Back to Journals » Journal of Pain Research » Volume 19
Peripheral Nerve Blocks Following Open Hepatectomy: A Systematic Review and Network Meta-Analysis
Authors Ma Z, Ma J, Liu Z, Hu J, Yan W, Wang D
Received 30 December 2025
Accepted for publication 14 April 2026
Published 21 April 2026 Volume 2026:19 591828
DOI https://doi.org/10.2147/JPR.S591828
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jinlei Li
Zhijun Ma,1 Jinxin Ma,2 Zhilong Liu,1 Jianhong Hu,1 Wenjun Yan,1 Dong Wang1
1Department of Anesthesiology, Gansu Provincial Hospital, Lanzhou, Gansu, 730000, People’s Republic of China; 2Department of Neurosurgery, Lanzhou University Second Hospital, Lanzhou, Gansu, 730000, People’s Republic of China
Correspondence: Dong Wang, Email [email protected]
Background: This network meta-analysis (NMA) was conducted to evaluate the analgesic efficacy of various nerve blocks in patients undergoing open partial hepatectomy.
Methods: We retrieved randomized controlled trials (RCTs) assessing different peripheral nerve blocks in patients undergoing open partial hepatectomy from databases including PubMed, Embase, Web of Science, and the Cochrane Library, spanning from inception until December 2025. The NMA was performed using STATA 17.0 software.
Results: A total of 17 RCTs involving 1056 patients and 8 techniques were included in the analysis. Continuous Transversus Abdominis Plane Block (cTAPB) and continuous Thoracic Paravertebral Block (cTPVB) significantly decreased morphine consumption within 24 hours. The Erector Spinae Plane Block (ESPB) and Thoracoabdominal Nerve Block (TANB) reduced resting Visual Analog Scale (VAS) scores at 6 hours. At 12 hours, resting VAS scores were decreased by ESPB and subcostal Transversus Abdominis Plane Block (sTAPB), while at 24 hours, resting VAS scores were lowered by TANB and cTAPB. For movement VAS scores, reductions were observed at 6 hours with ESPB and cTPVB, at 12 hours with ESPB and sTAPB, and at 24 hours with TANB and External Oblique Intercostal Plane Block (EOIPB). Additionally, ESPB and TANB were associated with a decrease in the incidence of postoperative nausea and vomiting (PONV).
Conclusion: While cTAPB and cTPVB ranked higher in terms of reducing 24-hour morphine consumption, the clinical difference between these techniques and other interventions was small. ESPB was more likely to reduce VAS within the first 12 hours and the PONV incidence. Nevertheless, the certainty of evidence for these findings remains low to moderate, and further high-quality randomized controlled trials are warranted to confirm their clinical utility.
Limitation: The studies included in our review exhibited inconsistencies in study design and analgesia protocols, which may introduce bias into our findings. The results may not be directly applicable to laparoscopic procedures. The absence of these unpublished data or ongoing trials could limit the comprehensiveness of our analysis.
Keywords: pain, nerve block, hepatectomy, systematic review, network meta-analysis
Introduction
Open hepatectomy is a common surgical procedure for various hepatic conditions, including liver tumors, metastases, and cirrhosis.1 Postoperative pain following open hepatectomy can be significant, adversely affecting patient recovery and prolonging hospital stays.2 Studies have shown that poor postoperative pain control can lead to complications such as delayed mobilization, increased levels of anxiety and distress, and a subsequent rise in healthcare costs.2 Therefore, effective pain management strategies are crucial for improving patient outcomes and reducing the overall burden on healthcare resources.
Current analgesic strategies following open hepatectomy often combine systemic medications with regional nerve blocks.3 This multimodal approach aims to optimize pain control while minimizing the side effects commonly associated with systemic opioids.4 Regional analgesia has been shown to provide superior pain relief, decrease the need for opioids, and promote earlier mobilization compared to systemic analgesia alone.4 The synergistic effect of combining systemic analgesics with regional nerve blocks not only enhances analgesia but also contributes to improved patient satisfaction and faster recovery times.4
Despite the recognized benefits of various nerve block techniques,5–8 there remains a lack of consensus regarding the most effective type of regional analgesia for patients undergoing open hepatectomy. Numerous regional blocks have been proposed, each with its own advantages and limitations; however, determining which technique best meets the specific analgesic needs of these patients remains uncertain, particularly as new nerve block techniques continue to emerge. Network meta-analysis (NMA) extends beyond traditional pairwise meta-analysis by enabling the simultaneous comparison of multiple interventions. It achieves this by integrating both direct and indirect evidence within a coherent analytical framework, whereas conventional meta-analyses are restricted to direct comparisons between two interventions. Therefore, the necessity of our study lies in conducting a systematic review and NMA to comprehensively evaluate and compare the analgesic efficacy of existing regional nerve blocks following open hepatectomy. This research aims to establish evidence-based recommendations that could enhance postoperative pain management for patients undergoing this complex surgical procedure.
Methods
The protocol for this review was preregistered and published in the International Prospective Register of Systematic Reviews (CRD420251239156). This NMA adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.9
Eligibility Criteria
Eligibility criteria were designed based on the PICOS framework: patients undergoing open partial hepatectomy (P); regional analgesic techniques, including erector spinae plane block (ESPB), thoracic paravertebral block (TPVB), transversus abdominis plane block (TAPB), quadratus lumborum block (QLB), thoracoabdominal nerve block (TANB), and external oblique intercostal plane block (EOIPB) (I); comparisons with one of the regional analgesic techniques, placebo, or no intervention (C); outcomes measured as morphine consumption within 24 hours, postoperative pain scores, or postoperative nausea and vomiting (PONV) (O); and inclusion of randomized controlled trials (RCTs) (S). Studies were excluded based on the following criteria: (1) incomplete data that could not be utilized for statistical analysis; (2) unpublished studies or those utilizing parallel and crossover randomized designs; and (3) studies with duplicated data or incomplete information.
Search Strategy
We conducted a comprehensive search across PubMed, Embase, Web of Science, and the Cochrane Library, without language restrictions, from inception until December 2025. Following the PICOS principles, the search utilized the following headings: “hepatectomy,” “liver,” “pain,” and “block.” We employed MeSH terms, free-text keywords, and Boolean operators (OR and AND) to refine our search. The complete search strategy for PubMed, as a representative example, is detailed in Table S1.
Study Selection
Two independent investigators sequentially reviewed all titles and abstracts, followed by full-text assessments. Any disagreements regarding study eligibility between the two reviewers were resolved by a third reviewer. We extracted relevant data from the eligible literature, ensuring accuracy through confirmation by both investigators. The following characteristics were systematically extracted from each included study: author, year of publication, country of origin, blinding methods, treatment descriptions, sample size, rescue analgesic regimens, and reported outcomes.
