Back to Journals » Journal of Asthma and Allergy » Volume 15
Dietary Factors Associated with Asthma Development: A Narrative Review and Summary of Current Guidelines and Recommendations
Authors Takkinsatian P, Mairiang D, Sangkanjanavanich S, Chiewchalermsri C ![]() , Tripipitsiriwat A, Sompornrattanaphan M
, Tripipitsiriwat A, Sompornrattanaphan M ![]()
Received 24 April 2022
Accepted for publication 15 August 2022
Published 24 August 2022 Volume 2022:15 Pages 1125—1141
DOI https://doi.org/10.2147/JAA.S364964
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Amrita Dosanjh
Preyanit Takkinsatian,1 Dara Mairiang,2 Sasipa Sangkanjanavanich,3,4 Chirawat Chiewchalermsri,5 Athiwat Tripipitsiriwat,6 Mongkhon Sompornrattanaphan7
1Department of Pediatrics, Faculty of Medicine, Vajira Hospital, Navamindradhiraj University, Bangkok, Thailand; 2Department of Pediatrics, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand; 3Division of Allergy, Immunology, and Rheumatology, Department of Medicine, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 4Department of Medicine, Phyathai 2 International Hospital, Bangkok, Thailand; 5Department of Medicine, Panyananthaphikkhu Chonprathan Medical Center, Srinakharinwirot University, Nonthaburi, Thailand; 6Division of Respiratory Disease and Tuberculosis, Department of Medicine, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand; 7Division of Allergy and Clinical Immunology, Department of Medicine, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Mongkhon Sompornrattanaphan, Division of Allergy and Clinical Immunology, Department of Medicine, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand, Tel/Fax +66 2419 8263, Email [email protected]
Abstract: Asthma is a complex disease, caused by a combination of genetic and environmental factors. The prevalence of asthma is increasing too rapidly to be attributable to genetic factors alone. Thus, environmental factors are becoming increasingly recognized as the cause of asthma. Modifying these environmental factors may be a simple approach for asthma prevention. To date, dietary intervention is an interesting modifiable factor because it can be implemented at the population level. The modification of systemic inflammation, oxidation, and microbial composition might be a mechanistic basis for prevention. This review summarizes the mechanistic basis and evidence from clinical studies on the association between dietary factors and asthma development. We also summarize the recommendations from many organizations and regional guidelines to assist the practicing physician to improve patient care.
Keywords: allergy prevention, asthma, breastfeeding, nutrition, probiotics, vitamin C, vitamin D, zinc
Introduction
Asthma is a complex disease, caused by a combination of genetic and environmental factors, leading to heterogeneous phenotypes.1 Extrinsic factors (ie, allergens, viruses, pollutants, diets, detergents, and microbiome dysbiosis) and intrinsic factors are considered as the drivers of cellular dysfunction, aberrant immune response, resulting in abnormal metabolic programming of immune cells. The disease has become one of the most common atopic disorders in both developed and developing countries.2 As the change in asthma prevalence has been too rapid to be explained by changes in the gene pool, environmental factors are becoming increasingly recognized as the cause of the recent trend in asthma prevalence. Among the environmental factors implicated in asthma pathogenesis, air pollution, dietary patterns, viral infections, and early microbial exposure have been studied.2–4 These modifiable factors may present relatively easy opportunities for asthma primary prevention. Dietary intervention is a modifiable factor of great interest because it can be implemented at the population level. The underlying mechanism could be due to modification effects on systemic inflammation, oxidation, and microbial composition, as summarized in Figure 1.5
 |
Figure 1 Mechanisms of dietary interventions on asthma. Abbreviations: APC, antigen-presenting cell; COX, cyclooxygenase; HMO, human milk oligosaccharides; IgA, immunoglobulin A; LOX, lipoxygenase; MHC, major histocompatibility complex; SCFAs, short-chain fatty acids; Th2, T helper 2 cell; Treg, regulatory T cell; 12,13-diHOME, 12,13-dihydroxy-9-octadecenoic acid. Note: This figure was created using BioRender.com. |
 |
Figure 2 Dietary interventions from current evidence on prenatal intake in pregnant mothers and postnatal intake in children for asthma primary prevention. Notes: Most guideline recommendations were based on limited evidence and could not make a firm conclusion. Created with BioRender.com. |
The investigators of randomized or nonrandomized studies of the effect of dietary factors in mother-infant dyads for prenatal intake in pregnant mothers and developing asthma or postnatal intake in children and the effect on developing asthma are confronted with major challenges in proving any protective effect. There is no gold standard diagnosis for asthma, so there is a risk of outcome misclassification bias, and it is difficult to avoid exposure measurement error in dietary factor intake in the study of free-living populations without intensive validation of measures of intake, such as food diaries, even in controlled experiments.6 Moreover, for longer term outcomes, such as developing asthma by 7 years old, dropout rates may be high, affecting the precision of estimates and thereby the power to detect a significant effect. Also, differential dropout rates correlated with the dietary factor or the outcome may bias results.7 Finally, there is the issue of sufficient sample size in a relatively rare outcome at the population level to detect small or moderate effects if those magnitudes of effect are assumed to be likely for most dietary factors. Using the optimal information size concept for meta-analysis power,8 this may require large or very large pooled sample sizes in meta-analyses. For example, a Phase III, 2-arm parallel group, placebo-controlled randomized controlled trial (RCT) with a 1:1 allocation ratio to confirm that a dietary factor can reduce the incidence of asthma in children by 20% assuming p-value significance of <0.05 (alpha of 5%) and power of 90% (beta of 10%) and a control group event rate of 5% would require a total pooled sample size of 18,060 participants.9 Thus, pooled meta-analyses would have to achieve sufficient pooled sample sizes to achieve acceptable precision to be conclusive. Higher control group event rates and larger putative reductions in incidence would reduce the burden of large pooled sample sizes.
In this review, we aim to describe how dietary interventions affect or have been hypothesized to affect asthma pathophysiology and to evaluate the evidence on the associations between dietary factors and developing asthma from clinical studies, providing commentary on methodologic concerns that should be considered by evidence appraisers. We also compare the recommendations from organizations and regional guidelines to assist the practicing physician to improve patient care.
Dietary Factors
Breastfeeding
Milk is the source of energy and nutrition during the first few months of life. Human milk consists of essential macronutrients, micronutrients, and also contains bioactive factors that affect biological processes involved in body functions, including immunoglobulins (Ig), anti-inflammatory cytokines, growth factors, and hormones.10
Human milk oligosaccharides (HMOs) are the key bioactive components uniquely found in human breast milk. One of the important components of HMOs is 2’-fucosyllactose (2’ FL). 2ʹFL is a non-digestible sugar.11 It promotes gut microbiota enrichment, has anti-adhesive effect on pathogens,12 and modulates the immune system.13 Ingested HMOs in the gut are fermented into short-chain fatty acids (SCFAs), including acetate, butyrate, and propionate. These SCFAs enhance the growth of Bifidobacterium and Lactobacillus.14 SCFAs also have anti-inflammatory properties by promoting regulatory T cell (Tregs) and induce mucosal immunoglobulin A (IgA) production.15
Random assignment of exclusive breastfeeding is problematic due to the patient autonomy of the mother. Hence, proving a treatment effect by RCT is challenging. Only two follow-up studies of one RCT have been reported.16,17 Among pregnant mothers intending to breastfeed, interventions by healthcare workers promoting exclusivity and prolonged breastfeeding were compared with not promoting breastfeeding for the outcome of participant self-reported “ever asthma”. At 6.5 and 11.5 years old, no significant differences were found in the relative effect on “ever asthma” ((OR 1.20; 95% CI 0.70, 1.90) vs (OR 0.76; 95% CI 0.47, 1.23), respectively).16,17 However, these studies were limited by inability to blind participants assessing the outcome “ever asthma” to the assigned interventions and the indirectness of both the investigated intervention compared to the intervention of true interest, quantified breastfeeding, and the closest possibilities to a gold standard outcome definition, for example, documented physician-diagnosed asthma or a detailed symptoms diary. Thus, we suggest these studies represent a very low level of evidence for the lack of the true effect. This is still inconclusive if only considering RCTs.
In the past decade, four systematic reviews with meta-analyses investigating asthma development and breastfeeding have been published.18–21 However, we only focus on the most recent because it substantially overlaps with previous reviews in included studies and comparisons and has stricter inclusion criteria for methodologic quality of analyzed studies. Xue et al’s20 recent meta-analysis was restricted to cohort studies with outcomes of physician-diagnosed asthma or by well-recognized guidelines unlike previous meta-analyses. “Ever breastfeeding” did not show a significant inverse association (OR 0.87; 95% CI 0.72, 1.04; I2=76%) among 89,861 mother-infant dyads in 18 studies although more exclusive among 30,587 mother-infant dyads in 17 studies and more breastfeeding among 116,649 mother-infant dyads in 36 studies showed a significant inverse association ((OR 0.81; 95% CI 0.72, 0.91; I2=44.0%) and (OR 0.84; 95% CI 0.75, 0.93; I2=62.4%), respectively). Subgroup analysis of 12 studies suggested the inverse association between more breastfeeding with developing asthma becomes uncertain after the age of 7 years. Another subgroup analysis suggested a significant inverse association in 11 studies between “ever breastfeeding” and developing asthma excluding methodologically low-quality studies (OR 0.77; 95% CI 0.63, 0.94; I2=44.8%).
Two observational cohort studies of the effect of breastfeeding on developing asthma in children at high risk of developing asthma have been conducted. A prospective cohort study among 624 mother-infant dyads of mothers with physician-diagnosed asthma found breastfeeding for greater than 6 months had a significant inverse association with the risk of “ever wheeze” at around 6 months of age (aRR 0.54; 95% CI 0.30, 0.96). However, it is notable that lesser durations of breastfeeding and “ever wheeze” by at 12 months of age were not significant.22 However, this study was limited by using caregiver-reported wheezing in an unblinded, nonrandomized study rather than a more valid asthma-specific outcome. A more recent urban population-based Australian cohort study HealthNuts of 5276 mother-infant dyads investigated whether physician-diagnosed eczema incidence during the first year of life affected the association between breastfeeding and physician-diagnosed asthma prevalence at 6 years old.23 This study found weak evidence that duration of breastfeeding scaled in months may correlate with a reduction in asthma prevalence at 6 years old only in infants without early development of eczema while there was no significant association in those with early development of eczema ((aOR 0.98; 95% CI 0.95, 1.00) vs (aOR 1.03; 95% CI 0.98, 1.08), respectively).
