Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Risk Factor Analysis and Nomogram for Predicting In-Hospital Mortality in ICU Patients with Heat Stroke: A National Multicenter Study
Authors Wang L, Fu X, He M, Shi L, Wan D, Wang Y, Wu Q, Yang J, Cai B, Xia H, Chen H, Zhang G, Lei X ![]() , Zhang W, Feng Z, Wang B, Zhang Z
, Zhang W, Feng Z, Wang B, Zhang Z
Received 1 August 2023
Accepted for publication 19 October 2023
Published 27 October 2023 Volume 2023:16 Pages 3189—3201
DOI https://doi.org/10.2147/JMDH.S428617
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Lietao Wang,1,* Xin Fu,1,* Min He,1,* Lvyuan Shi,1 Dingyuan Wan,1 Yucong Wang,1 Qin Wu,1 Jing Yang,1 Bayuan Cai,2 Hongtao Xia,3 Hongxu Chen,4 Ge Zhang,5 Xianying Lei,6 Wei Zhang,7 Zhongxue Feng,7 Bo Wang,1 Zhongwei Zhang1 On behalf of Heat Stroke Research Group in Southwestern China
1Department of Critical Care Medicine, West China Hospital, Sichuan University, Chengdu, 610041, People’s Republic of China; 2Department of Critical Care Medicine, The People’s Hospital of Jiajiang, Leshan, People’s Republic of China; 3Department of Critical Care Medicine, Suining Central Hospital, Suining, People’s Republic of China; 4Department of Critical Care Medicine, The Hospital of Traditional Chinese Medicine of Leshan, Leshan, People’s Republic of China; 5Department of Critical Care Medicine, The First People’s Hospital of Longquanyi District, Chengdu, People’s Republic of China; 6Department of Critical Care Medicine, The Affiliated Hospital of Southwest Medical University, Luzhou, People’s Republic of China; 7Department of Critical Care Medicine, State Key Laboratory of Biotherapy and Cancer Center, West China Hospital, Sichuan University and Collaborative Innovation Center of Biotherapy, Chengdu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bo Wang; Zhongwei Zhang, Department of Critical Care Medicine, West China Hospital, Sichuan University, No. 37, Guoxue Alley, Chengdu, 610041, People’s Republic of China, Tel/Fax +86-28-85422739, Email [email protected]; [email protected]
Objective: The aim of this nationwide multicenter study was to ascertain the risk factors associated with in-hospital mortality in patients with heat stroke admitted to intensive care units (ICUs) and to develop a nomogram for prognostic prediction.
Methods: A retrospective analysis was conducted on clinical data collected from ICU patients diagnosed with heat stroke across multiple centers nationwide. Univariate and multivariate logistic regression analyses were performed to identify significant risk factors for in-hospital mortality. Based on the results of the multivariate analysis, a nomogram was constructed to estimate the individualized probability of mortality. Internal validation of the nomogram was performed, and its performance was assessed using receiver operating characteristic (ROC) curves, calibration plots, and decision curve analysis (DCA).
Results: A total of 292 ICU patients with heat stroke were included in this study. Three risk factors, namely Cr (creatinine), AST (aspartate aminotransferase), and SBP (systolic blood pressure), were found to be significantly associated with in-hospital mortality. These risk factors were incorporated into the nomogram, which exhibited good discriminative ability (area under the ROC curve of the training and validation cohorts were 0.763 and 0.739, respectively) and calibration. Internal validation and decision curve analysis confirmed the stability and reliability of the nomogram.
Conclusion: This nationwide multicenter study identified key risk factors for in-hospital mortality in ICU patients with heat stroke. The developed nomogram provides an individualized prediction of mortality risk and can serve as a valuable tool for clinicians in the assessment and management of ICU patients with heat stroke.
Keywords: heat stroke, intensive care unit, in-hospital mortality, risk factors, nomogram
Background
With the increasing occurrence of extreme thermal events, heat stroke has become more common among patients in intensive care units (ICUs).1 Heat stroke (HS) is a heat-related medical condition characterized by an abrupt rise in core body temperature surpassing 40°C and impairment of the central nervous system.2 It can be categorized into classical heat stroke (CHS) or exertional heat stroke (EHS) based on the underlying causes and susceptible population.3,4 CHS occurs passively in individuals exposed to extreme temperatures, while EHS typically arises during strenuous physical activity.4 CHS often manifests as an epidemic and contributes to 9–37% of heat-related fatalities during heat waves.5,6 In the intensive care setting, the mortality rates for EHS and CHS are 26.5% and 63.2%, respectively.4
Heat stroke is characterized by a rapid onset, rapid progression, and involvement of multiple organs.7–12 Consequently, immediate treatment is crucial upon diagnosis of heat stroke.5,6,13–15
Heat stroke is a multi-organ dysfunction syndrome primarily characterized by a rapid elevation of core body temperature.16 Although its exact pathogenesis remains not entirely clear, it may involve various critical factors, including heat toxicity, innate immunity, endothelial cell damage, and the impact on skeletal muscles.4 Regarding heat toxicity, high temperatures can directly harm macromolecules such as DNA, proteins, and cell membranes, consequently leading to aberrations in cellular structures such as the cytoskeleton, mitochondria, Golgi apparatus, endoplasmic reticulum, and ultimately resulting in cell damage, necrosis, or apoptosis.17–19 In the context of innate immunity, it is theorized that heat stroke may trigger the activation of the innate immune system, causing an increase in white blood cells, release of inflammatory cytokines, adhesion molecules, and acute-phase proteins, thereby initiating an inflammatory response.20–24 In animal experiments, heat stroke has been shown to disrupt endothelial barrier function, manifesting as endothelial cell damage in organs such as the heart, lungs, liver, small intestine, and spleen, consequently leading to coagulation dysfunction and inflammation.18,20,25–27 While skeletal muscles exhibit relatively higher tolerance to heat injury, increased muscle tension and competition for blood flow between the skin and muscles can potentially lead to reduced muscle blood flow, tissue damage, including rhabdomyolysis, and subsequently renal overload and failure.10,28–31
Currently, there is a lack of specific and sensitive assessment scales to evaluate the condition and potential in-hospital outcomes of patients with severe heat stroke, leading to ineffective treatment guidance in clinical practice.
The aim of this study is to identify the risk factors associated with mortality in patients diagnosed with severe heat stroke and to develop a predictive nomogram model that can accurately assess the patients’ condition and predict their outcomes.
Patients and Methods
Patients
This retrospective case-control study aimed to analyze the clinical data of critically ill patients with heat stroke who received treatment at multiple centers between June 2022 and October 2022, this manuscript evaluates both classical and exertional heat stroke simultaneously. It was an observational multicenter study conducted retrospectively, specifically focusing on hospitalizations related to heat stroke across 83 hospitals in southwest of China.
The inclusion criteria for this study encompassed patients aged 18 years or older who met the diagnostic criteria for severe heat stroke. These criteria included both classic and exertional heat stroke, a documented history of exposure to hot and humid weather or strenuous activity, presence of hyperthermia with a core temperature exceeding 40°C, and the occurrence of associated neurological dysfunction upon admission, such as confusion, convulsions, or coma.
The exclusion criteria for this study included pregnant and lactating patients, individuals with underlying irreversible diseases affecting mortality, and those who had participated in other studies; they were excluded from the study.