Data Extraction and Data Retrieval
The primary outcome assessed was cumulative morphine consumption, quantified in intravenous morphine equivalent doses (mg) within the first 24 hours postoperatively.10 Secondary outcomes included the incidence of postoperative nausea and vomiting (PONV) within 24 hours, as well as resting and movement pain scores recorded at 6, 12, and 24 hours. Pain scores were standardized on a 0 to 10 Visual Analog Scale (VAS), with the VAS score at 6 hours defined as the maximum pain score recorded from 2 to 6 hours after surgery, and similar endpoints applied for scores at 8 to 12 hours and 20 to 24 hours.
Quality of Evidence
Two independent reviewers evaluated the risk of bias using the Cochrane Collaboration’s Risk of Bias Tool, which assesses the following domains: sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting, and other potential sources of bias.11 To evaluate the confidence in the findings from the network meta-analysis, we employed the Confidence in Network Meta-analysis (CINeMA 2.0.0) framework, which considers six domains: within-study bias, reporting bias, indirectness, imprecision, heterogeneity, and incoherence.12,13 The GRADE methodology was utilized to assess the quality of evidence for each outcome.14
Statistical Analysis
Statistical analysis was conducted using STATA 17.0 software, employing a random-effects model to synthesize the data. Effect estimates were reported as relative risk (RR) with 95% confidence intervals (CIs) for dichotomous variables, and mean differences (MD) with 95% CIs for continuous variables. Data expressed as medians with interquartile ranges were converted into means and standard deviations using the validated formulas from Luo and Wan.15,16 Network geometry maps provided visual representations of the relationships between pairs of interventions, while forest plots illustrated study outcomes and global heterogeneity results. Network league tables displayed the relative effectiveness of each intervention. The