Back to Journals » Infection and Drug Resistance » Volume 19
Development and Validation of a Preoperative Nomogram for Predicting Prolonged Hospital Stay After Spinal Tuberculosis Surgery
Received 21 September 2025
Accepted for publication 14 January 2026
Published 20 January 2026 Volume 2026:19 564043
DOI https://doi.org/10.2147/IDR.S564043
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hazrat Bilal
Li Li,* Alimujiang Yusufu,* Yuan Ma
Spine Surgery Department, Sixth Affiliated Hospital of Xinjiang Medical University, Urumqi, Xinjiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yuan Ma, Email [email protected]
Objective: The purpose of this study was to determine the risk factors that affect prolonged length of stay (LOS) after debridement, bone grafting, fusion and internal fixation for spinal tuberculosis, and to establish and validate a prediction model.
Methods: A retrospective study was conducted on 102 patients hospitalized for spinal tuberculosis at a single center from September 2017 to January 2024. Using the 75th percentile of length of stay as the cut-off value, a stay ≥ 13 days was defined as prolonged LOS. Univariate and binary logistic regression analyses were performed to identify independent risk factors. A nomogram prediction model was developed and its performance was evaluated using the area under the receiver operating characteristic curve AUC with internal validation.
Results: The average length of stay was (10.63± 3.01) days, with 26 patients (25.5%) having prolonged length of stay. Binary Logistic regression showed that Emaciation (OR=6.598, 95% CI 1.264– 42.462, P=0.031), severe pain (OR=10.776, 95% CI 2.613– 56.910, P=0.002), elevated Erythrocyte sedimentation Rate (OR=1.091, 95% CI 1.025– 1.183, P=0.014) and elevated C-reactive protei (OR=1.076, 95% CI 1.027– 1.141, P=0.005) were independent risk factors. The AUC of the joint prediction model was 0.928 (95% CI: 0.878– 0.977), indicating good predictive value.
Conclusion: Emaciation, severe pain, elevated Erythrocyte sedimentation Rate and elevated C-reactive protein are independent risk factors for prolonged length of stay after surgery for spinal tuberculosis. The developed nomogram can assist clinicians in preoperative identification of high-risk patients and optimizing perioperative management strategies.
Keywords: spinal tuberculosis, length of stay, LOS, risk factors, predictive model
Introduction
Tuberculosis (TB) remains a major global public health challenge, with an estimated 10.6 million new cases and 1.6 million deaths reported worldwide in 2021, according to the World Health Organization (WHO). Although pulmonary tuberculosis (PTB) constitutes the majority of cases, extrapulmonary tuberculosis (EPTB) accounts for approximately 15–20% of all TB cases, with spinal tuberculosis being one of the most common and debilitating forms of EPTB, particularly in endemic regions such as China.1,2 Spinal tuberculosis accounts for more than 50% of bone and joint tuberculosis. It is the most common clinical bone tuberculosis. It is caused by Mycobacterium tuberculosis invading the spine and is often secondary to pulmonary tuberculosis.3,4 Spinal tuberculosis is slow and insidious in onset, with pain as the main clinical manifestation. If diagnosis and treatment are not timely, irreversible nerve damage or even paralysis often occurs, bringing a heavy social and economic burden to patients.2,5 Combined anti-tuberculotic drugs is the gold standard for the treatment of spinal tuberculosis. The purposes of the operation are to clear tuberculosis lesions, relieve spinal cord and nerve compression, correct deformities, and restore spinal stability.5–7 However, surgery is characterized by large trauma, high postoperative complications, slow postoperative recovery, and long hospital stays.8,9 Prolonged length of stay (LOS) will increase the incidence of complications such as lower limb deep vein thrombosis, hypostatic pneumonia, and nosocomial acquired infections,10 thus affecting the prognosis of patients with spinal tuberculosis. Therefore, reducing LOS is an important indicator for evaluating the treatment effect.
The average LOS length of patients has been used as an important indicator to evaluate hospital medical resource utilization, diagnosis and treatment level and nursing management quality.3 Therefore, identifying the risk factors that may lead to prolonged LOS after spinal tuberculosis focus debridement, bone grafting, fusion and internal fixation, and then conducting targeted intervention or identification of these patients before surgery can further reduce the incidence of complications caused by prolonged hospitalization, reduce medical expenses and avoid waste of resources. This study intends to explore the key factors affecting LOS after focus debridement, bone grafting, fusion and internal fixation in patients with spinal tuberculosis, and build a prediction model, in order to provide theoretical guidance for perioperative management of patients with spinal tuberculosis and effective improvement of resource allocation in hospitals.
