Back to Journals » International Journal of General Medicine » Volume 19
Development and Validation of a Prediction Model for Intensive Care Unit-Acquired Weakness in Adult Patients with Sepsis: A Prospective, Observational, Single-Center Study
Authors Wang B, Liu Y, He G, Sun S, Han J, Zhang M, He L, Meng S
Received 16 October 2025
Accepted for publication 31 March 2026
Published 14 April 2026 Volume 2026:19 569937
DOI https://doi.org/10.2147/IJGM.S569937
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Binghan Wang,1,* Yuting Liu,1,* Guilan He,2 Sha Sun,1 Jianqiang Han,1 Min Zhang,1 Linna He,1 Siya Meng1
1Department of Critical Care Medicine, Shenzhen Nanshan People’s Hospital, Shenzhen, 518000, People’s Republic of China; 2Party and Government Office, Shenzhen Nanshan People’s Hospital, Shenzhen, 518000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Siya Meng, Department of Critical Care Medicine, Shenzhen Nanshan People’s Hospital, Shenzhen, 518000, People’s Republic of China, Email [email protected] Linna He, Department of Critical Care Medicine, Shenzhen Nanshan People’s Hospital, Shenzhen, 518000, People’s Republic of China, Email [email protected]
Purpose: This study aimed to develop and validate a clinical prediction model for intensive care unit-acquired weakness (ICU-AW) in sepsis patients, in order aid the early identification of high-risk patients and enable targeted intervention measures.
Patients and Methods: This prospective observational study was a single-center study conducted in a tertiary hospital in Shenzhen, China. Eligible inpatients diagnosed with sepsis between January 2023 and June 2024 were enrolled. The least absolute shrinkage and selection operator (LASSO) regression model was used to optimize the feature selection for the risk prediction model for ICU-AW in sepsis patients. Multivariable logistic regression analysis was applied to build a predicting model that incorporated the features selected in the LASSO regression model. Receiver operating characteristic (ROC) and calibration curves, and decision curve analysis (DCA) were applied to assess the model.
Results: A total of 344 patients were included in the present study. Among these patients, 257 and 87 patients were assigned to the modeling and validation groups, respectively. Six independent predictors were identified: age, multiple organ dysfunction syndrome (MODS), use of neuromuscular blocking agents (NMBAs), duration of mechanical ventilation, duration of sedation, and Acute Physiology and Chronic Health Evaluation II (APACHE II) score. The nomogram revealed good performance, with an area under the ROC curve (AUC) of 0.905 (95% CI: 0.871– 0.940) for the modeling group and 0.861 (95% CI: 0.784– 0.939) for the validation group. The calibration curves indicated a good agreement between the predicted and observed outcomes. The DCA demonstrated a broad benefit threshold and good clinical effectiveness.
Conclusion: The risk prediction model constructed in the present study demonstrated good predictive performance, providing a valuable reference for clinical practitioners to identify the risk of ICU-AW in patients with sepsis and implement prompt intervention.
Plain Language Summary: A multivariable model was established to predict the ICU-AW in septic patients, with easily obtainable predictive factors accessible from hospital information systems.The nomogram revealed good discriminative ability, calibration, and clinical utility, serving as a valuable tool for early identification and intervention.The limitations included the single-center design (restricting generalizability), small external validation cohort, and Medical Research Council (MRC) score-based ICU-AW diagnosis (only for conscious/cooperative patients), which potentially induced selection bias, and restricted the applicability to Chinese populations.
Keywords: sepsis, intensive care unit, acquired weakness, risk factors, nomogram, prediction model
Introduction
Sepsis is a life-threatening organ dysfunction caused by the dysregulated response of the body to infection, and is one of the most common causes of high morbidity and mortality in patients admitted to the intensive care unit (ICU).1,2 In recent years, with the standardization of sepsis diagnosis and treatment, and improvements in organ support technologies, the early mortality rate of this condition has significantly decreased.3 However, more sepsis survivors experience intensive care unit-acquired weakness (ICU-AW), which has become a common and severe complication among patients with sepsis. The pathogenesis of ICU-AW may involve excessive inflammatory responses following infection and trauma, leading to damage to neuromuscular tissues and interference with neuromuscular junction conduction. Compared with other patients, patients with sepsis have a higher incidence of ICU-AW.4 Muscle atrophy occurs in 50–100% of patients with sepsis in the ICU, and approximately 25–75% of sepsis survivors develop ICU-AW,5 resulting in delayed extubation, prolonged ICU stays, increased medical costs, and severe impacts on the quality of life of patients and long-term prognosis.6 The main characteristics of ICU-AW include significant reductions in muscle volume and quality, but its onset is often insidious, and usually identified only when muscle strength has noticeably declined.7
At present, the pathogenesis, risk factors, and diagnostic criteria for ICU-AW in patients with sepsis are not yet fully clear, which may lead to inadequate awareness or delayed diagnosis among healthcare providers.8 Therefore, it is crucial to construct a risk prediction model for ICU-AW in patients with sepsis. Although several researchers have explored this area,4,9 limitations such as small sample size (264 and 60 patients in the study conducted by Liu et al and Li et al, respectively,4,9 potential increase in sampling bias and reduction in result generalizability) and retrospective study design have hindered the promotion and application of constructed risk prediction models for ICU-AW in patients with sepsis. Furthermore, initial designs did not consider data on some participants in a related study, including comorbidities, the use of neuromuscular blocker agents (NMBAs), and etiology at admission, and the model was not externally validated.10 Thus, the present prospective observational study developed and validated a clinical prediction model for ICU-AW in adult patients with sepsis, with the aim of providing healthcare providers with a basis for the early and rapid assessment and identification of high-risk patients for ICU-AW, and enabling targeted intervention measures.
