission to Discharge)
The APST delivered a structured pain management pathway from admission to discharge, as detailed in Table 1. Key components included:
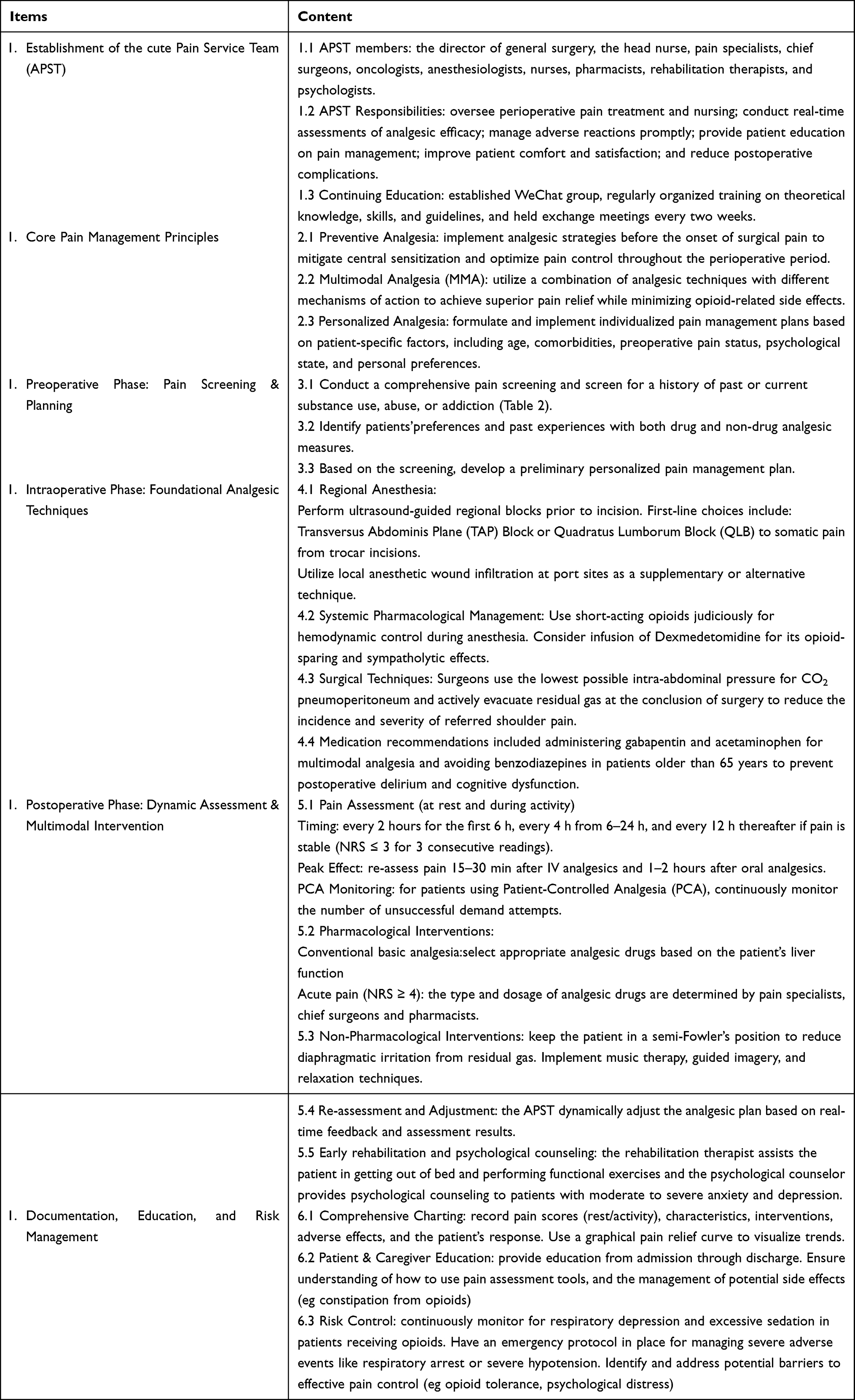 |
Table 1 Pain Management Program Based on Evidence Summary and Delphi Study for Patients After Hepatectomy |
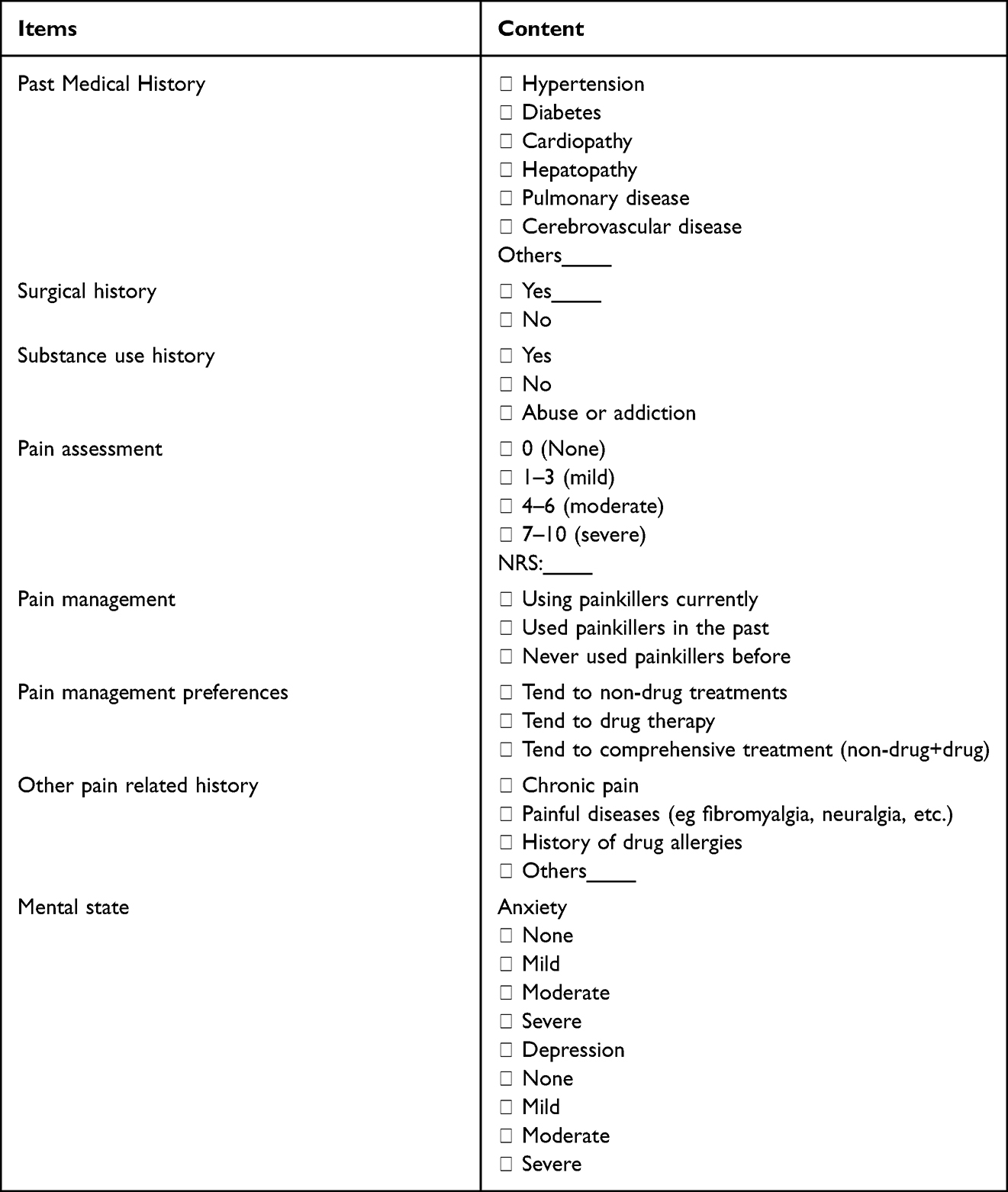 |
Table 2 Preoperative Pain Screening Form |
Preoperative Phase (Admission to Surgery Day)
- Pain Screening and Assessment: All patients completed a standardized preoperative pain screening questionnaire (Table 2) to identify risk factors (eg chronic pain history, opioid use). An anesthesiologist then performed a targeted pain consultation (Table 3) to evaluate pain sensitivity and develop an individualized analgesia plan.