Materials and Methods
Patients
From September 2017 to January 2024, 102 patients hospitalized in the Spinal Surgery Department of our hospital due to spinal tuberculosis were selected from the Sixth Affiliated Hospital of Xinjiang Medical University who underwent tuberculosis focus clearance and bone graft fusion. The 75th percentile of the patient’s hospital stay was used as the critical value. When the hospitalization time was greater than the 75th percentile, it was defined as prolonged hospitalization time.11 The workflow of this study is shown in Figure 1. This study was approved by the Ethics Committee of our hospital (No. LFYLLSC20230829-10) and followed the guidelines of the Helsinki Declaration. Each patient provided written informed consent before participating in the study.
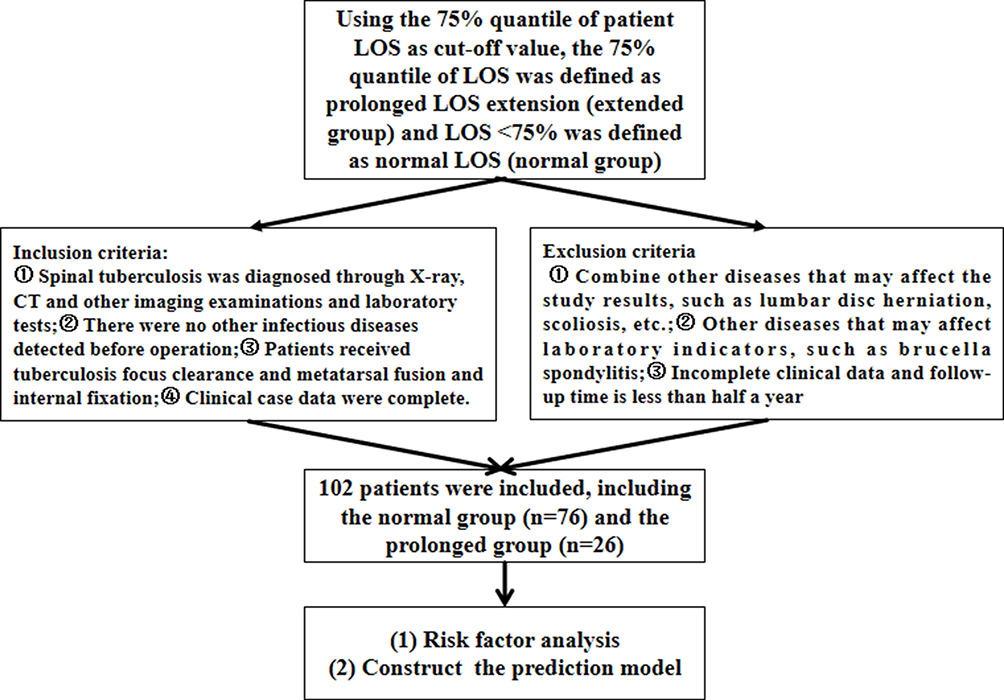 |
Figure 1 Flow chart of case screening. |
Diagnostic Criteria and Surgical Indications for Spinal Tuberculosis
Diagnostic criteria: The patient had or had previous tuberculosis in other parts, and clinical manifestations included low-grade fever, night sweats, weight loss, pain in spinal lesion sites, and pain on percussion; preoperative imaging examination showed disc destruction, paravertebral abscess, and compression myelopathy; Laboratory examination showed abnormalities in CRP, ESR, tuberculin test and other indicators; tuberculous granulation tissue or caseous necrosis was found in postoperative pathology.12
Surgical indications: (1) Spinal tuberculosis causes local refractory pain and poor quality of life, and symptoms are not significantly relieved after standardized anti-tuberculosis treatment; (2) Under standardized anti-tuberculosis treatment, the refractory pain symptoms are not relieved, and tuberculosis lesions and abscesses increase and progress; (3) Spinal tuberculosis is still delayed or spinal damage tends to expand; (4) Spinal tuberculosis lesions are compressed by pus, tuberculous granulation tissue, caseous necrotic substances, dead bones, etc. on the spinal cord, causing sensory and motor disorders; (5) Tuberculosis lesions lead to the destruction of local stability of the spine, and even local kyphosis and refractory pain; (6) After the spinal tuberculosis lesions are cured, obvious kyphosis remains behind, accompanied by local pain or delayed paralysis.13
Microbiological confirmation was obtained through acid-fast bacilli (AFB) staining, Mycobacterium tuberculosis culture, and/or molecular testing (such as GeneXpert MTB/RIF) from pus or tissue samples when available.
Inclusion and Exclusion Criteria
Inclusion criteria: ①Spinal tuberculosis was diagnosed through X-ray, CT and other imaging examinations and laboratory tests;②There were no other infectious diseases detected before operation;③Patients received tuberculosis focus clearance and metatarsal fusion and internal fixation;④Clinical case data were complete.