Material and Methods
Study Design and Participants
The present prospective observational study was conducted by convenient sampling, enrolling sepsis patients admitted to the ICU of a grade A tertiary hospital in Shenzhen between January 2023 and June 2024. The ICU has 32 beds, and is staffed by 31 physicians and 85 specialized nurses. The three primary patient populations managed in the ICU of the investigators included trauma, severe pneumonia, and sepsis. In 2025, a total of 1026 critically ill patients were admitted to the ICU, which included 471 patients diagnosed with sepsis. Established in collaboration with the University of Southern California, USA in 2015, the hospital serves as a demonstration institution for the “Urban Regional Trauma Center” program.
Based on the chronological order of admission, patients were divided into two groups: data obtained from 261 patients with sepsis (January-December 2023) were assigned to the modeling group for nomogram construction and internal validation, while 87 patients (January-June 2024) were assigned to the validation group for external model validation. The inclusion criteria were as follows: (1) age ≥18 years old; (2) patients diagnosed with sepsis within 48 hours after admission, according to the Sepsis 3.0 diagnostic criteria;11 (3) patients or their families who provided informed consent, and voluntarily participated in the present study. The exclusion criteria were, as follows: (1) length of stay in the ICU was <72 hours; (2) patients who had cerebrovascular disease, central nervous system disorders, Guillain-Barré syndrome, or spinal cord injury; (3) patients with quadrilateral joint surgery, fractures or lower limb thrombosis, or patients who required immobilization; (4) patients who could not undergo the muscle strength assessment for various reasons.
Sample size was determined using the Tests for the Odds Ratio in Logistic Regression with One Binary X (Wald Test) module in the PASS 2021 software (NCSS, LLC, Kaysville, UT, USA). The calculation was based on a two-sided Wald test with a significance level (α) of 0.05 and a statistical power (1−β) of 0.90. Based on our clinical experience and the literature review,12,13 the incidence in the non-exposed group (without constraint implementation) was P0 = 0.339, while the incidence in the exposed group (with implementing constraints) was P1 = 0.661, reflecting an expected odds ratio of 3.802 and an exposure rate of 44.7%. Under these parameters, the minimum required sample size was calculated as 107 cases. Considering a potential 20% dropout rate, the enrollment was targeted to collect 134 cases. Finally, a total of 348 cases were included for the present study, with the modeling group and validation group allocated at a 3:1 ratio. Therefore, the modeling group (261 cases) was used for internal validation, while the validation group (87 cases) was used for external validation. The present study was approved by the ethics committee of Shenzhen Nanshan People’s Hospital, Shenzhen, China (Approval number: #KY-2022-012-01).
Data Collection and Definitions
A clinical survey form was developed based on the literature and expert consultations. The survey included the following: (1) General information: age, sex, body mass index (BMI), and arm circumference (from the midpoint of the line connecting the acromion to the olecranon of the ulna) at admission to the ICU; (2) Cause of disease: lung infection, urinary tract infection, abdominal cavity infection, bloodstream infection, multiple organ dysfunction syndrome (MODS), diabetes, hypertension, septic shock, and application of restraints; (3) Treatment factors: duration of mechanical ventilation (total number of hours from the initiation of mechanical ventilation via endotracheal intubation or tracheostomy to its discontinuation), establishment mode of mechanical ventilation (the type of invasive airway method used for mechanical ventilation throughout the ICU hospitalization), the use of sedatives and analgesics, duration of sedation (the total number of days from the start to the end of continuous sedative infusion during mechanical ventilation, converted from cumulative hours of sedative administration when intermittent dosing was used), the use of NMBA, the use of glucocorticoids, the use of vasoactive drugs, and renal replacement therapy; (4) Laboratory test indicators: blood lactic acid, fasting blood glucose, blood calcium, C-reactive protein, procalcitonin, and serum albumin values. All indicators were the test results for the fasting venous blood samples collected in the morning when the patient was admitted to the ICU. (5) The relevant rating scales included the Acute Physiology and Chronic Health Evaluations Scoring System II (APACHE II), the Sequential Organ Failure Assessment (SOFA), and the Nutritional Risk Screening 2002 (NRS 2002) scores, which were assessed within 24 hours after entering the ICU.
At present, the most widely used assessment tool for ICU-AW is the Medical Research Council (MRC) score.7 The evaluation criteria for ICU-AW were as follows: new, flaccid, symmetric muscle weakness during ICU admission, normal cranial nerve function, and MRC score <48 points. The MRC primarily evaluates the level of motion of 12 muscle groups (bilateral shoulder abduction, elbow flexion, wrist extension, hip flexion, knee extension, and ankle dorsiflexion). Each muscle group is assigned 0–5 points. The total score of the 12 indicator groups is 0–60 points, in which 0 point represents quadriplegia and 60 points represent normal muscle strength. If the total score was <48 points, ICU-AW was diagnosed.
Assessment of ICU-AW
Before the study began, the researchers conducted centralized and professional training for all study participants. In addition, rehabilitation therapists conducted bedside training on the MRC score for the ICU nursing staff. Finally, on-site evaluations were performed to determine the evaluation ability of the clinical data collection personnel, ensuring that any issues encountered during the investigation can be promptly resolved. After the study began, the researchers strictly followed the inclusion and exclusion criteria to determine whether the patient could be enrolled to the study, and provided an informed consent. During sedation treatment, the use of sedative drugs was reduced or stopped to maintain a Richmond Agitation Sedation Scale (RASS) score between −1 and 1. Trained ICU nurses assessed the MRC score daily. If the MRC score was <48 on two consecutive assessments with a 24-hour interval, the patient was classified as ICU-AW. In contrast, if the MRC score was ≥48 or above in both assessments, the patient was classified as non-ICU-AW, and patients who could not be evaluated were not included. If the patient developed ICU-AW, the evaluations were halted, while if the patient did not develop ICU-AW, the evaluations were continued until the patient completed the ICU treatment. In addition, the researchers verified the completeness, precision, and authenticity of the collected data weekly by reviewing the electronic medical records of the patients and clinical indicator collection forms.
