Back to Journals » Journal of Inflammation Research » Volume 18
Development and Internal Validation of a Nomogram for Predicting Acute Kidney Injury After Cardiac Valve Surgery Using the Serum Uric Acid-to-Albumin Ratio
Authors Zhao X ![]() , Wang J, Bai W, Zhang W, Huang C, Qin Z, Wei K, Han M
, Wang J, Bai W, Zhang W, Huang C, Qin Z, Wei K, Han M ![]() , Yan L, Gu Y, Shao F
, Yan L, Gu Y, Shao F
Received 4 September 2025
Accepted for publication 24 November 2025
Published 28 November 2025 Volume 2025:18 Pages 16747—16760
DOI https://doi.org/10.2147/JIR.S563670
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Wenjian Li
Xiaoru Zhao,1,* Juntao Wang,2,* Wenxin Bai,1 Wenwen Zhang,1 Chunling Huang,1 Zengyuan Qin,1 Kaiyue Wei,1 Minghui Han,1,3 Lei Yan,1,3 Yue Gu,1,3 Fengmin Shao1,3
1Department of Nephrology, Zhengzhou University People’s Hospital, Henan Provincial People’s Hospital, Zhengzhou, Henan, People’s Republic of China; 2Department of Nephrology, The First People’s Hospital of Shangqiu, Shangqiu, Henan, People’s Republic of China; 3Henan Provincial Clinical Research Center for Kidney Disease, Henan Provincial Key Laboratory of Kidney Disease and Immunology, Henan Provincial People’s Hospital, Zhengzhou, Henan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fengmin Shao; Yue Gu, Email [email protected]; [email protected]
Background: The serum Uric Acid-to-Albumin Ratio (sUAR) is a novel inflammatory indicator. We aimed to construct and validate a prediction model for acute kidney injury (AKI) following cardiac valve surgery (CVS) based on the preoperative sUAR.
Methods: We retrospectively collected clinical data from adult patients undergoing CVS with cardiopulmonary bypass at the Heart Center of Henan Provincial People’s Hospital between December 2020 to December 2021. The primary outcome was postoperative AKI, defined according to the KDIGO creatinine criteria. Patients were categorized as either AKI or non-AKI based on this outcome. Multivariate logistic regression to identify independent risk factors. A nomogram model was developed. The receiver operating characteristic (ROC) curve assessed discrimination. The calibration curve and Hosmer-Lemeshow test evaluated calibration. Clinical practicability was assessed through decision curve analysis (DCA) and clinical impact curve (CIC). The Bootstrap method was used for internal verification.
Results: A total of 440 patients were enrolled, and the incidence of AKI was 33.4%. Multivariate analysis revealed that sUAR (per μmol/g, OR=1.467, 95% CI 1.311– 1.642, P< 0.001), age (per 10 years, OR=1.612, 95% CI 1.261– 2.062, P< 0.001), atrial fibrillation (OR=2.485, 95% CI 1.573– 3.924, P< 0.001), hemoglobin (per g/L, OR=0.985, 95% CI 0.973– 0.998, P=0.025) were the independent risk factors. The nomogram based on sUAR achieved an area under the curve (AUC) of 0.779 (95% CI 0.734– 0.824, P< 0.001) for predicting AKI. The average AUC after internal validation of the nomogram model was 0.776 (95% CI 0.767– 0.779). The calibration curve and Hosmer-Lemeshow test indicated that the predicted and observed results agreed well, while the DCA and CIC curves demonstrated favorable clinical applicability within a specific threshold range.
Conclusion: The prediction model incorporating sUAR provides reliable discrimination and clinical utility for assessing AKI risk following CVS.
Keywords: acute kidney injury, prediction model, cardiac valve surgery, serum uric acid-to-albumin ratio, nomogram
Introduction
Acute kidney injury (AKI) is a serious complication following cardiac surgery in the intensive care unit (ICU).1,2 According to previous reports, the incidence of cardiac surgery-associated AKI (CSA-AKI) varies between 5% to 49%.3,4 Increased postoperative mortality, longer ICU stays, and higher health care costs are all correlated with CSA-AKI.4,5 Given the current dearth of clinically applicable interventions for CSA-AKI, early recognition of high-risk groups is essential for both CSA-AKI prevention and therapy. Several AKI-risk prediction models for cardiac surgery have been identified,6–8 such as the Cleveland Clinic Score,9 the Mehta score,10 the AKICS Score,11 and the Simplified Renal Index score.12 These models provide an important foundation for clinical risk assessments. However, these models have not been widely used in clinical practice.6,7 A nomogram is a graphical calculation tool that shows the contribution of each predictive factor to the overall risk visually, offering superior interpretability and ease of use compared to complex algorithmic scores.13 This approach facilitates rapid, visual risk assessments at the bedside, which is crucial for timely clinical decision-making.13,14
Previous studies have indicated that preoperative high uric acid (UA) and low albumin (ALB) levels are significant risk factors.15–17 The serum Uric Acid-to-Albumin Ratio (sUAR),18 a composite indicator integrating both serum UA and ALB. It is linked to both AKI development and mortality in ICU patients, and has also been described as a novel inflammatory indicator for AKI.18,19 Recent research has reported that elevated sUAR was a risk factor for post-contrast AKI.18 AKI incidence is relatively high in cardiac valve surgery (CVS), which is a common cardiac surgical procedure performed under cardiopulmonary bypass (CPB).20 The establishment of existing AKI clinical prediction models for cardiac surgery often requires a considerable number of variables, and these models have not incorporated sUAR. As a composite biomarker, the sUAR could provide a more integrative and robust risk assessment than single and conventional indicators, potentially leading to good predictive performance for AKI after CVS. Currently, the relationship between sUAR and AKI after CVS has not been investigated. It remains uncertain whether the sUAR can predict AKI following CVS. This study aims to explore the correlation between sUAR and postoperative AKI, and to build a nomogram model for AKI following CVS based on sUAR, with the expectation of providing a basis for the early intervention of AKI following CVS in clinical practice.
Methods
Study Population
During the period from December 2020 to December 2021, adult patients undergoing CVS at the Heart Center of Henan Provincial People’s Hospital were enrolled in this retrospective study. The inclusion criteria were: (1) elective CVS under CPB; (2) age ≥18 years old. The exclusion criteria were: (1) estimated glomerular filtration rate (eGFR)<60 mL·min−1·(1.73m2)−1, chronic kidney disease (CKD), dialysis before the operation, renal transplant patients, patients with preoperative AKI, or kidney stone patients; (2) patients with chronic liver disease, gout, malignant tumors, severe infection, infective endocarditis, and autoimmune disease; (3) intraoperative or within the first 24 hours postoperative death; (4) underwent coronary artery bypass graft (CABG) surgery during the same period; (5) patients with missing preoperative serum creatinine (SCr), UA, ALB or postoperative SCr.
Data Collection
All of the enrolled patients’ clinical data were collected. Preoperative clinical data included age, gender, comorbidities, the latest preoperative laboratory blood biochemical parameters, and so on. Intraoperative clinical data included CPB time, type of valve surgery (valvuloplasty, single valve replacement, double valve replacement). Based on the latest preoperative SCr, the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula was used to calculate the eGFR.21 The sUAR was calculated as the serum UA/ALB. To decrease the influence of extreme values and reduce skewness, the concentration of N-terminal pro-B-type natriuretic peptide (NT-proBNP) was natural log transformed.22
Definition of Postoperative AKI
Postoperative AKI was defined as a ≥26.5 μmol/L increase in SCr within 48h, or an increase in SCr to ≥1.5 times baseline within 7 days, based on the KDIGO guidelines in 2012.23 As the urine output data were not precisely recorded for patients, the urine output criteria were not used.