Exclusion criteria: ①Combine other diseases that may affect the study results, such as lumbar disc herniation, scoliosis, etc.;②Other diseases that may affect laboratory indicators, such as brucella spondylitis;③Incomplete clinical data and follow-up time is less than half a year.
Outcome Measures
Collect patient general data, surgical data, laboratory test results and imaging results. General data include gender, age, body mass index (BMI), whether he is emaciated (weight loss exceeds 5% in the past 3 months),14 whether he is Pain severity (VAS):≤6 = mild/moderate, >6 = severe), diabetes, history of smoking, history of alcohol consumption, history of anticoagulation, preoperative anti-tuberculosis time, and whether he is combined with other parts.
Surgical data include surgical sitesurgical, approach surgical time, intraoperative blood loss, postoperative anemia, blood transfusion, postoperative drainage volume and number of fused vertebrae.
Laboratory test results include white blood cells, CRP (The normal reference range is ≤8-10 mg/L), ESR (Males typically have 0–15 mm/h, females 0–20 mm/h), albumin (ALB), hemoglobin (HB) and D-dimer; Imaging results include whether there is x-ray vertebral destruction, x-ray osteophytes, x-ray endplate hardening, CT vertebral destruction, CT endplate hardening, MRI paravertebral abscess, and MRI spinal stenosis.
Preoperative Intervention and Surgical Methods
All patients received regular oral quadruple anti-tuberculosis drugs before surgery:isoniazid 0.3g/d+ rifampicin 0.45g/d+ pyrazinamide 30mg/(kg·d)+ ethambutol 15mg/(kg·d), and the chemotherapeutic drugs were adjusted according to drug sensitivity results.13
After anesthesia, the patient was placed in a prone position. Place the patient’s abdomen on a soft cushion, disinfect the surgical area, and apply sterile gauze. 2g of cefuroxime sodium was injected intravenously, and the tissue was separated layer by layer through a posterior median incision to expose the diseased tissue and thoroughly debridement. The remaining disc, nucleus pulposus and endplate cartilage were curettaged for complete decompression. Screws were implanted, attachment rods were installed, and intervertebral bone grafting was performed. The left posterior wound was rinsed, anti-tuberculosis drugs (streptomycin 1g+ isoniazid 300mg) and 2 drainage tubes were placed at the lesion, and the incision was sealed in layers12 (The specific surgical method is shown in Figure 2A–H).
 |
Figure 2 A 53-year-old male patient with lumbar tuberculosis bacilli spondylitis underwent posterior lumbar fusion and pedicle screw fixation. Notes: Preoperative lumbar anteroposterior and lateral X-rays (A and B) demonstrate tuberculous bacillary spondylitis of the L2 vertebra. Preoperative transverse and sagittal CT scans (C and D) reveal bone erosion and destruction of the lumbar vertebral body with vertebral body fragmentation. Postoperative anteroposterior and lateral X-rays (E and F) confirm proper positioning of the pedicle rods without fracture, with complete bony fusion between vertebral bodies. Postoperative transverse and sagittal CT scans (G and H) demonstrate adequate vertebral bone grafting. |
Cefuroxime sodium (2g intravenous) was administered as a prophylactic antibiotic against common surgical site infections, following institutional protocols for clean-contaminated spinal surgeries. This is in addition to the ongoing anti-tuberculosis chemotherapy.
Statistical Analysis
Statistical analysis was performed using SPSS26.0 statistical software (IBM, USA). Measurement data such as age, D-dimer and albumin follow a normal distribution after normality test and are expressed as x±s, and inter-group comparisons are performed using independent sample t-test; measurement data such as BMI, erythrocyte sedimentation rate, C-reactive protein, and white blood cell count do not follow a normal distribution after normality test and are expressed as M(Q1, Q3), and inter-group comparisons are performed using Mann Whitney U-test. Gender, weight loss, degree of pain, diabetes, smoking history, drinking history, anti-coagulation history, anti-tuberculosis time, whether there is tuberculosis in other sites, whether there is spinal stenosis, paravertebral abscess, endplate sclerosis, osteophytes, etc. Counting data are expressed using frequency (cases,%), and comparisons between groups are used using X2 test or Fisher’s exact test (The 75th percentile of LOS was selected as the cut-off value to define prolonged hospitalization, a method consistent with previous studies investigating prolonged stay in surgical populations where no standard clinical definition is available).