We draw conclusions about the association between breastfeeding and developing asthma from the evidence from clinical studies. It is highly likely both exclusive and non-exclusive human milk feeding have small protective effects against developing asthma evidenced by pooled analysis of a large sample from high quality cohort studies demonstrating a dose–response relationship. Prolonged breastfeeding is desirable for a greater protective effect. It is inconclusive as to whether any protective effect persists in children older than 7 years. The small protective effect in younger children becomes a significant public health benefit at the population level. The one randomized trial was very low-quality evidence. Weak evidence from one large, population-based cohort study suggests the protective effect of increased duration of breastfeeding against asthma in later childhood may be lost among infants with higher risk of atopic disease. Moreover, there are opportunities to refine research methods. Randomization of future studies on breastfeeding intervention may be challenging, if not impossible, due to the mother’s right to autonomy. Thus, we suggest in the era of increasing implementation of population-based electronic health records and database linkage, large prospective cohort studies collecting sufficient data on confounders may be able to obtain acceptable marginal effect counterfactual comparisons for the average treatment effect very close to those of RCTs by innovative methods, such as g methods.24 Future studies should define the asthma outcome to reduce misclassification as much as possible, such as physician-diagnosed asthma. Non-differential misclassification between compared groups attenuates the relative effect towards null and differential misclassification biases away from null. If outcomes or exposures are misclassified or measured with error, methods for adjustment exist for sensitivity analysis.25 Widespread misclassification and measurement error patterns due to outcome definitions may partially explain the inconsistency of the association of breastfeeding and developing asthma observed between studies in some meta-analytic systematic reviews.
Recommendations on breastfeeding practice guidelines are summarized in Table 1. Most recommendations on breastfeeding are based on the general health benefits to mother and child and are not specifically about allergy prevention.
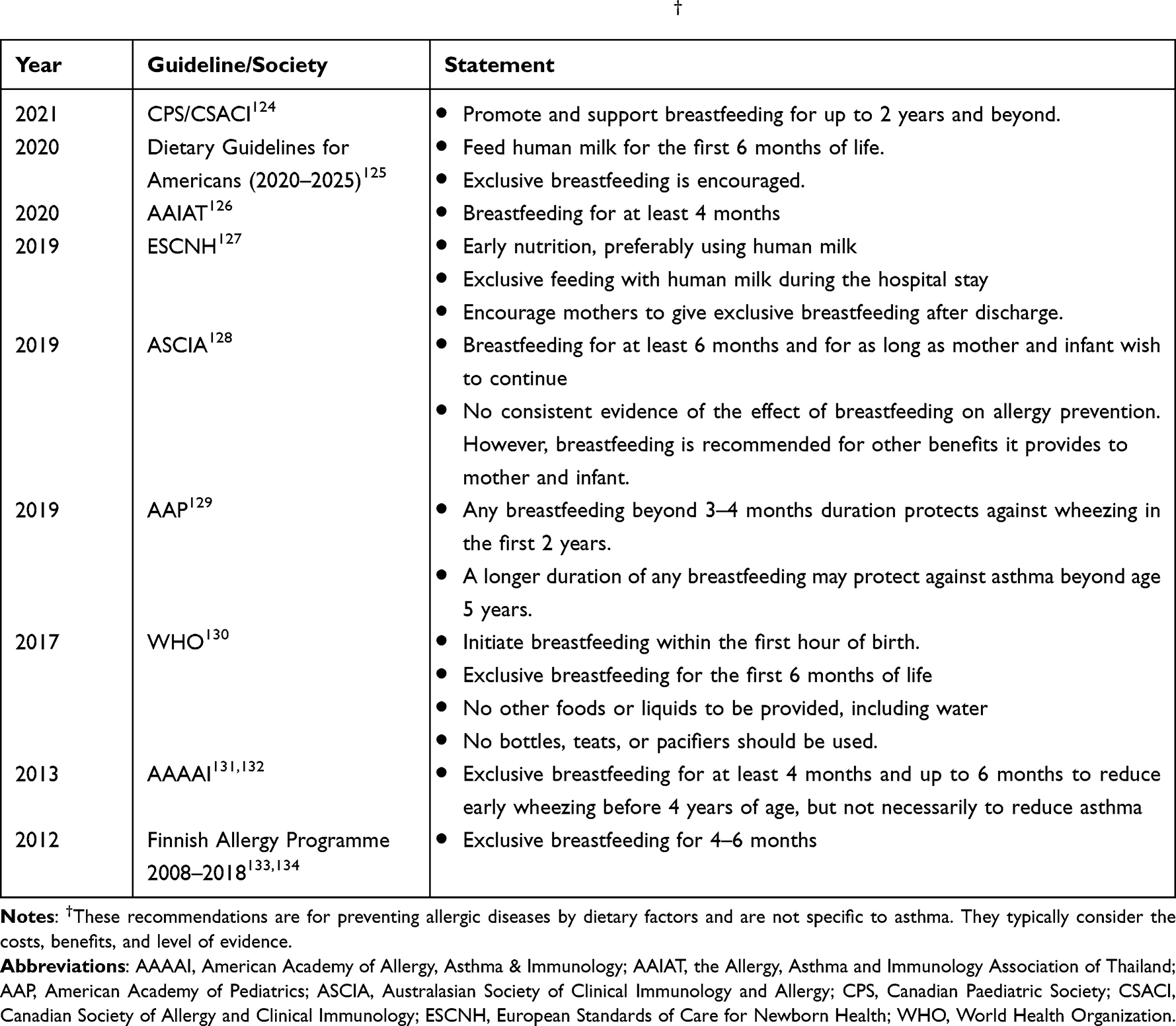 |
Table 1 Summary of Recommendations on Breastfeeding Practice† |
Probiotics
Probiotics are microorganisms resulting in health benefits for the host if ingested in an adequate amount. Prebiotics are selectively fermented ingredients causing particular changes to the composition of the gastrointestinal microbiota, conferring health benefits. Products containing both are defined as synbiotics.26
The microorganisms colonizing the human body form the microbiome influencing the human immune system.27 The human gut microenvironment undergoes specific changes from birth, according to their constant pressure and the maturing the immune system.28,29 The microbiome influences the metabolome at both near and distant body sites and the metabolome can affect the microbiome.30,31 Probiotics can restore the composition of the gut microbiome, resulting in health benefits by modulating both innate and adaptive immunity. Probiotics could induce systemic tolerance by reducing T helper 2 (Th2) response and increasing Tregs.32 Several probiotics could induce Tregs and their functions by a different mechanism, for example, Clostridium,33 Bifidobacterium,34 Lactobacillus,35 Escherichia coli Nissle 1917,36 and the probiotic mixture VSL#3 (four Lactobacillus spp., three Bifidobacterium spp., and one Streptococcus spp.).37 Additionally, probiotics are associated with increased immunoglobulin A production, which has a role in antimicrobial immunity.38 In innate immunity, probiotics could activate the mucosal barrier to improve mucous production, monocytes to increase circulating monocytes, and dendritic cells to augment dendritic cell activity.39,40 Probiotics also increased the production of SCFAs metabolites, promoting Treg activation in lung tissues.41
The most recent meta-analysis of prenatal maternal probiotic intake to prevent the development of asthma in their offspring reported two asthma outcome-specific studies.42 A placebo-controlled RCT of intake of probiotics from 36 weeks of gestational age to 3 month after birth among 415 pregnant mothers with an asthma outcome in their children defined as multiple episodes of wheezing with inhaled glucocorticoids use, or signs of suspected hyper-reactivity without concurrent upper respiratory infection at 2 years old and its follow-up study at 6 years were reported.43,44 No significant results were found. However, the dropout rate was high. Another placebo-controlled RCT of probiotic intake from 14 to 16 weeks of gestational age to 6 month after birth among 423 pregnant mothers with an outcome of any history of wheeze in their children at 6 and 12 months of age also did not report significant results.45 Although the methodologic quality of these studies was good, the non-significant findings were not pooled in meta-analysis due to methodologic heterogeneity. Those findings were from exploratory subgroup analyses.
In terms of observational evidence on the association between probiotics and atopy/wheezing in children, one cross-sectional study showed children with atopy and wheezing at 1 year of age had significantly decreased populations of Bifidobacterium, Ruthie, Faecalibacterium Lachnospira, and Veillonella in their guts at 3 months of age.46 In terms of RCTs, the most recent meta-analysis of six placebo-controlled RCTs among 1659 children showed postnatal probiotics use did not prevent a well-defined asthma outcome.47 It is possible that the large proportions of included children with high risk of developing asthma represents a highly selected population, so these findings may not be generalizable to those without such high risk.
Our conclusions based on the clinical study evidence on prenatal maternal probiotic intake are that the effect is inconclusive because they are based on exploratory subgroup analyses that could not be soberly pooled. Further high-quality randomized studies with well-defined primary endpoints for asthma-specific outcomes are required. Our conclusions on postnatal probiotics intake in children are that the effect is inconclusive due to most studies selecting children with high risk of developing asthma. Further studies in unselected populations are needed.
According to our conclusions, the recommendations relating to probiotics and prebiotics used in allergy prevention are based on insufficient evidence. The differing recommendations between organization guidelines are summarized in Table 2.