Grouping
Patients were assigned to the AKI and non-AKI groups based on the occurrence of AKI during the seven days after CVS. The latest preoperative SCr was used as the baseline SCr.
Sample Size
A priori sample size justification: We performed a sample size calculation using the method proposed by Riley et al and implemented in the pmsampsize R package.24 According to a previous study,25 we assumed that the incidence of AKI following CVS was 0.346, the target C-statistic for the model was set to 0.814, and six parameters were intended to be included. The calculation indicated that the minimum sample size required for new model development was 348. Therefore, our final sample size of 440 met this requirement.
Events-Per-Parameter (EPP) evaluation: The primary binary outcome (postoperative AKI) occurred in 147 patients (events, E), and the total number of parameters (P) was four in our final model (the continuous variables sUAR, age, and HGB contributed three parameters, and the categorical variable AF with two levels contributed one parameter). Consequently, the EPP ratio in our study was 147/4=36.75, which met the conventional criterion of EPP≥10.24
Study Protocol
This study was conducted in accordance with the Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis (TRIPOD) and Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.26,27
Statistical Analysis
SPSS 26.0, MedCalc 20.022, and R 4.5.0 were used for statistical analyses. A P value <0.05 was considered statistically significant (two-tailed). We used the mean value imputation or median imputation to handle missing values based on the distribution of the variables, since only five continuous variables with less than 1% missing data in this study. Categorical variables were compared using the Chi-square test and presented as frequencies with percentages. According to the Shapiro–Wilk test, continuous variables were expressed as mean ± standard deviation or median (25th and 75th percentiles) and compared using the independent samples t-test or Mann–Whitney U-test. Variables with P<0.05 in the univariate analysis of the study were selected for univariate logistic regression analysis. Variables with P < 0.05 and no evidence of collinearity in the univariate logistic regression analysis were then added to the multivariate stepwise logistic regression model (forward: conditional) to identify independent risk factors of AKI following CVS and build a nomogram prediction model. Variance inflation factor (VIF) was used to quantify multicollinearity, and thresholds were set at VIF<5, which indicated weak collinearity. The restricted cubic spline (RCS) analysis was applied to assess the potential relationships between the continuous predictors and AKI risk. To enhance the clinical meaningfulness of odds ratios (ORs), the effect estimates for sUAR, age, and hemoglobin (HGB) were expressed in increments of 1 μmol/g,10 years, and 1 g/L, respectively, in multivariate analysis. These increments were set according to the previous literature.18,28,29