Results
General Patient Information
We included a total of 102 patients with spinal tuberculosis based on the inclusion and exclusion criteria. Among them, 26 were males and 76 were females. The hospitalization time of all patients was 10.63±3.01 (5–20) days, and 75% of the patients were hospitalized for 13 days. Therefore, those with hospitalization time ≥13 days were assigned to the extended group (26 patients, 25.5%), and those with hospitalization time <13 days were assigned to the normal group (76 patients, 74.5%). See Figure 3.
 |
Figure 3 Histogram of LOS characteristics of spinal tuberculosis patients undergoing surgery. |
Single Factor Analysis of Prolong LOS
There were no statistically significant differences in patients ‘age, gender, diabetes, smoking, alcohol consumption, anticoagulant history, preoperative anti-tuberculosis treatment time, and whether or not there were tuberculosis in other sites (P>0.05, see Table 1); there were no statistical differences in surgical approach, hospital stay, postoperative drainage volume and surgical site between the two groups (P>0.05, see Table 1); there were no statistical differences in preoperative WBC, D-Dimer, ALB, HB, spinal stenosis, vertebral body destruction, endplate sclerosis and osteophytes between the two groups (P>0.05, see Table 2).
 |
Table 1 Comparison of General Patient Profiles (Single Factor Analysis) |
 |
Table 2 Comparison of Preoperative Laboratory and Imaging Findings (Single Factor Analysis) |
BMI in both groups (Z=−2.297, P =0.022), pain (X2=13.581, P<0.001), emaciated (X2=5.974, P=0.015), intraoperative blood loss (X2=5.162, P=0.023), number of fused vertebrae (X2=11.227, P<0.001), CRP (Z=−5.445, P<0.001) and ESR (Z=−4.85, P <0.001) were statistically significant, see Tables 1 and 2.
Bivariate Logestic Regression Analysis of Prolong LOS
BMI, emaciated, pain, ESR, CRP, number of fused vertebral bodies and intraoperative blood loss were included in the binary logistic regression analysis. The results showed that weight loss (OR= 6.598, P =0.031), severe pain (OR= 10.776, P =0.002), elevated ESR (OR= 1.091, P =0.014) and elevated CRP (OR= 1.076, P =0.005) were risk factors leading to prolonged LOS in patients with spinal tuberculosis after surgery. See Table 3.
 |
Table 3 Binary Logistic Regression Analysis of the Prolonged Hospital Stay After Spinal Tuberculosis |
Predictive Power of Independent Risk Factors
C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) are key predictors for prolonged postoperative hospital stays in spinal tuberculosis patients. CRP, with an AUC of 0.859, demonstrates high sensitivity (92.3%) and effectively screens high-risk patients when the threshold is>18.6mg/L. However, its low specificity (68.4%) may lead to false positives. ESR, showing better balance (sensitivity 73.1% + specificity 86.8%), achieves optimal accuracy (>44 mm/h) at a threshold of 44 mm/h. Pain (AUC 0.696) shows moderate predictive value as a symptom indicator, while weight loss (AUC=0.619) frequently misses cases due to insufficient sensitivity (42.3%). Clinical practice should prioritize dynamic monitoring of inflammatory markers (see Table 4).
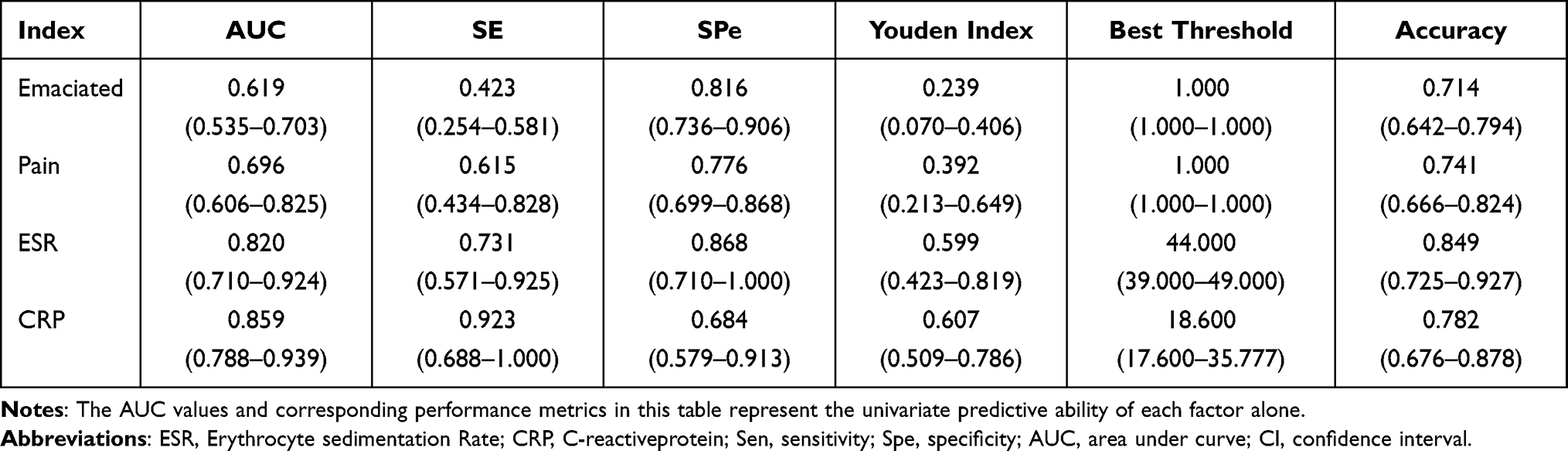 |
Table 4 Efficacy of Independent Risk Factors to Predict Prolonged Hospital Stay After Spinal Tuberculosis Surgery |
Construction and Evaluation of Line Chart Model
The selected independent risk factors were incorporated into a model to construct a risk prediction model for prolonged hospitalization in spinal tuberculosis patients after lesion debridement, fusion, and internal fixation surgery, as shown in Figure 4A. The figure displays individual scores (top to bottom) as follows: ESR, CRP, emaciated status, and pain. Each indicator corresponds to a specific scale. By summing the scores of relevant indicators, we can assess the approximate probability of prolonged hospitalization.