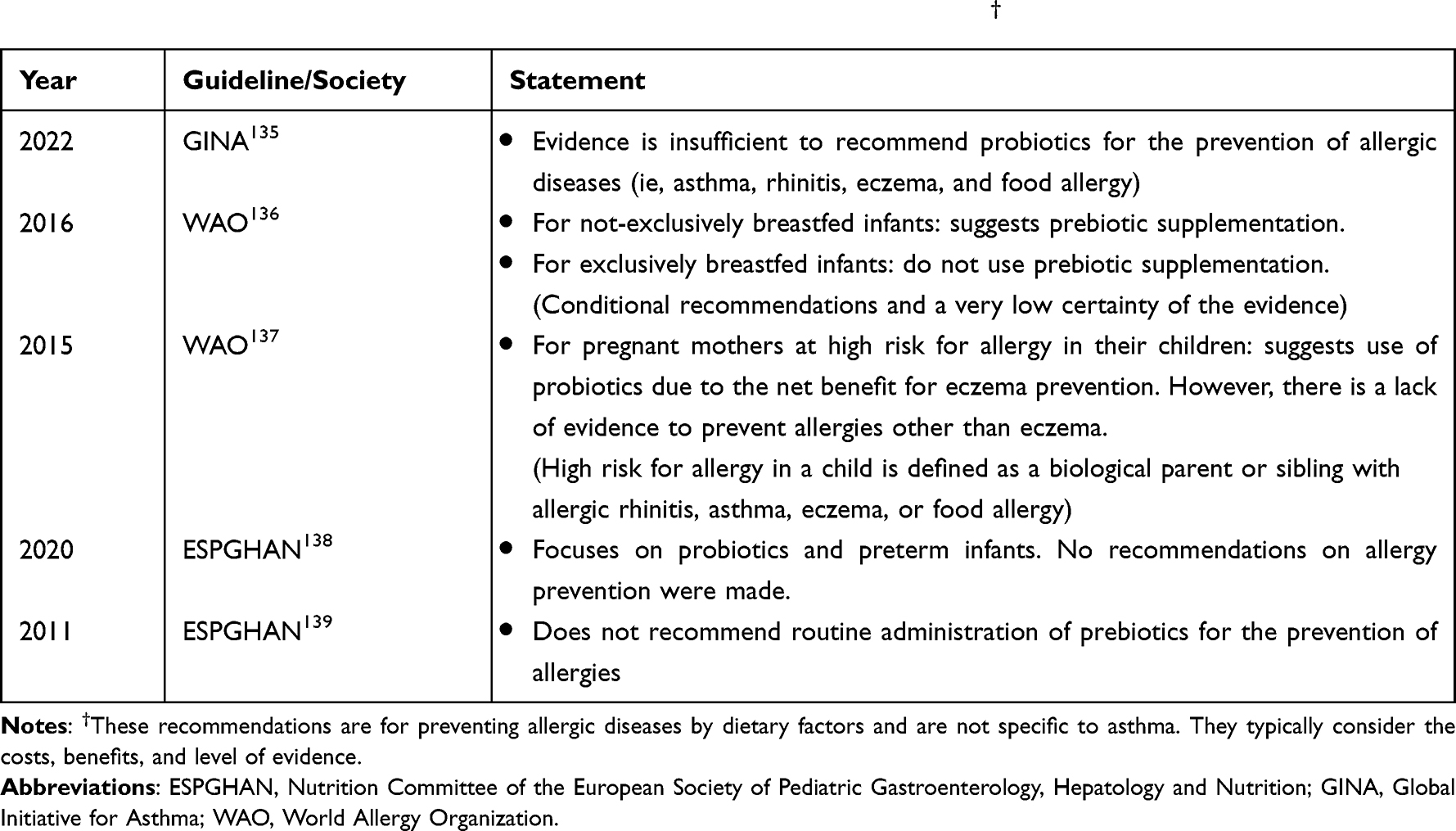 |
Table 2 Summary of Recommendations on Intake of Probiotics and Prebiotics† |
Fatty Acids
Fatty acids are an important component of lipids in plants and animals. Fatty acids are aliphatic carboxylic acids, containing a hydrocarbon chain and a carboxyl group at the other end. Fatty acids are classified as saturated fatty acid (SFA), monounsaturated fatty acid (MUFA), and polyunsaturated fatty acid (PUFA), according to their double-bond structure.48 Fatty acids commonly combine with glycerol, forming triglycerides in nature.
Fatty acids influence multiple physiologic processes in the human body. The PUFAs, namely, omega-6 (n-6) and omega-3 (n-3) fatty acids, regulate the immune system.49 Foods with a high amount of n-3 fatty acids include fatty fish, algae, and several high-fat plant foods while n-6 fatty acids are mainly found in margarine and vegetable oil.50 Lipid mediators known to regulate inflammation are derived from 1) omega-6 (n-6) and its metabolites, namely arachidonic acid (AA) and linoleic acid (LA), and 2) omega-3 and its metabolites, namely eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA). AA-derived mediators mainly consist of prostaglandins (PG) and cysteinyl leukotrienes (Cysts). Through enzymatic oxidation by cyclooxygenase (COX), PGE2, thromboxane A2, and PGD2 are produced. The latter two metabolites have been shown to be proinflammatory and have been associated with bronchoconstriction while PGE2 promotes airway smooth muscles relaxation.51,52 Several studies have shown that AA-derived lipoxin A4 (LXA4) and EPA- and DHA-derived (protectins, resolvins, and maresins) are dysregulated in severe asthmatics.53,54
There is observational study evidence from one large population-based cohort study that high plasma PUFA level in 4986 pregnant women in during the second trimester was significantly associated with lower risk of asthma/persistent wheeze in their children at 6 years old.55 In terms of RCTs, the effect of fatty acids in pregnant mothers on asthma prevention has been investigated in two recent meta-analyses reporting discordant findings. Venter et al56 found among 1743 mother-infant dyads in four RCTs, no significant difference between n-3 fatty acids supplementation during pregnancy and mostly vegetable oil controls (one study had no control substance) and risk of having asthma/wheeze in children, age ranging from 6 months to 16 years (OR 0.70; 95% CI 0.45, 1.08; I2=51%) while Lin et al reported a significantly reduced incidence of wheeze/asthma in children, age ranging from 6 months to 16 years (RR 0.81; 95% CI 0.66–0.99; I2=41.8%) among 2047 mother-infant dyads in six RCTs.57
Observational study evidence has been reported on the association of postnatal fatty acids intake in children and asthma/recurrent wheeze. A birth cohort study investigating dietary PUFAs intake and plasma PUFAs level found a significant negative associated with asthma and/or recurrent wheeze and atopy in 235 children aged 3 years.58 In a nested case-control study of 84 children comparing from the PASTURE birth cohort study, those without asthma at 6 years old had significantly higher consumption of unprocessed farm milk, which has a higher n-3 fatty acids content.59 Similar to pregnant women, the effect of PUFA intake on developing asthma might be modified by gene-nutrient interaction. In children with fatty acid deficiency variants, a higher intake of fish-derived EPA and DHA was strongly associated with reduced asthma risk up to mid-adolescence.60 In terms of RCTs, there are discordant results between the most recent meta-analysis including only RCTs and the most recent meta-analysis including only birth cohort studies comparing between of PUFA (fish oil capsules or omega-3 fatty acids) intake and mostly vegetable oil control groups for the outcome of childhood asthma/wheeze. In a meta-analysis of RCTs pooling 2415 children in five studies, no significant reduction of wheeze/asthma was found (OR 0.97; 95% CI 0.65, 1.47; I2=52%); 4 of 5 of the included RCTs recruited children with high risk of asthma/atopic disease.61 Conversely, a meta-analysis of large birth cohorts pooling 9212 children from three studies found fish oil may have a protective effect (OR 0.76; 95% CI 0.61, 0.94; I2=11.5%).62
We conclude based on clinical studies that the overall effect of fatty acid supplements in pregnant women is inconclusive. The use of a fixed effect model instead of a random effects one in the meta-analysis with significant results produced anti-conservative confidence intervals and precludes generalization.63,64 Notably, the sample size of RCTs if subgrouping studies by their outcome definitions in the literature was too small for confident estimation of confidence intervals for generalization.65 At least five studies are required for random effects modeling for correct confidence interval coverage, so more high quality RCTs are required.66,67 For postnatal fatty acids intake in children to prevent the development of asthma, children with high risk of asthma may not protect against childhood asthma. More high-quality RCTs are required to confirm this. However, the conclusion may not be generalizable to children without high risk of asthma. The findings from the meta-analysis of large birth cohorts may better represent a tentative effect of fatty acid intake in children without high risk of asthma because pooled results were adjusted for confounding risk factors of developing asthma. Nevertheless, there were too few studies in that analysis for confident estimation, and the estimated effect may be biased by residual confounding in nonrandomized studies. Thus, we conclude that the evidence is inconclusive. More RCTs in unselected populations are required.
We summarize the current recommendations on fatty acid-rich food and the dietary pattern for allergy prevention in Table 3.
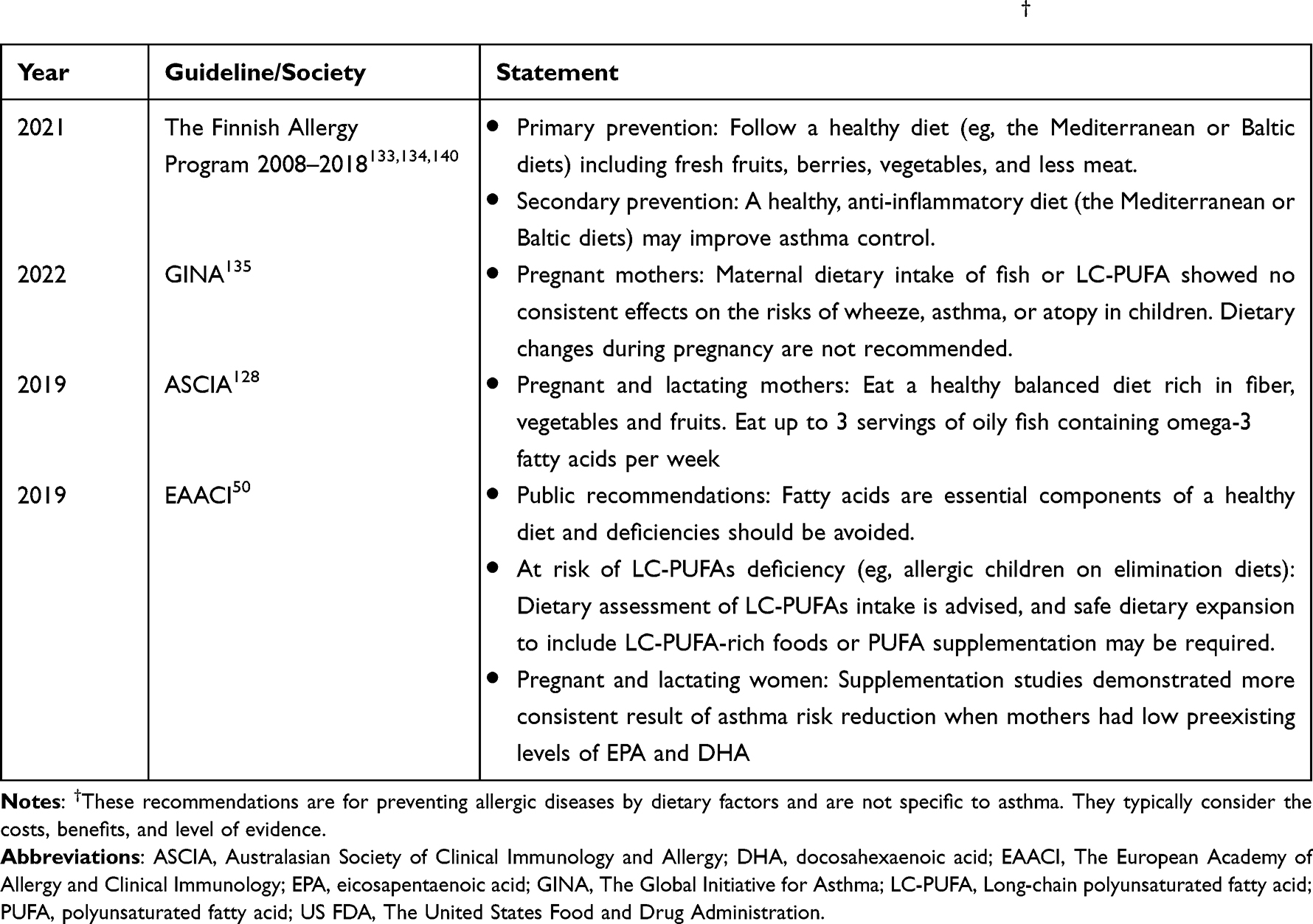 |
Table 3 Summary of Recommendations on Fatty Acid-Rich Food and the Dietary Pattern† |
Mediterranean Diet
The Mediterranean Diet incorporates traditional healthy foods from countries bordering the Mediterranean Sea. It includes a high amount of vegetables, fruits, legumes, nuts, beans, cereals, grains, fish, and unsaturated fats but a low intake of meat and dairy foods.68 They have been recognized for health benefits, especially the reduction of non-communicable metabolic diseases, such as type 2 diabetes mellitus, cardiovascular diseases, and neurodegenerative diseases.69 However, studies showed controversial findings regarding hyperresponsive airway disease. Within this diet, vegetables, fruits, and whole-grain have antioxidant properties, which may have a direct effect in reducing systemic and airway inflammation, ameliorating the effects of Th2 immune responses and nuclear factor kappa B (NF-κB).70 The high fiber component in the Mediterranean Diet is further fermented by gut microbiome, generating SCFAs.71 Butyrate is the most potent histone deacetylation inhibitor, promoting the transcription factor FOXP3, which polarizes naïve T cells to Treg cells. Finally, less energy intake is usually associated with the consumption of healthy foods, which may lead to weight reduction and improved asthma symptoms control.72,73
To the best of our knowledge, the association between the consumption of Mediterranean Diet during pregnancy or infancy and an asthma incidence has only been demonstrated in nonrandomized studies of diet scores rather than by an individual component. The diet scores KIDMED74 and Mediterranean Diet scale68 have been used to assess adherence to the Mediterranean Diet. Studies in the most recent meta-analysis used extreme phenotypes group comparison between the high adherence group and the low adherence group to obtain more statistical power.75 This meta-analysis of prenatal maternal Mediterranean Diet and parent-reported or physician-diagnosed childhood asthma outcome pooling 2852 mother-infant dyads from two observational studies reported no significant association. When the defined outcome was wheeze at 12 months old, a significant inverse association was reported pooling 5089 mother-infant dyads from three observational studies (OR 0.92; 95% CI 0.88, 0.95; I2=0%).
