")
Back to Journals » International Journal of General Medicine » Volume 15
Assessment of the Community Pharmacists’ Knowledge and Attitudes Toward Pain and Pain Management in Saudi Arabia
Authors Alorfi NM , Ashour AM , Algarni AS , Alsolami FA, Alansari AM, Tobaiqy M
Received 21 August 2022
Accepted for publication 28 November 2022
Published 7 December 2022 Volume 2022:15 Pages 8527—8537
DOI https://doi.org/10.2147/IJGM.S387066
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Nasser M Alorfi,1 Ahmed M Ashour,1 Alanood S Algarni,1 Faris A Alsolami,2 Abdulrhman M Alansari,3 Mansour Tobaiqy4
1Department of Pharmacology and Toxicology, College of Pharmacy, Umm Al-Qura University, Makkah, Saudi Arabia; 2Khulais General Hospital, Ministry of Health, Makkah, Saudi Arabia; 3Alsafiah Health Care Center, Ministry of Health, Madinah, Saudi Arabia; 4Department of Pharmacology, College of Medicine, University of Jeddah, Jeddah, Saudi Arabia
Correspondence: Nasser M Alorfi, Umm Al-Qura University, Al Abdeyah, Mecca, 24381, Saudi Arabia, Email [email protected]
Background: Pain is a global health issue that affects an individual’s quality of life. Its alleviation and management will enhance patients’ experience. Community pharmacists can help manage pain severity through their valuable roles in medical teams and by managing the consequences of pain.
Objective: This study aimed to evaluate community pharmacists’ knowledge and attitudes toward pain and pain management in Saudi Arabia.
Methods: A cross-sectional study was performed to evaluate community pharmacists’ knowledge and attitudes toward pain and pain management in Saudi Arabia. Pharmacists aged ≥ 21 years, with a degree in pharmacy were included in this study. Each respondent participated in an online survey covering cancer-oriented pain and assessment of pain; pharmacology; abuse of substances; and physical dependence. An independent t-test and One-way ANOVA, with least significant difference as a post-hoc test, were employed, in addition to the General Linear Regression Model using Main Effect as the model.
Results: This study revealed that the pain-related knowledge and attitude among community pharmacists in Saudi Arabia were inadequate. Age (p = 0.003), work experience (p = 0.036), nature of work (p = 0.001), and work location (p = 0.003) were determined as significant factors affecting their overall knowledge and attitude toward pain.
Conclusion: Overall, attempts to expand community pharmacists’ knowledge and foster an appropriate attitude toward pain management among them in Saudi Arabia are highly recommended. Additional academic courses, studies, and tailored neuroscience courses will improve their awareness and knowledge of pain and pain management.
Keywords: pharmacist, pain, knowledge, attitude, practice
Introduction
Pain is a multidimensional experience accompanied mainly by actual or potential tissue damage affecting the quality of life.1 Pain is a subjective feeling, as no accurate or ideal tool exists to measure the level of pain experienced by a patient. To measure pain, a number of assessment scales are utilized such as the visual analog scale, numerical rating scale, verbal rating scale, brief pain inventory, and others.2–4 Pain is considered to be an indicator of many health issues.5
Both pharmacological and non-pharmacological interventions could help to reduce the severity of pain.6,7 It can be managed with a wide range of medications such as acetaminophen, non-steroidal anti-inflammatory drugs (NSAIDs), and opioids.8,9 Moreover, several types of pain can be alleviated and managed by healthcare providers to lessen the experience of pain.10,11 Pain can be classified according to its duration and other causative factors.12 The International Association for the Study of Pain (IASP) stated that 20% of adults experience pain and another 10% are diagnosed with chronic pain each year globally.13 However, many healthcare providers in a range of countries possess inadequate knowledge and attitude toward managing pain.14–17 The leading factor contributing to this is a lack of proper training and education on pain management available to healthcare professionals.14,18,19 Knowledge and attitudes toward pain management, especially among physicians and nurses, have been studied extensively.18,20,21 Several studies have focused on the knowledge and attitudes toward pain management possessed by medicine, nursing, and pharmacy undergraduate students.22–24
Pharmacists plays a critical role in providing valuable information to other healthcare professionals on suitable medical therapies and interventions that target drug difficulties.25,26 A considerable amount of literature has been published on pharmacist-led educational and medication reviews, which are effective for pain management.27 However, to the best of our knowledge, limited studies have been performed on the knowledge and attitudes of community pharmacists in terms of pain management. Thus, this research aims to evaluate the knowledge and attitudes of pharmacists in Saudi Arabia regarding pain and pain management.
Methods
Research Design
A cross-sectional study was conducted online via Google Form. The link to the survey was sent via community pharmacy chain managers across different geographical regions in Saudi Arabia from January to April 2022. Pharmacists aged at least 21 years old with a degree in pharmacy were included in this study. The survey was anonymous with no possibility of participant identification.
Sample Size and Sampling Procedure
The sample size was calculated based on the total number of pharmacists working in private sector in Saudi Arabia which is around 23.000 pharmacists.28 The statistical program Raosoft was used to determine the sample size at a 95% confidence interval, and a 5% margin of error; the estimated sample size was 344.
The Questionnaire
The socio-demographic variables collected for this study were age, gender, work experience, educational level, nature, and work location. These variables were assessed for their possible association with overall knowledge and attitudes toward pain and pain management. Each respondent participated in an online survey on the topic of knowledge and perspectives of pain established by Ferrell.29 The survey questionnaire comprised two main sections: twenty-two true-or-false questions and fifteen multiple-choice questions. The thirty-seven questions were divided into four domains: cancer-related and assessment of pain, pharmacology, substance abuse, and physical dependence. The survey was piloted on a sufficient sample of community pharmacists and validated by two assistants of pharmacology at Umm Al-Qura University, Mecca, Saudi Arabia for its for testing applicability and reliability of the questionnaire.
Statistical Analysis
Data were assessed using IBM SPSS version 23 (IBM Corp., Armonk, N.Y., USA) and GraphPad Prism version 9.3.18 (GraphPad Software, Inc., San Diego, CA, USA). Categorical and nominal variables were presented in the form of counts and percentages. Continuous variables were presented by mean and standard deviation. The total score of The Knowledge and Attitudes Survey Regarding Pain (KASRP) was determined using a simple additive method, followed by conversion to a hundred-point scale. In addition, four parts were presented: Cancer-related pain (Q05, Q23, Q25, Q28, Q30), Pain assessment (Q01-Q04, Q12, Q31, Q32), Pharmacology (Q06-Q11, Q13-Q21, Q24, Q26-Q29, Q34-Q35, Q37), and Substance abuse and physical dependence (Q20, Q22, Q33, Q36).