- Patient Education: Patients and caregivers received standardized education on the NRS, patient-controlled analgesia (PCA) pump use, and the multimodal analgesia protocol.
- Preemptive Analgesia: Oral gabapentin and celecoxib were administered 1 hour preoperatively to reduce central sensitization.
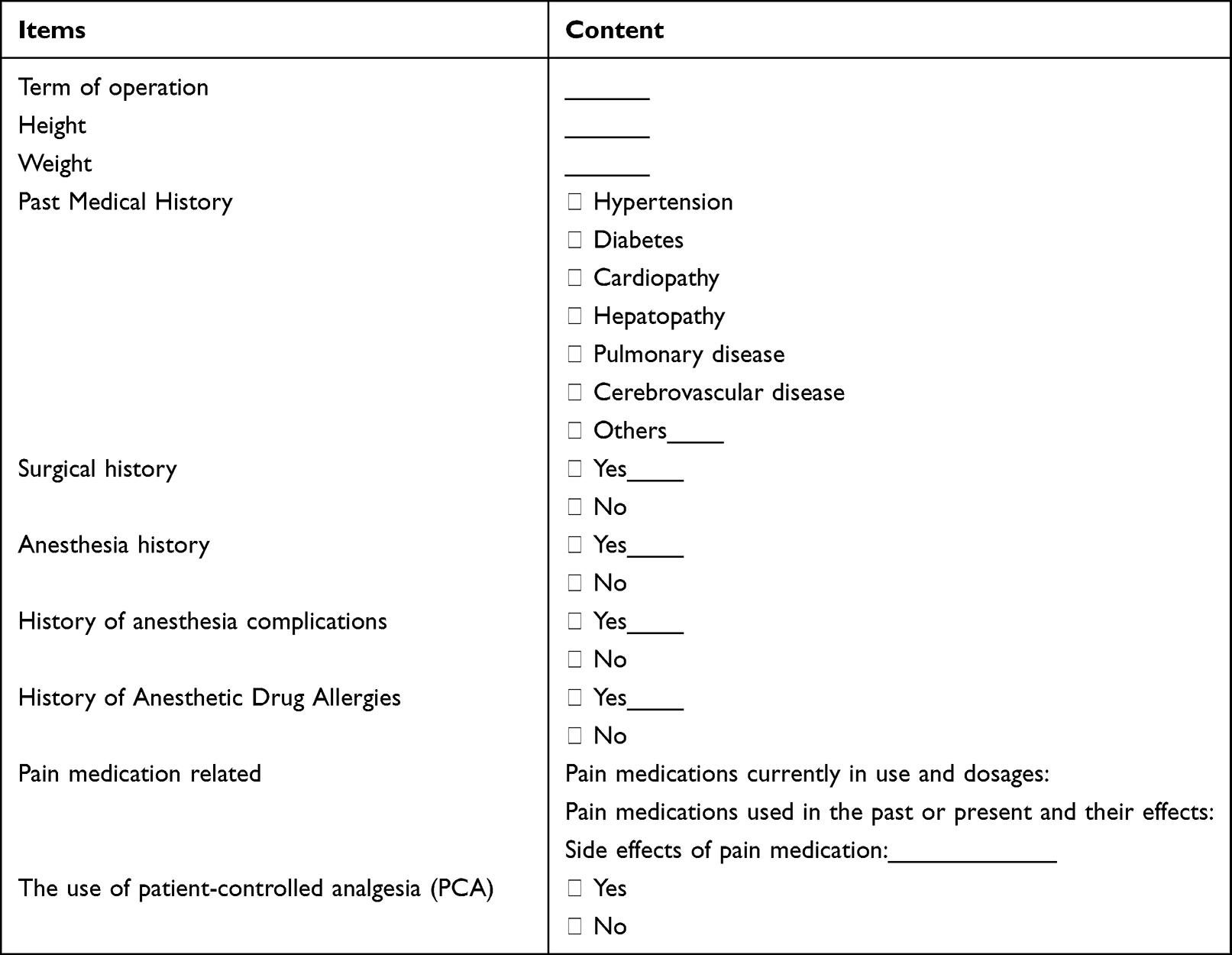 |
Table 3 Preoperative Pain Related Visit Form for Anesthesia |
Intraoperative Phase
- Ultrasound-Guided Regional Analgesia: Transversus abdominis plane (TAP) block combined with quadratus lumborum block (QLB) was performed to provide somatic analgesia.
- Opioid-Sparing Strategy: A low-dose remifentanil infusion was combined with dexmedetomidine to minimize intraoperative opioid exposure.
Postoperative Phase (Post-op to Discharge)
- Dynamic Pain Assessment: Pain was assessed every 4 hours using the NRS postoperatively, and 15–60 minutes after analgesic intervention (Figure 2). The intensity, nature, location, occurrence frequency, and associated symptoms of pain were recorded in detail for each assessment.
- Multimodal Analgesia: A standardized protocol was implemented, combining PCA, scheduled oral acetaminophen and gabapentin, and rescue analgesia for breakthrough pain.
- Non-Pharmacological Interventions: Bedside nurses implemented early mobilization in a semi-Fowler’s position, breathing exercises, and distraction techniques.
- Psychological Support: Psychologists delivered psychological counseling to address anxiety and pain catastrophizing.
- Early Rehabilitation: Rehabilitation therapists initiated functional exercises 24 hours postoperatively to reduce immobility-related pain.
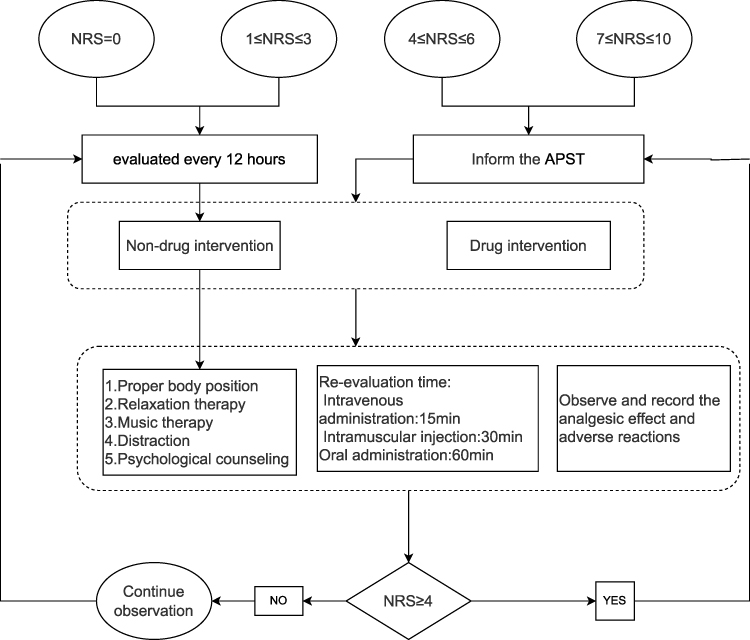 |
Figure 2 The dynamic assessment and management of pain. |
Discharge Transition
- A post-discharge pain management plan was provided, including oral analgesic prescriptions and a follow-up schedule.