In the same meta-analysis for prenatal maternal Mediterranean Diet,75 childhood high versus low adherence to a Mediterranean Diet for the association with developing asthma was also compared in 78,587 children from pooling of five cross-sectional studies, one case-control study, and one cohort study. No significant protective effect was reported. When the outcome was defined as wheeze in three cross-sectional studies, a significant protective effect was reported (OR 0.51; 95% CI 0.37, 0.70; I2=0%).
Based on the clinical study evidence, we conclude that whether a prenatal Mediterranean Diet in pregnant mothers protects against developing asthma is inconclusive because of the lack of reported RCTs, the lack of positive findings in meta-analyses of observational studies using a strict asthma outcome, too few studies for confidence interval validity in meta-analysis, and the large proportion of cross-sectional studies, which may have a risk of reverse causality of the exposure and effect relationship. Inconsistency between asthma and wheeze outcome definitions may be due to misclassification in unblinded observational studies. Further, high quality randomized and nonrandomized studies are required with good asthma outcomes definitions. For postnatal Mediterranean Diet intake in children, we consider the evidence to be inconclusive because of the lack of reported RCTs along with discordant results from meta-analysis of observational studies between developing asthma and developing wheeze outcomes, which had results based on too few studies to conclude.
Vitamin D
Vitamin D is a fat-soluble nutrient that plays role in many systemic functions, such as a modulator of calcium absorption and immune regulation.76 Vitamin D is primarily acquired from sun exposure and to a lesser extent from food. However, lack of sufficient vitamin D is common worldwide with an estimated at least 1 billion people with vitamin D deficiency/insufficiency. The prevalence of vitamin D deficiency among adult populations ranged between 5.9% and 640%, and the Asian population had a higher rate than the Caucasian population.77,78
Vitamin D can regulate the innate and adaptive immune responses.79 Active vitamin D has an immunoregulatory effect80 by decreasing dendritic cell function, stimulating IL-10 production, and promoting Treg functions.81 Promoting Treg function results in suppression of DCs and inhibition of effector Th1, Th2, and Th17 cells, inhibiting allergen-specific IgE production and inducing IgG4 secretion. Treg also suppresses mast cells, basophils, and eosinophils, interacting with resident tissue cells and participating in tissue remodeling in allergic asthma and allergic rhinitis patients.82 The vitamin D receptor (VDR) is a member of the steroid receptor superfamily. Previously published data on the connection of polymorphisms in the VDR gene with asthma have produced conflicting results.83–87 Genetic variation in genes other than VDR was implicated in vitamin D metabolism, and signaling pathways were also discovered in asthmatic children.88 A murine model in VDR-knocked out mice showed they did not develop asthma.89 Thus, VDR expression is required for the development of lung inflammation.90 Furthermore, the presence of VDR in human bronchial smooth muscle cells has recently been reported, and vitamin D regulates the expression of a large number of genes, including those involved in smooth muscle cell contraction, inflammation, glucocorticoid, and prostaglandin regulation.91
A meta-analysis among 1513 mother-infant dyads in three RCTs showed that vitamin D3 supplementation during pregnancy reduced the risk of wheeze/asthma in offspring at 6 years old (OR 0.72; 95% CI 0.56–0.92; I2=0%).56 In meta-analysis of observational studies, vitamin D supplementation during pregnancy compared with no vitamin D in 16,527 mother-infant pairs from six observational studies (one case-control and five cohort studies) was inversely associated with risk of developing asthma in children (OR 0.78, 95% CI 0.69–0.89; I2=63%). The age when the outcomes were observed is varied from 2 to 10 years. When the outcome was defined as asthma/wheeze, the inverse association remained (OR 0.65 (95% CI 0.54, 0.79; I2=79%)).92
In terms of the effect of postnatal vitamin D supplements, there was limited evidence from two observational studies that were not pooled and did not find significant results.93 However, one double-blinded, placebo-controlled RCT in 300 pre-term, black infants showed that sustained vitamin D supplementation reduced risk of recurrent wheezing at 12 months.94
We conclude based on clinical studies that there is sufficient consistency between more and less asthma-specific outcome definitions in the meta-analysis of observational studies that it is quite likely that vitamin D supplementation during pregnancy has a small protective effect against developing asthma. Future meta-analyses of larger cohorts of high-quality RCTs should greatly increase the confidence in this conclusion. For postnatal vitamin D intake in children, the evidence is inconclusive. Despite the high methodologic quality of the one available RCT, it was a medium-sized, single-centered trial in a highly selected population. Thus, no generalized conclusion can be drawn for an unselected population.
The recommendations on vitamin D intake in asthma prevention are summarized in Table 4.
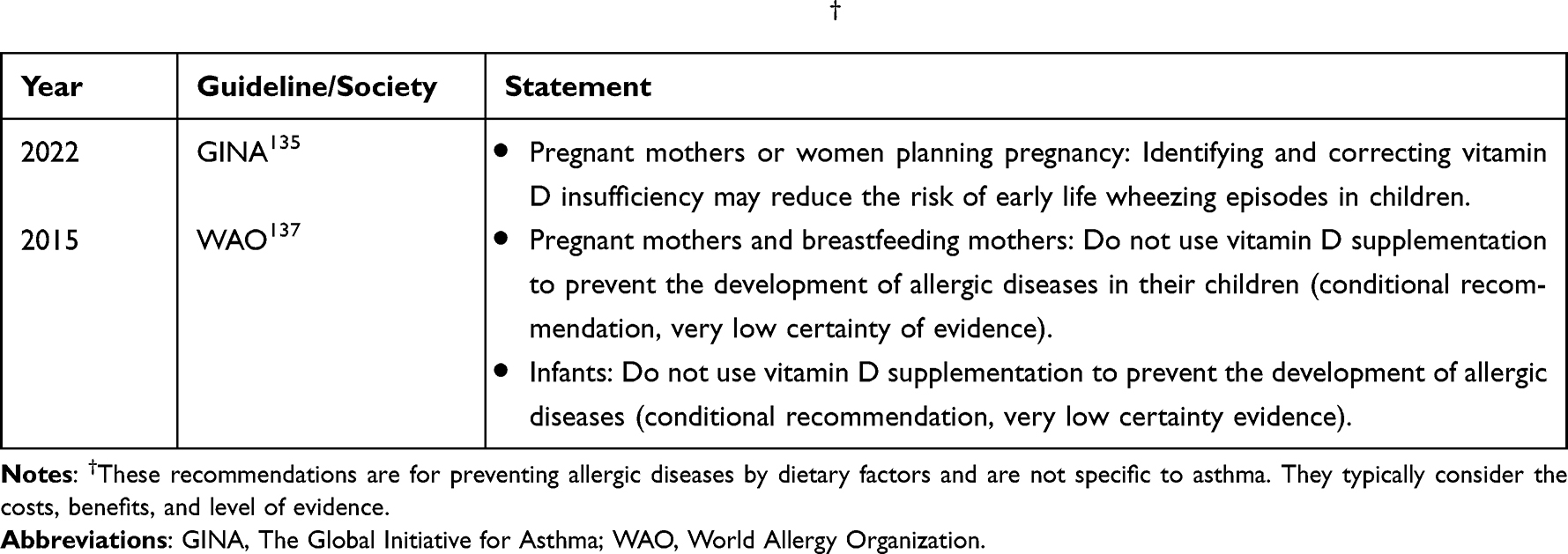 |
Table 4 Summary of Recommendations on Vitamin D Intake† |
Vitamin C
Vitamin C (ascorbic acid) is a potent water-soluble antioxidant found in various fruits and vegetables. It has been associated with lower risks of cardiovascular disease, stroke, and cancer.95 Vitamin C has also shown anti-inflammatory properties. Vitamin C supplementation reduces C-reactive protein (CRP) in individuals with elevated CRP levels.96 Vitamin C could have beneficial effects on asthma through its immune-modulatory (eg, prostaglandin inhibition), antioxidant, and anti-inflammatory properties. In experimental models, vitamin C has been linked to decreased airway responsiveness as well as reduced perivascular and peribronchiolar infiltration by inflammatory cells.97,98
In terms of asthma prevention, the most recent meta-analysis of observational studies showed no association between vitamin C supplements in pregnant women and offspring asthma (2 studies) or wheeze (5 studies).99 One small, multi-centered, double-blinded, placebo-controlled trial showed that vitamin C supplements in 159 pregnant smoking mother-infant dyads showed a significant decrease “ever wheeze” at 1 year old in the offspring in a secondary analysis.100 Regarding postnatal vitamin C supplementation, a systematic review of both RCTs and observational studies found no significant treatment effect or inverse associations, respectively, between vitamin C and developing asthma or wheeze, and these findings were obtained from meta-analytic models with less than five studies per type of study design except for cross-sectional ones, of which there were seven.101
We conclude based on clinical studies that there is insufficient high-quality evidence on prenatal maternal vitamin C supplementation and the risk of developing asthma. More high-quality RCTs or observational cohort studies are required. Despite the high quality of the RCT of vitamin C supplementation in smoking pregnant mothers, more RCTs need to be performed in smoking mothers as it was a small RCT. Furthermore, we conclude that there is insufficient evidence of the effect of vitamin C supplementation in children and the risk of developing asthma, and more high-quality studies are needed.