The predictive power was assessed by the area under the receiver operating characteristic (ROC) curve (AUC). The difference in AUC was compared by the DeLong test. The calibration curve and the Hosmer-Lemeshow test were applied to evaluate the calibration. The clinical practicability was assessed by the decision curve analysis (DCA) and clinical impact curve (CIC). The model was internally validated with 1000 bootstrap resamplings.
Results
Clinical Data Comparison
The analysis included 440 eligible patients in total (Figure 1). Of these, 147 patients (33.4%) developed postoperative AKI, 87 (19.8%) stage I AKI, 42 (9.5%) stage II AKI, and 18 (4.1%) stage III AKI. AKI patients were older, had higher preoperative levels of urea, SCr, UA, blood glucose, LnNT-proBNP, and sUAR, and had a larger percentage of atrial fibrillation (AF) than non-AKI patients, while the preoperative levels of eGFR, lymphocyte (LY), HGB, and serum ALB were lower (all P<0.05) (Table 1).
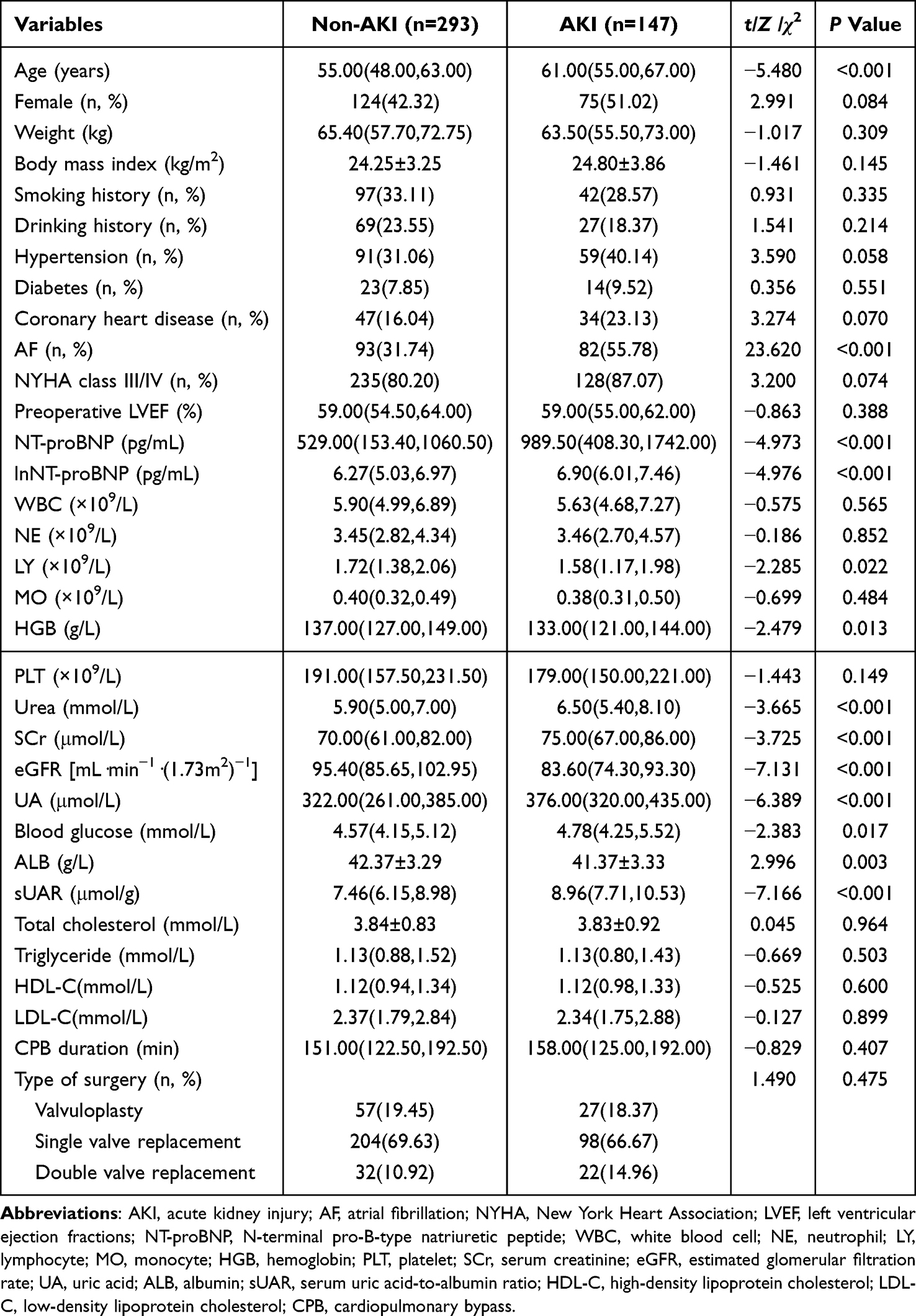 |
Table 1 Comparison of the Variables Between the AKI and Non-AKI Groups |
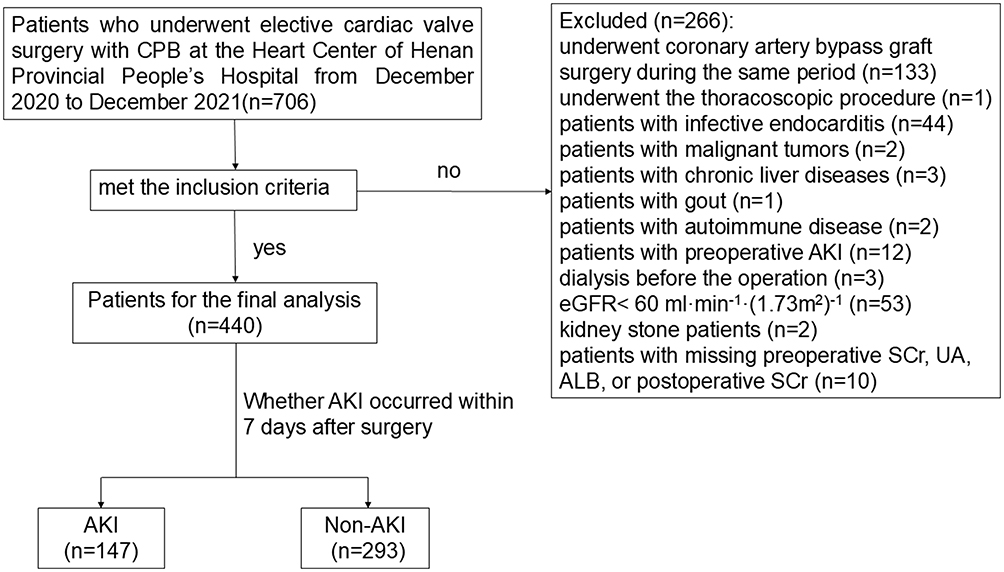 |
Figure 1 Study enrollment flowchart. |
Variable Screening
The univariate logistic regression analysis included variables in Table 1 with P<0.05, and the results showed that advanced age, AF, preoperative LnNT-proBNP, HGB, urea, SCr, eGFR, UA, blood glucose, ALB, and sUAR were influencing factors for AKI following CVS (Table 2). Based on the results displayed in Table 2 and the collinearity analysis (Table S1), the variables of age, AF, preoperative LnNT-proBNP, HGB, urea, SCr, eGFR, blood glucose, and sUAR were included in the multivariate analysis, indicating that the high preoperative sUAR (per μmol/g, odds ratio [OR]=1.467, 95% confidence interval [CI] 1.311–1.642, P<0.001), advanced age (per 10 years, OR=1.612, 95% CI 1.261–2.062, P<0.001), AF (per g/L, OR=2.485, 95% CI 1.573–3.924, P<0.001), and low HGB (OR=0.985, 95% CI 0.973–0.998, P=0.025) were independent risk factors for AKI following CVS (Table 3). As shown in Figure S1, the RCS curve demonstrated that there were no non-linear relationships between sUAR (P for nonlinear=0.191), age (P for nonlinear=0.516), HGB (P for nonlinear=0.432), and AKI risk.
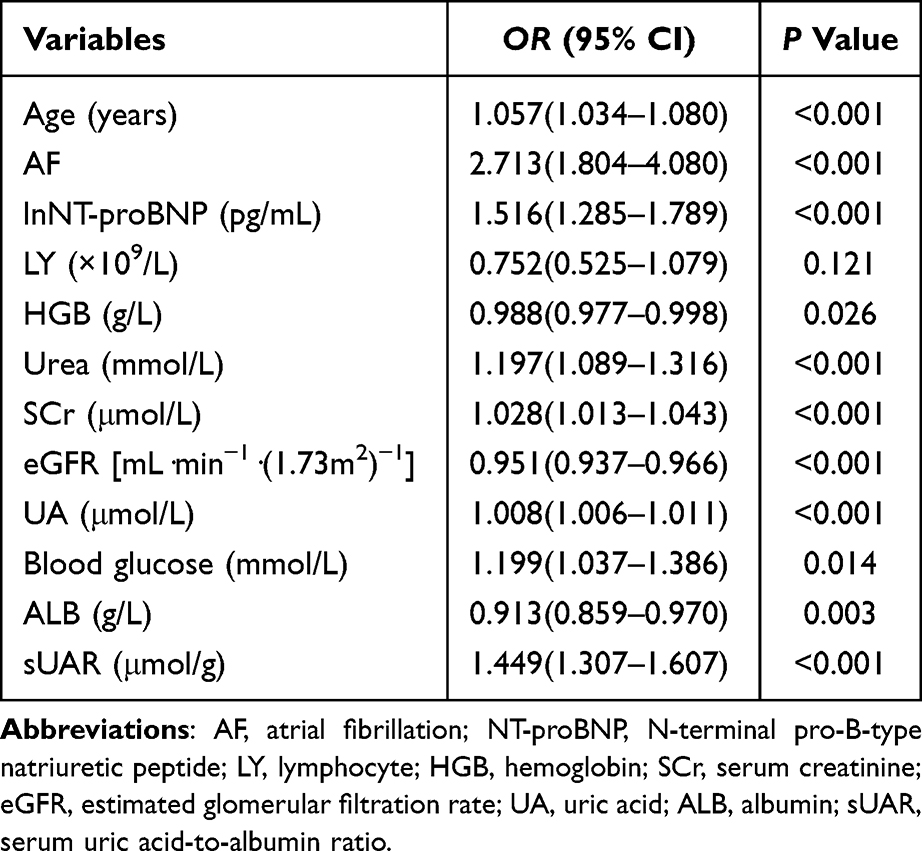 |
Table 2 Univariate Logistic Regression Analysis |
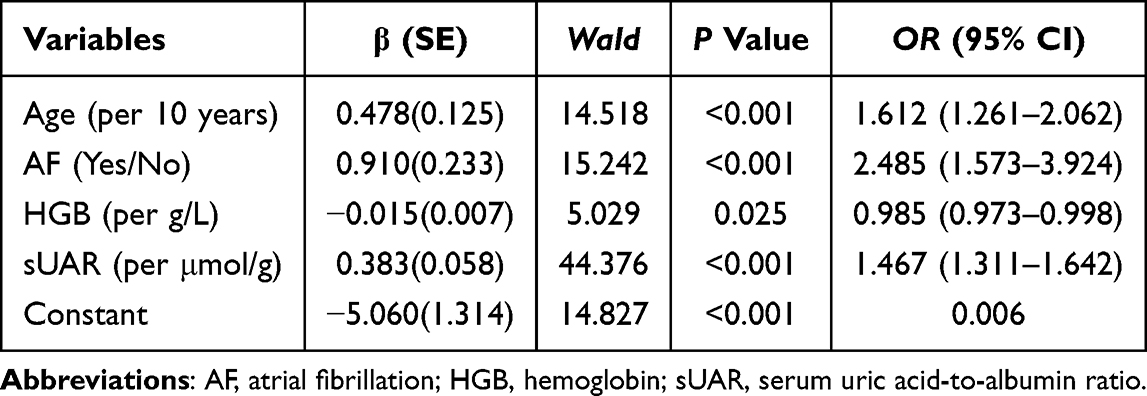 |
Table 3 Multivariate Logistic Regression Analysis |
Development and Validation of Nomogram Prediction Model
Predictive Ability
The AUCs of age, AF, HGB, and sUAR were 0.660 (95% CI 0.607–0.713, P<0.001), 0.620 (95% CI 0.572–0.669, P<0.001), 0.572 (95% CI 0.515–0.603, P=0.013), and 0.709 (95% CI 0.660–0.759, P<0.001), respectively. The evaluation metrics were summarized in Table 4.