- Patients were instructed to maintain a pain diary to track pain scores and medication use.
Control Group
Patients in the control group received standardized routine pain treatment and nursing care delivered by attending physicians and ward nurses.
Preoperative Care
Routine preoperative health education was provided, including a brief introduction to the Numerical Rating Scale (NRS) for pain assessment and basic non-pharmacological pain interventions. No dedicated pain risk screening, stratified assessment, or individualized analgesia planning was implemented for the patients.
Postoperative Care
- Vital Sign and Pain Monitoring: Routine postoperative vital sign observation was performed, and pain assessment was conducted systematically every 4 hours using the NRS. The intensity, nature, location, occurrence frequency, and associated symptoms of pain were recorded in detail for each assessment.
- Analgesic Intervention Protocol: For patients with an NRS score ≥4, ward nurses would immediately notify the attending physician, who then conducted a comprehensive clinical assessment and formulated symptomatic analgesic regimens. Non-steroidal anti-inflammatory drugs and opioids were routinely administered as the first-line analgesic medications, with adjunctive non-pharmacological interventions (eg music therapy, psychological counseling) implemented as appropriate based on clinical practice.
- Post-intervention Re-evaluation and Documentation: Pain intensity was re-assessed at 30 or 60 minutes after the implementation of any analgesic intervention. All processes, including pain assessment, analgesic administration, intervention implementation and re-evaluation results, were recorded in detail in the medical records.
Measurements
Two independent evaluators were trained and examined before participating in the study.
Baseline Data Collection
Sociodemographic characteristics (eg age, gender, marital status, education level, economic status), clinical characteristics (eg smoking status, alcohol status, presence of comorbidity, child-pugh and pain score) and laboratory indexes (eg liver function indexes and tumor markers) were obtained and recorded using a prepared collection form. All participants were anonymized and gave a specific ID.
Numerical Rating Scale (NRS)
NRS is used to evaluate the pain level, and is marked on a scale of 0 to 10, with 0 indicating no pain and 10 indicating the most pain. Patients were asked to choose a number that represented their pain level. This study only showed the NRS scores at the time points of transferring to the ward after surgery (T0), 4 h (T1), 12 h (T2), 24 h (T3), 48 h (T4) and 72 h (T5) after operation.
Four Grade Functional Activity Score (FAS)
Four Grade FAS is used to evaluate the impact of pain on functional activities during deep breathing, coughing, turning over and getting out of bed. Specific Content is as shown in Table 4. Cronbach’s alpha values for Four Grade FAS were 0.980.15 In this study, the functional activities of deep breathing, cough, turning over after surgery at 4 h (T1), 12 h (T2), 24 h (T3), 48 h (T4), and 72 h (T5), and getting out of bed for the first time, 48 h and 72 h after operation were evaluated.
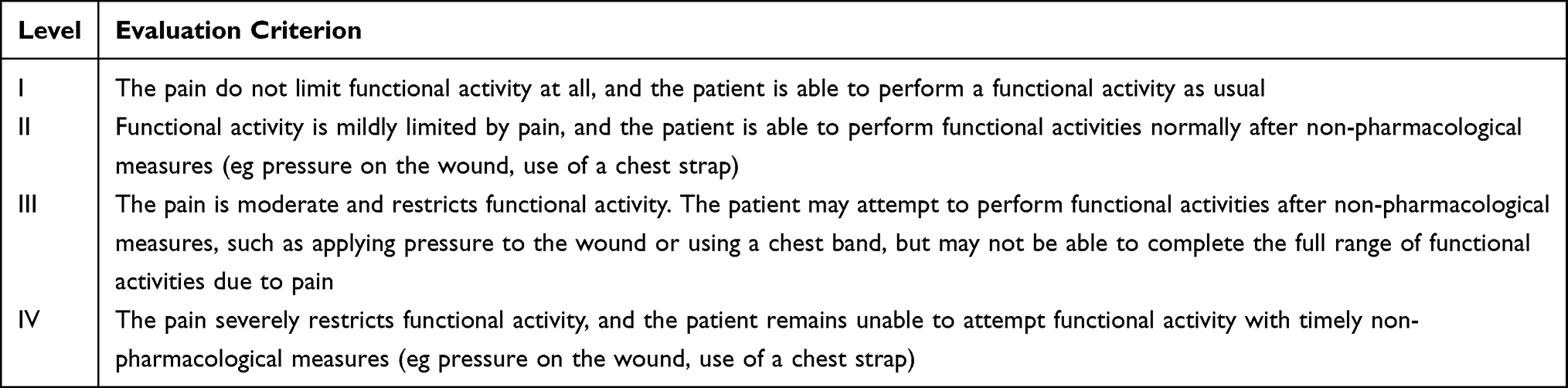 |
Table 4 The Content of Four Grade Functional Activity Score |
The Houston Pain Outcome Instrument (HPOI)
The HPOI is a comprehensive tool for assessing pain control and satisfaction of patients.16 It includes six dimensions: Pain expectations (2 items) (not been presented), pain Experience (3 items), emotional impact of pain (8 items), impact on daily activities (4 items), satisfaction with pain management methods (7 items), and satisfaction with pain education (6 items). Each item is scored on a 0–10 scale, with higher scores indicating better outcomes or higher satisfaction. Additionally, the HPOI includes an Overall Satisfaction score, which assesses the patient’s general satisfaction with pain management on a 0–10 scale. The time assessment is on the day of discharge. The Cronbach’s alpha values of the HPOI were 0.770, and the Cronbach’s alpha values of each component scale were 0.808–0.894.17
Quality of Life
QOL-LCV2.0 is developed by Wanchonghua and colleagues18 with reference to the QOL assessment scale for cancer patients and combination with China’s cultural background and some special conditions of patients with liver cancer. The scale is divided into four areas: physiology function (6 items), psychological function (6 items), symptoms and side effects (5 items), social function (5 items), with a total of 22 items and a self-evaluation. The scores of each item is evaluated by the digital scoring method of 0–10 levels, with a total score of 220 points, but excluding the last item, which has a maximum score of 100 points. The Cronbach’s alpha values for the four areas of the QOL-LCV2.0 were 0.78, 0.81, 0.75, and 0.68, respectively.19 The time assessment is on the day of discharge.
Other Outcomes
The results assessment also included several objective outcomes, including the number of presses of the patient-controlled analgesia (PCA) pump within 48 hours postoperatively, postoperative opioid consumption and the frequency of rescue analgesia administration (data extracted from the electronic medical records of healthcare institutions).