Vitamin E
Vitamin E is a collection of fat-soluble compounds, found in many foods, such as nuts, seeds, green vegetables, and vegetable oils, and it has distinctive antioxidant activities.102 Naturally occurring vitamin E exists in eight chemical forms (α-, β-, γ- and δ-tocopherol as well as α-, β-, γ- and δ-tocotrienol), of which α-tocopherol has the greatest bioavailability and is the best characterized.103
Vitamin E has been shown to affect the immune system due to its antioxidant and anti-inflammatory properties.104,105 Vitamin E could inhibit NF-κB pathways106,107 and could prevent the release of reactive oxygen species.108 Vitamin E also inhibits pro-inflammatory cytokines, such as IL-1, IL-6, and TNF-α.103,109,110 The gene expression of IL-4, a central cytokine in the Th2 allergic inflammatory pathway, could be inhibited by vitamin E.111 Vitamin E also prevents the suppression of nuclear factor-like 2,112 the master transcription factor regulating the expression of Phase II antioxidant and detoxifying enzymes. Pregnant mothers with lower intakes of vitamin E showed heightened responses of cord blood mononuclear cells to antigen stimulation.113
In terms of prenatal prevention, the most recent meta-analysis of observational cohort studies showed that vitamin E supplementation in 35,770 pregnant mothers in six studies was not significantly inversely associated with developing childhood asthma (OR 0.97; 95% CI 0.95, 1.00; I2=50%), but there was a significant inverse association with childhood wheezing (OR 0.65; 95% CI 0.56, 0.75; I2=0%) among 6680 pregnant mothers in seven studies.114 Interestingly, the meta-analysis of the asthma outcome was dominated by one study contributing to 97% of the pooled result.115 This study collected food diaries at 25 weeks of gestational age from a population-based cohort of pregnant Danish mothers and performed acceptable covariate adjustment for confounding, finding no significant association between intensity of vitamin E intake an developing asthma. However, serum vitamin E levels were not used to validate food diaries by objective correlation in any of the pregnant mothers, and the outcome defined for asthma included caregiver-reported “ever asthma” in the systematic review. Subgroup analyses using “ever prescribed for asthma” and “ever hospitalized for asthma” still showed non-significant associations in 28,399 mother-infant dyads.
In terms of postnatal vitamin E and asthma risk, the nested case-control from the Finnish birth cohort showed no significant association between serum tocopherols level between age 1–4 years and asthma risk by the age of 5 years in confounder-adjusted models.116
We conclude that the evidence on vitamin E supplementation for pregnant mothers is inconclusive. There is a lack of RCTs, and the most recent meta-analysis of the asthma outcome is dominated by a single cohort study without objective validation of the exposure measurement. We suggest that future studies using food diaries should include such objective validation of a randomized subsample of the cohort with meticulous methods to reduce measurement error and probe its effects by sensitivity analysis. We conclude that there is no evidence on vitamin E supplementation in children to prevent the development of asthma. There is only one negative-findings nested case-control of the association of mean levels of serum α-tocopherol and γ-tocopherol in infants and developing asthma.
Zinc
Zinc is an essential micronutrient and a cofactor for the function of numerous proteins Zinc regulates immune system via various mechanisms. Firstly, zinc is involved in posttranslational modifications of proteins as it affects the activity of protein kinases and phosphatases.117 Secondly, zinc regulates intracellular signaling pathways via the control of signaling pathways including the NFkB signaling pathway and the T cell receptor signaling.118 Thirdly, zinc depletion decreases Th1 immune responses and promotes Th2 responses.119 Finally, zinc suppresses eosinophilic airway inflammation.120
In terms of zinc level in children and its association with asthma, a recent meta-analysis showed no significant difference between the standard mean differences of zinc level in asthmatic children compared to the control group.121
A meta-analysis of observational studies prenatal maternal dietary zinc intake and the risk of developing asthma and wheezing outcomes99 found that developing asthma by the age of 5 years was not significant among 3694 mother-infant dyads in two studies and that developing wheeze by the age of 1–2 years was significant (OR 0.57, 95% CI 0.40, 0.81; I2=0%). The most recent meta-analysis of observational studies and RCTs56 presented the two observational studies, Litonjua et al,122 a placebo-controlled RCT of 881 mother-infant dyads, and Miyake et al,123 a cohort study of 763 mother-infant dyads, unpooled and reported significant findings.
To date, there are no reports about postnatal zinc intake in children for prevention of developing asthma.
We conclude from clinical studies that there is insufficient evidence on prenatal maternal zinc intake and prevention of developing asthma in their children. The evidence is inconclusive due to too few studies for valid confidence interval coverage estimation in meta-analysis and inconsistent results between asthma and wheeze outcomes. There is no evidence regarding postnatal zinc intake in children for prevention of developing asthma.
Conclusion
We summarize from evaluations of evidence from clinical studies that it is likely that breastfeeding and prolonged breastfeeding has a protective effect against developing asthma, and that vitamin D supplementation for pregnant mothers is quite likely to have a protective effect against developing asthma. Prenatal intake in pregnant mothers or postnatal intake in children of prebiotics or probiotics, dietary fatty acids, intensity of adherence to the Mediterranean Diet, vitamin C, vitamin E, or zinc for a protective effect for developing asthma were inconclusive due to a variety of reasons, including insufficient numbers of studies, lack of studies, or performance of studies in highly selected populations (Figure 2). If feasible, more high-quality RCTs using good dietary factor exposure and asthma incidence outcome definitions along with objective validation of exposure measurements would allow evidence appraiser to draw more confident conclusions. International consensus on these along with standardization of eligibility criteria and regimens of dietary factor if possible would be helpful so that meta-analyses can appropriately pool larger numbers of studies with larger pooled sample sizes for better power. Alternatively, if performing RCTs is impracticable, innovative nonrandomized study methods exist to estimate the same marginal relative average treatment effect as RCTs.
Abbreviations
2’ FL, 2’-fucosyllactose; AA, arachidonic acid; AAAAI, American Academy of Allergy, Asthma & Immunology; AAIAT, the Allergy Asthma and Immunology Association of Thailand; AAP, American Academy of Pediatrics; ACT, Asthma Control Test; ASCIA, Australasian Society of Clinical Immunology and Allergy; ALA, Alpha-linoleic acid; BALF, bronchoalveolar lavage fluid; CPS, Canadian Paediatric Society; CRP, C-reactive protein; CSACI, Canadian Society of Allergy and Clinical Immunology; DCs, Dendritic cells; DGA, Dietary Guidelines for Americans; DHA, docosahexaenoic acid; EAACI, The European Academy of Allergy and Clinical Immunology; EPA, eicosapentaenoic acid; ESCNH, European Standards of Care for Newborn Health; FENO, fractioned exhaled nitric oxide; FEV, Forced expiratory volume; FVC, forced vital capacity; GINA, Global Initiative for Asthma; HMOs, Human milk oligosaccharides; Ig, Immunoglobulin; IL, Interleukin; IPD, individual participant data; LA, linoleic acid; lcFOS, long-chain fructo-oligosaccharides; LC-PUFAs, long-chain polyunsaturated fatty acids, MUFA, monounsaturated fatty acid; n-3, Omega-3; n-6, Omega-6; PD1, protectin D1; PEFR, peak expiratory flow rate; PST, Pediatric Society of Thailand; PUFA, polyunsaturated fatty acid; RCT, Randomized controlled trial; SCFAs, short-chain fatty acids; scGOS, short-chain galacto-oligosaccharides; SFA, saturated fatty acid; Th2, T helper 2; TNF-α, Tumor necrosis factor-α; Tregs, regulatory T cells; UPFs, ultra-processed foods; US FDA, The United States Food and Drug Administration; VDR, Vitamin D receptor; WAO, World Allergy Organization; WGO, World Gastroenterology Organisation; WHO, World Health Organization.
Acknowledgments
We would like to thank Dr. Anthony Tan for editing the English language.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
All authors declare no personal or professional conflicts of interest relating to this review article.
References
1. Reddel HK, Bacharier LB, Bateman ED, et al. Global initiative for asthma strategy 2021: executive summary and rationale for key changes. Am J Respir Crit Care Med. 2022;205(1):17–35. doi:10.1164/rccm.202109-2205PP
2. Leung ASY, Tham EH, Li J, et al. The role of the environment in shaping the trends of childhood asthma - an Asian perspective. Pediatr Allergy Immunol. 2021;32(6):1152–1164. doi:10.1111/pai.13508
3. Sompornrattanaphan M, Thongngarm T, Ratanawatkul P, Wongsa C, Swigris JJ. The contribution of particulate matter to respiratory allergy. Asian Pac J Allergy Immunol. 2020;38(1):19–28. doi:10.12932/AP-100619-0579
4. Wadhwa V, Lodge CJ, Dharmage SC, Cassim R, Sly PD, Russell MA. The association of early life viral respiratory illness and atopy on asthma in children: systematic review and meta-analysis. J Allergy Clin Immunol Pract. 2020;8(8):2663–72 e7. doi:10.1016/j.jaip.2020.03.032
5. Alwarith J, Kahleova H, Crosby L, et al. The role of nutrition in asthma prevention and treatment. Nutr Rev. 2020;78(11):928–938. doi:10.1093/nutrit/nuaa005
6. Keogh RH, Shaw PA, Gustafson P, et al. STRATOS guidance document on measurement error and misclassification of variables in observational epidemiology: part 1-basic theory and simple methods of adjustment. Stat Med. 2020;39(16):2197–2231. doi:10.1002/sim.8532
7. Matsui EC, Keet CA. Weighing the evidence: bias and confounding in epidemiologic studies in allergy/immunology. J Allergy Clin Immunol. 2017;139(2):448–450. doi:10.1016/j.jaci.2016.09.030
8. Guyatt GH, Oxman AD, Kunz R, et al. GRADE guidelines 6. Rating the quality of evidence–imprecision. J Clin Epidemiol. 2011;64(12):1283–1293. doi:10.1016/j.jclinepi.2011.01.012