For each patient, a comprehensive set of information was collected, including demographic data (age, sex, height, weight), hospital status, including heart rate (HR), systolic blood pressure (SBP), diastolic blood pressure (DBP), heart rate (RR), and laboratory test results on the first day of admission. The laboratory tests encompassed targets such as albumin (ALB), platelet count (PLT), white blood cell count (WBC), neutrophils (NEUT), total cholesterol (TC), lymphocytes (LYM), alkaline phosphatase (ALP), blood urea nitrogen (BUN), creatinine (Cr), aspartate aminotransferase (AST), alanine aminotransferase (ALT), total bilirubin (TIBL), direct bilirubin (DIBL), lactate (Lac), and prothrombin time (PT). All data utilized in this study were extracted from electronic medical records or hospital databases upon the patients’ initial admission. Considering the retrospective design of this study, an informed consent exemption was obtained from the Ethics Committee on Biomedical Research, West China Hospital of Sichuan University, and no human intervention was involved in the data collection process. The Biomedical Ethics Committee of West China Hospital, Sichuan University, approved the study protocol (approval number: 2022-1542, registration number: ChiCTR2200066314).
Result Analysis
The primary outcome of this study was the survival or non-survival of severe heat stroke patients upon hospital discharge.
Statistical Analysis
The dataset was divided into training and validation datasets in a ratio of 7:3. This division was performed while ensuring that both datasets maintained a comparable distribution of survivors and non-survivors through stratified resampling.
Categorical variables were compared between survivors and non-survivors using Chi-Square or Fisher’s exact tests. Continuous variables were presented as mean ± standard deviation or median with interquartile range, while categorical variables were expressed as percentages. Univariate logistic regression analysis was performed to identify potential prognostic factors. Factors that showed significance with a p-value less than 0.05 in the univariate analysis, along with the clinician’s treatment experience, were included in the forward stepwise multivariate logistic regression model. Hazard ratios and corresponding 95% confidence intervals (CIs) were calculated.
Model discrimination, which reflects the ability of the model to distinguish between survivors and non-survivors, was assessed using the area under the Receiver Operating Characteristic (ROC) curve, also known as the Concordance Index (C-Index). A C-index of 1.00 represents perfect discrimination, while a C-index of 0.5 indicates no discrimination. Based on the results of the multivariate logistic regression analysis, a nomogram was constructed using the root mean square package of R software to estimate the overall risk of death. The ROC curve was plotted, and the area under the ROC curve (AUC) was calculated to evaluate the discriminative power of the nomogram. To assess the stability of the heatstroke nomogram, internal validation was performed using a 30% sample. A calibration plot was generated to assess the agreement between observed and predicted probabilities, the calibration curve is a method of evaluating a model, with the horizontal coordinate being the predicted probability of an event and the vertical coordinate being the actual probability of an event. The dashed diagonal line in the figure is the reference line, that is, the prediction probability is equal to the actual probability. The further the deviation from the diagonal line, the greater the prediction error. Additionally, decision curve analysis (DCA) was applied to the nomogram to assess the net benefit was calculated for each clinical severity scoring system, evaluates the clinical practicability of the model quantitatively by calculating the net benefit. The net benefit accounts for the trade-off between sensitivity and specificity. A good model should have a high net benefit value under the threshold required by its clinical problem. In this study, there is one horizontal solid gray line (the None line) and three slanted solid gray lines (the second is the All line, and the first and third lines are the confidence intervals of the All lines,). The None line represents an expectation that no adverse outcome will occur in All patients, and the ALL line represents an expectation that no adverse outcome will occur in all patients. The bright red is realized as the decision curve of the model, and the two lines in light red are the confidence intervals of the decision curve.
All statistics were performed using SPSS 26.0 (SPSS Inc) and R 4.2.2 (R Foundation for Statistical Computing, Vienna, Austria) software. P < 0.05 was considered statistically significant.
Results
During the 5-month study span, a sum of 873 patients diagnosed with heat stroke was identified across 83 hospitals. Out of these, 292 patients were included in the study, with 219 patients assigned to the training cohort and 73 patients to the validation cohort (Figure 1). The median age of the patients was 72 years (IQR: 63–79 years). Among the included patients, 131 (44.9%) were women, while the majority (55.1%) were men. Before discharge, 93 patients (31.85%) succumbed to the condition, while 199 patients (68.15%) survived.
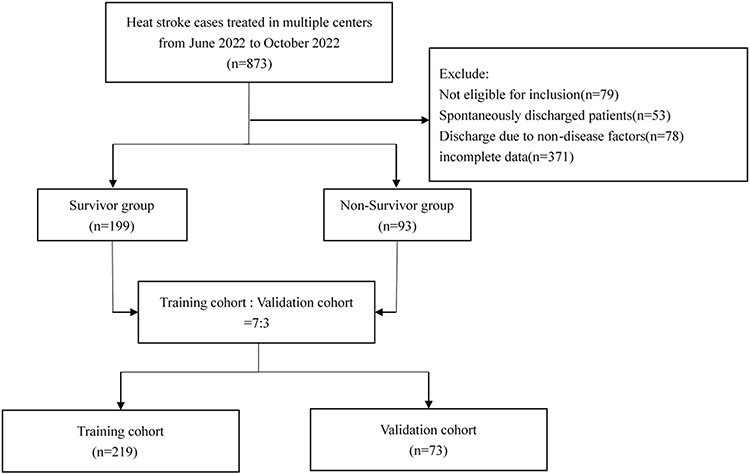 |
Figure 1 Flow chart for patients’ selection. |
The comparison of baseline characteristics between survivors and non-survivors revealed no significant differences in age, gender, body mass index (BMI), respiratory rate, and laboratory test results including white blood cell count (WBC), total cholesterol (TC), alkaline phosphatase (ALP), direct bilirubin (DIBL), and total bilirubin (TBIL). However, several indicators showed statistically significant differences between surviving and non-surviving patients. These indicators included albumin (ALB) (p<0.001), platelet count (PLT) (p=0.002), neutrophils (NEUT) (p=0.001), lymphocytes (LYM) (p<0.001), blood urea nitrogen (BUN) (p=0.003), creatinine (Cr) (p<0.001), alanine aminotransferase (ALT) (p<0.001), aspartate aminotransferase (AST) (p<0.001), heart rate (HR) (p=0.021), systolic blood pressure (SBP) (p<0.001), diastolic blood pressure (DBP) (p<0.001), lactate (Lac) (p<0.001), and prothrombin time (PT) (p<0.001). Detailed baseline characteristics of the patients can be found in Table 1 and Table 2.