Statistical Analysis
The normality of continuous variables was assessed using the Shapiro–Wilk test. Continuous variables with normal distribution were analyzed using the independent samples t test and are presented as mean ± standard; Non-normally distributed continuous variables and ordinal data were analyzed using the Mann–Whitney U-test and are summarized as median (P25, P75). Categorical variables were expressed as frequencies and percentages, and intergroup differences were evaluated using the Chi-square test or Fisher’s exact test. The ranked data were analyzed using the Mann–Whitney U-test. For the repeated‑measures analysis of NRS scores, a generalized estimating equation (GEE) model was employed. GEE was selected because this study focuses on population-average effects, and the method is robust to misspecification of the correlation structure. To control type I error due to multiple testing, the Holm–Bonferroni correction was applied to the significance of the main effect of time and the group*time interaction. All reported P values were based on two-sided tests, with a P value of less than 0.05 considered as significant. The SPSS Statistics 25.0 was used to analyse the data.
Results
Participant General Characteristics
The two groups were homogeneous regarding the general characteristic. The experimental group included 29 patients (65.52% men, mean age 59.10 ± 14.18 years), and the control group included 28 patients (78.57% men, mean age 57.96 ± 7.58 years). The baseline sociodemographic and clinical characteristics and laboratory indicators of the experimental and control groups shown no significant differences (P > 0.05) (Table 5).
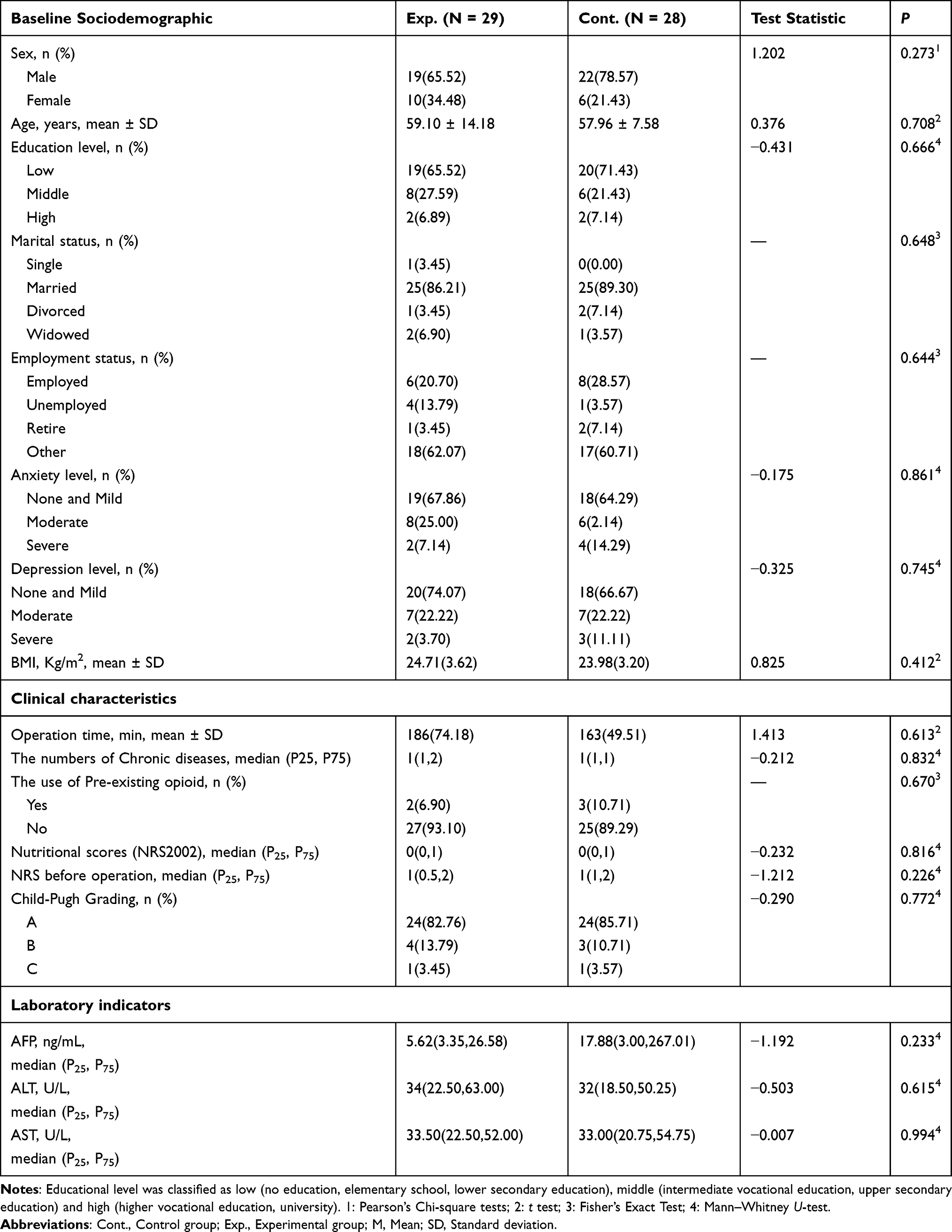 |
Table 5 Baseline Sociodemographic, Clinical Characteristics and Laboratory Indicators of Study Participants (N = 57) |
NRS Scores
There was no significant difference in NRS scores between the experimental and the control group when they were transferred to the ward after surgery (T0) (Table 6). Nevertheless, at T1(t = −3.979, P < 0.001), T2(t = −2.426, P = 0.019), T3(t = −4.192, P < 0.001), T4 (t = −2.924, P = 0.005) and T5(t = −2.797, P = 0.007), the NRS scores of the experimental group were lower than that of the control group (Table 6).