9. Altman DG. Practical Statistics for Medical Research. Boca Raton, Fla.: Chapman & Hall/CRC; 1999:xii, 611.
10. Ballard O, Morrow AL. Human milk composition: nutrients and bioactive factors. Pediatr Clin North Am. 2013;60(1):49–74. doi:10.1016/j.pcl.2012.10.002
11. Bode L, Jantscher-Krenn E. Structure-function relationships of human milk oligosaccharides. Adv Nutr. 2012;3(3):383S–91S. doi:10.3945/an.111.001404
12. Bode L. Human milk oligosaccharides: prebiotics and beyond. Nutr Rev. 2009;67(Suppl 2):S183–91. doi:10.1111/j.1753-4887.2009.00239.x
13. Donovan SM, Comstock SS. Human milk oligosaccharides influence neonatal mucosal and systemic immunity. Ann Nutr Metab. 2016;69(Suppl 2):42–51. doi:10.1159/000452818
14. van Esch B, Porbahaie M, Abbring S, et al. The impact of milk and its components on epigenetic programming of immune function in early life and beyond: implications for allergy and asthma. Front Immunol. 2020;11:2141. doi:10.3389/fimmu.2020.02141
15. Woo V, Alenghat T. Host-microbiota interactions: epigenomic regulation. Curr Opin Immunol. 2017;44:52–60. doi:10.1016/j.coi.2016.12.001
16. Kramer MS, Matush L, Vanilovich I, et al. Effect of prolonged and exclusive breast feeding on risk of allergy and asthma: cluster randomised trial. BMJ. 2007;335(7624):815. doi:10.1136/bmj.39304.464016.AE
17. Flohr C, Henderson AJ, Kramer MS, et al. Effect of an intervention to promote breastfeeding on asthma, lung function, and atopic eczema at age 16 years: follow-up of the PROBIT randomized trial. JAMA Pediatr. 2018;172(1):e174064. doi:10.1001/jamapediatrics.2017.4064
18. Dogaru CM, Nyffenegger D, Pescatore AM, Spycher BD, Kuehni CE. Breastfeeding and childhood asthma: systematic review and meta-analysis. Am J Epidemiol. 2014;179(10):1153–1167. doi:10.1093/aje/kwu072
19. Lodge CJ, Tan DJ, Lau MX, et al. Breastfeeding and asthma and allergies: a systematic review and meta-analysis. Acta Paediatr. 2015;104(467):38–53. doi:10.1111/apa.13132
20. Xue M, Dehaas E, Chaudhary N, O’Byrne P, Satia I, Kurmi OP. Breastfeeding and risk of childhood asthma: a systematic review and meta-analysis. ERJ Open Res. 2021;7(4):00504–2021. doi:10.1183/23120541.00504-2021
21. Brew BK, Allen CW, Toelle BG, Marks GB. Systematic review and meta-analysis investigating breast feeding and childhood wheezing illness. Paediatr Perinat Epidemiol. 2011;25(6):507–518. doi:10.1111/j.1365-3016.2011.01233.x
22. Harvey SM, Murphy VE, Gibson PG, et al. Maternal asthma, breastfeeding, and respiratory outcomes in the first year of life. Pediatr Pulmonol. 2020;55(7):1690–1696. doi:10.1002/ppul.24756
23. Peters RL, Kay T, McWilliam VL, et al. The interplay between eczema and breastfeeding practices may hide breastfeeding’s protective effect on childhood asthma. J Allergy Clin Immunol Pract. 2021;9(2):862–71 e5. doi:10.1016/j.jaip.2020.09.006
24. Naimi AI, Cole SR, Kennedy EH. An introduction to g methods. Int J Epidemiol. 2017;46(2):756–762. doi:10.1093/ije/dyw323
25. Shaw PA, Gustafson P, Carroll RJ, et al. STRATOS guidance document on measurement error and misclassification of variables in observational epidemiology: part 2-more complex methods of adjustment and advanced topics. Stat Med. 2020;39(16):2232–2263. doi:10.1002/sim.8531
26. Guarner F, Mary Ellen Sanders RE, Fedorak R, et al. Probiotics and prebiotics; 2017. Available from: https://www.worldgastroenterology.org/UserFiles/file/guidelines/probiotics-and-prebiotics-english-2017.pdf.
27. Sender R, Fuchs S, Milo R. Are we really vastly outnumbered? Revisiting the ratio of bacterial to host cells in humans. Cell. 2016;164(3):337–340. doi:10.1016/j.cell.2016.01.013
28. Eslami M, Bahar A, Keikha M, Karbalaei M, Kobyliak NM, Yousefi B. Probiotics function and modulation of the immune system in allergic diseases. Allergol Immunopathol. 2020;48(6):771–788. doi:10.1016/j.aller.2020.04.005
29. Lopez-Santamarina A, Gonzalez EG, Lamas A, Mondragon ADC, Regal P, Miranda JM. Probiotics as a possible strategy for the prevention and treatment of allergies. A narrative review. Foods. 2021;10(4):701.
30. Lee-Sarwar KA, Lasky-Su J, Kelly RS, Litonjua AA, Weiss ST. Metabolome-microbiome crosstalk and human disease. Metabolites. 2020;10(5):181. doi:10.3390/metabo10050181
31. Lee-Sarwar KA, Kelly RS, Lasky-Su J, et al. Integrative analysis of the intestinal metabolome of childhood asthma. J Allergy Clin Immunol. 2019;144(2):442–454. doi:10.1016/j.jaci.2019.02.032
32. Zheng D, Liwinski T, Elinav E. Interaction between microbiota and immunity in health and disease. Cell Res. 2020;30(6):492–506. doi:10.1038/s41422-020-0332-7
33. Atarashi K, Tanoue T, Shima T, et al. Induction of colonic regulatory T cells by indigenous Clostridium species. Science. 2011;331(6015):337–341. doi:10.1126/science.1198469
34. Henrick BM, Rodriguez L, Lakshmikanth T, et al. Bifidobacteria-mediated immune system imprinting early in life. Cell. 2021;184(15):3884–98.e11. doi:10.1016/j.cell.2021.05.030
35. Karimi K, Inman MD, Bienenstock J, Forsythe P. Lactobacillus reuteri-induced regulatory T cells protect against an allergic airway response in mice. Am J Respir Crit Care Med. 2009;179(3):186–193. doi:10.1164/rccm.200806-951OC
36. Weise C, Zhu Y, Ernst D, Kühl AA, Worm M. Oral administration of Escherichia coli Nissle 1917 prevents allergen-induced dermatitis in mice. Exp Dermatol. 2011;20(10):805–809. doi:10.1111/j.1600-0625.2011.01326.x
37. Hart AL, Lammers K, Brigidi P, et al. Modulation of human dendritic cell phenotype and function by probiotic bacteria. Gut. 2004;53(11):1602–1609. doi:10.1136/gut.2003.037325
38. Kawashima T, Ikari N, Kouchi T, et al. The molecular mechanism for activating IgA production by Pediococcus acidilactici K15 and the clinical impact in a randomized trial. Sci Rep. 2018;8(1):5065. doi:10.1038/s41598-018-23404-4
39. Prescott SL, Björkstén B. Probiotics for the prevention or treatment of allergic diseases. J Allergy Clin Immunol. 2007;120(2):255–262. doi:10.1016/j.jaci.2007.04.027
40. Hemarajata P, Versalovic J. Effects of probiotics on gut microbiota: mechanisms of intestinal immunomodulation and neuromodulation. Therap Adv Gastroenterol. 2013;6(1):39–51. doi:10.1177/1756283X12459294
41. Natarajan N, Pluznick JL. From microbe to man: the role of microbial short chain fatty acid metabolites in host cell biology. Am J Physiol Cell Physiol. 2014;307(11):C979–85. doi:10.1152/ajpcell.00228.2014
42. Colquitt AS, Miles EA, Calder PC. Do probiotics in pregnancy reduce allergies and asthma in infancy and childhood? A systematic review. Nutrients. 2022;14(9):1852. doi:10.3390/nu14091852
43. Dotterud CK, Storrø O, Johnsen R, Oien T. Probiotics in pregnant women to prevent allergic disease: a randomized, double-blind trial. Br J Dermatol. 2010;163(3):616–623. doi:10.1111/j.1365-2133.2010.09889.x
44. Simpson MR, Dotterud CK, Storrø O, Johnsen R, Øien T. Perinatal probiotic supplementation in the prevention of allergy related disease: 6 year follow up of a randomised controlled trial. BMC Dermatol. 2015;15:13. doi:10.1186/s12895-015-0030-1
45. Wickens K, Barthow C, Mitchell EA, et al. Maternal supplementation alone with Lactobacillus rhamnosus HN001 during pregnancy and breastfeeding does not reduce infant eczema. Pediatr Allergy Immunol. 2018;29(3):296–302. doi:10.1111/pai.12874
46. Arrieta MC, Stiemsma LT, Dimitriu PA, et al. Early infancy microbial and metabolic alterations affect risk of childhood asthma. Sci Transl Med. 2015;7(307):307ra152. doi:10.1126/scitranslmed.aab2271
47. Wawryk-Gawda E, Markut-Miotła E, Emeryk A. Postnatal probiotics administration does not prevent asthma in children, but using prebiotics or synbiotics may be the effective potential strategies to decrease the frequency of asthma in high-risk children - a meta-analysis of clinical trials. Allergol Immunopathol. 2021;49(4):4–14. doi:10.15586/aei.v49i4.69
48. Brown HA, Marnett LJ. Introduction to lipid biochemistry, metabolism, and signaling. Chem Rev. 2011;111(10):5817–5820. doi:10.1021/cr200363s
49. Radzikowska U, Rinaldi AO, Celebi Sozener Z, et al. The influence of dietary fatty acids on immune responses. Nutrients. 2019;11(12):2990. doi:10.3390/nu11122990
50. Venter C, Meyer RW, Nwaru BI, et al. EAACI position paper: influence of dietary fatty acids on asthma, food allergy, and atopic dermatitis. Allergy. 2019;74(8):1429–1444. doi:10.1111/all.13764
51. Lee-Sarwar KA, Lasky-Su J, Kelly RS, Litonjua AA, Weiss ST. Gut microbial-derived metabolomics of asthma. Metabolites. 2020;10(3):97. doi:10.3390/metabo10030097
52. Wendell SG, Baffi C, Holguin F. Fatty acids, inflammation, and asthma. J Allergy Clin Immunol. 2014;133(5):1255–1264. doi:10.1016/j.jaci.2013.12.1087
53. Kazani S, Planaguma A, Ono E, et al. Exhaled breath condensate eicosanoid levels associate with asthma and its severity. J Allergy Clin Immunol. 2013;132(3):547–553. doi:10.1016/j.jaci.2013.01.058
54. Miyata J, Fukunaga K, Iwamoto R, et al. Dysregulated synthesis of protectin D1 in eosinophils from patients with severe asthma. J Allergy Clin Immunol. 2013;131(2):
55. Rucci E, den Dekker HT, de Jongste JC, et al. Maternal fatty acid levels during pregnancy, childhood lung function and atopic diseases. The Generation R study. Clin Exp Allergy. 2016;46(3):461–471. doi:10.1111/cea.12613
56. Venter C, Agostoni C, Arshad SH, et al. Dietary factors during pregnancy and atopic outcomes in childhood: a systematic review from the European Academy of Allergy and Clinical Immunology. Pediatr Allergy Immunol. 2020;31(8):889–912. doi:10.1111/pai.13303
57. Lin J, Zhang Y, Zhu X, Wang D, Dai J. Effects of supplementation with omega-3 fatty acids during pregnancy on asthma or wheeze of children: a systematic review and meta-analysis. J Matern Fetal Neonatal Med. 2020;33(10):1792–1801. doi:10.1080/14767058.2018.1529161
58. Lee-Sarwar K, Kelly RS, Lasky-Su J, et al. Dietary and plasma polyunsaturated fatty acids are inversely associated with asthma and atopy in early childhood. J Allergy Clin Immunol Pract. 2019;7(2):529–38.e8. doi:10.1016/j.jaip.2018.07.039
59. Brick T, Schober Y, Böcking C, et al. ω-3 fatty acids contribute to the asthma-protective effect of unprocessed cow’s milk. J Allergy Clin Immunol. 2016;137(6):1699–706.e13. doi:10.1016/j.jaci.2015.10.042
60. Talaei M, Sdona E, Calder PC, et al. Intake of n −3 polyunsaturated fatty acids in childhood, FADS genotype and incident asthma. Eur Respir J. 2021;58(3):2003633. doi:10.1183/13993003.03633-2020
61. Muley P, Shah M, Muley A. Omega-3 fatty acids supplementation in children to prevent asthma: is it worthy?-A systematic review and meta-analysis. J Allergy. 2015;2015:312052. doi:10.1155/2015/312052
62. Yang H, Xun P, He K. Fish and fish oil intake in relation to risk of asthma: a systematic review and meta-analysis. PLoS One. 2013;8(11):e80048. doi:10.1371/journal.pone.0080048
63. Bender R, Friede T, Koch A, et al. Methods for evidence synthesis in the case of very few studies. Res Synth Methods. 2018;9(3):382–392. doi:10.1002/jrsm.1297