The levels of pharmacists’ knowledge of and attitudes toward pain were classified as: Good (≥ 75% KASRP total score), Fair (50–75% KASRP total score), or Poor (≤ 50% KASRP total score). An independent t-test and One-way ANOVA, with Least Significant Difference (LSD) as a post-hoc test, assuming the distribution was usual, were employed to compare the two groups’ means and more than two groups. Otherwise, Games-Howell was utilized as an alternative for LSD as the post-hoc test. In addition, the General Linear Regression Model (GLRM), using Main Effect as the model, was used to identify significant predictors. Lastly, a p-value of < 0.05 was used to reject the null hypothesis.
Ethical Consideration
The protocol for the study was reviewed and approved by the ethical scientific research committee at Umm Al-Qura University (approval number (HAPO-02-K-012-2022-01-922).
Results
As shown in Table 1, 601 participants (82.0% males, 18.0% females) took part in this study. Almost half (47.9%) of them were aged between 27 and 32 years old, 39.6% were more than 32 years old, and the remaining 12.5% were aged between 21 and 26 years old. Just over one-third (35.9%) were pharmacy graduates with 5 to 10 years of experience, followed by 34.3% with more than ten years of experience, and 28.0% with less than five years of experience. A small percentage (1.8%) were graduates without experience. Eighty-seven percent of the participants graduated with a bachelor’s degree in pharmacy, followed by 6.8% who were postgraduates in pharmacy, 4.0% who had a diploma in pharmacy, and 1.7% who were still pharmacy students. The majority (83.0%) of the participants were working in the private sectors, such as community pharmacies, polyclinics, and pharmaceutical companies, and the rest were working in other sectors such as government (13.3%), university (3.3%), stores (0.2%), or not at all (0.2%).
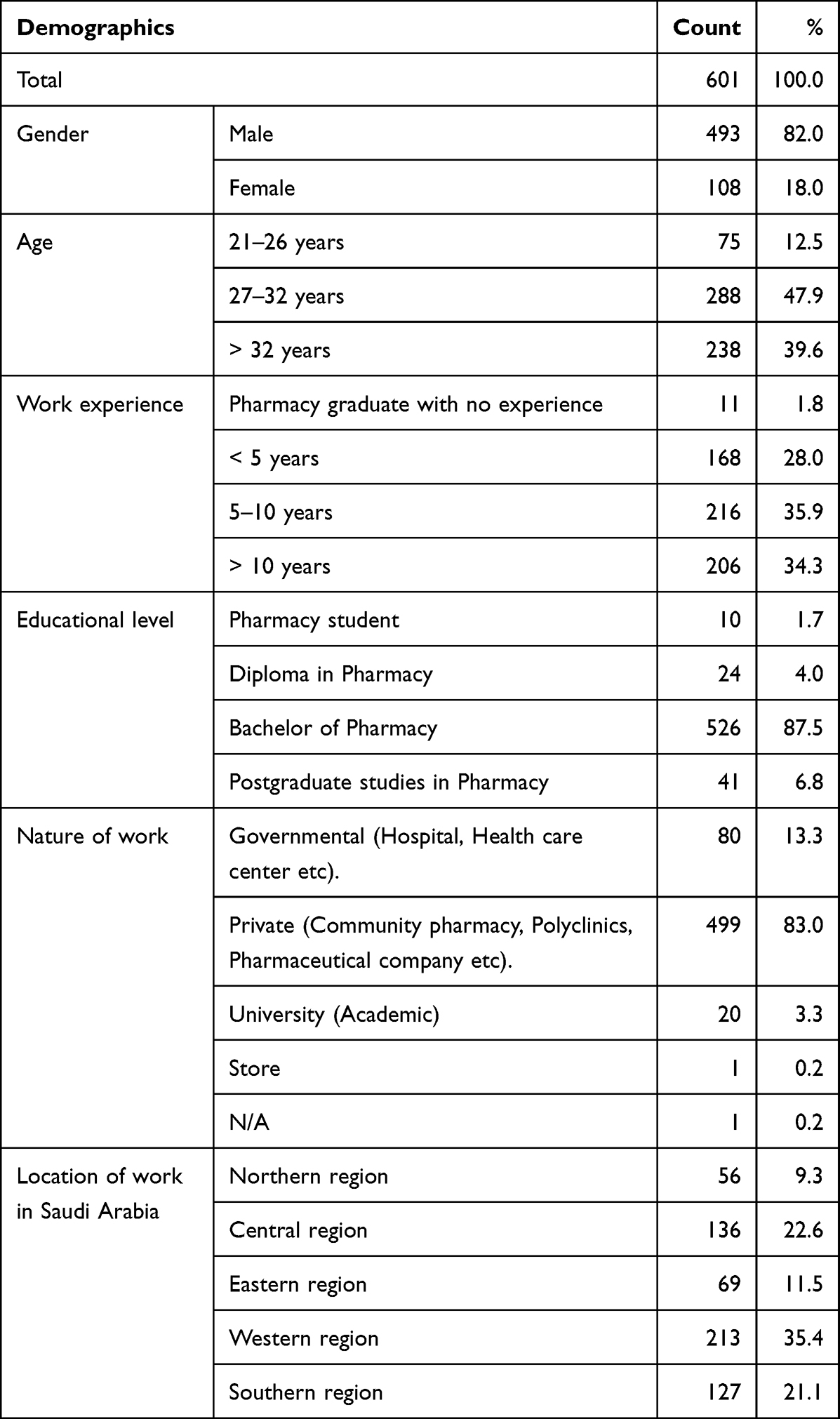 |
Table 1 Socio-Demographic Characteristics of the Study Participants |
Location-wise, 35.4% of the participants came from the Western region, followed by 22.6% from the Central region, 21.1% from the Southern region, 11.5% from the Eastern region, and 9.3% from the Northern region.