Statistical Analysis
All analyses were performed using SPSS 23.0 (IBM, Armonk, NY, USA) and R 4.0.2 (The R Project for Statistical Computing, www.r-project.org). Normally distributed continuous variables were presented in mean ± standard deviation, and comparisons between groups were performed using two independent samples t-test. Non-normally distributed continuous variables were expressed in median and interquartile range (IQR). Group comparisons were performed using the Mann–Whitney U-test. Categorical variables were presented in n (%), and analyzed using the Chi-square test.
Variables included in the multivariate logistic regression analysis were selected using a two-step approach. First, all candidate variables were analyzed using the univariate analysis (Chi-square/Fisher’s exact test for categorical variables, t-test/Mann–Whitney U-test for continuous variables). Then, variables with a p-value of <0.05 in univariate analysis were retained as potential predictors. Second, variables retained from univariate screening were further refined using the least absolute shrinkage and selection operator (LASSO) regression analysis, which penalizes regression coefficients to automatically select the most predictive variables, and reduce model overfitting. Merely variables selected through the combined univariate screening and LASSO regression refinement process were entered into the final multivariate logistic regression model to identify the independent risk factors for ICU-AW, and construct the regression equation.
The visual nomogram was constructed using the R software based on the final regression equation, in order to predict the risk of ICU-AW in sepsis patients. The bootstrap resampling method (1000 automatic samples) was used for the internal and external validation of the model. The area under the receiver operating characteristic curve (AUC) was used to evaluate the model’s discriminatory ability, while calibration curves and the Brier score were used to assess calibration accuracy. Clinical utility was evaluated using decision curve analysis (DCA). A two-sided p-value of <0.05 was considered statistically significant.
Results
Demographic Characteristics
Among the 348 eligible sepsis patients during the study period, four patients were excluded, because these patients died before reaching the endpoint event (Figure 1). Finally, a total of 344 patients were analyzed. The modeling group included 257 patients, with a median age of 63.36 (IQR: 53.00, 75.00) years old. Among these patients, 178 were male, and 79 were female. Furthermore, among these patients, 130 patients developed ICU-AW, resulting in an incidence rate of 50.58%. The validation group included 87 patients, with a median age of 62.93 (IQR 53.00, 74.00) years old. Among these patients, 56 were male, and 31 were female. Furthermore, among these patients, 40 patients developed ICU-AW, resulting in an incidence rate of 45.98%. There were no statistically significant differences in clinical characteristics between the modeling and validation groups (all p>0.05) (Table 1).
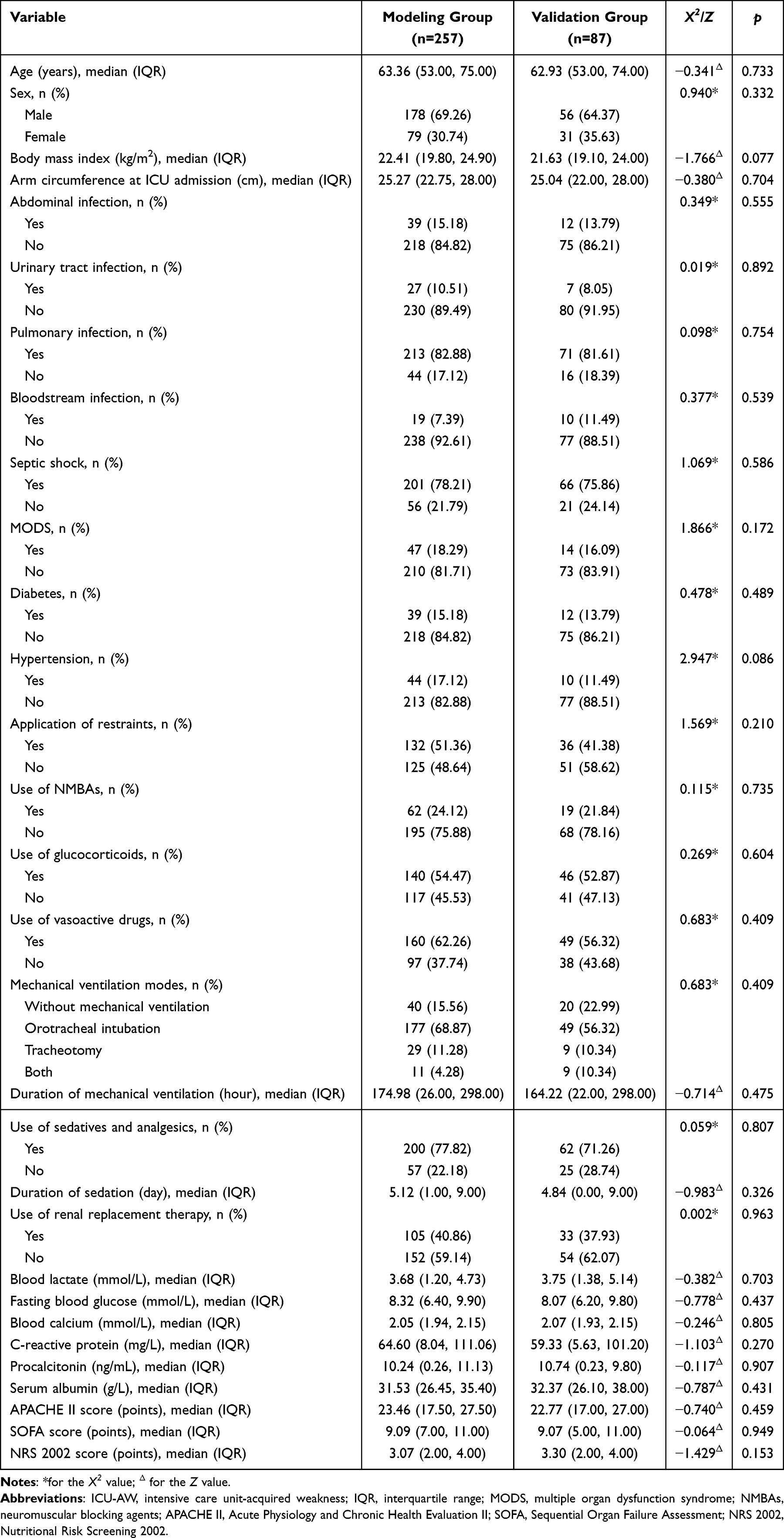 |
Table 1 Comparison of ICU-AW in Sepsis Patients Between the Modeling and Validation Groups |
 |
Figure 1 Patient enrollment flowchart. |
Univariate Analysis
The univariate analysis results of the present study revealed that the two groups were different in terms of patient age, MODS, use of NMBAs, use of glucocorticoids, duration of mechanical ventilation, use of sedative and analgesic drugs, duration of sedation, use of renal replacement therapy, blood lactate levels, APACHE II score, and SOFA score. The difference was statistically significant (p<0.05) (Table 2). Thus, a total of 11 variables were incorporated into the LASSO regression analysis.