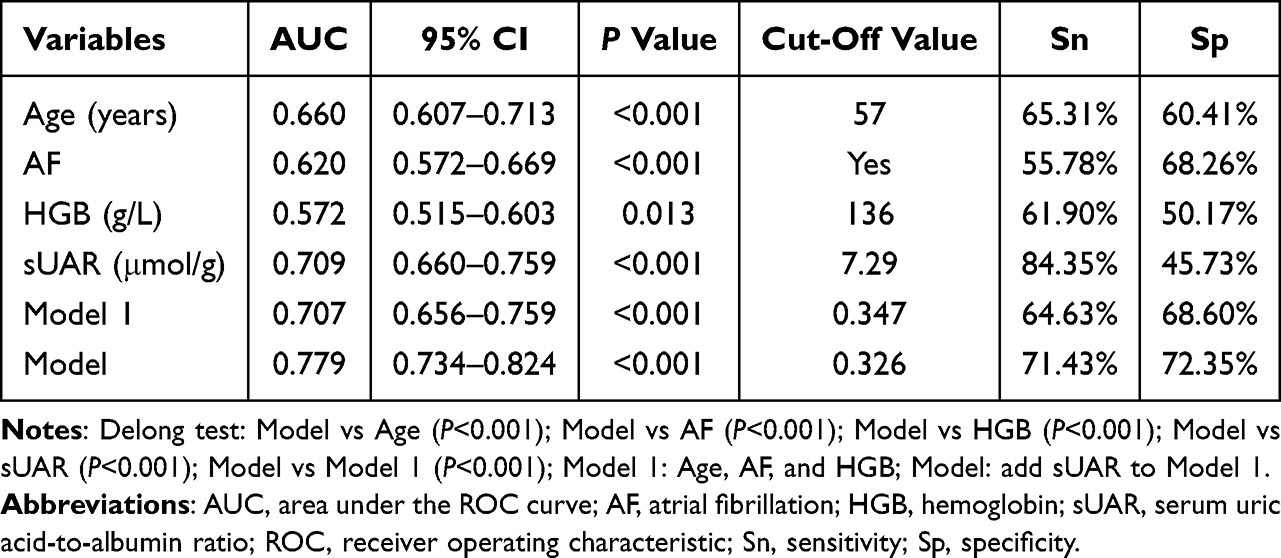 |
Table 4 Predictive Value of Age, AF, HGB, sUAR, Model 1, and Model |
In addition, we compared the sUAR with UA and ALB. The results showed that the AUC of the sUAR was greater than that of UA (AUC=0.687, 95% CI 0.636–0.737) and ALB (AUC=0.588, 95% CI 0.532–0.644) alone (Figure S2 and Table S2).
We constructed model 1 combined with age, AF, and HGB, and then added the sUAR to model 1 to construct the final model. Comparative analysis showed that the AUC of the final model (AUC=0.779, 95% CI 0.734–0.824) was superior to that of model 1(AUC=0.707, 95% CI 0.656–0.759), and the difference is statistically significant (P<0.001), indicating that the sUAR enhanced the model’s discriminatory ability. Using the DeLong test, we further compared the model’s predictive ability with that of sUAR, age, AF, and HGB. The results demonstrated that the model’s AUC was also superior to those of sUAR, age, AF, and HGB (Figure 2 and Table 4).
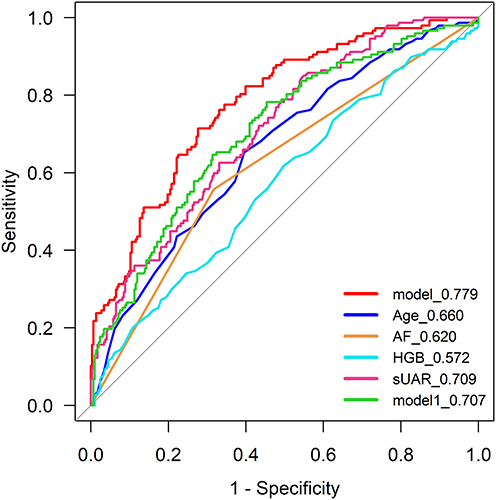 |
Figure 2 ROC curve for predicting AKI. Notes: model1: Age, AF, and HGB; model: add sUAR to model 1. |
Therefore, we built a nomogram model based on the sUAR, age, AF, and HGB (Figure 3). ROC analysis revealed that the model’s AUC was 0.779 (95% CI 0.734–0.824, P<0.001) (Figure 2 and Table 4). And the model’s average AUC was 0.776 (95% CI 0.767–0.779) following internal validation (Figure 4), suggesting that the model had good discrimination capacity.
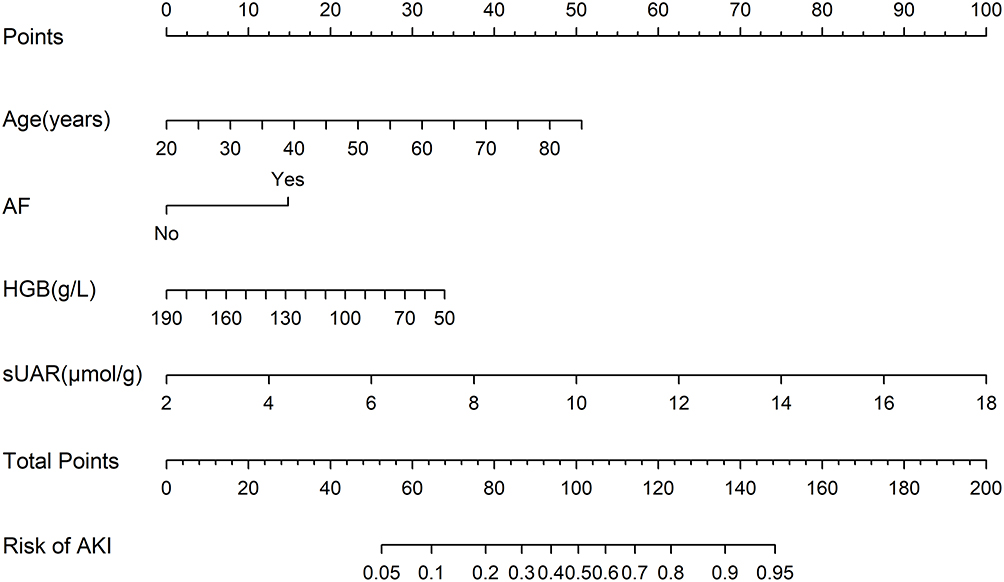 |
Figure 3 Nomogram for predicting AKI following cardiac valve surgery. |
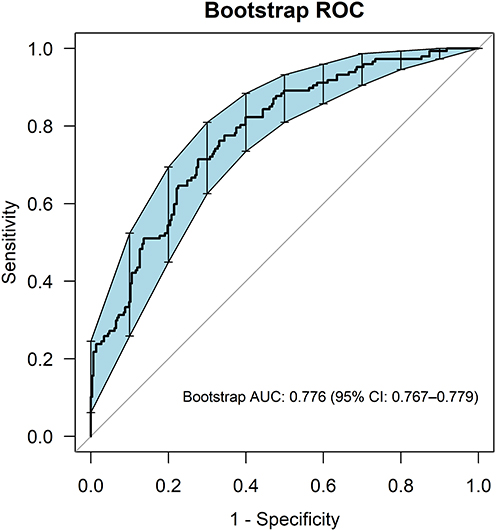 |
Figure 4 ROC curve for bootstrap validation. |
Calibration Degree
The model’s calibration and ideal curve were found to be reasonably consistent in the calibration plot (Bootstrap method, n=1000) (Figure 5). Combined with the result of the Hosmer-Lemeshow test (χ2=6.795, P=0.559) and Figure S3 (intercept: −0.00, slope: 1.00), suggesting that the predicted and actual probabilities agreed well.