The first part of the questionnaire comprised of true-or-false questions regarding the knowledge and attitudes of pharmacists toward pain, as shown in Figure 1. The majority of the participants answered the following true-or-false questions correctly:
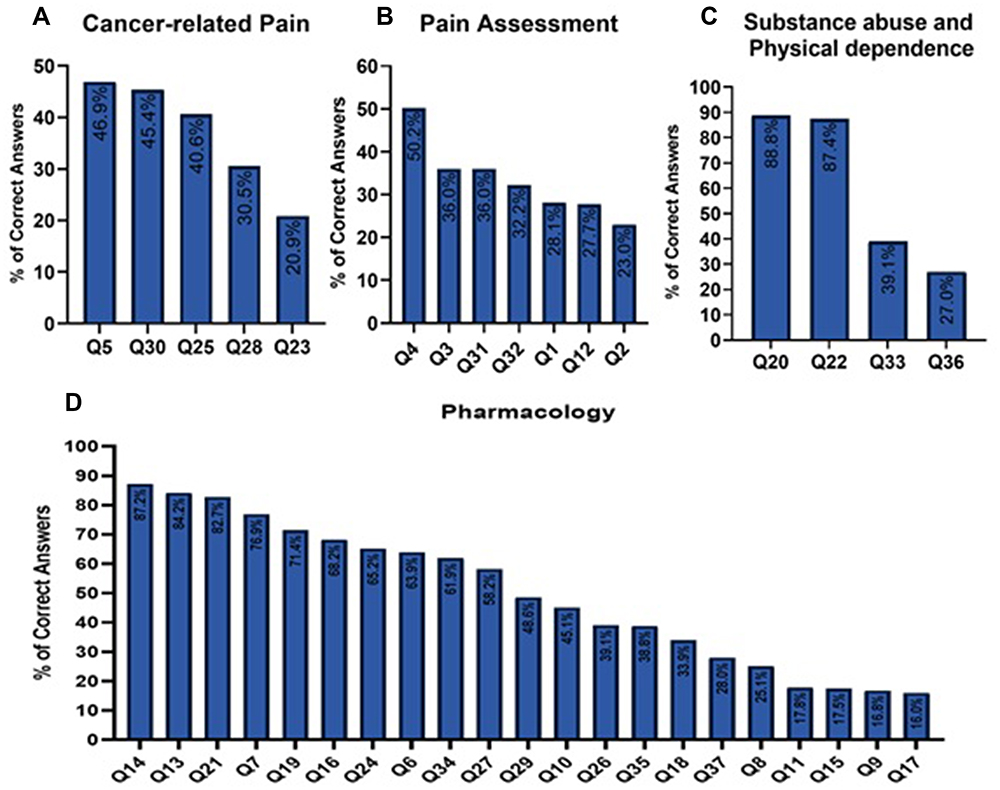 |
Figure 1 Percentage of correct responses obtained from the study participants for questions on (A) cancer-related pain, (B) pain assessment, (C) substance abuse and physical dependence, and (D) pain-related pharmacology. |
Q14: After an initial dose of opioid analgesic is given, subsequent doses should be adjusted in accordance with the individual patient’s response (87.2%).
Q20: Narcotic/opioid addiction is defined as a chronic neurobiologic disease, characterized by behaviors that include one or more of the following: impaired control over drug use, compulsive use, continued use despite harm, and craving (86.9%).
Q22: Sedation assessment is recommended during opioid pain management because excessive sedation precedes opioid-induced respiratory depression (85.5%).
Q13: Patient’s spiritual beliefs may lead them to think pain and suffering are necessary (84.2%).
Q21: The term “equianalgesia” means approximately equal analgesia and is used when referring to the doses of various analgesics that provide approximately the same amount of pain relief (82.7%).
Q07: Combining analgesics that work by different mechanisms (eg, combining an NSAID with an opioid) may result in better pain control with fewer side effects than using a single analgesic agent (76.8%).
Q19: Benzodiazepines are not effective pain relievers and are rarely recommended as part of an analgesic regiment (71.4%).
Q16: Vicodin (hydrocodone 5 mg + acetaminophen 300 mg) PO is approximately equal to 5–10 mg of morphine PO (68.2%).
Q06: Respiratory depression rarely occurs in patients who have been receiving stable doses of opioids over a period of months (63.9%).
The second part of the questionnaire consisted of multiple-choice questions on knowledge and attitudes toward pain, as illustrated in Figure 1. The majority of the participants answered the following questions correctly:
Q24: Intravenous route administration of opioid analgesics for patients with brief, severe pain of sudden onset such as trauma or post-operative pain (65.2%).
Q34: The time to peak effect for morphine given IV is 15 minutes (61.9%).
Q27: Analgesics for post-operative pain should initially be given around the clock on a fixed schedule (58.2%).
Despite not being answered by the majority of the participants correctly, the highest number of correct answers was noted on the following questions:
Q29: The most likely reason a patient with pain would request increased doses of pain medication is that the patient is experiencing increased pain (48.6%).
Q30: Ibuprofen, hydromorphone, and gabapentin are useful for the treatment of cancer pain (40.6%).
Q35: The time to peak effect for orally administered morphine is 1–2 hours (38.8%).
Q33: There is about 5–15% likelihood of developing pain in patients with problems related to alcohol and/or drug abuse problems (38.3%).
Q32: Patients should be individually assessed to determine cultural influences as the best approach for cultural considerations in caring for patients in pain (29.8%).
The survey was divided into four parts to evaluate the knowledge and attitudes of pharmacists with regard to pain management, as mentioned in Table 2. In terms of correct answers, questions on substance abuse and physical dependence scored the highest at 59.28 ± 20.3, followed by pharmacology with 49.83 ± 10.4, cancer-related pain with 32.95 ± 19.8, and pain assessment with 30.81 ± 19.0. Overall, slightly more than three-quarters (75.7%) of the participants were deemed to have poor knowledge and attitudes regarding pain, followed by 24.1% with fair scores and only 0.2% with a good score. The results of Cronbach’s alpha revealed the following scores for each part: 0.204 for pain assessment, 0.143 for pharmacology, −0.019 for substance abuse and physical dependence, and −0.114 for cancer-related pain. Each socio-demographic factor was correlated with overall knowledge and attitudes toward pain management, as exemplified in Table 3. Age (p = 0.003), work experience (p = 0.036), nature of work (p = 0.001), and work location (p = 0.003) were found to be significant factors affecting the pharmacists’ overall knowledge and attitudes toward pain. Test of between-subject effects, as provided in Table 4, revealed that the pharmacists’ overall knowledge and attitudes regarding pain were significantly influenced by the nature of their work, as well as the work location. Table 4 describes how each variable contributes to overall knowledge and attitude toward pain. The results showed that there is a significant difference in the overall knowledge and attitude regarding pain between the participants working in the Central (p = 0.015), Eastern (p = 0.021), and Western (p = 0.001) regions, and those in the Southern region. Regarding the nature of the work, there was no significant differences in the knowledge and attitudes of those working for the government (p = 0.251) or privately (p = 0.508), compared to those working in the university. The detailed parameter estimates for knowledge and attitude regarding pain management are explained in Table 5. Convergent validity results revealed a significant correlation between each domain and the overall knowledge and attitude regarding pain (p < 0.001 for each of the four domains), as exemplified in Table 6.