64. Higgins JPT; Cochrane Collaboration. Cochrane Handbook for Systematic Reviews of Interventions.
65. von Hippel PT. The heterogeneity statistic I(2) can be biased in small meta-analyses. BMC Med Res Methodol. 2015;15:35. doi:10.1186/s12874-015-0024-z
66. Schulz A, Schürmann C, Skipka G, Bender R. Performing meta-analyses with very few studies. Methods Mol Biol. 2022;2345:91–102.
67. Seide SE, Röver C, Friede T. Likelihood-based random-effects meta-analysis with few studies: empirical and simulation studies. BMC Med Res Methodol. 2019;19(1):16. doi:10.1186/s12874-018-0618-3
68. Trichopoulou A, Costacou T, Bamia C, Trichopoulos D. Adherence to a Mediterranean diet and survival in a Greek population. N Engl J Med. 2003;348(26):2599–2608. doi:10.1056/NEJMoa025039
69. Medina-Remon A, Kirwan R, Lamuela-Raventos RM, Estruch R. Dietary patterns and the risk of obesity, type 2 diabetes mellitus, cardiovascular diseases, asthma, and neurodegenerative diseases. Crit Rev Food Sci Nutr. 2018;58(2):262–296. doi:10.1080/10408398.2016.1158690
70. Hosseini B, Berthon BS, Wark P, Wood LG. Effects of fruit and vegetable consumption on risk of asthma, wheezing and immune responses: a systematic review and meta-analysis. Nutrients. 2017;9(4):341. doi:10.3390/nu9040341
71. Chambers ES, Preston T, Frost G, Morrison DJ. Role of gut microbiota-generated short-chain fatty acids in metabolic and cardiovascular health. Curr Nutr Rep. 2018;7(4):198–206. doi:10.1007/s13668-018-0248-8
72. Reyes-Angel J, Han YY, Litonjua AA, Celedon JC. Diet and asthma: is the sum more important than the parts? J Allergy Clin Immunol. 2021;148(3):706–707. doi:10.1016/j.jaci.2021.04.030
73. Yip W, Hughes MR, Li Y, et al. Butyrate shapes immune cell fate and function in allergic asthma. Front Immunol. 2021;12:628453. doi:10.3389/fimmu.2021.628453
74. Caballero-Pérez CA. An update of the KIDMED questionnaire, a Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. 2019;14:2543–2547.
75. Zhang Y, Lin J, Fu W, Liu S, Gong C, Dai J. Mediterranean diet during pregnancy and childhood for asthma in children: a systematic review and meta-analysis of observational studies. Pediatr Pulmonol. 2019;54(7):949–961. doi:10.1002/ppul.24338
76. Chambers ES, Hawrylowicz CM. The impact of vitamin D on regulatory T cells. Curr Allergy Asthma Rep. 2011;11(1):29–36. doi:10.1007/s11882-010-0161-8
77. Amrein K, Scherkl M, Hoffmann M, et al. Vitamin D deficiency 2.0: an update on the current status worldwide. Eur J Clin Nutr. 2020;74(11):1498–1513. doi:10.1038/s41430-020-0558-y
78. Siddiqee MH, Bhattacharjee B, Siddiqi UR, MeshbahurRahman M. High prevalence of vitamin D deficiency among the South Asian adults: a systematic review and meta-analysis. BMC Public Health. 2021;21(1):1823. doi: 10.1186/s12889-021-11888-1
79. Hewison M. Vitamin D and innate and adaptive immunity. Vitam Horm. 2011;86:23–62.
80. Tsoukas CD, Provvedini DM, Manolagas SC. 1,25-dihydroxyvitamin D3: a novel immunoregulatory hormone. Science. 1984;224(4656):1438–1440. doi:10.1126/science.6427926
81. Penna G, Adorini L. 1 alpha, 25-dihydroxyvitamin D3 inhibits differentiation, maturation, activation, and survival of dendritic cells leading to impaired alloreactive T cell activation. J Immunol. 2000;164(5):2405–2411. doi:10.4049/jimmunol.164.5.2405
82. Akdis CA, Akdis M. Mechanisms and treatment of allergic disease in the big picture of regulatory T cells. J Allergy Clin Immunol. 2009;123(4):
83. Poon AH, Mahboub B, Hamid Q. Vitamin D deficiency and severe asthma. Pharmacol Ther. 2013;140(2):148–155. doi:10.1016/j.pharmthera.2013.06.006
84. Raby BA, Lazarus R, Silverman EK, et al. Association of vitamin D receptor gene polymorphisms with childhood and adult asthma. Am J Respir Crit Care Med. 2004;170(10):1057–1065. doi:10.1164/rccm.200404-447OC
85. Saadi A, Gao G, Li H, Wei C, Gong Y, Liu Q. Association study between vitamin D receptor gene polymorphisms and asthma in the Chinese Han population: a case-control study. BMC Med Genet. 2009;10:71. doi:10.1186/1471-2350-10-71
86. Vollmert C, Illig T, Altmuller J, et al. Single nucleotide polymorphism screening and association analysis–exclusion of integrin beta 7 and vitamin D receptor (chromosome 12q) as candidate genes for asthma. Clin Exp Allergy. 2004;34(12):1841–1850. doi:10.1111/j.1365-2222.2004.02047.x
87. Wjst M. Variants in the vitamin D receptor gene and asthma. BMC Genet. 2005;6:2. doi:10.1186/1471-2156-6-2
88. Wjst M, Altmuller J, Faus-Kessler T, Braig C, Bahnweg M, Andre E. Asthma families show transmission disequilibrium of gene variants in the vitamin D metabolism and signalling pathway. Respir Res. 2006;7:60. doi:10.1186/1465-9921-7-60
89. Wittke A, Weaver V, Mahon BD, August A, Cantorna MT. Vitamin D receptor-deficient mice fail to develop experimental allergic asthma. J Immunol. 2004;173(5):3432–3436. doi:10.4049/jimmunol.173.5.3432
90. Wittke A, Chang A, Froicu M, et al. Vitamin D receptor expression by the lung micro-environment is required for maximal induction of lung inflammation. Arch Biochem Biophys. 2007;460(2):306–313. doi:10.1016/j.abb.2006.12.011
91. Bosse Y, Maghni K, Hudson TJ. 1alpha, 25-dihydroxy-vitamin D3 stimulation of bronchial smooth muscle cells induces autocrine, contractility, and remodeling processes. Physiol Genomics. 2007;29(2):161–168. doi:10.1152/physiolgenomics.00134.2006
92. Shi D, Wang D, Meng Y, Chen J, Mu G, Chen W. Maternal vitamin D intake during pregnancy and risk of asthma and wheeze in children: a systematic review and meta-analysis of observational studies. J Matern Fetal Neonatal Med. 2021;34(4):653–659. doi:10.1080/14767058.2019.1611771
93. Yepes-Nunez JJ, Brozek JL, Fiocchi A, et al. Vitamin D supplementation in primary allergy prevention: systematic review of randomized and non-randomized studies. Allergy. 2018;73(1):37–49. doi:10.1111/all.13241
94. Hibbs AM, Ross K, Kerns LA, et al. Effect of vitamin D supplementation on recurrent wheezing in black infants who were born preterm: the D-wheeze randomized clinical trial. JAMA. 2018;319(20):2086–2094. doi:10.1001/jama.2018.5729
95. Padayatty SJ, Katz A, Wang Y, et al. Vitamin C as an antioxidant: evaluation of its role in disease prevention. J Am Coll Nutr. 2003;22(1):18–35. doi:10.1080/07315724.2003.10719272
96. Block G, Jensen CD, Dalvi TB, et al. Vitamin C treatment reduces elevated C-reactive protein. Free Radic Biol Med. 2009;46(1):70–77. doi:10.1016/j.freeradbiomed.2008.09.030
97. McKeever TM, Britton J. Diet and asthma. Am J Respir Crit Care Med. 2004;170(7):725–729. doi:10.1164/rccm.200405-611PP
98. Jeong YJ, Kim JH, Kang JS, Lee WJ, Hwang YI. Mega-dose vitamin C attenuated lung inflammation in mouse asthma model. Anat Cell Biol. 2010;43(4):294–302. doi:10.5115/acb.2010.43.4.294
99. Beckhaus AA, Garcia-Marcos L, Forno E, Pacheco-Gonzalez RM, Celedon JC, Castro-Rodriguez JA. Maternal nutrition during pregnancy and risk of asthma, wheeze, and atopic diseases during childhood: a systematic review and meta-analysis. Allergy. 2015;70(12):1588–1604. doi:10.1111/all.12729
100. McEvoy CT, Schilling D, Clay N, et al. Vitamin C supplementation for pregnant smoking women and pulmonary function in their newborn infants: a randomized clinical trial. JAMA. 2014;311(20):2074–2082. doi:10.1001/jama.2014.5217
101. Nurmatov U, Devereux G, Sheikh A. Nutrients and foods for the primary prevention of asthma and allergy: systematic review and meta-analysis. J Allergy Clin Immunol. 2011;127(3):
102. Health. OoDSatNIo. Dietary supplement fact sheet: vitamin E; 2022. Available from: http://ods.od.nih.gov/factsheets/VitaminE.