 |
Table 2 Comparison of ICU-AW in Patients with Sepsis |
LASSO Regression Analysis
Variables identified in the univariate analysis were incorporated into the LASSO regression. At the optimal λ value of 0.04074497, 10 significant predictors with nonzero coefficients were selected via 10-fold cross-validation. The results did not demonstrate multicollinearity among the following variables: age, MODS, use of NMBAs, use of glucocorticoids, duration of mechanical ventilation, use of sedatives and analgesics, duration of sedation, blood lactate, APACHE II score, or SOFA score (Figures 2 and 3).
 |
Figure 2 Selection process for the tuning parameter λ via cross-validation. |
 |
Figure 3 Variable selection via LASSO regression analysis. |
Multivariate Analysis
The occurrence of ICU-AW was taken as the dependent variable, and 10 variables selected by univariate analysis were entered as independent variables in the binary logistic regression model. The following were entered as continuous variables: age, duration of mechanical ventilation, duration of sedation, blood lactate level, APACHE II score, and SOFA score. The remaining five variables (MODS, use of NMBAs, use of glucocorticoids, and use of sedatives and analgesics) were coded as binary variables (no = 0, yes = 1). The results revealed the following as significant predictors of ICU-AW in sepsis patients: age (OR: 1.044), MODS (OR: 3.349), use of NMBA (OR: 16.293), duration of mechanical ventilation (OR: 1.004), duration of sedation (OR: 1.243), and APACHE II score (OR: 1.101) (Table 3).
 |
Table 3 Risk Factors for ICU-AW in Sepsis Patients Using Multivariate Logistic Regression Analysis |
Construction of the Nomogram
Based on the six independent predictors selected by logistic regression analysis, a nomogram was constructed to predict the risk of ICU-AW in sepsis patients (Figure 4). The final regression equation underlying the nomogram was as follows: Logit(P) = −6.345 + 0.043 × age + 1.209 × MODS + 2.791 × use of NMBAs + 0.004 × duration of mechanical ventilation + 0.218 × duration of sedation + 0.096 × APACHE II score, where P was the predicted probability of ICU-AW occurrence. In order to estimate P, each predictor was assigned a specific number of points on the nomogram scale. The points for all predictors were summed, and the total score was located on the bottom “Total Points” scale to determine the corresponding predicted probability of ICU-AW. Higher total scores indicated a higher predicted risk of ICU-AW.
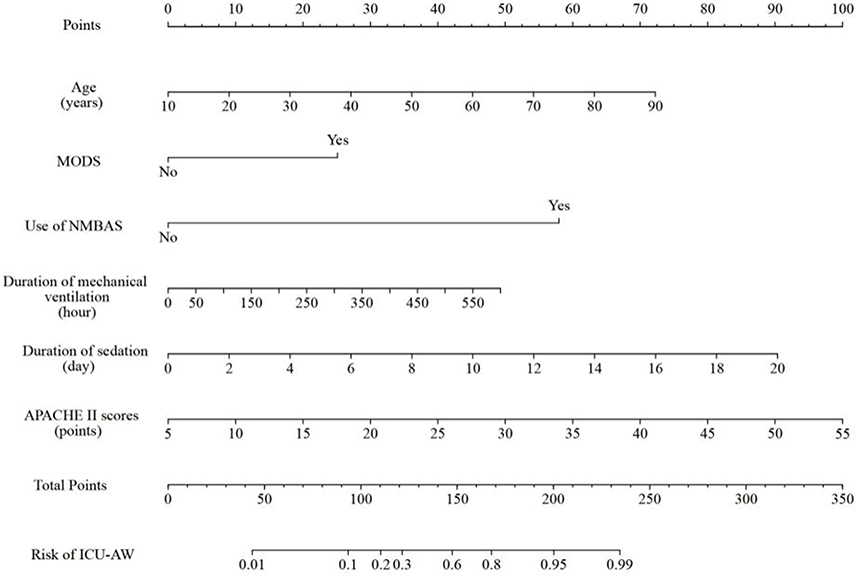 |
Figure 4 Nomogram for the risk of ICU-AW in sepsis patients. |
Validation of the Prediction Model
The predictive performance of the model was evaluated by plotting the ROC curve. The AUC for the modeling group was 0.905 (95% CI: 0.871–0.940), with an optimal cut-off value of 0.630, a sensitivity of 0.738, and a specificity of 0.913 (Figure 5). The calibration curve demonstrated a good agreement between the observed and predicted probabilities, as supported by the Hosmer-Lemeshow test (X2=7.217, p=0.513) and Brier score (0.127) (Figure 6). For the validation group, the AUC was 0.861 (95% CI: 0.784–0.939), with an optimal cut-off value of 0.431, a sensitivity of 0.850, and a specificity of 0.787 (Figure 5). The Hosmer-Lemeshow test (X2=10.469, p=0.234) and Brier score (0.153) indicated satisfactory calibration, and the calibration curve of the nomogram closely approximated the ideal line (Figure 6). The DCA revealed that the net benefit of the model exceeded that of the two reference lines in a reasonable threshold probability range (Figure 7), suggesting the superior clinical utility of the model.