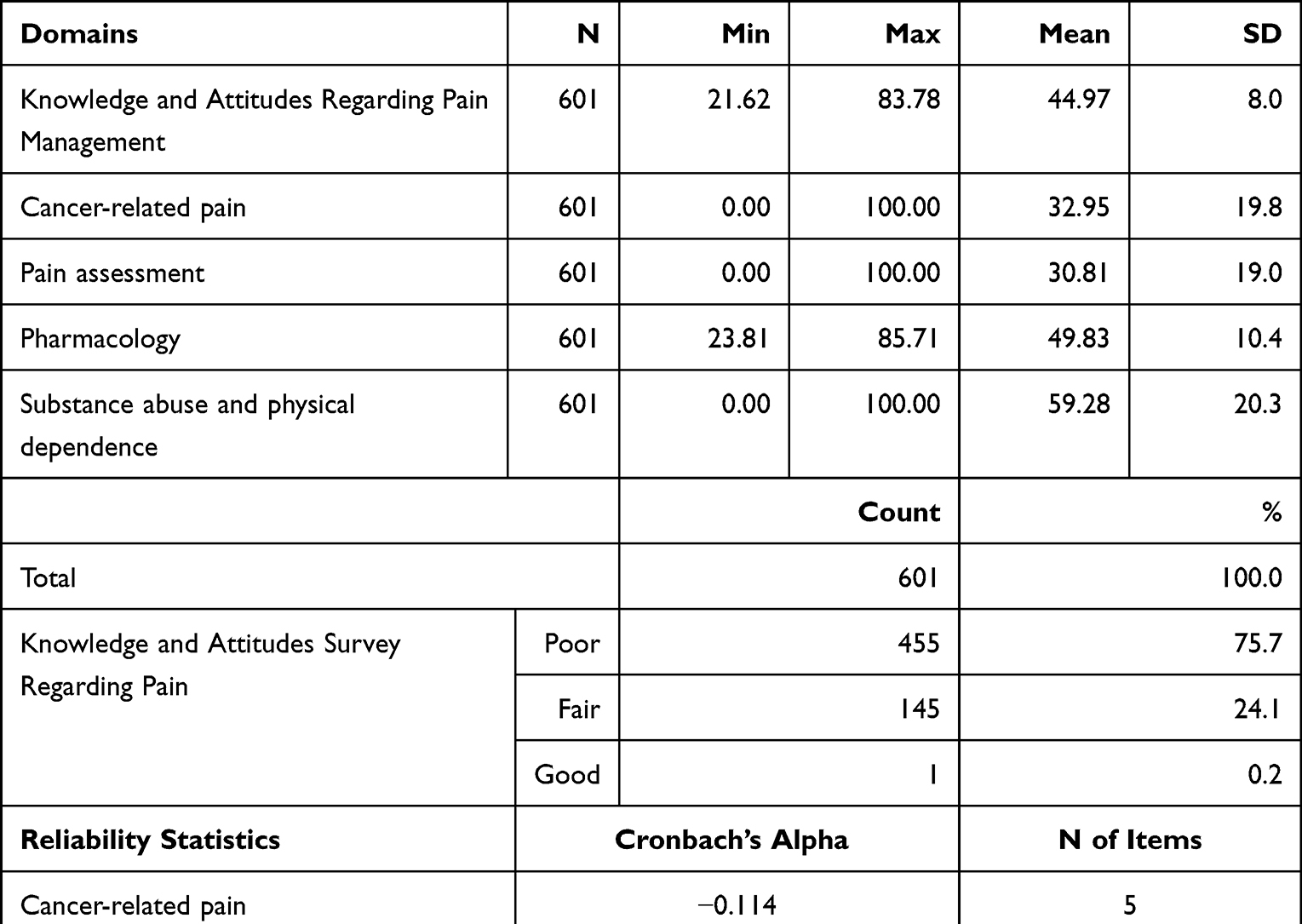 |
Table 2 Participant Scores and Reliability Statistics on Knowledge and Attitude on Pain Management |
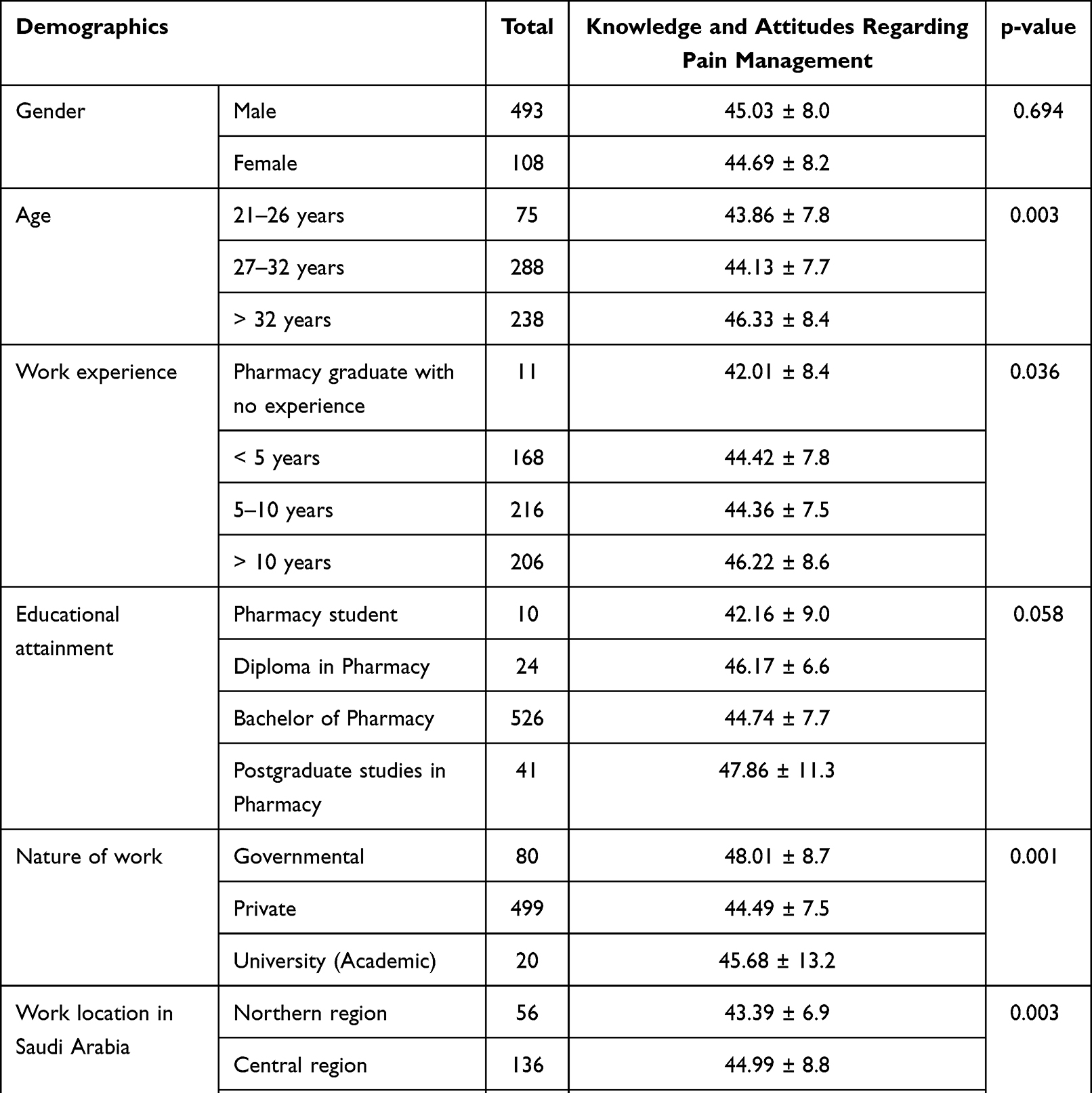 |
Table 3 Correlation Between Socio-Demographic Factors and Knowledge and Attitude Towards Pain Management |
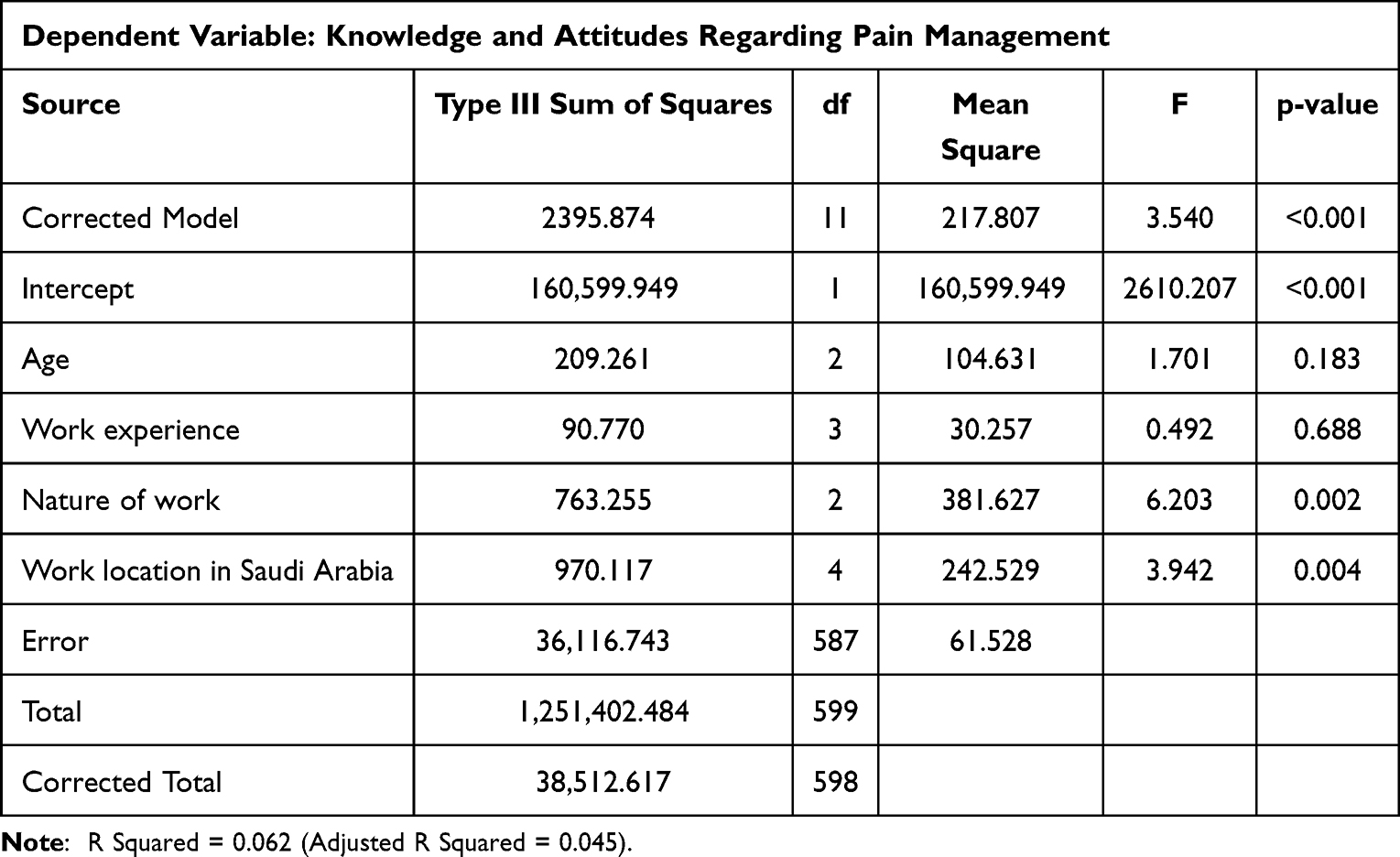 |
Table 4 Tests of Between-Subjects Effects for Knowledge and Attitude Regarding Pain Management |
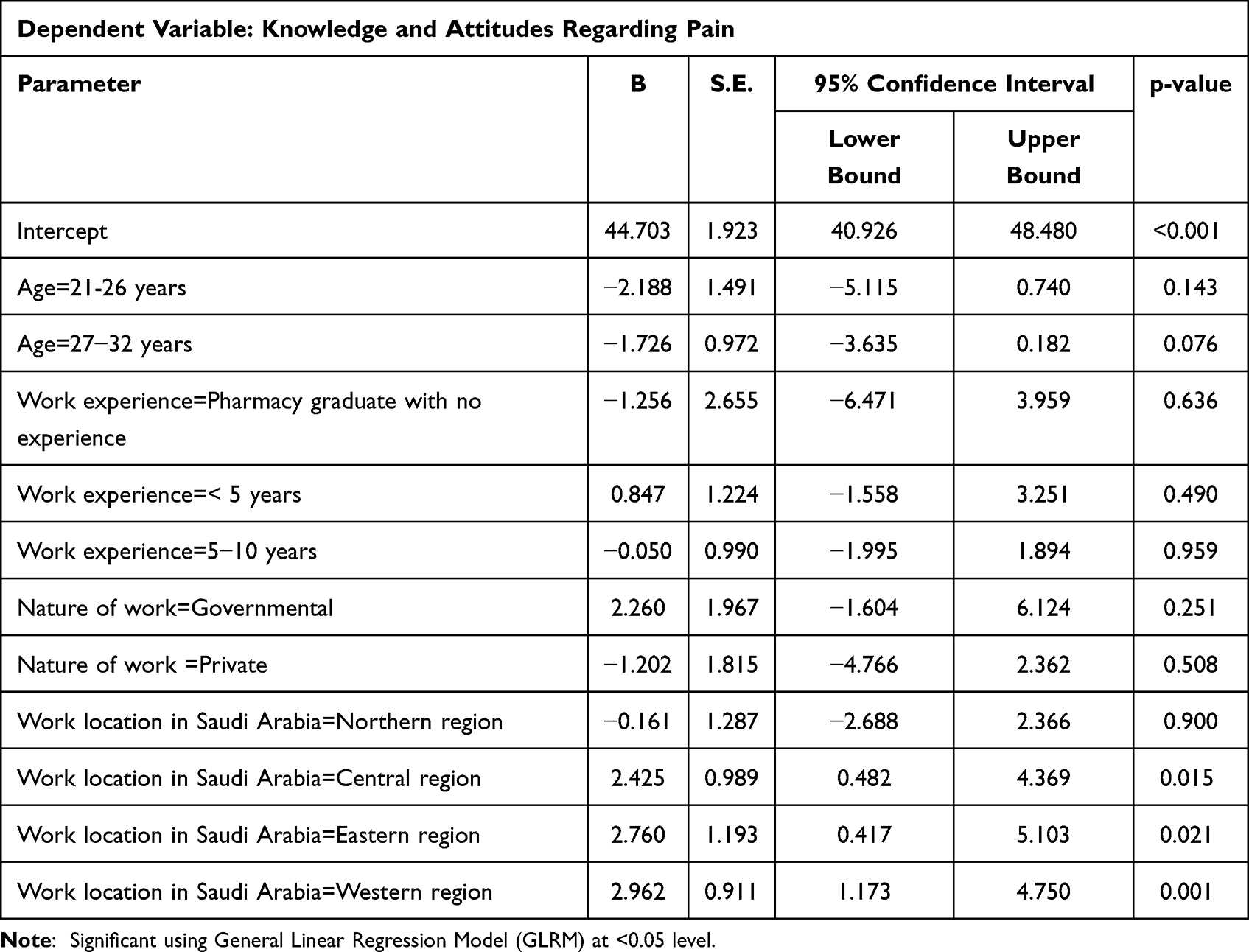 |
Table 5 Parameter Estimates for Knowledge and Attitude Regarding Pain Management |
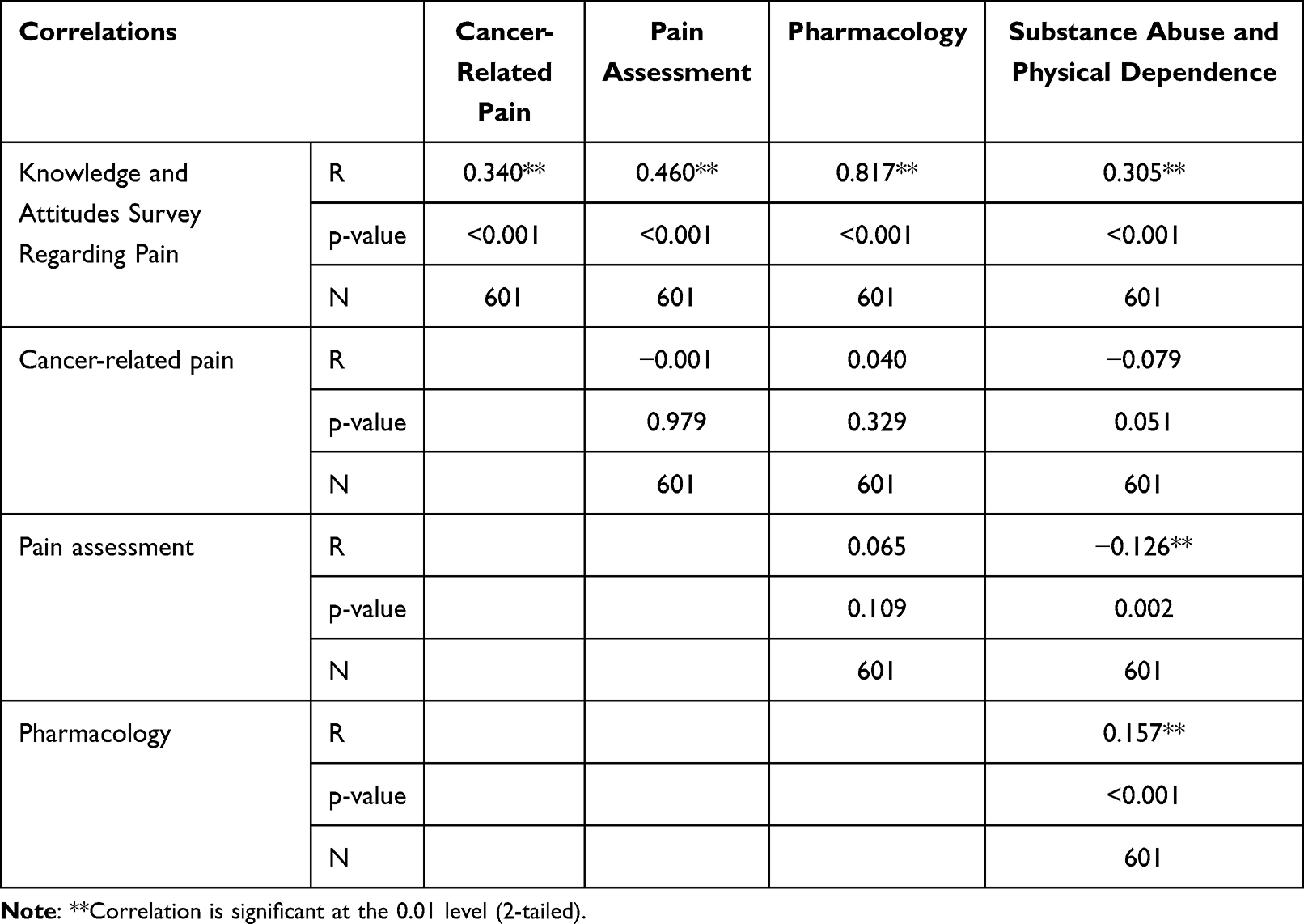 |
Table 6 Convergent Validity Statistic for Each Domain of Knowledge and Attitude of Participants Toward Pain Management |
Discussion
Goals of pain knowledge and assessment for community pharmacists are to determine pain characteristics; aid in diagnosis; formulate choice of therapy and evaluate the effectiveness of therapy. The present study revealed that community pharmacists in Saudi Arabia have inadequate knowledge of pain and pain management. Pharmacists