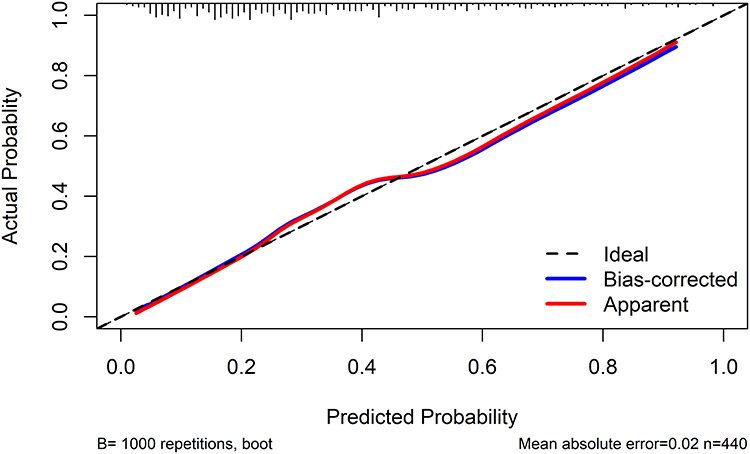 |
Figure 5 Calibration curve of the nomogram prediction model for AKI. |
Clinical Practicability
DCA demonstrated that when the threshold probability fell between 0.09 and 0.99, the model had a good net benefit in predicting AKI following CVS (Figure 6). In a similar vein, CIC demonstrated that the nomogram was clinically useful within certain threshold probabilities (Figure 7).
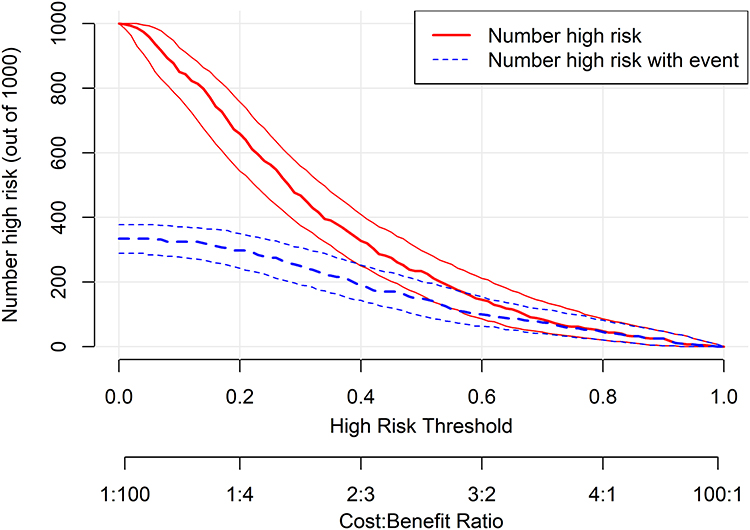 |
Figure 6 Decision curve analysis (DCA) of the Nomogram prediction model. |
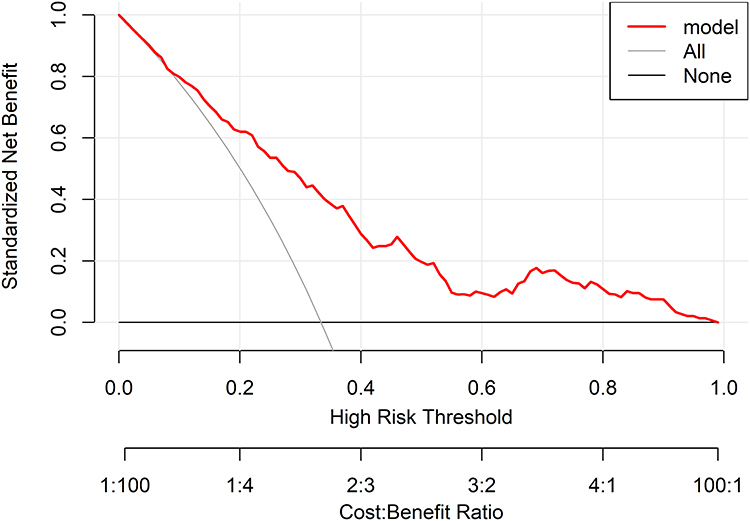 |
Figure 7 Clinical impact curve (CIC) of the Nomogram prediction model. |
Discussion
Following cardiac surgery, CSA-AKI is a common complication that is related to longer hospital stays, worse short and long-term prognoses, and increased treatment costs.3–5 In patients undergoing CVS, postoperative AKI is more likely to occur.30 Thereby, it is especially crucial to screen AKI risk factors following CVS, recognize high-risk groups early, and carry out reasonable intervention to minimize postoperative AKI incidence.31
It demonstrates that the sUAR was an independent indicator of AKI after CVS in this study. In addition, age, AF, and HGB were also identified as independent influencing factors of postoperative AKI in this study. Internal validation demonstrated that the prediction model established based on sUAR had good discrimination and calibration, while DCA and CIC indicated that the model was clinically useful. This model demonstrated a good predictive ability in predicting AKI following CVS, which could assist medical staff in recognizing high-risk patients of AKI and formulating personalized treatment plans.
Some studies have found that serum UA and serum ALB were independently associated indicators of AKI.32–34 According to earlier research, decreased serum ALB and elevated serum UA were risk factors for AKI following cardiac surgery.35–39 In AKI patients after non-cardiac surgery, the preoperative serum ALB levels were low.40 In this study, we discovered that preoperative serum UA and ALB were the influencing factors of postoperative AKI. sUAR is calculated from serum UA and ALB. In ICU patients, sUAR was related to AKI.19 Recent studies have shown that sUAR is a good predictor of post-contrast AKI.18,41 In our study, the AUC for sUAR was 0.709 (P<0.001), indicating that sUAR had a moderate predictive value for AKI following CVS. The exact mechanisms by which elevated sUAR levels affect the development of AKI after CVS are still unknown. The functions that serum UA and ALB may help explain why. Firstly, UA has characteristics of both an antioxidant and a pro-oxidant agent. Elevated UA levels are linked to inflammation and oxidative stress, as well as renin-angiotensin system activation, nitric oxide system inhibition, endothelial dysfunction, and renal dysfunction.36,38,42–44 Secondly, serum ALB has antioxidant activity and can reduce the necrosis of renal tubular cells; its elevated metabolism and decreased synthesis indicate an inflammatory state.34,45 Finally, the pathogenesis of AKI following CVS is complex, and many factors play significant roles in its development and occurrence, such as inflammation, ischemia-reperfusion damage, hemolysis, hypoperfusion, oxidative stress, and so on.4,46 Therefore, sUAR is a composite indicator of inflammation and oxidative stress, which could be the possible mechanism for the correlation between sUAR and AKI after CVS.