 |
Figure 5 Prediction model for ICU-AW risk in the ROC curves for patients with septic shock in the model group and validation group. |
 |
Figure 6 Prediction model for ICU-AW risk in the calibration curves for sepsis patients in the modeling and validation groups. |
 |
Figure 7 Decision analysis curve for the prediction model. |
Discussion
The present study revealed that the prevalence of ICU-AW in sepsis patients was 50.58%, which is within the 25–75% range reported in previous studies.12,13 Relevant studies have revealed that sepsis is an independent risk factor for ICU-AW, a clinical entity alternatively termed as, sepsis-associated acquired weakness (SAW). This condition is characterized by significant muscle mass reduction, decreased myofiber diameter, and diminished muscle strength, ultimately leading to persistent physical impairment.3,14 Although the precise pathophysiological mechanisms underlying SAW remain incompletely understood, and no definitive therapeutic interventions are presently available, this represents a dynamic and potentially reversible condition. Early recognition and timely intervention can effectively attenuate the progression of ICU-AW.15 Consequently, the identification of risk factors and development of early risk prediction models for ICU-AW in sepsis patients are of paramount clinical importance, since these would allow timely interventions to reduce the incidence of ICU-AW, and improve long-term patient outcomes.
The nomogram model revealed a good prediction effect. The AUC was 0.905 for the modeling group, and 0.861 for the verification group, indicating that the model has good discrimination ability. Furthermore, the Hosmer-Lemeshow test results all revealed p>0.05, indicating that the model has good consistency. Moreover, the DCA results suggested that the net benefit value of the model is higher than the reference line under a certain threshold probability, indicating that the performance of the prediction model in clinical benefit is better.
The six predictors in the nomogram are easy to obtain. The medical staff can calculate the total score of the predictors, and distinguish high-risk and low-risk groups according to the best critical value (0.630), which is characterized by strong feasibility and practicability. For example, a sepsis patient admitted to the ICU had the following details: 45 years old (30 points), combined with MODS (25 points), used NMBA (57 points) in treatment, mechanical ventilation time was 200 hours (15 points), sedation time was eight days (35 points), and the APACHE II score was 18 points (27 points). The total score was 189 points (30+25+57+15+35+27=189 points) by nomogram analysis. This corresponded to a risk of ICU-AW of approximately 0.9, which is a high-risk group that requires the implementation of early intervention.
The present study results suggest that age is an independent risk factor for ICU-AW in sepsis patients (OR: 1.044), which was also reported in another study.16 Muscle mass and muscle contractility can decline with age, resulting in greater weakness than would be expected from muscle atrophy. In severe cases, due to systemic inflammatory responses, protein loss, and reduced anabolic stimulation, muscle loss in older patients can be particularly rapid.17 Therefore, for older patients, greater attention should be given to muscle strength assessment, which can be assessed at every shift, in order to identify abnormal muscle strength in patients in time, and perform rehabilitation training in a timely manner.
Patients with MODS have a 15% higher incidence of ICU-AW, when compared to patients without MODS.18 In the present study, MODS was identified as an independent risk factor for ICU-AW in sepsis patients (OR: 3.349, 95% CI: 1.300–9.029), which is consistent with previous research findings.19 The underlying pathophysiological mechanisms may involve two interconnected pathways. First, sepsis complicated by MODS triggers a systemic inflammatory response characterized by the progressive elevation of pro-inflammatory cytokines. Concurrent prolonged administration of antimicrobial agents adversely affects the microvascular environment and metabolic homeostasis, ultimately leading to impaired energy metabolism and nutrient supply in neuromuscular tissues, resulting in myocyte injury.13 Second, the release of inflammatory mediators increase capillary permeability, causing structural damage to muscle tissues that progressively affects the central nervous system. This cascade induces oxidative stress, and stimulates the further massive release of pro-inflammatory cytokines, thereby exacerbating muscular dysfunction, and culminating in the development of ICU-AW.18,20 De Jonghe et al19 suggested that a reduction in the incidence or duration of MODS by preventing severe sepsis and septic shock is expected to result in a reduction in the incidence of ICU-AW. In the context of infectious diseases, the implementation of interventional therapy at the earliest possible juncture is imperative for the suppression of the inflammatory storm. In cases where sepsis is accompanied by MODS, the judicious administration of antimicrobial agents is paramount to curtail the infection, and mitigate the inflammatory response. This approach is instrumental in improving the prognoses of ICU-AW patients.
NMBAs are commonly used in the ICU to reduce voluntary respiratory effort in mechanically ventilated patients, thereby improving human-machine synchronization, and reducing ventilator-induced injuries. However, the use of NMBAs also reduces the excitability of the diaphragm, which can lead to impaired nerve conduction in patients, and prolonged duration of mechanical ventilation. Meanwhile, sepsis patients are in a state of systemic inflammation, in which NMBAs may further affect immune and inflammatory responses, thereby affecting muscle function and recovery.21 A related study21,22 revealed that the use of NMBAs is strongly associated with the appearance of ICU-AW. The present study revealed that the use of NMBAs was an independent risk factor for ICU-AW in sepsis patients (OR: 16.293). Therefore, NMBAs should be used with caution in the treatment of sepsis patients. That is, the use of NMBAs should be limited to 48 hours, in order to minimize harm, while reducing the risk of ICU-AW. However, since these results were primarily derived from observational studies that exhibited significant heterogeneity, there is presently insufficient evidence to definitively establish a link between the use of NMBA and ICU-AW.