103. Singh U, Devaraj S. Vitamin E: inflammation and atherosclerosis. Vitam Horm. 2007;76:519–549.
104. Mora JR, Iwata M, von Andrian UH. Vitamin effects on the immune system: vitamins A and D take centre stage. Nat Rev Immunol. 2008;8(9):685–698. doi:10.1038/nri2378
105. Pekmezci D. Vitamin E and immunity. Vitam Horm. 2011;86:179–215. doi:10.1016/B978-0-12-386960-9.00008-3
106. Morante M, Sandoval J, Gomez-Cabrera MC, et al. Vitamin E deficiency induces liver nuclear factor-kappaB DNA-binding activity and changes in related genes. Free Radic Res. 2005;39(10):1127–1138. doi:10.1080/10715760500193820
107. Suzuki YJ, Packer L. Inhibition of NF-kappa B activation by vitamin E derivatives. Biochem Biophys Res Commun. 1993;193(1):277–283. doi:10.1006/bbrc.1993.1620
108. Jialal I, Devaraj S, Kaul N. The effect of alpha-tocopherol on monocyte proatherogenic activity. J Nutr. 2001;131(2):389S–94S. doi:10.1093/jn/131.2.389S
109. Devaraj S, Jialal I. Alpha-tocopherol decreases interleukin-1 beta release from activated human monocytes by inhibition of 5-lipoxygenase. Arterioscler Thromb Vasc Biol. 1999;19(4):1125–1133. doi:10.1161/01.ATV.19.4.1125
110. Munteanu A, Zingg JM. Cellular, molecular and clinical aspects of vitamin E on atherosclerosis prevention. Mol Aspects Med. 2007;28(5–6):538–590. doi:10.1016/j.mam.2007.07.001
111. Li-Weber M, Giaisi M, Treiber MK, Krammer PH. Vitamin E inhibits IL-4 gene expression in peripheral blood T cells. Eur J Immunol. 2002;32(9):2401–2408. doi:10.1002/1521-4141(200209)32:9<2401::AID-IMMU2401>3.0.CO;2-S
112. Dworski R, Han W, Blackwell TS, Hoskins A, Freeman ML. Vitamin E prevents NRF2 suppression by allergens in asthmatic alveolar macrophages in vivo. Free Radic Biol Med. 2011;51(2):516–521. doi:10.1016/j.freeradbiomed.2011.04.040
113. Devereux G, Barker RN, Seaton A. Antenatal determinants of neonatal immune responses to allergens. Clin Exp Allergy. 2002;32(1):43–50. doi:10.1046/j.0022-0477.2001.01267.x
114. Wu H, Zhang C, Wang Y, Li Y. Does vitamin E prevent asthma or wheeze in children: a systematic review and meta-analysis. Paediatr Respir Rev. 2018;27:60–68. doi:10.1016/j.prrv.2017.08.002
115. Maslova E, Hansen S, Strøm M, Halldorsson TI, Olsen SF. Maternal intake of vitamins A, E and K in pregnancy and child allergic disease: a longitudinal study from the Danish National Birth Cohort. Br J Nutr. 2014;111(6):1096–1108. doi:10.1017/S0007114513003395
116. Hamalainen N, Nwaru BI, Erlund I, et al. Serum carotenoid and tocopherol concentrations and risk of asthma in childhood: a nested case-control study. Clin Exp Allergy. 2017;47(3):401–409. doi:10.1111/cea.12904
117. Wessels I, Maywald M, Rink L. Zinc as a Gatekeeper of Immune Function. Nutrients. 2017;9(12):1286. doi:10.3390/nu9121286
118. Maywald M, Wessels I, Rink L. Zinc signals and immunity. Int J Mol Sci. 2017;18(10):2222. doi:10.3390/ijms18102222
119. Honscheid A, Rink L, Haase H. T-lymphocytes: a target for stimulatory and inhibitory effects of zinc ions. Endocr Metab Immune Disord Drug Targets. 2009;9(2):132–144. doi:10.2174/187153009788452390
120. Lu H, Xin Y, Tang Y, Shao G. Zinc suppressed the airway inflammation in asthmatic rats: effects of zinc on generation of eotaxin, MCP-1, IL-8, IL-4, and IFN-gamma. Biol Trace Elem Res. 2012;150(1–3):314–321. doi:10.1007/s12011-012-9493-7
121. Ghaffari J, Alizadeh-Navaei R, Dabaghzadeh A, Ghaffari N. Serum zinc level and children`s asthma: a systematic and meta-analysis review article. Caspian J Intern Med. 2021;12(3):236–242. doi:10.22088/cjim.12.3.236
122. Litonjua AA, Lange NE, Carey VJ, et al. The Vitamin D Antenatal Asthma Reduction Trial (VDAART): rationale, design, and methods of a randomized, controlled trial of vitamin D supplementation in pregnancy for the primary prevention of asthma and allergies in children. Contemp Clin Trials. 2014;38(1):37–50. doi:10.1016/j.cct.2014.02.006
123. Miyake Y, Sasaki S, Tanaka K, Hirota Y. Consumption of vegetables, fruit, and antioxidants during pregnancy and wheeze and eczema in infants. Allergy. 2010;65(6):758–765. doi:10.1111/j.1398-9995.2009.02267.x
124. Abrams EM, Orkin J, Cummings C, Blair B, Chan ES. Dietary exposures and allergy prevention in high-risk infants. Paediatr Child Health. 2021;26(8):504–505. doi:10.1093/pch/pxab064
125. U.S. Department of Agriculture and U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2020-2025 [Internet]. 2020 Dec. Available from: https://www.dietaryguidelines.gov. Accessed August 17, 2022.
126. The Allergy, Asthma and Immunology Association of Thailand. AAIAT-Allergy Prevention Guideline 2020 Short Summary [Internet]. 2021 Jul. Available from: https://allergy.or.th/2016/resources_guideline.php. Accessed August 17, 2022.
127. The European Standards of Care for Newborn Health project report [Internet]. Available from: European Standards of Care for Newborn Health. Available from: https://www.efcni.org/wp-content/uploads/2018/11/2018_11_16_ESCNH_Report_final.pdf. Accessed August 17, 2022.
128. Joshi PA, Smith J, Vale S, Campbell DE. The Australasian Society of Clinical Immunology and Allergy infant feeding for allergy prevention guidelines. Med J Aust. 2019;210(2):89–93. doi:10.5694/mja2.12102
129. Greer FR, Sicherer SH, Burks AW; Committee On N, Section On A, Immunology. The effects of early nutritional interventions on the development of atopic disease in infants and children: the role of maternal dietary restriction, breastfeeding, hydrolyzed formulas, and timing of introduction of allergenic complementary foods. Pediatrics. 2019;143(4). doi:10.1542/peds.2019-0281
130. Guideline: protecting, promoting and supporting breastfeeding in facilities providing maternity and newborn services. Geneva: World Health Organization; 2017. Available from: https://www.who.int/publications/i/item/9789241550086.
131. Fleischer DM, Spergel JM, Assa’ad AH, Pongracic JA. Primary prevention of allergic disease through nutritional interventions. J Allergy Clin Immunol Pract. 2013;1(1):29–36. doi:10.1016/j.jaip.2012.09.003
132. Fleischer DM, Spergel JM, Assa’ad AH, Pongracic JA. Primary prevention of allergic disease through nutritional interventions: guidelines for healthcare professionals. Am Acad Asthma Allergy Immunol. 2015;1:29–36.
133. Pelkonen AS, Kuitunen M, Dunder T, et al. Allergy in children: practical recommendations of the Finnish Allergy Programme 2008–2018 for prevention, diagnosis, and treatment. Pediatr Allergy Immunol. 2012;23(2):103–116. doi:10.1111/j.1399-3038.2012.01298.x
134. Haahtela T, Valovirta E, Saarinen K, et al. The Finnish Allergy Program 2008–2018: society-wide proactive program for change of management to mitigate allergy burden. J Allergy Clin Immunol. 2021;148(2):319–26 e4. doi:10.1016/j.jaci.2021.03.037
135. Asthma GIf. Global Strategy for Asthma Management and Prevention. 2022.
136. Cuello-Garcia CA, Fiocchi A, Pawankar R, et al. World Allergy Organization-McMaster University Guidelines for Allergic Disease Prevention (GLAD-P): prebiotics. World Allergy Organ J. 2016;9:10. doi:10.1186/s40413-016-0102-7
137. Fiocchi A, Pawankar R, Cuello-Garcia C, et al. World Allergy Organization-McMaster University Guidelines for Allergic Disease Prevention (GLAD-P): probiotics. World Allergy Organ J. 2015;8(1):4. doi:10.1186/s40413-015-0055-2
138. van den Akker CHP, van Goudoever JB, Shamir R, et al. Probiotics and preterm infants: a position paper by the European Society for Paediatric Gastroenterology Hepatology and Nutrition Committee on Nutrition and the European Society for Paediatric Gastroenterology Hepatology and Nutrition Working Group for probiotics and prebiotics. J Pediatr Gastroenterol Nutr. 2020;70(5):664–680. doi:10.1097/MPG.0000000000002655
139. Braegger C, Chmielewska A, Decsi T, et al. Supplementation of infant formula with probiotics and/or prebiotics: a systematic review and comment by the ESPGHAN committee on nutrition. J Pediatr Gastroenterol Nutr. 2011;52(2):238–250. doi:10.1097/MPG.0b013e3181fb9e80
140. Haahtela T, von Hertzen L, Anto JM, et al. Helsinki by nature: the nature step to respiratory health. Clin Transl Allergy. 2019;9:57. doi:10.1186/s13601-019-0295-2
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Dietary Supplementations and Depression
Thurfah JN, Christine, Bagaskhara PP, Alfian SD, Puspitasari IM
Journal of Multidisciplinary Healthcare 2022, 15:1121-1141
Published Date: 17 May 2022
Dietary Intervention and Supplements in the Management of Psoriasis: Current Perspectives
Chung M, Bartholomew E, Yeroushalmi S, Hakimi M, Bhutani T, Liao W
Psoriasis: Targets and Therapy 2022, 12:151-176
Published Date: 22 June 2022
Physicians’ Understanding of the Role of the Microbiome in Allergies and Asthma: A Questionnaire-Based Study in Saudi Arabia
AlKhater S
Journal of Asthma and Allergy 2022, 15:1081-1091
Published Date: 16 August 2022
Study on Intestinal Flora and Asthma: Knowledge Graph Analysis Based on CiteSpace (2001–2021)
Zheng H, Dai H, Yan X, Xiang Q
Journal of Asthma and Allergy 2023, 16:355-364
Published Date: 5 April 2023
Evaluating the Efficacy and Safety of EZC Pak, a 5-Day Combination Echinacea-Zinc-Vitamin C Dose Pack with or without Vitamin D, in the Management of Outpatient Upper Respiratory Infections
Radhakrishnan A, Spencer S, Yanamala N, Malepati S
Infection and Drug Resistance 2023, 16:2561-2572
Published Date: 3 May 2023