This study found that AF was an independent risk factor. According to a previous report, patients with AF at admission had a 2.6 times greater incidence of AKI during hospitalization compared to those with sinus rhythm.47 Because AF reduces the cardiac output, it leads to systemic congestion,48,49 which, in turn, causes the renal venous pressure to increase and then results in the renal perfusion pressure decreasing. Since GFR is primarily determined by renal perfusion pressure, AF’s damage to glomerular perfusion can lead to renal function impairment.50 Additionally, AF causes activation of the neurohormonal system, such as the renin-angiotensin-aldosterone pathway,51 which might negatively impact renal function if sustained. Furthermore, AF may result in thromboembolism, which can lead to renal infarction.50 Other independent risk factors in this study included age and preoperative HGB, which were consistent with previous studies.4,28,46 According to previous studies, prolonged CPB time was considered a risk factor for AKI.52 It could be due to the relatively small sample size that we were unable to find a statistically significant difference in CPB time between AKI patients and non-AKI patients after surgery.
Several clinical prediction models for AKI risk assessment following cardiac surgery have been identified.6,8–12 The Cleveland Clinic Score,9 a classic renal risk score for cardiac surgery, was established to predict AKI requiring dialysis following cardiac surgery.8,15 These prediction models provide an important foundation for AKI risk assessments. However, these risk scores incorporate multiple clinical risk factors that do not include the sUAR, and the collection and calculation processes are rather complex. Accordingly, they have not been widely used in clinical practice.7,15 In addition, the [TIMP2] × [IGFBP7],53 comprising urine biomarkers reflecting early renal tubular cell injury, has been widely studied to identify severe AKI risk.46,54 However, the widespread adoption of these markers could be limited by costs and the need for specialized testing platforms. In our study, the AUC of the sUAR was superior to that of UA and ALB alone. Additionally, ROC curve analysis showed that the predictive performance of the model containing the sUAR was improved compared with that of the model without the sUAR. These results indicated that the sUAR provides a practical tool for clinicians to assess the risk of postoperative AKI in CVS patients before surgery. The AUC for the nomogram model based on the sUAR was 0.779 (95% CI 0.734–0.824), and the average AUC after internal validation of the nomogram model was 0.776 (95% CI 0.767–0.779), indicating that the nomogram model had a moderate predictive value for AKI following CVS. The UA and ALB tests required for the sUAR are routine laboratory items in most hospitals worldwide, which is highly conducive to the sUAR’s promotion and popularization in clinical environments with diverse resources. In addition, the sUAR, as a novel composite predictor, uniquely links two critical pathways involved in the development of AKI—systemic stress and inflammation. It further integrates systemic information that is often overlooked by existing risk scores, thereby providing pathophysiological insights beyond SCr and eGFR. Moreover, it also offers powerful clinical interpretability. An increase in the sUAR directly informs the clinician of either elevated UA (implying oxidative stress and inflammation) or reduced ALB (reflecting poor nutrition or inflammation), providing direct evidence for personalized patient management. Of course, there are some scenarios where the sUAR may be misleading; therefore, sUAR must be interpreted with caution in clinical practice. For instance, in patients with severe hypoalbuminemia due to acute systemic infection, an elevated sUAR may be primarily driven by a sharp decline in ALB levels, which may reflect the severity of the acute inflammatory response, rather than direct kidney injury. Consequently, a comprehensive assessment based on the overall clinical context is essential.
Limitations and Future Directions
The results of this study provide warning signs for patients at a high risk of AKI after CVS. In the future, the prediction model can be embedded into the electronic medical record system to achieve automatic calculations. For high-risk patients identified by the model before the operation, the system will automatically issue an alarm and trigger a standardized bundle of postoperative nephroprotective measures, such as optimizing hemodynamics, avoiding nephrotoxic drugs, and closely monitoring SCr and urine output.46 This series of active renal protection intervention measures would reduce the incidence of postoperative AKI and improve patient outcomes. Most importantly, a prospective, interventional randomized controlled trial will be essential for validating the clinical utility of our model.
It has some limitations in this study. First, it was a single-center retrospective study. As such, it was unable to completely rule out the impact of some unmeasured confounding variables. Second, some cases were excluded due to missing variables and the sample size’s relative limitations, which could result in a certain degree of bias. Exclusion of CKD, combined CABG, and other patients may introduce bias, and therefore, our results may not apply to these higher-risk groups. External validation in multicenter studies involving more diverse populations is required in the future. Third, as patients’ urine output data were not recorded, AKI was diagnosed only using the SCr criteria, and the urine output criteria were not used. Future prospective validation using the full KDIGO criteria is necessary. Fourth, it was unable to compare our model directly against established renal risk scores for cardiac surgery due to missing data for several key variables. A future prospective study, designed to collect all necessary data for a head-to-head comparison against risk scores such as the Cleveland Clinic Score, is essential to definitively establish the clinical utility and incremental benefit of sUAR. Besides, it is also necessary to prospectively study whether the combination of sUAR and other biomarkers (such as [TIMP2] × [IGFBP7]) can improve the prediction of AKI after cardiac surgery. Finally, there is a lack of external validation of the prediction model, which requires further verification from other centers.
Conclusion
The elevated preoperative sUAR was independently associated with a high risk of AKI following CVS. The prediction model constructed based on sUAR has good predictive value and clinical applicability, which can assist medical professionals in recognizing patients at a greater risk of AKI early during the perioperative period and take corresponding intervention measures to reduce postoperative AKI risk and improve prognosis. Before being put into clinical application, prospective and multi-center studies are still needed to externally validate this model.
Data Sharing Statement
The data supporting the research results of this study can be obtained from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The Medical Ethics Committee of Henan Provincial People’s Hospital approved the study (approval number: 2020-Lunshen-206). The ethics committee waived the informed consent, since the study was retrospective in nature. The data were anonymous, and all personal identifiers were removed before analysis to ensure patient confidentiality. This study was conducted according to the Declaration of Helsinki.
Author Contributions
Xiaoru Zhao: Conceptualization, Formal analysis, Investigation, Writing–Original Draft. Juntao Wang: Conceptualization, Formal analysis, Investigation, Writing–Original Draft. Wenxin Bai: Investigation, Formal analysis, Data Curation. Wenwen Zhang: Methodology, Data Curation. Chunling Huang: Formal analysis, Investigation. Zengyuan Qin: Investigation, Formal analysis. Kaiyue Wei: Methodology, Investigation. Minghui Han: Validation, Data Curation, Formal analysis, Software, Visualization. Lei Yan: Methodology, Writing–Review & Editing. Yue Gu: Supervision, Resources, Conceptualization. Fengmin Shao: Supervision, Resources, Conceptualization, Project administration, Funding Acquisition. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. All authors gave final approval of the version to be published.