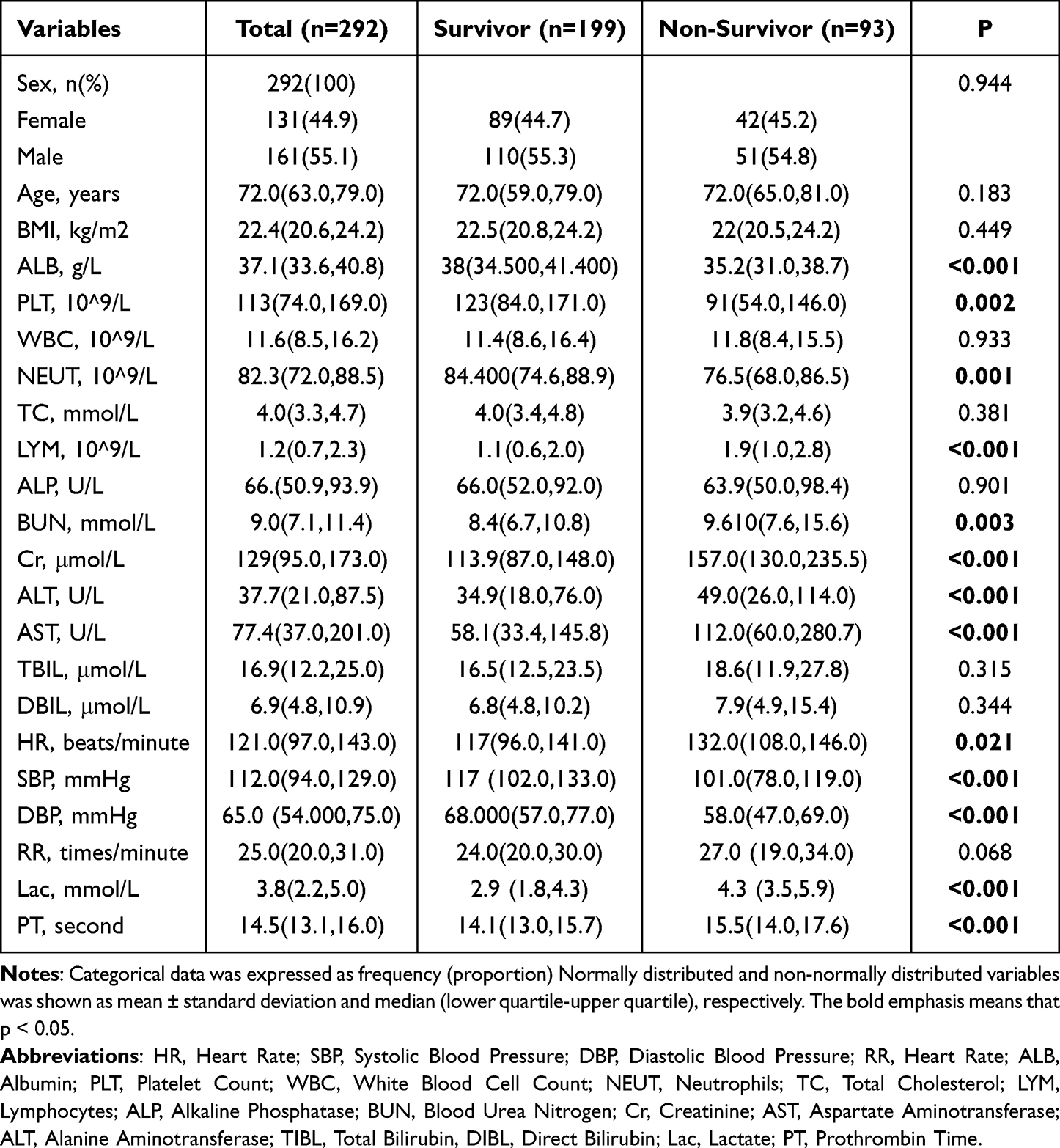 |
Table 1 Baseline Demographic Characteristics of Included Patients |
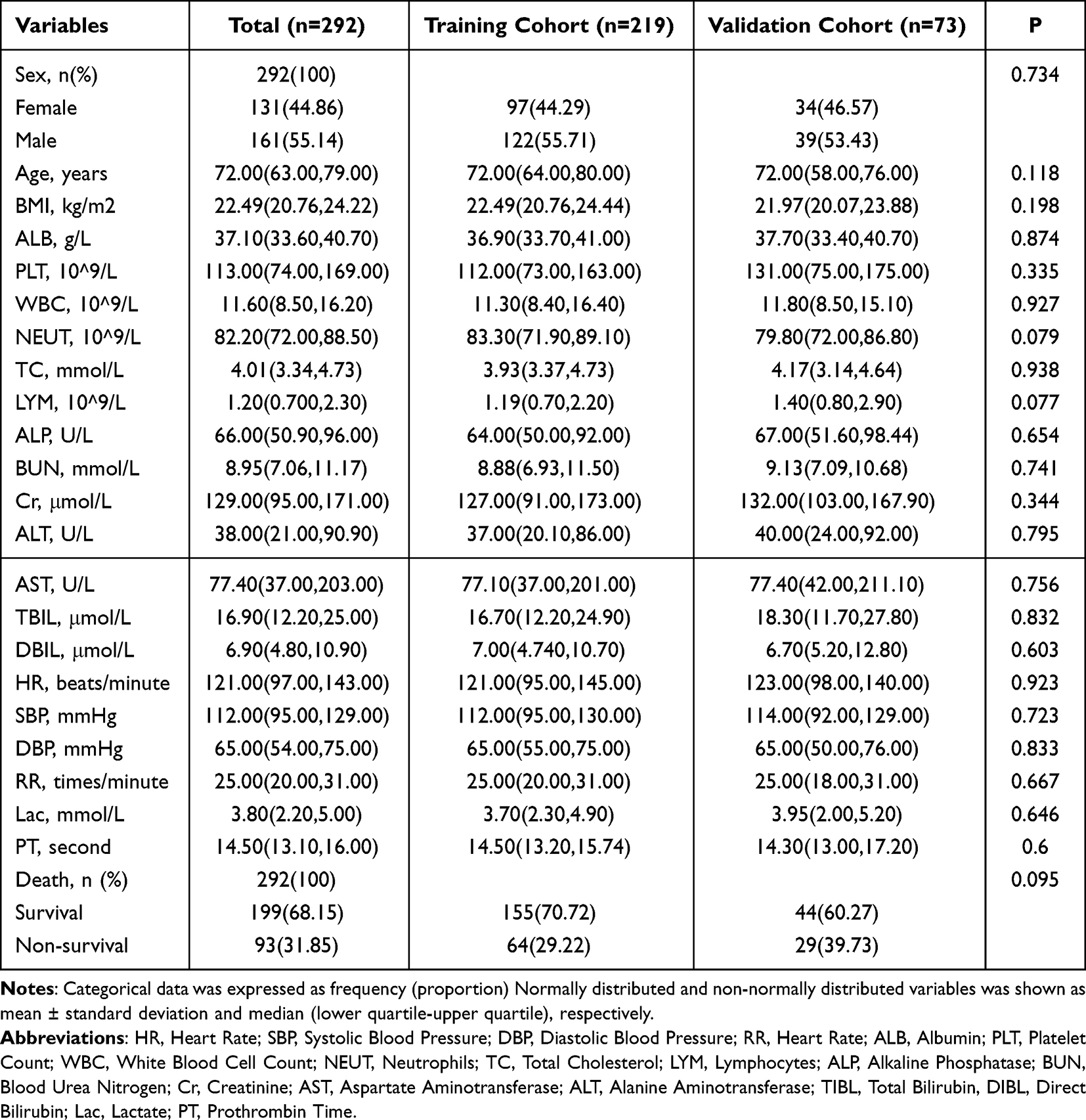 |
Table 2 Demographical and Clinical Characteristics Between Patient with the Training Cohort and the Validation Cohort |
A univariate analysis was conducted to examine 21 potential predictors and their association with mortality outcomes in heat stroke patients. The results revealed that nine predictors were significantly associated with prognosis in heat stroke patients: albumin (ALB) (p=0.013), lymphocytes (LYM) (p=0.011), blood urea nitrogen (BUN) (p=0.019), creatinine (Cr) (p<0.001), alanine aminotransferase (ALT) (p=0.002), aspartate aminotransferase (AST) (p=0.002), total bilirubin (TBIL) (p=0.02), systolic blood pressure (SBP) (p<0.001), lactate (Lac) (p=0.044), and prothrombin time (PT) (p<0.001).