Surface Under the Cumulative Ranking Curve (SUCRA) was used to estimate ranking probabilities for all interventions, with lower values indicating superior effects. Publication bias was assessed using a funnel plot, and node-splitting inconsistency testing was employed to identify local inconsistencies. A P-value of <0.05 was considered statistically significant for all analyses. Sensitivity and subgroup analyses were planned to explore potential sources of heterogeneity as necessary.
Results
We identified a total of 561 potentially relevant records, ultimately including 17 RCTs that examined 8 distinct regional analgesia techniques in this NMA.17–33 The study selection process is illustrated in Figure 1, and Table 1 details the characteristics of the included studies. The primary outcome was reported in 11 of the RCTs, with the ESPB and TAPB being the most frequently utilized interventions.
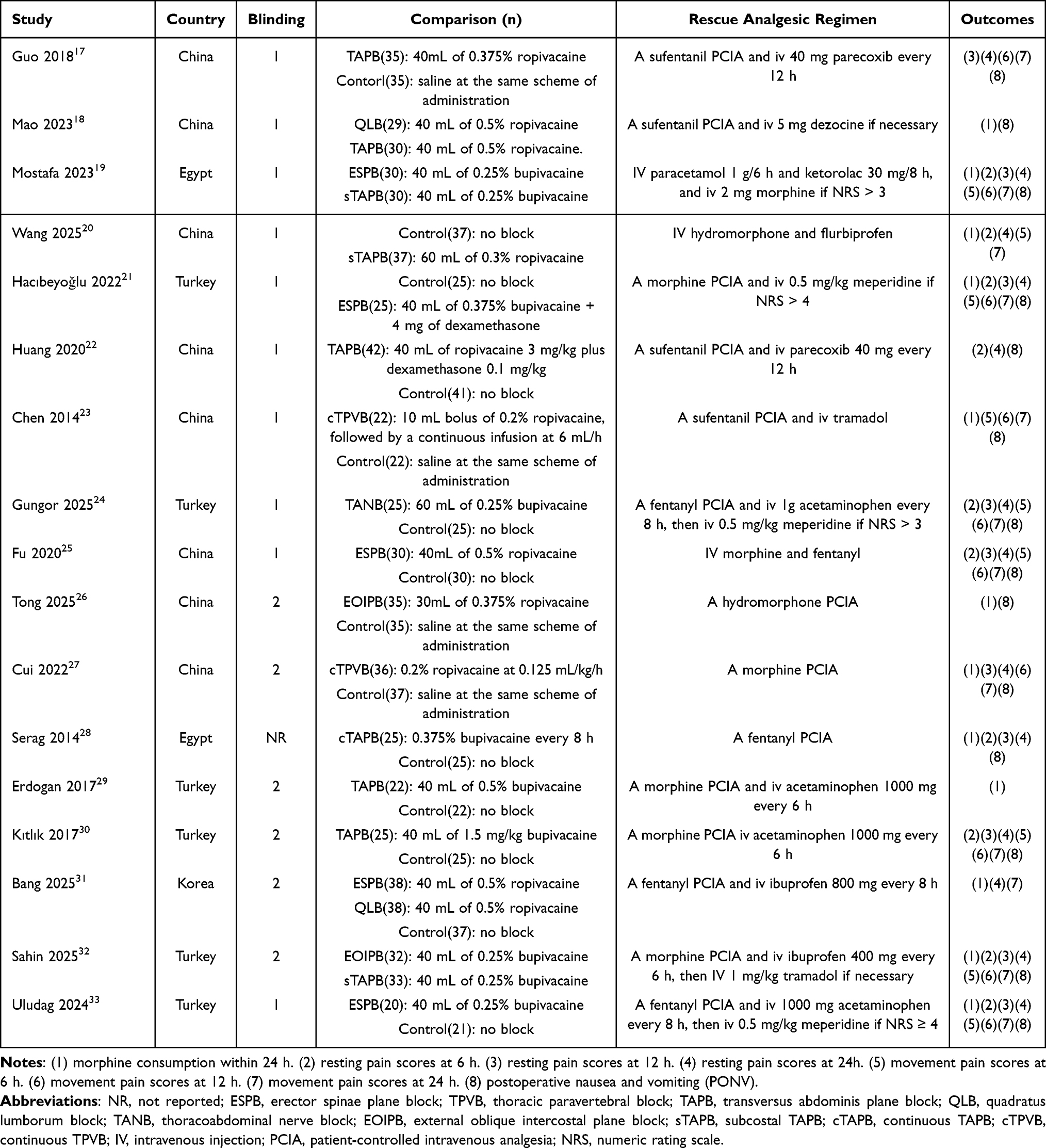 |
Table 1 Study Characteristics of Included studies17–33 |
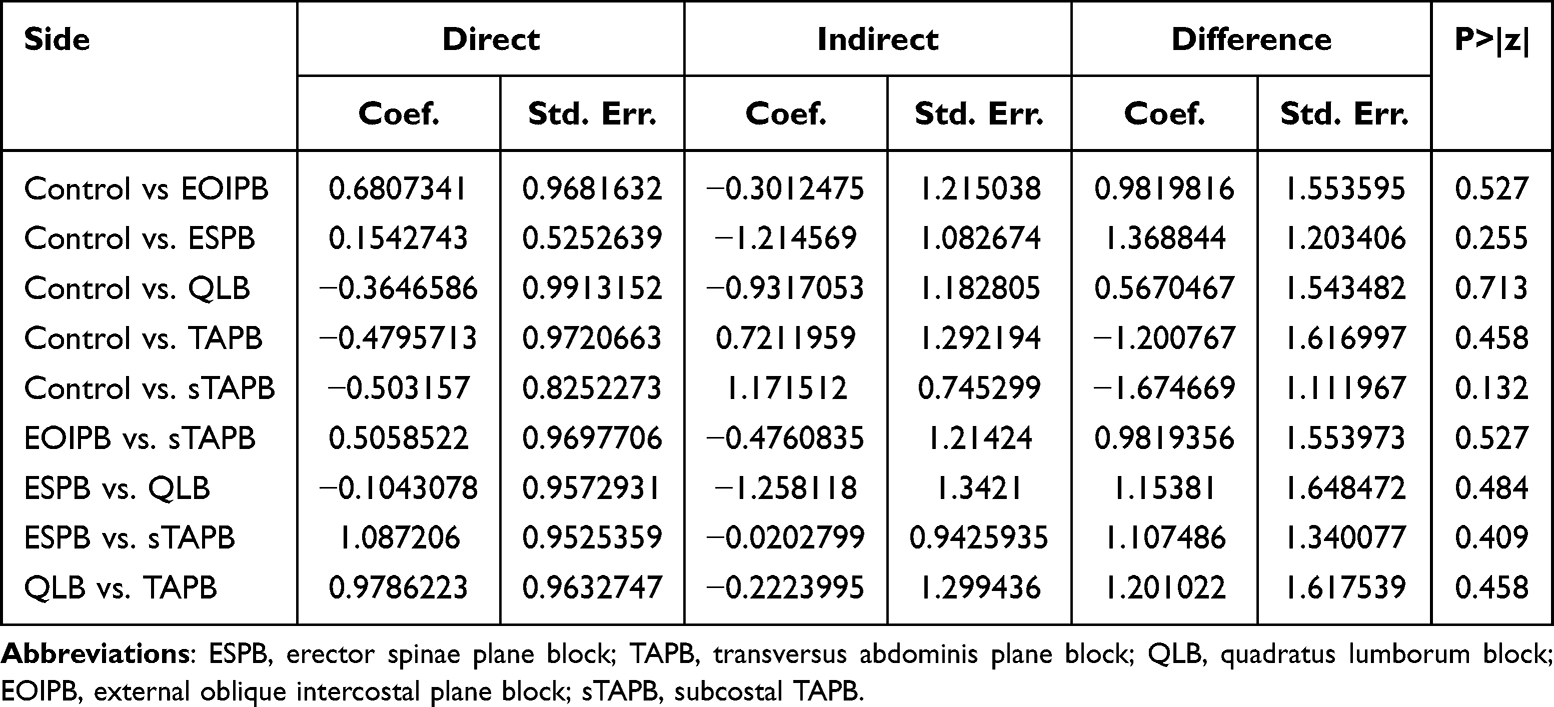 |
Table 2 Node-Splitting of Morphine Consumption |
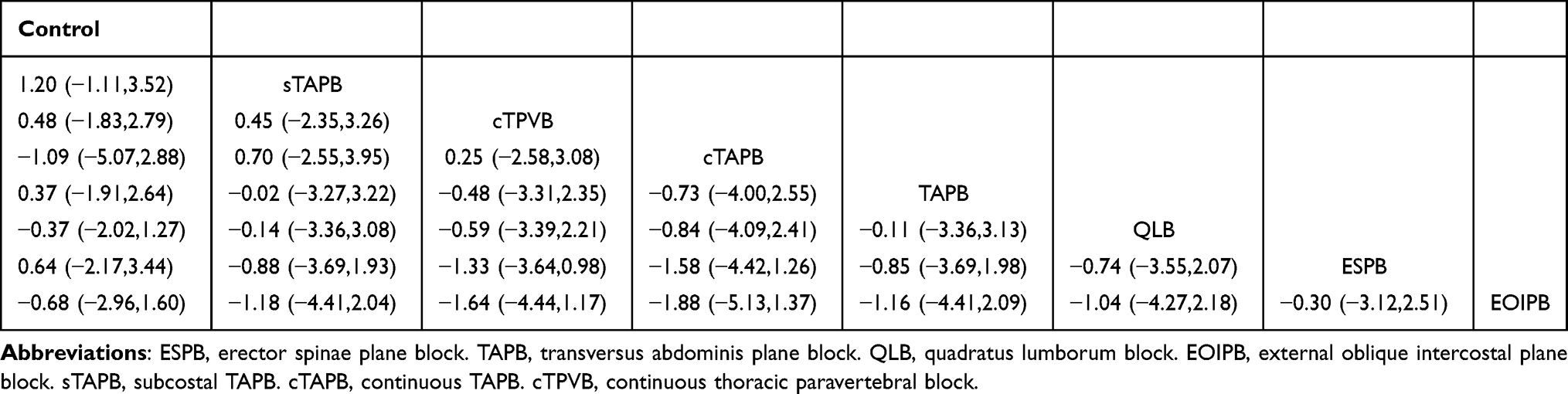 |
Table 3 Netleague of Resting VAS at 6 h After Surgery |
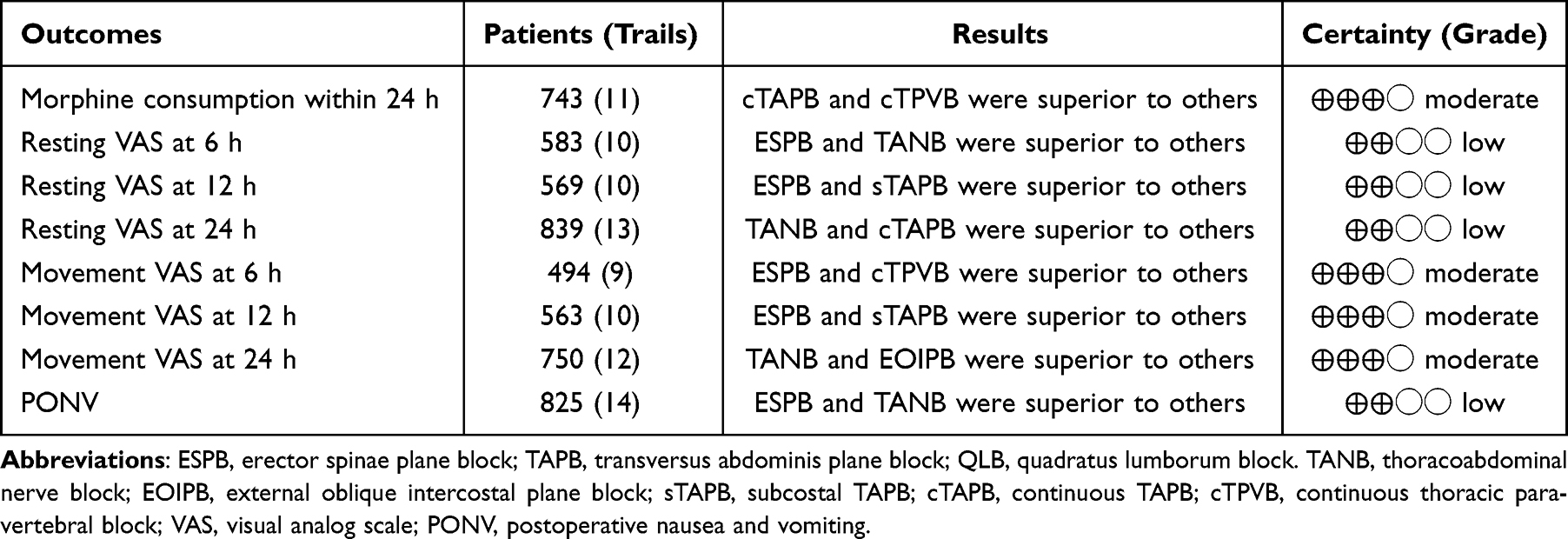 |
Table 4 Summary of Evidence |
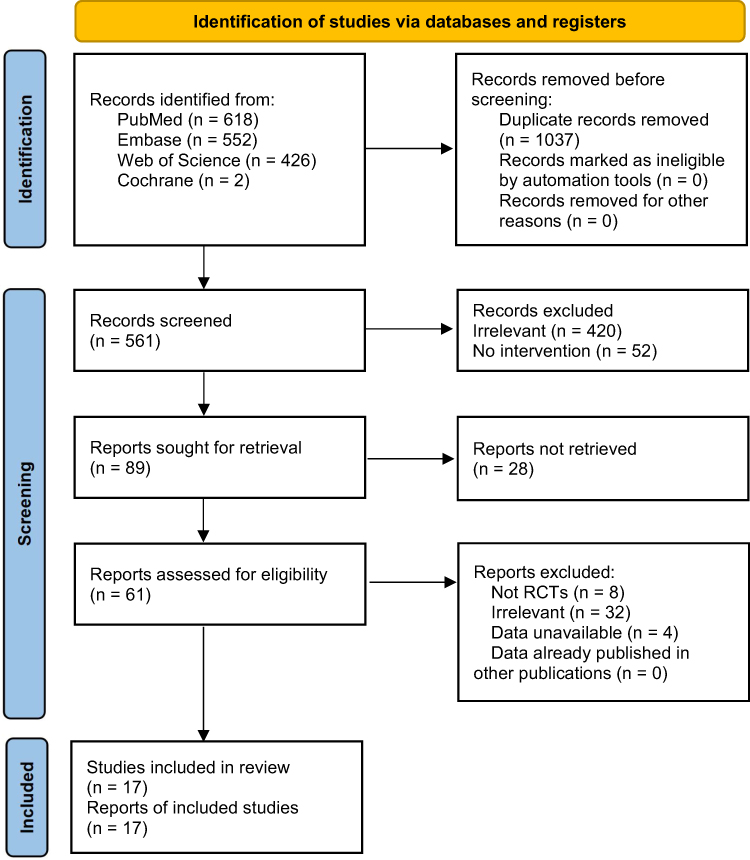 |
Figure 1 PRISMA flow diagram of study selection. |
Primary Outcome
Cumulative Morphine Consumption Within 24 h
Eleven studies with 743 patients were included. The network geometry of eligible comparisons displayed complete, as all nodes could be connected (Figure 2). The network forest plot did not show any global heterogeneity between trials and the results supported the consistency model (Figure 3). The result of inconsistency testing did not show any significant local inconsistency (Table 2). Figure 4 showed that cTAPB attained the lowest SUCRA value (28.1), followed closely by cTPVB (30.8), and subcostal TAPB (sTAPB, 46.4), while EOIPB (77.0) occupied the higher positions in the ranking. Small study bias or any publication bias was not observed in funnel plot (Figure 5). The risk of bias might increase due to an undisclosed blinding method in a study28 (Figure 6). Additionally, Table 3 showed the difference in effect size between all treatments.