Funding
This work was supported by the Funding of Zhongyuan Scholar Workstation (No. 234400510024), Henan Provincial Major Science and Technology Project (No. 241100310100), Technology Attack Plan Project of Henan Province (No. 242102311062), and Medical Science and Technology Attack Plan Project of Henan Province (No. SBGJ202302002).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mariscalco G, Lorusso R, Dominici C, Renzulli A, Sala A. Acute kidney injury: a relevant complication after cardiac surgery. Ann Thorac Surg. 2011;92(4):1539–1547. doi:10.1016/j.athoracsur.2011.04.123
2. Kumar AB, Suneja M. Cardiopulmonary bypass-associated acute kidney injury. Anesthesiology. 2011;114(4):964–970. doi:10.1097/ALN.0b013e318210f86a
3. Thiele RH, Isbell JM, Rosner MH. AKI associated with cardiac surgery. Clin J Am Soc Nephrol. 2015;10(3):500–514. doi:10.2215/cjn.07830814
4. Wang Y, Bellomo R. Cardiac surgery-associated acute kidney injury: risk factors, pathophysiology and treatment. Nat Rev Nephrol. 2017;13(11):697–711. doi:10.1038/nrneph.2017.119
5. Lau D, Pannu N, James MT, et al. Costs and consequences of acute kidney injury after cardiac surgery: a cohort study. J Thorac Cardiovasc Surg. 2021;162(3):880–887. doi:10.1016/j.jtcvs.2020.01.101
6. Cheruku SR, Raphael J, Neyra JA, Fox AA. Acute Kidney Injury after Cardiac Surgery: prediction, Prevention, and Management. Anesthesiology. 2023;139(6):880–898. doi:10.1097/aln.0000000000004734
7. McIlroy DR. Predicting acute kidney injury after cardiac surgery: much work still to be done. Br J Anaesth. 2021;127(6):825–828. doi:10.1016/j.bja.2021.09.005
8. Tseng PY, Chen YT, Wang CH, et al. Prediction of the development of acute kidney injury following cardiac surgery by machine learning. Crit Care. 2020;24(1):478. doi:10.1186/s13054-020-03179-9
9. Thakar CV, Arrigain S, Worley S, Yared JP, Paganini EP. A clinical score to predict acute renal failure after cardiac surgery. J Am Soc Nephrol. 2005;16(1):162–168. doi:10.1681/asn.2004040331
10. Mehta RH, Grab JD, O’Brien SM, et al. Bedside tool for predicting the risk of postoperative dialysis in patients undergoing cardiac surgery. Circulation. 2006;114(21):2208–2216;quiz2208. doi:10.1161/circulationaha.106.635573
11. Palomba H, de Castro I, Neto AL, Lage S, Yu L. Acute kidney injury prediction following elective cardiac surgery: AKICS Score. Kidney Int. 2007;72(5):624–631. doi:10.1038/sj.ki.5002419
12. Wijeysundera DN, Karkouti K, Dupuis JY, et al. Derivation and validation of a simplified predictive index for renal replacement therapy after cardiac surgery. JAMA. 2007;297(16):1801–1809. doi:10.1001/jama.297.16.1801
13. Bonnett LJ, Snell KIE, Collins GS, Riley RD. Guide to presenting clinical prediction models for use in clinical settings. BMJ. 2019;365:737. doi:10.1136/bmj.l737
14. Li X, Wang X, Yan B, et al. Development and validation of a nomogram for predicting calcification of arteriovenous access in hemodialysis patients. Ren Fail. 2025;47(1):2542980. doi:10.1080/0886022x.2025.2542980
15. Pan L, Deng Y, Dai S, et al. Development and internal validation of a prediction model for acute kidney injury following cardiac valve replacement surgery. Int J Cardiol. 2023;370:345–350. doi:10.1016/j.ijcard.2022.10.147
16. Hu P, Mo Z, Chen Y, et al. Derivation and validation of a model to predict acute kidney injury following cardiac surgery in patients with normal renal function. Ren Fail. 2021;43(1):1205–1213. doi:10.1080/0886022x.2021.1960563
17. Hu P, Chen Y, Wu Y, et al. Development and validation of a model for predicting acute kidney injury after cardiac surgery in patients of advanced age. J Card Surg. 2021;36(3):806–814. doi:10.1111/jocs.15249
18. Zhang Y, Xu Z, He W, et al. Elevated Serum Uric Acid/Albumin Ratio as a Predictor of Post-Contrast Acute Kidney Injury After Percutaneous Coronary Intervention in Patients with ST-Segment Elevation Myocardial Infarction. J Inflamm Res. 2022;15:5361–5371. doi:10.2147/jir.S377767
19. Yeter HH, Eyupoglu D, Pasayev T, Cetik S, Akcay OF, Yildirim T. Role of Uric Acid Albumin Ratio in Predicting Development of Acute Kidney Injury and Mortality in Intensive Care Unit Patients. Turkish J Nephrol. 2019;28(3):160–167. doi:10.5152/turkjnephrol.2019.3416
20. Xu J, Jiang W, Shen B, et al. Acute Kidney Injury in Cardiac Surgery. Contrib Nephrol. 2018;193:127–136. doi:10.1159/000484969
21. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–612. doi:10.7326/0003-4819-150-9-200905050-00006
22. Wang C, Gao Y, Tian Y, et al. Prediction of acute kidney injury after cardiac surgery from preoperative N-terminal pro-B-type natriuretic peptide. Br J Anaesth. 2021;127(6):862–870. doi:10.1016/j.bja.2021.08.015
23. Kellum JA, Lameire N. Diagnosis, evaluation, and management of acute kidney injury: a KDIGO summary (Part 1). Crit Care. 2013;17(1):204. doi:10.1186/cc11454
24. Riley RD, Ensor J, Snell KIE, et al. Calculating the sample size required for developing a clinical prediction model. BMJ. 2020:
25. Jia X, Ma J, Qi Z, Zhang D, Gao J. Development and validation of a prediction model for acute kidney injury following cardiac valve surgery. Front Med Lausanne. 2025;12:1528147. doi:10.3389/fmed.2025.1528147
26. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–1457. doi:10.1016/s0140-6736(07)61602-x
27. Collins GS, Moons KGM, Dhiman P, et al. TRIPOD+AI statement: updated guidance for reporting clinical prediction models that use regression or machine learning methods. BMJ. 2024:
28. Che M, Li Y, Liang X, et al. Prevalence of acute kidney injury following cardiac surgery and related risk factors in Chinese patients. Nephron Clin Pract. 2011;117(4):c305–311. doi:10.1159/000321171
29. Di Pierro M, Pozzi M, Frazzei M, et al. Hemolysis Index and Cardiopulmonary Bypass Time as Predictors of Cardiac Surgery-associated Acute Kidney Injury: an Observational Cohort Study. J Cardiothorac Vasc Anesth. 2025;39(11):2953–2962. doi:10.1053/j.jvca.2025.07.038
30. Grayson AD, Khater M, Jackson M, Fox MA. Valvular heart operation is an independent risk factor for acute renal failure. Ann Thorac Surg. 2003;75(6):1829–1835. doi:10.1016/s0003-4975(03)00166-8
31. Jiang Y, Song Y. Analysis of Risk Factors and Intervention Strategies for Acute Kidney Injury After Cardiac Valve Replacement. J Inflamm Res. 2023;16:3523–3529. doi:10.2147/jir.S425485