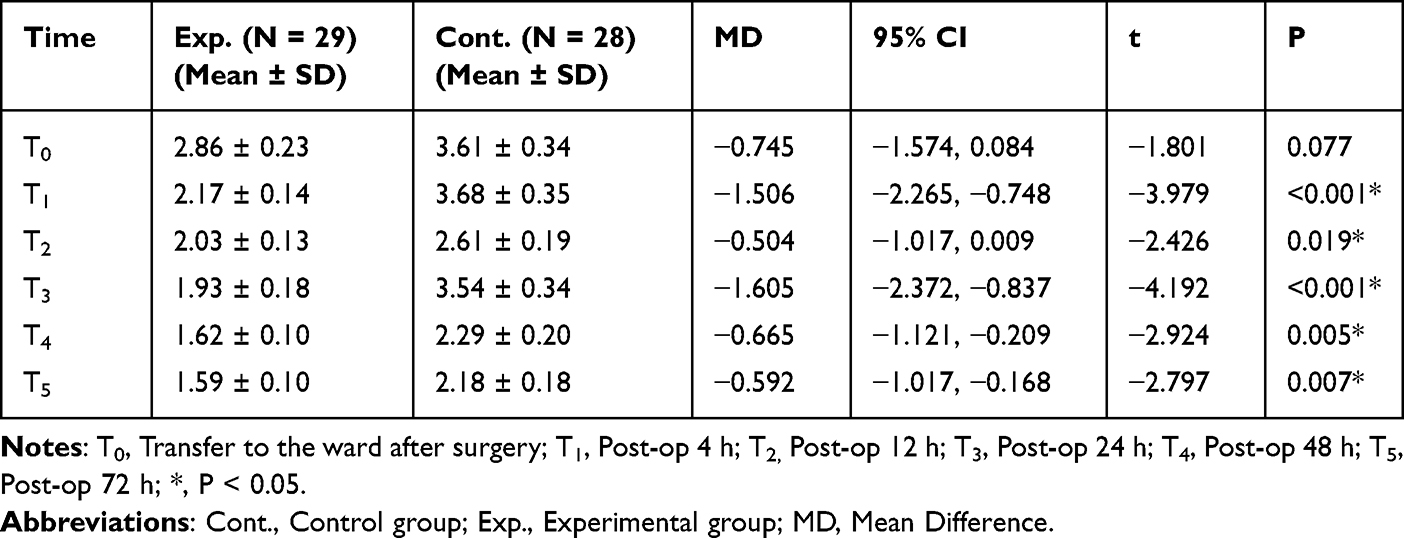 |
Table 6 The Differences of NRS Scores Between Both Groups at T0, T1, T2, T3, T4 and T5 According to the General Estimating Equation |
From the perspective of the main effect of time, the NRS score of the experimental group decreased significantly over time, and by 72 hours, it was 1.276 points lower than at T0. And the difference was statistically significant compared with T0 at each time point (Table 7). To control for the increased risk of Type I error due to multiple comparisons across five post-operative time points, Holm-Bonferroni correction was applied (adjusted α = 0.01). As shown in Table 7, regarding the main effect of time, pain scores shown a sustained and significant decline from T2 onward (adjusted P ≤ 0.01 for T2–T5), whereas the reduction at T1 was not significant after correction (adjusted P = 0.022). For the group*time interaction, significant differences in pain trajectories between the experimental and control groups were observed at T1, T3, and T4 (adjusted P ≤ 0.01 for all), while the interactions at T2 (adjusted P = 0.028) and T5 (adjusted P = 0.013) were not statistically significant following correction.
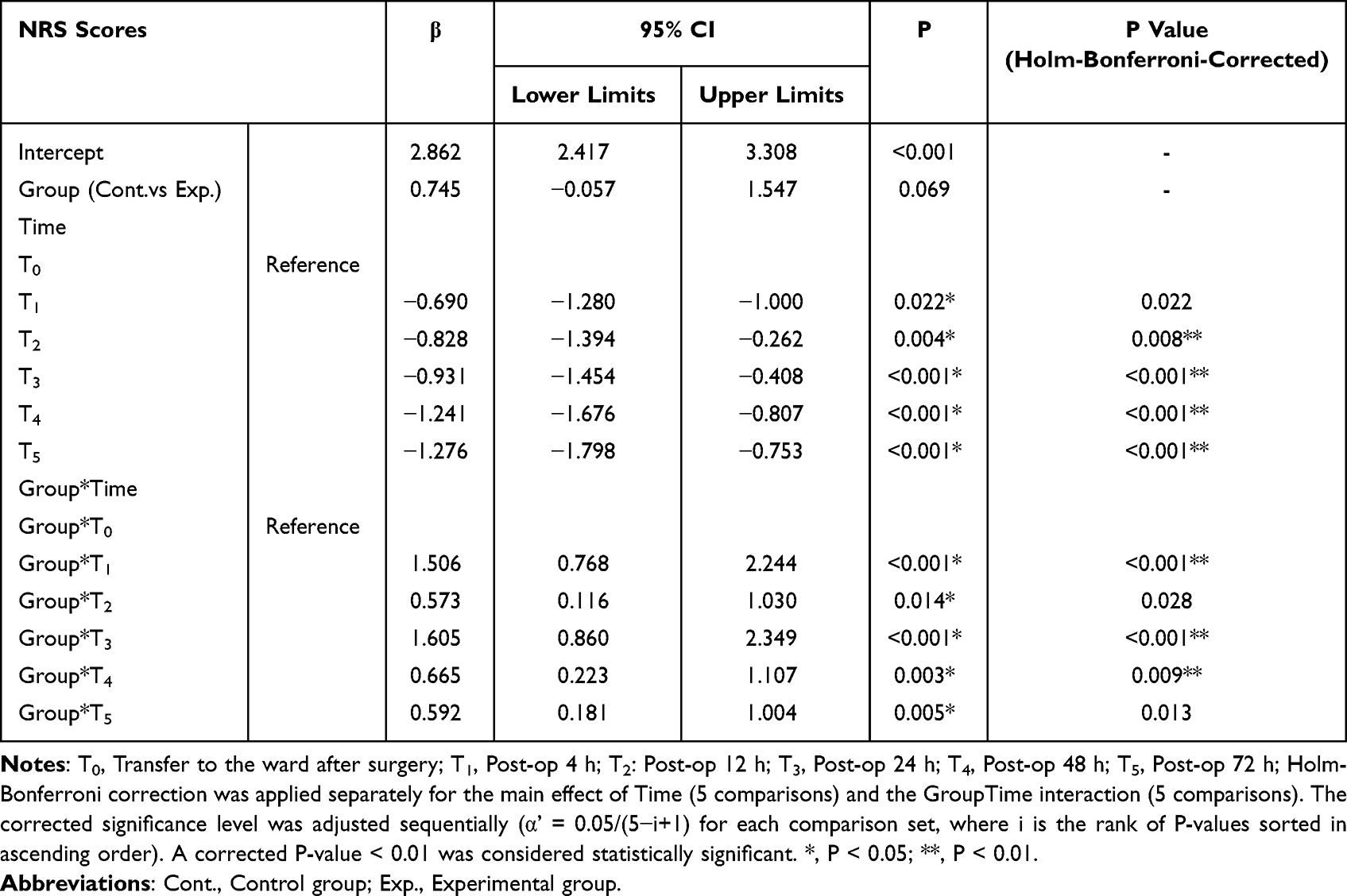 |
Table 7 Changes in NRS Scores at T1, T2, T3, T4 and T5 in Control and Experimental Group Compared to T0 Based on Generalized Estimating Equation Model |
Four Grade Functional Activity Score (FAS)
There was no statistical difference between the experimental group and the control group when the patients were first assessed for deep breathing (z = −1.024, P = 0.306), coughing (z = −1.239, P = 0.196), turning over (z = −1.476, P = 0.140) and first getting out of bed (z = −1.136, P = 0.256) after surgery. Compared to the control group, the experimental group had specific statistical significance in deep breathing at T2 (z = −3.472, P = 0.001), T3(z = −2.217, P = 0.027), T4 (z = −2.316, P = 0.021), and T5 (z = −2.166, P = 0.030), coughing at T3 (z = −2.446, P = 0.014), T4 (z = −2.803, P = 0.005), and T5 (z = −2.580, P = 0.010), turning over at T4 (z = −2.639, P = 0.008) and T5 (z = −2.493, P = 0.013), and getting out of bed for activities at T4 (z = −2.205, P = 0.027) and T5 (z = −3.151, P = 0.002) after surgery (Table 8).