 |
Figure 4 Intraoperative bleeding and ‘number of fused vertebrae. (A) Visualized prediction model for prolonged postoperative LOS in spinal tuberculosis (dot plot); (B) Calibration curve of the prediction mo (C) ROC curve of the prediction model for prolonged hospitalization after lesion debridement and internal fixation in spinal tuberculosis patients; (D) Forest plot. |
The calibration curve (Figure 4B) shows that the X-axis and Y-axis represent the predicted probability of postoperative hospitalization duration extension and the actual probability of hospitalization duration extension, respectively. A curve closer to the diagonal indicates better alignment between the actual and ideal curves. As shown in the figure, the modeling group demonstrates superior fitting performance. The model’s performance was evaluated through internal validation (bootstrap) using the ROC curve and calibration curve. Decision-curve analysis was conducted to evaluate the clinical net benefit of the model. The AUC of the modeling group’s ROC curve reached 0.928 (95% CI: 0.878–0.977), indicating strong predictive efficacy, as illustrated in Figure 4C. Forest plots are used to show the odds ratio (OR) and its confidence interval of each variable in the Logistic regression model (Figure 4D).
Discussion
The combination of anti-tuberculosis drugs and surgery is currently the standard treatment regimen for spinal tuberculosis. The drug treatment cycle is long, and poor patient compliance often compromises therapeutic efficacy. While surgical intervention yields significant therapeutic effects, it is associated with considerable trauma, prolonged hospitalization and recovery times, and a higher risk of adverse events.15 Postoperative length of stay (LOS) is a key metric for evaluating cost-effectiveness, quantifying surgical success, and serves as an important target for clinical quality improvement.16 Prolonged LOS increases the risk of in-hospital infections and escalates the cost burden for both patients and healthcare institutions. Effective preoperative intervention is therefore essential to mitigate the risk of extended hospitalization.17 Accordingly, this study aimed to analyze potential risk factors for prolonged LOS following debridement and bone graft fusion for spinal tuberculosis, with the goal of identifying and ultimately preventing factors that contribute to extended hospital stays.
This study analyzed the preoperative clinical characteristics of 102 patients with spinal tuberculosis who underwent focal debridement, bone graft fusion, and internal fixation, to explore risk factors for prolonged LOS. The average LOS for all patients was 10.63 ± 3.01 days, which is consistent with currently reported LOS following spinal tuberculosis surgery.6 Using the 75th percentile (13 days) as the cutoff, 26 patients were classified into the prolonged LOS group. Several potential risk factors for extended hospitalization were screened, including general condition, surgery-related indicators, and imaging/laboratory parameters. Univariate analysis revealed statistically significant differences between the two groups in BMI, weight loss, pain severity, number of fused vertebrae, intraoperative blood loss, ESR, and CRP (P < 0.05). Subsequent binary logistic regression analysis identified weight loss, severe pain, elevated ESR, and elevated CRP as independent risk factors for prolonged LOS after spinal tuberculosis surgery. To enhance the predictive model’s sensitivity, these factors were incorporated. The results showed that severe pain (OR = 10.776, P = 0.002) and elevated ESR (OR = 1.091, P = 0.014) were significant predictors. The AUC values for pain, ESR, and CRP in ROC analysis were 0.696, 0.820, and 0.859, respectively. The combined prediction model achieved an AUC of 0.934, indicating good predictive value.