play a crucial part in caregiver and patient education on the administration, dosage, effects, and timeframe for pain management medications.30,31 Their selection of drugs used to control pain range from mild, over-The-counter (OTC) preparations such as acetaminophen to potent general anesthetics are very critical. In this study, the deficiency in knowledge and poor attitude toward pain management could be explained by two main factors: minimal education and training on pain management and low priority/attention in the healthcare sector. Even healthcare professionals such as physicians and nurses possess insufficient knowledge of managing pain, which necessitates the need for more training and education for health workers on this topic.32 Information deficiency and a negative demeanor are major contributing variables in pain assessment. A study carried out by Al-Abdelmuhsin et al (2021) to examine final-year pharmacy students’ knowledge of and attitude toward pain management employed a cross-sectional survey using a self-completion method. Sixty pharmacy students completed the survey and the results showed that 43% of the pharmacy students knew the current answers.33 This shows the current situation of pain management knowledge amongst pharmacy students in KSA. Surprisingly, the majority of the respondents held the view that patients might sleep even if they were in severe pain. In agreement with our findings, a previous study observed that about 53.0% of students judged patients’ pain poorly, and only 10% knew the suggested course of medialization for cancer patients.34 This proves that the pharmacy practical education system in Saudi Arabia needs to improve its educational programs related to pain management at pharmacy colleges. An intensive program should be taught that prevents drug misuse, improves the medication safety system, prevents medication errors, improves patient outcomes and avoids unnecessary economic burdens on healthcare organizations. A national pharmacy pain management program is critical for the systems at the Ministry of Health institutions in Saudi Arabia.