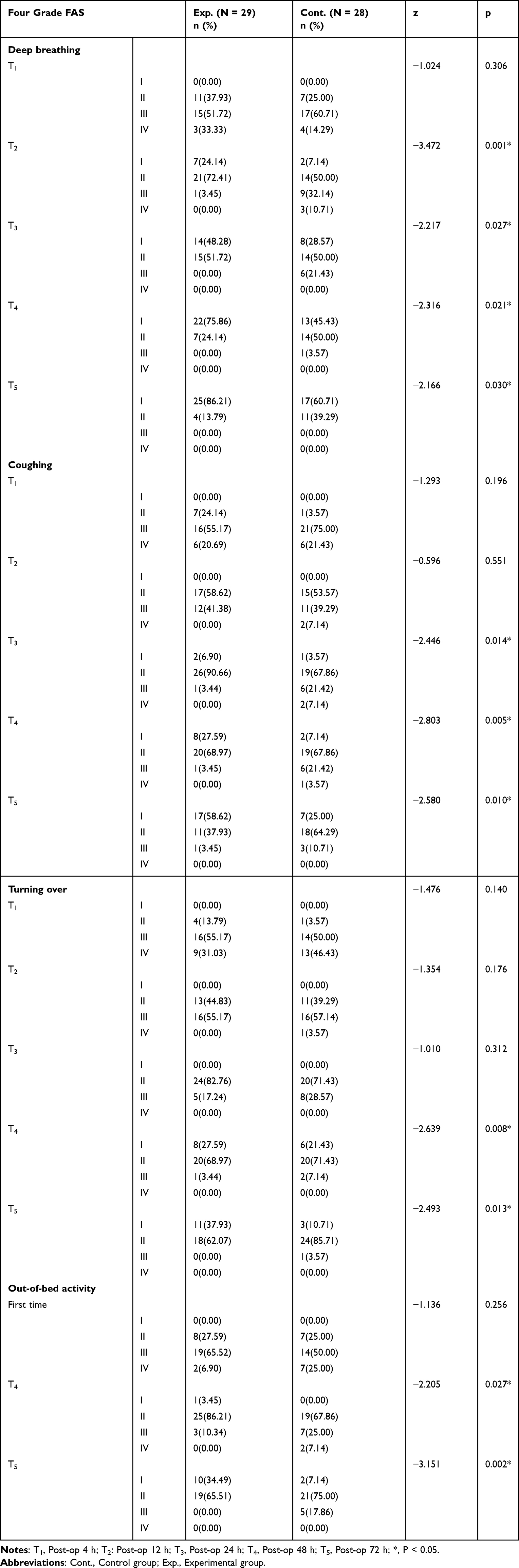 |
Table 8 Comparison of Results of Four-Grade FAS Evaluation Among Two Groups Based on The Mann–Whitney U-Test |
The HPOI and Quality of Life
The all dimensions of HPOI were statistically significant (P < 0.05) (Table 9). These results showed that the method can effectively improve patients’ satisfaction with pain control. In terms of quality of life, there were statistically significant differences between the experimental and control groups in physical function (t = −3.396, P = 0.001) and symptoms and side effects (t = −2.737, P = 0.008) at discharge (Table 9). However, regarding psychological and social functions, the two groups had no significant difference (t = 1.825, P = 0.073).
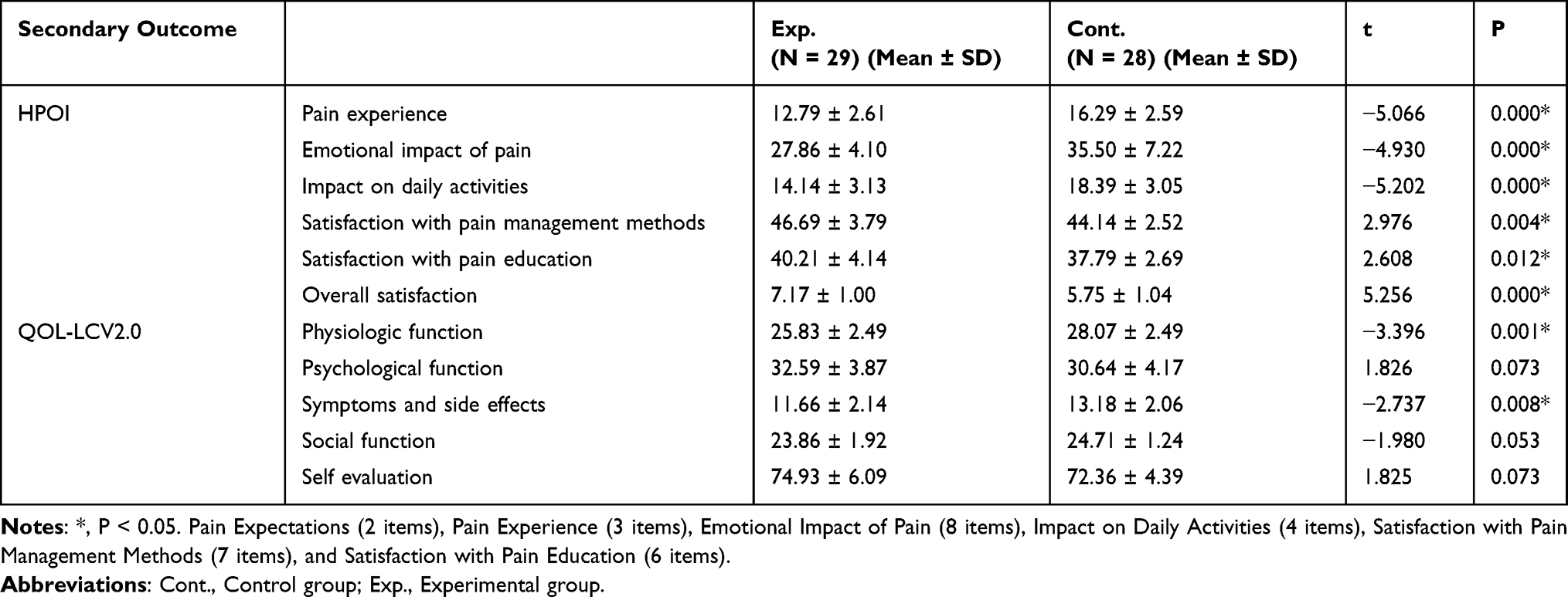 |
Table 9 Comparison of Pain Control Satisfaction, Quality of Life and Opioid Dose Between the Two Groups of Patients |
Others Outcomes
The median number of patient-controlled analgesia (PCA) pump presses within 48 hours postoperatively was significantly lower in the experimental group, with a median of 0.00 (0.00, 4.00), compared to 6.50 (0.00, 11.75) in the control group (Z = −2.484, P = 0.013). Additionally, the dose of the Opioid used in the experimental group was lower than that in the control group, and the difference was statistically significant (50 (0, 100) vs 100 (38.75, 200), Z = −2.345, P = 0.019). Furthermore, the frequency of rescue analgesia in the experimental group was significantly lower than that in the control group (0.00 (0.00, 1.00) vs 1.00 (1.00, 2.00), Z = −3.415, P = 0.001).
Discussion
Our study shown that pain management strategies for hepatectomy based on evidence summaries and Delphi studies had good clinical effect. The results showed that this intervention reduced the NRS scores of patients at 4 h, 12 h, 24 h, 48 h, and 72 h after surgery, alleviated the impact of pain on deep breathing, coughing, turning over, and getting out of bed, and improved patients’ satisfaction with pain control.