Independent Risk Factors and LOS
Emaciation: Spinal tuberculosis is a chronic infectious disease. The persistence and replication of Mycobacterium tuberculosis consume host nutrients, and the immune response mounted to combat the infection further increases energy expenditure, often leading to chronic weight loss. Allard et al14 conducted a multicenter prospective study of 409 patients, assessing nutritional status via Subjective Global Assessment (SGA) and weight measurements at admission and discharge. Their results indicated that diminished nutritional status or weight loss ≥5% was associated with a longer hospital stay (≥7 days), which aligns with our findings.
Severe Pain: Pain is often the earliest symptom of spinal tuberculosis but may not initially alert patients. As the disease progresses and vertebral destruction worsens, pain intensity typically increases, severely impacting patients’ daily lives.18 We recorded preoperative VAS pain scores, categorizing scores ≤6 as mild/moderate and >6 as severe. Patients with severe pain had significantly longer LOS. This may be attributed to local bone destruction from expanding tuberculous lesions, which can directly irritate, compress, or damage abdominal visceral sensory spinal nerves or their central connections, causing abdominal pain. Clinical manifestations are predominantly abdominal pain, with approximately one-quarter of cases accompanied by low back pain. About 75% of patients exhibit paravertebral tenderness and increased erector spinae muscle tension, while abdominal signs are often minimal.18,19
ESR and CRP: As an infectious disease, spinal tuberculosis can trigger a systemic increase in inflammatory cells. Previous studies have shown that the erythrocyte sedimentation rate (ESR) reflects the severity of systemic inflammatory response and can be used to assess disease severity and predict prognosis in spinal tuberculosis.20 Masotti et al,21 in a retrospective analysis of 115 elderly patients with community-acquired pneumonia, confirmed that elevated ESR is an independent risk factor for prolonged hospitalization. C-reactive protein (CRP) is another crucial inflammatory marker. Research indicates that CRP is involved in various physiological and pathological processes in spinal tuberculosis patients.22 Prior literature has also demonstrated that elevated CRP is a risk factor for prolonged LOS after elective orthopedic surgery and for increased infection rates following total hip arthroplasty.23 Our study corroborates that both elevated CRP and ESR are independent risk factors for prolonged LOS after spinal tuberculosis surgery.
Furthermore, comorbidities and poor nutritional status are recognized not only as risk factors for prolonged hospitalization but also for suboptimal treatment response and the development of drug resistance in tuberculosis. Low BMI and malnutrition can impair host immunity, alter drug pharmacokinetics, and are associated with an increased risk of acquiring drug-resistant TB, thereby complicating long-term management outcomes.24,25 Although our study focused on short-term surgical outcomes, future research should investigate the interplay between preoperative nutritional status, inflammatory markers, and the long-term risk of treatment failure or recurrence in spinal TB.
Limitations of this study: (1) The sample size was relatively small, including only 102 patients hospitalized for spinal TB, which may limit the generalizability of the findings. (2) The single-center retrospective design may introduce bias. (3) The established prediction model lacks external validation; we plan to collect and analyze multi-center data for future external validation. (4) Our study was limited to the short-term outcome of postoperative LOS. We acknowledge that valuable long-term outcomes, such as disease recurrence rates, radiographic evidence of bony fusion, and functional scores, were not analyzed. This was primarily due to challenges in conducting long-term follow-up for this specific patient population in our region, including patient mobility and difficulties in retaining participants from remote areas over extended periods. Future prospective studies with dedicated long-term follow-up protocols are essential to correlate the identified risk factors with these critical long-term endpoints.(5) Our analysis focused on a set of routine preoperative investigations. We acknowledge that other crucial biomarkers known to influence TB treatment response and surgical recovery, such as serum albumin, calcium, and vitamin D levels, were not systematically evaluated in this retrospective cohort. Future prospective studies should incorporate a comprehensive nutritional and metabolic panel to refine the predictive model.
Conclusions
In conclusion, the main factors affecting prolonged LOS after spinal tuberculosis debridement, bone grafting, and internal fixation include recent significant weight loss, severe pain, and elevated ESR and CRP levels. Preoperative CRP and ESR reflect the degree of systemic inflammation.26,27 Early diagnosis and appropriate antibiotic use to control infection are crucial. Non-steroidal anti-inflammatory drugs should be administered if necessary to reduce inflammation. Concurrently, strict aseptic technique during surgery is vital to lower the incidence of postoperative infection and shorten hospital stay.28 Although intraoperative blood loss and the number of fused vertebrae were not independent risk factors for prolonged LOS in our model, minimizing both can reduce surgical trauma, potentially decrease hospitalization time, and facilitate patient recovery. Proactive management of these risk factors—through rational surgical planning, optimization of surgical techniques, and efficient resource utilization—can support informed clinical decision-making and ultimately improve patient outcomes.