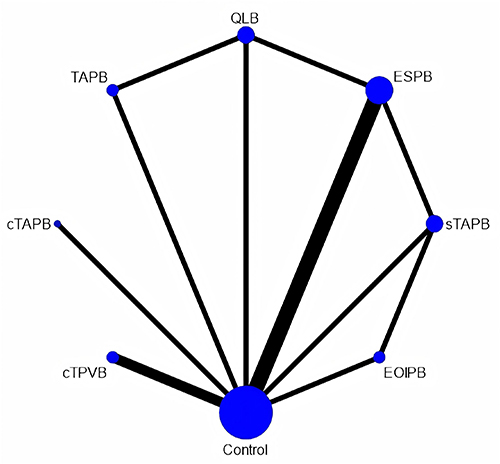 |
Figure 2 Network map. Abbreviations: ESPB, erector spinae plane block; QLB, quadratus lumborum block; TAPB, transversus abdominis plane block; sTAPB, subcostal TAPB; EOIPB, external oblique intercostal plane block; cTAPB, continuous TAPB; cTPVB, continuous thoracic paravertebral block. |
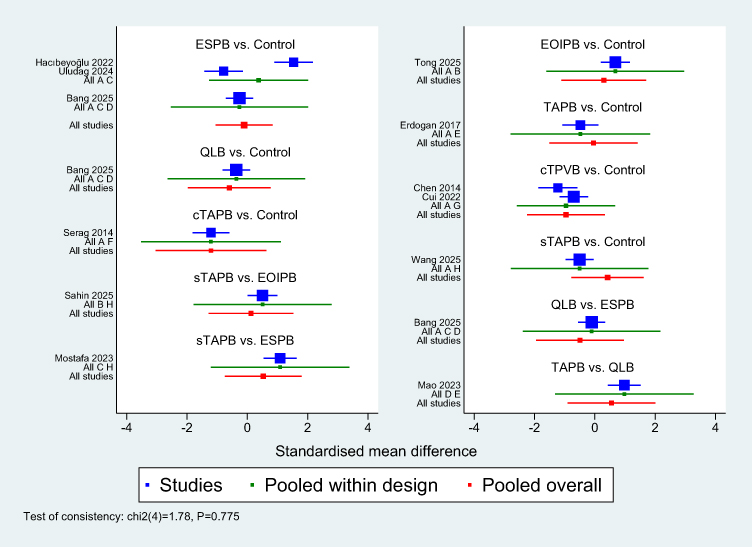 |
Figure 3 Forest plot. |
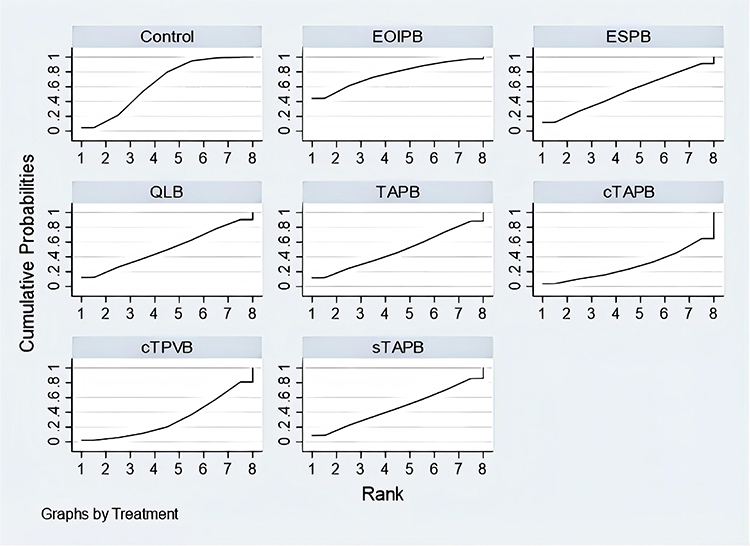 |
Figure 4 SUCRA. Control (64.8), EOIPB (77.0), ESPB (53.1), QLB (51.0), TAPB (48.6), cTAPB (28.1), cTPVB (30.8), sTAPB (46.4). Abbreviations: ESPB, erector spinae plane block; QLB, quadratus lumborum block; TAPB, transversus abdominis plane block; sTAPB, subcostal TAPB; EOIPB, external oblique intercostal plane block; cTAPB, continuous TAPB; cTPVB, continuous thoracic paravertebral block. |
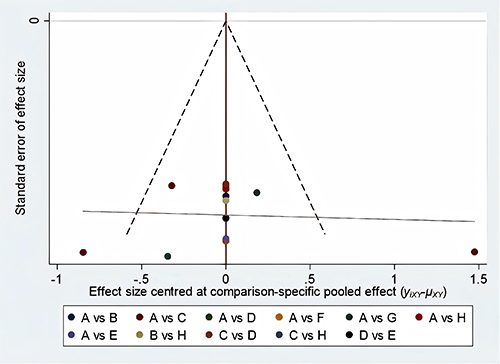 |
Figure 5 Funnel plot. |
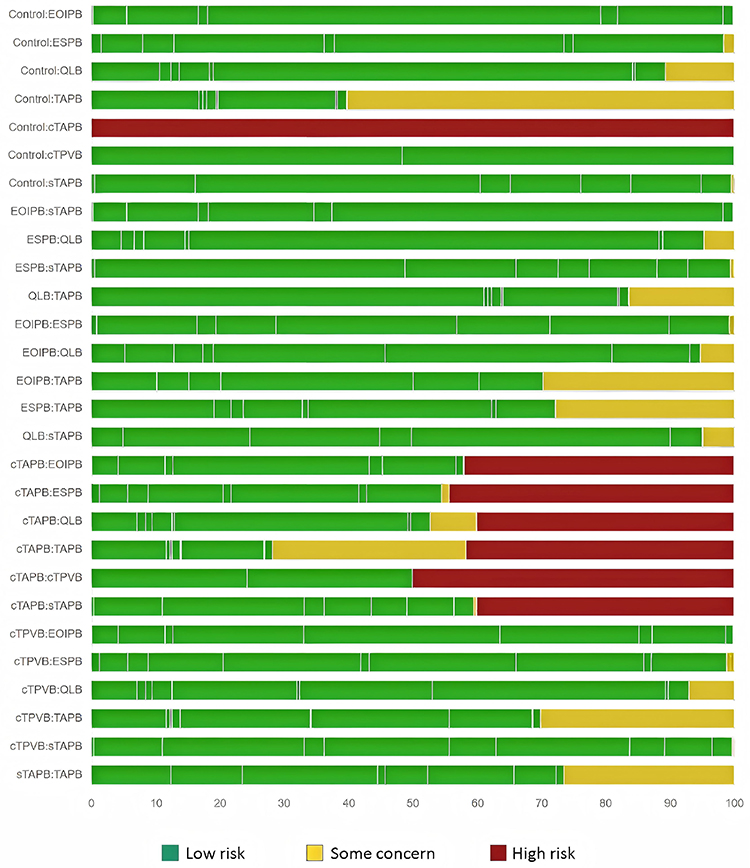 |
Figure 6 Risk of bias. |
Secondary Outcomes
Resting VAS at 6 h
Ten studies with 583 patients were included. The network geometry of eligible comparisons displayed complete. There were no significant global heterogeneity and local inconsistency could be found. The result of SUCRA showed that ESPB attained the lowest value (17.1), followed closely by TANB (41.7), and sTAPB (52.1), while EOIPB (55.9) and cTAPB (66.6) occupied the higher positions in the ranking. The netleague showed the difference in effect size between all treatments. All results were shown in Figure S2A–C, Table S2A and B.
Resting VAS at 12 h