The present study revealed that prolonged mechanical ventilation was strongly associated with ICU-AW in sepsis patients, which is consistent with the findings reported by Takahashi et al15 Sepsis is often associated with acute and chronic organ dysfunction. Most patients with sepsis experience respiratory dysfunction, and require mechanical ventilation. Prolonged mechanical ventilation is an important risk factor for ICU-AW.4 The degree of diaphragmatic injury after 48 hours of mechanical ventilation has been reported to be positively correlated with the level of ventilatory support, leading to diaphragmatic weakness and atrophy.23 The incidence of ICU-AW has been documented to range within 26–65% in patients who have been subjected to mechanical ventilation for a duration of 5–7 days. Furthermore, the prevalence of ICU-AW in patients who require prolonged mechanical ventilation (defined as a duration of ≥10 days) has been reported to reach as high as 67%.23,24 Sepsis affects both the limb muscles and diaphragm, resulting in diaphragm dysfunction and limb muscle weakness effectual overlap.15 Furthermore, patients undergoing prolonged mechanical ventilation are typically exposed to a combination of protective restraints, increased use of muscle relaxants and sedation, sepsis, hypoxemia, and malnutrition, which can collectively contribute to the development of ICU-AW. Therefore, it is imperative to meticulously regulate the duration of mechanical ventilation. Clinically, a multifaceted approach that involves lung-protective ventilation with low tidal volume, the precise and gradual adjustment of support strength, and the promotion of human-machine coordination can be used to curtail the duration of mechanical ventilation, with such measures being tailored to the condition and tolerance level of the patient. Furthermore, the implementation of early rehabilitation measures within 48–72 hours after mechanical ventilation has been shown to reduce the incidence of ICU-AW.
The present study identified sedation duration as an independent risk factor for ICU-AW in sepsis patients (OR: 1.243, 95% CI: 1.140–1.369). The systemic inflammatory reaction in sepsis triggers sympathetic overactivation, and induces a hypermetabolic state. Sedative therapy can mitigate excessive sympathetic stimulation, and reduce metabolic oxygen demand.25 Mechanical ventilation, which is a common respiratory support modality for septic ICU patients, typically requires sedation to minimize ventilator synchrony, and prevent complications, such as unplanned extubation.4 However, prolonged sedation may contribute to neuromuscular dysfunction.25 A relevant animal study revealed that benzodiazepine sedatives (eg midazolam) induced more severe diaphragmatic dysfunction, when compared with non-benzodiazepine alternatives (dexmedetomidine or propofol), thereby increasing the risk of ICU-AW.26 Extensive sedation has been linked to prolonged braking, invasive ventilation, and increased risk of morbidity and mortality.27 Thus, it is important to note the recent emphasis on the role of sedation as a risk factor for ICU-AW.28 Consequently, international guidelines have recommended that sedation should be carefully assessed and reduced to the necessary minimum.29 Therefore, non-benzodiazepine sedatives (eg dexmedetomidine or propofol) should be prioritized for sedation therapy. Furthermore, the patient’s condition should be closely monitored, the sedative effect should be evaluated (eg using the RASS/Sedation-Agitation Scale [SAS]), the dosage should be adjusted in time, and the use of sedative drugs should be minimized. For patients who require continuous sedation, daily sedation interruption (DSI) should be implemented to minimize drug accumulation.
APACHE II scores are widely used to assess the prognosis, and characterize the severity of the disease in ICU patients. Higher APACHE II scores indicate a more severe disease, worse clinical outcomes, and elevated risk of mortality.30 The APACHE II score was identified as an independent risk factor for ICU-AW in sepsis patients. The present findings revealed that the ICU-AW group had significantly higher APACHE II scores, when compared with the non-ICU-AW group (26.24 [21.00, 29.00] vs 20.62 [12.00, 26.00], p<0.001). Each 1 point increase in APACHE II score was associated with a 1.101-fold higher incidence of ICU-AW, indicating that patients with higher scores are more susceptible to develop ICU-AW. Consistent with the findings reported by Guo et al, higher APACHE II scores (indicative of greater systemic pathophysiological derangement) were strongly associated with ICU-AW incidence, which was likely due to the prolonged immobilization and metabolic dysregulation in critically ill patients.31 Therefore, medical personnel should prioritize the APACHE II score upon admission to the ICU as a key prognostic indicator. The timely correction of abnormal physiological parameters may significantly influence patient outcomes, particularly in preventing ICU-AW.
Several previous studies have explored the risk factors and constructed models to predict the ICU-AW in the ICU. Lie et al performed a retrospective study for 264 ICU patients, with 114 patients developing ICU-AW. After the univariate and multivariate binary logistic regression analyses, they developed a scoring scale that included the APACHE II score, mechanical ventilation time, protective constraint, and serum lactic acid level to predict the ICU-AW, with an AUC of 0.913, a sensitivity of 76.3%, and a specificity of 90.7%.4 Li et al reported a cross-sectional study for 60 sepsis patients in the ICU. After the univariate and multivariate binary logistic regression analyses, they concluded that the mean value of the APACHE II score, average SOFA score, and its combination can predict the ICU-AW, with an AUC of 0.787, 0.881 and 0.905, respectively (sensitivity: 75%, 90% and 90%, respectively; specificity: 80%, 80% and 85%, respectively).9 Another recent prospective cohort study conducted by Lei et al developed a nomogram model to predict the ICU-AW based on the analysis of 116 sepsis patients in the ICU. The model included several serum inflammatory biomarkers, such as C-reactive protein and interleukin-6, as well as the muscle thickness (vastus intermedius) and cross-sectional area (rectus femoris) measured by ultrasound, with an AUC of 0.966, a sensitivity of 88%, and a specificity of 95.8%.10 All of these previously reported models were developed in a single set of ICU patients, without validation groups. Thus, these retrospective studies could lead to selection and information bias. Furthermore, ultrasound measurements for muscle thickness and the cross-sectional area are not widely available in most clinical settings. Compared to these previous models, the present nomogram prediction model carries the advantage of being developed in a prospective study, involving clinically easily accessible variables, being validated in a different set of ICU patients, and having a similar prediction accuracy as those in previous models.
The present study has several limitations. As a single-center prospective observational study, the present findings may be limited by potential selection bias and reduced generalizability. Furthermore, the relatively small external validation cohort requires further multicenter studies with a larger sample size to verify the applicability of the model, and facilitate its clinical adoption. In addition, the diagnosis of ICU-AW in the present study was primarily based on the MRC score criteria, which are only applicable to patients who are conscious, and able to cooperate with the examination. Consequently, there is a possibility that selection bias may have occurred in the inclusion of the study population. For ICU-AW in non-responsive, comatose critically ill patients, electrophysiological testing (eg electromyography) and muscle ultrasonography may be incorporated as complementary diagnostic modalities to the MRC score. Finally, the generalizability of the present prediction model may be limited to the Chinese population, since this was derived and validated exclusively using clinical data obtained from patients treated within Chinese healthcare settings. This population-specific limitation underscores the need for external validation studies in diverse ethnic and healthcare systems before broader international applications can be recommended. Therefore, the validity and reproducibility of the prediction model in the present study requires further investigation in future research.