Further analysis using multivariate regression, incorporating the factors that showed statistically significant differences in the univariate analysis, revealed that Cr (odds ratio [OR]=1.005, 95% confidence interval [CI]: 1.001–1.008, p=0.006), AST (OR=1.002, 95% CI: 1.000–1.003, p=0.01), and SBP (OR=0.981, 95% CI: 0.969–0.992, p=0.001) were identified as independent risk factors for the prognosis of heat stroke (Table 3).
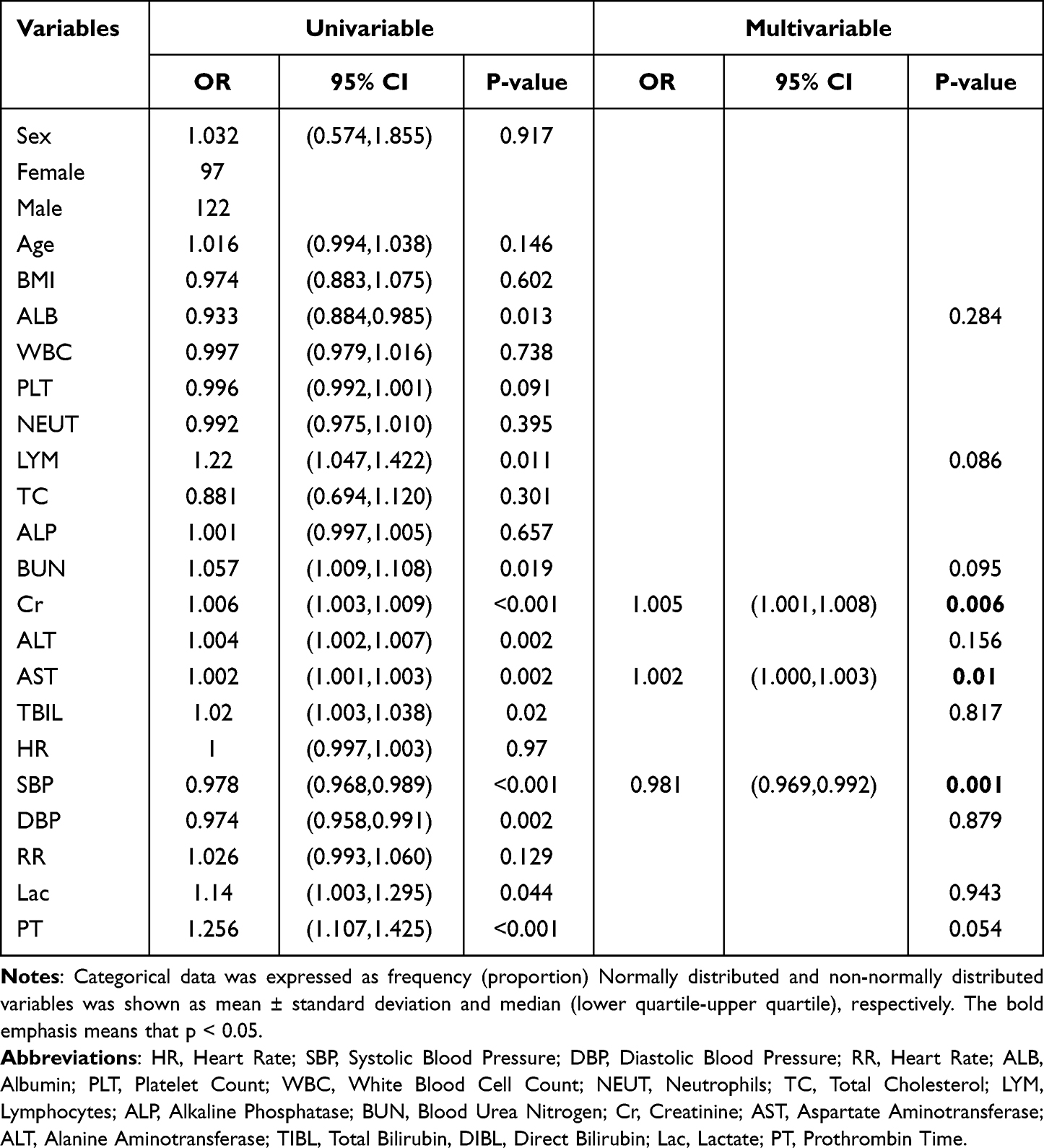 |
Table 3 Univariable and Multivariable Logistic Regression for Analyzing the Associated Factors for Heat Stroke Patient |
Additionally, the prognostic value of Cr, AST, SBP, and the Nomogram in severe heat stroke patients was evaluated. The predictive accuracy of these four indicators was compared using ROC curve analysis. The area under the curve (AUC) values for Cr, AST, SBP, and the Nomogram were as follows: Cr = 0.760 (95% CI: 0.697–0.815), AST = 0.660 (95% CI: 0.594–0.723), SBP = 0.660 (95% CI: 0.594–0.723), and Nomogram = 0.762 (95% CI: 0.700–0.817). The AUC of the Nomogram was higher compared to Cr, AST, and SBP alone, indicating that the Nomogram is the most reliable predictor for predicting the prognosis of severe heat stroke patients and can be utilized as a predictive tool (Figure 2).
 |
Figure 2 Areas under the curves of Cr, AST, SBP and Nomogram (A) The area under the curve of Cr was 0.760. (B) The area under the curve of AST was 0.660. (C) The area under the curve of SBP was 0.660. (D) The area under the curve of Nomogram was 0.762. (E) Compared with other independent predictive indicators, the area under the curve of Nomogram in the combined group was largest, thus indicating that Nomogram was the most accurate and reliable indicator for predicting the prognosis of patients with HS. |
Using the training cohort, a model incorporating Cr, AST, and SBP was developed, and a nomogram was constructed to predict the probability of in-hospital mortality in heat stroke patients (Figure 3).
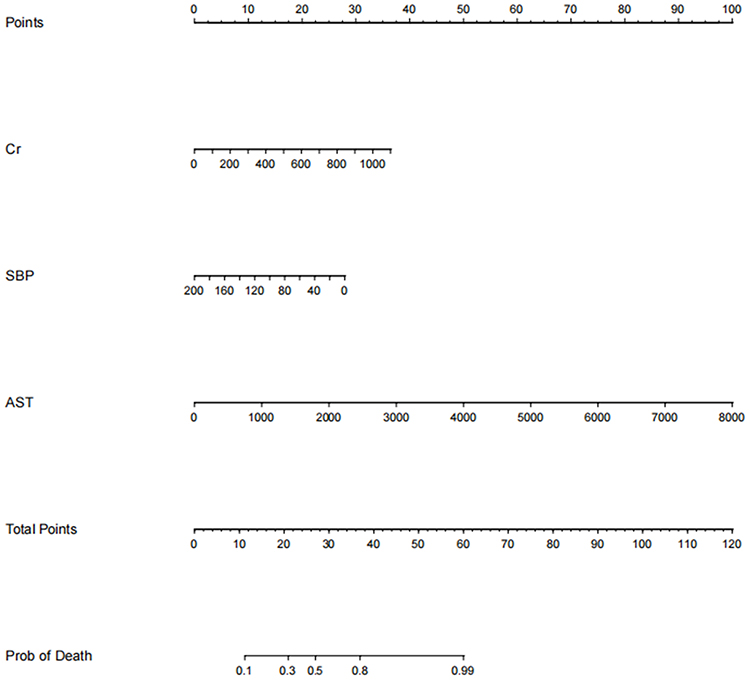 |
Figure 3 Nomogram of predicting the probability of in-hospital mortality in heat stroke patients. The first line shows the point assignment of each variable. Lines 2–4 show the variables included in the model. When using a nomogram for a single patient, a point is assigned to each variable based on clinicopathological characteristics, and all points are added. Each score in the total score in row 5 will correspond to the probability of risk in the last row. |
Furthermore, ROC curves were established for both the training cohort and the validation cohort. The AUC of the nomogram in the training cohort was 0.763, with a sensitivity of 0.609 and a specificity of 0.877 (Figure 4A). In the validation cohort, the AUC of the nomogram was 0.739, with a sensitivity of 0.862 and a specificity of 0.545 (Figure 4B).