Another study was carried out to assess community pharmacists’ knowledge and to allow them to become familiar with practices and knowledge related to screening for risk factors, as well as providing safety information regarding the prescription of NSAIDs to patients. This was a self-administered, cross-sectional and questionnaire-based study and it continued for four months. All of the participants worked as community pharmacists. The results showed that 42.5% did not pass on the correct information about concomitant drugs and around 39.1% of them failed to provide fittingly good communication regarding risk factors.35 This finding shows that a large proportion of community pharmacists in Saudi Arabia urgently need to screen their patients and provide them with the correct information so that they can communicate and follow up. As public knowledge of the exact utilization of non-steroidal mitigating drugs is low, the outcome may well be unfavorable if they take the incorrect dose of a medication or do not comprehend the correct way to utilize the medication. Pharmacist prescribing is by and large increasing, so as to make the best use of their abilities and to lessen the burden on existing prescribers. Another cross-sectional survey was conducted to explore pharmacists knowledge and practices regarding painkillers at King Abdul-Aziz Medical City-Central Region.36 The learning and experience of pharmacists of the practices and information were also assessed by Wajid (2015). The survey findings showed that amongst the surveyed pharmacists, approximately two-thirds (63.6%) were completely confident, while 32% were moderately confident, and a solitary 4.5% were not confident at all.37 Pain is prevalent in clinical settings and consider calling for medical attention. As such, healthcare professionals, especially pharmacists, are expected to be highly competent and to deliver quality services fit for the patient. These competencies include appropriate assessment of pain based on information provided by the patient, and providing strategies for patients to alleviate or manage their pain.38,39
Conclusion
Overall, the results revealed that the majority of pharmacists across Saudi Arabia have inadequate knowledge of and a negative attitude toward pain and pain management. Thus, there is an immense need to revise the curriculum on pain management in the various healthcare colleges around the country in order to enhance scientific knowledge, attitudes, and performance regarding pain and its management. Likewise, pharmacists who are actively practicing their profession must continue their medical education and training in order to bridge this gap in knowledge and understanding.
Limitation
This study is among the few that have evaluated the level of knowledge regarding pain and pain management in Saudi Arabia. While it depicts significant gaps in knowledge regarding the Pain, it does not exclude the presence of response bias, hence may limit the generalization of the findings. This study is also limited to making associations rather than establishing causation with a cross-sectional research design. Nonetheless, the findings of this study would be relevant in advancing the current body of knowledge regarding pain and pain management.
Acknowledgments
The authors would like to acknowledge the assistance of Dr. Ahmed Elalamy for his valuable support in data collection. The output presented in this paper has not been previously published, is not under consideration for publication somewhere else, and that all authors authorize its publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Raffaeli W, Arnaudo E. Pain as a disease: an overview. J Pain Res. 2022;10:2003. doi:10.2147/JPR.S138864
2. Chiarotto A, Maxwell LJ, Ostelo RW, Boers M, Tugwell P, Terwee CB. Measurement properties of visual analogue scale, numeric rating scale, and pain severity subscale of the brief pain inventory in patients with low back pain: a systematic review. J Pain. 2019;20(3):245–263. doi:10.1016/j.jpain.2018.07.009
3. Karcioglu O, Topacoglu H, Dikme O, Dikme O. A systematic review of the pain scales in adults: which to use? Am J Emerg Med. 2018;36(4):707–714. doi:10.1016/j.ajem.2018.01.008
4. Caraceni A, Cherny N, Fainsinger R, et al. Pain measurement tools and methods in clinical research in palliative care: recommendations of an expert working group of the European association of palliative care. J Pain Symptom Manage. 2022;23(3):239–255. doi:10.1016/S0885-3924(01)00409-2
5. Schaible HG, Richter F. Pathophysiology of pain. Langenbeck’s Arch Surg. 2022;389(4):237–243.
6. Maciel HIA, Costa MF, Costa ACL, De Oliveira Marcatto J, Manzo BF, Bueno M. Pharmacological and nonpharmacological measures of pain management and treatment among neonates. Rev Bras Ter Intensiva. 2022;31(1):21–26.
7. Ketenci A, Zure M. Pharmacological and non-pharmacological treatment approaches to chronic lumbar back pain. Turkish J Phys Med Rehabil. 2021;67(1):1. doi:10.5606/tftrd.2021.8216
8. Moore RA, Derry C. Efficacy of OTC analgesics. Int J Clin Pract. 2013;67(178):21–25. doi:10.1111/ijcp.12054
9. Rosenblum A, Marsch LA, Joseph H, Portenoy RK. Opioids and the treatment of chronic pain: controversies, currentstatus, and future directions. Exp Clin Psychopharmacol. 2008;16(5):405. doi:10.1037/a0013628
10. Tobaiqy M, Radwi M, Attieh Z, Almalki AM, Alhasan AH. Healthcare professionals’ views and perceptions of analgesic and antipyretic use in paediatric patients in four major Saudi hospitals. Heliyon. 2020;6(9):e05073. doi:10.1016/j.heliyon.2020.e05073
11. Maxwell C, Robinson K, McCreesh K. Managing shoulder pain: a meta-ethnography exploring healthcare providers’ experiences. Revue francophone des laboratoires: RFL. 2021;2022:1–13. doi:10.1016/S1773-035X(21)00341-5
12. Yong RJ, Mullins PM, Bhattacharyya N. Prevalence of chronic pain among adults in the United States. Pain. 2022;163(2):E328–32. doi:10.1097/j.pain.0000000000002291
13. IASP. Fact Sheets - International Association for the Study of Pain (IASP); 2022. Available from: https://www.iasp-pain.org/resources/fact-sheets/.