Conclusion
The nomogram model developed in the present study, which incorporated six predictive factors (age, MODS, use of NMBAs, duration of mechanical ventilation, duration of sedation, and APACHE II score), demonstrated good discriminative ability, calibration, and clinical utility. This can effectively predict the risk of ICU-AW in sepsis patients, providing clinicians with a valuable tool for its early identification and intervention. Furthermore, the visual nomogram improved the convenience of risk assessment in clinical practice.
Abbreviations
APACHE II, Acute Physiology and Chronic Health Evaluation II; AUC, area under the receiver operating characteristic curve; DCA, decision curve analysis; DSI, daily sedation interruption; ICU, intensive care unit; ICU-AW, intensive care unit-acquired weakness; IQR, interquartile ranges; LASSO, least absolute shrinkage and selection operator; MODS, multiple organ dysfunction syndrome; MRC, Medical Research Council; NMBAs, neuromuscular blocking agents; NRS 2002, Nutritional Risk Screening 2002; RASS, Richmond Agitation Sedation Scale; ROC, receiver operating characteristic; SOFA, Sequential Organ Failure Assessment.
Data Sharing Statement
The datasets used and/or analyzed in the study are available from the corresponding author, Siya Meng, upon reasonable request.
Ethics Approval and Informed Consent
The study was approved by the ethics committee of Shenzhen Nanshan People’s Hospital, Shenzhen, China (approval number #KY-2022-012-01).
All procedures performed in the study that involved human participants were conducted following the Declaration of Helsinki (as revised in 2013). An informed consent was obtained from all patients. The participants provided an informed consent before participating in the study. The consents were obtained directly from the patient(s).
Acknowledgments
We would like to express our sincerest gratitude to Beirong Mo and Shouzhen Cheng.
Author Contributions
All authors made a significant contribution to the work reported, regardless of whether the contribution was in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas. All authors took part in the drafting, revision, or critical review of the article. All authors provided the final approval for the version to be published, agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Shenzhen Nanshan District Technology R&D and Creative Design Project (NS2023043), the Shenzhen Nanshan District Technology R&D and Creative Design Project (NS2023098), the Shenzhen Basic Research Project (Natural Science Fund), the Basic Research General Project (JCYJ20230807115808017, JCYJ20230807115808018), the Sanming Project of Medicine in Shenzhen (SZSM202403005), and the Municipal Financial Subsidy of Nanshan District Medical Key Discipline Construction and Major Science and Technology Project in Healthcare System of Nanshan District Shenzhen (NSZD2025006).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Weng L, Xu Y, Yin P, et al. National incidence and mortality of hospitalized sepsis in China. Crit Care. 2023;27(1):84. doi:10.1186/s13054-023-04385-x
2. Evans L, Rhodes A, Alhazzani W, et al. Executive summary: surviving sepsis campaign: international guidelines for the management of sepsis and septic shock 2021. Crit Care Med. 2021;49(11):1974–17. doi:10.1097/CCM.0000000000005357
3. Markwart R, Saito H, Harder T, et al. Epidemiology and burden of sepsis acquired in hospitals and intensive care units: a systematic review and meta-analysis. Intensive Care Med. 2020;46(8):1536–1551. doi:10.1007/s00134-020-06106-2
4. Liu J, Xu Z, Luo S, Bai Y, Feng J, Li F. Risk factors for ICU-acquired weakness in sepsis patients: a retrospective study of 264 patients. Heliyon. 2024;10(11):e32253. doi:10.1016/j.heliyon.2024.e32253
5. Herridge MS, Batt J, Santos CD. ICU-acquired weakness, morbidity, and death. Am J Respir Crit Care Med. 2014;190(4):360–362. doi:10.1164/rccm.201407-1263ED
6. Van Aerde N, Meersseman P, Debaveye Y, et al. Five-year impact of ICU-acquired neuromuscular complications: a prospective, observational study. Intensive Care Med. 2020;46(6):1184–1193. doi:10.1007/s00134-020-05927-5
7. Vanhorebeek I, Latronico N, Van den Berghe G. ICU-acquired weakness. Intensive Care Med. 2020;46(4):637–653. doi:10.1007/s00134-020-05944-4
8. Klawitter F, Oppitz MC, Goettel N, et al. A global survey on diagnostic, therapeutic and preventive strategies in intensive care unit-acquired weakness. Medicina. 2022;58(8). doi:10.3390/medicina58081068
9. Li M, Shao H, Wang C, et al. Risk factors and their predictive value for intensive care unit acquired weakness in patients with sepsis. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021;33(6):648–653. doi:10.3760/cma.j.cn121430-20210329-00459
10. Lei L, He L, Zou T, et al. Predicting early diagnosis of intensive care unit-acquired weakness in septic patients using critical ultrasound and biological markers. BMC Anesthesiol. 2025;25(1):39. doi:10.1186/s12871-025-02911-8
11. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
12. van Wagenberg L, Witteveen E, Wieske L, Horn J. Causes of mortality in ICU-acquired weakness. J Intensive Care Med. 2020;35(3):293–296. doi:10.1177/0885066617745818
13. Mitobe Y, Morishita S, Ohashi K, et al. Skeletal muscle index at intensive care unit admission is a predictor of intensive care unit-acquired weakness in patients with sepsis. J Clin Med Res. 2019;11(12):834–841. doi:10.14740/jocmr4027
14. Latronico N, Herridge M, Hopkins RO, et al. The ICM research agenda on intensive care unit-acquired weakness. Intensive Care Med. 2017;43(9):1270–1281. doi:10.1007/s00134-017-4757-5
15. Takahashi Y, Morisawa T, Okamoto H, et al. Diaphragm dysfunction and ICU-acquired weakness in septic shock patients with or without mechanical ventilation: a pilot prospective observational study. J Clin Med. 2023;12(16):5191. doi:10.3390/jcm12165191
16. Li Y, Li F, Xing B. Analysis of risk factors of concurrent ICU acquired weakness in elderly patients with sepsis undergoing mechanical ventilation and the early predictive value of mNUTRIC score. J Pra Med. 2022;38:2568–2573.