 |
Figure 4 ROC of Nomogram model in the training and validation cohorts. (A) The AUC of Nomogram in the training cohort was 0.763 (B) The AUC of Nomogram in the validation cohort was 0.739. |
Internal validation was also conducted to assess the performance of the nomogram. The calibration curves demonstrated good agreement between the training and validation cohorts (Figure 5).
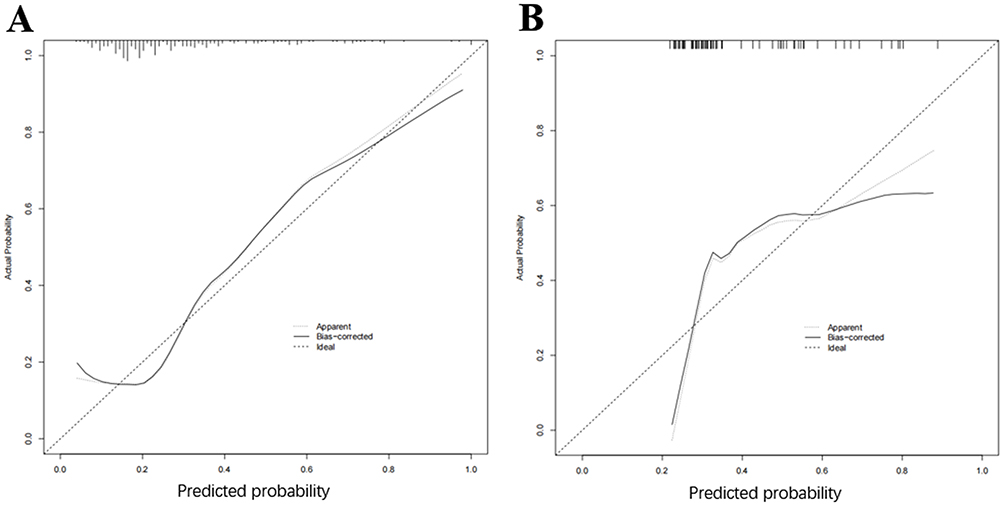 |
Figure 5 Calibration curve based on Nomogram model in the training and validation cohorts. (A) Clinical calibration curve analysis of the training cohort. (B) Clinical calibration curve analysis of the validation cohort. |
Moreover, decision curve analysis was performed to evaluate the clinical utility of the model. The decision curve indicated that within the threshold range of 20% to 80%, the model’s decision curve was above the None line and the All line, demonstrating its clinical practicability in this range (Figure 6).
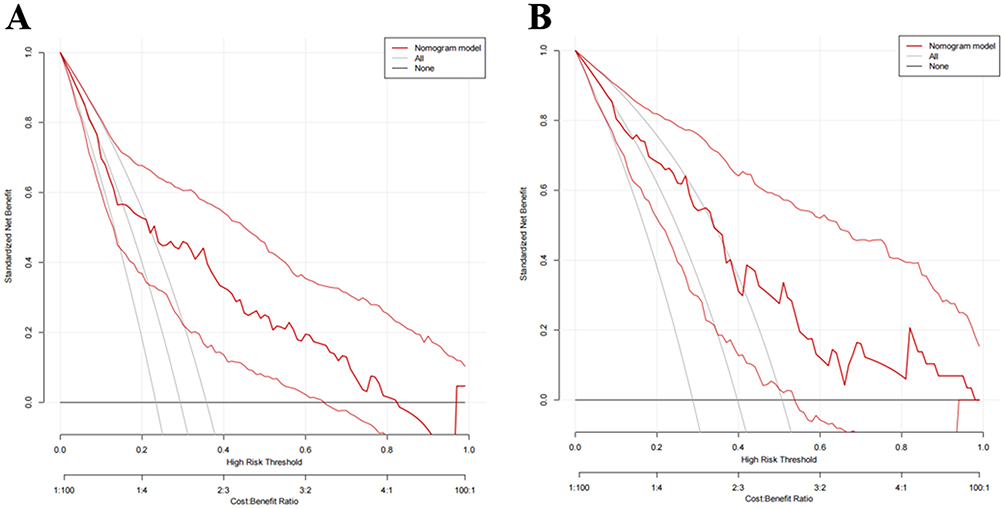 |
Figure 6 Decision curve analysis (DCA) based on Nomogram model in the training and validation cohorts. (A) Clinical DCA of the training cohort. (B) Clinical DCA of the validation cohort. |
Discussion
This study contrasting a single-factor analysis with a predictive model for estimating hospital outcomes of individuals with severe heat stroke. The AUC of the nomogram (AUC = 0.762, 95% CI: 0.700–0.817), was superior to that of Cr (AUC= 0.760, 95% CI: 0.697–0.815), AST (AUC = 0.660,95% CI: 0.594–0.723), and SBP (AUC = 0.660, 95% CI: 0.594–0.723) in isolation, signifying that the nomogram stands as the most dependable predictor for forecasting the prognosis of severe heat stroke patients and can serve as a valuable predictive tool. The results demonstrated that the model exhibited appropriate accuracy and consistency.
Among the potential or existing complications in critically ill heat stroke patients, acute kidney injury (AKI), acute liver injury (ALI), and shock are commonly observed.3,4,8 In this study, it was observed that Cr remained an independent risk factor for recovery from hyperthermia, even following adjustment for confounding variables (odds ratio [OR]=1.005, 95% confidence interval [CI]: 1.001–1.008, p=0.006). AKI is characterized by impaired renal function exhibit elevated plasma creatinine levels, reduced urine volume and flow rate, decreased fractional sodium excretion, and mildly increased urine specific gravity.32–35 The incidence of AKI in hospitalized patients is approximately 10–15%, while in the intensive care unit, it exceeds 50%. Notably, AKI is more prevalent in exertional heat stroke (EHS) compared to classical heat stroke (CHS), occurring in around 20% of exertional heat stroke cases. In some instances, AKI can progress to renal failure necessitating dialysis.34,36–38 Elevated body temperature associated with heat stroke leads to inevitable kidney damage, characterized by tubular cell death.39 Studies on sepsis have suggested that AKI independently contributes to increased patient mortality by causing electrolyte and acid-base disturbances, fluid retention, metabolic dysfunction, impaired neutrophil function, and compromised infection clearance.6 Both heat stroke and sepsis trigger extensive inflammatory responses and affect multiple organ functions. Heat stroke-induced AKI can be attributed to the systemic inflammatory response syndrome (SIRS) elicited by heat stroke and related inflammatory responses.3
In patients with heat stroke, acute liver injury (ALI) can occur to varying degrees, and in some cases, it can progress to hepatic failure, particularly in patients with exertional heat stroke (EHS).40–44 ALI is characterized by an early increase in serum levels of aspartate aminotransferase (AST) and lactate dehydrogenase, peaking after a few days, followed by a rise in bilirubin levels on the second or third day.45–48 Our investigation revealed that AST (OR=1.002, 95% CI: 1.000–1.003, p=0.01) unequivocally constituted an independent risk factor. AST levels can serve as an objective indicator of liver function in patients with heat stroke.