Ten studies with 569 patients were included. The network geometry of eligible comparisons displayed complete. There were no significant global heterogeneity and local inconsistency could be found. The result of SUCRA showed that ESPB attained the lowest value (27.1), followed closely by sTAPB (37.0), and EOIPB (40.2), while cTPVB (59.1) and TAPB (60.2) occupied the higher positions in the ranking. The netleague showed the difference in effect size between all treatments. All results were shown in Figure S3A–C, Table S3A and B.
Resting VAS at 24 h
Thirteen studies with 839 patients were included. The network geometry of eligible comparisons displayed complete. There were no significant global heterogeneity and local inconsistency could be found. The result of SUCRA showed that TANB attained the lowest value (38.5), followed closely by cTAPB (44.5), and EOIPB (50.1), while TAPB (52.6) and cTPVB (54.2) occupied the higher positions in the ranking. The netleague showed the difference in effect size between all treatments. All results were shown in Figure S4A–C, Table S4A, and B.
Movement VAS at 6 h
Nine studies with 494 patients were included. The network geometry of eligible comparisons displayed complete. There were no significant global heterogeneity and local inconsistency could be found. The result of SUCRA showed that ESPB attained the lowest value (27.4), followed closely by cTPVB (47.8), and EOIPB (52.0), while TANB (54.4) and TAPB (55.0) occupied the higher positions in the ranking. The netleague showed the difference in effect size between all treatments. All results were shown in Figure S5A–C, Table S5A and B.
Movement VAS at 12 h
Ten studies with 563 patients were included. The network geometry of eligible comparisons displayed complete. There were no significant global heterogeneity and local inconsistency could be found. The result of SUCRA showed that ESPB attained the lowest value (25.4), followed closely by sTAPB (37.1), and EOIPB (40.8), while TAPB (59.8) and cTPVB (61.8) occupied the higher positions in the ranking. The netleague showed the difference in effect size between all treatments. All results were shown in Figure S6A–C, Table S6A and S6B.