14. Al Qadire M, Al Khalaileh M. Jordanian nurses knowledge and attitude regarding pain management. Pain Manag Nurs. 2014;15(1):220–228. doi:10.1016/j.pmn.2012.08.006
15. Buczkowski K, Krajnik M, Jacek Budzyński SC. Management of cancer pain in Primary Care in Poland buczkowski advances in palliative medicine; 2007. Available from: https://journals.viamedica.pl/advances_in_palliative_medicine/article/view/29460.
16. Kim H, Choi S, Kim S, et al. The knowledge, attitudes, performance, and barriers of nurses to pain in oncology settings: a multi-center study. Asian Oncol Nurs. 2021;21(1):15. doi:10.5388/aon.2021.21.1.15
17. Pflughaupt M, Scharnagel R, Goßrau G, Kaiser U, Koch T, Sabatowski R. Befragung schmerztherapeutisch interessierter Ärzte zum Umgang mit Opioiden [Physicians’ knowledge and attitudes concerning the use of opioids in the treatment of chronic cancer and non-cancer pain]. Schmerz. 2010;24(3):267–275. German. doi:10.1007/s00482-010-0913-3
18. Fink R. Pain assessment: the cornerstone to optimal pain management. Proc. 2000;13(3):236. doi:10.1080/08998280.2000.11927681
19. Finley GA, Forgeron P, Arnaout M. Action research: developing a pediatric cancer pain program in Jordan. J Pain Symptom Manage. 2008;35(4):447–454. doi:10.1016/j.jpainsymman.2007.05.006
20. Fallatah SMA. Pain knowledge and attitude survey among health-care professionals at a university hospital in Saudi Arabia. Saudi J Med Med Sci. 2022;5(2):155.
21. Bashayreh IH, Al-Ghabeesh SH, Batiha AM, et al. Exploring factors among healthcare professionals that inhibit effective pain management in cancer patients. Cent Eur J Nurs Midwifery. 2019;10(1):967–976.
22. Duke G, Haas BK, Yarbrough S, Northam S. Pain management knowledge and attitudes of baccalaureate nursing students and faculty. Pain Manag Nurs. 2013;14(1):11–19. doi:10.1016/j.pmn.2010.03.006
23. Al-Khawaldeh OA, Al-Hussami M, Darawad M. Knowledge and attitudes regarding pain management among Jordanian nursing students. Nurse Educ Today. 2013;33(4):339–345. doi:10.1016/j.nedt.2013.01.006
24. Endalew NS, Tawuye HY, Melesse DY. Knowledge and attitude towards pain relief in labor among final year midwifery students: a cross-sectional study. Int J Surg Open. 2020;Jan(24):38–42. doi:10.1016/j.ijso.2020.03.006
25. Kehrer JP, Eberhart G, Wing M, Horon K. Pharmacy’s role in a modern health continuum. Can Pharm J CPJ. 2013;146(6):321. doi:10.1177/1715163513506370
26. Rixon S, Braaf S, Williams A, Liew D, Manias E. Pharmacists’ Interprofessional Communication About Medications in Specialty Hospital Settings. Health Communication. 2014;30(11):1065–1075. doi:10.1080/10410236.2014.919697
27. Mishriky J, Stupans I, Chan V, Mishriky J, Stupans I, Chan V. Expanding the role of Australian pharmacists in community pharmacies in chronic pain management - a narrative review. Pharm Pract. 2019;17(1):1410.
28. Ministry of health. Statistical Yearbook - Statistical Yearbook; 2021. Available from: https://www.moh.gov.sa/en/Ministry/Statistics/book/Pages/default.aspx.
29. Ferrell BR, McGuire DB, Donovan MI. Knowledge and beliefs regarding pain in a sample of nursing faculty. J Prof Nurs. 1993;9(2):79–88. doi:10.1016/8755-7223(93)90023-6
30. Hadi MA, Alldred DP, Briggs M, Munyombwe T, José Closs S. Effectiveness of pharmacist-led medication review in chronic pain management: systematic review and meta-analysis. Clin J Pain. 2014;30(11):1006–1014. doi:10.1097/AJP.0000000000000063
31. Dole EJ, Murawski MM, Adolphe AB, Aragon FD, Hochstadt B. Provision of pain management by a pharmacist with prescribing authority. Am J Heal Pharm. 2007;64:85–89. doi:10.2146/ajhp060056
32. Xue Y, Schulman-Green D, Czaplinski C, Harris D, McCorkle R. Pain attitudes and knowledge among RNs, pharmacists, and physicians on an inpatient oncology service. Clin J Oncol Nurs. 2007;11(5):687–695. doi:10.1188/07.CJON.687-695
33. Al-Abdelmuhsin L, Al-Ammari M, Babelghaith SD, et al. Assessment of pharmacists’ knowledge and practices towards prescribed medications for dialysis patients at a tertiary hospital in Riyadh Saudi Arabia. Healthcare. 2021;9(9):1098. doi:10.3390/healthcare9091098
34. Ajabnoor AM, Cooper RJ. Pharmacists’ prescribing in Saudi Arabia: cross-sectional study describing current practices and future perspectives. Pharm. 2020;8(3):160.
35. Malebari AM, Khayyat AN, Mahdali RA, Alamoudi JS, Alsayed BY, Alrasheed SA. Evaluation of the community pharmacists’ performance in the screening of non-steroidal anti-inflammatory drugs risks in Saudi Arabia. Saudi Med J. 2020;41:849–857. doi:10.15537/smj.2020.8.25221
36. Alshahrani SM, Orayj K, Alqahtani AM, Algahtany MA. Community pharmacists’ perceptions towards the misuse and abuse of pregabalin: a cross-sectional study from aseer region, Saudi Arabia. Healthcare. 2021;9(10):1281. doi:10.3390/healthcare9101281
37. Hossan AA, Wajid S, Ghazi A, et al. Knowledge and Attitude of Future Health Care Professionals towards Pain in Central Saudi Arabia. Indian J Pharm Pract. 2015;8:4.
38. Green CR, Wheeler JRC, Marchant B, LaPorte F, Guerrero E. Analysis of the physician variable in pain management. Pain Med. 2001;2(4):317–327. doi:10.1046/j.1526-4637.2001.01045.x
39. Bernardi M, Catania G, Lambert A, Tridello G, Luzzani M. Knowledge and attitudes about cancer pain management: a national survey of Italian oncology nurses. Eur J Oncol Nurs. 2007;11(3):272–279. doi:10.1016/j.ejon.2006.09.003
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.