Shock is another common complication in heat stroke patients, occurring in 18–65% of cases and being associated with increased morbidity and mortality.45,49–52 According to Chinese studies, the mortality rate in the intensive care unit (ICU) for classical heat stroke (CHS) patients is 63.2%, and EHS patients account for 8.6%-18.0% of cases of exertional heat-related diseases, with a mortality rate usually exceeding 30% when combined with hypotension.8 Shock in heat stroke patients is primarily characterized by sepsis-like distributive shock on hemodynamic monitoring, which manifests as elevated cardiac output, low systemic vascular resistance, and normal or reduced cardiac filling pressures.52–56 Hypodynamic shock, distinguished by decreased cardiac output and boosted systemic vascular resistance, exists particularly common in elderly patients.52,56–58 This study demonstrated that SBP (OR=0.981, 95% CI: 0.969–0.992, p=0.001) functioned as an independent risk factor in the prognosis of patients exposed to thermal radiation. Therefore, monitoring and controlling blood pressure is crucial for heat stroke patients.
The models developed in this study utilized variables obtained from blood biomarkers measured within 24 hours of admission. These biomarkers are readily available, cost-effective, and provide quick results, making them practical for clinical use. The inclusion of relevant independent variables such as acute kidney injury, acute liver injury, and shock allows for a comprehensive assessment of heat stroke characteristics and helps clinicians in rapidly evaluating patient severity in clinical working. In cases where the clinician lacks knowledge regarding the severity of the patient’s condition, this model can furnish a precise and expeditious prognosis assessment.
Limitations
Despite including a larger sample size compared to other studies, inherent limitations of retrospective studies and potential data biases cannot be completely eliminated. Additionally, the study did not account for the potential impact of climate on patient outcomes, even though heat stroke is a condition associated with climate change. The nomogram-based predictive model also does not incorporate underlying disease factors such as coagulation function, diabetes, and hypertension, which are known to affect prognosis in heat stroke patients. These factors may have an influence on the developed model and its applicability in real-world scenarios. In our study, the inclusion of participants who had previously participated in other research endeavors may introduce external variables, treatment effects, or biases that were not originally accounted for in our study’s design. In order to uphold the reliability of our findings, we opted to exclude those participants who had previously taken part in other studies conducted during the data collection period. The inclusion of participants from prior studies has the potential to introduce confounding factors, which can complicate the analysis and make it difficult to attribute the observed outcomes solely to the variables of interest in our retrospective study. By excluding such participants, our objective was to mitigate potential confounding effects and enhance the clarity and validity of our analysis.
Conclusion
The nomogram developed in this study incorporates three readily available indicators for severe heat stroke and serves as a practical tool for efficiently evaluating patients in a clinical setting. The nomogram provides a straightforward method for assessing the risk level of patients with severe heat stroke. By considering key biomarkers and clinical factors, the nomogram offers clinicians a convenient and effective approach to predicting outcomes and guiding treatment decisions in severe heat stroke cases. The combination of these three risk factors collectively represented the most robust prognostic indicator. Furthermore, a significant advantage of these findings is their swift accessibility.
Abbreviations
ICU, intensive care unit; HS, Heat stroke; CHS, Classical Heatstroke; EHS, Exertional Heatstroke; IQRs, Interquartile Ranges; ROC, Receiver Operating Characteristic; DCA, Decision Curve Analysis; HR, Heart Rate; SBP, Systolic Blood Pressure; DBP, Diastolic Blood Pressure; RR, Heart Rate; ALB, Albumin; PLT, Platelet Count; WBC, White Blood Cell Count; NEUT, Neutrophils; TC, Total Cholesterol; LYM, Lymphocytes; ALP, Alkaline Phosphatase; BUN, Blood Urea Nitrogen; Cr, Creatinine; AST, Aspartate Aminotransferase; ALT, Alanine Aminotransferase; TIBL, Total Bilirubin, DIBL, Direct Bilirubin; Lac, Lactate; PT, Prothrombin Time. SIRS, inflammatory response syndrome AKI, Acute Kidney Injury; ALI, Acute Liver Injury.
Data Sharing Statement
We will share individual deidentified participant data, including clinical measurements, demographic information, and laboratory results, as well as study documents like the protocol and consent forms, through a secure online repository upon publication, and this data will be accessible for a minimum of five years.
Ethical Approval
All procedures performed in this study were accorded with the ethical standards of the West China Hospital (NO: 2022-1542). The study was conducted in accordance with the principles of the Declaration of Helsinki. To ensure participant confidentiality, all data collected were coded and analyzed anonymously.
Acknowledgments
We express our gratitude to the following hospitals for their invaluable assistance and support in our research endeavors: Department Of Critical Care Medicine, The First People’s Hospital Of Ziyang City, Ziyang, China; Department Of Critical Care Medicine, The First People’s Hospital Of Guanghan City, Deyang, China; Department Of Critical Care Medicine, Sichuan Lezhi Hospital Of Traditional Chinese Medicine, Ziyang, China; Department Of Critical Care Medicine, Chengdu Qingbaijiang District People’s Hospital, Chengdu, China; Department Of Critical Care Medicine, Ziyang People’s Hospital, Ziyang, China; Department Of Critical Care Medicine, The Second People’s Hospital Of Neijiang, Neijiang, China; Department Of Critical Care Medicine, Zizhong People’s Hospital, Neijiang, China; Department Of Critical Care Medicine, The People’s Hospital Of Jianyang City, Jianyang, China; Department Of Critical Care Medicine, The People’s Hospital Of Zhongjiang, Deyang, China; Department Of Critical Care Medicine, Hejiang People’s Hospital, Luzhou, China; Department Of Critical Care Medicine, The People’s Hospital Of Jiajiang, Leshan, China; Department Of Critical Care Medicine, Suining Central Hospital, Suining, China; Department Of Critical Care Medicine, The Traditional Chinese Medicine Hospital Of Leshan, Leshan, China;Department Of Critical Care Medicine, The First People’s Hospital Of Longquanyi District, Chengdu, China; Department Of Critical Care Medicine, The Affiliated Hospital Of Southwest Medical University, Luzhou, China; Department Of Critical Care Medicine, Zizhong County Traditional Chinese Medicine Hospital, Neijiang, China; Department Of Critical Care Medicine, Mianyang People’s Hospital, Mianyang, China; Department Of Critical Care Medicine, Yingshan County People’s Hospital, Nanchong, China; Department Of Critical Care Medicine, Anyue Hospital Of Traditional Chinese Medicine, Ziyang, China; Department Of Critical Care Medicine, Guang’an People’s Hospital, Guang’An, China; and all other participating hospitals.
Author Contributions
Lietao Wang, Xin Fu and Min He contributed equally to this work and should be considered as co-first author. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest related to this study.