Movement VAS at 24 h
Twelve studies with 750 patients were included. The network geometry of eligible comparisons displayed complete. There were no significant global heterogeneity and local inconsistency could be found. The result of SUCRA showed that TANB attained the lowest value (31.9), followed closely by EOIPB (47.1), and TAPB (51.5), while QLB (53.9) and cTPVB (60.9) occupied the higher positions in the ranking. The netleague showed the difference in effect size between all treatments. All results were shown in Figure S7A–C, Table S7A and B.
Postoperative Nausea and Vomiting (PONV)
Fourteen studies with 825 patients were included. The network geometry of eligible comparisons displayed complete. There were no significant global heterogeneity and local inconsistency could be found. The result of SUCRA showed that ESPB attained the lowest value (25.3), followed closely by TANB (29.6), and QLB (30.3), while sTAPB (66.2) and cTPVB (65.4) occupied the higher positions in the ranking. The netleague showed the difference in effect size between all treatments. All results were shown in Figure S8A–C, Table S8A and B.
Discussion
The results of our NMA revealed small differences in the efficacy of various regional analgesia techniques for managing postoperative pain following open hepatectomy. Notably, both cTAPB and cTPVB are more likely to reduce morphine consumption within the first 24 hours postoperatively, as suggested by the SUCRA rankings. However, the clinical differences were small when compared with other other interventions. Meanwhile, the analgesic effect of a single injection is not as prolonged as that achieved with continuous infusion of local anesthetics (LAs). The ESPB was shown to be an effective treatment for reducing both resting and movement VAS scores within the first 12 hours. ESPB effectively targets the sensory nerves supplying the thoracic region, thereby blocking both incisional and visceral pain, which results in superior analgesic effects compared to TAPB, sTAPB, cTAPB, TANB, and EOIPB. Furthermore, when compared to TPVB and QLB, ESPB may offer broader analgesic coverage due to the more extensive spread of local anesthetic within the muscle plane, potentially affecting multiple dermatomes and a larger area of pain reception. While TANB appeared to be more effective in reducing resting and movement VAS scores at 24 hours, it is important to note that the effectiveness of current nerve blocks may diminish over time, and the observed low VAS values could be attributed to the use of rescue analgesic medications. Although ESPB and TANB were associated with a reduced incidence of PONV, we do not recommend these techniques specifically for this purpose, as no direct causal relationship was established, and PONV is influenced by multiple factors. Additionally, our study found no evidence of global heterogeneity or local inconsistency; however, the overall levels of evidence were diminished by some studies lacking sufficiently rigorous methodologies (Table 4).
Currently, there are few studies that discuss the analgesic effects of peripheral nerve blocks in open partial hepatectomy. Abdildin’s research indicated that the TAPB decreased resting pain at 24 hours postoperatively; however, it did not reduce total opioid consumption and PONV. These findings are consistent with our own results, suggesting that the incisional pain following open surgery can be quite severe, and TAPB does not effectively enhance the quality of analgesia.34 Postoperative pain following open liver resection primarily arises from several sources. First, incisional pain occurs due to the tissue damage associated with abdominal incision, affecting the skin, muscles, and abdominal wall nerves, leading to localized discomfort.35 Second, visceral pain may result from irritation or injury to the intra-abdominal organs, particularly the liver and surrounding structures, which can elicit deep, dull pain in the abdominal cavity.36 Additionally, the postoperative inflammatory response contributes to pain by releasing inflammatory mediators that sensitize nociceptive pathways.37 Currently, there is considerable variation in the analgesic coverage provided by different regional anesthesia techniques, and not all methods are capable of fully addressing incisional pain. Additionally, some techniques may not be effective for managing visceral pain.
The ESPB involves the injection of LA into the plane superficial to the erector spinae muscles. This technique effectively targets the dorsal rami of the spinal nerves, providing analgesia for both somatic and visceral pain in the thoracic and abdominal regions.38 ESPB is associated with a wide analgesic coverage, making it particularly effective for managing postoperative pain.38 Its advantages include a low risk of complications and a straightforward technique, although potential risks such as infection, hematoma, and rare instances of pneumothorax should be considered.38 The TPVB involves the injection of LA into the paravertebral space, which is the area lateral to the vertebral column and contains the ventral and dorsal rami of the spinal nerves, as well as the sympathetic chain.39 By targeting this space, TPVB blocks the transmission of nociceptive signals from multiple spinal segments, effectively providing analgesia for somatic pain from the thoracic and abdominal walls.39 While TPVB is effective at providing segmental analgesia, it carries risks such as inadvertent vascular or pleural puncture, and complications can include unilateral block failure, hematoma, and neural injury.39
The TAPB involves injecting LA into the fascial plane between the transversus abdominis muscle and the internal oblique muscle, effectively blocking the lower intercostal, subcostal, and iliohypogastric nerves.40 The TAPB provides effective analgesia for the anterior abdominal wall, helping manage somatic pain associated with abdominal surgeries.40 The sTAPB is a variation of the TAPB, where LA is injected subcostally to block the nerves innervating the abdominal wall.19 This block is designed to provide targeted analgesia for the upper abdominal region and incisional pain following surgery.19 Nevertheless, like TAPB, its limitations lie in its primary focus on somatic pain, potentially insufficiently addressing visceral discomfort.19 The QLB involves the injection of LA in the proximity of the quadratus lumborum muscle, targeting the thoracic and lumbar nerves.41 This technique has the potential to provide analgesia for both the abdominal and flank regions, and providing analgesia for visceral pain.41
The TANB involves the injection of LA near the thoracoabdominal nerves. This technique is effective for providing analgesia primarily for incisional pain and is valuable for patients undergoing upper abdominal surgeries.42 The EOIPB entails injecting LA in the plane between the external oblique muscle and the underlying intercostal muscles.43 This technique targets the intercostal nerves, providing effective analgesia for the lateral and anterior thoracic wall and is particularly beneficial in managing postoperative pain following thoracic and abdominal surgery.43 Additionally, cTAPB and cTPVB allows for continuous infusion of LA, providing sustained analgesia for abdominal surgery patients. However, potential complications include catheter-related issues leading to infection or catheter misplacement, which must be monitored closely for optimal patient outcomes and careful tuning of local anesthetic dosages to avoid systemic toxicity.
Based on the above review, it is evident that the ESPB may be a suitable regional analgesia technique for patients undergoing open liver resections, as it offers a relatively broad coverage of incisional pain while also alleviating visceral pain. The TPVB may have better overall efficacy than ESPB, the comparison of VAS scores within the first 12 hours does not support its use as the preferred option for this specific surgical population. Moreover, the other analgesic techniques evaluated did not show significant advantages over ESPB. Additionally, the continuous infusion techniques appear to provide a more effective strategy for reducing morphine consumption. Therefore, future research should focus on exploring the efficacy of continuous infusion protocols within the context of ESPB to further enhance postoperative pain management in liver surgery patients.