Unlike previous studies,20 the current intervention was developed by evidence summary and delphi study, and its implementation was facilitated by APST. This approach highlighted both the scientific validity and practical applicability in clinical settings. In this study, there was no statistically significant difference in NRS scores between the two groups when patients were transferred to the general ward after surgery (t = −1.801, P = 0.077), which may be due to the fact that early postoperative pain management mainly depended on standardized perioperative analgesia protocols,21 and masked short-term differences in different intervention strategies. It may also be due to the residual effect of anesthesia or that it takes 1–4 hours for the prostaglandins and bradykinin released from the surgical incisions to reach a sufficient concentration to stimulate the nociceptive nerves,22 resulting in no significant difference in early postoperative pain. Our findings showed that the NRS scores of the experimental group at 4 h, 12 h, 24 h, 48 h and 72 h after operation were lower than those of the control group, which was similar to the results of a study of pain control using multimodal analgesia in patients with liver cancer after laparotomy.23 Our study showed that the experimental group reported NRS scores of 2.03 ± 0.13, 1.93 ± 0.18, and 1.62 ± 0.10 at 12 h, 24 h, and 48 h postoperatively, respectively, which were markedly lower than the control group’s scores of 2.61 ± 0.19, 3.54 ± 0.34, and 2.29 ± 0.20, which were lower than those reported by Xu et al,23 may be because of the fact that the subjects in this study were laparoscopic postoperative patients with small incision, less trauma and faster recovery. Of particular interest was the rebound in NRS scores observed in the control group at 24 h postoperatively, a phenomenon likely linked to increased pain during early ambulation and mechanical stress on surgical incisions. In contrast, the experimental group maintained a consistent downward trend in NRS scores, further indicating the effectiveness of the intervention protocol. This divergence underscored the advantage of our tailored intervention in addressing dynamic postoperative pain challenges. Although the overall effect was significant, the between-group difference at 12 h and 72 h postoperatively did not reach statistical significance after correction for multiple comparisons. This may be attributable to the fact that pain in the control group was also relieved to a certain extent by basic analgesia, resulting in a relatively narrowed difference between the two groups at specific point. The results of this study show that the frequency of rescue analgesia in the experimental group was significantly lower than that in the control. Within the 72 postoperative hours, patients in the intervention group reported 12 times of moderate to severe pain, but the number of rescue analgesic administration was 5, while patients in the control group reported 25 times of moderate to severe pain, and the number of rescue analgesic administration was 20. The pressing times of controlled analgesia pump and the dosage of opioids used in the experimental group were lower than those in the control group. To further illustrate the effectiveness of dynamic assessment and management of pain and reduce the dosage of analgesics and opioids. Compared with previous studies, our findings are consistent with the growing body of evidence supporting the efficacy of multimodal analgesia protocols in reducing postoperative pain and opioid consumption. For instance, a recent meta-analysis of multimodal analgesia in hepatectomy for hepatocellular carcinoma demonstrated a significant reduction in postoperative pain scores and opioid use, similar to our results.24 These studies collectively highlight the benefits of integrating non-pharmacological interventions into multimodal analgesia protocols to enhance pain control and reduce reliance on opioids.
Active pain refers to the pain when the patient performs functional activities25 (such as effective coughing, deep breathing, getting out of bed, and joint function exercises). Previous studies have used the Visual Analog Scale (VAS) or Numeric Rating Scale (NRS) to assess active pain. However, this study used a four grade Functional Activity Score method to evaluate the impact of pain on deep breathing, coughing, turning over, and getting out of bed, so as to guide clinical intervention. In the early postoperative period, both the experimental and control groups experienced moderate to severe active pain limiting functional activities in more than half of the patients, with no statistically significant differences between the groups. However, the total number of patients who were above grade III in the experimental group was less than that in the control group. This suggested that the program did not show a significant effect on active pain control in the early postoperative period. Meanwhile, this result indicated that functional activity limitations in the early postoperative period may exist under the current pain management model, suggesting that there are common shortcomings in existing pain control strategies and that the perioperative analgesic protocol may need to be further optimized. And future research on postoperation pain should focus on reducing active pain. Regarding pain control satisfaction, all dimensions of HPOI in the experimental group showed a significant difference after intervention compared to the control group (P < 0.05). These results confirmed the good effect of postoperative pain management program on pain in patients after hepatectomy. The advantage of the experimental group in the dimensions of pain control and education satisfaction might be attributed to the synergistic effect of multimodal intervention,26 such as preoperative patient education and a systematic pain management plan combined with multidisciplinary pain control, constituting a comprehensive and systematic intervention.
Notably, in terms of quality of life, the experimental group was only better than the control group in physical and bodily functions (p < 0.05), with no significant differences found in social function and mental health. This result may be due to the fact that the sample size calculation was based on the primary outcomes and did not fully account for the statistical power required for secondary outcomes or potential subgroup analyses. The study may be underpowered to detect between-group differences for these measures. Future studies with larger sample sizes are needed to verify these exploratory findings. Also, this may suggest that the current intervention prioritized the restoration of patients’ physiological functions over socio-psychological aspects, and that social function and mental health often require a longer time to recover.27 It also indicated that the current intervention focused on physical rehabilitation and acute pain management, with insufficient intensity of intervention on social support systems and psychological stress. It is recommended to incorporate psychological and social support measures into follow-up plan to address the psychosocial burden unique to patients with liver cancer.
Limitation
This study only evaluated short-term analgesic effects (within 72 hours) and lacked assessment of long-term outcomes, such as chronic pain, readmission or quality of life. Also, to prevent treatment diffusion and contamination, control group data were collected before experimental group data; therefore, a randomized controlled trial was not performed. Furthermore, the lack of blinding for both patients and outcome assessors introduces a risk of performance and detection bias, particularly for patient-reported outcomes such as NRS scores, the HPOI and Quality of life. It is important to note that the significant reduction in objective analgesic endpoints—including total opioid consumption, frequency of patient-controlled analgesia (PCA) demands, and the need for rescue analgesia in the intervention group compared to the controls—provides convergent validity. This strengthens the argument that the observed pain relief reflects a genuine clinical effect rather than merely a reporting artifact. Any such bias would most likely overestimate the intervention’s benefit due to positive expectations from patients and care providers. Consequently, our secondary finding of no significant improvement in psychosocial function—another subjective domain—gains greater credibility, as it suggests that potential bias did not uniformly inflate all positive outcome measures. Since the study was conducted in a single center due to limited resources, there may be selection bias in the medical setting. We anticipate that a multicenter study will be conducted in the future to further validate our findings. The per-protocol analysis of the data excluded participants who did not adhere or were lost to follow-up, which may have overestimated treatment effects and compromised generalizability of the findings.
Conclusions
The Evidence-Based and Multidisciplinary pain management program is a good strategy to reduce postoperative pain, alleviate the impact of pain on functional activities, and improve patient satisfaction. Future studies should focus on multi-center, large-sample randomized controlled trials to further verify the long-term effect and wide applicability. Also, more objective indicators and standardized intervention measures are combined to improve the accuracy and comparability of the study, and provide a more comprehensive and effective solution for postoperative pain management of liver cancer.
Data Sharing Statement
All data and program codes are available upon reasonable request to the corresponding author.