References
1. Li K, Chen Y. Characterizing the indicator-based, day-and-night, and climate-based variations in response of surface urban heat island during heat wave across global 561 cities. Sustain Cities Soc. 2023;99:104877. doi:10.1016/j.scs.2023.104877
2. Douma MJ, Aves T, Allan KS, et al. First aid cooling techniques for heat stroke and exertional hyperthermia: a systematic review and meta-analysis. Resuscitation. 2020;148:173–190. doi:10.1016/j.resuscitation.2020.01.007
3. Epstein Y, Yanovich R, Longo DL. Heatstroke. N Engl J Med. 2019;380(25):2449–2459. doi:10.1056/NEJMra1810762
4. Bouchama A, Abuyassin B, Lehe C, et al. Classic and exertional heatstroke. Nat Rev Dis Primers. 2022;8(1):8. doi:10.1038/s41572-021-00334-6
5. Fouillet A, Rey G, Laurent F, et al. Excess mortality related to the August 2003 heat wave in France. Int Arch Occup Environ Health. 2006;80(1):16–24. doi:10.1007/s00420-006-0089-4
6. Jones TS, Liang AP, Kilbourne EM, et al. Morbidity and mortality associated with the July 1980 heat wave in St Louis and Kansas City, Mo. JAMA. 1982;247(24):3327–3331. doi:10.1001/jama.1982.03320490025030
7. Wang F, Zhang Y, Li J, Xia H, Zhang D, Yao S. The pathogenesis and therapeutic strategies of heat stroke-induced liver injury. Criti Care. 2022;26(1):391. doi:10.1186/s13054-022-04273-w
8. Gauer R, Meyers BK. Heat-related illnesses. Am Fam Physician. 2019;99(8):482–489.
9. Marchand M, Gin K. The cardiovascular system in heat stroke. CJC Open. 2022;4(2):158–163. doi:10.1016/j.cjco.2021.10.002
10. Laitano O, Oki K, Leon LR. The role of skeletal muscles in exertional heat stroke pathophysiology. Int J Sports Med. 2021;42(8):673–681. doi:10.1055/a-1400-9754
11. Ogden HB, Child RB, Fallowfield JL, Delves SK, Westwood CS, Layden JD. The gastrointestinal exertional heat stroke paradigm: pathophysiology, assessment, severity, aetiology and nutritional countermeasures. Nutrients. 2020;12(2):537. doi:10.3390/nu12020537
12. Sasai F, Roncal-Jimenez C, Rogers K, et al. Climate change and nephrology. Nephrol Dial Transplant. 2023;38(1):41–48. doi:10.1093/ndt/gfab258
13. Semenza JC, Rubin CH, Falter KH, et al. Heat-related deaths during the July 1995 heat wave in Chicago. N Engl J Med. 1996;335(2):84–90. doi:10.1056/nejm199607113350203
14. Bobb JF, Obermeyer Z, Wang Y, Dominici F. Cause-specific risk of hospital admission related to extreme heat in older adults. JAMA. 2014;312(24):2659–2667. doi:10.1001/jama.2014.15715
15. Chalise SN, Mirza E, Malik R. Heat stroke leading to a fatal outcome. Cureus. 2023;15(1):e33226. doi:10.7759/cureus.33226
16. González-Alonso J, Quistorff B, Krustrup P, Bangsbo J, Saltin B. Heat production in human skeletal muscle at the onset of intense dynamic exercise. J Physiol. 2000;524 Pt 2(Pt 2):603–615. doi:10.1111/j.1469-7793.2000.00603.x
17. Kültz D. Molecular and evolutionary basis of the cellular stress response. Annu Rev Physiol. 2005;67:225–257. doi:10.1146/annurev.physiol.67.040403.103635
18. Roberts GT, Ghebeh H, Chishti MA, et al. Microvascular injury, thrombosis, inflammation, and apoptosis in the pathogenesis of heatstroke: a study in baboon model. Arterioscler Thromb Vasc Biol. 2008;28(6):1130–1136. doi:10.1161/atvbaha.107.158709
19. Richter K, Haslbeck M, Buchner J. The heat shock response: life on the verge of death. Mol Cell. 2010;40(2):253–266. doi:10.1016/j.molcel.2010.10.006
20. Bouchama A, Roberts G, Al Mohanna F, et al. Inflammatory, hemostatic, and clinical changes in a baboon experimental model for heatstroke. J Appl Physiol. 2005;98(2):697–705. doi:10.1152/japplphysiol.00461.2004
21. King MA, Leon LR, Morse DA, Clanton TL. Unique cytokine and chemokine responses to exertional heat stroke in mice. J Appl Physiol. 2017;122(2):296–306. doi:10.1152/japplphysiol.00667.2016
22. Iwaniec J, Robinson GP, Garcia CK, et al. Acute phase response to exertional heat stroke in mice. Exp Physiol. 2021;106(1):222–232. doi:10.1113/ep088501
23. Dehbi M, Uzzaman T, Baturcam E, Eldali A, Ventura W, Bouchama A. Toll-like receptor 4 and high-mobility group box 1 are critical mediators of tissue injury and survival in a mouse model for heatstroke. PLoS One. 2012;7(9):e44100. doi:10.1371/journal.pone.0044100
24. Dehbi M, Baturcam E, Eldali A, et al. Hsp-72, a candidate prognostic indicator of heatstroke. Cell Stress Chaperones. 2010;15(5):593–603. doi:10.1007/s12192-010-0172-3
25. Tong H, Wan P, Zhang X, et al. Vascular endothelial cell injury partly induced by mesenteric lymph in heat stroke. Inflammation. 2014;37(1):27–34. doi:10.1007/s10753-013-9708-x
26. Chen HS, Tong HS, Zhao Y, Hong CY, Bin JP, Su L. Differential expression pattern of exosome long non-coding RNAs (lncRNAs) and MicroRNAs (miRNAs) in vascular endothelial cells under heat stroke. Med Sci Monit. 2018;24:7965–7974. doi:10.12659/msm.909983
27. Huang W, Mao L, Xie W, et al. Impact of UCP2 depletion on heat stroke-induced mitochondrial function in human umbilical vein endothelial cells. Int J Hyperthermia. 2022;39(1):287–296. doi:10.1080/02656736.2022.2032846
28. Thongprayoon C, Petnak T, Kanduri SR, et al. Impact of rhabdomyolysis on outcomes of hospitalizations for heat stroke in the United States. Hosp Pract. 2020;48(5):276–281. doi:10.1080/21548331.2020.1792214
29. Clarkson PM, Kearns AK, Rouzier P, Rubin R, Thompson PD. Serum creatine kinase levels and renal function measures in exertional muscle damage. Med Sci Sports Exerc. 2006;38(4):623–627. doi:10.1249/01.mss.0000210192.49210.fc
30. Laitano O, Sheikh LH, Mattingly AJ, Murray KO, Ferreira LF, Clanton TL. Osmolality selectively offsets the impact of hyperthermia on mouse skeletal muscle in vitro. Front Physiol. 2018;9:1496. doi:10.3389/fphys.2018.01496
31. Hyatt HW, Powers SK. The role of Calpains in skeletal muscle remodeling with exercise and inactivity-induced atrophy. Int J Sports Med. 2020;41(14):994–1008. doi:10.1055/a-1199-7662
32. Xue L, Guo W, Li L, et al. Metabolomic profiling identifies a novel mechanism for heat stroke‑related acute kidney injury. Mol Med Rep. 2021;23(4). doi:10.3892/mmr.2021.11880
33. Fan H, Zhao Y, Zhu JH, et al. Thrombocytopenia as a predictor of severe acute kidney injury in patients with heat stroke. Ren Fail. 2015;37(5):877–881. doi:10.3109/0886022x.2015.1022851