Limitations
Despite the comprehensive nature of this systematic review and network meta-analysis, there are several limitations to consider. Firstly, the difference of the included studies may affect the consistency of the findings, as variations in study design, patient populations, and analgesia protocols can introduce bias. Secondly, our findings are specifically applicable to open hepatectomy and may not be directly extrapolated to laparoscopic procedures, necessitating further research in that area. Thirdly, while efforts were made to include all relevant studies, there may still be unpublished data or ongoing trials that could contribute to the findings, limiting the comprehensiveness of our analysis. Finally, the emergence of new regional blocks and analgesic strategies may rapidly change the landscape of pain management in open hepatectomy, meaning that our findings could become outdated as new evidence emerges.
Conclusions
Our systematic review and NMA indicated that cTAPB and cTPVB ranked higher in terms of reducing morphine consumption within 24 hours, but there was no significant clinical difference between these techniques and other interventions. Additionally, the ESPB was more likely to reduce pain scores within the first 12 hours postoperatively and decrease the incidence of PONV within 24 hours. Nevertheless, the certainty of evidence for these findings remains low to moderate, and further high-quality randomized controlled trials are warranted to confirm their clinical utility.
Funding
This work was supported by the Provincial Natural Science Foundation of Gansu (25JRRA287), the Gansu Provincial Anesthesia and Brain Function Clinical Medical Research Center project (21JR7RA675), and the Gansu Province Key Talent Project: Talent Cultivation in Anesthesiology of Gansu Province Based on a Diversified Innovative Training System (2023RCXM13).
Disclosure
The authors declare that they have no competing interests.
References
1. Yagi S, Hirata M, Miyachi Y. et al. Liver Regeneration after Hepatectomy and Partial Liver Transplantation. Int J Mol Sci. 2020;21(21):8414. doi:10.3390/ijms21218414
2. Rouxel P, Beloeil H. Enhanced recovery after hepatectomy: a systematic review. Anaesth Crit Care Pain Med. 2019;38(1):29–13. doi:10.1016/j.accpm.2018.05.003
3. Dudek P, Zawadka M, Andruszkiewicz P, et al. Postoperative Analgesia after Open Liver Surgery: systematic Review of Clinical Evidence. J Clin Med. 2021;10(16):3662. doi:10.3390/jcm10163662
4. Kang RA, Ko JS. Living liver donor pain management. Curr Opin Organ Transplant. 2023;28(6):391–396. doi:10.1097/MOT.0000000000001099
5. Gavriilidis P, Roberts KJ, Sutcliffe RP. Local anaesthetic infiltration via wound catheter versus epidural analgesia in open hepatectomy: a systematic review and meta-analysis of randomised controlled trials. HPB. 2019;21(8):945–952. doi:10.1016/j.hpb.2019.02.007
6. Cao Y, Shen J. Meta-analysis of multimodal analgesia for reducing postoperative wound pain after hepatectomy for hepatocellular carcinoma. Sci Rep. 2025;15(1):15494. doi:10.1038/s41598-025-00069-4
7. Li J, Pourrahmat MM, Vasilyeva E, et al. Efficacy and Safety of Patient-controlled Analgesia Compared With Epidural Analgesia After Open Hepatic Resection: a Systematic Review and Meta-analysis. Ann Surg. 2019;270(2):200–208. doi:10.1097/SLA.0000000000003274
8. Qian J, Wang X. Efficacy of erector spinae plane block for postoperative analgesia after liver surgeries: a systematic review and meta-analysis. BMC Anesthesiol. 2024;24(1):246. doi:10.1186/s12871-024-02635-1
9. Page MJ, Moher D, Bossuyt PM, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372:n160. doi:10.1136/bmj.n160
10. Adams MCB, Sward KA, Perkins ML, et al. Standardizing research methods for opioid dose comparison: the NIH HEAL morphine milligram equivalent calculator. Pain. 2025;166(8):1729–1737. doi:10.1097/j.pain.0000000000003529
11. Higgins JP, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. doi:10.1136/bmj.d5928
12. Papakonstantinou T, Nikolakopoulou A, Higgins JPT, et al. CINeMA: software for semiautomated assessment of the confidence in the results of network meta-analysis. Campbell Syst Rev. 2020;16(1):e1080. doi:10.1002/cl2.1080
13. Nikolakopoulou A, Higgins JPT, Papakonstantinou T, et al. CINeMA: an approach for assessing confidence in the results of a network meta-analysis. PLoS Med. 2020;17(4):e1003082. doi:10.1371/journal.pmed.1003082
14. Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):9246. doi:10.1136/bmj.39489.470347.AD
15. Luo D, Wan X, Liu J, et al. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res. 2018;27(6):1785–1805. doi:10.1177/0962280216669183
16. Wan X, Wang W, Liu J, et al. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14:135. doi:10.1186/1471-2288-14-135
17. Guo JG, Li HL, Pei QQ, et al. The analgesic efficacy of subcostal transversus abdominis plane block with Mercedes incision. BMC Anesthesiol. 2018;18(1):36. doi:10.1186/s12871-018-0499-3
18. Mao Y, Zhao W, Hao M, et al. Ultrasound-Guided Quadratus Lumborum Block at the Lateral Supra-Arcuate Ligament versus Subcostal Transversus Abdominis Plane Block for Postoperative Analgesia Following Open Hepatectomy: a Randomized Controlled Trial. J Pain Res. 2023;16:1429–1440. doi:10.2147/JPR.S404810
19. Mostafa M, Mousa MS, Hasanin A, et al. Erector spinae plane block versus subcostal transversus abdominis plane block in patients undergoing open liver resection surgery: a randomized controlled trial. Anaesth Crit Care Pain Med. 2023;42(1):101161. doi:10.1016/j.accpm.2022.101161
20. Wang C, Xu W, Li Y, et al. Effects of Ultrasound-Guided Oblique Subcostal Transversus Abdominis Block Combined with Patient-Controlled Intravenous Analgesia on Analgesia and Early Recovery after Open Hepatectomy: a Randomized Controlled Clinical Trial. Clin J Pain. 2025. doi:10.1097/AJP.0000000000001338
21. Hacıbeyoğlu G, Topal A, Küçükkartallar T, et al. Investigation of the effect of ultrasonography-guided bilateral erector spinae plane block on postoperative opioid consumption and pain scores in patients undergoing hepatectomy: a prospective, randomized, controlled study. Sao Paulo Med J. 2022;140(1):144–152. doi:10.1590/1516-3180.2020.0757.R1.08062021
22. Huang HM, Chen RX, Zhu LM, et al. Combined use of transversus abdominis plane block and laryngeal mask airway during implementing ERAS programs for patients with primary liver cancer: a randomized controlled trial. Sci Rep. 2020;10(1):14892. doi:10.1038/s41598-020-71477-x
23. Chen H, Liao Z, Fang Y, et al. Continuous right thoracic paravertebral block following bolus initiation reduced postoperative pain after right-lobe hepatectomy: a randomized, double-blind, placebo-controlled trial. Reg Anesth Pain Med. 2014;39(6):506–512. doi:10.1097/AAP.0000000000000167
24. Gungor H, Ince A, Ciftci B, et al. Ultrasound-Guided Modified Thoracoabdominal Nerve Block Through Perichondrial Approach for Postoperative Analgesia Management in Living Liver Donors: a Randomized, Prospective, Controlled Study. Clin Transplant. 2025;39(9):e70224. doi:10.1111/ctr.70224
25. Fu J, Zhang G, Qiu Y. Erector spinae plane block for postoperative pain and recovery in hepatectomy: a randomized controlled trial. Medicine. 2020;99(41):e22251. doi:10.1097/MD.0000000000022251
26. Tong C, Li Y, Du F, et al. Ultrasound-guided external oblique intercostal plane block with ropivacaine for analgesia after open hepatectomy- a randomized controlled study. Anesthesiology. 2025. doi:10.1097/ALN.0000000000005846
27. Cui XL, Xu N, Zhang ZY, et al. Ultrasound-Guided Continuous Thoracic Paravertebral Block Improves Patient’s Quality of Recovery After Open Hepatectomy: a Randomized, Double-Blind, Placebo-Controlled Trial. Chin Med Sci J. 2022;37(1):15–22.