17. Yang T, Li Z, Jiang L, Wang Y, Xi X. Risk factors for intensive care unit-acquired weakness: a systematic review and meta-analysis. Acta Neurol Scand. 2018;138(2):104–114. doi:10.1111/ane.12964
18. Peñuelas O, Muriel A, Frutos-Vivar F, et al. Prediction and outcome of intensive care unit-acquired paresis. J Intensive Care Med. 2018;33(1):16–28. doi:10.1177/0885066616643529
19. de Jonghe B, Lacherade JC, Sharshar T, Outin H. Intensive care unit-acquired weakness: risk factors and prevention. Crit Care Med. 2009;37(10 Suppl):S309–315. doi:10.1097/CCM.0b013e3181b6e64c
20. de Carvalho M. Intensive care unit-acquired weakness: neuropathology. J Clin Neurophysiol. 2020;37(3):197–199. doi:10.1097/WNP.0000000000000651
21. Price DR, Mikkelsen ME, Umscheid CA, Armstrong EJ. Neuromuscular blocking agents and neuromuscular dysfunction acquired in critical illness: a systematic review and meta-analysis. Crit Care Med. 2016;44(11):2070–2078. doi:10.1097/CCM.0000000000001839
22. Bellaver P, Schaeffer AF, Leitao CB, Rech TH, Nedel WL. Association between neuromuscular blocking agents and the development of intensive care unit-acquired weakness (ICU-AW): a systematic review with meta-analysis and trial sequential analysis. Anaesth Crit Care Pain Med. 2023;42(3):101202. doi:10.1016/j.accpm.2023.101202
23. Hermans G, Van den Berghe G. Clinical review: intensive care unit acquired weakness. Crit Care. 2015;19(1):274. doi:10.1186/s13054-015-0993-7
24. Chlan LL, Tracy MF, Guttormson J, Savik K. Peripheral muscle strength and correlates of muscle weakness in patients receiving mechanical ventilation. Am J Crit Care. 2015;24(6):e91–98. doi:10.4037/ajcc2015277
25. Mart MF, Pun BT, Pandharipande P, Jackson JC, Ely EW. ICU survivorship-the relationship of delirium, sedation, dementia, and acquired weakness. Crit Care Med. 2021;49(8):1227–1240. doi:10.1097/CCM.0000000000005125
26. Li SP, Zhou XL, Zhao Y. Sedation with midazolam worsens the diaphragm function than dexmedetomidine and propofol during mechanical ventilation in rats. Biomed Pharmacother. 2020;121:109405. doi:10.1016/j.biopha.2019.109405
27. Kamdar BB, Combs MP, Colantuoni E, et al. The association of sleep quality, delirium, and sedation status with daily participation in physical therapy in the ICU. Crit Care. 2016;19(1):261. doi:10.1186/s13054-016-1433-z
28. Piva S, Fagoni N, Latronico N. Intensive care unit-acquired weakness: unanswered questions and targets for future research. F1000Res. 2019;8:F1000. Faculty Rev-508 [pii]. doi:10.12688/f1000research.17376.1
29. Lewis K, Balas MC, Stollings JL, et al. A focused update to the clinical practice guidelines for the prevention and management of pain, anxiety, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2025;53(3):e711–e727. doi:10.1097/CCM.0000000000006574
30. Salluh JI, Soares M. ICU severity of illness scores: APACHE, SAPS and MPM. Curr Opin Crit Care. 2014;20(5):557–565. doi:10.1097/MCC.0000000000000135
31. Guo Y, Shan W, Xiang J. Predictive modeling of ICU-AW inflammatory factors based on machine learning. BMC Neurol. 2024;24(1):483. doi:10.1186/s12883-024-03981-w
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Tracking Epidemiological Characteristics and Risk Factors of Multi-Drug Resistant Bacteria in Intensive Care Units
Wu C, Lu J, Ruan L, Yao J
Infection and Drug Resistance 2023, 16:1499-1509
Published Date: 15 March 2023
Risk Factors for Granulomatous Mastitis and Establishment and Validation of a Clinical Prediction Model (Nomogram)
Zeng Y, Zhang D, Fu N, Zhao W, Huang Q, Cui J, Chen Y, Liu Z, Zhang X, Zhang S, Mansoor KM
Risk Management and Healthcare Policy 2023, 16:2209-2222
Published Date: 20 October 2023
Risk Factor Analysis and Nomogram for Predicting In-Hospital Mortality in ICU Patients with Heat Stroke: A National Multicenter Study
Wang L, Fu X, He M, Shi L, Wan D, Wang Y, Wu Q, Yang J, Cai B, Xia H, Chen H, Zhang G, Lei X, Zhang W, Feng Z, Wang B, Zhang Z
Journal of Multidisciplinary Healthcare 2023, 16:3189-3201
Published Date: 27 October 2023
Dynamic Nomogram for Subsyndromal Delirium in Adult Intensive Care Unit: A Prospective Cohort Study
Cheng J, Lao Y, Chen X, Qiao X, Sui W, Gong X, Zhuang Y
Neuropsychiatric Disease and Treatment 2023, 19:2535-2548
Published Date: 22 November 2023
Development and Validation of a Nomogram for Predicting Sepsis-Associated Acute Respiratory Distress Syndrome
Yan C, Cai Y, Cai W, Wang Q, Li W, Geng Q
International Journal of General Medicine 2025, 18:5917-5925
Published Date: 29 September 2025