34. Thongprayoon C, Qureshi F, Petnak T, et al. Impact of acute kidney injury on outcomes of hospitalizations for heat stroke in the United States. Diseases. 2020;8(3):28. doi:10.3390/diseases8030028
35. Wen FL, Xu YJ, Xue LE, et al. Proteomics analyses of acute kidney injury biomarkers in a rat exertional heat stroke model. Front Physiol. 2023;14:1176998. doi:10.3389/fphys.2023.1176998
36. Satirapoj B, Kongthaworn S, Choovichian P, Supasyndh O. Electrolyte disturbances and risk factors of acute kidney injury patients receiving dialysis in exertional heat stroke. BMC Nephrol. 2016;17(1):55. doi:10.1186/s12882-016-0268-9
37. Goto H, Shoda S, Nakashima H, et al. Early biomarkers for kidney injury in heat-related illness patients: a prospective observational study at Japanese Self-Defense Force Fuji Hospital. Nephrol Dial Transplant. 2023;38(3):644–654. doi:10.1093/ndt/gfac166
38. Glaser J, Lemery J, Rajagopalan B, et al. Climate change and the emergent epidemic of CKD from heat stress in rural communities: the case for heat stress nephropathy. Clin J Am Soc Nephrol. 2016;11(8):1472–1483. doi:10.2215/cjn.13841215
39. Sato Y, Roncal-Jimenez CA, Andres-Hernando A, et al. Increase of core temperature affected the progression of kidney injury by repeated heat stress exposure. Am J Physiol Renal Physiol. 2019;317(5):F1111–f1121. doi:10.1152/ajprenal.00259.2019
40. Bi X, Deising A, Frenette C. Acute liver failure from exertional heatstroke can result in excellent long-term survival with liver transplantation. Hepatology (Baltimore, Md). 2020;71(3):1122–1123. doi:10.1002/hep.30938
41. Kew M, Bersohn I, Seftel H, Kent G. Liver damage in heatstroke. Am J Med. 1970;49(2):192–202. doi:10.1016/s0002-9343(70)80075-4
42. Sun J, Zhang J, Wang X, et al. Gut-liver crosstalk in sepsis-induced liver injury. Criti Care. 2020;24(1):614. doi:10.1186/s13054-020-03327-1
43. Ribeiro F, Bibi M, Pereira M, Ferreira S, Pessegueiro H, Araújo R. Severe acute liver injury related to heat stroke. Eur J Case Rep Intern Med. 2020;7(2):001382. doi:10.12890/2020_001382
44. Schlader ZJ, Davis MS, Bouchama A. Biomarkers of heatstroke-induced organ injury and repair. Exp Physiol. 2022;107(10):1159–1171. doi:10.1113/ep090142
45. O’Donnell TF
46. Clemens MM, McGill MR, Apte U. Mechanisms and biomarkers of liver regeneration after drug-induced liver injury. Adv Pharmacol. 2019;85:241–262. doi:10.1016/bs.apha.2019.03.001
47. Chinnappan R, Mir TA, Alsalameh S, et al. Low-cost point-of-care monitoring of ALT and AST is promising for faster decision making and diagnosis of acute liver injury. Diagnostics. 2023;13(18):2967. doi:10.3390/diagnostics13182967
48. Chinnappan R, Mir TA, Alsalameh S, et al. Aptasensors are conjectured as promising ALT and AST diagnostic tools for the early diagnosis of acute liver injury. Life. 2023;13(6):1273. doi:10.3390/life13061273
49. Austin MG, Berry JW. Observations on one hundred cases of heatstroke. J Am Med Assoc. 1956;161(16):1525–1529. doi:10.1001/jama.1956.02970160005002
50. Donham BP, Frankfurt SB, Cartier RA, O’Hara SM, Sieg VC. Low incidence of death and renal failure in United States military service members hospitalized with exertional heat stroke: a retrospective cohort study. Mil Med. 2020;185(Suppl 1):362–367. doi:10.1093/milmed/usz214
51. Misset B, De Jonghe B, Bastuji-Garin S, et al. Mortality of patients with heatstroke admitted to intensive care units during the 2003 heat wave in France: a national multiple-center risk-factor study. Crit Care Med. 2006;34(4):1087–1092. doi:10.1097/01.Ccm.0000206469.33615.02
52. Sprung CL. Hemodynamic alterations of heat stroke in the elderly. Chest. 1979;75(3):362–366. doi:10.1378/chest.75.3.362
53. Al-Harthi SS, El-Deane MSS, Akhtar J, Al-Nozha MM. Hemodynamic changes and intravascular hydration state in heat stroke. Ann Saudi Med. 1989;9(4):378–383. doi:10.5144/0256-4947.1989.378
54. Dahmash NS, Al Harthi SS, Akhtar J. Invasive evaluation of patients with heat stroke. Chest. 1993;103(4):1210–1214. doi:10.1378/chest.103.4.1210
55. Blumlein D, Griffiths I. Shock: aetiology, pathophysiology and management. Br J Nurs. 2022;31(8):422–428. doi:10.12968/bjon.2022.31.8.422
56. Standl T, Annecke T, Cascorbi I, Heller AR, Sabashnikov A, Teske W. The nomenclature, definition and distinction of types of shock. Dtsch Arztebl Int. 2018;115(45):757–768. doi:10.3238/arztebl.2018.0757
57. Suresh MR, Chung KK, Schiller AM, Holley AB, Howard JT, Convertino VA. Unmasking the hypovolemic shock continuum: the compensatory reserve. J Intensive Care Med. 2019;34(9):696–706. doi:10.1177/0885066618790537
58. Kashani K, Omer T, Shaw AD. The intensivist’s perspective of shock, volume management, and hemodynamic monitoring. Clin J Am Soc Nephrol. 2022;17(5):706–716. doi:10.2215/cjn.14191021
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Model That Predicts the Risk of Diabetic Nephropathy in Type 2 Diabetes Mellitus Patients: A Cross-Sectional Study
Yang J, Jiang S
International Journal of General Medicine 2022, 15:5089-5101
Published Date: 20 May 2022
Paraspinal Muscle Degeneration: A Potential Risk Factor for New Vertebral Compression Fractures After Percutaneous Kyphoplasty
Si F, Yuan S, Zang L, Fan N, Wu Q, Wang T, Wang A
Clinical Interventions in Aging 2022, 17:1237-1248
Published Date: 13 August 2022
Tracking Epidemiological Characteristics and Risk Factors of Multi-Drug Resistant Bacteria in Intensive Care Units
Wu C, Lu J, Ruan L, Yao J
Infection and Drug Resistance 2023, 16:1499-1509
Published Date: 15 March 2023
Construction and Validation of a Novel Nomogram for Predicting the Recurrence of Diffuse Large B Cell Lymphoma Treated with R-CHOP
Gong Y, Yan H, Yang Y, Zhai B, Huang Z, Zhang Z
Pharmacogenomics and Personalized Medicine 2023, 16:291-301
Published Date: 1 April 2023
Development and Validation of a Prediction Model for Intensive Care Unit-Acquired Weakness in Adult Patients with Sepsis: A Prospective, Observational, Single-Center Study
Wang B, Liu Y, He G, Sun S, Han J, Zhang M, He L, Meng S
International Journal of General Medicine 2026, 19:569937
Published Date: 14 April 2026