32. Ejaz AA, Johnson RJ, Shimada M, et al. The Role of Uric Acid in Acute Kidney Injury. Nephron. 2019;142(4):275–283. doi:10.1159/000499939
33. Hahn K, Kanbay M, Lanaspa MA, Johnson RJ, Ejaz AA. Serum uric acid and acute kidney injury: a mini review. J Adv Res. 2017;8(5):529–536. doi:10.1016/j.jare.2016.09.006
34. Wiedermann CJ, Wiedermann W, Joannidis M. Hypoalbuminemia and acute kidney injury: a meta-analysis of observational clinical studies. Intensive Care Med. 2010;36(10):1657–1665. doi:10.1007/s00134-010-1928-z
35. Wei XB, Jiang L, Liu YH, et al. Serum uric acid as a simple risk factor in patients with rheumatic heart disease undergoing valve replacement surgery. Clin Chim Acta. 2017;472:69–74. doi:10.1016/j.cca.2017.07.019
36. Lapsia V, Johnson RJ, Dass B, et al. Elevated uric acid increases the risk for acute kidney injury. Am J Med. 2012;125(3):302.e309–317. doi:10.1016/j.amjmed.2011.06.021
37. Lee EH, Choi JH, Joung KW, et al. Relationship between Serum Uric Acid Concentration and Acute Kidney Injury after Coronary Artery Bypass Surgery. J Korean Med Sci. 2015;30(10):1509–1516. doi:10.3346/jkms.2015.30.10.1509
38. Kaufeld T, Foerster KA, Schilling T, et al. Preoperative serum uric acid predicts incident acute kidney injury following cardiac surgery. BMC Nephrol. 2018;19(1):161. doi:10.1186/s12882-018-0970-x
39. Lee EH, Baek SH, Chin JH, et al. Preoperative hypoalbuminemia is a major risk factor for acute kidney injury following off-pump coronary artery bypass surgery. Intensive Care Med. 2012;38(9):1478–1486. doi:10.1007/s00134-012-2599-8
40. Li N, Qiao H, Guo JF, et al. Preoperative hypoalbuminemia was associated with acute kidney injury in high-risk patients following non-cardiac surgery: a retrospective cohort study. BMC Anesthesiol. 2019;19(1):171. doi:10.1186/s12871-019-0842-3
41. Şaylık F, Çınar T, Akbulut T, Selçuk M. Serum Uric Acid to Albumin Ratio Can Predict Contrast-Induced Nephropathy in ST-Elevation Myocardial Infarction Patients Undergoing Primary Percutaneous Coronary Intervention. Angiology. 2023;74(1):70–78. doi:10.1177/00033197221091605
42. Filiopoulos V, Hadjiyannakos D, Vlassopoulos D. New insights into uric acid effects on the progression and prognosis of chronic kidney disease. Ren Fail. 2012;34(4):510–520. doi:10.3109/0886022x.2011.653753
43. Yu MA, Sánchez-Lozada LG, Johnson RJ, Kang DH. Oxidative stress with an activation of the renin-angiotensin system in human vascular endothelial cells as a novel mechanism of uric acid-induced endothelial dysfunction. J Hypertens. 2010;28(6):1234–1242.
44. Borghi C, Agabiti-Rosei E, Johnson RJ, et al. Hyperuricaemia and gout in cardiovascular, metabolic and kidney disease. Eur J Intern Med. 2020;80:1–11. doi:10.1016/j.ejim.2020.07.006
45. Don BR, Kaysen G. Serum albumin: relationship to inflammation and nutrition. Semin Dial. 2004;17(6):432–437. doi:10.1111/j.0894-0959.2004.17603.x
46. Yu Y, Li C, Zhu S, et al. Diagnosis, pathophysiology and preventive strategies for cardiac surgery-associated acute kidney injury: a narrative review. Eur J Med Res. 2023;28(1):45. doi:10.1186/s40001-023-00990-2
47. Wang G, Yang L, Ye N, et al. In-hospital acute kidney injury and atrial fibrillation: incidence, risk factors, and outcome. Ren Fail. 2021;43(1):949–957. doi:10.1080/0886022x.2021.1939049
48. Hsu LF, Jaïs P, Sanders P, et al. Catheter ablation for atrial fibrillation in congestive heart failure. N Engl J Med. 2004;351(23):2373–2383. doi:10.1056/NEJMoa041018
49. Manning WJ, Silverman DI, Katz SE, et al. Impaired left atrial mechanical function after cardioversion: relation to the duration of atrial fibrillation. J Am Coll Cardiol. 1994;23(7):1535–1540. doi:10.1016/0735-1097(94)90652-1
50. Park S, Lee S, Kim Y, et al. Atrial fibrillation and kidney function: a bidirectional Mendelian randomization study. Eur Heart J. 2021;42(29):2816–2823. doi:10.1093/eurheartj/ehab291
51. Collard D, van Brussel PM, van de Velde L, et al. Estimation of Intraglomerular Pressure Using Invasive Renal Arterial Pressure and Flow Velocity Measurements in Humans. J Am Soc Nephrol. 2020;31(8):1905–1914. doi:10.1681/asn.2019121272
52. Jin J, Chang SC, Shen B, et al. Usefulness of High Estimated Pulmonary Artery Systolic Pressure to Predict Acute Kidney Injury After Cardiac Valve Operations. Am J Cardiol. 2019;123(3):440–445. doi:10.1016/j.amjcard.2018.10.023
53. Liu KD, Vijayan A, Rosner MH, Shi J, Chawla LS, Kellum JA. Clinical adjudication in acute kidney injury studies: findings from the pivotal TIMP-2*IGFBP7 biomarker study. Nephrol Dial Transplant. 2016;31(10):1641–1646. doi:10.1093/ndt/gfw238
54. Zarbock A, Küllmar M, Ostermann M, et al. Prevention of Cardiac Surgery-Associated Acute Kidney Injury by Implementing the KDIGO Guidelines in High-Risk Patients Identified by Biomarkers: the PrevAKI-Multicenter Randomized Controlled Trial. Anesth Analg. 2021;133(2):292–302. doi:10.1213/ane.0000000000005458
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Predicting the Risk of Unplanned Readmission at 30 Days After PCI: Development and Validation of a New Predictive Nomogram
Xu W, Tu H, Xiong X, Peng Y, Cheng T
Clinical Interventions in Aging 2022, 17:1013-1023
Published Date: 5 July 2022
Development and Validation of a Nomogram for Predicting 28-Day Mortality on Admission in Elderly Patients with Severe Community-Acquired Pneumonia
Song Y, Wang X, Lang K, Wei T, Luo J, Song Y, Yang D
Journal of Inflammation Research 2022, 15:4149-4158
Published Date: 21 July 2022
A Predictive Model Based on Inflammatory and Coagulation Indicators for Sepsis-Induced Acute Kidney Injury
Xin Q, Xie T, Chen R, Zhang X, Tong Y, Wang H, Wang S, Liu C, Zhang J
Journal of Inflammation Research 2022, 15:4561-4571
Published Date: 11 August 2022
Development and Validation of a Prediction Model for Chronic Post-Surgical Pain After Thoracic Surgery in Elderly Patients: A Retrospective Cohort Study
Wu XD, Zeng FF, Yu XX, Yang PP, Wu JP, Xv P, Wang HT, Pei YM
Journal of Pain Research 2022, 15:3079-3091
Published Date: 29 September 2022
Risk Factors for Granulomatous Mastitis and Establishment and Validation of a Clinical Prediction Model (Nomogram)
Zeng Y, Zhang D, Fu N, Zhao W, Huang Q, Cui J, Chen Y, Liu Z, Zhang X, Zhang S, Mansoor KM
Risk Management and Healthcare Policy 2023, 16:2209-2222
Published Date: 20 October 2023