Abbreviations
LOS, length of stay; ROC, receiver operating characteristic; AUC, area under curve; CI, confidence interval; BMI, Body mass index; ESR, Erythrocyte sedimentation Rate; CRP, C-reactive protein; HB, hemoglobin; ALB, albumin; WBC, white blood cell; CT, Computed Tomography; MRI, Magnetic Resonance Imaging; Sen, sensitivity; Spe, specificity; OR, Odds Ratio.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
We confirm that all experiments were performed in accordance with the Declaration of Helsinki. The study was approved by the Ethical Committee of the Xinjiang Medical University Affiliated Sixth Hospital. Each patient provided written informed consent before participating in the study.
Acknowledgments
The authors sincerely thank the entire staff of the Department of Spinal Surgery, the Sixth Affiliated Hospital of Xinjiang Medical University, for their assistance throughout the study.
Author Contributions
Li Liand Alimujiang Yusufu contributed equally to this work, as co-first author.
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. Bagcchi S. WHO’s global tuberculosis report 2022. Lancet Microbe. 2023;4(1):e20. doi:10.1016/S2666-5247(22)00359-7
2. Liu XT, Su H, Xin Z, et al. Risk factors of postoperative complications and predictive value of nutritional index for preoperative prognosis in patients with spinal tuberculosis. J Pract Med. 2024;40(7):972–11.
3. Zhou YF, Wang AS, Zhao X, et al. Risk factors analysis and predictive model construction of prolonged hospital stay after focal debridement and fusion of spinal tuberculosis. Chin J Spinal Cord. 2024;34(1):53–61.
4. Qin SB. The concept of accelerated rehabilitation surgery and standardization of surgical solutions for spinal tuberculosis. Chin J Tuberculosis Prevention. 2022;44(6):529–530.
5. Khanna K, Sabharwal S. Spinal tuberculosis: a comprehensive review for the modern spine surgeon. Spine J. 2019;19(11):1858–1870. doi:10.1016/j.spinee.2019.05.002
6. Li QD, Baorong H, Liu TJ, et al. Risk factors and predictive models of prolonged hospital stay after focal debridement, bone graft fusion and internal fixation for spinal tuberculosis. Chin J Spinal Cord. 2024;34(1):62–69.
7. Jain AK, Rajasekaran S, Jaggi KR, et al. Tuberculosis of the spine. J Bone Joint Surg Am. 2020;102(7):617–628. doi:10.2106/JBJS.19.00001
8. Chen WJ, Zhu WT. Study on efficacy and safety of simple posterior approach surgery for thoracolumbar spinal tuberculosis. J North Sichuan Med College. 2017;32(5):734–737.
9. Zhang LJ, Tao X, Xia LL, et al. Value of clinical pathway table for accelerated rehabilitation cluster nursing care in patients with spinal tuberculosis during perioperative period. Chin J Tuberculosis Prevention. 2020;42(9):981–986.
10. Yasheng P, Maerdan M, Weibin S, et al. Risk factors for prolonged hospital stay after brucella spondylitis surgery. Chin J Orthop. 2023;43(21):1433–1440.
11. Nijland LMG, De Castro SMM, Van Veen RN. Risk factors associated with prolonged hospital stay and readmission in patients after primary bariatric surgery. Obes Surg. 2020;30(6):2395–2402. doi:10.1007/s11695-020-04507-2
12. Abudurexiti T, Haibier A, Yusufu A, et al. Retrospective analysis of the efficacy and safety of endoscopic spinal tuberculosis focus removal versus posterior pedicle lesion removal, bone grafting, and internal fixation combined with drug chemotherapy for thoracolumbar tuberculosis. Infect Drug Resist. 2024;17:733–748. doi:10.2147/IDR.S449684
13. Orthopaedics Professional Committee of Tuberculosis Society of Chinese Medical Association. Surgical treatment guidelines for spinal tuberculosis in China (2022 Edition). China Orthopaedic J. 2022;30(17):1537–1548.
14. Allard JP, Keller H, Jeejeebhoy KN, et al. Decline in nutritional status is associated with prolonged length of stay in hospitalized patients admitted for 7 days or more: a prospective cohort study. Clin Nutr. 2016;35(1):144–152. doi:10.1016/j.clnu.2015.01.009
15. Hairong D, Na D, Zhenping W, et al. Comparison of percutaneous pedicle screw fixation and traditional open surgery for spinal tuberculosis. Chin Med J. 2023;58(04):397–400.