28. Serag Eldin M, Mahmoud F, El Hassan R, et al. Intravenous patient-controlled fentanyl with and without transversus abdominis plane block in cirrhotic patients post liver resection. Local Reg Anesth. 2014;7:27–37. doi:10.2147/LRA.S60966
29. Erdogan MA, Ozgul U, Uçar M, et al. Effect of transversus abdominis plane block in combination with general anesthesia on perioperative opioid consumption, hemodynamics, and recovery in living liver donors: the prospective, double-blinded, randomized study. Clin Transplant. 2017;31(4). doi:10.1111/ctr.12931
30. Kıtlık A, Erdogan MA, Ozgul U, et al. Ultrasound-guided transversus abdominis plane block for postoperative analgesia in living liver donors: a prospective, randomized, double-blinded clinical trial. J Clin Anesth. 2017;37:103–107. doi:10.1016/j.jclinane.2016.12.018
31. Bang YJ, Yoo SY, Kang R, et al. Comparison of three different methods of postoperative analgesic effects in laparoscopic major liver resection (systemic analgesia vs. erector spinae plane block vs. quadratus lumborum block): a randomized controlled trial. J Clin Anesth. 2025;107:112019. doi:10.1016/j.jclinane.2025.112019
32. Sahin T, Kavakli AS, Eren E, et al. Ultrasound-guided external oblique intercostal plane block versus subcostal transversus abdominis plane block for postoperative analgesia in living liver donors: a prospective randomized trial. J Clin Anesth. 2025;106:111971. doi:10.1016/j.jclinane.2025.111971
33. Uludag Yanaral T, Gungor H, Ince A, et al. Ultrasound-guided bilateral erector spinae plane block in the management of postoperative analgesia in living liver donors: a randomized, prospective study. Minerva Anestesiol. 2024;90(12):1082–1089. doi:10.23736/S0375-9393.24.18085-6
34. Abdildin Y, Tapinova K, Nugumanova M, et al. Transversus abdominis plane block in adult open liver surgery patients: a systematic review with meta-analysis of randomized controlled trials. J Visc Surg. 2023;160(4):253–260. doi:10.1016/j.jviscsurg.2022.11.003
35. Brennan TJ, Zahn PK, Pogatzki-Zahn EM. Mechanisms of incisional pain. Anesthesiol Clin North Am. 2005;23(1):1–20. doi:10.1016/j.atc.2004.11.009
36. Grundy L, Erickson A, Brierley SM. Visceral Pain. Annu Rev Physiol. 2019;81:261–284. doi:10.1146/annurev-physiol-020518-114525
37. Li Y, Yang M, Wu F, et al. Mechanism of electroacupuncture on inflammatory pain: neural-immune-endocrine interactions. J Tradit Chin Med. 2019;39(5):740–749.
38. Oostvogels L, Weibel S, Meißner M, et al. Erector spinae plane block for postoperative pain. Cochrane Database Syst Rev. 2024;2(2):CD013763. doi:10.1002/14651858.CD013763
39. Slinchenkova K, Lee K, Choudhury S, et al. A Review of the Paravertebral Block: benefits and Complications. Curr Pain Headache Rep. 2023;27(8):203–208. doi:10.1007/s11916-023-01118-1
40. Tran DQ, Bravo D, Leurcharusmee P, et al. Transversus Abdominis Plane Block: a Narrative Review. Anesthesiology. 2019;131(5):1166–1190. doi:10.1097/ALN.0000000000002842
41. Elsharkawy H, El-Boghdadly K, Barrington M. Quadratus Lumborum Block: anatomical Concepts, Mechanisms, and Techniques. Anesthesiology. 2024;141(6):1226. doi:10.1097/ALN.0000000000005221
42. Tanaka N, Ida M, Suzuka T, et al. Modified thoracoabdominal nerves block through perichondrial approach for surgical patients: a scoping review. BMC Anesthesiol. 2025;25(1):258. doi:10.1186/s12871-025-03133-8
43. Erskine RN, White L. A review of the external oblique intercostal plane block - a novel approach to analgesia for upper abdominal surgery. J Clin Anesth. 2022;82:110953. doi:10.1016/j.jclinane.2022
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Psychological Interventions on Abstinence in Patients with Alcohol Use Disorder: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials
Zhang P, Zhan J, Wang S, Tang Y, Chen H, Wang Y, Wei X, Wen H, Pan T, Chen Z, Tang C, Xu N, Lu L
Neuropsychiatric Disease and Treatment 2022, 18:1815-1830
Published Date: 23 August 2022
Effect of Exercise Interventions on Health-Related Quality of Life in Patients with Fibromyalgia Syndrome: A Systematic Review and Network Meta-Analysis
Zhang KD, Wang LY, Zhang ZH, Zhang DX, Lin XW, Meng T, Qi F
Journal of Pain Research 2022, 15:3639-3656
Published Date: 22 November 2022
Different Intensities of Evening Exercise on Sleep in Healthy Adults: A Systematic Review and Network Meta-Analysis
Yue T, Liu X, Gao Q, Wang Y
Nature and Science of Sleep 2022, 14:2157-2177
Published Date: 14 December 2022
Efficacy of Acupuncture-Related Therapy for Migraine: A Systematic Review and Network Meta-Analysis
Liu Y, Wang Y, Mi C, Wang Z, Han Y, Qi X, Ding X
Journal of Pain Research 2024, 17:1107-1132
Published Date: 15 March 2024
Effect of Exercise Interventions for Rheumatoid Arthritis: A Systematic Review and Network Meta-Analysis of Randomised Controlled Trials
Zhang Y, He Z, Yin Z, Wang J, Gao W, Jie L
Journal of Pain Research 2025, 18:5109-5126
Published Date: 30 September 2025