Acknowledgments
We are grateful to all participants and staff. This work was supported by the Xuzhou Science and Technology Bureau (Project No.: KC23281), Xuzhou Medical University - Qilu Clinical Research Fund Projectthe (QL-ZD001) and High-Level Hospital Construction Project of the Affiliated Hospital of Xuzhou Medical University (PYJH2025309).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Maki H, Hasegawa K. Advances in the surgical treatment of liver cancer. Biosci Trends. 2022;16(3):178–18. doi:10.5582/bst.2022.01245
2. Kwon JH, Ko JS, Kim HJ, et al. Comparison of the analgesic effect of intrathecal morphine between laparoscopic and open living donor hepatectomy: propensity score matching analysis. Medicine. 2023;102(35):e34627. doi:10.1097/MD.0000000000034627
3. Ishida Y, Okada T, Kobayashi T, Funatsu K, Uchino H. Pain management of acute and chronic postoperative pain. Cureus. 2022;14(4):e23999. doi:10.7759/cureus.23999
4. Marshall K, McLaughlin K. Pain management in thoracic surgery. Thoracic Surg Clin. 2020;30(3):339–346. doi:10.1016/j.thorsurg.2020.03.001
5. Graf J, Stengel A. Psychological burden and psycho-oncological interventions for patients with hepatobiliary cancers-a systematic review. Front Psychol. 2021;12:662777. doi:10.3389/fpsyg.2021.662777
6. Husni M, Jahrami H, Al Shenawi H, et al. Postoperative patient pain severity and its association with anxiety, depression, and sleep quality. Cureus. 2024;16(2):e54553. doi:10.7759/cureus.54553
7. Joshi GP, Kehlet H. Postoperative pain management in the era of ERAS: an overview. Best Pract Res Clin Anaesth. 2019;33(3):259–267. doi:10.1016/j.bpa.2019.07.016
8. Dieu A, Huynen P, Lavand’homme P, et al. Pain management after open liver resection: procedure-specific postoperative pain management (PROSPECT) recommendations. Reg Anesth Pain Med. 2021;46(5):433–445. doi:10.1136/rapm-2020-101933
9. Omar A, Kaseb A, Elbaz T, et al. Egyptian society of liver cancer recommendation guidelines for the management of hepatocellular carcinoma. J Hepatocell Carcinoma. 2023;10:1547–1571. doi:10.2147/JHC.S404424
10. Villegas Estévez FJ, López Alarcón MD, Beato C, Sanz-Yagüe A, Porta-Sales J, Morera López RM. Procedural pain in patients with cancer: a Delphi expert management consensus. BMJ Support Palliative Care. 2023;13(e2):e428–e436. doi:10.1136/bmjspcare-2020-002668
11. Beverly A, Kaye AD, Ljungqvist O, Urman RD. Essential elements of multimodal analgesia in enhanced recovery after surgery (ERAS) guidelines. Anesthesiol clin. 2017;35(2):e115–e143. doi:10.1016/j.anclin.2017.01.018
12. Nuseir K, Kassab M, Almomani B. Healthcare providers’ knowledge and current practice of pain assessment and management: how much progress have we made? Pain Res Manag. 2016;2016:8432973. doi:10.1155/2016/8432973
13. Wang Y, Song X, Wang S, et al. Construction of pain management strategies after hepatectomy: evidence summary and Delphi study. J Pain Res. 2024;17:4541–4559. doi:10.2147/JPR.S494243
14. Ke Q, Luo H, Li R, Fan Y. Application of multi-model analgesia in patients with partial hepatectomy for liver cancer. Chin Nurs Res. 2019;33(20):3611–3612.
15. Tong Y, Cheng Y, Zheng H, Feng J, Chen F, Bi D. Research on the reliability, validity and application effect of the Four-Grade functional activity scoring method. J Nurs Train. 2016;31(11):968–971.
16. Zhang YE, Xu X, Gong R. Postoperative pain management outcomes at a chinese hospital: a cross-sectional survey. J Perianesthesia Nurs. 2023;38(3):434–439. doi:10.1016/j.jopan.2022.07.002
17. Shen Q, Li Z. A study on the reliability and validity of the Houston Pain Questionnaire. Chin J Nurs. 2006;41(11):1049–1051.
18. Li W, Qi Y, c W, et al. Items selection on the specific module of quality of life instruments for patients with liver cancer (QLICP-LI). Chin Cancer. 2011;20(10):746–749.
19. Zhu B, Wang C, Wang K, Yuan J, Xu C, Meng Q. Comparisons among FLIC, SF-36 and QOL-LC in measuring quality of life of patients with liver cancer. Chin J Evid-Based Med. 2012;12(10):1175–1179.
20. Small C, Laycock H. Acute postoperative pain management. Br J Surg. 2020;107(2):e70–e80. doi:10.1002/bjs.11477
21. Melloul E, Hübner M, Scott M, et al. Guidelines for perioperative care for liver surgery: enhanced recovery after surgery (ERAS) society recommendations. World J Surg. 2016;40(10):2425–2440. doi:10.1007/s00268-016-3700-1
22. Petho G, Reeh PW. Sensory and signaling mechanisms of bradykinin, eicosanoids, platelet-activating factor, and nitric oxide in peripheral nociceptors. Physiol Rev. 2012;92(4):1699–1775. doi:10.1152/physrev.00048.2010
23. Xu C, Qian H, Chen L. Effect of multimodal analgesic nursing intervention on pain control in patients with liver cancer after laparotomy. J Nurs Train. 2017;32(5):449–451.
24. Cao Y, Shen J. Meta-analysis of multimodal analgesia for reducing postoperative wound pain after hepatectomy for hepatocellular carcinoma. Sci Rep. 2025;15(1):15494. doi:10.1038/s41598-025-00069-4
25. Macintyre PE, Scott DA, Schug S, et al. Acute Pain Management:scientific Evidence[M].
26. O’Neill A, Lirk P. Multimodal analgesia. Anesthesiol Clin. 2022;40(3):455–468. doi:10.1016/j.anclin.2022.04.002
27. Yamamoto H, Tanaka S, Kasugai D, et al. Physical function and mental health trajectories in COVID-19 patients following invasive mechanical ventilation: a prospective observational study. Sci Rep. 2023;13(1):14529. doi:10.1038/s41598-023-41684-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Assessment of the Community Pharmacists’ Knowledge and Attitudes Toward Pain and Pain Management in Saudi Arabia
Alorfi NM, Ashour AM, Algarni AS, Alsolami FA, Alansari AM, Tobaiqy M
International Journal of General Medicine 2022, 15:8527-8537
Published Date: 7 December 2022
Spinal Anaesthesia as an Adjunct to General Anaesthesia for Laparoscopic Abdominoperineal Rectal Amputation
Antunes M, Baumgärtel A, Gjessing PF, Ytrebø LM
Journal of Pain Research 2023, 16:1855-1865
Published Date: 31 May 2023
Construction of Pain Management Strategies After Hepatectomy: Evidence Summary and Delphi Study
Wang Y, Song X, Wang S, Bai T, Li R, Liu H, Liu Y, Han Z
Journal of Pain Research 2024, 17:4541-4559
Published Date: 27 December 2024
Pharmacological Pain Management in Adults with Venous Ulceration: A Systematic Review
Saghdaoui LB, Lampridou S, Baldo L, Onida S, Hohenschurz-Schmidt D, Chumbley GM, Atkin L
Journal of Pain Research 2026, 19:588661
Published Date: 1 April 2026
Peripheral Nerve Blocks Following Open Hepatectomy: A Systematic Review and Network Meta-Analysis
Ma Z, Ma J, Liu Z, Hu J, Yan W, Wang D
Journal of Pain Research 2026, 19:591828
Published Date: 21 April 2026