16. Strada A, Bolognesi N, Manzoli L, et al. Diagnostic anticipation to reduce emergency department length of stay: a retrospective cohort study in Ferrara University hospital, Italy. BMC Health Serv Res. 2020;20(1):624. doi:10.1186/s12913-020-05472-3
17. Fan ZJ, Liu HZ, Chen Q, et al. Risk factors for prolonged hospital stay in patients with thoracolumbar burst fracture. Chin J Bone Joint. 2024;13(07):572–576.
18. Zhang HJ, Lu ZH, Lin W, et al. Clinical analysis of intractable pain in spinal tuberculosis. Shanxi Med J. 2014;(24):2900–2902.
19. Li W, Chen JH, Ruan WH. Clinical analysis of three-combination therapy for metastatic spinal pain. Jilin Med J. 2011;32(15):2998.
20. Gu W, Lai WP, Sun CH. Clinical value of erythrocyte sedimentation rate combined with hs-CRP level in predicting prognosis of spinal tuberculosis patients. Chin Med Innov. 2024;21(6):121–125.
21. Masotti L, Ceccarelli E, Cappelli R, et al. Length of hospitalization in elderly patients with community-acquired pneumonia. Aging. 2000;12(1):35–41. doi:10.1007/BF03339826
22. Cho JH, Lee DC, Lee HJ. Association of duration of smoking cessation or cumulative smoking amount with serum hs-CRP level in Korean adults: a nationwide population-based cross-sectional study. Toxics. 2022;10(9):533. doi:10.3390/toxics10090533
23. Yoshida B, Nguyen A, Formanek B, et al. Hypoalbuminemia and elevated CRP are risk factors for deep infections and urinary tract infections after lumbar spine surgery in a large retrospective patient population. Global Spine J. 2023;13(1):33–44. doi:10.1177/2192568221990647
24. Vyawahare C, Mukhida S, Khan S, Gandham NR, Kannuri S, Bhaumik S. Assessment of risk factors associated with drug-resistant tuberculosis in pulmonary tuberculosis patients. Indian J Tuberc. 2024;71 Suppl 1:S44–S51. doi:10.1016/j.ijtb.2023.07.007
25. Khan S, Vyawahare C, Mirza S, Gandham NR, Mukhida S. Lest we forget spinal tuberculosis (Potts’s spine): case series with unusual presentation. Indian J Tuberc. 2023;70(2):258–262. doi:10.1016/j.ijtb.2022.08.003
26. Li G, Weng J, Xu C, et al. Factors associated with the length of stay in total knee arthroplasty patients with the enhanced recovery after surgery model. J Orthop Surg Res. 2019;14(1):343. doi:10.1186/s13018-019-1389-1
27. Stambough JB, Curtin BM, Odum SM, et al. Does Change in ESR and CRP Guide the Timing of Two-stage Arthroplasty Reimplantation? Clin Orthop Relat Res. 2019;477(2):364–371. doi:10.1097/01.blo.0000533618.31937.45
28. Alsaeed OM, Bukhari AA, Alshehri AA, et al. The use of antibiotics for the prevention of surgical site infections in two government hospitals in Taif, Saudi Arabia: a retrospective study. Cureus. 2022;14(7):e26731. doi:10.7759/cureus.26731
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Lung Ultrasound-Based Nomogram for the Prediction of Refractory Mycoplasma pneumoniae Pneumonia in Hospitalized Children
Liu G, Wang G, Yang Z, Liu G, Ma H, Lv Y, Ma F, Zhu W
Infection and Drug Resistance 2022, 15:6343-6355
Published Date: 31 October 2022
Establishment and Validation of a Predictive Nomogram for Hallux Valgus with Pain Under the Second Metatarsal
Bai Z, Cao X, Yang Y, Sun X, Dong Y, Wen J, Sun W
Journal of Pain Research 2022, 15:3523-3536
Published Date: 7 November 2022
Development and Validation of a Predictive Model for Chronic Postsurgical Pain After Arthroscopic Rotator Cuff Repair: A Prospective Cohort Study
Dai X, Yuan M, Dang M, Liu D, Fei W
Journal of Pain Research 2023, 16:3273-3288
Published Date: 27 September 2023
Unraveling the Predictors of Enlarged Perivascular Spaces: A Comprehensive Logistic Regression Approach in Cerebral Small Vessel Disease
Li N, Shao JM, Jiang Y, Wang CH, Li SB, Wang DC, Di WY
International Journal of General Medicine 2024, 17:2513-2525
Published Date: 1 June 2024
Establishment and Validation of an Early Predictive Model for Severe Acute Pancreatitis
Yang K, Song Y, Su Y, Li C, Ding N
Journal of Inflammation Research 2024, 17:3551-3561
Published Date: 4 June 2024